ENT -lecture1
36
ANATOMY THE EXTERNAL EAR CONSISTS OF TWO PARTS THE 1 THE AURICLE 2 THE EXTERNAL ACOUSTIC MEATUS & EXTERNAL AUDITORY CANAL THE AURICLE & THE EXTERNAL MEATUS ARISE FROM THE SIX AURICULAR ECTODERMAL TUBERCLES WHICH FUSE AT THE 6 TH WEEK OF IU LIFE
Transcript of ENT -lecture1
ANATOMY
THE EXTERNAL EAR CONSISTS OF TWO PARTS THE
1 THE AURICLE2 THE EXTERNAL ACOUSTIC MEATUS &
EXTERNAL AUDITORY CANAL
THE AURICLE & THE EXTERNAL MEATUS ARISE FROM THE SIX AURICULAR ECTODERMAL TUBERCLES WHICH FUSE AT THE 6TH WEEK OF IU LIFE
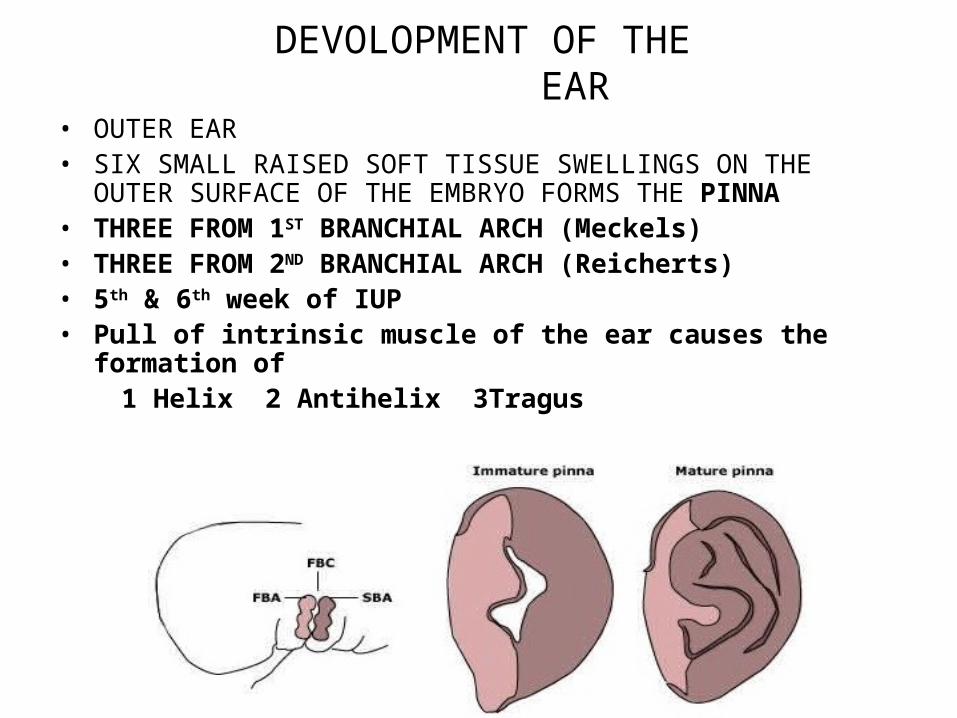
DEVOLOPMENT OF THE EAR
• OUTER EAR• SIX SMALL RAISED SOFT TISSUE SWELLINGS ON THE OUTER SURFACE OF
THE EMBRYO FORMS THE PINNA• THREE FROM 1ST BRANCHIAL ARCH (Meckels)• THREE FROM 2ND BRANCHIAL ARCH (Reicherts)• 5th & 6th week of IUP• Pull of intrinsic muscle of the ear causes the formation of 1 Helix 2 Antihelix 3Tragus
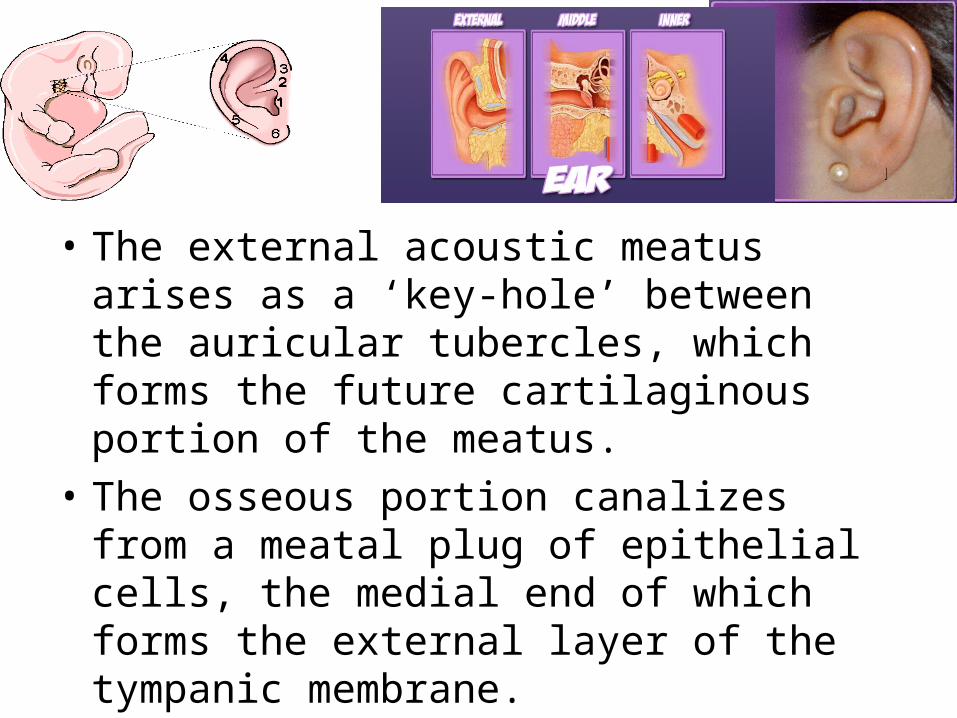
• The external acoustic meatus arises as a ‘key-hole’ between the auricular tubercles, which forms the future cartilaginous portion of the meatus.
• The osseous portion canalizes from a meatal plug of epithelial cells, the medial end of which forms the external layer of the tympanic membrane.
EXTERNAL EAR
• The ear canal is formed from an invagination of surface epithelium in the fifth week of intrauterine life .It is filled with a solid core of epithelium.
• Canalistion of the external ear canal occurs in the 2nd trimester and approximately ends at the 28th week of gestation
• This solid core of cells meets a similar evagination from the pharynx, trapping inbetween a layer of mesothelium
Fusion of these cells at the juncture results in the formation of the three layers of the tympanic membrane
MALFORMATIONS OF THE EXTERNAL EAR
• TYPES OF MALFORMATIONS• SIZE OF AURICLE• Microtia small ear• Macrotia large ear• Anotia absence of ear
• SHAPE OF THE EAR• Cup-shaped• Lop ear• Dysplastic elfin ear –pointed• Lobe malformations
• POSITION OF THE EAR• Melotia- low set ears --ear located on the cheek due to lack of aural ascent• Synotia –ears are very close to each other in the midline
• AURICULAR FISTULAS & SINUS , AURICULAR APPENDAGES
•
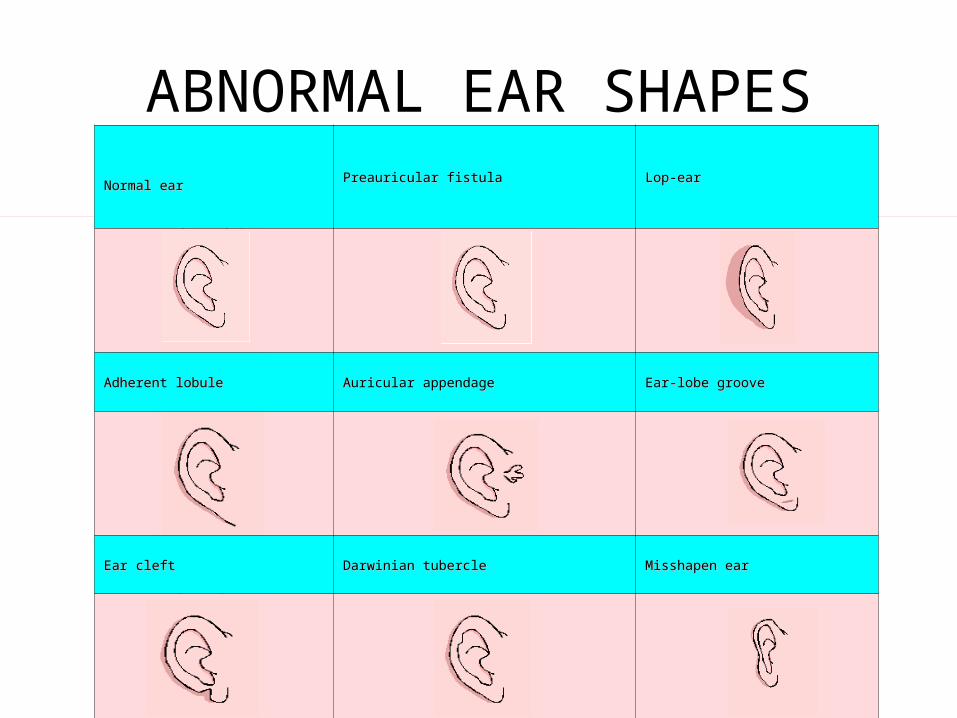
ABNORMAL EAR SHAPESNormal earNormal ear
Preauricular fistulaPreauricular fistula Lop-earLop-ear
Adherent lobuleAdherent lobule Auricular appendageAuricular appendage Ear-lobe grooveEar-lobe groove
Ear cleftEar cleft Darwinian tubercleDarwinian tubercle Misshapen earMisshapen ear
CAUSES OF MALFORMATIONS
• Malformations of the auricle and bony meatal atresia are often combined and may be associated with anomalies of the middle and internal ear.
• They often form part of many chromosomal anomalies and syndromes.
• GENETIC DEFECTS • VIRUS OR TOXIC EFFECTS OF DRUGS DURING PREGNANCY
PREAURICULAR SINUS• BLIND TRACTS IN FRONT OF THE EAR• DUE TO NON FUSION OF THE TUBERCLES• WHEN INFECTED THEY WILL HAVE SYMPTOMS.• ↑ RISE IN TEMPERATURE• PAIN• SWELLING • DISCHARGE• Tr -- antibiotic, analgesics ,• after symptoms subside• tract is outlined by dye and excision is done• healing takes place by secondary intention with • scar formation
COLLAURAL FISTULA• IT IS AN ANOMALY OF THE 1ST BRANCHIAL CLEFT
• ONE OPENING IN THE FOOR OF THE EXT.AUDITORY MEATUS
• ANOTHER BEHIND THE ANGLE OF THE MANDIBLE CLOSE TO THE ANTERIOR BORDER OF THE STERNOMASTOIDTHE TRACT PASSES THROUGH THE PAROTID IN CLOSE PROXIMITY TO THE
FACIAL NERVE
Tr--- EXCISION OF THE TRACT
Congenital swelling of the pinna
• Dermoid cyst (mature skin, hair ,sweat gland, teeth nails etc.)• Tr –Excision under anaesthesia• Haemangioms &lymphangiomas vascular & lymphatic malformations• Tr -- Sclerotic agents are injected and
then excision done under anaesthesia
NORMAL PINNA
CONDITIONS OF PINNA &EXTERNAL AUDITORY MEATUS
• 1 CONGENITAL• 2 INFLAMMATORY• 3 INFECTIVE• 4 REACTIVE• 5 TRAUMATIC• 6 TUMOURS OF THE EXT EAR BENIGN & MALIGNANT• 7 MISCELLANEOUS
CongenitalAnomalies of the auricle Microtia• Definition: Microtia means small ears. microtia transmitted as a dominant and rather harmless trait to severe
forms with conductive hearing loss. Pathogenesis: Abnormal development of the first and second branchial
arches. • Associated anomalies: Commonly associated is Hemifacial microsomia: consisting of unilateral microtia, macrostomia and failure of formation of
the mandibular ramus and condyle.
Macrotia:• Definition: Macrotia means large ears. The auricle is usually very large
but well shaped without other ear malformations. The most exaggerated portion is the scaphoid fossa.
• The condition is usually bilateral and symmetric and may cause psychological disturbance due to excessive size of the ears.
Anotia• Definition: Complete absence of the auricle. Skin of
the cheek passes smoothly over the aural area without definite elevation or depression.
Extremely rare, sporadic and usually unilateral. May be associated with facial paralysis and absence of the tonsil on the abnormal side.
• Cup-shaped ear Definition: Small auricles that grow forward over the
meatus.• Lop ear Definition: The external ear stands away from the
head at a greater angle • (Normal angle of the auricle to the median plane
averages 25 degrees in boys and 18 degrees in girls). Lop ears are usually larger than normal ears.
• Bat ear –abnormal anteriorly placed pinna• Tr –surgery at the age of SIX• Melotia – displacement of the pinna caudally• Polyotia – multiple tags of skin &cartilage around pinna ,can be seen on a line drawn from tragus to angle of mouth• Wildermuth,s ear (Mozart’s ear) here antihelix is more prominent than the helix. Lobe may be absent or adherent to the skin of neck
• Darwin’s tubercle – small elevation on the posterosuperior part of the helix
It is an inherited condition• Treacher Collins Syndrome or Mandibulo facial dystosis it is autosomal dominant condition—1st & 2nd
arch Anomalies present are:Microtia + congenital atresia of ext. auditory canalHypoplasia of mandible + middle 3rd of face + malar prominenceAntimongoloid palpabral fissuresNotching of lower eye lid + atrophic lid margins• Conductive deafness• down-slanting eyes • notched lower eyelids • underdevelopment or absence of cheekbones and the side wall and
floor of the eye socket • lower jaw is often small and slanting • forward hair in the sideburn area • underdeveloped, malformed and / or prominent ears
Tr – by plastic surgery constructive procedures
Congenital atresia of Ext.auditory meatus
• The canal is formed in the 24 wk of IU life Middle and inner ear – 1st trimester• Failure to canalize ,outer meatus may be filled
with fibrous tissue or boneTr– excision of the tissue recanalisation with split skin graft
INFLAMMATORY CONDITIONS
ERYSIPELAS—St Anthony’s fire Streptococcus haemolyticus infection of skinof pinnaRed raised ,oedematous eruptionsSharply defined edgesSevere malaise & temperature Tr –Large doses of penicillin antiinflammatory drugs
PERICHONDRITIS• INFLAMMATION OF THE PERICHONDRIUM COVERING THE CARTILAGE OF PINNA• IT MAY BE A SEQUELAE TO TRAUMA→HAEMATOMA→INFECTION OTITIS EXTERNA FURUNCLE OF PINNA OPERATIONS INVOLVING CUTTING OF CARTILAGE WHILE INFECTION IS PRESENTs/s UNIFORM ENLARGEMENT OF PINNA SURFACE RED & SHINY SEVERE PAIN FEVER , MALAISE & BODY ACHESRecurrent infection →cauliflower ear ( boxer,s ear)Tr– broad spectrum antibiotics –amoxycillin, ciprofloxacillin ,tinidazole or inj. gentamycin 80 mg anti inflammatory drugs local dressing of magnesium sulphate or ecthyol in glycerine. If abscess has formed I & D
INFECTIVE CONDITIONSOF EXT. AUDITORY MEATUS • FURUNCULOSIS • IT IS A STAPHYLOCCOCAL INFECTION OF THE HAIR FOLLICLES (CATILGENOUS
PART)• S/s –Severe pain→ jaw & head• Swelling of the canal• Tragus sign+• Hearing normal• On examination bursting point seen in ext. auditory canal• Tympanic membrane normal• Postauricular sulcus obliterated if infection spreads posteriorly• Regional lymph nodes tender & palpableTr -- Diabetes to be ruled out in recurrent cases Broad spectrum antibiotics Anti-inflammatory drugs Meatus packed with antibiotic steroid cream (also acts as splint to the cartilage & counter pressure for tension) Hot fomentation locally Surgical intervention not required Precaution –not to meddle with the external Auditory canal while healing is taking
place
OTITIS EXTERNA• GENERALISED INFECTION OF THE SKIN OF THE EXTERNAL CANAL by
staphylococci, Streptococci haemolyticus ,Pseudomonas pyocyanea ,B. proteus & E. coli
• ACUTE OR CHRONIC• PREDISPOSING FACTOR –hot & humid weather (Singapore ear )• Scratching with dirty nails & objects• Bathing in dirty swimming pools• Allergic diathesis (tendency)• Excessive sweating, changes the Ph to alkaline favouring growth of
organismsS/S Pain or discomfort ,serous discharge, debris in the canal No hearing loss oedema ,redness, tenderness of pinna ( circumduction sign)Tr – Systemic antibiotics Anti inflammatory drugs Wick soaked in antibiotic & steroid cream Avoid predisposing factors
Malignant otitis externa or necrotising otitis externa
• Fulminating type of otitis externa caused by pseudomonas –seen mostly in diabetic patients.
• It can occur in patients taking immunosuppressive drugs like, methotrxate , cyclophosphamide , cyclosporine etc.
• In patients on steroid therapy or having hypogammaglobulinaemia
S/S destruction of tissues of canal ,pre &post auricular areas by enzymes like lecithinase and haemolysins, infection may spread to the base of skull & jugular foramen causing cranial nerve palsiesTr--- Heavy doses of antibiotics like gentamycin, tobramycin,
cefotaxime 1gm iv/im twice daily Local debridement of tissue & bone &control of diabetesMortality rate is high
Otomycosis• It is a fungal infection of the external auditory canal• Aspergillus fumigatus or Aspergillus Niger• Candida albicans• Wet blotting paper like debris seen in the canal S/S occurs in hot humid conditions irritation ,itching ,dull pain & discharge sense of blockade with mild conductive deafnessTr--- keep the ear dry remove fungal mass by syringing spirit cleaning antifungal drops –clotrimazole or 2% salicylic acid in alcohol local application of gention violet amphotericinB can be used in resistant cases
Viral infections• Herpes zoster oticus or Ramsay Hunt syndrome• Affects the 7th cranial nerve• 5th 9th 10th cranial nerves also may be involved• Chicken pox virus (varicella) is the cause ,attacks the geniculate ganglion• Tr– Antibiotics to avoid secondary infection• Antiviral drugs—aclovir 800mg 4-5times a day• Antiinflammatory drugs• Corticosteroids as tablets or cream• Management of facial nerve palsy• Bullous myringitis haemorrhagica• viral infection during epidemic of influenza• Severe ear ache, fever, body aches• On examination small haemorrhagic bullae seen on the TM & wall of the canal, slight conductive lossTr--- antibiotics, analgesics & local steroid drops
Reactive conditions• EXZEMATOUS OTITIS EXTERNA ---ALLERGY DUE TO
FOOD,JEWELLERY,COSMETICS,ANTIBIOTICS OR CHEMICALSTr—AVOID THE IRRITATING FACTORS application of antibiotic cream
• NEURODERMATITIS– COMPULSIVE ITCHING DUE TO PSYCHOLOGICAL FACTORS
Tr---PSYCHOTHERAPY
• SEBORRHOEIC OTIS EXTERNA—SCALY DERMATITIS
DUE TO SEBORRHIC CAPITISTr—THE SCALP CONDITION
TRAUMATIC CONDITIONS• HAEMATOMA PINNA—Due to fights• Tr---Incision & drainage
• Frost bite –it occurs in extreme cold weatherTr ---Keep body warm vasodilators application of silver nitrate 0.5% systemic antibiotics
• Pseudocyst Pinna —small cystic swelling below the skin due to trauma
Tr---Aspiration or incision & drainage under aseptic conditions
BenignTumours of external ear• Exostosis – • bony over growth, single pedunculated or • multiple sessile . Usually bilateral• Etiology unknown –may be cold water bathing• Asymptomatic—no treatment• Symptomatic—occludes the lumen, irritation or deafnessTr –electric drilling to remove it ,avoid injury to 7th nerve • Adenomas • from the sebaceous glands Tr –excision• Ceruminoma or hydradenoma • arises from ceruminous glands ,very rare , may turn malignant Tr--- excision
Malignant tumours of the external ear• Basal cell carcinoma (rodent ulcer)• Arises from the basal layer as a nodule• Margins of ulcer not everted• No metastasis to lymph nodesTr –resection if small if extensive –complete excision of pinna followed by plastic reconstruction of pinna. Radiotherapy if inoperableSquamous cell carcinoma• In external auditory canal or on pinna• Predisposing factor is chronic OtorrheaS/S elderly patient ,blood stained discharge or bleeding ear, polyp or granulation tissue seen on otoscopic examination enlarged lymph nodes ,facial nerve may be involved Margins of ulcer are evertedTr— Pinna-- radical excision—total auriclectomy External canal– wide excision –extended radical mastoidectomy followed by radio therapy
Miscellaneous conditions of the external ear
• Wax –secretions of ceruminous (watery) & sebaceous glands (fatty)• + desquamated keratin + debris & dust• Due to oxidative process it becomes brown• Normally wax comes out due to movement of jaw (eating & talking)• It acts as antibacterial & it is natures way to remove dust and foreign body• It may form in excess due to hot humid dusty condition or excess desquamationS/S blockage ,itching ,diminished hearing, earache tinnitus &vertigoTr– if hard should be softened –wax solvent soda glycerine drops then removed by syringing with warm sterile water or by wax hook• Keratosis obliterans –cholesteatoma of ext.ear• Wax + dequamated keratinised epithelium + cholesterol grannules• forms a pearly white mass• Causes widening of the bony canal• pain ,deafness & granulation tissue formationsS/S of chronic sinusitis & bronchiectasisTr--- mass softened & removed by syringing under anaesthesia• Foreign body of ear can be animate e.g. insects maggots• or inanimate e.g. seeds, beads, buttonsS/S history, irritation, earache, diminished hearingTr—syringing, or by ring curette or if impacted, removed under anaesthesia sometimes may have to use post aural route
CERUMEN or WAXCeruminous glands in the skin secrete cerumen.
Sebaceous glands do not actively secrete but form their secretions by passively breaking down
cells
Hairs on the skin help in auto cleaning
There are no sweat glands in the skin of the external auditory canal
• Two types of cerumen1)Dry –found in the orients & Mongolians2)Wet– found in the Caucasians ,Africans & HispanicsCerumen is genetically relatedand chromosome 16 is identified as carrying the
locus.Cerumen is supposed to become dry and leave
the external auditory canalIt has slight antibacterial ,antifungal properties
and acts as a insect repellant
Migration of the epidermal cells• The cells of the tympanic membrane and the
external auditory canal migrate outwards • This migration helps in healing small injuries in
the external ear, transports the cerumen out• Failure to do so may cause conditions like
cholesteatoma• Vigorous cleaning by ear buds may push the
cerumen deeper covering the tympanic membrane causing hearing loss.
Innervations of the skin of the external auditory canal
• The sensory receptors and bare axons are innervated by four Cranial nerves
1) Sensory portion of the mandibular division of the trigeminal nerve.
2) Facial nerve 3) Glossopharyngeal nerve4) Vagus innervates the Post. Wall of ext. canal
and the tympanic membrane This nerve branch is a part of the Arnold’s
nerve which also recieves a branch of the glossopharyngeal nerve.
• Innervation of the glossopharyngeal nerve explains why a person coughs when the skin of the inner portion of the canal is touched .
• Innervtion of the glossopharyngeal along with vagus explains why some people who are sensitive faint when the ear is being cleaned for wax or syringing is done for cleaning the ear.
COMPLICATIONS• INJURY TO TYMPANIC MEMBRANE• OSSCILES & LABRYNTH
• OTITIS EXTERNA / OTITIS MEDIA
• FORIGN BODY GRANNULOMA
• TETANUS DUE TO SHARP INFECTED FOREIGN BODY