
Enhanced Recovery Compliance against elements of ER pathway by Specialty 22 th July 2011.
24
Enhanced Recovery Compliance against elements of ER pathway by Specialty 22 th July 2011
-
Upload
marylou-james -
Category
Documents
-
view
214 -
download
0
Transcript of Enhanced Recovery Compliance against elements of ER pathway by Specialty 22 th July 2011.
Enhanced Recovery Compliance against elements of
ER pathway by Specialty
22th July 2011
Introduction
The aim of this report is to share national level data on enhanced recovery pathways and so to provide benchmarking information to organisations implementing ER.
The data included in this report was recorded on the national enhanced recovery toolkit. This tool allows a trust to audit their local implementation of enhanced recovery against a standard enhanced recovery pathway and also to benchmark their local audit against what others reporting around the country.

Introduction (cont)• This report includes data from 29 trusts across England. These trusts are likely to be a mix of those that are new to enhanced recovery as well as those that have more experience of enhanced recovery pathways of care.
• Patients admissions were from 02/01/2011 to 03/06/2011
• The data extract includes •658 colorectal patients (26 hospital trusts)•467 gynaecology patients (13 hospital trusts)•1,149 MSK patients (14 hospital trusts)•50 Urology patients (5 hospital trusts)
• Each sheet shows compliance for a different element of the ER pathway and how this varies between specialities. The definition for each element is shown at the bottom of each page.
To access the toolkit: https://www.natcansatmicrosite.net/enhancedrecovery
Any comments to [email protected]
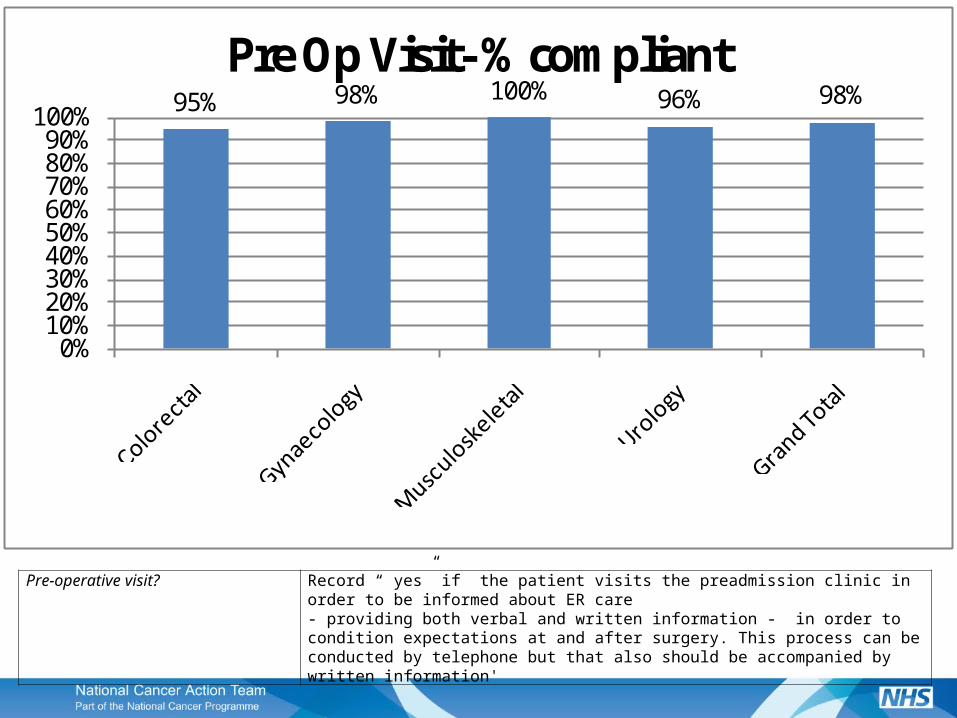
95% 98% 100% 96% 98%
0%10%20%30%40%50%60%70%80%90%
100%
Pre Op Visit- % compliant
Pre-operative visit? Record “ yes” if the patient visits the preadmission clinic in order to be informed about ER care- providing both verbal and written information - in order to condition expectations at and after surgery. This process can be conducted by telephone but that also should be accompanied by written information'

99% 100% 100% 100% 100%
0%
20%
40%
60%
80%
100%
Patient Assessed for Surgery- % compliant
Patient assessed as fit for surgery Record “yes” if patient attends a pre-assessment clinic to ensure optimal physical preparation for surgery and is assessed as fit for surgery. This can occur at a preadmission clinic attendance'

96%
71%
94% 96%90%
0%10%20%30%40%50%60%70%80%90%
100%
Patient Explanation ERP- % compliant
Patient given written and verbal explanation of ER pathway
Record “Yes” if the patient is given written and verbal explanation of ER pathway and related care and their role in their recovery
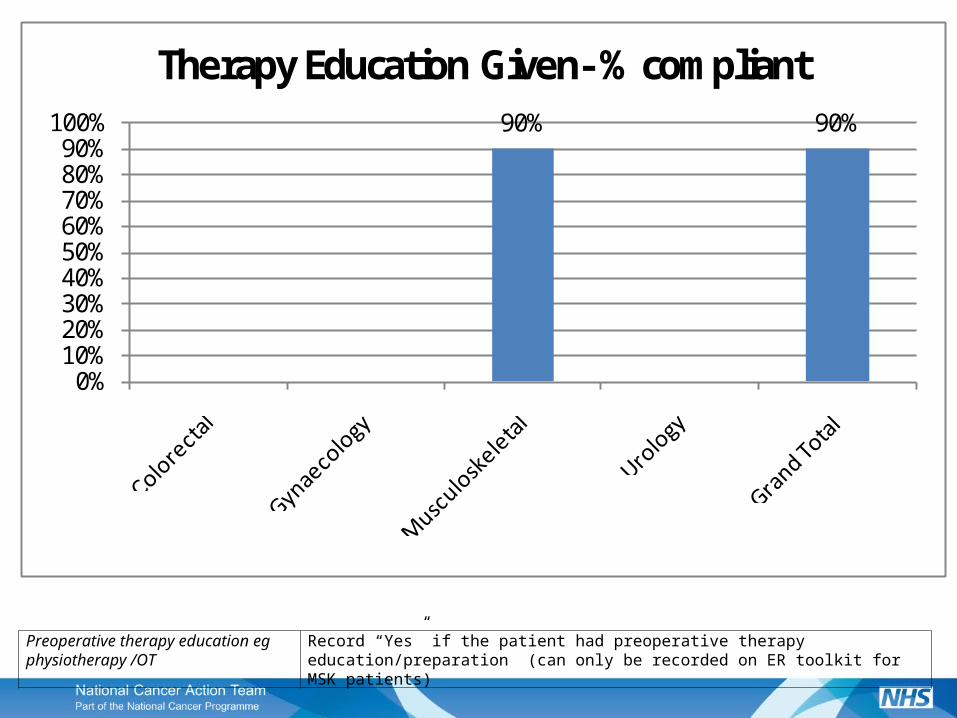
90% 90%
0%10%20%30%40%50%60%70%80%90%
100%
Therapy Education Given- % compliant
Preoperative therapy education eg physiotherapy /OT
Record “Yes” if the patient had preoperative therapy education/preparation (can only be recorded on ER toolkit for MSK patients)
87% 87%
0%10%20%30%40%50%60%70%80%90%
100%
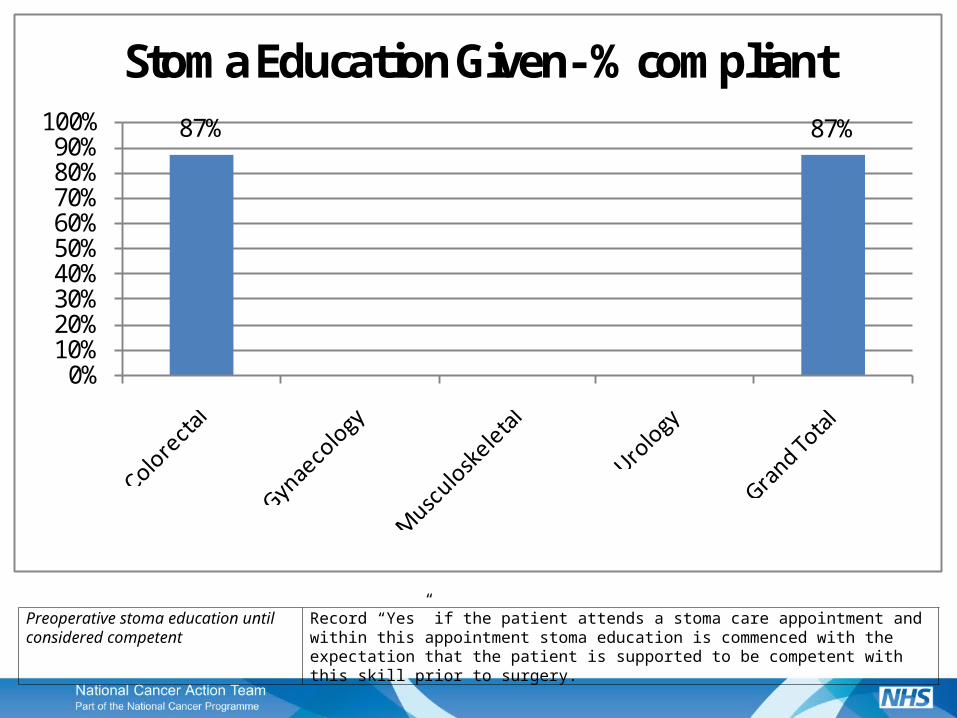
Stoma Education Given- % compliant
Preoperative stoma education until considered competent
Record “Yes” if the patient attends a stoma care appointment and within this appointment stoma education is commenced with the expectation that the patient is supported to be competent with this skill prior to surgery.
51%
81%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Rectal Colon
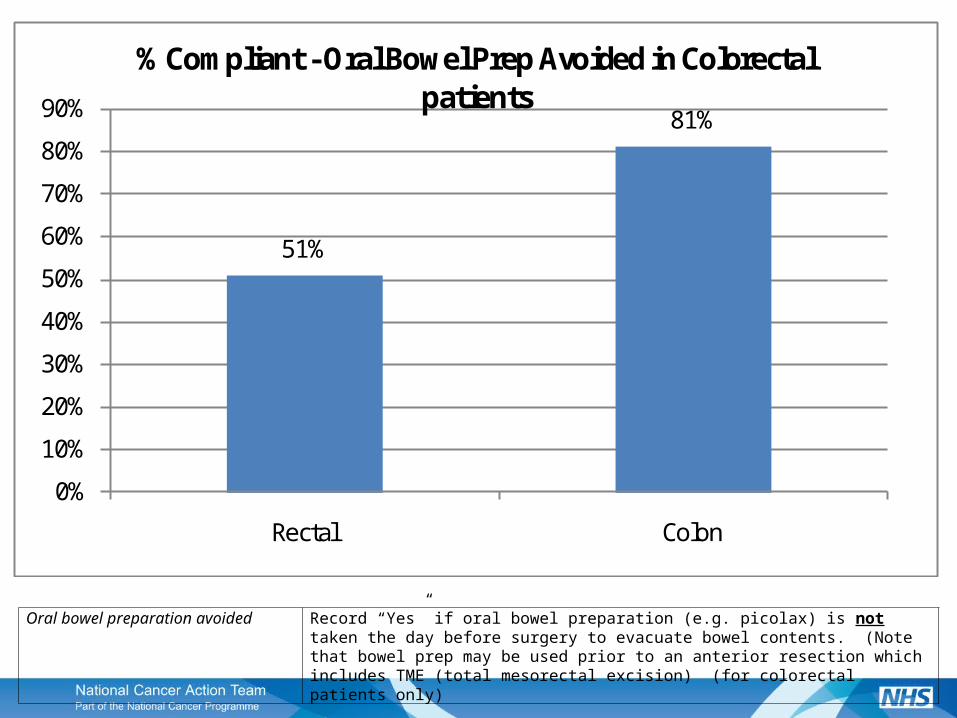
% Compliant - Oral Bowel Prep Avoided in Colorectal patients
Oral bowel preparation avoided Record “Yes” if oral bowel preparation (e.g. picolax) is not taken the day before surgery to evacuate bowel contents. (Note that bowel prep may be used prior to an anterior resection which includes TME (total mesorectal excision) (for colorectal patients only)
63%
94% 96% 96%87%
0%10%20%30%40%50%60%70%80%90%
100%
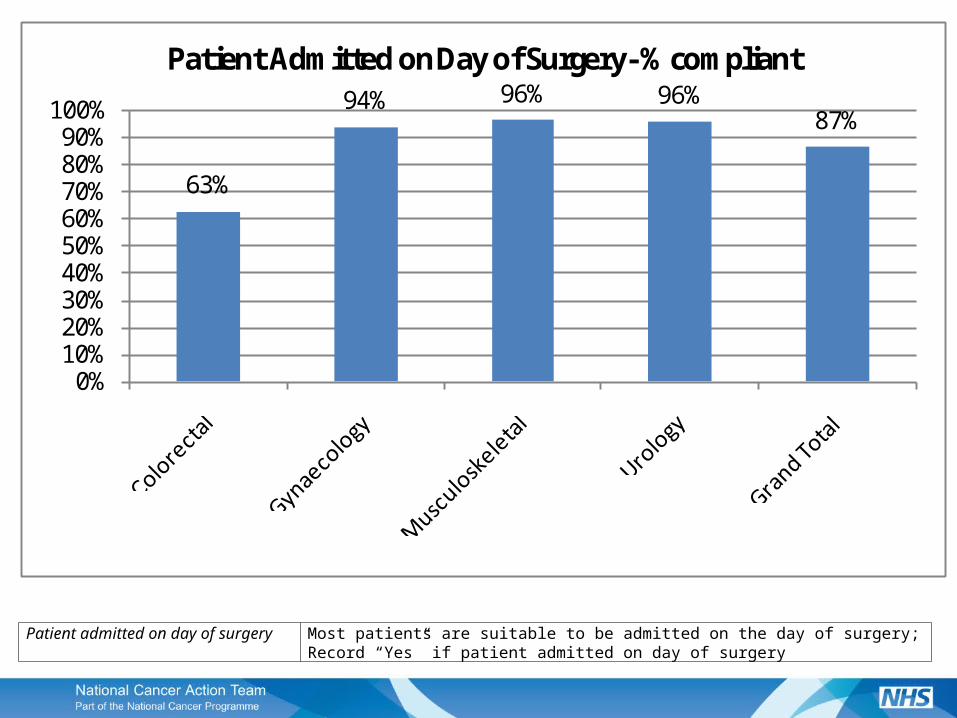
Patient Admitted on Day of Surgery- % compliant
Patient admitted on day of surgery Most patients are suitable to be admitted on the day of surgery; Record “Yes” if patient admitted on day of surgery

92%
38%
21%
74%
45%
0%10%20%30%40%50%60%70%80%90%
100%
Carbohydrates Given- % compliant
Carbohydrate drinks given preoperatively
maltodextran drinks given 12 hours prior to surgery and up to two hours before going to the operating theatre provided gastric emptying is not impaired.

99% 97% 97% 100% 98%
0%10%20%30%40%50%60%70%80%90%
100%
Avoidance of Sedatives- % compliant
Avoidance of long acting sedative pre-medication
Record “Yes” if long acting pre- medication drug such as a temezepam / diazepam has not been given within 24 hours of surgery

97% 98% 100% 97% 99%
0%10%20%30%40%50%60%70%80%90%
100%
Antibiotics Prior- % compliant
Administration of appropriate antibiotics prior to skin incision
Definition within 60 minutes of knife to skin as per the WHO/NPSA safer surgery checklist (for colorectal patients only)

77%
45%
91%80% 77%
0%10%20%30%40%50%60%70%80%90%
100%
Epidural or Regional Analgesia- % compliant
Epidural or regional analgesia used Epidural or regional analgesia used to provide adequate analgesia in the immediate postoperative period and to allow mobilisation (Note there is not a consensus about whether epidurals are necessary in laparoscopic surgery)

79%
20%
85%81%
58%
40%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Colorectal Gynaecology Urology
% compliant - Epidural or Regional Analgesia - shown by Laparoscopic/Open
Laparoscopic
Open
Epidural or regional analgesia used Epidural or regional analgesia used to provide adequate analgesia in the immediate postoperative period and to allow mobilisation (Note there is not a consensus about whether epidurals are necessary in laparoscopic surgery)
Was the operation commenced laparoscopically?
In order to simplify the data collection the toolkit asks whether the operation was started laparoscopically. This includes both total laparoscopic and laparoscopically assisted proceduresSelect from “Yes”, “No”, “Not Applicable”.

79%
50% 53%61% 60%
0%10%20%30%40%50%60%70%80%90%
100%
Individual Fluid Therapy- % compliant
Individualised goal directed fluid therapy
To prevent overloading with intravenous fluids during surgery; this may be achieved by use of an oesophageal Doppler or other advanced haemodynamic monitor. Must be individualised for each patient and administered to achieve specific haemodynamic targets.

98%86%
98% 100% 96%
0%10%20%30%40%50%60%70%80%90%
100%
Hypothermia Prevention- % compliant
Hypothermia prevention (intra-operative warming)
Patient temperature 36.0-37.5 Centigrade throughout the operation (will usually involve using active warming measures such as forced air warming and fluid warmers).

78% 80% 83%
94%
0%10%20%30%40%50%60%70%80%90%
100%
Anterior resection APE Colectomy Colorectal - Other
% Compliant - Avoidance of abdominal drains by colorectal operation
The avoidance of abdominal drains except following TME
Routine use of drains has not been shown to reduce complications and can actually cause problems except following total mesorectal excision. (for colorectal patients only)

94%86%
94% 91%
0%10%20%30%40%50%60%70%80%90%
100%
NG Tube Removed- % compliant
NG Tube removed before exit from theatre
Definition not required (not applicable for MSK patients)

89% 94% 97% 94% 94%
0%10%20%30%40%50%60%70%80%90%
100%
Avoid Crystalloid Overload- % compliant
Avoidance of post operative crystalloid overload
Intravenous crystalloid infusion discontinued on first postoperative day (day 1).

60% 60%50%
88%
56%
0%10%20%30%40%50%60%70%80%90%
100%
Avoid Systemic Opiates- % compliant
Avoidance of systemic opiates used postoperatively
Analgesia that ideally does not include opiates is recommended to prevent complications such as constipation. Record “yes” if no oral, intramuscular or intravenous opiates used postoperatively.

85% 88%97% 94% 92%
0%10%20%30%40%50%60%70%80%90%
100%
Post-Op Nutritian- % compliant
Early post operative nutrition / solid food intake
Patients are encouraged to eat and drink on day 0 (the operating day) after surgery, as tolerated, and this to continue subsequently. To provide further nutrition in the immediate post-operative period, nutritious supplement drinks are encouraged daily.
96% 98%87%
100%92%
0%10%20%30%40%50%60%70%80%90%
100%
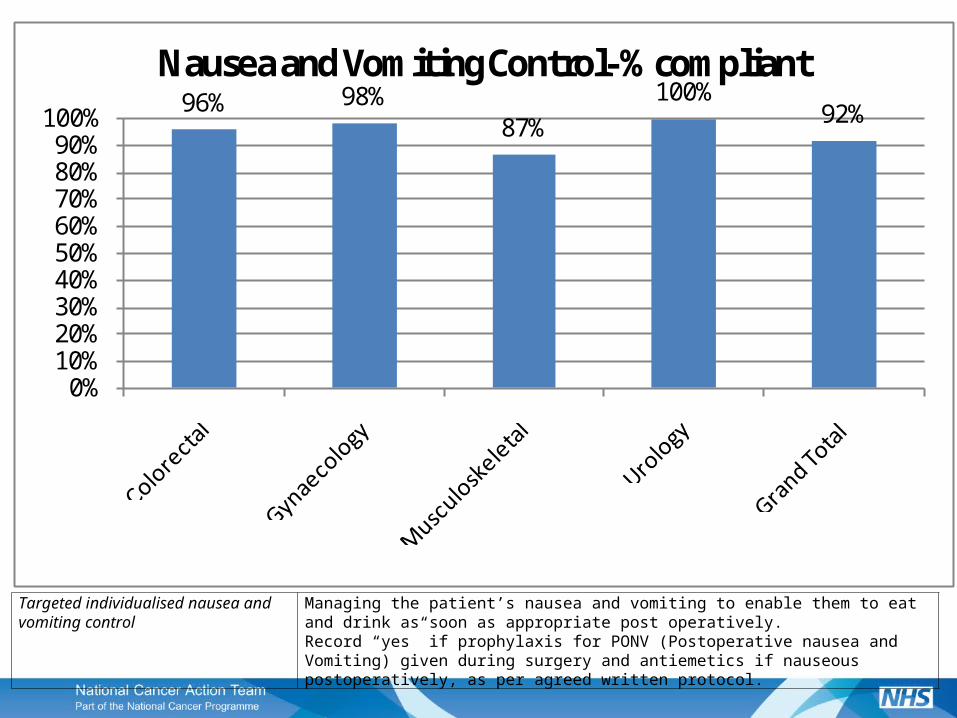
Nausea and Vomiting Control- % compliant
Targeted individualised nausea and vomiting control
Managing the patient’s nausea and vomiting to enable them to eat and drink as soon as appropriate post operatively. Record “yes” if prophylaxis for PONV (Postoperative nausea and Vomiting) given during surgery and antiemetics if nauseous postoperatively, as per agreed written protocol.

89% 94% 93%100%
92%
0%10%20%30%40%50%60%70%80%90%
100%
Early Mobilisation- % compliant
Mobilisation within 24 hours Record “Yes” only if the patient is able to mobilise within 24hrs. For orthopaedic patients this must be weight bearing mobilisation.

![CONSTIPATION Enhanced Primary Care Pathway [July 2016]](https://static.fdocuments.us/doc/165x107/587ca2351a28ab27378b7c83/constipation-enhanced-primary-care-pathway-july-2016.jpg)
















