
ENT assessment
62
13–1 Assessment of Ears, Nose, Mouth and Throat by Hakim Shah Updated on 09-12-2014
-
Upload
muhammad-shahid -
Category
Health & Medicine
-
view
276 -
download
28
Transcript of ENT assessment

13–1
Assessment of
Ears, Nose, Mouth and Throat
by
Hakim Shah
Updated on 09-12-2014

13–2
Objectives Identify the structures of the ears, nose,
mouth, and throat. Discuss the system-specific history for the
ears, nose, mouth, and throat. Describe normal findings in the physical
assessment of the ears, nose, mouth, and throat.
Describe common abnormalities found in the physical assessment of the ears, nose, mouth, and throat.
Perform the physical assessment of the ears, nose, mouth, and throat.
13–3
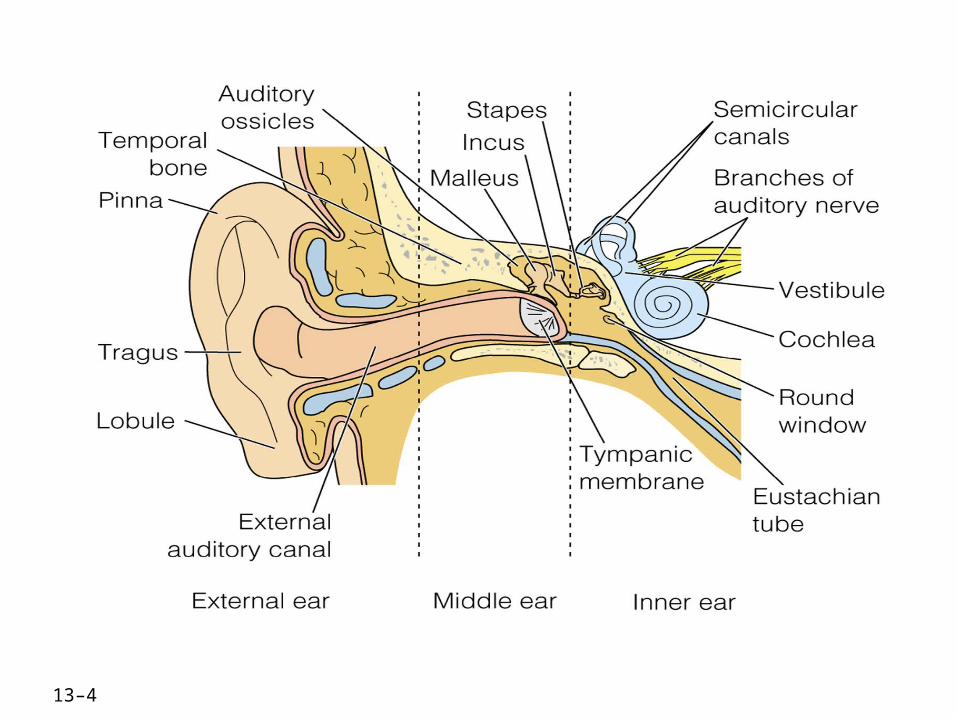
Anatomy and Physiology of the Ear
Three sections External ear Middle ear Inner ear
External ear Auricle or pinna External auditory canal
13–4
13–5
Middle ear Ossicles
Malleus (hammer) Incus (anvil) Stapes (stirrup)
Tympanic membrane Eustachian tube

13–6
Inner ear Labyrinth Vestibule Semicircular canals Cochlea
Frequency range of 20–20,000 Hz Decibel range 0–140

13–7
Health History
Ears Hearing loss Excessive cerumen
Nose Decreased ability to smell (elderly)
Mouth and throat Tooth loss Gum disease Decreased taste Tonsilitis Sore throat/infection

13–8
Common Chief Complaints
Ear Hearing loss Otorrhea Otalgia Tinnitus

13–9
Nose Pain Drainage Blockage or congestion Bleeding (Epistaxis)

13–10
Mouth and throat Halitosis Oral lesions Swelling Oral thrush Ulceration Pain Difficulty in swallowing Hoarseness of voice
13–11
Evaluation of Chief Complaint Quality Associated manifestations Aggravating factors Alleviating factors Frequency Timing
13–12
Past Health History Medical
Otitis media or externa Nasal polyps, sinusitis, allergic rhinitis Tonsillitis, caries, upper respiratory infections Chronic diseases such as diabetes mellitus, renal
disease, hypertension, immuno-suppression Dental pathology Nutritional disturbances
13–13
Surgical Cosmetic surgery of head or neck Repair of deviated septum Oral surgery Tympanostomy tubes
13–14
Medications Antibiotics Antihistamines Decongestants Steroids Chemotherapy Immunosuppressive drugs
13–15
Allergies Signs and symptoms Pollen, insect stings, animal dander
Injuries and accidents Foreign bodies Trauma Sports injuries
Special needs Use of assistive devices (hearing aids) Speech disorders
Childhood illnesses Frequent tonsillitis or ear infections
13–16
Social History Alcohol use Drug use Tobacco use Sexual practices Work and home environment Hobbies and leisure activities Stress
13–17
Health Maintenance Activities
Sleep Diet Use of safety devices Health check-ups

13–18
General Approach to Assessment
Greet patient Explain assessment techniques Quiet, well-lit environment Sitting position Compare right to left Systematic approach

13–19
Equipment Otoscope Nasal speculum Penlight Tuning fork in 256 , 512 and 1024 Hz Tongue blade Watch Gauze square Cotton-tipped applicators
13–20
Assessment of the Ear
Examination consists of three parts:1. Auditory screening
2. Inspection and palpation of external ear
3. Otoscopic assessment

13–21
Take history of:
_Ear aches Infections Discharge Hearing loss Environmental noise Tinnitus Vertigo Self care

13–22
Auditory Screening Voice-whisper test and Vestibular apparatus
Normal finding: able to repeat words whispered at a distance of 2 feet
Tuning fork tests Weber test Rinne test Determine whether hearing loss is conductive or
sensorineural

13–23
Voice whisper and balance test
Test hearing acuity: Conversational speech note behavioral response to conversational speech ( lip reading, frowning, straining forward, turning to catch sounds asks you to repeat, misunderstands your questions)
Voice test: Test one ear at time cover opposite ear , shied lips 1 to 2 feet whisper two syllable words have patient repeat
Romberg Test: (vestibule apparatus) test stand with feet together and arms at sides, close eyes should hold position for 20 seconds without loosing balance
13–24
Tuning fork test Weber Test: Place vibrating tuning fork
midline on the skull ask if tone is equal bilaterally or better in one ear.
Rinne test: have patient signal when the vibrating tuning fork can no longer be heard place fork near the ear cannel should still hear sound AC>BC

13–25
Otoscopic Examination
Otoscopic exam external canal- color , redness, swelling for cerumen, discharge, foreign bodies, lesions,.
Tympanic membrane- normal is shiny translucent with pearl-gray color, flat slightly pulled in at center flutters with swelling membrane should be intact.
13–26
Normal findings
Weber test Normal finding: able to hear sound
equally in both ears Rinne test
Normal finding: air conduction > bone conduction

13–27
External Ear
Inspection Note position, size, color, and shape
color Palpation
Auricle Tragus Mastoid bone TMJ

13–28
Normal findings Flesh color Positioned centrally and in proportion
to the head No foreign bodies, redness, drainage,
deformities, nodules, or lesions
13–29
Abnormal findings Pale, red, cyanotic Small-size or large-size ears Purulent drainage Clear or bloody drainage Hematoma behind ear over mastoid Pain or tenderness on palpation

13–30
Otoscopic AssessmentInspect both ears External ear canal:
lesions, swelling, discharge, hairs, foreign body, cerenum
Tympanic memebrane Pull auricle upward and back ward to
straighten the auditory canal
13–31
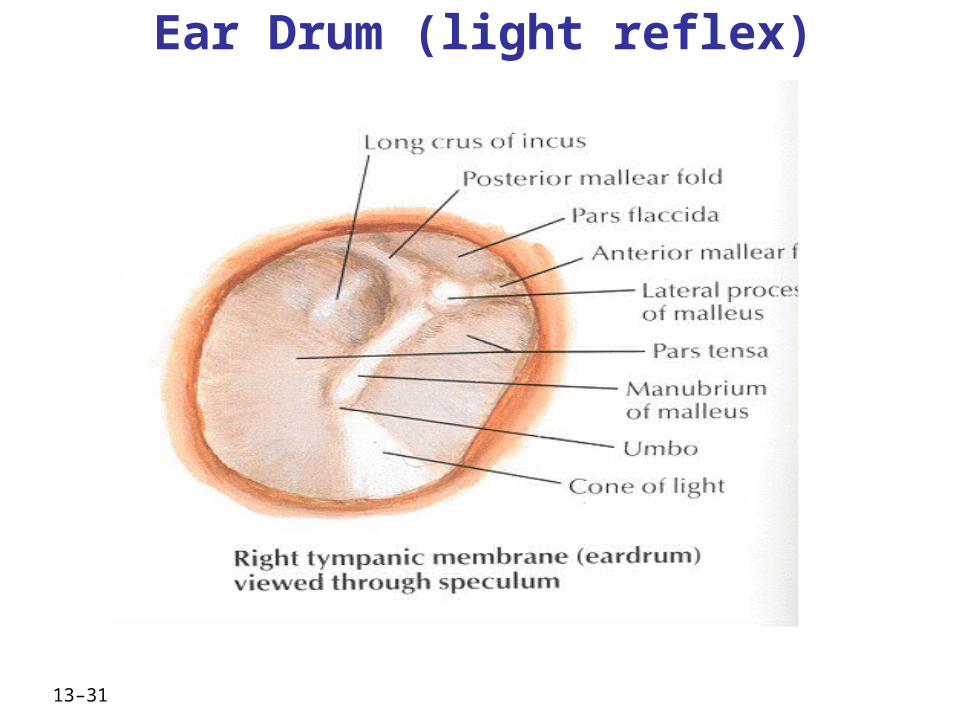
Ear Drum (light reflex)
13–32
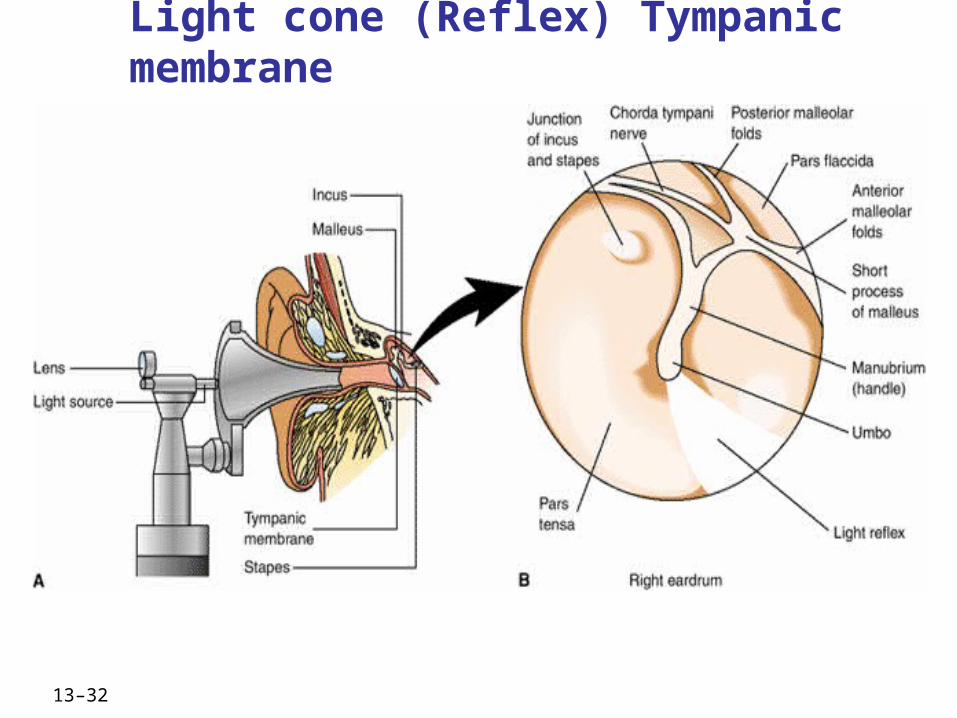
Light cone (Reflex) Tympanic membrane
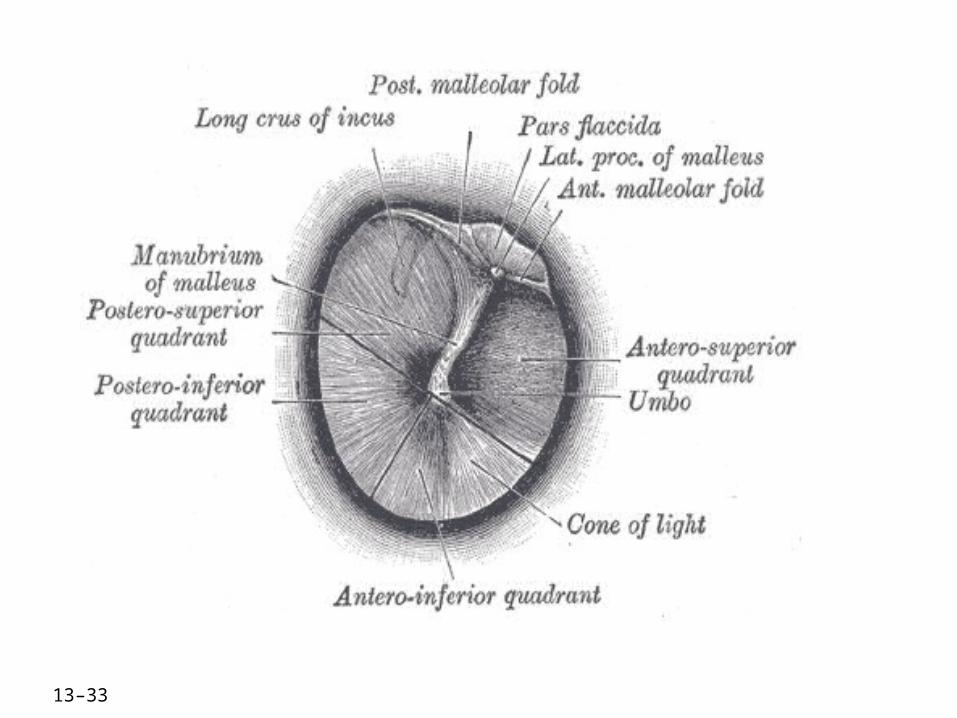
13–33

13–34
Normal findings Tympanic membrane is pearly gray with
well-defined landmarks Light reflex present at 5 o’clock in right
ear and 7 o’clock in left ear Tympanic membrane moves when patient
blows against resistance No redness, swelling, tenderness, lesions,
drainage, foreign bodies
13–35
Abnormal findings Chalky patches on tympanic membrane Severe pain Redness, swelling, narrowing, pain Drainage Hard, dry, very dark yellow cerumen Reddened tympanic membrane
13–36
(continues)
Risk Factors for Otitis Media Less than 2 years of age Frequent upper respiratory infections Cold weather Male gender Family history Smoky environment Bottle fed Down syndrome
13–37
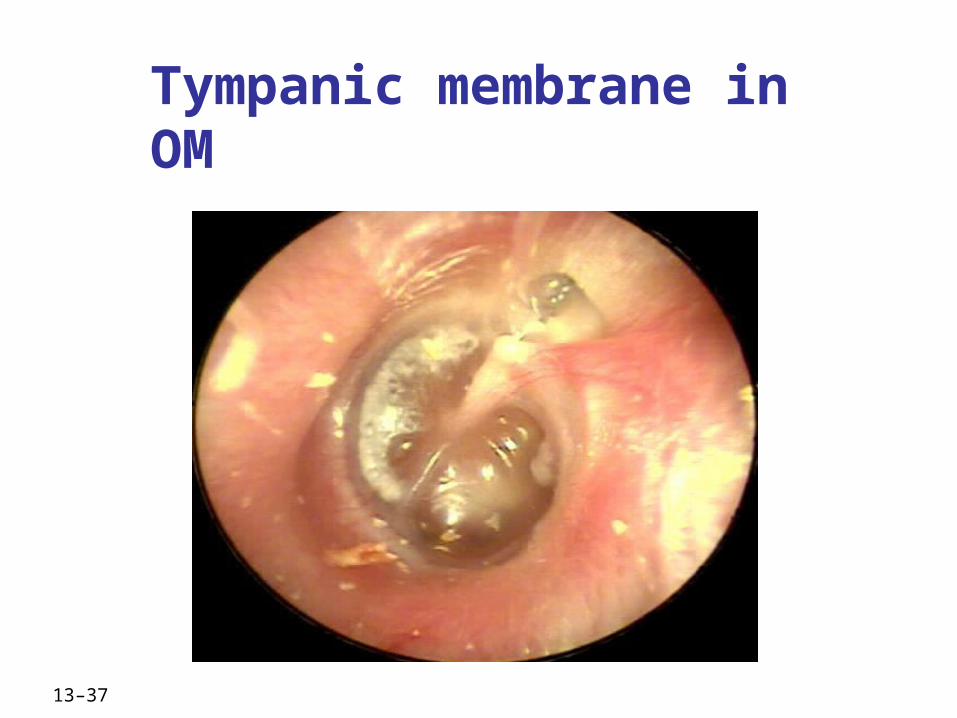
Tympanic membrane in OM
13–38
Structure and function : Nose, Mouth, and Throat
Nose Function in the respiratory system External nose Nasal cavity Septum Turbinate Paranasal sinuses
Frontal Maxillary Ethmoid Sphenoid

13–39
Paranasal Sinuses

13–40
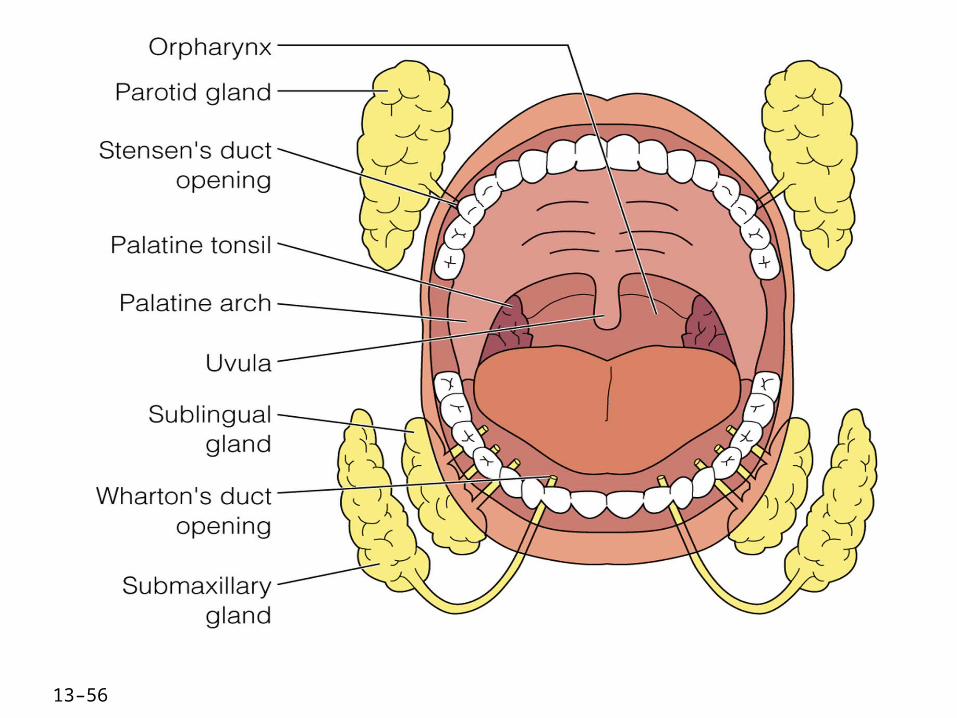
Mouth Function in the digestive and respiratory
system Hard and soft palates Uvula Tongue Salivary glands
Parotid Submandibular Sublingual
Teeth

13–41

13–42
Throat Oropharynx Tonsils Nasopharynx
13–43
Equipment for examination of Nose, Mouth and Throat Otoscope with short, wide-tipped nasal
speculum Pen light Two tongue blades Cotton gauze pad Gloves
13–44
Assessment of the Nose Take history of:
Discharge Frequent colds Sinus pain Trauma Epistaxis Allergies Altered smell

13–45
Inspection and palpation of nose
External nose Tenderness, discharge ,trauma, bleeding, lesions,
masses, swelling, asymmetry Test patency of nostril
Inspection of internal nose Speculum or otoscope with nasal speculum Nasal cavity
Nasal septumTurbinates
Sinus Areas- PalpateFrontal and maxillary sinusesTransillumination

13–46
Normal findings Located in midline of face No swelling, bleeding, lesions, or masses Both nostrils patent Septum midline Nasal mucosa is pink or dull red

13–47
Abnormal findings Broken, misshapen, swollen nose Occluded nasal passages Septum is deviated Nasal mucosa is red and swollen Purulent drainage
13–48
Assessment of the Sinuses Inspection (Sinus Transillumination) Palpation and percussion Normal findings
No discomfort during palpation or percussion
Resonance heard on percussion

13–49
(continues)
Assessment of the Mouth
Inspect Mouth Lips Teeth and gums Tongue U-shaped areas under the tongue Buccal mucosa Uvula Hard and soft palate

13–50
Mouth inspection and palpation
LIPS inspect for color, moisture, cracking, or lesions. Palpate lips, and face for mass and tenderness
TEETH/gums note any diseased absent, loose teeth gums should be pink or coral, check for swelling, retraction of gum margins spongy, bleeding discolored gums.
TONGUE color pink and even dorsal side roughened, ventral smooth, glistening, shows veins Inspect under tongue for nodules, lesions, ulcerations
13–51
Cont… Buccal mucosa looks pink, smooth,
moist, dark skinned people may have patchy hyperpigmentation
Uvula fleshy pendant midline uvula and soft palate rise with “ahhh” sound. anterior hard palate is white with irregular transverse rugae the posterior soft palate is pinker smooth, and upwardly movable.

13–52
Normal findings of Mouth Breath is fresh Pink, moist lips Tongue midline, symmetrical, with adequate
movement No pockets between gums and teeth No bleeding Smooth, white teeth; proper alignment, no
dental caries
13–53
Abnormal findings of Mouth Lesions, growths Dry, cracked lips Vesicles or blisters Red, tender, inflamed tongue, gums, buccal mucosa Thrush Coating on tongue Red, tender, swollen gingiva Bleeding gums
13–54
(continues)
Inspection of the Throat Position, size, color,and general
appearance of tonsils and uvula Gag reflex Color of oropharynx Presence of swelling, exudate,
lesions

13–55
Assessment of tonsils
Enlarged tonsils are graded Grade 1 – wnl Grade 2 – tonsils b/w pillars
and uvula Grade 3 – tonsils touching
uvula Grade 4 – tonsils touching
each other (kissing tonsils)
13–56

13–57
Neck assessment usually done with Thorax
13–58
Normal findings Soft palate and uvula rise when patient
says “ah” Uvula is midline Throat is pink and vascular No swelling, exudate, or lesions Gag reflex is present
13–59
Abnormal findings Posterior pharynx is red with white
patches Tonsils and uvula are red and swollen Hoarse voice Grayish membrane covering tonsils,
uvula, soft palate
13–60
Gerontological Variations Presbycusis Diminished sense of smell and taste Lesions Periodontal disease Oral alterations due to disease or
side effects of medications Tooth loss
13–61
Thank You

13–62
Reference Bickly L.S, B.(2011) Bates guide to
physical examination and history taking (10th ed).Philadelphia: J.B.Lippincott


















