Endocrinology EMR: Why Endocrinologists are switching to RevenueXL's PrognoCIS EHR

Endocrinologists Role In Infertility Management
Sidika E. Karakas, MD
Professor and ChiefDivision of Endocrinology, Diabetes and Metabolism
University of California, Davis

Thoma et al. Fertility and Sterility 99:1324, 2013
ALL WOMEN(n = 270)
NULLIPAROUS WOMEN
(n =139)
Infertility: Inability to become pregnant after 12 months of trying
Prevalence: 7.4% among married women in the United States
What is typical?
• Average age of menarche in USA is 12 y
• >90% females >15 y have >10 menses/y
Amenorrhea
• Primary—Absence of menses by age 16 y
• Secondary—Absence of menses for >6 mo
Oligomenorrhea
• Period intervals >35 days
• 4 to 9 periods/ year

What is our job as endocrinologists?
I. Ruling out non-endocrine infertility
II. Correct diagnosis of endocrine causes
III. Optimizing hormonal and metabolic milieu
for ovulation

Ruling out non-endocrine infertility
Identifying ovulatory women
by measuring progesterone during the 3rd week of
menstrual cycle (typically > 4)

Infertile Couple
Semen Analysis
• Volume: 2 – 5 ml
• Sperm count: 40 – 300 million
• Motility & velocity: > 50% active
• Morphology: > 30% normal
• Liquefaction: liquid gel
liquid in 20 min (otherwise seminal vesicle pathology)
• Fructose: None—Obstruction of
ejaculatory duct; absence of vas deference or seminal vesicles
• Culture

Correct Diagnosis of Endocrine Causes
PCOS-Centric View
PCOS
90%
Hypothalamic Weight loss; systemic illnessKallmann’s SyndromeHypogonadotropic
hypogonadism
PituitaryHyperprolactinemiaHypopituitarism
Ovary 5%Primary ovarian failure
5%
PCOS is responsible for 90% of anovulatory infertility

What is PCOS?
Roe, Rev Obstet Gynecol. 2011
PCOS Phenotypes
A) Hyperandrogenism + Anovulation + PCO
B) Hyperandrogenism + Anovulation
C) Hyperandrogenism + PCO
D) Anovulation + PCO
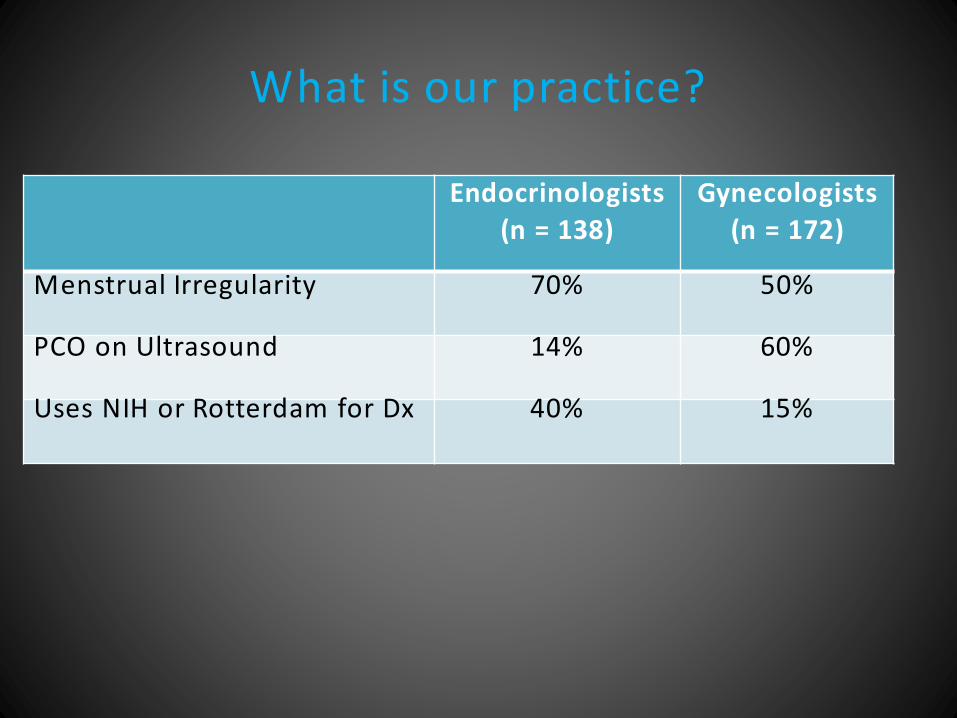
What is our practice?
Endocrinologists
(n = 138)
Gynecologists
(n = 172)
Menstrual Irregularity 70% 50%
PCO on Ultrasound 14% 60%
Uses NIH or Rotterdam for Dx 40% 15%
My screening tests for PCOS
AMH Testosterone panel (total-,
bioavailable- and free- testosterone plus SHBG)
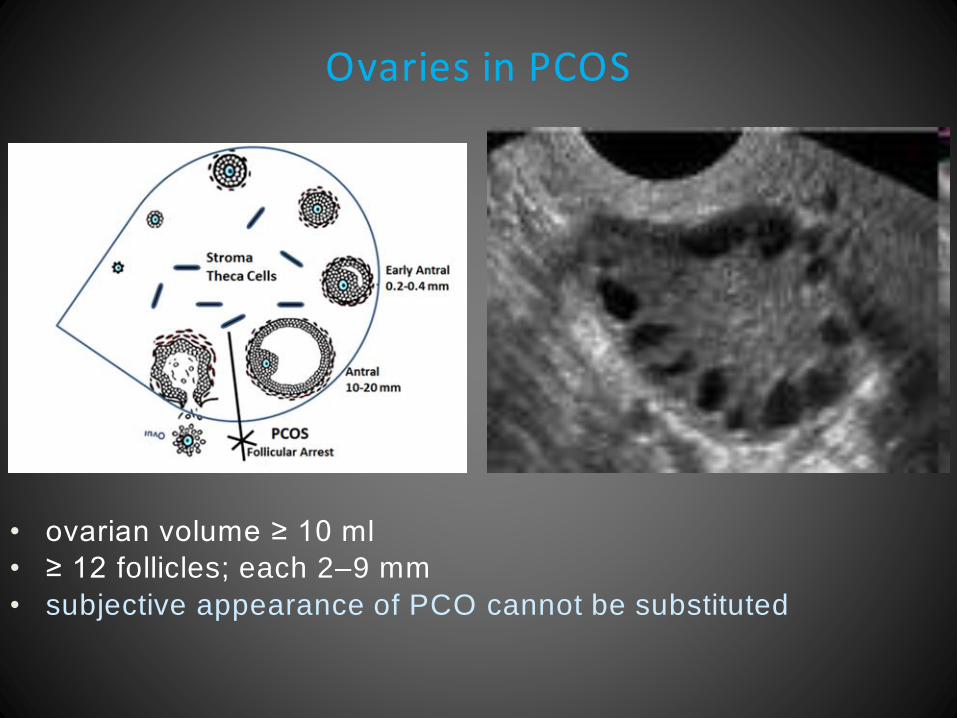
Ovaries in PCOS
• ovarian volume ≥ 10 ml
• ≥ 12 follicles; each 2–9 mm
• subjective appearance of PCO cannot be substituted
Anti-Mullerian Hormone (AMH)
• Glycoprotein
• Produced by granulosa cells of primary, pre-
antral and early antral follicles (2-7 mm)
• NOT by larger or atretic follicles
• Indicator of ovarian reserve

AMH
– Age 10-21: Average = 3 ng/mL
– > 5 ng/ml ---PCOS
– < 0.8 ng/ml ---Menopause
– > 1.3 ng/ml---Successful IVF
– 30% decrease during oral contraceptive therapy
AMH IS ELIMINATING THE NEED FOR TRANSVAGINAL US

• Free testosterone 2%
• Albumin bound 50%
• SHBG bound 44%
• Bioavailable testosterone---Testosterone not bound by SHBG
Why measure free or bioavailable
testosterone?

Total testosterone does not reflect
androgen exposure
Age 10-21: Average = 3 ng/mL>5 ng/ml ---PCOS
< 0.8 ng/ml ---Menopause
> 1.3 ng/ml---Successful IVF
Age 10-21: Average = 3 ng/mL>5 ng/ml ---PCOS
< 0.8 ng/ml ---Menopause
> 1.3 ng/ml---Successful IVF

Effect of Oral Contraceptive on Testosterone Bioavailability
Before After
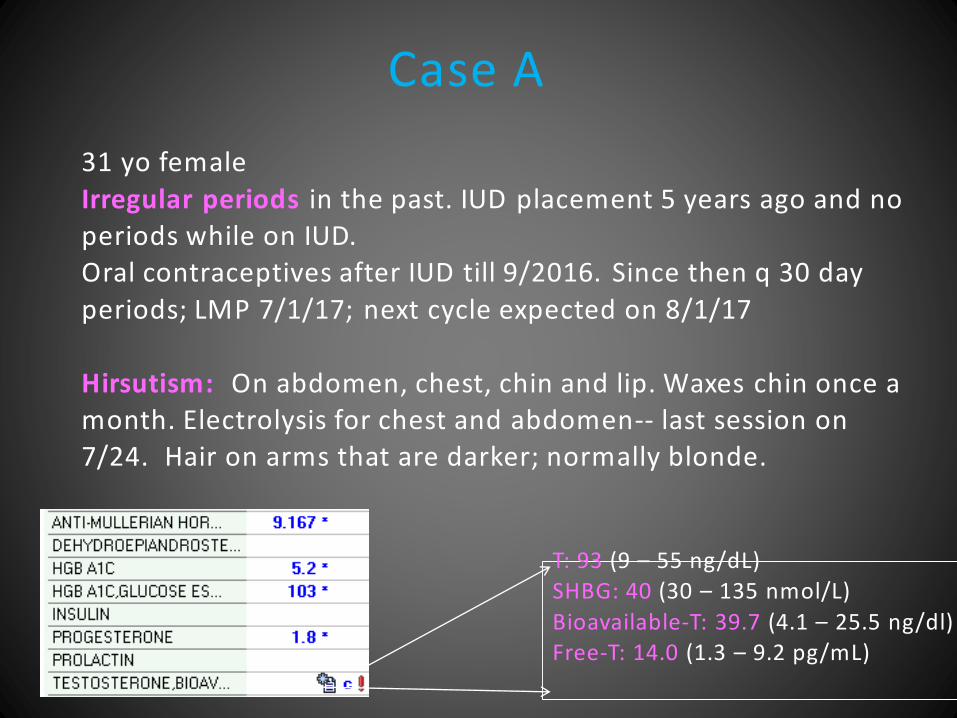
Case A
T: 93 (9 – 55 ng/dL)
SHBG: 40 (30 – 135 nmol/L)
Bioavailable-T: 39.7 (4.1 – 25.5 ng/dl)
Free-T: 14.0 (1.3 – 9.2 pg/mL)
31 yo female
Irregular periods in the past. IUD placement 5 years ago and no periods while on IUD. Oral contraceptives after IUD till 9/2016. Since then q 30 day
periods; LMP 7/1/17; next cycle expected on 8/1/17
Hirsutism: On abdomen, chest, chin and lip. Waxes chin once a month. Electrolysis for chest and abdomen-- last session on 7/24. Hair on arms that are darker; normally blonde.

Case B
T: 25 (9 – 55 ng/dL)
SHBG: 80 (30 – 135 nmol/L)
Bioavailable-T: 6.9 (4.1 – 25.5 ng/dl)
Free-T: 2.3 (1.3 – 9.2 pg/mL)
31 yo female
Heavy periods was referred for PCOS. No hirsutism. After seeing her labs, I questioned how was her diagnosis made; her
response was: The diagnosis was based on my symptoms and history. Heavy
periods run in my family. My endocrinologist didn't do much except give the meds based on the “PCOS pathway treatment plan .”

Necessary and Sufficient
– AMH
– Bioavailable testosterone
– DHEAS—to r/o adrenal androgen excess
– 17OHP—to r/o CAH (21OH deficiency)
– Prolactin—to r/o prolactinoma
– FSH—to r/o premature ovarian failure
– Cortisol –Only if there are supraclavicular fat pads
CASE 1
• 19 yo WF
• CC: Last period 17 mo ago
• Menarche 13 yo
• Irregular to start with: approximately q 3 mo
• No oral contraceptives
• No pregnancies
• No hirsutism
• No breast discharge

CASE 1 continued
• Gained 18 kg in the last 2 y
• Diets: Zone diet; lost 11 kg 3 y ago
• Hearing loss in left ear, bone abnormalities
• Ht: 1.72 m; Wt: 108.8 kg BMI: 36.5
• No hirsutism
• No acanthosis or skin tags
• No dorsoclavicular fat pads, no webbing
• Normal breasts; no discharge

AMH: < 0.003
Testosterone: 23 (N < 55)

AMH: < 0.003
Testosterone: 23 (N < 55)
FSH: 50.2
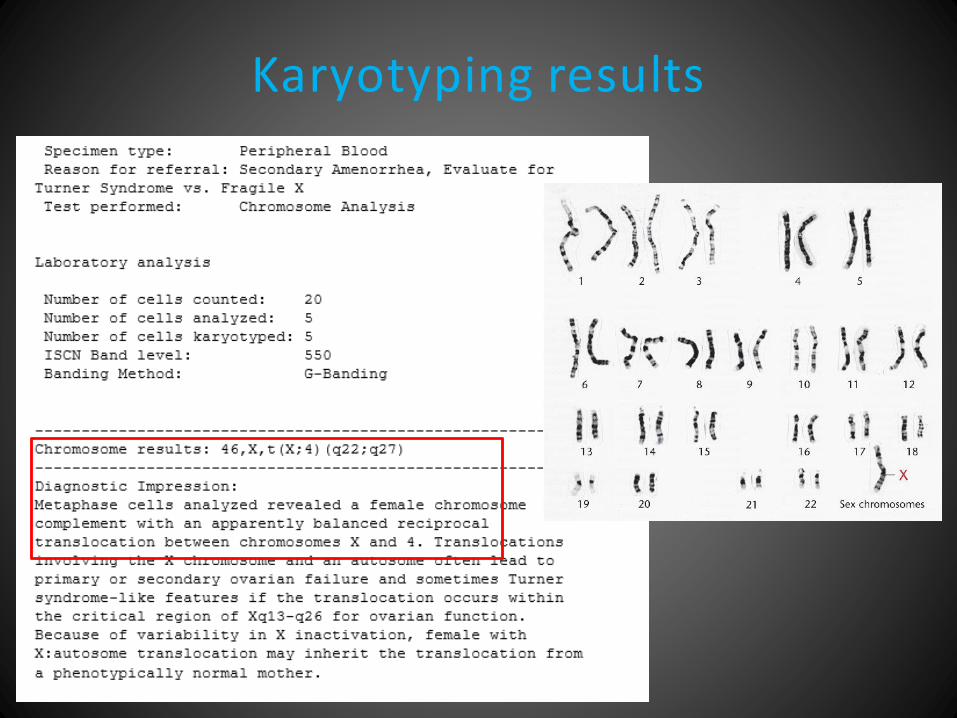
Karyotyping results
Fragile X• X-linked disorder
• Decreased or absent fragile X mental retardation
protein (FMRP) due to a loss-of-function mutation in the fragile X mental retardation 1 (FMR1) gene
• Caused by expansion of a trinucleotide (cytosine-guanine-guanine, CGG) repeat at the 5' untranslated
region
• Expansion of >200 repeats: Full mutation
• Expansion between 50 -200 repeats: Pre-mutation
• Pre-mutation is associated with premature ovarian failure

CASE 2
18 yo female
• CC: Only 1 period in entire life, during 7 th grade
• Normal breast growth, no discharge
• Shorter than siblings (4’11’’)
• Normal mental development
• Premature birth
• Cyst in the neck with permanent swelling, no
hypothyroidism

Case 2 continued
• Ht: 4’8’’; Wt: 134 lb; BMI: 34.8
• Neck asymmetrical, swollen on the R
• No facial hair
• Acanthosis + in the axilla
• Breast exam: Well developed; exam was not
done (mother & sister are in the room)
• White striae in the abdomen

AMH: 2.1
Testosterone: 11 (N < 55)
– Bioavailable-T: 5.5 (<20.6)
– Free-T: 1.8 (<7.4)

Endocrine Testing
• HCG : Negative
• FSH: 6.5
• Prolactin: 194 (<19.5)
• TSH: 1.22
• Growth hormone: 0.12
(0.05-8)
• IGF-1: 277 (165-585)

What is our job as endocrinologists?
• Optimizing hormonal and metabolic milieu for ovulation

PCOS—Two Sided Coin
Hormonal
Ovarian DysfunctionMetabolic
Insulin Resistance

Insulin Resistance in PCOS
PCOS women maintain normal glucose tolerance at the expense of hyperinsulinemia
By age 40 y, 1 out of 5 PCOS women develops T2 diabetes

Physical Clues for Insulin Resistance
Acanthosis and Skin Tags

Other Clues for Insulin Resistance
in PCOS Women with Normal Glucose Tolerance
8.1
1.4
27.4
6.9
5558
1.93.7 2.9
31.6
13.1
49
38
5.91.9
5.6
39.9
24.4
40
25
10.6
0
10
20
30
40
50
60
70
ISIMatsuda HOMA BMI Fasting
Insulin
HDL-C SHBG hs-CRP
S. Karakas et a. Diabetes Care 2010

HgBA1 > 5.7% is a Very Useful Marker in PCOS
HgBA1 < 5.7
(n = 25)
HgBA1 >5.7
(n = 23)
P value
Age (years) 31.1 ± 1.1 35.1 ± 1.1 0.039
Fasting glucose (mg/dl) 91.5 ± 0.9 99.6 ± 2.3 0.028
Adiponectin (ng/ml) 12.4 ± 0.9 8.8 ± 0.7 0.023
FS-IVGTT
SI 4.2 ± 0.6 2.0 ± 0.2 0.020
DI 1901 ± 217 1014 ± 82 0.011
CVD risk factors
Triglyceride (mg/dl) 92.6 ± 4.4 125.3 ± 9.5 0.018
hs-CRP (ng/ml)
FABP4 (ng/ml)
2.1 ± 0.1
34.8 ± 2.9
4.76 ± 0.5
58.5 ± 4.9
0.003
0.021
R. Mortada et al. Endo Prac 2013
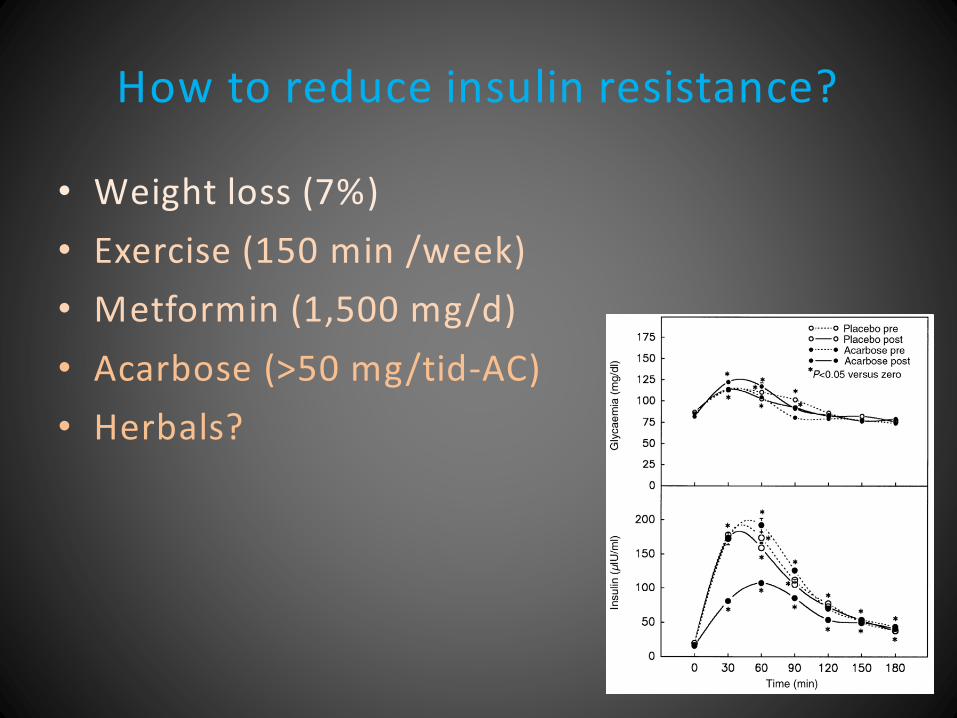
How to reduce insulin resistance?
• Weight loss (7%)
• Exercise (150 min /week)
• Metformin (1,500 mg/d)
• Acarbose (>50 mg/tid-AC)
• Herbals?

Effects of Weight Loss on Fertility
• 33 PCOS patients
• 25 lost 5% weight
• 11 of these lost >10%
• 15 women ovulated
• 10 became pregnant
P.G. Crosignani et al. Human Repro 18:1928, 2003.

Effect of Life Style Changes on AMH and Ovarian Function
DIET EXERCISE DIET plus EXERCISE
BMI 35.4±4.9 32.9±5.5*** 34.8±5.2 34.1±5.7* 38.1±7.0 36.9±8.0***
T (ng/mL) 0.51±0.22 0.40±0.19* 0.44±0.18 0.44±0.21 0.50±0.21 0.45±0.19
FT (pg/mL) 16.3±7.4 11.0±5.4** 13.0±6.1 12.0±6.6 17.2±9.0 12.6±6.8
AMH (ng/mL) 10.4±6.2 7.7±5.3** 9.2±5.5 9.2±5.9 9.9±6.0 8.5±5.6
Follicle number 12.4±3.9 9.4±2.4* 13.2±4.6 10.5±3.2** 12.8±4.7 10.1±3.4*
Ovulation 0 5/14(36%) 0 6/17 (35%) 0 4/12 (33%)
Nybacka et al. Fertil Steril 100: 1096, 2013
Duration: 4 months
Diet: -600 kcal restriction
Exercise: 45- 60 min; 2-3 times/wk

My Practice
METFORMIN (6-9 months)
Oral Contraceptive 3-4 months
Trying for pregnancy &
Progesterone monitoring

Clomiphene, Metformin or Both for Infertility in PCOS.
Legro et al. NEJM, 2007
Baseline Characteristics of 626 PCOS Women
Age (Years)28.1± 4
BMI35.3±8.6
Length of trying (mo)40.4±35.8
No Treatment262 (42%)
Previous Treatment374 (58%)
Treatment Outcomes
Metformin
(208)
Clomiphene
(209)
Combination
(209)
Ovulation 296/1019 (29%) 462/942 (49%) 582/964 (60%)
Conception 25/208 (12%) 62/209 (30%) 80/209 (38%)
Live Birth 15/208 (7%) 47/209 (23%) 56/209 (27%)
Pregnancy Loss 10/25 (40%) 16/62 (26%) 24/80 (30%)
Patient population
Obese Trying for a long time
Previously treated

European and Australian Experience
• In PCOS women with BMI ≤ 30 kg/m2 there is no difference between metformin vs. Clomiphene
Palomba S, Pasquali R, Orio F Jr, Nestler JE.
Clomiphene citrate, metformin or both as first-step approach in treating
anovulatory infertility in patients with polycystic ovary syndrome (PCOS):
A systematic review of head-to-head randomized controlled studies and meta-
analysis.
Clin Endocrinol (Oxf). 2009 Feb;70(2):311-21

Clomiphene vs. Aromatase Inhibitors

Ovulation Induction Protocols