Enhancing Diagnostic Precision Through Combined Genomic and ...€¦ · began with creation of the...
1
Mixed Neuroendocrine Non-Neuroendocrine Neoplasm (miNEN) Enhancing Diagnostic Precision Through Combined Genomic and Histopathological Analysis of Pancreatic Neuroendocrine Tumours Tamsin Robb 1 , Mee Ling Yeong 2 , Nicole Kramer 2 , Cherie Blenkiron 1 , Kate Parker 1 , Peter Tsai 1 , Sandra Fitzgerald 1 , Paula Shields 1 , Michael Findlay 1 , Cristin Print 1 , Ben Lawrence 1 1 University of Auckland, New Zealand 2 Auckland District Health Board, New Zealand Conclusions: Homing in on precise diagnoses Tamsin Robb t.robb@ auckland.ac.nz In tumours initially diagnosed as pNETs, DNA, RNA and histopathological evidence contributed to re-diagnosis as SPN or miNEN The NETwork! Project (New Zealand) began with creation of the NETwork! registry, which catalogues all Neuroendocrine tumour patients diagnosed between 1995- 2012 in the Auckland region and 2008-2012 across New Zealand. With strong support from NET patient support group (Unicorn Foundation New Zealand), we have ethical approval to retrospectively access clinical formalin-fixed paraffin embedded (FFPE) tissue blocks belonging to patients in the NETwork! Registry. We aim to conduct genomics on these annotated samples to understand NET biology, as it pertains to clinical management. Methods: 69 sporadic well-differentiated pancreatic neuroendocrine tumours (pNETs) from 60 individuals alongside matched normal tissues underwent targeted DNA sequencing (NimbleGen SeqCap), RNA expression analysis (Affymetrix Microarrays) and immunohistochemistry (IHC) alongside pathological examination, to search for molecular drivers; incidentally providing valuable evidence for re-diagnosis in three patients. Cases selected had a clinical and pathological diagnosis of well-differentiated pNET, expressed at least one of the three neuroendocrine IHC markers (chromogranin A, synaptophysin or CD56) and were surgically resectable at initial diagnosis. This poster describes 3 cases that were excluded from the main analysis because genomic analyses allowed us to recognise that they were not pNETs (for pNET analysis see ENETs 2018 Poster B10). Solid Pseudopapillary Neoplasm (SPN) Patient 029 Normal coverage track sequence reads sequence reads Patient 048 Normal Tumour 029P Tumour 048P sequence reads sequence reads coverage track coverage track coverage track Patient 029 Patient 048 030P CTNNB1 wild type 029P CTNNB1 mutation 048P CTNNB1 mutation Deep targeted DNA- seq Revealed activating mutations 1 in CTNNB1 encoding B-catenin, pathognomonic for SPNs - present in 90% of all SPN cases 2 . RNA expression RNAs up-regulated by β- catenin 3 were highly expressed, in accord with the mutation’s known activating effect. Histopathological analysis Revealed cellular relocalisation of β-catenin (brown) to the nucleus, concordant with SPN status and transcription factor function. In two cases (029 and 048), tumours were re-diagnosed as pancreatic SPNs; originally diagnosed as pNETs by morphological and IHC but noted uncertainty due to some variable SPN-like features. Alongside deep pathological examination, evidence for re-diagnosis came from β-catenin mutations, RNA expression patterns, IHC (β-catenin localisation) In one case (057), three tumour samples from the same patient showed possible features of mixed neuroendocrine non-neuroendocrine neoplasm (miNEN). Alongside deep pathological examination, evidence for re-diagnosis came from mutational landscape, aneuploidy analysis, and proliferation analysis. Mutational landscape Revealed mutations in APC, TP53 and FANCA, in contrast to mutations found in pNETs in this study. Aneuploidy analysis Revealed extensive aneuploidy in tumours from patient 057 in contrast to the degree and patterns of aneuploidy seen in pNETs in this study. Heatmap shows Z-transformed expression of RNAs encoding cellular proliferation proteins 5 sorted by 1 st principal component, highlighting the highly proliferative nature of Case 057. Using unsupervised clustering, Case 057 fell to the very left of the heatmap. Proliferation analysis Expression of RNAs encoding cellular proliferation proteins were distinctly elevated in tumours from patient 057 in contrast to pNETs in this study. Concordantly, these tumours had very high MKI67 RNA expression and ki-67 positive tumour cells. RNAs known to be up-regulated by β-catenin activity in colorectal cell lines were intersected with RNAs with significantly high or low expression (≥2 SD above / below the mean of expression of the RNA in our pNETs). Colours map RNA expression from maximally low expression (green) through mean (white) to maximally high expression (red) across pNETs. Numbers indicate Z-transformed expression. 1. Moreno-Bueno et al. (2001) PMID 11703283 2. Abraham et al. (2002) PMID 11943721 3. Herbst et al. (2014) PMID 24467841 4. Amarasinghe et al. (2014) PMID 25167919 5. Nagalla et al. (2013) PMID 23618380 6. Harris et al. 2017 PMID 27556576 Colouring of blocks indicates the dominant inferred copy number (CN) for each autosome in each tumour based on ADTEx analysis, 4 relative somatic read counts at germline heterozygous positions and normalized read counts in 3kb tiles across the genome. LoH (irrespective of CN) is indicated by red boxes. Numerals indicate CN when CN ≠ 2. • SPNs and miNENs share some cytological features with pNETs but are genomically distinct. • β-catenin IHC should be conducted more frequently when diagnosing pNETs. • While differentiation of uncommon pancreatic malignancies from pNETs can be challenging, it is important as the diagnosis has different prognostic implications. Genomic analysis provides a further tool for making this critical distinction. • We believe that combining genomic information with traditional pathological information is likely to generate more precise diagnoses for many tumour types 6 NEW ZEALAND
Transcript of Enhancing Diagnostic Precision Through Combined Genomic and ...€¦ · began with creation of the...

Mixed Neuroendocrine Non-Neuroendocrine Neoplasm (miNEN)
Enhancing Diagnostic Precision Through Combined Genomic and Histopathological Analysis
of Pancreatic Neuroendocrine TumoursTamsin Robb1, Mee Ling Yeong2, Nicole Kramer2, Cherie Blenkiron1, Kate Parker1, Peter Tsai1, Sandra Fitzgerald1, Paula Shields1, Michael Findlay1, Cristin Print1, Ben Lawrence1
1 University of Auckland, New Zealand 2 Auckland District Health Board, New Zealand
Conclusions: Homing in on precise diagnoses
Tamsin [email protected]
In tumours initially diagnosed as pNETs, DNA, RNA and histopathological evidence contributed to re-diagnosis as SPN or miNEN
The NETwork! Project (New Zealand) began with creation of the NETwork!registry, which catalogues all Neuroendocrine tumour patients diagnosed between 1995-2012 in the Auckland region and 2008-2012 across New Zealand. With strong supportfrom NET patient support group (Unicorn Foundation New Zealand), we have ethicalapproval to retrospectively access clinical formalin-fixed paraffin embedded (FFPE) tissueblocks belonging to patients in the NETwork! Registry. We aim to conduct genomics onthese annotated samples to understand NET biology, as it pertains to clinicalmanagement.
Methods: 69 sporadic well-differentiated pancreatic neuroendocrine tumours (pNETs)from 60 individuals alongside matched normal tissues underwent targeted DNAsequencing (NimbleGen SeqCap), RNA expression analysis (Affymetrix Microarrays) andimmunohistochemistry (IHC) alongside pathological examination, to search for moleculardrivers; incidentally providing valuable evidence for re-diagnosis in three patients. Casesselected had a clinical and pathological diagnosis of well-differentiated pNET, expressedat least one of the three neuroendocrine IHC markers (chromogranin A, synaptophysin orCD56) and were surgically resectable at initial diagnosis. This poster describes 3 cases thatwere excluded from the main analysis because genomic analyses allowed us to recognisethat they were not pNETs (for pNET analysis see ENETs 2018 Poster B10).
Solid Pseudopapillary Neoplasm (SPN)
Patient029
Nor
mal
coverage track
sequencereads
sequencereads
Patient048
Nor
mal
Tum
our 0
29P
Tum
our 0
48P
sequencereads
sequencereads
coverage track
coverage track
coverage track
Patient029
Patient048
030P CTNNB1 wild type
029P CTNNB1 mutation 048P CTNNB1 mutation
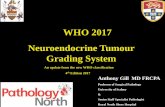
Deep targeted DNA-seqRevealed activating mutations1 in CTNNB1encoding B-catenin, pathognomonic for SPNs - present in 90% of all SPN cases2.
RNA expressionRNAs up-regulated by β-catenin3 were highly expressed, in accord with the mutation’s known activating effect.
Histopathological analysisRevealed cellular relocalisation of β-catenin (brown) to the nucleus, concordant with SPN status and transcription factor function.
In two cases (029 and 048), tumours were re-diagnosed as pancreatic SPNs; originallydiagnosed as pNETs by morphological and IHC but noted uncertainty due to somevariable SPN-like features.
Alongside deep pathological examination, evidence for re-diagnosis came fromβ-catenin mutations, RNA expression patterns, IHC (β-catenin localisation)
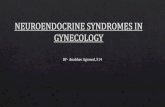
In one case (057), three tumour samples from the same patient showed possiblefeatures of mixed neuroendocrine non-neuroendocrine neoplasm (miNEN).
Alongside deep pathological examination, evidence for re-diagnosis came frommutational landscape, aneuploidy analysis, and proliferation analysis.
Mutational landscapeRevealed mutations in APC, TP53 and FANCA, in contrast to mutations found in pNETs in this study.
Aneuploidy analysisRevealed extensive aneuploidy in tumours from patient 057 in contrast to the degree and patterns of aneuploidy seen in pNETs in this study.
Heatmap shows Z-transformed expression of RNAs encoding cellular proliferation proteins5 sorted by 1st
principal component, highlighting the highly proliferative nature of Case 057. Using unsupervisedclustering, Case 057 fell to the very left of the heatmap.
Proliferation analysisExpression of RNAs encoding cellular proliferation proteins were distinctly elevated in tumours from patient 057 in contrast to pNETs in this study. Concordantly, these tumours had very high MKI67 RNA expression and ki-67 positive tumour cells.
RNAs known to be up-regulated by β-catenin activity in colorectal cell lines were intersected with RNAs withsignificantly high or low expression (≥2 SD above / below the mean of expression of the RNA in our pNETs).Colours map RNA expression from maximally low expression (green) through mean (white) to maximallyhigh expression (red) across pNETs. Numbers indicate Z-transformed expression.
1. Moreno-Bueno et al. (2001) PMID 11703283
2. Abraham et al. (2002) PMID 11943721
3. Herbst et al. (2014) PMID 24467841
4. Amarasinghe et al. (2014) PMID 25167919
5. Nagalla et al. (2013) PMID 23618380
6. Harris et al. 2017 PMID 27556576
Colouring of blocks indicates the dominant inferred copy number (CN) for each autosome in each tumourbased on ADTEx analysis,4 relative somatic read counts at germline heterozygous positions andnormalized read counts in 3kb tiles across the genome. LoH (irrespective of CN) is indicated by red boxes.Numerals indicate CN when CN ≠ 2.
• SPNs and miNENs share some cytological features with pNETs but are genomically distinct.• β-catenin IHC should be conducted more frequently when diagnosing pNETs.• While differentiation of uncommon pancreatic malignancies from pNETs can be challenging, it is important as the diagnosis has different prognostic implications. Genomic
analysis provides a further tool for making this critical distinction.• We believe that combining genomic information with traditional pathological information is likely to generate more precise diagnoses for many tumour types6
NE W ZEAL AND