Patient-centric care & telehealth - Sigi Marmorstein, Telehealth Consulting - TFSS
Upload
eiu-perspectivesCategory
view
394download
1
A report by The Economist Intelligence Unit
Enabling telehealth: Lessons for the Gulf
Commissioned by
1 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Contents
About this report 2
Executive summary 3
A note on definitions 4
Chapter 1 – New policies for the ‘connected care’ era 5
Case study: Mayo Clinic 6
Chapter 2 – Communications infrastructure 8
Chapter 3 - Skilling up 10
Map graphic: “Telehealth associations and user groups, global” 11
Chapter 4 – Lessons for the Gulf 12

2 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Enabling telehealth: Lessons for the Gulf is an Economist Intelligence Unit report about the enabling environment for telehealth, with a focus on policy, infrastructure, skills and institutional user groups. The findings are based on desk research and interviews with experts, conducted by the Economist Intelligence Unit. It draws from case study experience in North America, Europe, Australia and New Zealand, and identifies principles and practices relevant to the Gulf Cooperation Council region. This research was commissioned by Philips. The author was Frieda Klotz. The editor was Adam Green.
The Economist Intelligence Unit would like to thank the following experts for insights shared during the research of this report:
l Mario Gutierrez, executive director of the Center for Connected Health Policy
l Steve Ommen, a cardiologist and associate dean of the Mayo Clinic’s Center for Connected Care
l Stephan Schug, chief medical officer of the European Health Telematics Association
l Verina Waights, a senior lecturer in professional healthcare education at the Open University
l Kawaldip Sehmi, CEO, International Alliance of Patients’ Organisations
The Economist Intelligence Unit bears sole responsibility for the content of this report. The findings and views expressed in the report do not necessarily reflect the views of the sponsor.
About this report

3 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
The technologies of telehealth are advancing quickly as part of the ‘connected care’ revolution. Patients and health providers are ever more closely linked through real-time electronic tools. From digital imaging to allow remote viewing of CT scans, through to patient diagnosis, videoconferencing and monitoring, these tools could touch all aspects of the patient-provider relationship.
Much of the promise of telehealth is predicated on its ‘access’ benefits: the improved access of the patient to medical expertise regardless of location, and improved access of health providers to their patients, for the purpose of diagnosis, consultation and monitoring. Yet access to telehealth depends not only on telehealth technology. Policy frameworks must be modernised, communications infrastructures such as broadband and mobile network coverage must be improved, and skillsets – both of clinicians and patients – need to be strengthened. This briefing paper outlines three factors shaping the telehealth access environment: government readiness (e.g. legal and regulatory clarity and harmonisation, especially across states and borders), communications infrastructure, and skills.
Executive summary
Key findings
l Ensuring access to telehealth depends not just on the technologies, but on the broader enabling environment, especially policy harmonisation, communications infrastructure, and skills. The telehealth innovation frontier is advancing rapidly. But to fully realise its potential – and strengthen access to healthcare services – telehealth requires the right support. Health policy needs to adapt to the technological frontier, communications infrastructure needs to reach vulnerable citizens, and skills programs must be in place to maximise the utility of the new technologies.
l Governments should consider more efficient licensing if telehealth is to enable patients to access medical expertise outside of their state, province or country. Where governance standards converge, regulatory bodies should trust more in the licensing decisions of neighbouring authorities to create ‘portable’ medical licenses that allow health providers to interact with patients in other regions.
l Telehealth provision must go hand-in-hand with Internet infrastructure rollout, since vulnerable populations are the lowest users of the Internet. The digital divide stubbornly

4 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
persists even in more advanced economies. Some regions and populations, such as the disabled and elderly, cannot be assumed to be Internet users; to benefit from telehealth they need communications infrastructure and training.
l Focus on systems integration: Telehealth can enable a wider cast of actors to collaborate in patient care, from doctors to social workers and nutritionists. However, there is a challenge in balancing more users on the one hand, with the need to build usable systems with the requisite security and privacy. Careful planning is also needed to ensure new telehealth systems work
seamlessly with those already in place, to avoid medical specialties having ‘one-off’ solutions.
l Health providers may need support in working with new technologies. Medical providers vary considerably in their support for, and adoption of, telehealth. Hospitals and providers may wish to develop training programs to show relevance and usage, as well as to impart etiquette and best practice codes such as upholding the same standards of patient-doctor interaction that holds in face-to-face consultations.
Telehealth has a range of definitions depending on jurisdiction; a linguistic divergence that reflects the patchwork nature of the policies and structures that govern it. At its most basic level, it refers to the delivery of health services and information through telecommunications technologies, most often mobile and internet-based. For the World Health Organization (WHO) telehealth involves ‘computer assisted communications’ to ‘support management, surveillance and access to medical knowledge,’ as opposed to telemedicine, which is more narrowly defined by the WHO as ‘the use of telecommunications to diagnose and treat disease.’ The Australian government also distinguishes between telehealth and telemedicine, with the former focusing on the use of telecommunications that provide medical and health education and services, the latter incorporating exchange of health information
to provide care. Scotland, meanwhile, has coined the term ‘tele-healthcare,’ which it defines as “the convergence of tele-care and telehealth to provide a technology-enabled and integrated approach to the delivery of effective, high quality health and care services,” and which “can be used to describe a range of care options available remotely by telephone, mobile, broadband and videoconferencing.” In the US, each state characterises telehealth differently, some excluding email, phone or fax communications; and two states, Rhode Island and New Jersey, lack any definition at all.
For the purposes of this paper, we use a broad definition of telehealth that includes telemedicine and incorporates the full spectrum of health care services, covering a wide range of fields such as education, management and diagnosis.
A note on definitions
5 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Chapter I: New policies for connected care era1
The US is the world’s largest healthcare market and a testing ground for how telehealth access plays out in a developed economy setting. The private sector is already pushing into the telehealth space. “Given the fact that we’re such an entrepreneurial society, virtual healthcare is becoming one of the most, if not the most, attractive areas for investments from venture capital,” says Mario Gutierrez, executive director of the Center for Connected Health Policy, a non-profit research organisation in California. “There are billions of dollars rapidly being invested both in technology and in companies that provide care virtually.”
Companies such as Teladoc provide anytime-anywhere medical consultations, which are helpful for people on the lowest level of ‘Obamacare’ insurance plans. To avoid paying the high deductibles common to such plans, such patients can contact Teladoc on an episodic basis and pay out of pocket. “So in one sense the country is moving very quickly to make care available,” Gutierrez explains. “At a price—it’s not free, so people pay in cash.”
But these tools will work best when the right policy adaptations are made. The Centers for Medicare & Medicaid Services (CMS) is the agency that administers Medicare, the federal program for seniors of 65 and over, and Medicaid in the US. States tend to follow the lead of the CMS and private payers look to the states for guidance. “It really has been a challenge because the federal government has not moved very quickly to change the laws related to telehealth in the Medicare program,” Gutierrez says. “The laws
were written at a time when telehealth was in its nascent form in terms of the technology,” he explains. “They are basically stuck in the 70s.”
In health, as in so many other areas, technology moves faster than the policy frameworks. No two US states are alike in how telehealth is defined, regulated and practised. California, for instance, is considered one of the leaders currently for having shifted financial incentives away from fee-for-service and towards value. “California tends to be a leader in healthcare improvements and changes, there’s much more openness here to doing that from the state government,” Mario Gutierrez says. Other states, like Texas, seem to be more cautious about the new technologies.
Diverse regulation creates a complex environment for stakeholders, particularly companies wanting to provide services in multiple states. And although legislation is advancing—in 2015, 42 states introduced more than 200 telehealth-related pieces of legislation—many of these changes are not yet in effect. Incentives are one area in need of attention. Currently many systems work on a fee-for-service model which rewards providers for individual services rendered. This structure dissuades practitioners, clinics and hospitals from making efficiencies and adopting telehealth, because that would reduce their payments. Better models are those of the Mayo Clinic or Kaiser Permanente which have planned an orientation on maintaining health (rather than curing illness) by paying providers a fixed salary and emphasising a value-based care model.

6 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Time for portable licenses?Recently, several states developed an Inter-State Medical Licensure Compact in which a growing number of states agreed to recognise the diligence their peers have conducted in awarding a license to a doctor. One of the driving factors was telehealth. “Proponents of telemedicine have often cited the time-consuming state-by-state licensure process for multiple-license holders as a key barrier to overcome in order for telemedicine to continue to grow and thrive,” the program’s website states. “The Compact would make it easier and faster for physicians to obtain a license to practice in multiple states, thus helping extend the impact and availability of their care at a time when demand is expected to grow significantly.” Dr Ommen notes that the compact eases the barrier to providing telemedicine in another state and creates
momentum that could lead to a system of mutual recognition across the country. “It starts a conversation around breaking down those state-by-state barriers so that in the future perhaps we will move to a broader licensing arrangement.”
Such effort to reduce state-by-state barriers is relevant for Europe, which has experienced many years of regulatory harmonisation efforts through the European Union, and is also an instructive model for other regions around the world who may benefit from harmonising licenses across provinces and sub-regions or even between neighbouring countries. The world is made up of many advanced and fledgling economic and regulatory unions between countries, which provide a foundation for collaboration on telehealth license portability and broader telehealth regulatory harmonisation.
The Mayo Clinic has main campuses in Minnesota, Florida and Arizona, and operates a broader system with more than 70 clinics and hospitals across four states. It offers telehealth to patients, physicians, and even employers—via portals through which patients can; access their electronic health records or where external physicians can upload information on patients and monitor those whom they have referred to the clinic; asynchronous services allowing secure communications between patients and their team; and e-consultations with external physicians. In addition, Mayo engages in “synchronous,” real-time activities such as video medicine and emergency video services for tele-stroke, partnering with smaller or rural hospitals in the region. “As a medical community in the US and abroad, we see a grand potential for mobile-enabled care,” says Dr Steve Ommen, a cardiologist and associate dean of the Mayo Clinic’s Center for Connected Care. “We just don’t know how it’s going to play out at this point because it’s a change in paradigm for most practices.”
A key issue is license portability. Telehealth means patients can access doctors regardless
of location, but licensing and certification rules differ by country, state or province. In the US, doctors’ licensing is regulated by states, with slightly different requirements for licensure in each state. The Mayo Clinic’s asynchronous services are available to a national audience because such communications are not categorised as practising across state lines. For synchronous services though, such as video-consultations, the situation is different. A doctor is not permitted to offer direct-to-patient care to a person in another state. Thus, if the Mayo Clinic in Minnesota treats a New Yorker and that patient has questions after he or she returns home, the Minnesota-based physician who treated the patient can conduct a follow-up video visit only if he or she is licensed to practice in New York. “If the physician isn’t licensed in New York then we would need to say the patient either needs to do their follow-up care with someone in New York who is licensed there—their local team who referred them,” Ommen explains, “or they need to come back here for their follow-up visit.”
Case study: Mayo Clinic’s connected care

7 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
The centre and the satellites: Telehealth access in EuropeAs the world’s most advanced regional economic and political union, Europe provides a useful case study in telehealth harmonisation and integration. Telehealth in the European Union is regulated largely by the health systems of individual EU member states, but the European Commission also plays a part. “In this particular field we always have these two elements, where the EU has a role and where the member states come in,” explains Dr Stephan Schug, chief medical officer of the European Health Telematics Association. “Telehealth and e-health are just in the middle because it’s always a little bit ICT and a little bit health and social care. So it’s always a little bit ‘European regulation’ and some elements which are reserved for national regulations.”
The European Commission has included telehealth as a key element in its “Digital Agenda for Europe” towards 2020, with Action 75 promising to “give Europeans secure online access to their medical health data and achieve
widespread telemedicine deployment.” The Commission drafted a green paper outlining stakeholder views about m-health, and is developing a code of conduct for m-health services to foster public trust in the fast-growing health app industry. Covering topics such as privacy and security, the code aims to raise awareness among app developers of EU data protection rules and to facilitate compliance. It has funded a number of projects including European Patients Smart Open Services (epSOS), in which 25 countries agreed on specific formats for electronic patient data to make them interoperable, so doctors in different jurisdictions could process them meaningfully.
This is encouraging progress but there will always be limits to how far the European Commission can go. “[It] can help to remove any roadblocks on the way and encourage member states to jointly agree on goals and on measures and so on. But I would not expect that there could be anything like a telemedicine directive or a telemedicine regulation. This would be against the European constitution,” says Dr Schug.
Other OECD countries are also showing political will to develop the policy frameworks to support telemedicine. Australia launched an electronic health record system in 2012 accessible to all citizens providing a summary of each individual’s important health information. The Australian government has funded pilot programs across multiple aspects of telehealth to explore whether it makes health services more accessible in remote areas, reduces unnecessary hospitalisations, improves communication between patients and carers and offers better communication
during health emergencies. Canada, another country with large swathes of rural terrain, has invested heavily in telehealth. Since 2001 the Canadian government has poured $2.1bn into more than 400 projects across the provinces and territories. In March 2015, availability of electronic health records was at 91% in Canada. In 2014, more than 500,000 clinician-patient consultations took place, according to the annual report of Canada Health Infoway, a government-funded think-tank charged with increasing the use of digital health solutions.
Telehealth policies in Australia and Canada
8 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
For telehealth to promote access to care, the communications infrastructure, especially broadband and mobile network coverage, needs to function effectively. According to Dr Verina Waights, a senior lecturer in professional healthcare education at the Open University, UK, such infrastructural issues are relevant even in developed regions. “For America, Eurasia and ourselves the issues are remarkably similar,” she says. “At the moment some countries have much better infrastructures than others but even they have black spots where you cannot get good broadband. We feel that’s going to create major issues and probably create more diversity among people being able to access services.”
The promise of telehealth is that it will cater to hard-to-reach patients, but rural areas are those most poorly served by broadband access. According to Kawaldip Sehmi, CEO of the International Alliance of Patients’ Organisations, poor broadband access perpetuates inequalities between rural and urban areas, creating a digital divide, even within individual countries. “Broadband services in rural areas are so bad that most patients living in rural areas cannot access or enjoy the benefits of online products and services.”
Even in a developed nation like the UK, pockets of the country have insufficient broadband strength to facilitate telehealth. The British government has invested £1bn in mobile and broadband infrastructure and promises to deliver high speed broadband across the country by 2018. Waights recommends that internet access is built in to new housing projects. The strategy has been
Chapter 2 - Communications infrastructure2
trialled in pilot form in Birmingham, where a community housing association teamed up with a wireless provider and the city council to give free Wi-Fi to 200 residents along with internet training. “Change has got to come from both sides, both improving the infrastructure and making it affordable so that people see it as a necessity,” says Waights.
Joining up telehealth systems with broader communications investment is also in play elsewhere in the OECD. New Zealand has established a National Telehealth Forum, supported by the National Health IT Board, which is part of the Ministry of Health, and a government-funded high speed broadband initiative is underway in parallel. This integration of internet accessibility and broader healthcare access strategy helps, suggests Dr Robyn Whittaker, an m-health expert and lead investigator in an SMS-based smoking cessation randomised trial. “I think the m-health initiatives are more likely to be successful if closely tied into health services.”
Disparities in access are also relevant in the US, where some people still use dial-up to connect to the Internet. According to Mario Gutierrez, this includes individuals and facilities offering healthcare services. “There are rural hospitals out there that would really benefit from those services but are still operating on dial-up,” Gutierrez says. Using mobile connectivity instead of broadband may be the answer - the model has been adopted to cater to rural communities in Spain, where broadband access is weak but mobile phone coverage can compensate. Dr
9 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Schug notes that some telehealth services work successfully through SMS messages. “You do not need broadband everywhere,” he says. It is also well-known in parts of Africa: “Emerging nations that do not have the infrastructure have been able to leapfrog and move very quickly to using technologies for communication between providers and consumers,” says Dr Schug.
Balancing interoperability with data securityInfrastructure is only partly a question for governments to address. For health providers, careful planning goes into the delivery of telehealth systems and ‘information architectures’. It may be unique for each system, depending on its specialisation, other systems they use, and their size, explains the Mayo Clinic’s Dr Ommen. New tools must integrate seamlessly with those already in place. “You don’t want each specialty having its own ‘one-off’ solution. So you do have to spend some time planning that,” he says.
Investment is needed to join a main hospital with smaller, satellite partners, or to support people outside the hospital firewall who will be connecting with those inside it. If the Mayo Clinic partners with a smaller hospital to provide tele-stroke care, for instance, it also trains staff at the partner hospital so that they understand the software and hardware and know where to access customer support if necessary. For all these systems, cyber security becomes paramount. The Mayo Clinic’s Office of Information Security rigorously vets any new technology system to ensure it meets a high security standard. “I would guess that most big systems have teams in place that are worried about information security just
to protect the patient’s health records,” Ommen says.
Interoperability between provider tools is a key infrastructure consideration when systems are complex. In the US, the Affordable Care Act promoted the use of electronic health records, but the systems in use are proprietary and do not connect with each other. CVS, the nation’s second largest pharmacy chain, installed virtual health advisory systems that provide access to mid-level physicians. In August 2015, it announced a partnership with several online doctor forums: American Well, Doctor on Demand and Teladoc. This represented a big step forward for telehealth. But providers of these services will have no access to the records of the patients who visit them, leading to potentially hazardous care inconsistencies. Moreover, it is likely that over time providers will interact with a broader care team perhaps comprising nutritionists, social workers and mental health counsellors. The potential of telehealth to bring together such a wide cast of actors is clearly exciting - but also raises questions about how data and information systems can be built which are both usable by such a large range of stakeholders, whilst not being vulnerable to data security compromises and integration problems.
This challenge will fade over time, Dr Ommen suggests. “In the history of our lifetimes, at one point Microsoft software products were incompatible with Apple computers and now if you’re heavily leveraged with the Microsoft Office product suite you can use it on any computer you want and it works fairly seamlessly. That will happen in this solution as well.”
10 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Using communications technologies to deliver healthcare may seem intuitive. After all, many people today are comfortable using mobile and Internet tools to manage important tasks such as personal banking. But precisely for that reason, tailored training is required to remind practitioners that standard privacy procedures still hold sway in the telehealth arena. The Center for Connected Health Policy provides etiquette training for physicians, covering how to talk to patients with whom they engage virtually. “There are some misconceptions,” Gutierrez observes. “I’m sitting here with my laptop and am speaking with a client and I have my door open. Well, I should be thinking about that in the context of that person being there in-person. A lot of the issues related to privacy and security need to be addressed,” he says. Telehealth changes the dynamic of physician-patient interactions, and doctors may need training to adapt effectively.
A second skills issue concerns hesitation within the medical community about telehealth itself. In part this involves a simple change in attitudes, habits and expectations; many doctors still feel more comfortable seeing a patient in person. Doctors will need to ask themselves whether they really need to see a patient in person or are just following a routine. Some physicians may feel threatened, worried that large hospitals with extensive telemedicine systems will encroach on their business. When the Texas Medical Board introduced new rules governing and restricting telemedicine in the state, Teladoc brought a lawsuit arguing that the board was blocking competition and trying to shut down Teladoc’s business in the state. “Doctors are trying
Chapter 3: Skilling up3to protect their practice from telemedicine, basically,” a Dallas-based healthcare attorney, Brenda Tso told National Public Radio at the time. Teladoc won the case.
Skilled patients…and carersSkills and behaviour change are not only relevant on the provider side. Patients and carers are also affected. Being able to join a video conference requires a certain minimum level of digital skill or IT support that must not be assumed. In some European countries, such as Bulgaria and Romania, around 40% of households do not have internet access, according to Eurostat, the EU’s statistics agency.1 This cohort of non-internet users largely comprises elderly and disabled people, says Dr Verina Waights, who conducts research into helping elderly and disabled people access and use telehealth. In a recent project, she took the approach of letting the patients engage with technologies through interaction rather than instruction. She worked with elderly people, and with informal or family carers and professionals. “Not in a formal way,” she emphasises, “but helping them learn the way that children explore, where you give it a go and see what happens.”
Confidence for carersSimilar issues can affect the confidence of carers, Waights notes. When her team offered training, carers were reluctant to take what they saw as a course in computers or IT, seeing it as too advanced for their everyday needs. But when telehealth was seen as more integral to their lives — learning more about the health condition of
1 EU statistics database Available at http://ec.europa.eu/eurostat
11 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
the person they supported – they became more enthusiastic. Both professional and informal carers describe themselves as time poor, says Waights, whose research spanned the UK, Greece, the Netherlands and Spain. “Across all four countries, nobody wanted a computing course,” she says. “We embedded the skills through the things they did want to know about.”
Professional carers are beginning to receive digital training as a matter of routine. For example, Skills for Care, an organisation for workforce development in adult social care in the UK, offers a module on digital working and incorporates digital learning and information sharing in its overall strategy. About 80% of
carers and older people are unaware of the services and devices that could help them, says Waights. Her team raises awareness among those who might benefit. Co-design, involving senior citizens in solutions, could help. “We need [to be] working together with the people who will be using these devices and the solutions, right from the beginning,” she says. Through face-to-face training, her team helped older people with preliminary decisions, such as which types of computers to buy, how to send email, and how to broaden their online social engagement. “It’s looking at it in the round, rather than focusing on just one angle,” Waights says.
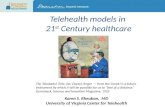
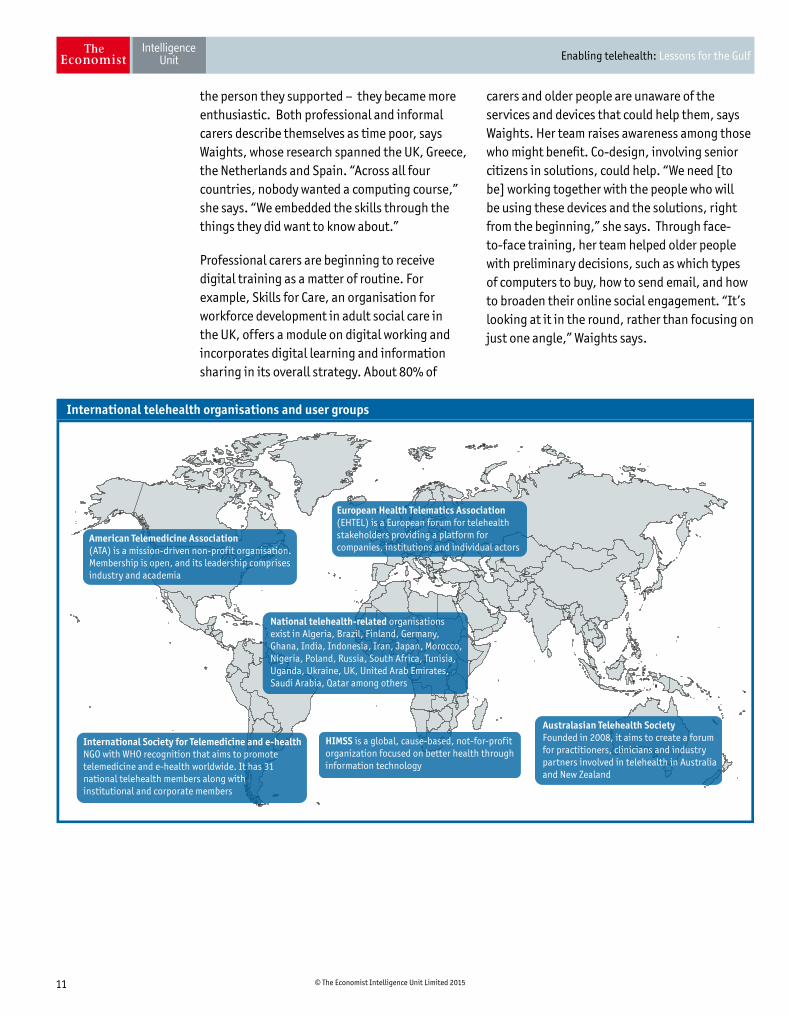
American Telemedicine Association(ATA) is a mission-driven non-profit organisation.Membership is open, and its leadership comprisesindustry and academia
Australasian Telehealth SocietyFounded in 2008, it aims to create a forumfor practitioners, clinicians and industrypartners involved in telehealth in Australiaand New Zealand
National telehealth-related organisationsexist in Algeria, Brazil, Finland, Germany,Ghana, India, Indonesia, Iran, Japan, Morocco,Nigeria, Poland, Russia, South Africa, Tunisia,Uganda, Ukraine, UK, United Arab Emirates,Saudi Arabia, Qatar among others
European Health Telematics Association(EHTEL) is a European forum for telehealthstakeholders providing a platform forcompanies, institutions and individual actors
International Society for Telemedicine and e-health NGO with WHO recognition that aims to promotetelemedicine and e-health worldwide. It has 31national telehealth members along withinstitutional and corporate members
International telehealth organisations and user groups
HIMSS is a global, cause-based, not-for-profit organization focused on better health through information technology
12 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
The total healthcare spending in the Gulf Cooperation Council (GCC) region is forecast to reach $60 billion by 2025, as a result of population growth and a rise in chronic, non-communicable diseases.2 Non-communicable disease are among the most complex and costly to manage, suggesting that a well-designed and flexible health system is vital to ensure the GCC region can provide standards of care needed in a tough new era. The region’s abilities to harness telehealth and provide the enabling framework hang in the balance: it has a generally high income level with strong rates of ICT penetration and infrastructure. At the same time, it has limited experience of regional healthcare regulation and harmonisation, and a skills shortage in healthcare.
The member states within the GCC, an economic and political union, are relatively well-integrated from an economic perspective. Intra-GCC trade has increased seven-fold since 2000, a year before the formation of the customs union, to just under $100bn in 2013. Plans to develop a GCC-wide rail network are underway, expected to further facilitate trade. Components are being developed independently, such as the Etihad Rail in the UAE, designed to connect to the larger GCC network. Through an interconnected power grid, the countries are also set up to share surplus electricity between member states, which could save governments up to $6bn in surplus power capacity. Through the Gulf Cooperation Council Interconnection Authority, they are able to monitor electricity consumption in real-time and assess potential gaps. Co-developed regulation under the Gulf Standards Organisation includes the Gulf Conformity Marking, the regional
Chapter 4: Lessons for the GCC4equivalent to the European CE marking. Such integration suggests a reasonable track-record to be utilised in a new areas such as telehealth although so far, there is limited concrete evidence of a joined-up approach.
Policy momentumLed by Saudi Arabia, Qatar and the UAE, there is evidence that GCC countries are keen adopters of telehealth. The GCC leads the Middle East in terms of telehealth enabling environments. E-health and telehealth strategies have government support in Saudi Arabia,3 Qatar4 and the United Arab Emirates,5 who have invested in initiatives to integrate telehealth with wider reforms. The GCC countries are developing regional harmonisation initiatives, evident in discussions about a “smart card” digital ID that would include people’s health information, which proponents hope will be interoperable across the region.6 There is a centralised GCC drug registration system currently, and GCC members have stated their aim to increase broader integration through a recommended “Unified Gulf Plan for Prevention and Control of Non Communicable Diseases 2014-2025”.
Each country in the region has its own policy stance. A rich nation with a growing population and increasing demands on its healthcare system, Saudi Arabia made telehealth a central part of its healthcare policy. In a public presentation in December 2013, the deputy minister for health, Mohammed Al Yemeni, stressed that Saudi Arabia “has allocated a huge budget for e-health, since access to healthcare services in remote and rural areas is of prime importance.”7
2 “GE and Gulf Capital to tap health market”, The National, January 30th 2010
3 Kingdom of Saudi Arabia Ministry of Health portal. Available at: http://www.moh.gov.sa/en/Ministry/nehs/Pages/Overview-of-eHealth.aspx
4 National E-Health and Data Management Strategy Draft for Stakeholder Consultation, PwC 2015. Available at: http://www.nhsq.info/app/media/3125
5 “Abu Dhabi Healthcare Strategic Plan Announced”, Abu Dhabi Health Authority press document. Available at: http://www.haad.ae/haad/tabid/58/ctl/Details/Mid/417/ItemID/463/Default.aspx
6 “GCC smart card steering committee commends UAE’s ‘Digital Authentication’ project”. United Arab Emirates media centre, 2014. Available at: http://www.id.gov.ae/en/media-centre/news/2014/10/31/gcc-smart-card-steering-committee-commends-uaes-digital-authentication-project.aspx
7 “The Social Impact of eHealth Integrated Health Innovations Conference Dubai, United Arab Emirates” presentation, Deputy Minister of Health for Planning & Health Economics. Available at: http://www.himssme.org/innovations13/docs/HIMSSME_IHIC13_SpeakersPresentation_MohammadAlyemeni.pdf
13 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
Saudi Arabia has created an eHealth Strategy and Change Management Office that has developed an evaluation framework to “define, quantify and track the eHealth strategy performance in addition to social and financial benefits of the eHealth investments” and the government portal lays out 1, 3 and 5 year commitments.8 This combination of political will and investment has led to Saudi Arabia being characterised as the “fastest growing health IT market in the Middle East,”9 by the Saudi Gazette, growing at 13.4% per year.10
Spending on IT services and products is also forecast to grow quickly in the United Arab Emirates, where Mubadala Healthcare, established by the Abu Dhabi government, recently joined forces with the Swiss firm Medgate to launch the Abu Dhabi Telemedicine Centre, which will offer around-the-clock consultations in Arabic and English. The Centre is covered by some national health insurance plans and provides eligible patients located across the country direct access to medical advice, thereby “increasing access to healthcare particularly for patients living in areas of the Emirates which may not have providers nearby,” Hasan Al Attas, its general manager, told Middle East Health Magazine. Abu Dhabi’s engagement with telehealth is also evident in key upcoming milestones such as hosting the World Telemedicine and e-Health Forum, sponsored by the International Society for Telemedicine and eHealth (ISfTeH), in March 2016.
Nearby, Qatar launched a national e-health strategy in June 2015, aiming to define national policies and regulations, establish standards for interoperability and data-sharing, and encourage the use of e-health.11 Authorities are also looking more broadly at technologies to support care delivery, such as Dubai Health Authority’s plans to deploy Android tablets as part of an effort to build ‘smart hospitals’ that will improve customer experience.
Looking to the OECD nations explored in this report, several trends are pertinent to the Gulf.
The first is license portability and regional harmonisation to allow users to benefit from the ‘borderless’ promise of telehealth. Countries must find the right balance between national versus supra-national rules. In the case of the UAE, there is the added complexity of a country comprised of seven individual Emirates, with different regulatory structures. Most medical expertise is clustered in Abu Dhabi and Dubai, but such knowledge need not be limited to these markets if patients in other Emirates can interact with medical specialists there.
Policy harmonisation may focus on efficient licensing structures first if telehealth is to enable patients to access medical expertise outside of their country, region or province. Where general governance standards converge, regulatory bodies in the GCC could build on the licensing decisions of neighbouring authorities to create ‘portable’ licenses that allow clinicians and medical providers to interact with patients in other regions. Governments and regions can look to initiatives such as the Inter-State Medical Licensure Compact as a valid model, although it requires significant trust in the decisions of other authorities. A more technical measure to support integration could be the linking up of existing digitisation programs – of health systems and patient health records – which is a priority in some nations who wish to build a unified electronic health records system. Such systems support the transmission of information across borders, although privacy and security related factors need to be borne in mind as the user base expands. A number of areas will need to be unified if a regional telehealth market is to emerge, such as definitions of telehealth and consistent data privacy and information protection.12
Infrastructure backdropMobile penetration across the Middle East rose rapidly from 3% in 2000 to 100% in 2012.13 Gulf countries have superior ICT infrastructure than their neighbours in Arab states,14 and governments’ commitment places the UAE, Qatar and Saudi Arabia, as well as Bahrain, at
8 Kingdom of Saudi Arabia Ministry of Health portal, ibid.
9 “KSA ‘fastest growing’ eHealth market in the Middle East”, Saudi Gazette. Available at: http://www.saudigazette.com.sa/index.cfm?method=home.regcon&contentid= 20141119224908
10 IDC Middle East and Africa Healthcare Provider 2013 IT Spending and 2014–2018 Forecast. Available at: https://www.idc.com/getdoc.jsp?containerId=prAE25365015
11 National E-Health and Data Management Strategy Draft for Stakeholder Consultation. Available at: http://www.nhsq.info/app/media/3125
12 “Telemedicine - the high tech answer to the UAE’s burgeoning health needs?”, “Albawaba Business”, May 10th 2015. Available at: http://www.albawaba.com/business/telemedicine-high-tech-answer-uaes-burgeoning-health-needs-692360
13 Technology, Media & Telecommunications Predictions 2015 Middle East, Deloitte.
14 “Bridging the digital divide through ICT: A comparative study of countries of the Gulf Cooperation Council, ASEAN and other Arab countries”, Kaba and Said. “Information Development”, November 2014 vol. 30 no. 4 358-365

14 © The Economist Intelligence Unit Limited 2015
Enabling telehealth: Lessons for the Gulf
the forefront of ‘network readiness’ in the MENA region.15 The Saudi market stands out, with 16m internet users representing over 50% of the population.
A 2014 report by GSMA, the mobile industry association, notes that Arab states were relatively late to launch higher speed networks but are now catching up. In the UAE, Saudi Arabia and Qatar, as much as 60% of internet connections now operate through 3G and 4G. Despite this, there are still broadband blind spots and portions of the population, especially the elderly and the disabled, who may not use the Internet. Mobile broadband rather than fixed broadband communication links may be the way forward for telehealth, especially in Saudi Arabia, where rural villages punctuate large areas of desert and fixed-line infrastructure is weak.
Engagement with the telecommunications players can be helpful, especially given the dominance of indigenous multinational telecommunications companies who provide a more efficient route to reach large populations than would be the case in more fragmented telecommunications markets. The UAE sought to bridge connectivity with telehealth tools through a 2012 agreement between Etisalat and du, large local telecommunications providers, to become directly involved in e-health. In January this year, the UAE government signed a deal with Etisalat and du to develop mobile health products. Etisalat has also deployed GE’s cloud-based Muse Cardiology Information System.
Skills and knowledge flowsNew skills, among patients and providers, are critical to enabling telehealth in the Gulf. Partnerships, such as that between Mubadala Healthcare in the UAE and Medgate, are one way to foster knowledge exchange. Strong international linkages can have benefits. In the UAE, Johns Hopkins has constructed a centre of healthcare excellence, and Harvard University has its own under way, which brings expertise and research capabilities.
However, the success of telehealth will rely not only on skills but also attitudes. A 2012 survey into
the use of telemedicine technologies in eastern Saudi Arabia found that “although telemedicine is promising and the Ministry of Health in Saudi Arabia has allocated a huge budget for e-health, the telemedicine modalities used were very limited.” Interest among health professionals was high but adoption was low, and those who did deploy it found it less easy to use than hoped. The study recommended more information about telemedicine and better training of health professionals.16 Governments also need to invest in training to ensure the neediest populations are comfortable with telehealth.
While the rapid rise on mobile phone usage, particularly among younger people, indicates a market ripe for telehealth adoption, there continues to be some reluctance among the public. Research into the use of tele-dermatology conducted by King Faisal University, Saudi Arabia, found that 14% of patients declined to send photographs of skin blemishes to doctors, citing social or religious reasons.17 Such cultural or social considerations must be kept in mind as policies and infrastructure around telehealth are developed. Telehealth cannot be seen as fully substitutable with conventional, in-person patient-doctor interactions.
The Gulf experience is some ways mimics that of the OECD nations explored earlier in this report. Ensuring access to telehealth depends here, as elsewhere, not just on the technologies, but on the broader enabling environment, especially infrastructure, policy and skills training. The innovation frontier is moving forward with increasing speed, capturing the interest of healthcare companies and venture capital. But to fully realise its potential – and to achieve its goal of strengthening access to health – telehealth requires the right enabling environments. The Gulf has an enormous healthcare challenge due to demographic shifts, affluence and the rise of ‘Western’ diseases. Watching from the experiences of North America, Europe, Australia and New Zealand could provide valuable experiences and lessons to guide decision-making in the Gulf.
16 “Successes and Challenges in the Implementation and Application of Telemedicine in the Eastern Province of Saudi Arabia”, El-Mahalli et al., Perspect Health Inf Manag. 2012 Fall; 9(Fall)
17 The Social Impact of eHealth Integrated Health Innovations Conference Dubai, United Arab Emirates presentation, ibid.
15 World Economic Forum, The Global Information Technology Report 2015

Cover image - © Graphicworld/Shutterstock
While every effort has been taken to verify the accuracy of this information, The Economist Intelligence Unit Ltd. cannot accept any responsibility or liability for reliance by any person on this report or any of the information, opinions or conclusions set out in this report.
LONDON20 Cabot SquareLondonE14 4QWUnited KingdomTel: (44.20) 7576 8000Fax: (44.20) 7576 8500E-mail: [email protected]
NEW YORK750 Third Avenue5th FloorNew York, NY 10017United StatesTel: (1.212) 554 0600Fax: (1.212) 586 1181/2E-mail: [email protected]
HONG KONG1301 Cityplaza Four12 Taikoo Wan RoadTaikoo ShingHong KongTel: (852) 2585 3888Fax: (852) 2802 7638E-mail: [email protected]
GENEVARue de l’Athénée 321206 GenevaSwitzerlandTel: (41) 22 566 2470Fax: (41) 22 346 93 47E-mail: [email protected]
DUBAIOffice 1301aAurora TowerPO Box 450056Dubai Media CityDubaiUnited Arab EmiratesTel: (971) 4 433 4208Fax: (971) 4 438 0224E-mail: [email protected]