Endocrinology of Parturition Prof. Errol R. Norwitz
18
Endocrinology of Parturition Prof. Errol R. Norwitz The screen versions of these slides have full details of copyright and acknowledgements 1 1 Errol R. Norwitz, M.D., Ph.D. Dept. of Obstetrics, Gynecology & Reprod. Sciences Yale University School of Medicine Endocrinology of Parturition . . 2 • Understand the molecular mechanisms responsible for onset of labor at term • Appreciate why these mechanisms fail leading to preterm or post-term birth • Discuss rationale behind interventions designed to prevent and/or treat abnormalities of labor Objectives 3 • The physiological process by which products of conception are passed from uterus to the outside world, and is common to all viviparous species • Labor is a clinical diagnosis characterized by: Regular painful uterine contractions Progressive cervical effacement and dilatation (or an initial examination of ≥ 80% effacement, or ≥ 2 cm dilatation in a nulliparous patient) What is labor?
Transcript of Endocrinology of Parturition Prof. Errol R. Norwitz

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 1
1
Errol R. Norwitz, M.D., Ph.D.
Dept. of Obstetrics, Gynecology & Reprod. Sciences
Yale University School of Medicine
Endocrinology of Parturition
. .
2
• Understand the molecular mechanisms
responsible for onset of labor at term
• Appreciate why these mechanisms fail leading
to preterm or post-term birth
• Discuss rationale behind interv entions designed
to prev ent and/or treat abnormalities of labor
Objectives
3
• The physiological process by which products
of conception are passed from uterus to the outside
world, and is common to all v iv iparous species
• Labor is a clinical diagnosis characterized by:
� Regular painful uterine contractions
� Progressive cervical effacement and dilatation
(or an initial examination of ≥80% effacement,
or ≥ 2 cm dilatation in a null iparous patient)
What is labor?

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 2
4
• The uterus undergoes a dramatic increase in weight and v olume
• The number of myometrial cells increases in early pregnancy, but thereafter remains stable
• Myometrial growth in the latter half of pregnancy results from an increase in cell size; This is accompanied by an increase in fibers, connectiv e tissue, blood v essels and lymphatics
• In the latter half of pregnancy, graduate thinning of the uterine wall occurs, forming the lower uterine segment
• The increase in size is accompanied by a 10-fold
increase in uterine blood flow; 80-90% of uterine blood flow goes to the placenta
• This increase parallels increase in placental size
and decrease in placental v ascular resistance
• In contrast to the uterus, which is made upof smooth muscle cells, the cerv ix is composed of fibrous
connectiv e tissue containing an extra cellular matrix
The reproductive tract changesin pregnancy
Corpus (body)
of the uterus
Cerv ix (neck)
of the uterus
5Term, labor
Term, no labor20 weeks
The cervix undergoes extensive remodeling during pregnancy
6
“The foetus in the womb”
Leonardo Da Vinci, circa 1510
What causes labor?

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 3
7
Labor timing
• In most mammalian species the fetus is in control
of the timing of labor
• Mechanical approach to labor
• Endocrine ev ents
• Paracrine/autocrine ev ents
8
Species-specific obstacles to reproduction
9
Uterus
Ov ary
SP-A from the fetal
lungs causes
activation and migration
of AF macrophages
into uterus leading to ↑↑↑↑ IL-1ββββ ,
NF-κB activation and labor
Condon J, et al., Proc. Natl. Acad. Sci. USA 2004, 101: 4978-83
Progesterone
Labor
X
PGF2αααα
X
*****

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 4
10
cholesterol
5 -pregnenolone
17αααα -hydroxypregnenolone
Fetus Mother
dehydroandrostenedione
?
↓↓↓↓ progesterone
Membrane phospholipids
estrone
17ββββ -estradiol
17-oxido-reductase
4 -androstenedione
PLA2
AA
PGE2
PGEM
15-OH PGDH
Hypothalamus
Posteriorpituitary
OT
aromatase
3ββββ -hydroxysteroid dehydrogenase
PGE2
Placenta/fetal membranes
COX-2
Hypothalamus
Anteriorpituitary
CRH
Cortisol
↑↑↑↑ PG receptors↑↑↑↑ OT receptors↑↑↑↑ gap junctions
+
+
-
17ββββ -estradiol
Adrenalgland
ACTH
+
PGF2αααα
LABOR
Uterus
PGE2
+
↓↓↓↓
+
17αααα hydroxylase/
17,20-lyase
17αααα hydroxylase/
17,20-lyase
11
• The end result is a progressiv e increase
in conj ugated estrogen in maternal plasma
during the latter part of gestation,
preceding the sharp rise
in estrogen that occurs prior to deliv ery
in response to cortisol mediated induction,
other cytochrome P450 enzyme in ruminants
and other non primate species
• It is likely that a parturition cascade exists
in humans, responsible for the remov al
of mechanisms maintaining uterine quiescence and for promoting uterine activ ity
• Giv en its teleological importance, such a cascade would likely hav e multiple
redundant loops to ensure a fail safe mechanism of securing pregnancy success
• In such a model, each element is connected to the next and many
of the elements demonstrate positiv e feed forward characteristics typical
of a cascade mechanism
• It may not be possible to identify one signaling mechanism uniquely responsible
for the initiation of labor; It may be prov en to describe
such mechanisms as being responsible for promoting labor
• Human labor is a multi factorial physiological ev ent inv olv ing an integrated set
of changes which occur gradually ov er a period of days to weeks Norwitz ER, et al., N. Engl. J. Med., 1999, 341: 660-6
12
16-OH-DHEAS from fetal adrenal
Fetus Mother
dehydroandrostenedione
Hypothalamus
Anteriorpituitary
preparesorgan
systemsfor delivery
? Fetaltrigger
Cortisol
Cortisol
Cortisone
11ββββ -HSD
progesterone
Placental OT
Membrane phospholipids
cholesterol
5 -pregnenolone
17αααα -OH-pregnenolone
estrone
17β-estradiol
estriol16-hydroxylase
17-oxido-reductase
4-androstenedione
placental
sulfatase
cortisol
PLA2
AA
(PGF2a) PGE2
(PGFM) PGEM
15-OH-PGDH
Placental vasodilatation LABOR
Hypothalamus
Posteriorpituitary
OT
aromatase
17αααα hydroxylase/
17,20-desmolase
3ββββ -HSD
Adrenalgland
Liver
Placenta/fetal membranes
COX
CRH
ACTH
DHEAS
from fetalzone ofadrenal gland
↑↑↑↑ PG receptors↑↑↑↑ OT receptors↑↑↑↑ gap junctions
PGF2αααα
SROM
fromdefinitiveadrenalcortex
PGE2
? negative feedback loop
-
+
+
+
+
+
+
+
+
Positivefeedback
loop
16-OH-DHEAS to placenta/ fetal membranes
+
placental CRH
• It is fetal 16-hydroxy-DHEAS that serves as a substrate for estrogen production in the human placenta and not progesterone as in other animal species
• This explains why there is no systemic withdrawal of progesterone levels prior to the onset of labor in humans
• Indeed, levels of progesterone measured in the maternal circulation one week prior to the onset of labor is similar to that during labor
• However, circulating progesterone levels are not an accurate reflection
of progesterone activity at the level of the uterus and there is mounting evidence to suggest that withdrawal of progesterone activity at the level of the uterus is a prerequisite for parturition in the human
• This is supported by evidence showing that the administration of a progesterone receptor antagonist at term leads to increased
uterine activity and cervical ripening
• Moreover, antenatal supplementation with progesterone from a 16 to 20 weeks gestation through 34-36 weeks has been shown to reduce the rate of preterm birth in some women at high risk
• Regardless of whether the trigger for parturition begins with the fetus or the placenta, it ends in the tissues of the maternal uterus, leading
to regular phasic uterine contraction and cervical effacement and dilatation

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 5
13
14
15
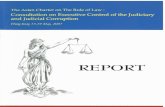
Cardinalmovements
A. Before engagement
H. Posterior shoulder delivery
F. Restitution
D. Complete rotation, early extension
B. Engagement, flexion, descent
C. Descent, rotation
E. Complete extension
G. Anterior shoulder delivery
Cardinal movements

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 6
16
Is there a genetic predisposition for PTB?
17
Indirect evidence
• Horse-donkey crossbreeding studies show
intermediate gestational length
Liggins GC, Biol. Neonate 1989, 55: 366-94
• Familial clustering of PTB
� PGDH deficiency may account for 15% of PTB
Iams J, et al., Am. J. Obstet. Gynecol. 1998, 178: 1035-40
Winkvist A, et al., Int. J. Epidemiol. 1998, 27: 248-54
Challis JR, et al., J. Perinat. Med. 1999, 27: 26-34
18
• Racial predisposition to PTB
� 2- to 4-fold ↑↑↑↑ risk in African-American women
� Disproportionate ↑↑↑↑ risk of PTB < 28 weeks
in African-American women
Indirect evidence (cont.)
Blackmore CA, et al., Ethn. Dis.1993, 3: 372-5
Carmichael SL, et al., Matern. Child Health J. 1998, 2: 67-70
Ekwo E, Moawad A., Assoc. Acad. Minor. Phys. 1998, 9: 16-21
Blackmore C, et al., Matern. Child Health J. 1999, 3: 189-93
Ventura SJ, Bachrach CA, Natl. Vital Stat. Rep. 2000, 48: 1-5

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 7
19National Center for Health Statistics; March of Dimes, 2001
• PTB in the U.S. is highest for African-Americans
>> Nativ e Americans > Hispanics > Whites, Asians
20
• High rate of recurrent PTB
� If the first delivery was at 20-31 weeks,
the risk of a similar recurrent PTB was 13.4%
(African-American) and 8.2% (Caucasian)
� If the first delivery was at 32-36 weeks,
the risk of a similar recurrent PTB was 3.8%
(African-American) and 1.9% (Caucasian)
Indirect evidence (cont.)
Turnbull AC, Obstetrics, 1989, pp. 189-204
Iams J, et al., Am. J. Obstet. Gynecol. 1998, 178: 1035-40
Ekwo E, et al., Assoc. Acad. Minor. Phys. 1998, 9: 16-21
21
• Twin studies of pregnancy outcomes suggest
the heritability of PTB to be around 17-36%
Indirect evidence (cont.)
Treloar SA, et al., Tw in Res. 2000, 3: 80-2
Claussen B, et al., Br. J. Obstet. Gynaecol. 2000, 107: 375-381
Crider KS, et al., Genet. Med. 2005, 7(9): 593-604
Svensson AS, et al., Am. J. Obstet. Gynecol. 2006, 194: 475-9

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 8
22
Unlikely to be an example of simple Mendelian genetics
23
Complex genetic model
• Primarily a single gene disorder
� Variable penetrance of the gene
� Genetic background (gene-gene interactions)
� Gene-environment interactions
• Multiple genes inv olv ed
• Epigenetic factors
� DNA methylation/histone acetylation
� siRNA
24
Gene-environment interaction and PTB
• A disproportionate ↑↑↑↑ in IL-1ββββ ov er IL-1ra
in v aginal secretions of pregnant women
with altered v aginal microflora is assoc with PTB
Genç MR, et al., Am. J. Obstet. Gynecol. 2004, 190: 1191- 7
• Maternal carriers of SNP in intron 2 of IL-1ra
is assoc. with ↓↓↓↓ pro-inflammatory IL-1ββββ response
to abnormal v aginal flora and ↓↓↓↓ rate of spont. PTB
(6% vs. 18%, P = 0.02)
Genç MR, et al., Am. J. Obstet. Gynecol. 2004, 191: 1324-30

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 9
25
• Also ↓↓↓↓ spontaneous PTB rate with maternal carriage
of 896 A>G SNP in TLR4 gene
� Maternal carriers have ↑↑↑↑ in vaginal pH, 10-fold ↑↑↑↑
in Gardnerella vaginalis and gram negative rods,
and an alteration in vaginal IL-1ββββ and IL-1ra levels
Gene-environment interaction and PTB (cont.)
Genç MR, et al., Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116: 152-6
26
• Maternal carriers of -308 G>A SNP in TNFαααα promoter
are assoc. with ↑↑↑↑ risk of PTB (OR, 2.7; 95% CI,
1.7-4.5), which was further ↑↑↑↑ in presence of BV
(OR, 6.1; 95% CI, 1.9-21.0)
Genç MR, et al., Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116: 152-6
Macones G, et al., Am. J. Obstet. Gynecol. 2004, 190: 1504-8
• Kand in African-American women (OR = 17)
Nguyen DP, et al., Obstet. Gynecol. 2004, 104: 293-300
Gene-environment interaction and PTB (cont.)
27
When labor goes right
Photo by Diane Arbus
When labor goes wrong

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 10
28
Preterm birth
29
Why all the fuss?
• Preterm birth complicates 8-12% of all deliv eries
• Leading cause of perinatal mortality and morbidity
• There has been no decrease in the incidence
of preterm birth ov er the past 30 years
30March of Dimes Perinatal Data Center, 2006; www.marchofdimes.com
0
2
4
6
8
10
12
14
1990 1992 1994 1996 1998 2000 2002
Percent of all births
2004
Preterm birth < 28 weeks’ gestation < 34 weeks < 37 weeks
10.6%10.8%10.7% 11.0%11.0%11.0%11.0%11.4%11.6%11.8%11.6%11.9%12.1%
12.5%12.9%
Preterm births, 1990-2004

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 11
31
Preterm births
for maternal
or fetal indication
- Diabetes
- IUGR
- Preeclamp sia
- Placenta previa
- Placental abruption
Tucker JM, et al., Obstet. Gynecol. 1991, 77: 343-7
20%
Preterm birth is a syndrome
• Preterm PROM
• Intra-amniotic
infection
• Idiopathic preterm labor
30%
30%
20%
Spontaneous Iatrogenic
32
Intrauterine infection/
inflammation
Preterm labor
Maternal
and/or
fetal stress
Excessiv e uterine
stretch
Hemorrhage
33
• Prior preterm birth
• African-American race
• Age < 18 or > 40 years
• Poor nutrition
• Anemia
• Low pre-pregnancy weight
• Low socioeconomic status
• Absent prenatal care
• Bacteriuria or UTI
• Genital/gingival infection
• Cigarette smoking
• Illicit drug use
• Cervical injury or anomaly
• Uterine anomaly or fibroids
• Excessive uterine activity
• Premature cervical dilatation
• Overdistended uterus (twins)
• ? Vaginal bleeding
• ?? Strenuous work
• ?? High personal stress
Risk factors

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 12
34
+
+
35Iams JD, et al., N. Engl. J. Med. 1996, 334: 567-72
(n=
2915)
50%le (35 mm)
10%le (25 mm)
90%le (45 mm)
36
Markers
• Activin/Inhibin
• Follistatin
• Ferritin
• CRP
• Interleukin-6
• CRH
• Progesterone
• Estrogens
• Metalloproteinases
• Collagenase
• Relaxin
• Fibronectin
Source
• Blood
• Serum
• Saliva
• Amniotic fluid
• Vagina
• Cervix
Biochemical/endocrine markers

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 13
37
Fetal fibronectin (fFN)
Amnion
Chorion
Fetalfibronectin
Decidua
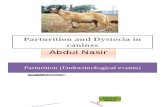
38Goldenberg RL, et al., Am. J. Public Health 1998, 88: 233-8
1 2 3 4 5 6 7 8 9 1011 12 131415 1617 1819 20 21
Positive fFN
Cervical length < 25 mm
Previous SPTB
BMI < 19.8
Vaginal bleeding
Bacterial vaginosis
Pelvic infection
Black race
RR of spont PTB < 32 weeks
Ris
k f
acto
rs
Contractions
Screening for preterm birth
39
Effective strategies for prevention of preterm birth
• Prev ention of multifetal pregnancies
• Cerv ical cerclage, if indicated
• Early diagnosis and treatment
of genitourinary infections and STDs
• Stop smoking and substance abuse
• Progesterone supplementation (?)

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 14
40
Preventive strategies without proven benefit
• Intensiv e prenatal care
• Bed rest, flexible workforce policies
• Screening asymptomatic women
for genital tract/gingiv al infections
• Broad-spectrum antibiotics
• Uterine tocolytic therapy (?)
41
42
Post-term pregnancy

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 15
43
2
4
6
8
%
of
all
deli
veri
es
EDC
Term
Post-term
(prolonged)
Gestational age (weeks)
10% (range, 3-14%)
4%(range, 2 7%)
What is the definitionof post-term pregnancy?
0
38 40 42 44
-
44
Accurate dating
• Menstrual history is often inaccurate
� Especially if irregular cycles, on hormonal
contraception, or intermenstrual bleeding
• Routine early ultrasound will ↓↓↓↓ incidence
of post-term pregnancy from 10% to 1.5-5%
� Not currently recommended in the U.S.
Warsof SL, et al., Clin. Obstet. Gynecol. 1983, 10: 445-7
Bennett K, et al., Am. J. Obstet. Gynecol. 2004, 190: 1077-81
45
Can we identify parturients at risk
of post-term pregnancy?
• Risk factors for post-term pregnancy ...
� Primiparity
� Prior post-term pregnancy
� Fetal anencephaly (without polyhydramnios)
� Congenital adrenal hypoplasia (CAH)
� Placental sulfatase deficiency (rare)
� Male fetus
• The majority of post-term pregnancies
hav e no known cause

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 16
46
• Perinatal death
(stillbirth)
• Fetal macrosomia
• Meconium
• “Fetal distress”
• Uteroplacental
insufficiency
4- fold ↑↑↑↑ at 43 wks and 5
to 7- fold ↑↑↑↑ at 44 wks (vs. 40 wks)
2.5- 10% (vs. 0.8-1% at 40 wks)
30- 38% (vs. 17% at 40 wks)
8% (vs. 5% at term)
20- 40%
Risks to the fetus
Complication Incidence
47
“Antepartum fetal deaths
perinatal deathsmoreaccount for
than do complications
of prematurity
or sudden infant death syndrome (SIDS)”
Cotzias CS, et al., Br. Med. J. 1999, 319: 287-8
48
Hilder L, et al., Br. J. Obstet. Gynaecol. 1998, 105: 169-73
Rand L, et al., Obstet. Gynecol. 2000, 96: 779-83
Smith GCS, Am. J. Obstet. Gynecol. 2001, 184: 489-96
Stillbirth
Infant mortality
Stillbirth
Infant mortality
PNMR per 1,000 liv e births PNMR per 1,000 ongoing pregnancies

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 17
49
Also increased risk of perinatal morbidity
• Post-term pregnancy is a risk factor for:
�Apgar score < 4 at 5 min (OR 3.6; 95% CI, 1.5-8.7)
�Neonatal convulsions(OR 3.4; 95% CI, 1.5-7.6)
�Meconium aspiration (OR 3.0; 95% CI, 2.6-3.7)
Clausson B, et al., Obstet. Gynecol. 1999, 94: 758-62
• Also an independent risk factor for newborn
encephalopathy (OR 13.2; 95% CI, 5.03-34.83)
Badawi N, et al., Br. Med. J. 1998, 317: 1549-53
50
• The timing of labor and birth is a critical
determinant of perinatal outcome
• The factors responsible for the onset of labor
at term remain poorly understood
• A better understanding of the factors responsible
for labor will improv e our ability to manage
abnormalities of labor
Conclusions
51
“Children are one third of our population and all of our future”
Select Panel for the Promotion of Child Health
U.S. Dept of Health and Human Services
W ashington, DC, 1981

Endocrinology of Parturition
Prof. Errol R. Norwitz
The screen versions of these slides have full details of copyright and acknowledgements 18
52