Engaging Communities for Improved Maternal & Newborn Health in Ethiopia
30
Engaging Communities for Improving Reproductive, Maternal, Newborn and Child Health (RMNCH) in Rural Ethiopia: L10K Experience and Current Strategy London School of Hygiene & Tropical Medicine 22 nd March, London
-
Upload
ideas-at-the-london-school-of-hygiene-and-tropical-medicine -
Category
Health & Medicine
-
view
271 -
download
0
Transcript of Engaging Communities for Improved Maternal & Newborn Health in Ethiopia
Engaging Communities for Improving Reproductive, Maternal,
Newborn and Child Health (RMNCH) in Rural Ethiopia:
L10K Experience and Current Strategy
London School of Hygiene & Tropical Medicine 22nd March, London
Background
• The MMR, NMR and U5MR in Ethiopia are still high (which are
respectively 4.2, 28, and 68 deaths per 1,000 live births)
• However, Ethiopia is committed towards achieving the MMR, NMR and
U5MR reduction targets of SDG 3
• Ethiopia’s health sector transformation plan (HSTP), 2015–2020, is
aligned with the SDG targets; and aims to reduce MMR, NMR and
U5MR respectively to 2, 10, and 38 deaths per 1,000 live births, by 2020
• Enhancing community empowerment, engagement and participation is
one of the strategic objectives of HSTP
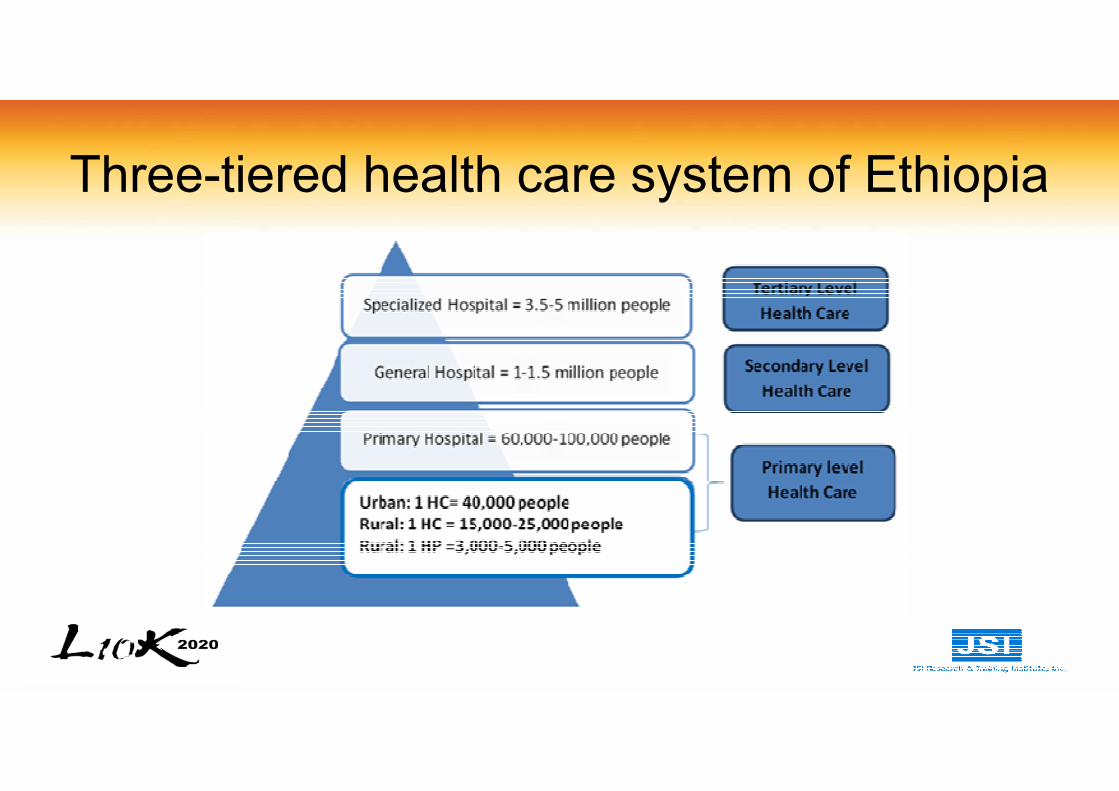
Three-tiered health care system of Ethiopia
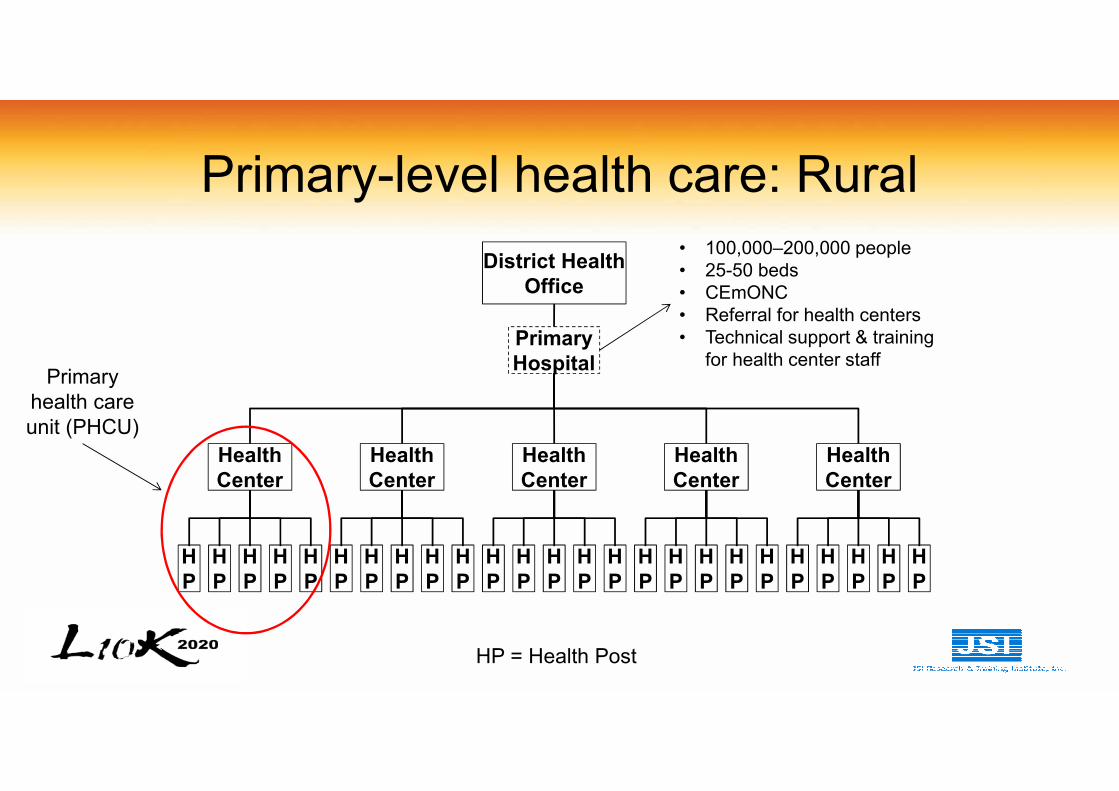
Primary-level health care: Rural
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
H
P
Health
Center
Health
Center
Health
Center
Health
Center
Health
Center
Primary
Hospital
District Health
Office
HP = Health Post
• 100,000–200,000 people
• 25-50 beds
• CEmONC
• Referral for health centers
• Technical support & training
for health center staffPrimary
health care
unit (PHCU)
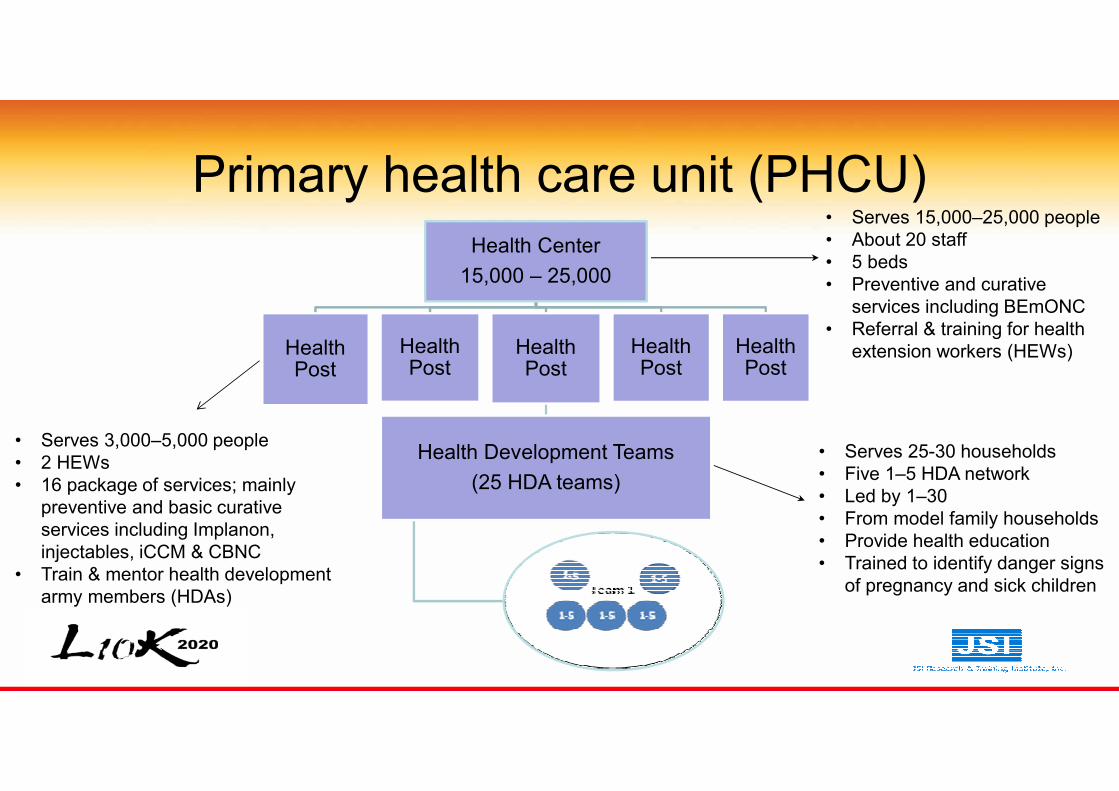
Primary health care unit (PHCU)
Health Center
15,000 – 25,000
Health Post
Health Post
Health Post
Health Development Teams
(25 HDA teams)
Health Post
Health Post
• Serves 15,000–25,000 people
• About 20 staff
• 5 beds
• Preventive and curative
services including BEmONC
• Referral & training for health
extension workers (HEWs)
• Serves 3,000–5,000 people
• 2 HEWs
• 16 package of services; mainly
preventive and basic curative
services including Implanon,
injectables, iCCM & CBNC
• Train & mentor health development
army members (HDAs)
• Serves 25-30 households
• Five 1–5 HDA network
• Led by 1–30
• From model family households
• Provide health education
• Trained to identify danger signs
of pregnancy and sick children

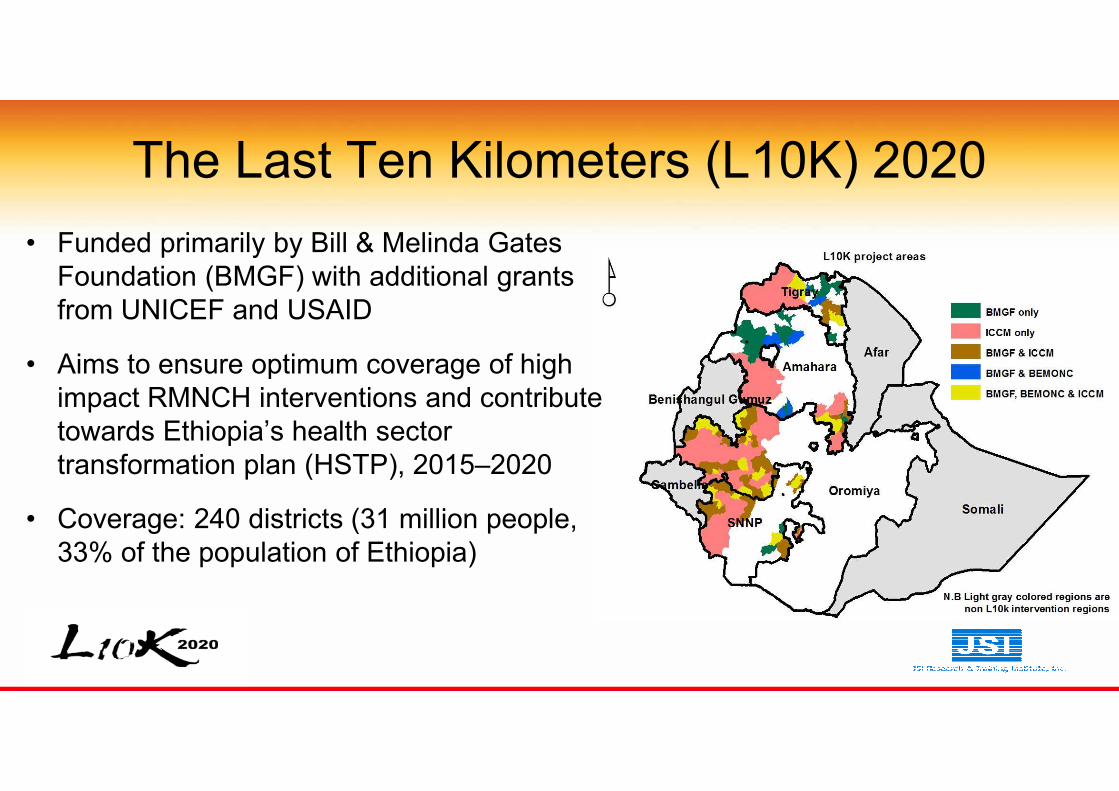
The Last Ten Kilometers (L10K) 2020
• Funded primarily by Bill & Melinda Gates
Foundation (BMGF) with additional grants
from UNICEF and USAID
• Aims to ensure optimum coverage of high
impact RMNCH interventions and contribute
towards Ethiopia’s health sector
transformation plan (HSTP), 2015–2020
• Coverage: 240 districts (31 million people,
33% of the population of Ethiopia)
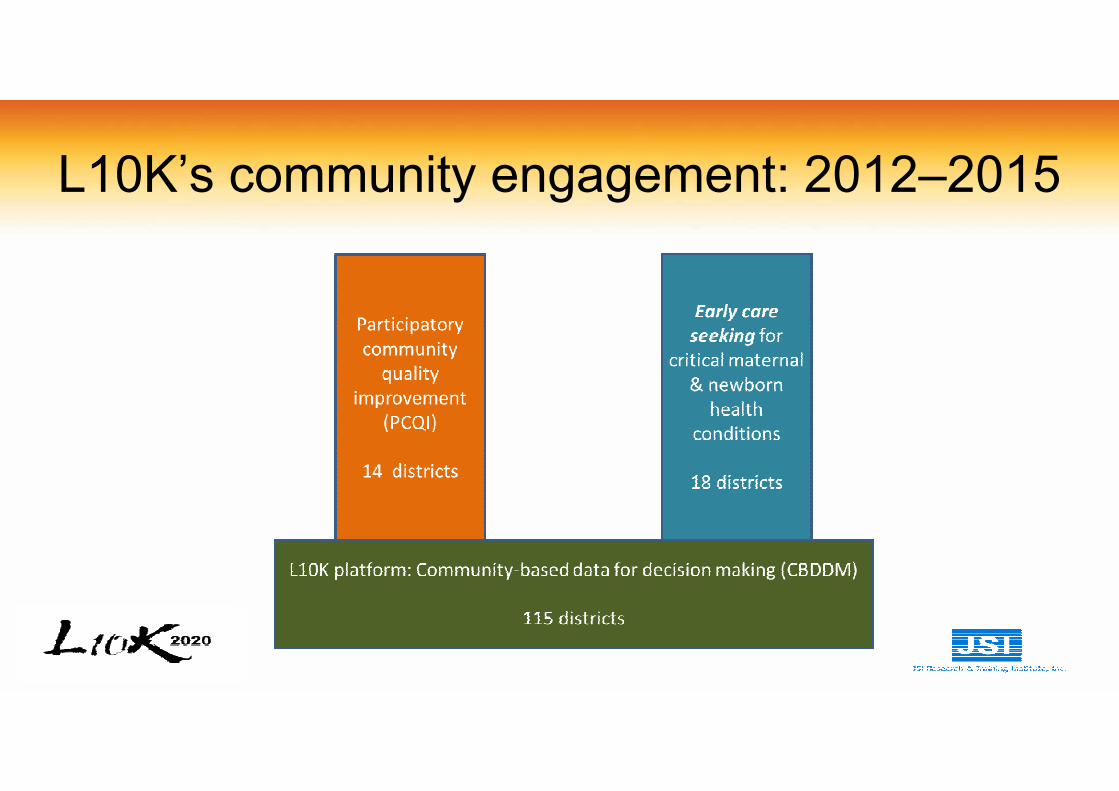
L10K’s community engagement: 2012–2015
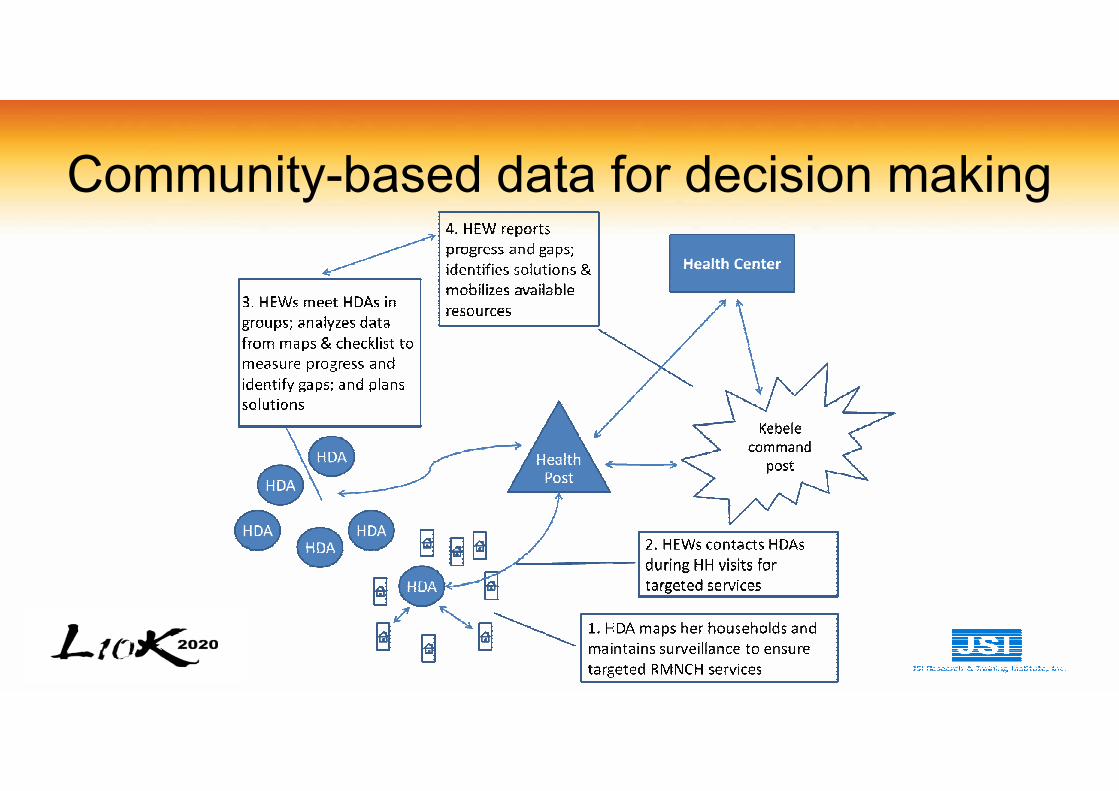
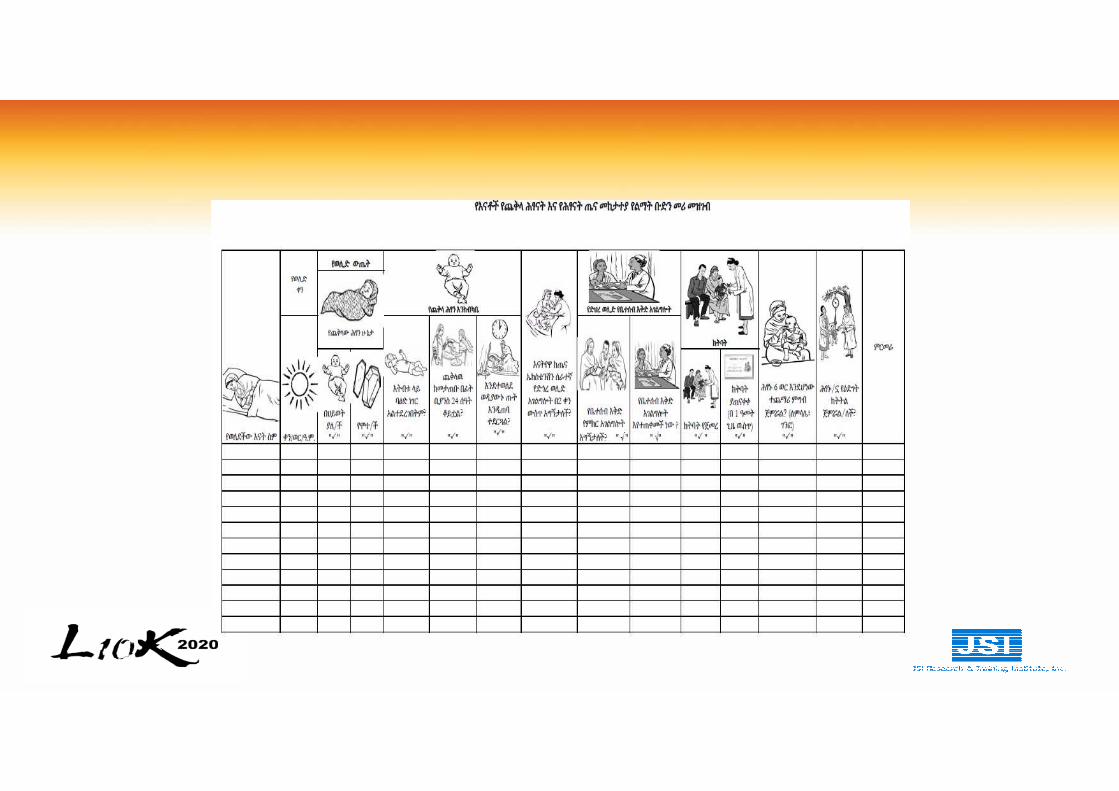
Community-based data for decision making

Surveillance for targeted RMNCH services
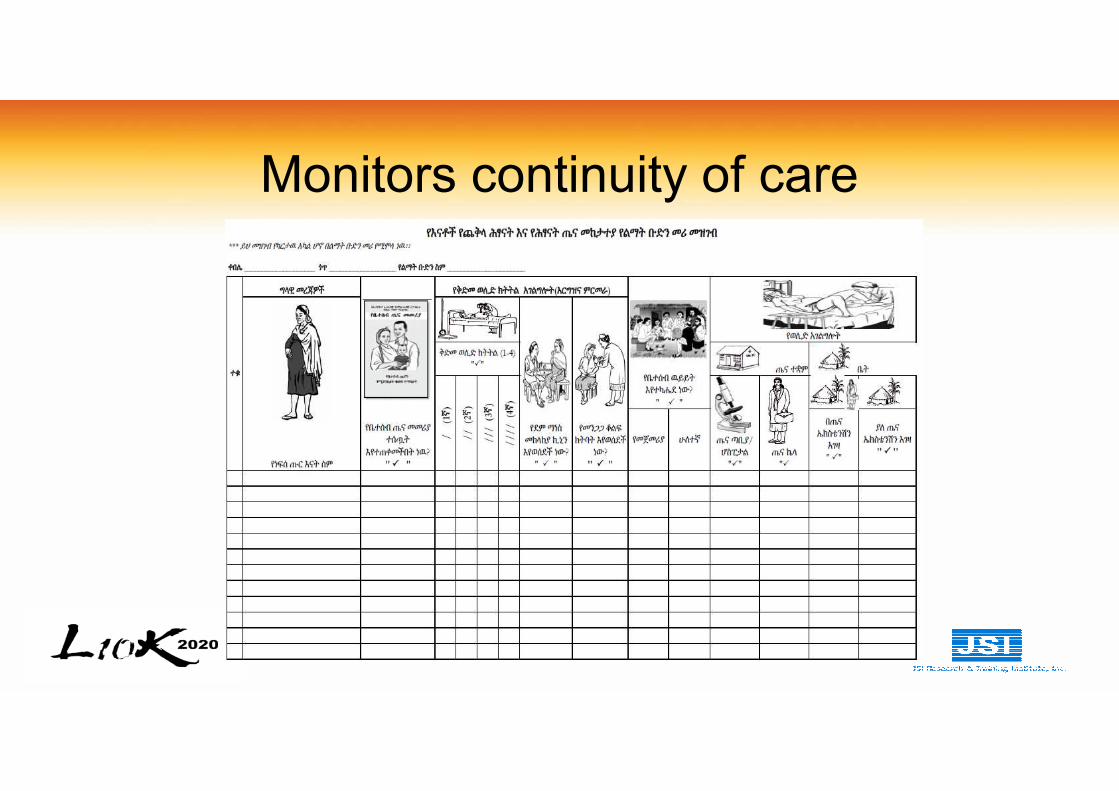
Monitors continuity of care
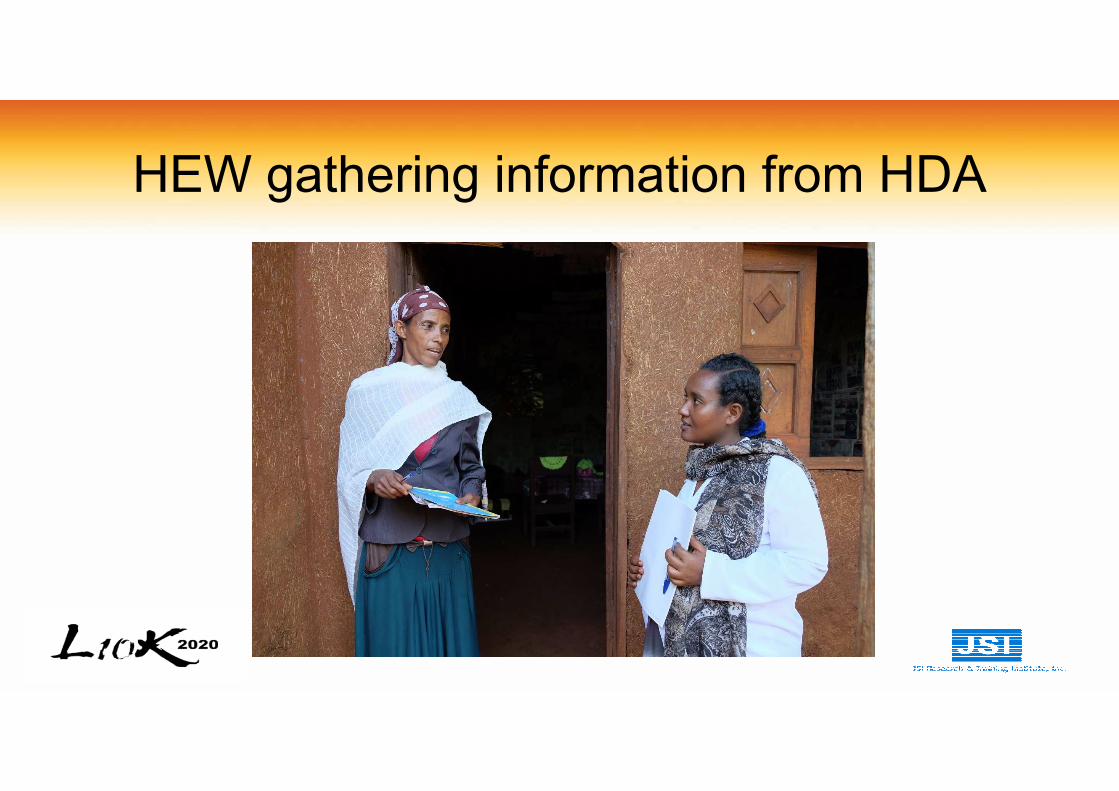
HEW gathering information from HDA
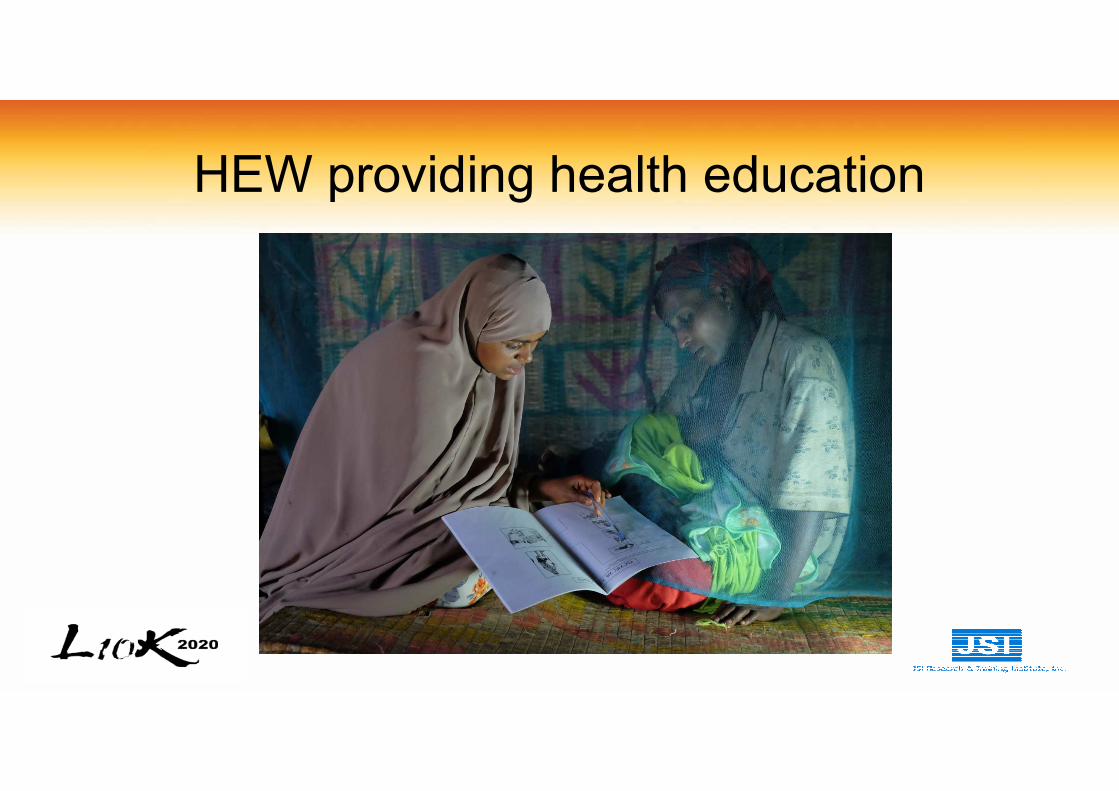
HEW providing health education
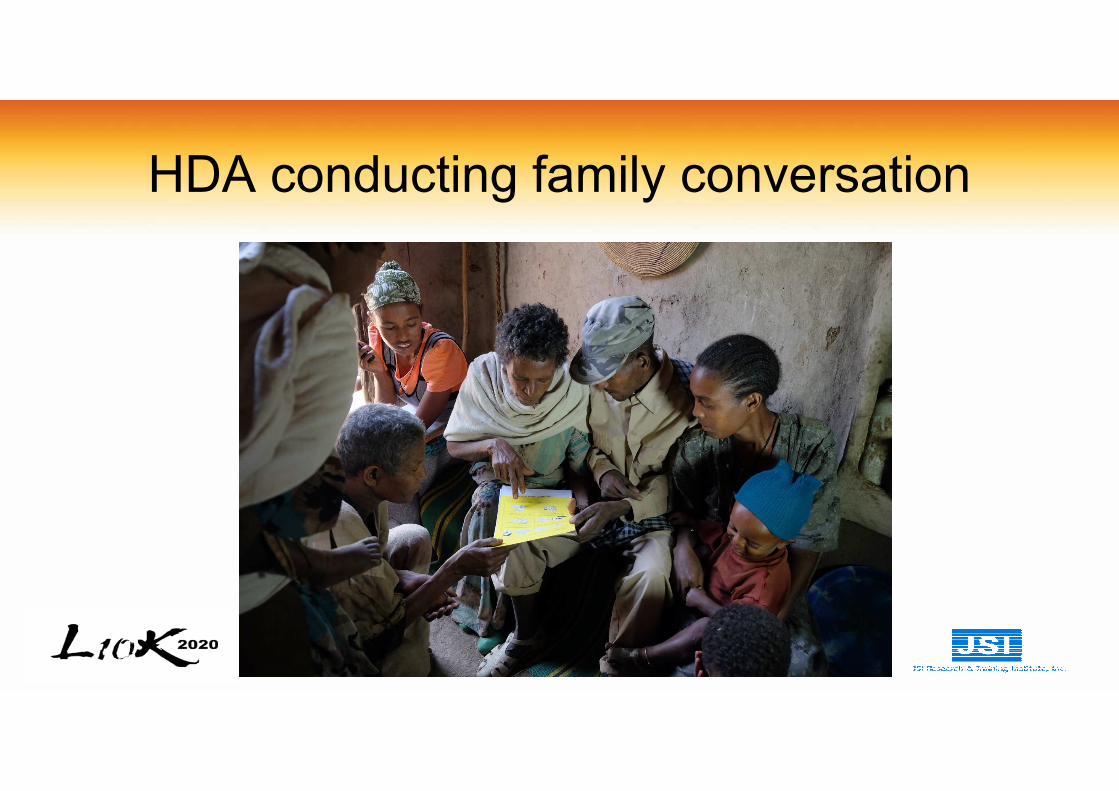
HDA conducting family conversation
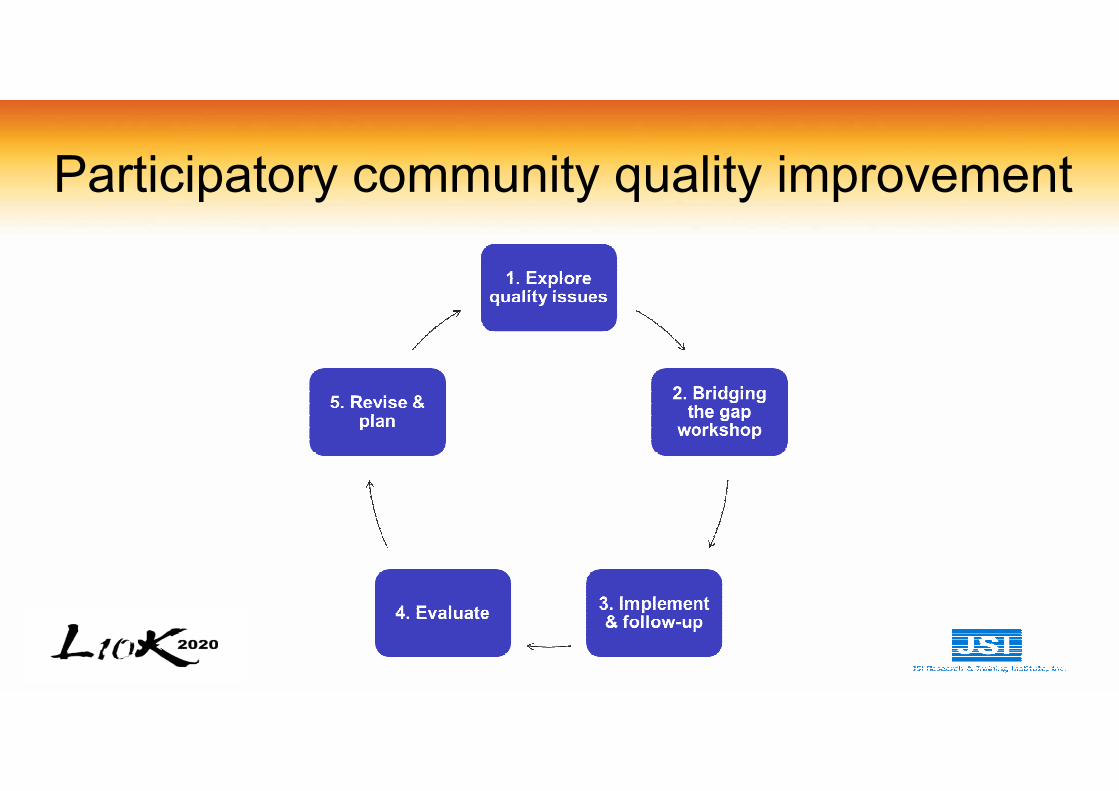
Participatory community quality improvement

Quality improvement team review meeting
Examples of community actions
• Facilitate transport of vaccines and other supplies
• Improved health post infrastructure (water, electricity)
• Transporting laboring mothers
• Building accommodations for HEWs
Referral Solutions
• Mapping of referral resources: key-informant interviews, desk review, FGD
• Participatory design of innovations:Consultative workshop and joint action plan
• Active management of referrals: implement, monitor and evaluate
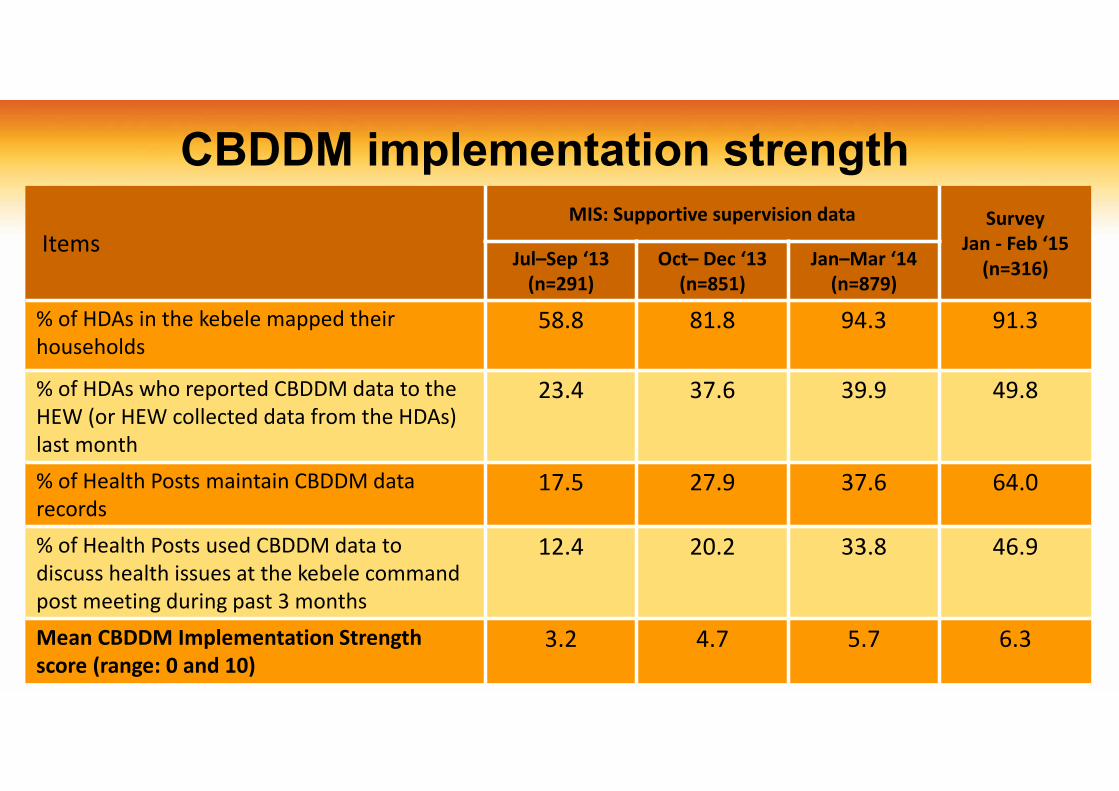
CBDDM implementation strength
Items
MIS: Supportive supervision data Survey
Jan - Feb ‘15
(n=316)Jul–Sep ‘13
(n=291)
Oct– Dec ‘13
(n=851)
Jan–Mar ‘14
(n=879)
% of HDAs in the kebele mapped their
households
58.8 81.8 94.3 91.3
% of HDAs who reported CBDDM data to the
HEW (or HEW collected data from the HDAs)
last month
23.4 37.6 39.9 49.8
% of Health Posts maintain CBDDM data
records
17.5 27.9 37.6 64.0
% of Health Posts used CBDDM data to
discuss health issues at the kebele command
post meeting during past 3 months
12.4 20.2 33.8 46.9
Mean CBDDM Implementation Strength
score (range: 0 and 10)
3.2 4.7 5.7 6.3
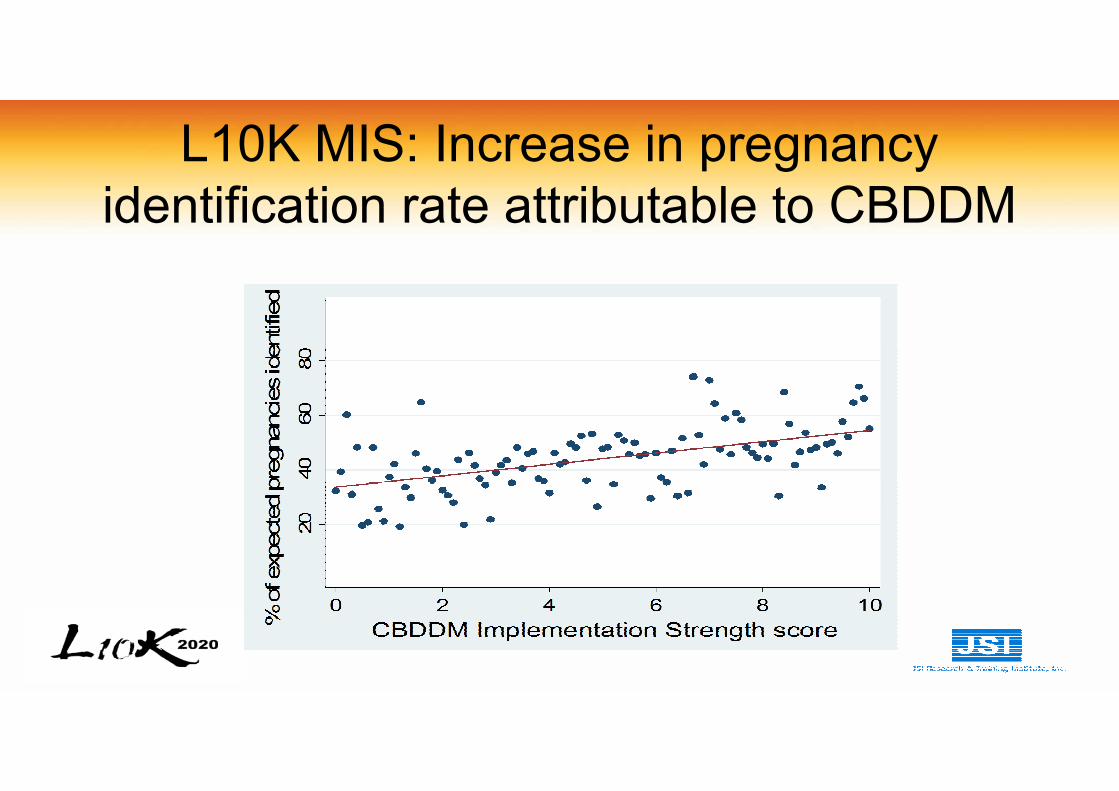
L10K MIS: Increase in pregnancy
identification rate attributable to CBDDM
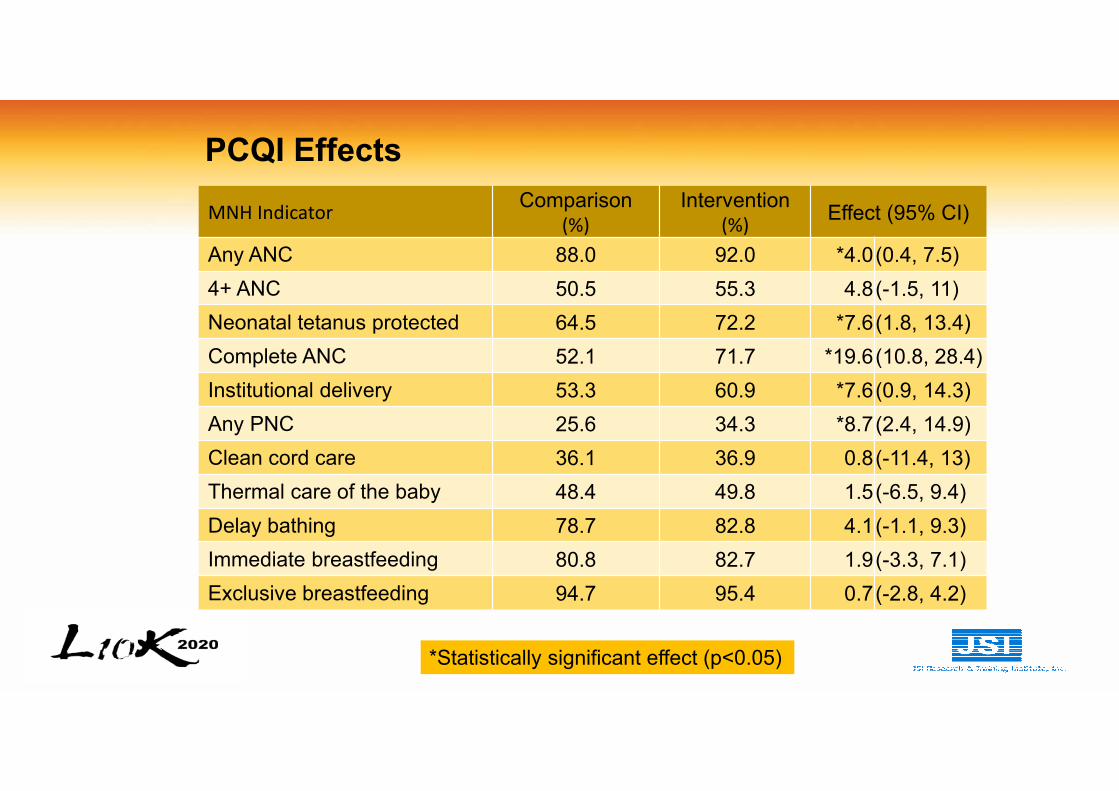
PCQI Effects
MNH IndicatorComparison
(%)
Intervention (%)
Effect (95% CI)
Any ANC 88.0 92.0 *4.0(0.4, 7.5)
4+ ANC 50.5 55.3 4.8(-1.5, 11)
Neonatal tetanus protected 64.5 72.2 *7.6(1.8, 13.4)
Complete ANC 52.1 71.7 *19.6(10.8, 28.4)
Institutional delivery 53.3 60.9 *7.6(0.9, 14.3)
Any PNC 25.6 34.3 *8.7(2.4, 14.9)
Clean cord care 36.1 36.9 0.8(-11.4, 13)
Thermal care of the baby 48.4 49.8 1.5(-6.5, 9.4)
Delay bathing 78.7 82.8 4.1(-1.1, 9.3)
Immediate breastfeeding 80.8 82.7 1.9(-3.3, 7.1)
Exclusive breastfeeding 94.7 95.4 0.7(-2.8, 4.2)
*Statistically significant effect (p<0.05)
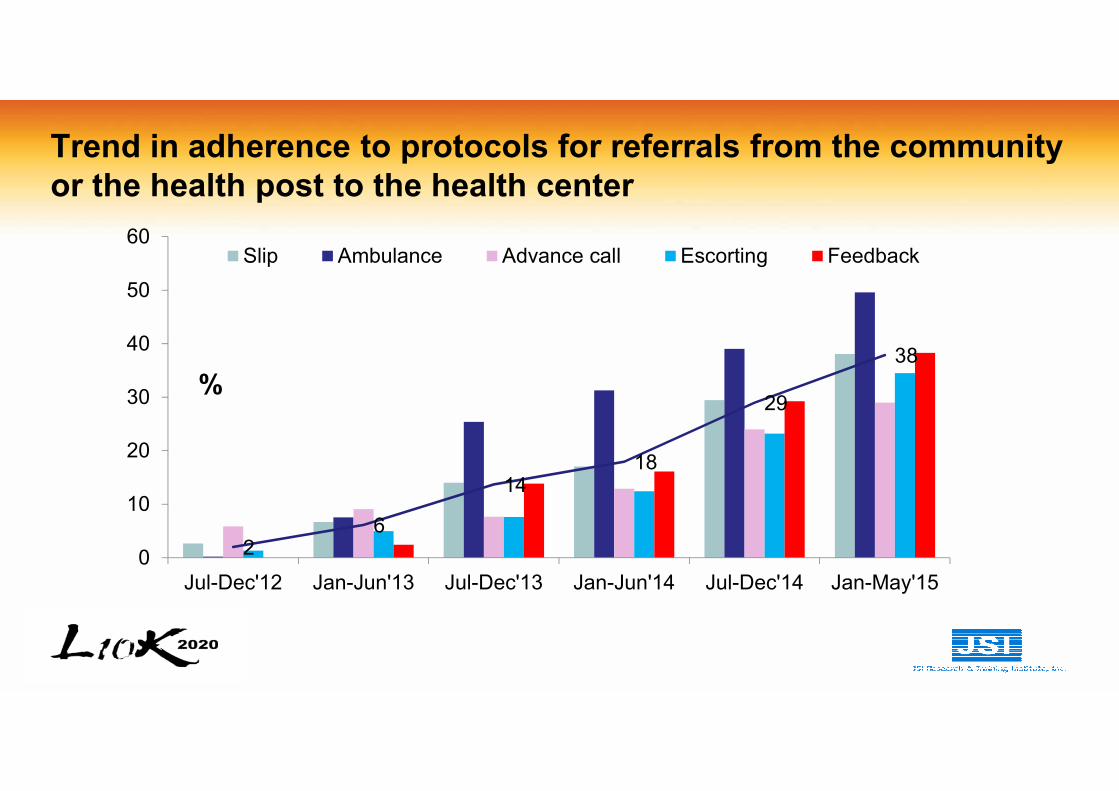
Trend in adherence to protocols for referrals from the community
or the health post to the health center
26
1418
29
38
0
10
20
30
40
50
60
Jul-Dec'12 Jan-Jun'13 Jul-Dec'13 Jan-Jun'14 Jul-Dec'14 Jan-May'15
%
Slip Ambulance Advance call Escorting Feedback
Policy outcome
• CBDDM is now part of the Integrated Refresher Training
for the HEWs
Lessons learned: CBDDM
• Drivers of adopting CBDDM as the national strategy
– Aligned with national priority—community engagement & pregnancy care
– The national HDA strategy needed a focused approach
– Aligned with HEW work flow
– Field visit by policy makers—strategy appeared doable and promising
– Participation in national level working groups
– Demonstrability of credible evidence
– Recognition and trust
– Donor support
Lessons learned: PCQI
• Community participation and empowerment can
strengthen the performance of health systems
• Demand to ensure quality of services at health centres
• Communities can be an integral part of quality
improvement strategies
Lessons learned: Referral Solutions
• Stakeholders’ ownership of problems and proposed
solution
• Engaging stakeholders across each level of the referral
system created an awareness of the challenges and a
greater sense of commitment to jointly address them
• Consultative and monthly and quarter review meetings
created a platform for building relationships across each
level of the referral system
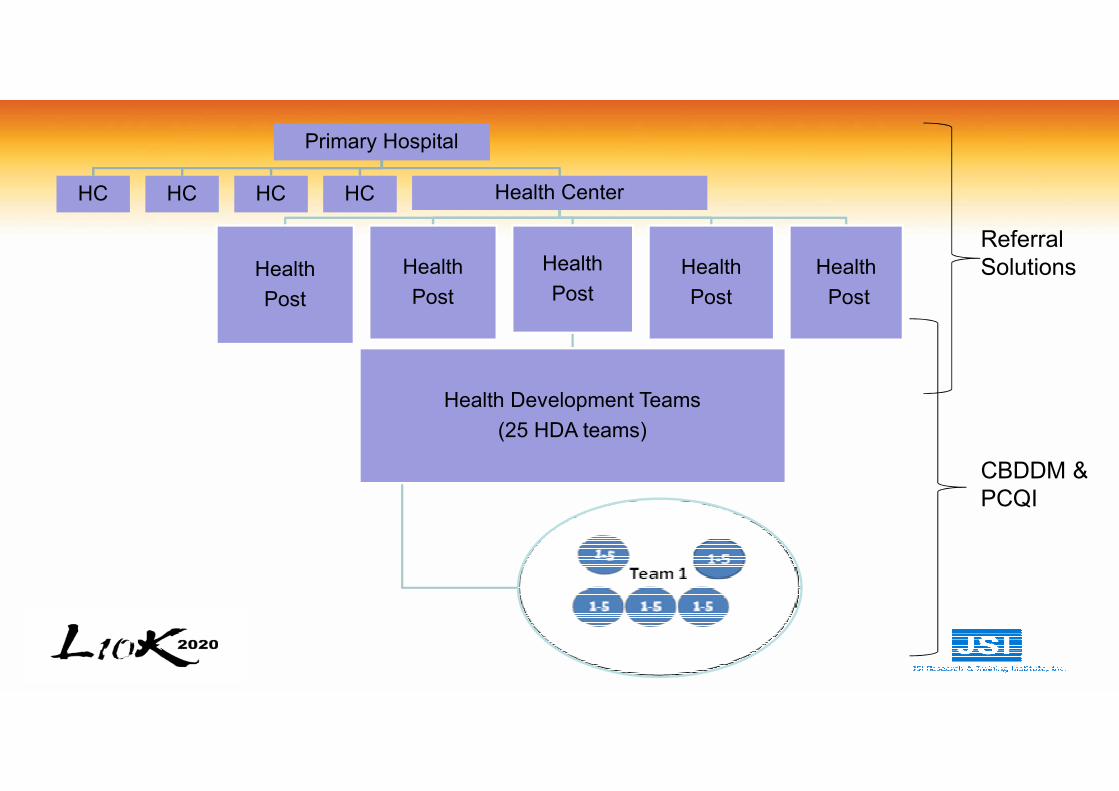
Primary Hospital
HC HC HC HC Health Center
Health
Post
Health
Post
Health
Post
Health Development Teams
(25 HDA teams)
Health
Post
Health
Post
CBDDM &
PCQI
Referral
Solutions
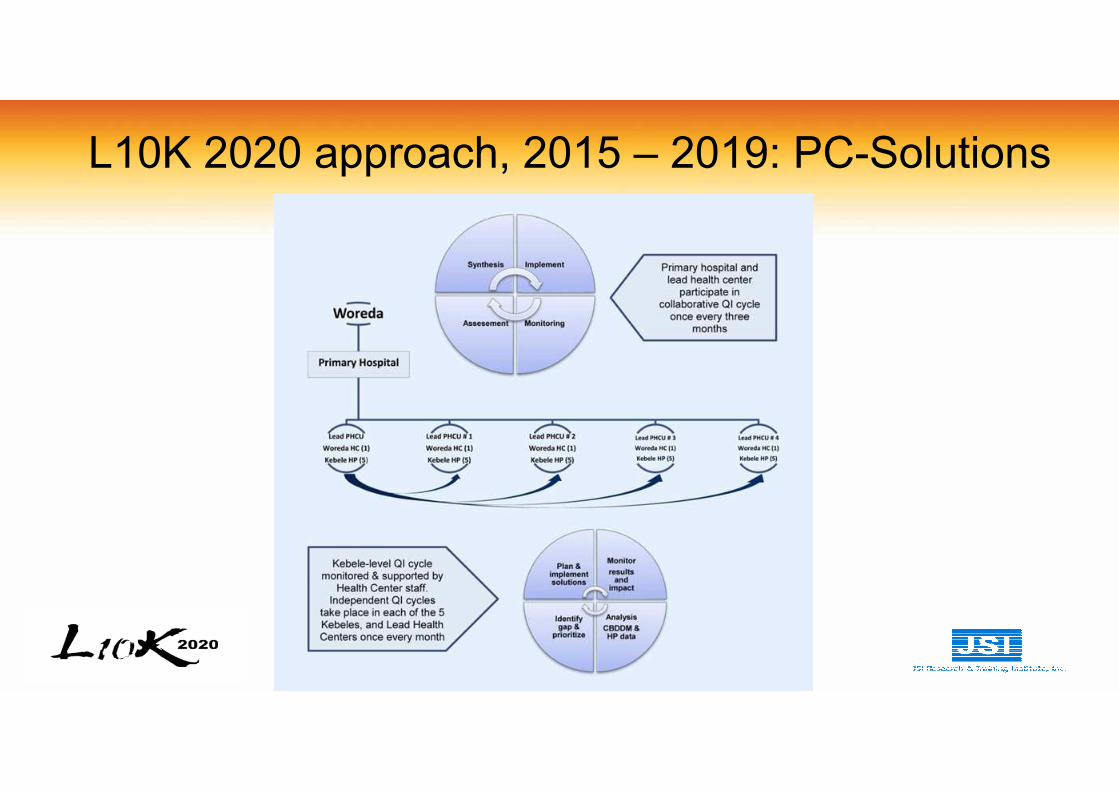
L10K 2020 approach, 2015 – 2019: PC-Solutions