Endodontics - Endodontists: the root canal specialists - AAE
10
Colleagues for Excellence Published for the Dental Professional Community by the American Association of Endodontists Winter 2007 Bisphosphonate-Associated Osteonecrosis of the Jaw ENDODONTICS
Transcript of Endodontics - Endodontists: the root canal specialists - AAE

Colleagues for Excellence
Published for the Dental Professional Community by the
American Association of Endodontists
Winter 2007
Bisphosphonate-Associated Osteonecrosis of the Jaw
Endodontics

here has been a burgeoning demand for information about bisphosphonates over the past three to four years due to an increasing awareness of this drug’s
rare adverse side effect of osteonecrosis of the jaw (ONJ). The medical and dental community’s realization of this complication has been correspondingly disseminated to the public through various media outlets, Internet Web sites and position statements proffered by the United States Food & Drug Administration, as well as several pharmaceutical companies. One only has to venture through the multitude of Internet search engines to see that the legal community is also an interested party to bisphosphonate-induced ONJ.
The dental profession is certainly in an advantageous position to educate the public and be at the forefront in diagnosing this condition. It is incumbent upon us to be knowledgeable about this issue and be acquainted with the most current treatment recommendations and guidelines available. The goal of this informational article is to enhance your understanding about this frequently prescribed class of drugs with regards to its pharmacokinetics, mode of action, types of bisphosphonates and the implications of bisphosphonate-induced ONJ.
Use of Bisphosphonates
In 2005, more than 39 million prescriptions for oral bisphosphonates were written (31). America’s aging baby boomer population will likely produce
an amplification of those numbers over the next two decades. Bone fractures are the biggest problem facing most elderly individuals with bone disease, especially those with osteoporosis. The cumulative impact of these fractures is quite devastating. Osteoporotic fractures in the United States in 1995 led to more than half a million hospitalizations, over 800,000 emergency room encounters, more than 2.6 million physician office visits and the placement of nearly 180,000 individuals into nursing homes (U.S. Surgeon General Report 2004). It has been estimated that over a 10-year period, white women age 45 and older in the United States could experience 5.2 million fractures of the hip, spine or forearm, resulting in two million person-years of disability related to the fractures.
Bisphosphonates are generally prescribed in the prevention and treatment of resorptive bone diseases such as osteoporosis and bone metastasis (with or without hypercalcemia) associated with breast and prostate cancer. They are also recognized as an effective therapeutic for Paget’s disease (osteitis deformans) and other conditions that precipitate bone fragility, such as chronic renal disease in patients undergoing dialysis.
Bisphosphonates and Osteonecrosis of the Jaws
Bonefos® (Clodronate) and Didronel® (Etidronate) first-generation bisphos-phonates do not have an amino group
moiety (nitrogen containing) on the R2 long-side chain. It is the R2 chain that imparts the potency and method of affect on bone cells. First-generation bisphosphonates (non-nitrogen containing) do not appear to be implicated in bisphosphonate-associated osteonecrosis of the jaws (ONJ). Second- and third-generation bisphosphonates (nitrogen containing) including Zometa®
Endodontics: Colleagues for Excellence
�
T

(zolendronate), Aredia® (pamidronate) and Fosamax® (alendronate) inhibit specific enzymatic activity necessary for osteoclast cell formation (33, 34). Bisphosphonates are administered either parenterally (intravenously) or orally. What is significant to these two routes of administration is the bioavailability of the drug. The oral bioavailability is in the area of one percent due to the higher ionization at physiologic pH when absorbed through the intestinal mucosa (8, 39). Greater bioavailability through parenteral administration and concomitant potency are likely responsible for the higher incidence of ONJ in this group.
The accumulated body of literature is replete with case reports, letters to the editor, reviews and drug alerts by the U.S. FDA and pharmaceutical companies (2, 19, 24, 9, 35, 1, 4, 7, 11, 18, 20, 22, 25, 26, 27, 29, 31, 37, 43, 45, 10, 41, 13). This collective information points to an association between bisphosphonates and ONJ. With no current available randomized controlled trials or higher levels of clinical evidence, the following information is presented based on retrospective analysis of case reports and expert opinions.
Signs and symptoms of bisphosphonate-associated ONJ:
• An irregular mucosal ulceration with exposed bone in the mandible or maxilla
• Pain or swelling in the affected jaw
• Infection with or without purulence
• An altered sensation (e.g., numbness or heavy sensation)
Additional important issues related to bisphosphonate-associated ONJ include:
• The site of occurrence of osteonecrosis is the jaws; presentation occurs more frequently in the mandible than the maxilla.
• The mechanism for bisphosphonate–associated ONJ is unknown.
• There may be a predictive test that can be employed to assess risk for ONJ for individuals on bisphosphonates: Serum C-telopeptide, i.e., sCTX (44). This blood test is a serum blood turnover marker. The lower the number of circulating collagen fractions (type I collagen) the greater the suppression of bone turnover. Suppression of bone turnover can be an indicator for increased bone mineral density (BMD) and can possibly be related to its effects from bisphosphonates.
• The treatment for bisphosphonate–associated ONJ is problematic. Case reports document no response or a limited response to local surgical wound debridement, marginal or segmental resection, antibiotics and hyperbaric oxygen. Therefore, recognition of risk factors and application of preventive dental treatment procedures are important for patients taking I.V. and perhaps oral bisphosphonates.
Common risk factors associated with the development of bisphosphonate-associated ONJ include:
• History of taking bisphosphonates, especially I.V. formulations. The concurrent use of steroids appears to contribute to this risk.
Endodontics: Colleagues for Excellence
�
Continued on p. 4

• Previous history of cancer (e.g., multiple myeloma or metastatic disease to bone), osteoporosis, Paget’s disease, chronic renal disease on dialysis or other indications for bisphosphonate treatment.
• A history of a traumatic dental procedure. Most case reports occur after a tooth extraction, although other traumatic dental procedures may also be associated with the occurrence of ONJ. One case report describes bisphosphonate–associated ONJ occurring six months after placement of five dental implants with the subsequent loss of all implants (38).
• Several reports indicate the spontaneous development of bisphosphonate-associated ONJ without a prior traumatic dental procedure.
As of the writing of this article, it is not established whether bisphosphonate-associated ONJ is a drug effect (i.e., observed with only a few bisphosphonates) or a class effect (i.e., may occur with all bisphosphonates with the incidence varying according to potency or other factors). To date, the majority of reports have described ONJ occurring in patients undergoing bisphosphonate infusion (e.g. zolendronate [Zometa®] or pamidronate [Aredia®]). Nevertheless, in several publications, oral bisphosphonates have been associated with ONJ (38, 2, 19, 3, 35, 26, 27, 31). A recent FDA Office of Drug Safety Post-Marketing Safety Review stated that bisphosphonate-associated ONJ “may be a class effect” (3). Recently revised product packages for oral bisphosphonate medications (e.g., alendronate [Fosamax®] and risedronate [Actonel®] now list bisphosphonate-associated ONJ as a possible adverse side effect (23, 30).
However, safety data acquired recently from two controlled studies in patients receiving an oral bisphosphonate, alendronate [Fosamax®], showed no correlation between oral bisphosphonates and ONJ. Study 1 tested the effect of alendronate on alveolar bone in 335 patients in a randomized clinical trial using a placebo, or 70 mg of alendronate weekly for two years. Study 2, a longitudinal, single-blind controlled design compared success in 50 consecutive patients. The study covered implant success and safety, also determining occurrence of ONJ. No incidence of ONJ was observed in either study. The conclusion of these two studies was that oral bisphosphonate usage was not associated with occurrence of ONJ (10). To date, only one case report of ONJ tangentially implicates endodontic treatment as a contributory factor (28). However, the conclusions tendered by the authors are not supported by the evidence presented.
Pending the availability of more definitive information, prudence should govern all patient treatment considerations for individuals on bisphosphonates. The magnitude of risk for ONJ likely varies with the bisphosphonate taken, patient factors (e.g., concurrent drugs, diseases, etc.) and dental treatment history. The existing knowledge at this time strongly suggests that patients on I.V. bisphosphonates have a higher risk for developing ONJ, while patients taking oral bisphosphonates have a significantly lower risk potential. This risk potential has been “estimated to occur in approximately 0.7 per 100,000 person-years exposure to alendronate (Fosamax®)” (ADA Council on Scientific Affairs 2006).
Endodontics: Colleagues for Excellence
�

Recommendations and Guidelines
The following is recommended when considering the endodontic implications in treating patients taking bisphosphonates:
• Recognize the risk factors of bisphosphonate-associated ONJ.
• Patients at higher risk for bisphosphonate-associated ONJ include those patients taking I.V. bisphosphonates. Preventive procedures are very important to reduce the risk of developing ONJ because treatment of ONJ is not predictable at this time. Preventive care might include caries control, conservative periodontal and restorative treatments, and, if necessary, appropriate endodontic treatment. Similar to the management of the patient with osteoradionecrosis, this might include nonsurgical endodontic treatment of teeth that otherwise would be extracted. Teeth with extensive carious lesions might be treated by nonsurgical endodontic therapy possibly followed by crown resection and restoration, similar to preparing an overdenture abutment. Surgical procedures such as tooth extractions, endodontic surgical procedures or placement of dental implants appear to impose an increased risk for developing osteonecrosis of the jaws and should be avoided if possible.
• Patients at lower risk for bisphosphonate-associated ONJ include those patients taking oral bisphosphonates. Appropriate clinical procedures might include intraoral examination, indicated dental procedures (e.g., regular checkups, caries control, indicated periodontal and restorative treatments), and patient education about the symptoms of bisphosphonate-associated osteonecrosis of the jaws and their relatively low risk of developing ONJ from surgery or soft tissue procedures.
• As usual, informed consent for endodontic procedures should involve a discussion of risks, benefits and alternative treatments with the patient.
Endodontics: Colleagues for Excellence
�
Continued on p. 6
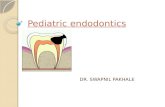
Subclass of Bisphosphonate Generic Name Trade Name Route ofAdministration Potency Ratings
Aminobisphosphonate Zolendronate(Zoledronic acid) Zometa® IV 10,000
Aminobisphosphonate Pamidronate Aredia® Oral & IV 100
Aminobisphosphonate Alendronate Fosamax® Oral 500
Aminobisphosphonate Ibandronate Boniva® Oral & IV 1,000
Aminobisphosphonate Risedronate Actonel® Oral 2,000
Non-aminobisphosphonate Tiludronate Skelid® Oral 10
Non-aminobisphosphonate Clodronate Bonefos®, Loron®
Ostac® Oral 10
Non-aminobisphosphonate Etidronate Didronel® Oral 1 (potency relative to that of etidronate)
Commonly Prescribed Bisphosphonates

• Consider bisphosphonate-associated ONJ when developing a differential diagnosis of nonodontogenic pain.
• Utilize the entire health care team, including the patient’s general dentist, oncologist and oral surgeon, when developing treatment plans for these patients.
• Cases of bisphosphonate-associated osteonecrosis of the jaws should be reported to the U.S. FDA MedWatch Online at: https://www.accessdata.fda.gov/scripts/medwatch/. Additional background information on how to report adverse effects of drugs can be found at www.fda.gov/opacom/backgrounders/problem.html.
• Be aware that the knowledge base for bisphosphonate-associated ONJ is rapidly increasing and it is likely that these recommendations may change over time. Thus, the prudent practitioner is encouraged to continue to review new publications in this area.
Endodontics: Colleagues for Excellence
�
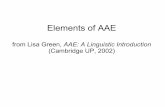
Figure 1. (A) Clinical presentation of posterior left quadrant and exposed bone #15. (B) Periapical radiograph of tooth #15 at presentation. (C) Panoramic radiograph at presentation. Sarathy et al. Bisphosphonate-Associated Osteonecrosis of the Jaws and Endodontic Treatment: Two Case Reports. Journal of Endodontics 2005: 10: 759-763. ©Copyright 2005. Reproduced with permission.
Figure 2. (A) View of upper left quadrant after sectioning of pontic. (B) Close-up view of tooth #15 and bone exposure. (C) Intraoperative view demonstrating intact sinus membrane. (D) Immediate postoperative close-up of panoramic film of operative site showing intact sinus wall. Sarathy et al. Bisphosphonate-Associated Osteonecrosis of the Jaws and Endodontic Treatment: Two Case Reports. Journal of Endodontics 2005: 10: 759-763. ©Copyright 2005. Reproduced with permission.
A B
C
A B
C D

Endodontics: Colleagues for Excellence
�
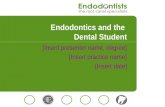
Figure 3. (A) A six-month postoperative occlusal view of surgical site. (B) A six-month postoperative facial view of surgical site. Sarathy et al. Bisphosphonate-Associated Osteonecrosis of the Jaws and Endodontic Treatment: Two Case Reports. Journal of Endodontics 2005: 10: 759-763. ©Copyright 2005. Reproduced with permission.
Figure 4. (A) Radiograph before periodontal surgery. (B, C) Pre-operative and post-endodontic radiographs. (D) Clinical photograph of case #2. Katz H. Endodontic Implications of Bisphosphonate-Associated Osteonecrosis of the Jaws: A Report of Three Cases. Journal of Endodontics 2005; 11: 831-834. ©Copyright 2005. Reproduced with permission.
Figure 5. The oral cavity showing exposed necrotic maxillary bone and a large oro-antral communication. Carter G et al. Bisphosphonates and Avascular Necrosis of the Jaw: A Possible Association. The Medical Journal of Australia 2005; 182: 413-415. ©Copyright 2005. Reproduced with permission.
Figure 6. Computed tomography showing significant bone destruction in the right maxilla (outlined). Carter G et al. Bisphosphonates and Avascular Necrosis of the Jaw: A Possible Association. The Medical Journal of Australia 2005; 182: 413-415. ©Copyright 2005. Reproduced with permission.
A B A
B C
D

Endodontics: Colleagues for Excellence
�
1. Carter, G., A. N. Goss and C. Doecke (2005). “Bisphosphonates and avascular necrosis of the jaw: a possible association.” Med J Aust 182(8): 413-5.
2. Carter, G. D. and A. N. Goss (2003). “Bisphosphonates and avascular necrosis of the jaws.” Aust Dent J 48(4): 268.
3. Chang, J. S. (2004). “ODS Postmarketing Safety Review.” Department of Health and Human Services, Public Health Service, Food and Drug Administration Retrieved Jan 4, 2006, from: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4095B2_03_04-FDA-TAB3.pdf.
4. Cheng, A., A. Mavrokokki, G. Carter, B. Stein, N. Fazzalari, D. Wislon and A. N. Goss (2005). “The dental implications of bisphosphonates and bone disease.” 2005 50 Suppl: S4-13.
5. Cheung, WK et al, Pharmacokinetics of Pamidronate Disodium in Cancer Patients Single Intravenous Infusion of 30-, 60- or 90-mg Dose over 4 or 24 Hours. Am J Ther, 1(3):228-235. (1994).
6. Dental Management of patients receiving oral bisphosphonate therapy. Expert panel recommendations. ADA Council on Scientific Affairs. JADA 2006; 137 (8) : 1144-50.
7. Durie, B. G., M. Katz and J. Crowley (2005). “Osteonecrosis of the jaw and bisphosphonates.” N Engl J Med 353(1): 99-102; discussion 99-102.
8. Ezra, A and Golub, G; Administration routes and delivery systems of bisphosphonates for the treatment of bone resorption. Adv Drug Deliv Rev. Aug;42(3):175-95. (2000).
9. Hellstein, J. W. and C. L. Marek (2004). “Bisphossy jaw, phossy jaw, and the 21st century: bisphosphonate-associated complications of the jaws.” J Oral Maxillofac Surg 62(12): 1563-5.
10. Jeffcoat, M.K., Safety of Oral Bisphosphonates: Controlled Studies on Alveolar Bone. Int J Oral Maxillofac Implants, 21: 349 – 353 (2006).
11. Katz, H. (2005). “Endodontic implications of bisphosphonate-associated osteonecrosis of the jaws: a report of three cases.” J Endod 31(11): 831-4.
References
AAE COLLEAGUES ONLINEExclusive Bonus Materials
This issue of the ENDODONTICS: Colleagues for Excellence newsletter is available online at www.aae.org with the following exclusive bonus material:
• Web site links to helpful bisphosphonate-associated ONJ resources
• Reference to 2006 textbook on bisphosphonate-associated ONJ by Robert Marx
• “Ask the Author” Discussion Board for all of your questions and comments
To access this exclusive content, click on Dental Professionals from the www.aae.org home page, and select ENDODONTICS: Colleagues for Excellence from the menu. This issue, as well as all back issues of this newsletter, are available for your ongoing reference!

Endodontics: Colleagues for Excellence
�
12. Lehenkari, P.P, et al., Further insight into mechanism of action of Clodronate: inhibition of mitochondrial ADP/ATP translocase by a nonhydrolyzable, adenine-containing metabolite. Mol. Pharmacol., 61, 1255-62 (2002).
13. Leite AF, Fiqueiredo PT, Melo NS, Acevedo AC, Cavalcanti MGP, Paula LM and Guerra ENS, Bisphosphonate-associated osteonecrosis of the jaws. Report of a case and literature review. Oral Sur, Oral Med, Oral Path; Vol 102, No 1, 14 -21. July 2006.
14. Licata, A. A. (2005). “Discovery, clinical development, and therapeutic uses of bisphosphonates.” Ann Pharmacother 39(4): 668-77.
15. Lindsay, R. and F. Cosman (2001). Osteoporosis. Harrison’s Principles of Internal Medicine. E. Braunwald, A. Facui, D. Kasperet al. New York, McGraw-Hill: 2226-37.
16. Lipton, A. (2003). “Bisphosphonate therapy in the oncology setting.” Expert Opin Emerg Drugs 8(2): 469-88.
17. Lipton, A. (2005). “New therapeutic agents for the treatment of bone diseases.” Expert Opin Biol Ther 5(6): 817-32.
18. Markiewicz, M. R., J. E. Margarone, 3rd, J. H. Campbell and A. Aguirre (2005). “Bisphosphonate-associated osteonecrosis of the jaws: a review of current knowledge.” J Am Dent Assoc 136(12): 1669-74.
19. Marx, R. E. (2003). “Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic.” J Oral Maxillofac Surg 61(9): 1115-7.
20. Marx, R. E., Y. Sawatari, M. Fortin and V. Broumand (2005). “Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment.” J Oral Maxillofac Surg 63(11): 1567-75.
21. Melo, M. D. and G. Obeid (2005). “Osteonecrosis of the jaws in patients with a history of receiving bisphosphonate therapy: strategies for prevention and early recognition.” J Am Dent Assoc 136(12): 1675-81.
22. Melo, M. D. and G. Obeid (2005). “Osteonecrosis of the maxilla in a patient with a history of bisphosphonate therapy.” J Can Dent Assoc 71(2): 111-3.
23. Merck (2005) “Merck Product Description of Fosamax.” Retrieved Jan 4, 2006, from:http://www.fosamax.com/fosamax/shared/documents/english/pi.pdf
24. Migliorati, C. A. (2003). “Bisphosphonates and oral cavity avascular bone necrosis.” J Clin Oncol 21(22): 4253-4.
25. Migliorati, C. A. (2005). “Bisphosphonate-associated oral osteonecrosis.” Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99(2): 135.
26. Migliorati, C. A., J. Casiglia, J. Epstein, P. L. Jacobsen, M. A. Siegel and S. B. Woo (2005). “Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper.” J Am Dent Assoc 136(12): 1658-68.
27. Migliorati, C. A., M. M. Schubert, D. E. Peterson and L. M. Seneda (2005). “Bisphosphonate-associated osteonecrosis of mandibular and maxillary bone: an emerging oral complication of supportive cancer therapy.” Cancer 104(1): 83-93.
28. Nase, J.B., Suzuki, J.B. (2006). Osteonecrosis of the jaw and oral bisphosphonate treatment. J Amer. Dent. Assoc. 2006:137 (8): 1115-9.
29. Novartis Pharmaceuticals Corporation. Appendix 11: Expert Panel Recommendations for the Prevention, Diagnosis and Treatment of Osteonecrosis of the Jaw. March 4, 2005, Retrieved Jan 25, 2006, from: http://www.fda.gov/ohrms/dockets/ac/05/briefing/2005-4095B2_02_12-Novartis-Zometa-App-11.pdf
30. P&G (2005) „Procter and Gamble. Actonel Product Information Sheet.” Retrieved Jan 6, 2006, from: http://www.actonel.com/global/prescribingInfo.jsp
31. Pringle, E. (2006). „Fosamax Does More Harm Than Good.” Scoop- Independent News: Opinion. April 18, 2006.
32. Purcell, P. M. and I. W. Boyd (2005). „Bisphosphonates and osteonecrosis of the jaw.” Med J Aust 182(8): 417-8.
33. Reszka, A.A. and Rodan, G.A., Mechanism of action of bisphosphonates (Review). Curr. Osteoporos. Rep., 1, 45-52 (2003).
34. Reszka, A.A. and Rodan, G.A., Nitrogen-containing bisphosphonate mechanism of action. (Review) Mini Rev. Med. Chem, 4, 711-9 (2004).
35. Rogers, M.J., New insights into the molecular mechanisms of action of bisphosphonates. (Review) Curr. Pharm. Des., 9, 2643-58 (2003).
36. Ruggiero, S. L. and B. Mehrotra (2004). „Ten years of alendronate treatment for osteoporosis in postmenopausal women.” N Engl J Med 351(2): 190-2; author reply 190-2.

Endodontics: Colleagues for Excellence
Did you enjoy this issue of ENDODONTICS? Are there topics you would like ENDODONTICS to cover in the future? We want to hear from you! Send your comments and questions to the American Association of Endodontists at the address below.
American Association of Endodontists211 E. Chicago Ave., Suite 1100Chicago, IL [email protected] • www.aae.org
The information in this newsletter is designed to aid dentists. Practitioners must use their best professional judgment, taking into account the needs of each individual patient when making diagnoses/treatment plans. The AAE neither expressly nor implicitly warrants any positive results, nor expressly nor implicitly warrants against any negative results, associated with the application of this information. If you would like more information, call your endodontic colleague or contact the AAE.
The AAE wishes to thank Dr. Marc Balson for authoring this issue of the newsletter, as well as the following article reviewers: Drs. James A. Abbott, Gerald C. Dietz Jr., David C. Hansen, Louis E. Rossman and John S. Olmsted.
Dr. Marc Balson, D.D.S., is a past president of the AAE, a Diplomate of the American Board of Endodontics and a member of the Scientific Advisory Panel for the Journal of Endodontics. He lectures nationally and internationally on bisphosphonates and various endodontic topics, and was a critical member of the AAE Special Committee to create a position statement on bisphosphonates. He maintains a private endodontic practice in Livingston, N.J.
Do you have questions for the author? Visit the Dental Professionals section of the AAE Web site at www.aae.org/dentalpro, and click on the link for this issue of ENDODONTICS: Colleagues for Excellence. Questions and comments for the author can be posted to a special discussion board dedicated to this topic.
37. Santini, D., B. Vincenzi, G. Dicuonzo, G. Avvisati, C. Massacesi, F. Battistoni, M. Gavasci, L. Rocci, M. C. Tirindelli, V. Altomare, M. Tocchini, M. Bonsignori and G. Tonini (2003). „Zoledronic acid induces significant and long-lasting modifications of circulating angiogenic factors in cancer patients.” Clin Cancer Res 9(8): 2893-7.
38. Sarathy, A. P., S. L. Bourgeois, Jr. and G. G. Goodell (2005). „Bisphosphonate-associated osteonecrosis of the jaws and endodontic treatment: two case reports.” J Endod 31(10): 759-63.
39. Starck, W. J. and B. N. Epker (1995). „Failure of osseointegrated dental implants after diphosphonate therapy for osteoporosis: a case report.” Int J Oral Maxillofac Implants 10(1): 74-8.
40. Vepsalainen,J.J, Bisphosphonate prodrugs. Current Med Chem.,9(12):1201-1208 (2002).
41. Vincenzi, B., D. Santini, G. Dicuonzo, F. Battistoni, M. Gavasci, A. La Cesa, C. Grilli, V. Virzi, S. Gasparro, L. Rocci and G. Tonini (2005). „Zoledronic acid-related angiogenesis modifications and survival in advanced breast cancer patients.” J Interferon Cytokine Res 25(3): 144-51.
42. Woo, S-B, et al., Systematic Review: Bisphosphonates and Osteonecrosis of the Jaws. Ann Int Med. 144: 753-761 (2006).
43. Wood, J., K. Bonjean, S. Ruetz, A. Bellahcene, L. Devy, J. M. Foidart, V. Castronovo and J. R. Green (2002). „Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid.” J Pharmacol Exp Ther 302(3): 1055-61.
44. Wooltorton, E. (2005). „Patients receiving intravenous bisphosphonates should avoid invasive dental procedures.” Cmaj 172(13): 1684.
45. Zaidi M, Epstein S, Friend K, Modeling of Serum C - Telopeptide Levels with Daily and Monthly Oral Ibandronate in Humans. Volume 1068 published April 2006 Ann. N.Y. Acad. Sci. 1068: 560–563 (2006). doi: 10.1196/annals. 1346.058 2006.
46. Zarychanski, R., E., Elphee, P. Walton and J. Johnston (2006). „Osteonecrosis of the jaw associated with pamidronate therapy.” Am J Hematol 81(1): 73-5.