Myvisualresume 13321897241742-phpapp02-120319154635-phpapp02

of 60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
1/60
Endoscopic
Parathyroid Surgery
Danny Yacoub MDGeorge Ferzl i MD, FACS
Professor of Surgery, SUNY
SUNY Downstate
Medical Center
Lutheran
Medical Center
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
2/60
The Legacy of Ivar Sandstrom (18521889)
New Gland, the last majororgan to be recognized inman, 1880.
Discovery met with silence.
First publication rejected.
Two national prizes.
I.V. Sandstrom, On new gland in man and several mammals, Bull Inst Hist Med6 (1938), pp. 192222.c
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
3/60
to each gland there are
often one or more small
arteriole branches from theinferior thyroid artery
I.V. Sandstrom, On new gland in man and several mammals, Bull Inst Hist Med6 (1938), pp. 192222.c
The Legacy of Ivar Sandstrom (18521889)
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
4/60
The Legacy of Ivar Sandstrom (18521889)
I.V. Sandstrom, On new gland in man and several mammals, Bull Inst Hist Med6 (1938), pp. 192222.c
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
5/60
First Parathyroid Surgery
1925 by Felix Mandl in Vienna, Austria
Patient had resolution of severe symptomsassociated with the disease after surgery.
Niederle BE etal,J Am Coll Surg. 2006
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
6/60
Captain Charles Martell Firstto be surgically treated in US, 1932.
Underwent 6 unsuccessful neck explorations.
O. Cope, The story of hyperparathyroidism at the Massachusetts General Hospital, N Engl J
Med274 (1966), pp. 11741182
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
7/60
Edward Churchill (1895-1972)
He performed his 7th operation
Median sternotomy
Successful operation
O. Cope, The story of hyperparathyroidism at the Massachusetts General Hospital,N Engl J Med
274 (1966), pp. 11741182
Unfortunately, Martell died soon
after due to tetany and
complications of nephrolithiasis.
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
8/60
Parathyroid Surgery
New Technology:
IOPTH
Tieless surgery
Intraoperative nerve monitoring Radioguided surgery
Needle localization
Video assisted surgery
Robotic surgery
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
9/60
Minimally Invasive Parathyroid Surgery
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
10/60
Why MIVAP? Cosmetic Results
Open surgery scar Minimally invasive / endoscopic scars
http://azfamily.beloblog.com/catsmeow/scar.html7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
11/60
Minimally invasive parathyroid surgery:
Endoscopic Central
Lateral
Other (transaxillary,transpectoral, transoral)
Minimally invasive MIVAP (min. invasive video
assistedparathyroidectomy)
Robotic assisted
Inferior parathyroid release inminimally invasive thyroidectomy
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
12/60
MIVAP-Results
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
13/60
MIVAP yield equivalent endocrine results as openprocedure
Oncologic result is equivalent in selected patients
Equivalent safety profile as open procedures
Postop pain is decreased
Patient satisfaction with procedure and cosmetic result issignificantly increased
MIVAP vs Open - Results
Miccoli et al., RCT, Surgery. 2001
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
14/60
1o end points: pHPT Hypocalcemia (All patients were cured)
2o end points: MIVAP vs. OMIP OR time: similar, ave. 42min vs. 49min (p=0.22)
scar length: ave. 17.2mm vs. 30.8mm (p
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
15/60
Parathyroid Surgery
Single parathyroid adenoma (80%-87%)
Double adenomas (2%-15%)
Asymmetric 4-gland hyperplasia (10%-15%)
Carcinoma (
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
16/60
Preoperative Imaging
Non Invasive Imaging: Sestamibi Scan
Ultrasound
CT scan
MRI
Positron Emission Tomography (PET) scan PET/CT
Invasive Imaging: Parathyroid FNA
Arteriography and selective venous sampling for PTH
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
17/60
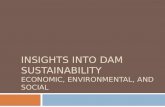
Parathyroid Locations
Possible locations of enlarged parathyroid glands in the neck and
superior mediastinum with the use of an anteroposterior projection (A)
and a lateral projection (B)
Udelsman R.Ann Surg244:471-479, 2006
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
18/60
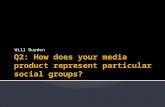
Aberrant Parathyroid Locations
Anatomic locations of abnormal parathyroid glands found at reoperation by single group.
Most common ectopic sites mirror routes of descent of upper parathyroid glands (short
migration path) and of lower parathyroid glands (longer migration path in association with
thymus)
Wang CA. Parathyroid re-exploration.Ann Surg. 1977;186:140
145
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
19/60
Preoperative Parathyroid Localization
Ultrasonography: Sensitivity 70-80%(less in MGD)
Specificity 40-100%(Ammori, Ann R Coll Surg Engl. 1998;80:433437)
CT and MRI: Sensitivity 60-80% (80% when done with IV contrast)
(Weber, Radiol Clin North Am. 2000;38:11051129)
Scintigraphy intraoperative gamma probe:
99mTc-Sestamibi SPECT: Sensitivity 85-95%(Originally described by Coakley et al., Nucl Med Commun. 1989;10:791794)
99mTc-Tetrofosmin provided it is used within a dual-tracer subtraction protoco(Gallowitsch et al., Invest Radiol. 2000;35:453459)
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
20/60
Sestamibi
EctopicAdenoma
Hyperplasia
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
21/60
Sonogram / Sestamibi
Are additional Localization Studies and Referral indicated for patients with Primary Hyperparathyroidism Who
have negative Sestamibi scan results? Elaraj, DM. Sippel, RS. Lindsay S. Sansano I. Duh QY. Clark OH.
Kebebew E.Arch SurgVol 145, No 6, 578-581 June 2010.
May 2005 - May 2007
487 patients underwent 492 neck explorations (88% initial 12% reoperation).
339 underwent focused parathyroid surgery (69%).
447 Sestamibi scans were positive (91%) and 82% were true positive
In patients with negative Sestamibi scan, Sono was positive in 51% (43% true positive).
Patients with positive sestamibi when compared to patients with negative sestamibi:
-Higher rate of single gland disease (87% vs 63%)
-Lower rates of of double adenomas (6% vs 22%) and asymmetric hyperplasia (7% vs 15%).
--No difference in the rate of ectopic glands.
--No difference in the cure rate (97% vs 89%).
-Conclusion: Additional imaging with sonogram is helpful for selecting minimally invasive
Parathyroidectomy in most patients with primary hyperparathyroidism who have negative
Sestamibi scan results.
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
22/60
Intra operative PTH assay. Prospective 361
consecutive patients undergoing minimally invasiveparathyroidectomy.Hwang RS et al.Ann Surg2010;251:1122-1126.
1- There is no role for IOPTH for Sestamibi positive patients.
2- It will guide the surgeon in Sestamibi negative / positive sonogram
patients: In these cases an inadequate fall in the 10- minute post excision
PTH level was highly predictive of multi glandular disease.A Selective Bayesian approach to Intraoperative PTH monitoring.
A Rising IoPTH Level Immediately after Parathyroid ResectionAre Additional Hyperfunctioning Glands Always Present? Anapplication of the Wisconsin Criteria.Cook MR et alAnn Surg 2010;251 1127-1130.
797 consecutive patients. 108 (14%) had a rising ioPTH 5 min after resection
of a single parathyroid gland, 36 (33%) continued to have elevated levels and
further exploration revealed additional hyperfunctioning glands. In 72 (67%)
the ioPTH started to drop within 20 min of gland resection and in all cases
correctly predicted operative success.
IOPTH / Sonogram
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
23/60
CT Sestamibi Fusion Scan
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
24/60
4D-CT Localization
45 patients underwent reoperative parathyroidectomy.
The sensitivity of 4D-CT for localization was 88%compared with 54% for Sestamibi imaging.
4D-CT correctly localized (p=0.0003) and laterlized(p=0.005) hyperfunctional parathyroid tissue thanSestamibi did.
Parathyroid Exploration in the Reoperative Neck:Improved Preoperative Localization with 4D-ComputedTomography.
Mortenson MM et al. JACS May 2008 Volume 206 No 5 pages 888-895.
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
25/60
CT Guidance
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
26/60
Ultrasound Guidance
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
27/60
MIVAT
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
28/60
Endoscopic ParathyroidectomyPrerequisite Conditions 1
1- The surgeon must be experienced in conventional
parathyroid surgery and trained for endoscopic neck
procedures
2- The patient must be carefully selected
3- The adenoma must be clearly localized
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
29/60
Patients Eligible for EndoscopicParathyroidectomy
No goiter
No previous neck surgery
Sporadic HPT I
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
30/60
Evaluation for Concomitant Thyroid Nodules and PHPT inPatients Undergoing Parathyroidectomy or Thyroidectomy
200 patients who underwent a parathyroidectomy
102 (51.1%) were found to have thyroid nodular
disease
Six percent of these 200 patients also had a thyroidmalignancy
Of the 326 patients who were primarily seen for thyroid
disease, the incidence of PHPT was 3.1%
Morita S, etal, Surgery, 2008
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
31/60
Racial Disparity / Double Adenoma
AA
12%
Non-AA
5%
AfricanAmericans
14
(12.4%)
Non-AfricanAmericans
21
(5.1%)
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
32/60
Sestamibi and Vitamin D Deficiency
Prevalence of vitamin D deficiency in PHPT
Predictive value of 25 (OH) D levels in having positivesestamibi scans.
428 consecutive patients who underwent preoperative sestamibi
scintigraphy and a targeted parathyroidectomy for PHPT.
Parathyroid sestamibi scanning is more useful for thissubset of patients
Kandil. E. et alArch of Otolaryngology, 2008
Ad Si d
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
33/60
Adenoma Size andBiochemical Measurements
Preoperative serum calcium and parathormone levels predict
adenoma weight and volume in primary hyperparathyroidism for a
single adenoma.
(Bindlish. Head Neck. 2002 Nov; 24 (11): 1000-3)
More than a 50% decrease in preexcision iPTH levels and
subsequent attainment of the normal range within 15 min is
considered satsifactory.
(Ozimek et al. Surg Endosc. 2010 May 20)
Adenoma weight may relate to the percentage decrease of iPTH
levels at the 10-minute postparathyroidectomy interval.
(Moretz et al. Laryngoscope. 2007 Nov; 117 (11): 1957-60)
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
34/60
Endoscopic/Conventional Parathyroidectomy
(98-2005 / 970 HPT I)
Endoscopic 538 (55.5%)
Conventional 432 (44.5%)
Jean - Francois Henry Department of Endocrine Suregery, University Hopspital La Timone.Marseilles, France Endoscopic Parathyroidectomy: Why and When ? World Journal of Surgery
Volume 32 Number 11, November 2008
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
35/60
Clear positive localization:
Posterior: lateral approach
Anterior: anterior approach
Negative or unclear localization:
Conventional approach
Endoscopic/Conventional Parathyroidectomy
Jean - Francois Henry Department of Endocrine Suregery, University Hopspital La Timone.Marseilles, France Endoscopic Parathyroidectomy: Why and When ? World Journal of SurgeryVolume 32 Number 11, November 2008
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
36/60
Contraindications: 432/970: 44.5 % Associated nodular goiter 174
No preoperative localization 107
Previous neck surgery 71
Suspicion of MGD 45
Acute HPT 8
Large tumor 7
Local anesthesia 9
Major ectopia 9
Spontaneous neck hematoma 2
Jean - Francois Henry Department of Endocrine Suregery, University Hopspital La Timone.Marseilles, France Endoscopic Parathyroidectomy: Why and When ? World Journal of Surgery
Volume 32 Number 11, November 2008
Endoscopic/Conventional Parathyroidectomy
E d i P th id t
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
37/60
Endoscopic Parathyroidectomyin the Previously Radiated Neck
May 2005-May 2007: 491 consecutive
parathyroidectomies for primary hyperparathyroidism. 52(12.6%) with history of neck radiation.
In the radiation exposure group, 40 (76.9%) had a
positive sestamibi scan vs 360 (81%) in the non radiated
group. The radiation group was older at presentation (p=0.001)
and the rate of previous history of thyroid cancer was
higher (p=0.02).
Patients with PHPT, previous RT, positive localizationstudy and a normal thyroid ultrasound would be ideal
candidates for minimally invasive parathyroidectomy.
Prior Head and Neck Radiation Exposure Is not a Contraindication to Minimally Invasive
Parathyroidectomy. Rahbari R. et al JACS Vol210 No 6. 942-948 June 2010.
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
38/60
MIVAP -Technique
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
39/60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
40/60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
41/60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
42/60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
43/60
Bilateral Axillo-Breast (BABA)
Subcutaneous dissection bilaterally from the incision to
the thyroid cartilage and the SCM
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
44/60
Axillary Approach
First introduced by Ikeda,2000
4-6 cm vertical skin
incision in the axilla forcamera port and two
working ports
0.5 cm incision on themedial side of the
anterior chest wall
T ill A h
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
45/60
Transaxillary Approach
R b ti A h
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
46/60
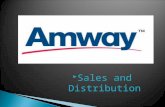
Robotic Approach
Arm 1
Camera
Arm 2Arm 3
This approach was
developed in South Korea
by Dr. Woong Chung atYonsei University College
of Medicine in Seoul. He
reported his experience
with 338 patients
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
47/60
Confidential
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
48/60
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
49/60
Confidential
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
50/60
Confidential
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
51/60
Fourth arm trocar
External retractor
Connected withcontinuous suction
system
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
52/60
Maryland dissector
Harmonic curved shears
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
53/60
Confidential
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
54/60
The Cervical / Direct Approaches:
- Anterior cervical approach
- Lateral cervical approach
- Video-assisted approach
Pros: Less pain, better cosmesis and shorter hospital stay
Cons: visible scars, not much different than open withsmall incision
The Extra-cervical Approaches:
- Axilla, chest or both.
Pros: scarless (in the neck)
Cons: extensive dissection, paresthesia, musclestiffness,operative time and learning curve
Endoscopic Parathyroidectomy
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
55/60
Conclusions
Endoscopic parathyroidectomy is feasible and
has good results.
The key to success is patient selection andsurgeon experience.
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
56/60
Endoscopic Parathyroidectomy
Should be proposed in carefully selected patients.
Has the main advantage of offering a magnified view and
a light that permit a safe dissection.
The lateral approach is particularly suitable for
adenomas posteriorly located in the neck
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
57/60
Endoscopic Parathyroidectomy
Small tumors
Benign tumors
No surgical reconstruction
C it t Th id Di
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
58/60
Concomitant Thyroid Disease
The use of a double-tracer technique (123I/99mTc-sestamibi or99mTc
pertechnetate/99m
Tc-sestamibi) or (99mTc-sestamibi scintigraphy) combinedwith US examination might be useful in planning the type and extent of surgery:
Bilateral neck exploration in the case of any PHPT patient with concomitant
multinodular goiter unilateral neck exploration in the case of a solitary
parathyroid adenoma with concomitant nodular goiter located in the ipsilateral
thyroid lobe
Gamma probe guided minimally invasive parathyroidectomy (GP-MIP) in the
case of a solitary 99mTc-sestamibi-avid parathyroid adenoma with a normal
thyroid gland endoscopic surgery in the infrequent case of a solitary 99mTc-
sestamibi negative (but US positive) parathyroid adenoma with a normal thyroid
gland.
Mariani et al. Journal of Nuclear MedicineVol. 44 No. 9 1443-1458
E d i /C ti l P th id t
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
59/60
Conversions: 13.2%
Operative time: 48' (16'-130')
Complications-Hematoma in sternocleidomastoid 3
Definitive recurrent nerve palsy 1
Capsular disruption 10
Persistent HPT: 3
Recurrent HPT: 1
Jean - Francois Henry Department of Endocrine Suregery, University Hopspital La Timone.Marseilles, France Endoscopic Parathyroidectomy: Why and When ?World Journal of Surgery
Volume 32 Number 11, November 2008
Endoscopic/Conventional Parathyroidectomy
E d i /C ti l P th id t
7/27/2019 endoscopicparathyroidsurgery-110216104950-phpapp02
60/60
CONVERSIONS 71/538: 13.2 %
Missed adenoma 18
Difficulties of dissection 16
QPTH assay true negative *18
QPTH assay false negative 4 Sestamibi false positive 11
Ultrasonography false positive 4
* 18 multiglandular diseases
Jean - Francois Henry Department of Endocrine Suregery, University Hopspital La Timone.Marseilles, France Endoscopic Parathyroidectomy: Why and When ? World Journal of SurgeryV l 32 N b 11 N b 2008
Endoscopic/Conventional Parathyroidectomy