End Stage Heart Failure - CRRTonline
23
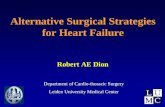
Stable Heart Failure Patients End Stage Heart Failure Advanced Therapy Patients
Transcript of End Stage Heart Failure - CRRTonline

Stable Heart Failure Patients
End Stage Heart Failure
Advanced Therapy Patients

22 24 26 28
US Average
UCSD
Readmission Rate 30 D
Decompensated HF 2011

The Three Elements of
Decompensated Heart Failure
Increased preload
Volume overload
Increased Afterload
Vasoconstriction
Myocardial dysfunction Decreased cardiac output
Vasodilators
Nitroglycerin, Nipride, Natricor
Pathophysiology Treatment
Diuretics
Lasix, Bumex
Inotropes Dobutamine,
Dopamine, Milrinone



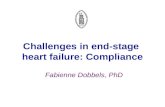
7% 6%
13%
26%
27%
16%
3% 2%
0
5
10
15
20
25
30
Enro
lled D
ischarg
es
(%)
(<-20) (–20 to –15) (-15 to –10) (–10 to –5) (–5 to 0) (0 to 5) (5 to 10) (>10)
Change in Weight (lbs)
Nearly 50% of ADHF patients
discharged with weight gain or
losing less than 5 lbs
Evidence of Incomplete Relief From Congestion
Change in Weight During Hospitalization January 2001 to April 2006 (n=96,094)
Adhere National Benchmark Report Data, January 2001 to April 2006.
Note: n represents the number of patients who have both baseline and discharge weight, and the percentage is calculated based on the total
patients in the corresponding population. Patients without baseline or discharge weight are omitted from the histogram calculations.
Outcomes with Standard Care

Diuretic Optimization Strategies
Evaluation in Acute Heart Failure
(DOSE) G. Michael Felker, MD, MHS, FACC
Christopher M. O’Connor, MD, FACC
on behalf of the
NHLBI Heart Failure Clinical Research Network

Aims
To evaluate the safety and efficacy of various initial
strategies of loop diuretic administration in patients with
ADHF
Route of administration:
Continuous infusion vs. Q12 hours bolus
Dosing
Low intensification (1 x oral dose) vs. high intensification (2.5 x
oral dose)

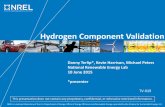
Death, Rehospitalization, or ED
Visit
HR for Continuous vs. Q12 = 1.19
95% CI 0.86, 1.66, p = 0.30 HR for High vs. Low = 0.83
95% CI 0.60, 1.16, p = 0.28
0
0.1
0.2
0.3
0.4
0.5
0.6
0 10 20 30 40 50 60
Days
Pro
po
rtio
n w
ith
De
ath
, R
eh
os
p,
or
ED
vis
it
High Low
0
0.1
0.2
0.3
0.4
0.5
0.6
0 10 20 30 40 50 60
Days
Pro
po
rtio
n w
ith
Death
, R
eh
osp
, o
r E
D V
isit
Continuous Q12

Conclusions
There was no statistically significant difference in global
symptom relief or change in renal function at 72 hours for
either:
Intermittent bolus vs. continuous infusion
Low intensification vs. high intensification

Aquaphoresis
for Diuretic
Resistance


My Own Aquapheresis
Statistics Treatment summary Oct 27, 2010 through May 11, 2011
Number of treatments (circuits): 19
Average treatment time: 27.73 hours
Average fluid removed/treatment: 4.12 Liters or
9.07 Lbs
Most common fluid removal rate(s): 46% (10 - 100 ml/hr)
38% (110 - 200 ml/hr)
Most common blood flow rate(s): 63% (25-30 ml/min)
28% (35-40 ml/min)
Source: Data downloaded from your Aquadex device(s)

Do Not Sit on the Stage D
Patient

Prognostication in Heart Failure: The
Heart Failure Trajectory

Supply and Demand
Transplant
Limited supply
High Demand
LVAD
Unlimited supply
Demand limited
strict selection criteria
Costs
Patient Preference
TX LVAD
Stage D CHF

HeartMate II LVAS Key Design Features
Relatively Simple Design
Valveless
Only one moving part, the rotor
Blood immersed bearings designed
for minimization of blood damage
All motor drive and control
electronics are outside of the
implanted blood pump
Speed range: 6,000 to 15,000
rpm
Flow range: 3 – 10 L/min

TAH Attributes
No right heart failure
No arrythmias, no antiarrythmic drugs
No inotropes
Low CVP, High Output, Control of the Circulation
No afterload dependence
Rescues patients in acutely decompensating cardiogenic
shock (crash and burn patients)


VAD Development: 2nd Generation
Updated Heartmate II outcomes
Medical Therapy
Heart Transplant
Outcomes with Heartmate II already competing with
gold standard treatment

Mechanical heart pump a temporary fix for the broken heart of a Portland teenager
Hentz fought the idea for days, snapping at family and nurses and shouting, "I hate you!" at one of her cardiologists, Dr. Eric Adler.

Is a VAD a treatment for
Cardiorenal Syndrome?
Unanswered question
Challenges
Need uniform diagnostic criteria
Most patients have concomitant medical-
renal disease
If patient gets better, than it was cardiorenal, if they
don’t , they either have bad right heart failure or some
other diagnosis.