
EMS Protocols - Thurston County
209
Thurston County EMS Protocols Medical Program Director Dr Larry Fontanilla, MD May 2011
Transcript of EMS Protocols - Thurston County

Thurston County
EMS Protocols
Medical Program Director Dr Larry Fontanilla, MD
May 2011

Thurston County
EMS Protocols
This document describes the methods by which the Thurston County EMS System will continue to provide the highest quality prehospital patient care available. We have incorporated evidence based guidelines with historically proven practices to produce this document. While it is impossible to address every possible variation of disease or traumatic injury, these policies, protocols, and procedures do provide a foundation for treating the vast majority of patients we encounter. Certainly our education, experience and clinical judgment will assist us as we provide the highest quality patient care available. Additionally, on-line medical control is available for those patient presentations that do not fall within the scope of the document.
Dr. Larry Fontanilla, MD Medical Program Director
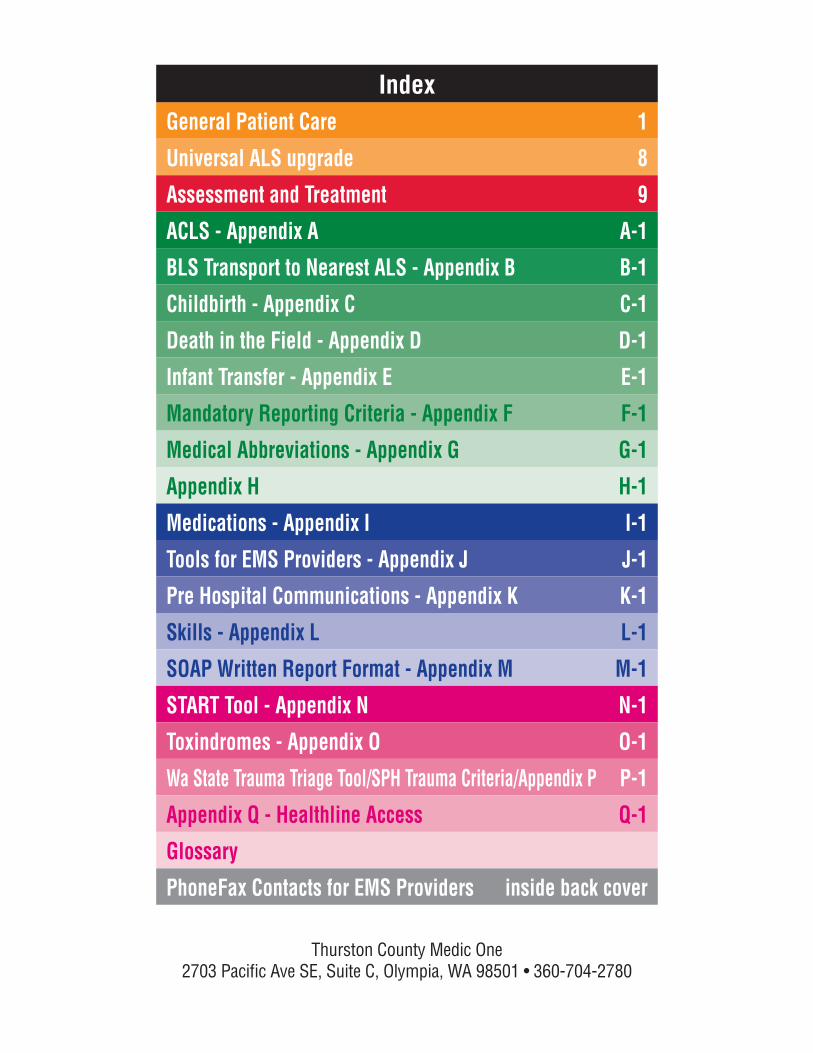
General Patient Care 1
Universal ALS upgrade 8
Assessment and Treatment 9
ACLS - Appendix A A-1
BLS Transport to Nearest ALS - Appendix B B-1
Childbirth - Appendix C C-1
Death in the Field - Appendix D D-1
Infant Transfer - Appendix E E-1
Mandatory Reporting Criteria - Appendix F F-1
Medical Abbreviations - Appendix G G-1
Appendix H H-1
Medications - Appendix I I-1
Tools for EMS Providers - Appendix J J-1
Pre Hospital Communications - Appendix K K-1
Skills - Appendix L L-1
SOAP Written Report Format - Appendix M M-1
START Tool - Appendix N N-1
Toxindromes - Appendix O O-1
Wa State Trauma Triage Tool/SPH Trauma Criteria/Appendix P P-1
Appendix Q - Healthline Access Q-1
Glossary
PhoneFax Contacts for EMS Providers inside back cover
Index
Thurston County Medic One


1
General Patient Care
I. Airway – management shall be in accordance with American Heart Association (AHA) Standards
Head tilt – chin lift (not for trauma) Jaw thrust
Suctioning Finger sweep (no blind finger sweeps for infants
or children) Abdominal thrusts (chest thrusts for infants)
Direct laryngoscopy and removal of an obstruction with Magill forceps
Positioning Insertion of an oropharyngeal airway Insertion of a nasopharyngeal airway Orotracheal intubation
− Eschmann-type stylette Laryngeal mask airway Surgical intubation with cricothyroidotomy device
II. – shall be enhanced, assisted or maintained using the following equipment/techniques:
III. Ventilation – shall be enhanced, assisted or maintained using the following equipment/techniques:
rate of 15-25 lpm
General Patient Care Procedures
Bold Italics indicate an ALS procedure

2
Gene
ral P
atie
nt C
are
1. Used to assist a conscious seated patient 2. Used to assist or breathe for an unconscious patient
(*medical patients only)3. Used in conjunction with an endotracheal tube
IV. Circulation
Control bleeding with direct pressure. If unsuccessful, elevate and use pressure points. As a last resort,
1. All cardiac arrest patients who do not meet the Death in Field (DIF) criteria (Appendix D) will have resuscitation attempted.
2. If a patient does not meet the criteria in the DIF
personnel shall begin resuscitation and apply an AED.3. Cardiopulmonary resuscitation shall be performed in
accordance with current AHA guidelines.
1. The goal of fluid resuscitation in the setting of hypovolemia or uncontrolled bleeding is to obtain and maintain a systolic blood pressure of 90-100 mmHg.
2. Initial fluid resuscitation for children less than 8 y/o and presenting with signs or symptoms of shock should consist of a 20 ml/kg bolus of normal saline, repeat x2 prn.
3. who exhibits signs or symptoms of hypoperfusion.
following sites:
General Patient Care Procedures

3
General Patient Care
General Patient Care Procedures
a) Right internal jugular veinb) Right subclavian veinc) Right or left femoral vein
5. intraosseous infusion:a) Adult – Medial aspect of the proximal tibiab) Child – Medial aspect of the proximal tibia
V. Disability – evaluation of mechanism of injury (MOI) should be completed for every patient who is suspected of having a spinal injury
situation otherwise suggests a change in their health status, should receive a complete assessment.
and paramedics shall use the Spinal Immobilization Decision Tool (Appendix L) for those patients with uncertain mechanism or injury.
of spinal injury or who meet the exclusion criteria of the Spinal Immobilization Decision Tool shall have full spinal immobilization applied.
discomfort. Pregnant patients should have the
should be immobilized:1. Long bone: Immobilize joint above and below the
injury. Splint in gross anatomical alignment. Tension should be applied and the limb stabilized during realignment and splinting. If the fracture cannot be reduced because of severe pain or remains in a position incompatible with transport, an ALS upgrade is indicated.
4
Gene
ral P
atie
nt C
are
General Patient Care Procedures
2. Joint: Immobilize long bone above and below the injury. Splint in the position found. If no pulse attempt to realign one time.
3. Distal PMS should be evaluated and recorded before and after splinting.
administration of pain medication.
VI. Pain management
of all patients in severe pain.
pain should be attempted such as placing the patient
immobilizing and splinting painful areas.
physiologic signs of severe pain including: diaphoresis, tachycardia, hypertension, tachypnea, pallor or significant grimacing.
management if they:
interventions, andshow physical or physiologic signs of pain, andrate their discomfort at 7 or greater, and
receive an IV opiate injection Any patient receiving opiate pain management, will
be transported by ALS and must:
measurements every 5 minutes
5
General Patient Care have code summary attached to their patient
care reportVII. Communication
accompanied by an explanation for the upgrade.
responding medic units.
are required to give a complete verbal report (Appendix
scene cannot cancel an EMT or higher-level response to the scene.
supervising physician when:1. Directed to do so by protocol.2. The paramedic has evaluated a patient and is
the scene. 3. The paramedic is on scene with a patient who meets
Steps 1-4 Washington State Trauma Triage Tool
for any critical patient is desirable. The base station physician is always available for
consultation with the paramedic.
the receiving facility to give a short verbal report. If patient condition changes significantly while en route (e.g. Section VIII, “Ground transport”), the receiving facility should receive an updated report as soon as possible.
1. A verbal report must be given at every handoff of a patient.
General Patient Care Procedures
6
Gene
ral P
atie
nt C
are
2. The first-arriving unit will provide an initial written report of patient care to the transporting unit. The EMS provider who performs the hands-on exam is responsible for writing the report.
3. Each EMS unit that performs an assessment of the patient shall provide a written report that accompanies the patient to the hospital. The provider performing the examination shall complete the narrative (SOAP) portion of this report.
the elements of a complete SOAP note (Appendix M), including medications and vital signs.
replace or qualify as a written report.
VIII. Transport
1. In general, patients should be transported to the hospital of their choice. Patients in need of specialty care (e.g. pediatric center, trauma center) require consult with the base station physician.
en route to a hospital, a request for ALS upgrade should be made; the ALS unit dispatched should
1. Any field provider may request air transport via TCOMM. An ALS upgrade is required. Transport destination shall be determined by the ALS provider in consultation with medical control physician.
2. The primary provider of air transport services for
General Patient Care Procedures
7
General Patient Care3. Use of air transport should be coordinated with the
incident commander.
with a report for any patient transported by air.ALL
should be afforded the best possible safety measures available while being transported:1. When possible, patients should be transported
sitting up. 2. Fasten all manufacturer-supplied gurney safety belts.
patient compartment during transport.
their seat belts whenever possible.5. Children should be restrained in a size-appropriate
child-restraint device whenever possible.
IX. Dispute resolution
disputes between personnel on the scene is preferred.
disagree about treatment, the most conservative
personnel on the scene disagree about whether an ALS upgrade is necessary, an ALS upgrade for evaluation will be requested.
a course of action for a particular patient, the most conservative approach (usually an ALS transport) will be followed.
General Patient Care Procedures
Univ
ersa
l ALS
Upg
rade
s
8
Universal ALS Upgrades
I. An ALS evaluation is required if any of the conditions listed below are present:
compromise
radial pulse)
lung sounds
to vehicle)
9
Assessment and Treatm
entAssessment and Treatment
MedicalAbdominal / Back Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Allergic Reaction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Animal Bites . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Bleeding (Non-traumatic) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Breathing Difficulty. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Chest Pain / Discomfort / Heart Problems . . . . . . . . . . . . . . . . 21Choking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Diabetic Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Environmental Emergencies. . . . . . . . . . . . . . . . . . . . . . . . . . . 27Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31Mental / Emotional / Psych. . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Overdose / Poisoning (Toxic Exposure) . . . . . . . . . . . . . . . . . . 35Pregnancy / Childbirth / OB-GYN . . . . . . . . . . . . . . . . . . . . . . . 37Seizures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Unconscious / Syncope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
TraumaAbdominal Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Burns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48Chest Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51Extremity Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Head and Neck Trauma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55Spinal Trauma. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59Submersion Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
10
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
Pertinent Objective Findings
ALS Upgrade Required For
syncope or heavy vaginal bleeding
greater than 50
Abdominal / Back Pain

11
Assessment and Treatm
entAssessment / Differential Diagnosis
disease
Plan/Treatment
ALS
Abdominal / Back Pain

12
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
and severity
possible allergens®
Pertinent Objective Findings
or tongue
ALS Upgrade Required For
AND has a history of anaphylactic reaction to this allergen
Allergic Reaction

13
Assessment and Treatm
entAssessment / Differential Diagnosis
Plan/Treatment
® (if indicated)
patient’s albuterol
it’s present
ALS
Allergic Reaction

14
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
Pertinent Objective Findings
around site
− Altered or decreased mental status
− Hypotension − Tachycardia− Tachypnea
− Oral paresthesia or unusual tastes
ALS Upgrade Required For
Assessment / Differential Diagnosis
Animal Bites

15
Assessment and Treatm
entPlan/Treatment
Poison Center at 800-709-0911
ALS
Animal Bites

16
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
diarrhea − Coumadin®
− Cancer− Ulcer− Alcoholism− Recent surgery
Pertinent Objective Findings
ALS Upgrade Required For
Bleeding (Non-traumatic)

17
Assessment and Treatm
entAssessment / Differential Diagnosis
Plan/Treatment
ALS
Bleeding (Non-traumatic)

18
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
− Smoking− Asthma / Reactive
− COPD− Intubated previously
− Anxiety/hyperventilation
Pertinent Objective Findings
mental status
sentences
rhonchi)
10 or greater than 36
greater than 140
hypotension
peripheral)
edema)
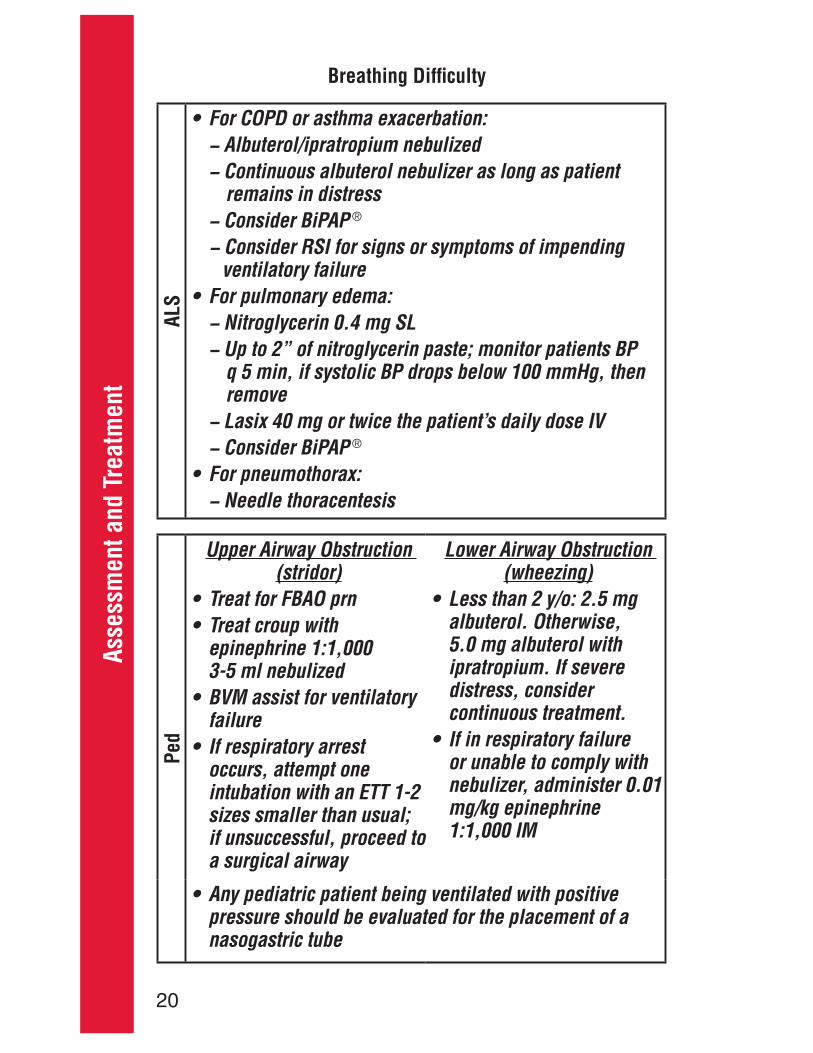
Breathing Difficulty

19
Assessment and Treatm
entALS Upgrade Required For
Assessment / Differential Diagnosis
syndrome
Plan/Treatment
the patient
Breathing Difficulty
20
Asse
ssm
ent a
nd T
reat
men
t
ALS
®
®
Ped
Breathing Difficulty
21
Assessment and Treatm
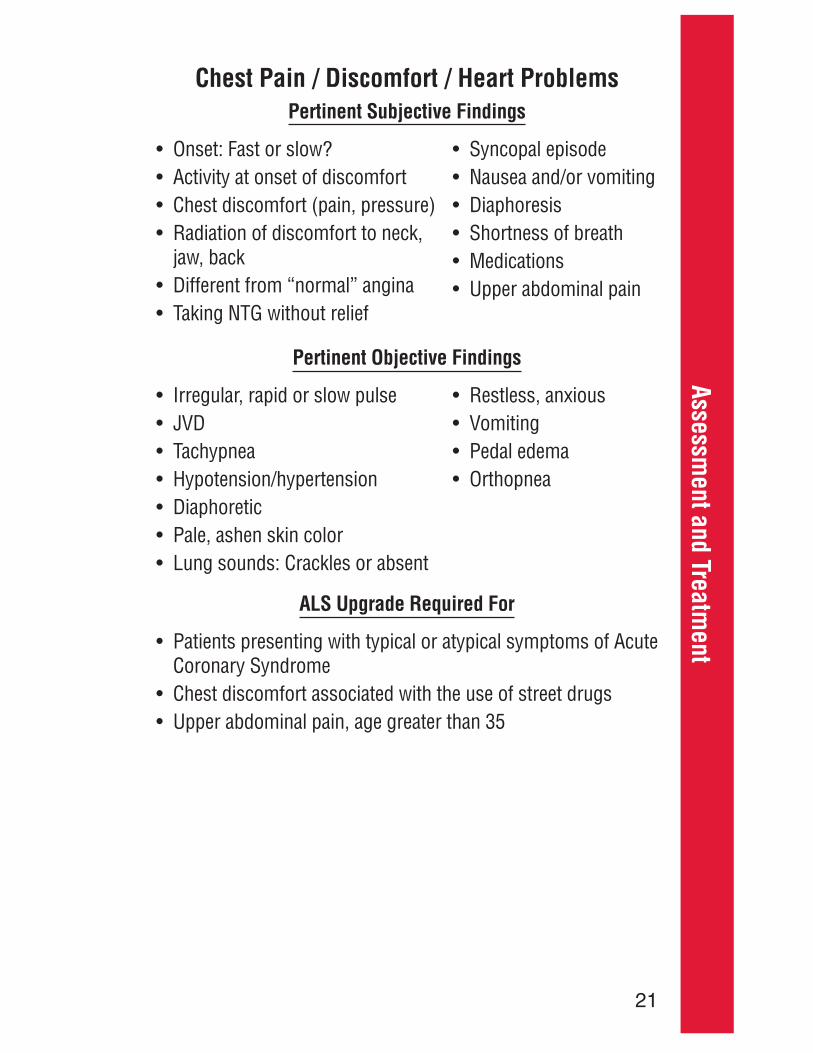
entPertinent Subjective Findings
Pertinent Objective Findings
ALS Upgrade Required For
Coronary Syndrome
Chest Pain / Discomfort / Heart Problems

22
Asse
ssm
ent a
nd T
reat
men
tAssessment / Differential Diagnosis
Syndrome
Plan/Treatment
chest discomfort
ALS
Ped
Chest Pain / Discomfort / Heart Problems
23
Assessment and Treatm
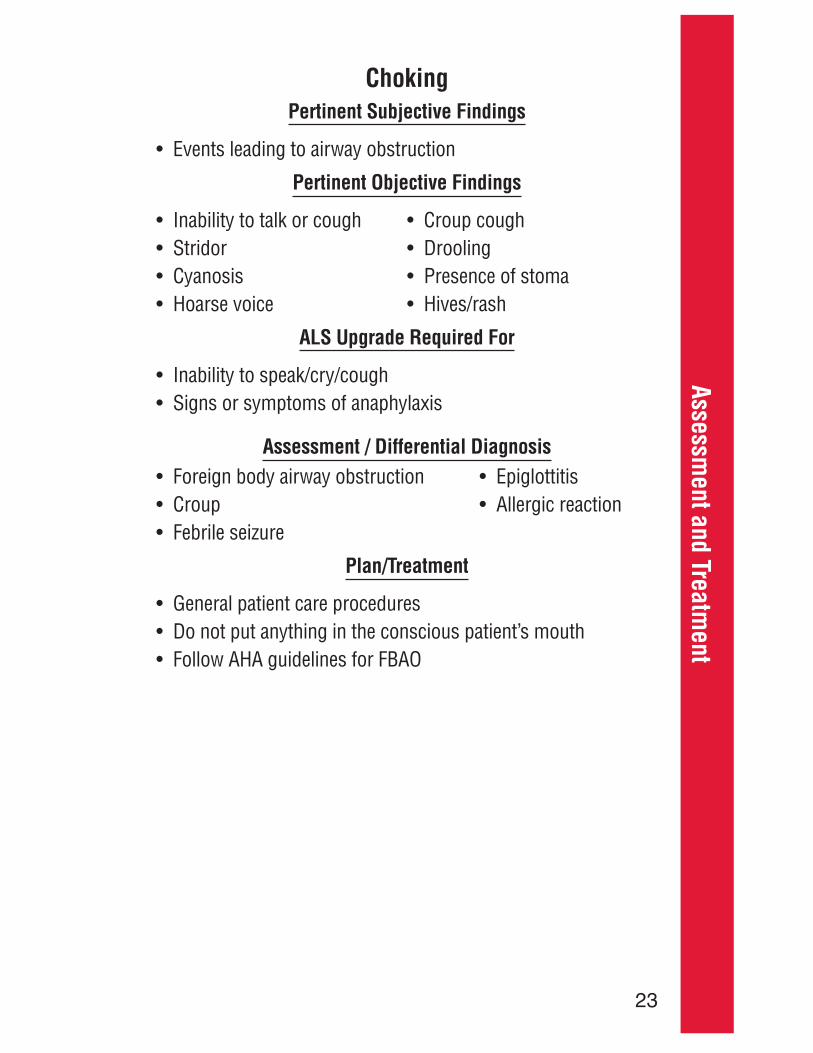
entPertinent Subjective Findings
Pertinent Objective Findings
ALS Upgrade Required For
Assessment / Differential Diagnosis
Plan/Treatment
Choking

24
Asse
ssm
ent a
nd T
reat
men
t
ALS
Peds
Choking Emergencies

25
Assessment and Treatm
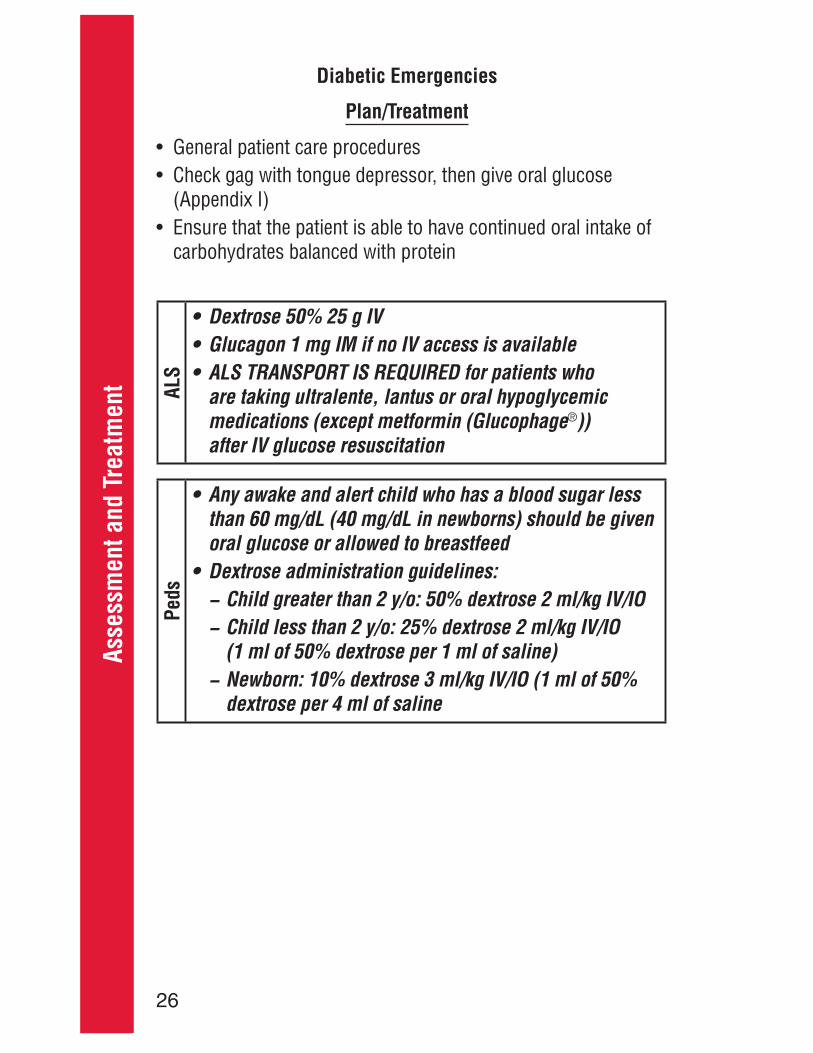
entDiabetic Emergencies
Pertinent Subjective Findings
(Time last taken)− Oral hypoglycemic agents
Pertinent Objective Findings
− Altered or decreased mental status
− Signs or symptoms of shock
− Altered or decreased mental status
− Irregular respirations− Odor of ketones on breath− Dehydration (dry mucous
tachycardia)
ALS Upgrade Required For
Assessment / Differential Diagnosis
− Insulin− Oral hypoglycemic agents− Alcohol− Aspirin− Beta blockers
26
Asse
ssm
ent a
nd T
reat
men
tPlan/Treatment
(Appendix I)AL
S
®
Peds −
−
−
Diabetic Emergencies
27
Assessment and Treatm
entEnvironmental Emergencies
Pertinent Subjective Findings
prior to c/o symptoms
engaged in prior to c/o symptoms
hostile environment
is taking
− Cramps− Dizziness
− Has any attempt been made to
exposure accidental or

28
Asse
ssm
ent a
nd T
reat
men
tPertinent Objective Findings
mental status
− Skin irritation at contact site
− Respiratory distress
Salivation Lacrimation Urination Defecation Gastrointestinal Emesis
− Tachycardia− Tachypnea
or hard skin− Absence of
shivering− Bradycardia
− Hypotensive
ALS Upgrade Required For
Assessment / Differential Diagnosis
hazardous materials
Environmental Emergencies

29
Assessment and Treatm
entEnvironmental Emergencies
Plan/Treatment
− Rest patient
inducing shivering
− Check rectal temperature
− Handle patient very gently− Check carotid pulse for a full minute before starting CPR
protocol as per normothermic patients
axilla and groin− Check rectal temperature
treatment recommendations
30
Asse
ssm
ent a
nd T
reat
men
t
ALS
Peds
Environmental Emergencies
31
Assessment and Treatm
entHeadache
Pertinent Subjective Findings
mental status
side(s))
rigidity)
Pertinent Objective Findings
mental statussensation
ALS Upgrade Required For
or diastolic blood pressure greater than 110

32
Asse
ssm
ent a
nd T
reat
men
tAssessment / Differential Diagnosis
(SAH)
Plan/Treatment
ALS
Headache
33
Assessment and Treatm
entPertinent Subjective Findings
illness or injury
disorders
the patient
attempts
abused substance
patient’s environment
Pertinent Objective Findings
substances
ALS Upgrade Required For
from the scene to the hospital
Mental / Emotional / Psych
34
Asse
ssm
ent a
nd T
reat
men
tAssessment / Differential Diagnosis
− Schizophrenia− Depression− Mania− Anxiety
− Alcohol/acidosis− Epilepsy/electrolytes/
endocrine− Insulin (hypo/
hyperglycemia)− Overdose− Uremia/underdose− Trauma− Infection− Psychosis− Pump/poison− Stroke/shock
Plan/Treatment
ALS
Mental / Emotional / Psych

35
Assessment and Treatm
entPertinent Subjective Findings
Pertinent Objective Findings
status− Salivation− Lacrimation− Urination− Defecation− Gastrointestinal − Emesis
(See Appendix O for signs and symptoms of specific poisoning syndromes)
ALS Upgrade Required For
Overdose / Poisoning (Toxic Exposure)

36
Asse
ssm
ent a
nd T
reat
men
tAssessment / Differential Diagnosis
Plan/Treatment
treatment recommendations
ALS
Overdose / Poisoning (Toxic Exposure)

37
Assessment and Treatm
entPertinent Subjective Findings
pregnancies
ultrasound)
− Number of pads/tampons used per hour
− Passing any tissue
abd/back pain
− Hypertension− Miscarriage
Pertinent Objective Findings
and duration)
prolapsed/nuchal cord)
vaginal discharge
Pregnancy / Childbirth / OB-GYN
38
Asse
ssm
ent a
nd T
reat
men
tALS Upgrade Required For
− Contractions 2 min apart (first pregnancy)− Contractions less than 5 min apart (other pregnancy)
uterine contractions
syncope or heavy vaginal bleeding
or greater than 90 mmHg diastolic
Assessment / Differential Diagnosis
(miscarriage)
Pregnancy / Childbirth / OB-GYN
39
Assessment and Treatm
entPlan/Treatment
pregnancy or childbirth
side for transport
− Emergent transport
in birth canal
− Emergent transport
− Massage uterus− Encourage baby to nurse
− Supportive care− Treat for seizures as needed
ALS
Pregnancy / Childbirth / OBGYN

40
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
medications
abstinence
seizure
Pertinent Objective Findings
bladder)
mental status
ALS Upgrade Required For
or abrupt onset of severe headache
Seizures

41
Assessment and Treatm
entAssessment / Differential Diagnosis
alcohol use
Plan/Treatment
ALS
Peds
Seizures

42
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
or similar
− Anti-hypertensives− Blood thinners− Aspirin
Pertinent Objective Findings
mental status
sensation
or receptive)
ALS Upgrade Required For
Stroke
43
Assessment and Treatm
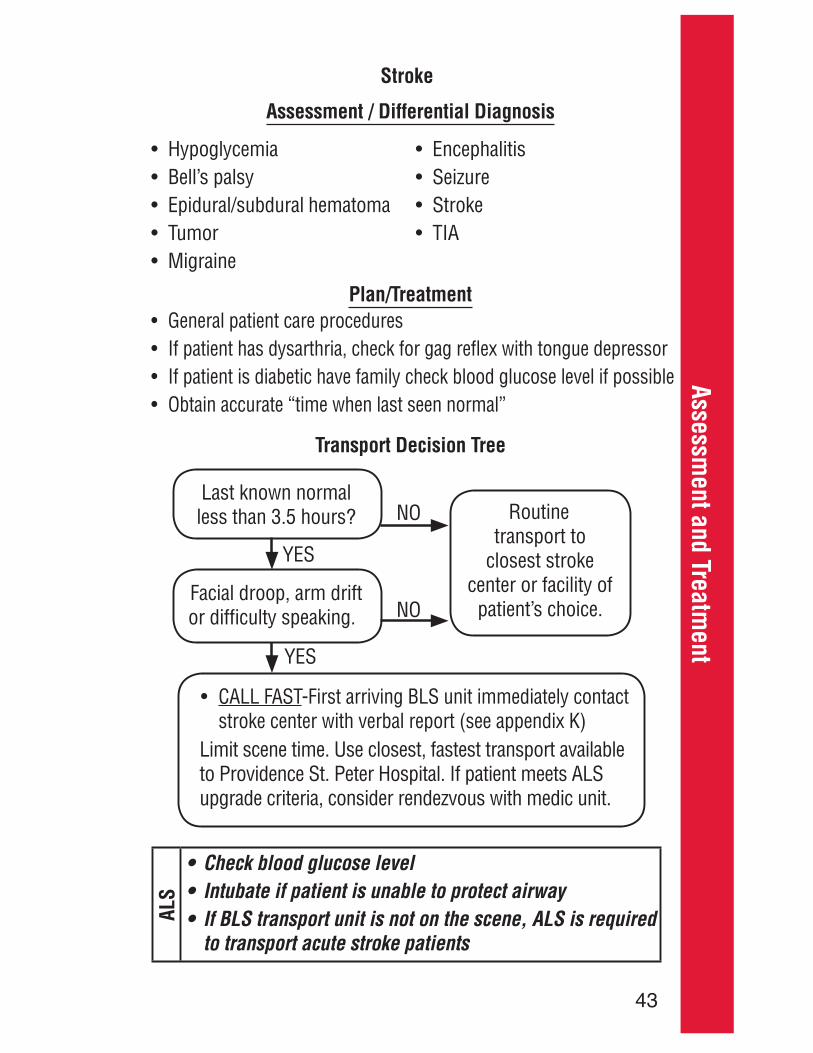
entStroke
Assessment / Differential Diagnosis
Plan/Treatment
Transport Decision Tree
ALS
or difficulty speaking.
Routine transport to
closest stroke center or facility of
patient’s choice.
NO
YES
YES
NO

44
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
rescue breathing
Pertinent Objective Findings
paraphernalia
hypoglycemic medications
ALS Upgrade Required For
Assessment / Differential Diagnosis
− Alcohol/acidosis− Epilepsy/electrolytes/endocrine− Insulin (hypo/hyperglycemia)− Overdose− Uremia/underdose− Trauma− Infection− Psychosis− Pump/poison− Stroke/shock
− Cardiac dysrhythmia− Stroke− Hyperventilation − Orthostatic
Unconscious / Syncope

45
Assessment and Treatm
entPlan/Treatment
General patient care proceduresAL
SPe
ds
Unconscious / Syncope

46
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
belts/airbag)
Pertinent Objective Findings
genitalia
distended abdomen
abdominal organs
the ribs
ALS Upgrade Required For
Abdominal Trauma

47
Assessment and Treatm
entAbdominal Trauma
Assessment / Differential Diagnosis
Plan/Treatment
bulky dressing
ALS
Peds as high as the nipple line
pediatric trauma patients
48
Asse
ssm
ent a
nd T
reat
men
tPertinent Subjective Findings
steam/smoke
hazardous materials
respiratory disease
electrical burn
Pertinent Objective Findings
mouth/nose area (BSA)
ALS Upgrade Required For
5 y/o
Burns
49
Assessment and Treatm
entBurns
Assessment / Differential Diagnosis
Plan/Treatment
and then dry patient− Remove burnt or contaminated clothing (that is not melted
to the skin)
percent of BSA affected
blankets to prevent hypothermia
an enclosed space

50
Asse
ssm
ent a
nd T
reat
men
t
ALS
Peds
Burns

51
Assessment and Treatm
entChest Trauma
Pertinent Subjective Findings
belts/airbag)
Pertinent Objective Findings
movement
neck and shoulders
ALS Upgrade Required For
Assessment / Differential Diagnosis
52
Asse
ssm
ent a
nd T
reat
men
tPlan/Treatment
− Apply occlusive dressing and secure on three sides− If patient develops increased respiratory difficulty or tension
affected side
− Splint in position of comfort using patient’s body and
ALS
Peds
Chest Trauma

53
Assessment and Treatm
entExtremity Trauma
Pertinent Subjective Findings
condition(s)
Pertinent Objective Findings
of shock
function or sensation
amputation
ALS Upgrade Required For
Assessment / Differential Diagnosis
Non-accidental trauma

54
Asse
ssm
ent a
nd T
reat
men
tPlan/Treatment
– Distal PMS should be evaluated and recorded before and after splinting.
− Direct pressure to control bleeding
for bleeding− Immobilize
sterile normal saline
time placed in the container− Transport the amputated part to the same hospital as
the patient
ALS
Extremity Trauma
55
Assessment and Treatm
entHead and Neck TraumaPertinent Subjective Findings
belts/helmets)
status
condition(s)
Pertinent Objective Findings
retrograde)
consciousness
− Posturing− Abnormal pupillary
responses
pattern)

56
Asse
ssm
ent a
nd T
reat
men
tALS Upgrade Required For
Assessment / Differential Diagnosis
− Alcohol/acidosis− Epilepsy/electrolytes/
endocrine− Insulin (hypo/hyperglycemia)− Overdose− Uremia/underdose
− Trauma− Infection− Psychosis− Pump/poison− Stroke/shock
Head and Neck Trauma

57
Assessment and Treatm
entPlan/Treatment
at 24 breaths per minute
care not to depress skull fractures− Remove objects impaled in cheeks and pack both inside
and outside to control bleeding
− Irrigate to remove non-impaled foreign substances
patient not to look around
avulsed tooth in saline and attempt to replace in its socket prior to transport
− Do not remove foreign objects
occlusive dressing.
Head and Neck Trauma

58
Asse
ssm
ent a
nd T
reat
men
t
ALS
Head and Neck Trauma
59
Assessment and Treatm
entSpinal Trauma
Pertinent Subjective Findings
region of body affected (dermatome)
condition(s)
substances
belts/helmets)
Pertinent Objective Findings
to injury mental status
ALS Upgrade Required For
Assessment / Differential Diagnosis
60
Asse
ssm
ent a
nd T
reat
men
tPlan/Treatment
− Unsafe scene
paramedics only
blanket roll under the backboard on the patient’s right side
ALS
Peds
Special attention should be placed on obtaining neutral
(shoulders to feet) because of the larger occipital portion of the head.
Spinal Trauma
61
Assessment and Treatm
entPertinent Subjective Findings
of diving platform (MOI for spine injury)
compressions/rescue breathing
hours
− Depth of dive− Ascent rate
− Dyspnea
Pertinent Objective Findings
neurological exam
ears/nose
ALS Upgrade Required For
Submersion Injury
62
Asse
ssm
ent a
nd T
reat
men
tAssessment / Differential Diagnosis
Plan/Treatment
ALS
Peds
Submersion Injury

A-1
Appendix A – ACLS Algorithms
Pulseless Arrest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-2Tachycardia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-4Bradycardia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-5Pediatric Pulseless Arrest. . . . . . . . . . . . . . . . . . . . . . . . . . . . A-6Pediatric Tachycardia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-8Pediatric Bradycardia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-10Neonatal Resuscitation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . A-12
Appendix A – ACLS Algorithms

A-2
Appe
ndix
A –
ACL
S Al
gorit
hms
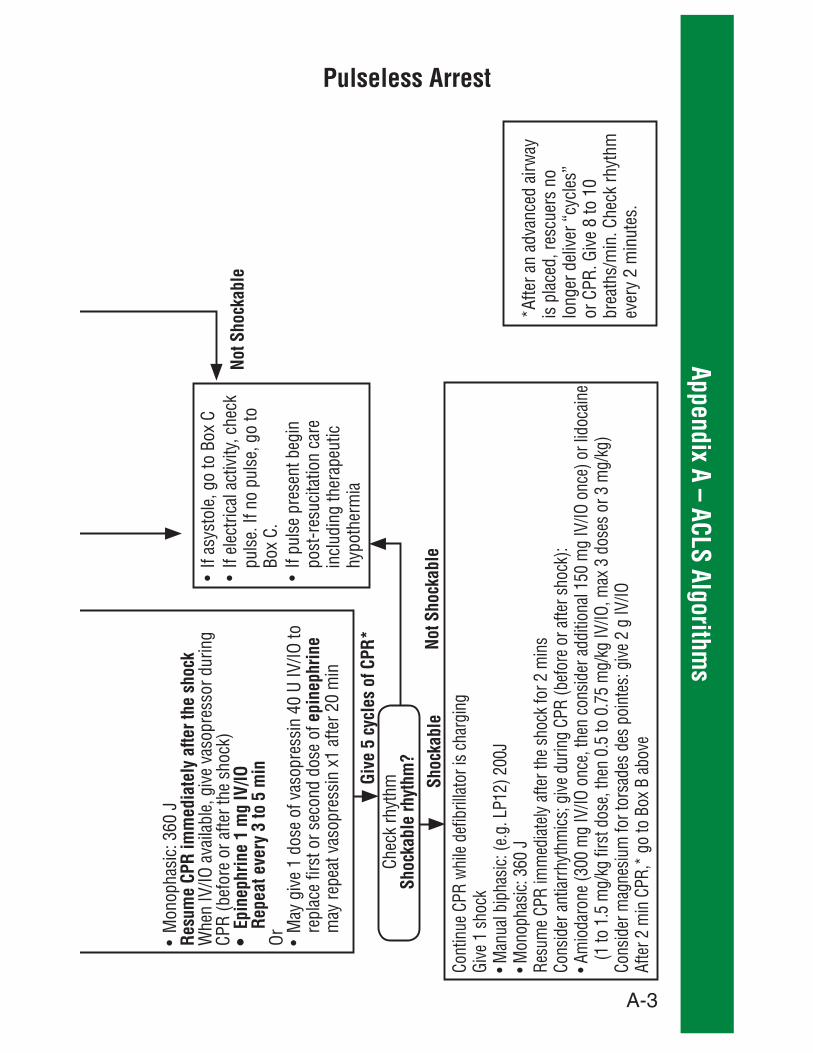
Pulseless Arrest
PULS
ELES
S AR
REST
VF/V
TAs
ysto
le/P
EASh
ocka
ble
Not S
hock
able
AC
Give
5 c
ycle
s of
CPR
*
Give
1 s
hock
Shoc
kabl
e
Shoc
kabl
e rh
ythm
?
Give
2 m
in o
f CPR
*
Shoc
kabl
e
Shoc
kabl
e rh
ythm
?
Shoc
kabl
e rh
ythm
?
Not S
hock
able
B
Resu
me
CPR
imm
edia
tely
for 2
min
Epin
ephr
ine
Re
peat
eve
ry 3
to 5
min
Or M
ay g
ive
1 do
se o
f vas
opre
ssin
40
U IV
/IO to
re
plac
e fir
st o
r sec
ond
dose
of e
pine
phrin
e
Give
1 s
hock
Resu
me
CPR
imm
edia
tely
for
2 m
in
A-3
Appendix A – ACLS Algorithms
Pulseless Arrest
Resu
me
CPR
imm
edia
tely
afte
r the
sho
ck
Re
peat
eve
ry 3
to 5
min
epin
ephr
ine
Give
5 c
ycle
s of
CPR
*
Shoc
kabl
eSh
ocka
ble
rhyt
hm?
Not S
hock
able
Not S
hock
able
A-4
Appe
ndix
A –
ACL
S Al
gorit
hms
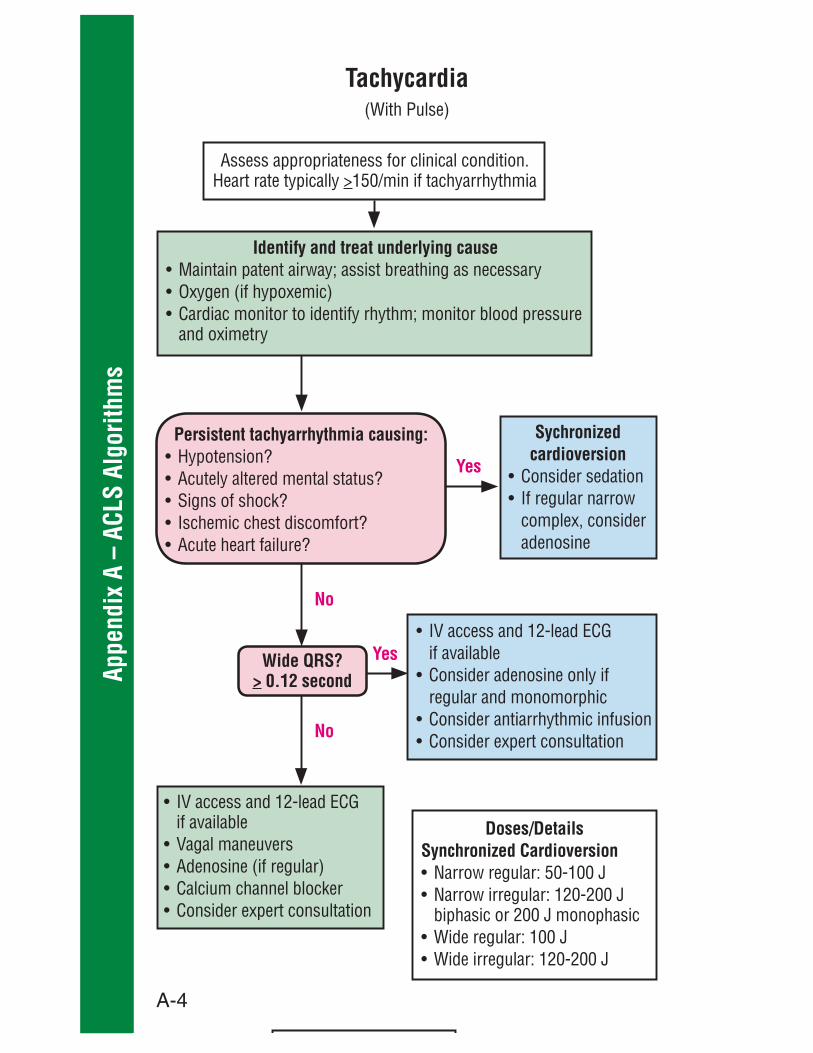
Tachycardia
>
Identify and treat underlying cause
Yes
No
Persistent tachyarrhythmia causing:
No
Wide QRS?> 0.12 second
Sychronized cardioversion
adenosine
Yes
Doses/DetailsSynchronized Cardioversion

A-5
Appendix A – ACLS Algorithms
Monitor and
observe
Bradycardia
Identify and treat underlying cause
Yes
No Persistent bradyarrhythmia causing:
Atropine
orDopamine
orEpinephrine
Consider:

A-6
Appe
ndix
A –
ACL
S Al
gorit
hms
Pediatric Cardiac Arrest
VF/VT Asystole/PEA
Start CPR
Rhythmshockable?
Rhythmshockable?
Rhythmshockable?
Rhythmshockable?
Rhythmshockable?
Go to 6 or 7
CPR 2 min
CPR 2 min
CPR 2 min
CPR 2 min
CPR 2 min
Yes No
Shock
Shock
Shock
Yes
Yes
No
No Yes
Yes
No
No
A
B
D
F
H
I

A-7
Appendix A – ACLS Algorithms
Shock Energy for Defibrilation
>
Drug TherapyEphinephrine IO/IV Dose:
Amiodarone IO/IV Dose:
Pediatric Cardiac Arrest

A-8
Appe
ndix
A –
ACL
S Al
gorit
hms
Iden
tify
and
treat
und
erly
ing
caus
e
Tach
ycar
dia
dura
tion
Prob
able
Sin
us T
achy
card
ia
Prob
able
Sup
rave
ntric
ular
Tac
hyca
rdia
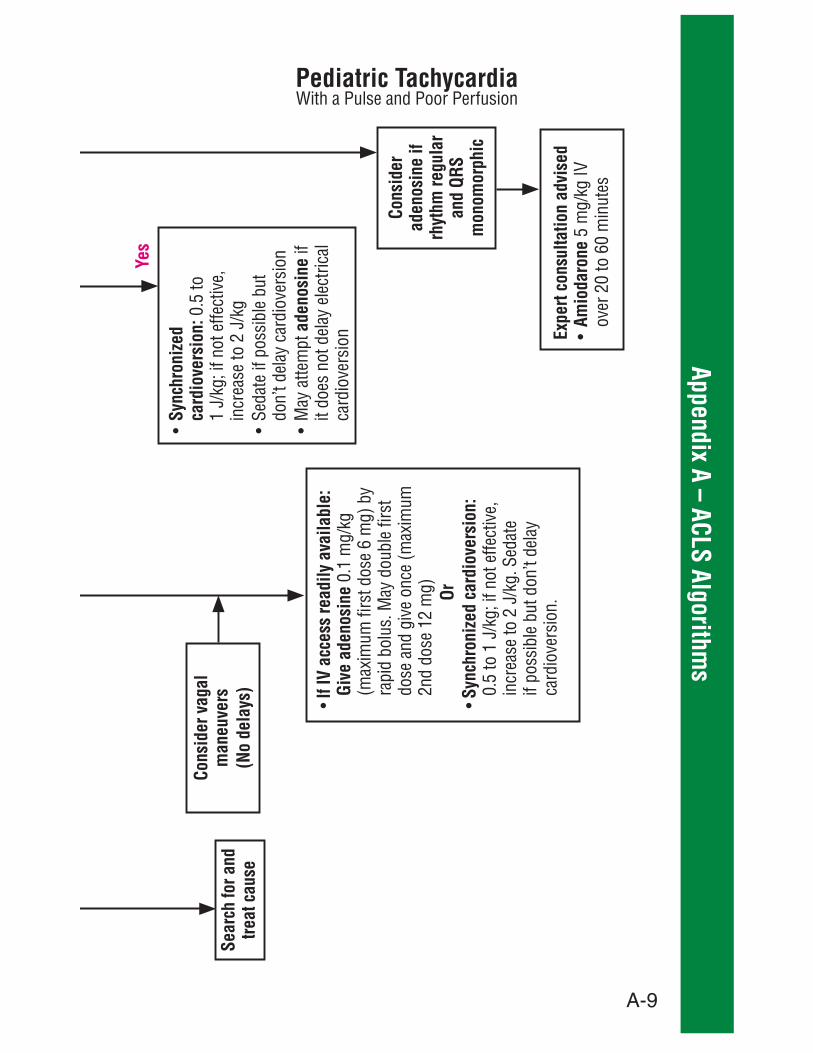
Pediatric Tachycardia
No
Card
iopu
lmon
ary
com
prom
ise
A-9
Appendix A – ACLS Algorithms
Sync
hron
ized
ca
rdio
vers
ion:
0.5
to
aden
osin
e it
does
not
del
ay e
lect
rical
Expe
rt co
nsul
tatio
n ad
vise
dAm
ioda
rone
Cons
ider
vag
al
man
euve
rs
(No
dela
ys) If IV
acc
ess
read
ily a
vaila
ble:
Gi
ve a
deno
sine Or
Sync
hron
ized
car
diov
ersi
on:
Pediatric Tachycardia
Sear
ch fo
r and
tre
at c
ause
Cons
ider
ad
enos
ine
if rh
ythm
regu
lar
and
QRS
mon
omor
phic
Yes

A-10
Appe
ndix
A –
ACL
S Al
gorit
hms
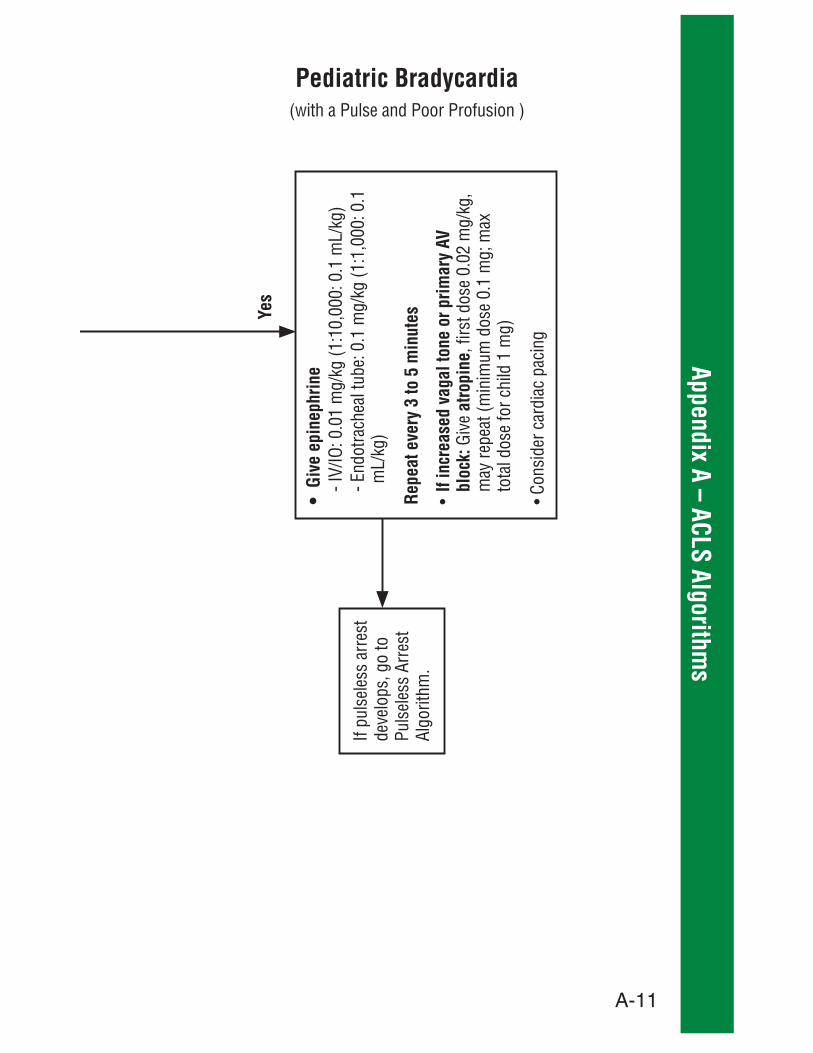
Pediatric Bradycardia
Perfo
rm C
PR
Yes
No
No
Iden
tify
and
treat
und
erly
ing
caus
e
A-11
Appendix A – ACLS Algorithms
Repe
at e
very
3 to
5 m
inut
es
If in
crea
sed
vaga
l ton
e or
prim
ary
AV
bloc
k:
atro
pine
Puls
eles
s Ar
rest
Pediatric Bradycardia
Yes

A-12
Appe
ndix
A –
ACL
S Al
gorit
hms
Neonatal Resuscitation
Term
ges
tatio
n?Br
eath
ing
or c
ryin
g?Go
od to
ne?
Labo
red
brea
thin
g or
per
sist
ent
cyan
osis
?Rout
ine
care
Yes,
sta
yw
ith m
othe
r
No
Yes
No
War
m, c
lear
airw
ay if
nec
essa
ry,
dry,
stim
ulat
e
HR b
elow
100
,ga
spin
g, o
r apn
ea?
PPV,
Spo
, mon
itorin
g
Birth
30 s
ec
60 s
ec
Clea
r airw
aySp
o 2, m
onito
ring
Cons
ider
BiP
AP®
HR b
elow
100
?No
Yes
Yes
No

A-13
Appendix A – ACLS Algorithms
Neonatal Resuscitation
Yes
HR b
elow
60?
Take
ven
tilat
ion
corr
ectiv
e st
eps
Cons
ider
intu
batio
nCh
est c
ompr
essi
ons
Coor
dina
te w
ith P
PV
HR b
elow
60?
IV e
pine
phrin
e
Post
resu
scita
tion
care
Take
ven
tilat
ion
corr
ectiv
e st
eps
Intu
bate
if n
o ch
est r
ise!
Cons
ider
NoNo
Yes

A-14
Appe
ndix
A –
ACL
S Al
gorit
hms

B-1
Appendix B – BLS transport to Nearest ALS (Policy 27)Policy purposeTo ensure a mechanism for providing patients with the most rapid availability of ALS measures
Policy statementIn the event BLS is on scene with a patient requiring ALS upgrade, and the ALS unit has a prolonged response time, BLS personnel will stabilize the patient and:
1. Contact the responding ALS unit(s) to arrange for one of the following:a. Transport to a rendezvous point, orb. If a rendezvous with the ALS unit would take longer than
the transport to the hospital, consult the incoming ALS unit, then transport to the nearest hospital.
2. The ALS unit will be responsible for:a. Deciding the proper course of action (1.a. or 1.b. above)b. Calling base station to inform the base station physician
of decision if the ALS patient is going to be transported BLS (1.b. above)
3. Transporting unit will be responsible for calling the receiving facility to provide patient information
Appendix B – BLS Transport to Nearest ALS (Policy 27)
C-1
Appe
ndix
C –
Chi
ldbi
rth1. Perform risk assessment for field delivery:
a) If contractions are between 2 and 5 minutes apart, transport to the nearest facility
b) If contractions are greater than 5 minutes apart, transport to the patient’s hospital of choice
c) If contractions are less than 2 minutes apart, patient feels urge to push or have a bowel movement or the baby is crowning, plan for a field delivery unless contraindicated below:
position and expedite transport
unless the baby is crowning
unless the baby is crowning. If the decision to deliver in the field is made, call for an additional medic unit and plan to transport after the first child is delivered.
was told by her physician not to deliver vaginally, expedite transport, even if baby is crowning
2. If birth is not imminent then transport to appropriate facility:a) Place patient in left lateral recumbent position and provide
supplemental oxygen as neededb) Provide early notification of the patient’s status to
receiving facility
a) Prepare a delivery location (consider the modesty of the patient, the privacy of the family and the safety of the unborn child)
the delivery of the child
Appendix C – Childbirth

C-2
Appendix C – Childbirthnarrow, moves too easily and is top-heavy
b) Gather equipment and supplies:
regulators, etc.)
and ready
a) When the patient feels she needs to push, encourage her to push for as long as possible (usually 10 sec), then take a deep breath and bear down again
part of a gloved hand to prevent the baby from delivering too fast
membrane by pinching and remove it from baby’s head
nose using a bulb syringe. If meconium is present in
suction as necessary.
the back of the baby’s neck and feeling for the umbilical cord wrapped around the neck. If the cord is present, gently slip it over the head (cord could wrap multiple times).
baby’s head, apply both umbilical clamps and cut the cord between the two clamps
Appendix C – Childbirth
C-3
Appe
ndix
C –
Chi
ldbi
rthissues dealt with, have mother deliver the baby’s body:
the other as the shoulders prepare to deliver
gentle pressure to guide the head posteriorly (relative to mother) first, to deliver the anterior shoulder and then guide the head anteriorly to deliver the posterior
usually follows quickly
the baby and cut the cord in between the clamps
using towels
and cover to keep warm
status to facility of choice or nearest hospital
delivery of the baby. When the patient says she feels the
to the hospital with the patient
with blood.
nurse her baby to assist in controlling postpartum hemorrhaging.
Appendix C – Childbirth

D-1
Appendix D – Death in Field (DIF) and paramedics may withhold or terminate resuscitation
cases or if in doubt at any time, resuscitation should begin
d) Incineration
g) Evisceration of brain or heart
valid (signed)
resuscitation if the patient has been diagnosed with a terminal illness and there is a reasonable indication that the patient and his or her family did not want to have cardiopulmonary resuscitation performed.
personnel should perform all resuscitative measures regardless of any documentation.
start breathing with airway positioning
of trauma shall be determined to be dead in the field and not transported if:
Appendix D – Death in Field (DIF)

D-2
Appe
ndix
D–
Deat
h in
Fie
ld (D
IF)
the head and is pulseless and apneic after opening airway
trauma to the chest and is pulseless and apneic after opening airway
c) The patient presents in asystole
6. Medical cardiac arrest – The patient in non-traumatic (medical) cardiac arrest shall be determined to be dead in the field and not transported after consultation with the supervising physician in any of the following circumstances:a) The patient’s initial presenting rhythm is asystole and
no previous resuscitative efforts were initiatedb) At any time during the resuscitation, the patient stays
in an asystolic or agonal rhythm that is refractory to ACLS measures
c) After full ACLS resuscitative measures have been instituted and the patient’s ETCO2 remains at 10 mmHg or below for 10 minutes
d) A patient in PEA does not respond to appropriate ACLS measures
victims of electrocution, lightning and drowning should have resuscitative efforts begun and be transported to the nearest hospital unless the supervising physician orders otherwise
whether to discontinue or withhold resuscitation
Appendix D – Death in Field (DIF)

D-3
Appendix D – Death in Field (DIF)b) All cases of non-resuscitation will have an ECG strip
documenting the cardiac rhythm, with the time and date recorded on the strip. If using a LP 12, attach it to the patient care report
c) All consultations with the supervising physician will be documented, including the time, physician’s name and instructions
Appendix D – Death in Field (DIF)
E-1
Appe
ndix
E –
Infa
nt T
rans
fer
Appendix E – Infant Transfer
paid and volunteer firefighters and fire department-certified
72 hours old).
transfer custody of a child whether the child is less than 72 hours old as determined to a reasonable degree of medical certainty.
is a parent of the child.
identifying information as a condition of transferring custody of the newborn, and shall attempt to protect the anonymity of the parent.
history or information by providing the parent with the approved
department-approved pamphlet, which includes referral information regarding “adoption options, counseling, appropriate medical and emotional aftercare services, domestic
Procedures for infant transfers include:
accordance with protocols and provide the appropriate level
transferring person is a parent of the child, without requesting name, social security number or other identifying information.
E-2
Appendix E – Infant TransferAppendix E – Infant Transfer
time of birth of the child to ascertain whether the child is a
immediately try to attain completion of the family medical history questionnaire. When that is completed, the parent will be given the pamphlet with referral information, but such information shall be provided even if the parent refuses to provide any medical history or information.
statute, the qualified person shall attempt to obtain family medical history and address the immediate health and safety
9. In the event that employees or members of the department who do not meet the definition of qualified person are asked to accept transfer of a newborn from a parent, or any child from any person, they must ask the transferor to wait a few minutes while they summon a qualified person by

F-1
Appe
ndix
F –
Man
dato
ry R
epor
ting
Crite
ria
required to report:
1) When there is reasonable cause to believe that abandonment, abuse, financial exploitations, or neglect of a vulnerable adult has occurred, mandated reporters shall immediately report to
2) If there is reason to suspect that sexual or physical assault has occurred, mandated reporters shall immediately report to the appropriate law enforcement agency (city police or
reasonable cause to believe that a child or adult dependent or developmentally disabled person has suffered abuse or neglect,
Reporting procedure
answering service will provide referral to the appropriate agency
or herself;
or his or her family’s home.
Appendix F – Mandatory Reporting Criteria

F-2
Appendix F – Mandatory Reporting Criteria
of adults can take several forms:
engages in self-destructive behavior)
noncommunicative, depressed or nonresponsive
participate in family or community activities
abuse in children can be different from in adults and vary somewhat with the age of the child.
of children can take several forms:
Appendix F – Mandatory Reporting Criteria

F-3
Appe
ndix
F –
Man
dato
ry R
epor
ting
Crite
ria1. Insure safety and provide medical aid as needed to save or
assist the child2. If child is clearly dead, do not move the body
stay at the scene or not)
of speakers
abilities and scene observations
interest or knowledge of sexual acts, reports or inappropriate touching, etc.
diaper rash; hungry; underweight; lack of food, formula or care; parent or child use of drugs or alcohol, etc.
Appendix F – Mandatory Reporting Criteria cont.

G1
Appendix G – Medical Abbreviations
G1
Appendix G – Medical Abbreviations
> Greater than
syndrome
immunodeficiency syndrome
Appearance, Pulse, Grimace, Activity, Respirations
unresponsive
isolation
c̄ With
2
pulmonary disease
resuscitation
accident
confinement (due date for delivery)
symptoms
2 End-tidal carbon dioxide
FemaleFx Fractureg Grams
GI Gastrointestinal
throat
illness
diabetes mellitusIM Intramuscular

G-2
Appe
ndix
G –
Med
ical
Abb
revi
atio
ns
Appendix G – Medical Abbreviations
distention
hypertrophy Male
(helicopter)
mEq Milliequivalentmg MilligramMI Myocardial infarction
ml Millilitermm Millimeter
diabetes mellitus
2
Onset, Provoker(s), Quality, Radiation, Severity, Time
contraction
tachycardia
PE Patient examPupils equal, round and reactive to light with accommodation
psi Pounds per square inch
supraventricular tachycardia
Pt Patient
contractionPx Painq Everyqd Every dayqh Every hourqid Four times a dayqod Every other day

G-3
Appendix G – Medical Abbreviations
Appendix G – Medical Abbreviations
s̄ Without
S Allergies, Medications, Pertinent past history Last oral intake, Events leading to 911 call
2
WPW Wolff-Parkinson-White syndrome
H-1
Appe
ndix
H
I-1
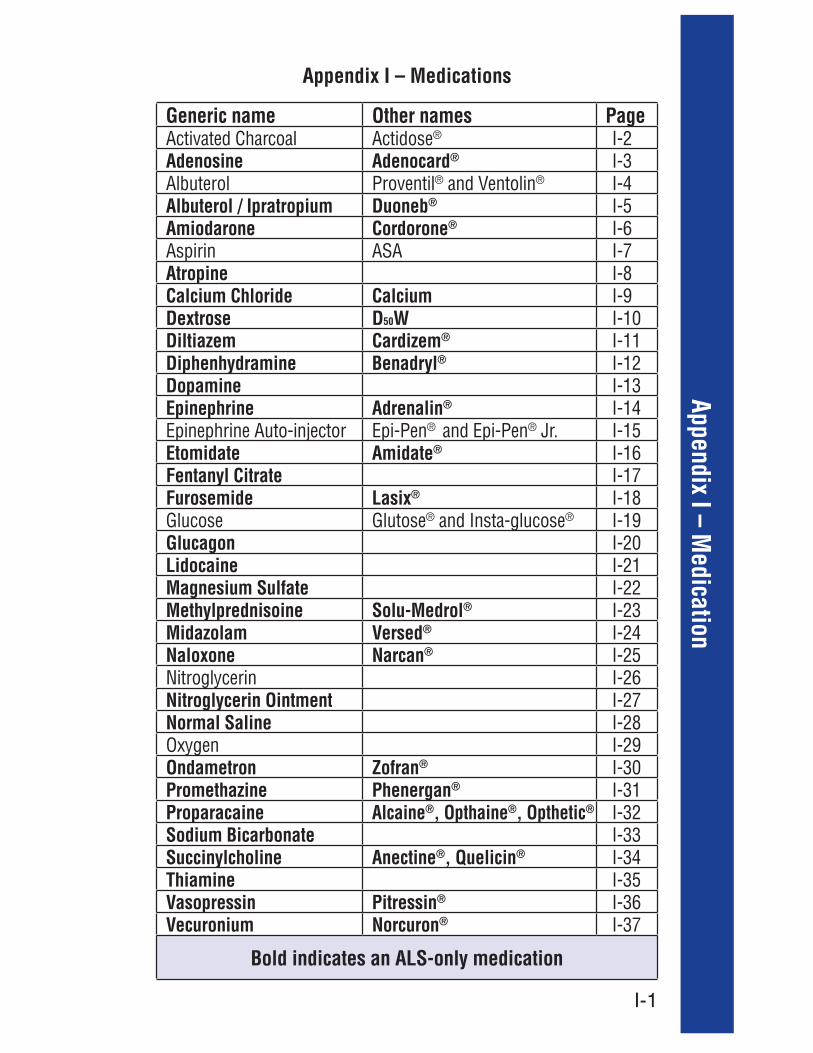
Appendix I – Medication
Generic name Other names PageActivated Charcoal Actidose® I-2Adenosine Adenocard® I-3Albuterol Proventil® and Ventolin® I-4Albuterol / Ipratropium Duoneb® I-5Amiodarone Cordorone® I-6Aspirin ASA I-7Atropine I-8Calcium Chloride Calcium I-9Dextrose D50W I-10Diltiazem Cardizem® I-11Diphenhydramine Benadryl® I-12Dopamine I-13Epinephrine Adrenalin® I-14Epinephrine Auto-injector Epi-Pen® and Epi-Pen® Jr. I-15Etomidate Amidate® I-16Fentanyl Citrate I-17Furosemide Lasix® I-18Glucose Glutose® and Insta-glucose® I-19Glucagon I-20Lidocaine I-21Magnesium Sulfate I-22Methylprednisoine Solu-Medrol® I-23Midazolam Versed® I-24Naloxone Narcan® I-25Nitroglycerin I-26Nitroglycerin Ointment I-27Normal Saline I-28Oxygen I-29Ondametron Zofran® I-30Promethazine Phenergan® I-31Proparacaine Alcaine®, Opthaine®, Opthetic® I-32Sodium Bicarbonate I-33Succinylcholine Anectine®, Quelicin® I-34Thiamine I-35Vasopressin Pitressin® I-36Vecuronium Norcuron® I-37
Bold indicates an ALS-only medication
Appendix I – Medications
I-2
Appe
ndix
I –
Med
icat
ion
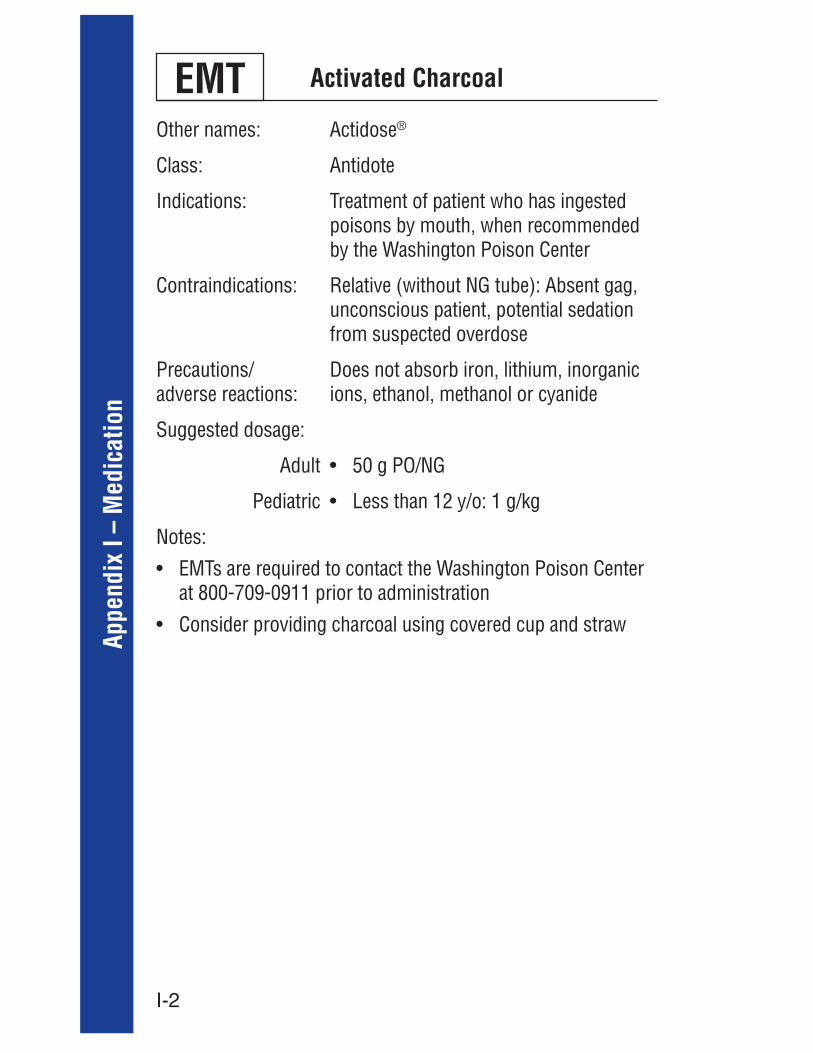
Activated CharcoalEMTOther names: Actidose®
Class: Antidote
Indications: Treatment of patient who has ingested poisons by mouth, when recommended by the Washington Poison Center
Contraindications: Relative (without NG tube): Absent gag, unconscious patient, potential sedation from suspected overdose
Precautions/ adverse reactions:
Does not absorb iron, lithium, inorganic ions, ethanol, methanol or cyanide
Suggested dosage:
Adult
Pediatric
Notes:
at 800-709-0911 prior to administration

I-3
Appendix I – Medication
Adenosine
Other names: Adenocard®
Class: Anti-dysrhythmicIndications: Narrow complex SVTContraindications: Wide complex tachycardia, second-
syndrome; caution in patients with asthma and COPD
Precautions/ adverse reactions:
Severe bradycardia, VF, VT, afib,
bronchospasm; will cause temporary
and a general transient ill feelingSuggested dosage:
Adult
Pediatric
may repeat with 12 mg after 1-2 minutes
I-4
Appe
ndix
I –
Med
icat
ion
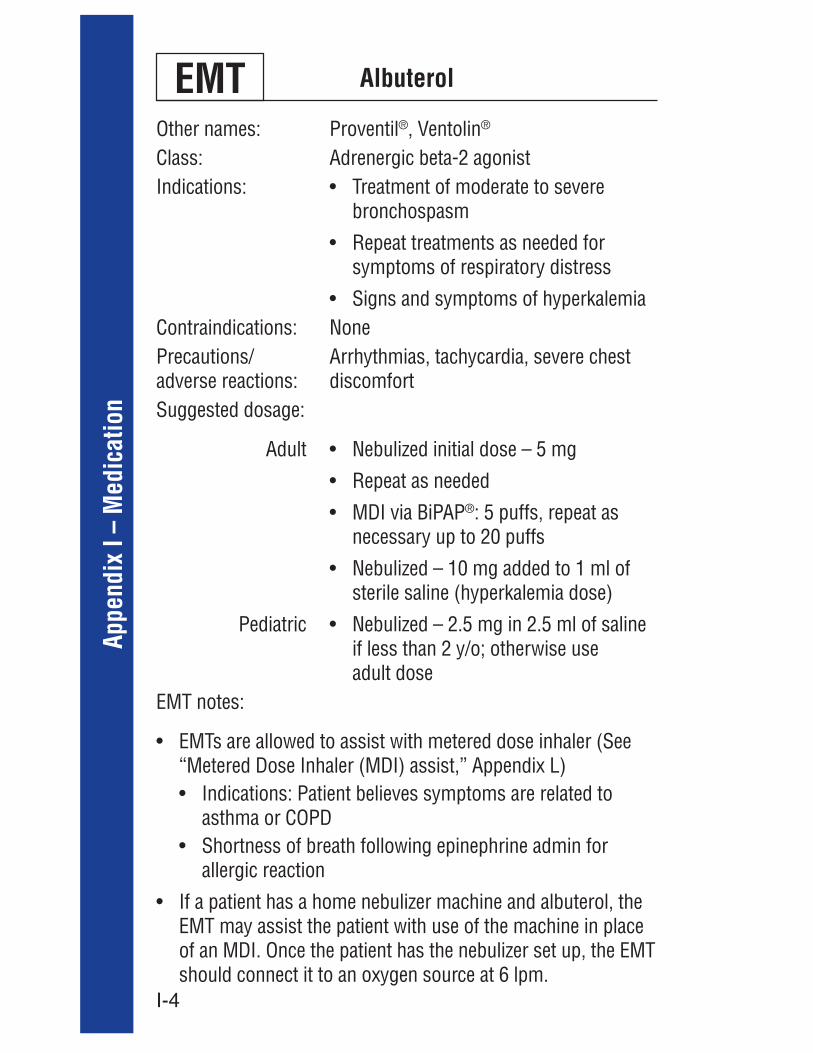
AlbuterolEMTOther names: Proventil®, Ventolin®
Class: Adrenergic beta-2 agonist Indications:
bronchospasm
symptoms of respiratory distress
Contraindications: NonePrecautions/ adverse reactions:
Arrhythmias, tachycardia, severe chest discomfort
Suggested dosage:
Adult
Pediatric
®: 5 puffs, repeat as necessary up to 20 puffs
if less than 2 y/o; otherwise use adult dose
asthma or COPD
allergic reaction
should connect it to an oxygen source at 6 lpm.

I-5
Appendix I – Medication
Albuterol / Ipratropium
Other names: Duoneb® , Combivent®
Class:bronchodilator
Indications: Initial treatment of moderate to severe bronchospasm
Contraindications: None
Precautions/ adverse reactions:
Arrhythmias, tachycardia, severe chest discomfort
Suggested dosage:
Adult/pedsrepeat as needed for persistent respiratory distress
®: 5 puffs

I-6
Appe
ndix
I –
Med
icat
ion
Amiodarone
Other names: Cordarone®
Class: Anti-dysrhythmic
Indications: For patients with recurrent VF or pulseless VT after one dose of lidocaine
Contraindications:
Precautions / adverse reactions:
None
Suggested dosage:
Adult
Pediatric

I-7
Appendix I – Medication
Aspirin EMTOther names: Generic
Class: Anti-platelet, non-narcotic analgesic, non-steroidal anti-inflammatory, antipyretic
Indications: Signs and/or symptoms of acute coronary syndrome
Contraindications: Allergy to Asprin
Precautions/ adverse reactions:
None
Suggested dosage:
Adult
Pediatric

I-8
Appe
ndix
I –
Med
icat
ion
Atropine
Other names: Generic
Class: Anticholinergic parasympatholytic
Indications:
Contraindications: HR: greater than 180
Precautions / adverse reactions:
Tachycardia, nausea, ventricular ectopy
Suggested dosage:
Adult
Pediatric
needed every 3-5 minutes up to 0.04 mg/
1.0 mg IVP, then2.0 mg IVP, then5.0 mg IVP, then10.0 mg IVP
Escalate the dose every 10 minutes until respiratory secretions dry up
repeat once
0.5 mg) for pre-medication in RSI

I-9
Appendix I – Medication
Calcium Chloride 10%
Other names: Generic
Class: Electrolyte replacementIndications:
arrhythmia thought to be secondary
supervising physician for administration regimen)
respiratory depression
Contraindications: Ventricular fibrillation, digitalis toxicity, hypercalcemia
Precautions/ adverse reactions: bradycardia, dysrhythmias, cardiac arrest;
can potentiate toxicity of digitalis on the heart
Suggested dosage:
Adult
Pediatricmin slow IVP)
tape for dose
I-10
Appe
ndix
I –
Med
icat
ion
Dextrose 50%
Other names: D50WClass: CaloricIndications: Symptomatic hypoglycemia Contraindications: Hyperglycemia, delirium tremensPrecautions/ adverse reactions:
Pre-treat hypoglycemic alcoholic patients with thiamine
Suggested dosage:
Adult
Pediatric
blood glucose remains less than
(1:1 D50W:NS)
(1:4 D50W:NS) for neonate
resuscitation tape for dosing
I-11
Appendix I – Medication
Diltiazem
Other names: ®
Class:Indications:
Contraindications: Wide complex SVT
Known WPW disease
Pulmonary congestionPrecautions/ adverse reactions:
Hypotension, arrhythmias, CHF
Suggested dosage:
Adult
Pediatric
unsuccessful after 10 mins follow-up 10 mg IVP
pediatric pts
I-12
Appe
ndix
I –
Med
icat
ion
Diphenhydramine
Other names: ®
Class: AntihistamineIndications:
Contraindications: Anticholinergic poisoningPrecautions/ adverse reactions:
Drowsiness, dilated pupils, tinnitus, dry mouth
Suggested dosage:
Adult
Pediatric

I-13
Appendix I – Medication
Dopamine
Other names: GenericClass: VasopressorIndications:
syndromes
and symptomsContraindications: Ventricular fibrillation, tachy-
dysrhythmias, pheochromocytomaPrecautions/ adverse reactions: with peripheral vascular disease.
Reduce dose by half in patients with significant renal disease.
Suggested dosage:
Adult
Pediatric
250 ml NS
greater than 90 mmHg

I-14
Appe
ndix
I –
Med
icat
ion
Epinephrine
Other names: Adrenalin®
Class: AdrenergicIndications:
due to anaphylactic respiratory distress or
VT, pediatric bradycardia
Contraindications: NonePrecautions/ adverse reactions:
artery disease
Suggested dosage:
Adult
Pediatric
® or IV or SVN, 0.3-0.5 mg (3-5 ml 1:10,000)
- Drip IV, IO 4-8 mcg/min (1 mg in 250ml of saline = 4 microgram/ml)
length-based resuscitation tape)

I-15
Appendix I – Medication
Epinephrine Auto-injector Epi-Pen®, Epi-Pen® Jr. EMT
Other names:
Epinephrine
Class: AdrenergicIndications:
symptoms of anaphylaxis:
(hypotension) OR difficulty swallowing (throat edema), and consents to treatment
® Jr. is indicated in patients
(66 pounds)
Precautions/ adverse reactions:
coronary artery disease
Suggested dosage:
Adult
Pediatric
® ® Jr.

I-16
Appe
ndix
I –
Med
icat
ion
Etomidate
Other names: Amidate®
Class: General anestheticIndications:
succinylcholine during RSI
Contraindications: None in emergent settingPrecautions/ adverse reactions: nausea, vomitingSuggested dosage:
Adult
Pediatric
given over 30-60 seconds; may repeat
occur within 2 minutes
10 y/o
I-17
Appendix I – Medication
Fentanyl Citrate
Other names: GenericClass: Narcotic analgesicIndications: Severe painContraindications:
head injuryPrecautions/ adverse reactions: with evidence of alcohol or sedative
intoxication
ill patients
who use narcotics chronicallySuggested dosage:
Adult
Pediatric
300 mg
consult supervising physician for repeat dosing
Notes:
supervising physician is mandatory
Sp02to the patient report
I-18
Appe
ndix
I –
Med
icat
ion
Furosemide
Other names: ®
Class:Indications:
120 mmHg) with volume overloadContraindications: Hepatic coma, suspected electrolyte
disturbances, hypotension, patients with allergies to sulfonamides
Precautions/ adverse reactions:
Efficiency goes down in patients with renal failure
Suggested dosage:
Adult
Pediatric
slow IVP
resuscitation tape
I-19
Appendix I – Medication
Glucose
Other names: Glutose®, Insta-glucose®
Class: CaloricIndications: Patient with an altered or decreased
of diabetesContraindications:
unable to swallowPrecautions/ adverse reactions:
Use caution to prevent aspiration of the glucose paste
Suggested dosage:
Adult
PediatricNotes:
EMT
I-20
Appe
ndix
I –
Med
icat
ion
Glucagon
Other names: GenericClass: EndocrineIndications:
establish IV access
relatively contraindicated by age or
++
supervising physician for dosing regimen)
supervising physician for dosing regimen)
Contraindications: NonePrecautions/ adverse reactions: may return
Zofran® concurrentlySuggested dosage:
Adult
Pediatricmin (max 1 mg/dose)

I-21
Appendix I – Medication
Lidocaine
Other names: GenericClass: Anti-dysrhythmicIndications:
uncertain type
Contraindications:atrial fibrillation with rapid aberrant ventricular response
Precautions/ adverse reactions: 70 y/o or if patient presents with acute
jaundice
Suggested dosage:
Adult
Pediatric

I-22
Appe
ndix
I –
Med
icat
ion
Magnesium Sulfate
Other names: GenericClass: Anti-convulsant, mineralIndications:
Contraindications:treated with paralytic agents
Precautions/ adverse reactions:
Will lower calcium; observe for hypotension, paralysis and CNS depression; will tend to reverse the effect of digitalis, pulmonary edema
Suggested dosage:
Adult
Pediatric
ml given IV over 4 minutes
20 ml given rapid IVP
2 g diluted with NS to 20 ml given IV over 5-20 minutes

I-23
Appendix I – Medication
Methylprednisolone
Other names: ®
Class: GlucorticoidIndications:
severe bronchospasm
Contraindications: Known hypersensitivity to the product or its constituents
Precautions/ adverse reactions:
None in emergent setting
Suggested dosage:
Adult
Pediatric(12 years
or less)

I-24
Appe
ndix
I –
Med
icat
ion
Midazolam
Other names: Versed®
Class:Indications:
Contraindications: None in emergent settingPrecautions/ adverse reactions: especially when mixed with narcotics,
Suggested dosage:
Adult
Pediatric
mins to max of 10 mg
mg prn
or IN
3 min to max 5 mg
I-25
Appendix I – Medication
Naloxone
Other names: Narcan®
Class: Narcotic antagonistIndications: Narcotic overdoseContraindications: Neonate with possible drug dependencePrecautions/ adverse reactions: overdosesSuggested dosage:
Adult
Pediatrictape for proper weight-based dosing

I-26
Appe
ndix
I –
Med
icat
ion
Nitroglycerin EMTOther names: Nitrotab, Nitrostat®
Class: Vasodilator, anti-anginalIndications:
cardiac event
Hypertensive pulmonary edemaContraindications: ® or Cialis® or
® in past 48 hours
Tachycardia (HR>100/min)
Precautions/ adverse reactions:
Hypotension, headache
Suggested dosage:
Adult
Pediatric
100 mmHg systolic

I-27
Appendix I – Medication
Nitroglycerin Ointment
Other names: Nitrobid®
Class: Vasodilator, anti-anginalIndications: Symptoms suggestive of ACS or CHF
cardiac event
Contraindications: ® or Cialis® or ® in past 48 hours
Tachycardia (HR>100/min)
Precautions/ adverse reactions:
Hypotension (additive effect with
tachycardia, headacheSuggested dosage:
Adult
Pediatric
Apply as soon as possible along with first sublingual nitro)
remains above 100 mmHg, increase to 2 inches
above 100 mmHg after 10 minutes, increase to 2 inches

I-28
Appe
ndix
I –
Med
icat
ion
Normal Saline
Other names:Class: Isotonic crystalloidIndications:
Contraindications: Pulmonary edemaPrecautions/ adverse reactions: of fluid overloadSuggested dosage:
Adult
Pediatric
I-29
Appendix I – Medication
OxygenEMTFIRST RESPONDER
Other names: GenericClass:Indications:
respiratory distress, respiratory arrestContraindications: NonePrecautions/ adverse reactions:
None
Suggested dosage:

I-30
Appe
ndix
I –
Med
icat
ion
Other names: Zofran®
Class: Anti-emeticIndications: Nausea, vomitingContraindications:Precautions/ adverse reactions:
Caution in liver disfunction
Suggested dosage:
Adult
Pediatric
Ondansetron

I-31
Appendix I – Medication
Promethazine
Other names: Phenergan®
Class: Anti-emeticIndications:
of medications such as fentanyl and glucagon
Contraindications: Age less than 2 yearsPrecautions/ adverse reactions:
Dystonia, sedation; consider lower end of dosing range in elderly patients
Suggested dosage:
Adult
Pediatric
elderly), repeat once as needed; always dilute in 10 ml saline
up to adult dose
I-32
Appe
ndix
I –
Med
icat
ion
Proparacaine
Other names: Alcaine® and Opthetic® and Opthaine®
Class: AnestheticIndications: Temporary ophthalmic anesthesia for
eye injuriesContraindications: NonePrecautions/ adverse reactions:
None
Suggested dosage:
Adult
Pediatric
I-33
Appendix I – Medication
Sodium Bicarbonate
Other names: GenericClass: Electrolyte (acid/base)Indications:
with calcium and albuterol (consult supervising physician)
Contraindications: Hypertension, hypertensive pulmonary edema
Precautions/ adverse reactions:
None
Suggested dosage:
Adult
Pediatricresuscitation tape
I-34
Appe
ndix
I –
Med
icat
ion
Succinylcholine
Other names: Anectine® and Quelicin®
Class:Indications: Intubation in patients with intact gag
reflex or whose degree of pharyngeal muscle tone prevents intubation
Contraindications:history of malignant hyperthermia, pseudocholinesterase deficiency, organophosphate poisoning
Precautions/ adverse reactions:
of throat cancer, non-arrested croup or epiglottitis
myasthenia gravis, muscular
(burns or other in previous three to 10 days)
Suggested dosage:
Adult
Pediatricresuscitation tape

I-35
Appendix I – Medication
Thiamine
Other names:Class: VitaminIndications: Hypoglycemic patients with a history
of alcoholism; given prior to the administration of dextrose
Contraindications: NonePrecautions/ adverse reactions:
None
Suggested dosage:
Adult
Pediatric

I-36
Appe
ndix
I –
Med
icat
ion
Vasopressin
Other names: Pitressin®
Class: EndocrineIndications: VF, pulseless VTContraindications: None in the setting of cardiac arrestPrecautions/ adverse reactions:
None
Suggested dosage:
Adult
Pediatric
minutes as substitute for epinephrine in cardiac arrest
I-37
Appendix I – Medication
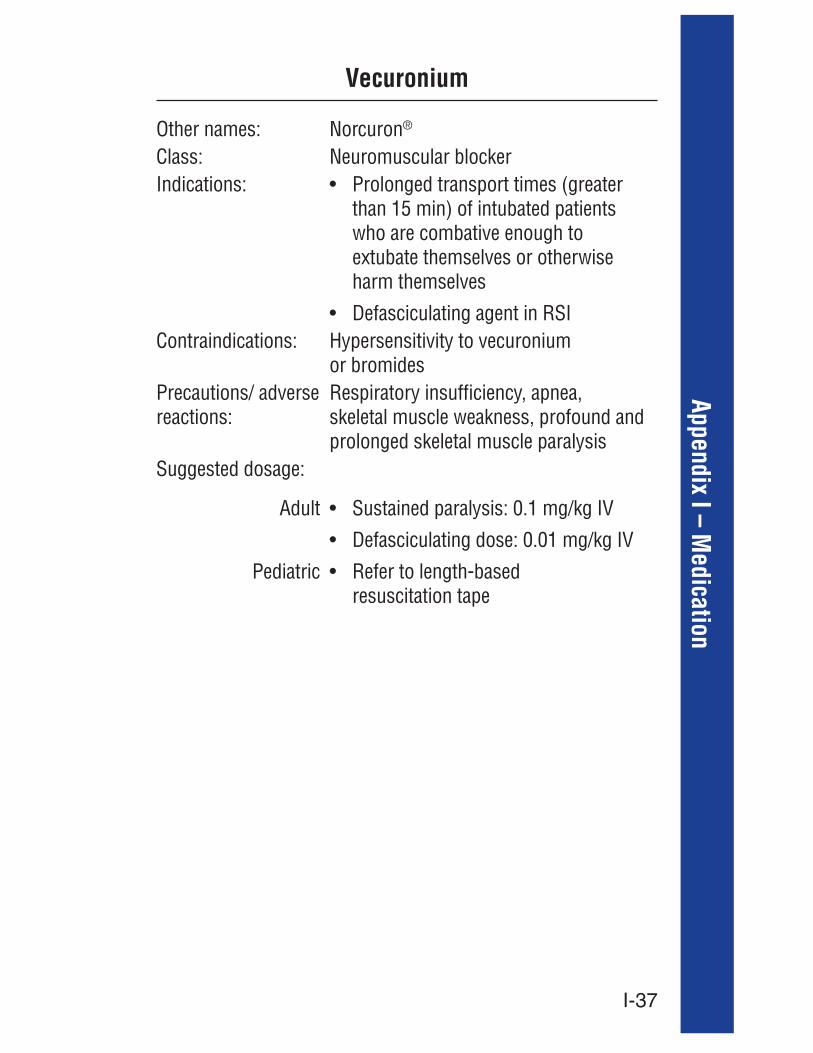
Vecuronium
Other names: Norcuron®
Class:Indications:
than 15 min) of intubated patients who are combative enough to extubate themselves or otherwise harm themselves
Contraindications: Hypersensitivity to vecuronium or bromides
Precautions/ adverse reactions:
Respiratory insufficiency, apnea,
Suggested dosage:
Adult
Pediatricresuscitation tape
I-38
Appe
ndix
I –
Med
icat
ion

J-1
Appendix J – Other Tools for EMS Providers
Appendix J – Other Tools for EMS ProvidersI. Normal vital signs
AGE PULSE RESPIRATIONSBLOOD PRESSURE
AVERAGE SYSTOLIC
AVERAGE DIASTOLIC
Newborn (1-28 days)
110-150 60 80 46
3 months 110-140 40 90 606-12 months 100-140 40 90 60
1 year 100-140 26 90 602 years 90-100 20 98 64
3-5 years 80-100 20 100 7010 years 70-100 16 114 60
Adolescent 70-100 12 118 60Adult 60-100 12 120 70
II. Rule of Nines for burn victims
AREA OF THE BODY ADULT CHILD9 percent 18 percent
Entire arm, each 9 percent 9 percentChest 9 percent 9 percentAbdomen 9 percent 9 percent
9 percentpercent9 percent
Front of leg, each 9 percent Entire leg is 14 percent9 percent
Genitalia 1 percent 1 percent
III. APGAR score for newborns
after delivery.
Clinical sign 0 points 1 point 2 pointsAppearancePulse Absent Above 100Grimace No response Grimaces CriesActivity Some flexion Active motionRespiratory Absent Slow, irregular Good cry
J-2
Appe
ndix
J –
Oth
er T
ools
for E
MS
Prov
ider
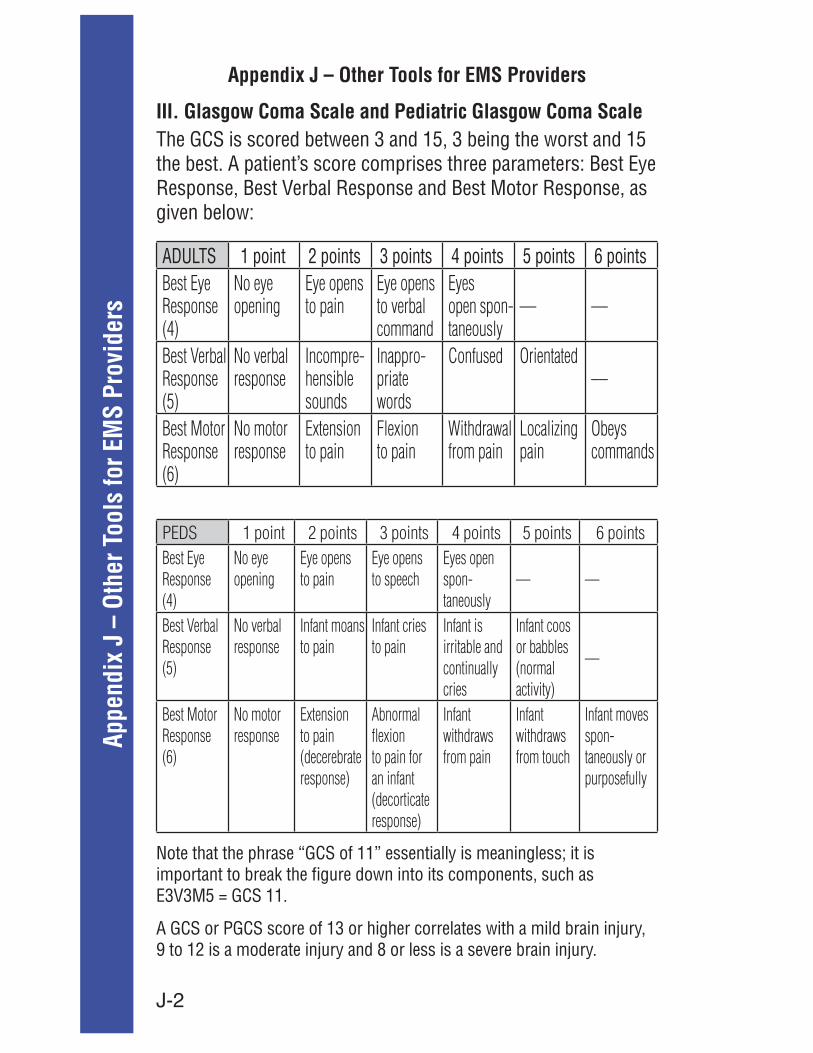
sIII. Glasgow Coma Scale and Pediatric Glasgow Coma ScaleThe GCS is scored between 3 and 15, 3 being the worst and 15
given below:
1 point 2 points 3 points 4 points 5 points 6 pointsBest Eye Response (4)
No eye opening
Eye opens to pain
Eye opens to verbal command
Eyes open spon-taneously
–– ––
Best Verbal Response (5)
No verbal response
Incompre-hensible sounds
Inappro-priate words
Confused Orientated––
Best Motor Response (6)
No motor response
Extension to pain
Flexion to pain
Withdrawal from pain
Localizing pain
Obeys commands
PEDS 1 point 2 points 3 points 4 points 5 points 6 pointsBest Eye Response (4)
No eye opening
Eye opens to pain
Eye opens to speech
Eyes open spon-taneously
–– ––
Best Verbal Response (5)
No verbal response
Infant moans to pain
Infant cries to pain
Infant is irritable and continually cries
Infant coos or babbles (normal activity)
––
Best Motor Response (6)
No motor response
Extension to pain (decerebrate response)
Abnormal flexion to pain for an infant (decorticate response)
Infant withdraws from pain
Infant withdraws from touch
Infant moves spon-taneously or purposefully
A GCS or PGCS score of 13 or higher correlates with a mild brain injury, 9 to 12 is a moderate injury and 8 or less is a severe brain injury.
Appendix J – Other Tools for EMS Providers
K-1
Appendix K – Pre-hospital Verbal Comm
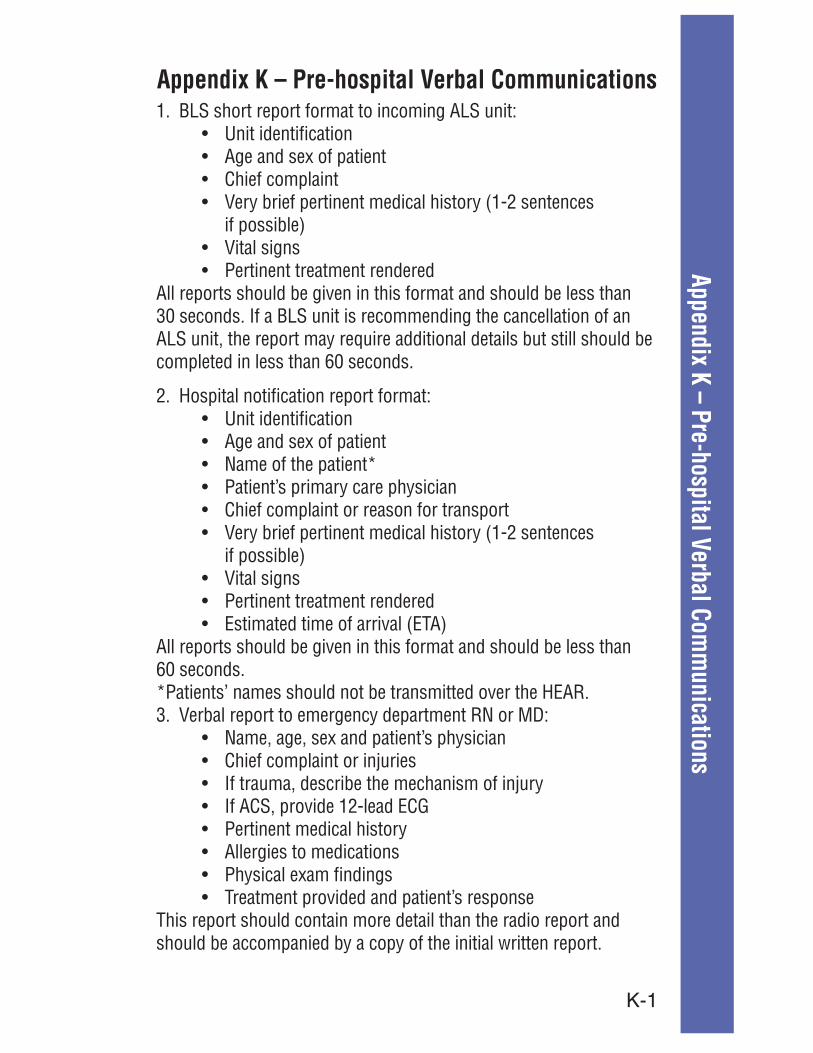
unicationsAppendix K – Pre-hospital Verbal Communications
if possible)
All reports should be given in this format and should be less than
completed in less than 60 seconds.
2. Hospital notification report format:
if possible)
All reports should be given in this format and should be less than 60 seconds.
This report should contain more detail than the radio report and should be accompanied by a copy of the initial written report.
L-1
Appe
ndix
L –
Ski
llsACS Management. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-2Airway – Difficult Airway Management . . . . . . . . . . . . . . . . . . . . . . . . . . . L-12 Insertion of Nasopharyngeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-32 Insertion of Oropharyngeal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-35Bag Valve Mask Ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-6Bleeding Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-8Blood, Obtaining a Specimen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-34Cannulation – Internal Jugular Intravenous . . . . . . . . . . . . . . . . . . . . . . . L-21 Femoral Intravenous . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-16 Peripheral Intravenous . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-40 Subclavian Intravenous . . . . . . . . . . . . . . . . . . . . . . . . . . . L-52Capnography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-9Cricothyrotomy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-10Defibrillation – Automated External Defibrillation. . . . . . . . . . . . . . . . . . . . L-3 Automated External Defibrillator Algorithm . . . . . . . . . . . . L-5 Manual . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-28ECG set-up, 12-lead . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-14Electrical Cardioversion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-13Epi-Pen® Administration. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-15Glucometery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-18Helmet Removal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-19Hypothermia (Therapeutic). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-20Immobilization – Joint . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-26 Long Bone. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-27 Pelvic Wrap Splint. . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-38 Spinal Immobilization Decision Tool . . . . . . . . . . . . . . . L-48 Spinal Immobilization Decision Algorithm . . . . . . . . . . L-49 Spinal Immobilization . . . . . . . . . . . . . . . . . . . . . . . . . . L-50 Traction Device . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-54Introsseous Infusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-26Intravenous Line Setup. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-28Intubation – Nasogastric . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-34Intubation – Orotracheal. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-22Melker® Cricothyrotomy Kit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-31Metered Dose Inhaler (MDI) Assist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-29Mouth-to-Mask Ventilation with Supplemental Oxygen . . . . . . . . . . . . . . . . L-30Needle Thoracentesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-33Nasogastric. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-31Oxygen Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-37Orotracheal Intubation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-36Pericardiocentesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-39Pulse Oximetry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-41Rapid Sequence Induction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-42Restraint Guidelines – Patients with Altered LOC. . . . . . . . . . . . . . . . . . . . . L-44Restraint Guidelines – Patients who are Violent/Combative. . . . . . . . . . . . . L-46Suctioning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-53Transcutaneous Pacing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-55Ventilation Mechanical . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-56Ventilation Non-Invasive BiPAP® . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . L-57
Appendix L – Skills
L-2
Appendix L – SkillsProvider level:
Indications:− Uncomfortable “pressure,” “fullness,”
“squeezing” or discomfort in the chest or neck that lasts more than a few minutes, or that goes away and comes back
− Discomfort that radiates to shoulders, neck or arms
− Chest discomfort with lightheadedness, fainting, sweating, nausea or shortness of breath
-OR-Patient exhibits any of the following signs or symptoms believed to be of cardiac origin:− Atypical chest, stomach or abdominal discomfort − Unexplained nausea (without vomiting)
or lightheadedness (not vertigo) without chest discomfort
− Shortness of breath and difficulty breathing (without chest discomfort)
− Unexplained anxiety, weakness or fatigue− Palpitations, cold sweat or paleness
Contraindications: None
Equipment: DefibrillatorProcedure:
Capture 12-lead prior to moving patient and prior to ALS NTG administration
Attach 12-lead to patient care report Prior to sending 12-lead, include patient name
and age If evidence of STEMI exists, consult base station
physician as early as possible Establish IV access (Appendix L) Administer fentanyl (Appendix I) as appropriate Treat rhythm disturbances as appropriate
(Appendix A)
Acute Coronary Syndrome Management
L-3
Appe
ndix
L –
Ski
llsProvider level:
Indications: Patients 1 > year of age who have confirmed circulatory arrest
Contraindiations: See Death in Field criteria, Appendix DEquipment: DefibrillatorProcedure: 1. Immediately upon arrival, verify respiratory
and circulatory arrest by the absence of consciousness, normal respirations and a carotid pulse.
2. Initiate CPR and resuscitation protocols. If it is an unwitnessed cardiac arrest, perform CPR for 2 minutes before initiating defibrillation protocol.
3. Turn the defibrillator power on and begin a verbal report.
4. Immediately attach the defibrillation pads with
a. If a shock is indicated, immediately charge and deliver a single shock. After the single shock, immediately begin 2 minutes of CPR (see algorithm).*
b. If no shock is indicated, immediately begin 2 minutes of CPR (see algorithm).*
c. After 2 minutes of CPR, reanalyze the rhythmi. If a shock is indicated, immediately charge
and deliver a single shock. After a single shock, begin 2 minutes of CPR.*
ii. If no shock is indicated, immediately check pulse. 1. If no pulse, then begin 2 minutes of
CPR. 2. If a pulse is detected, provide other care
per algorithm.
Automated External Defibrillation
*compression should be continued through charging cycle if possible

L-4
Appendix L – SkillsSpecial patient and pediatric guidelines:
A. Pediatric arrest: For children < 1 year old, verify cardiac arrest and begin effective CPR. DO NOT initiate defibrillation protocol.
B. For children 1 to 8 years use pediatric pads
C. For children 8 years of age and over: Follow adult defibrillation protocols
D. Traumatic arrest: Defibrillation is ineffective in traumatic cardiac arrest. If major blood loss/ trauma is obvious, initiate basic life support. If major blood loss/trauma is NOT obvious, initiate defibrillation protocols.
E. Patients attached to a public access defibrillator (PAD): If EMS Defibrillation providers arrive to find the patient attached to a PAD device, that device should be removed and replaced with the
initiated. This should be accomplished with minimal interruption of CPR.
F. Documentation Submittal: Review of any event in which the defibrillator is attached in cardiac arrest is mandatory. The complete event data and the medical incident report MUST be transmitted to Thurston County Medic One within 4 days of the event.
Automated External Defibrillation

L-5
Appe
ndix
L –
Ski
llsVerify Pulselessness
AED Algorithm
Witnessed Unwitnessed
CPR until ready to defib 2 min CPR
Analyze
2 min CPR
Analyze/shock
- CPR while charging- immediately resume CPR after shock
etc.
1) Compressions 30:2 ventilations2) Asynchronous ventilations every 10 compressions after patient is intubated3) Narrate resuscitation into recorder4) Call 704-2785 to report cardiac arrest (include date, FD, patient name)5) Provide MIR, download to Medic One within 96 hours
L-6
Appendix L – Skills Bag Valve Mask Ventilation
Provider level:
FATS technique (non-trauma patient)

L-7
Appe
ndix
L –
Ski
lls: Two-person bag valve mask
Seated bag valve mask
Bag Valve Mask Ventilation Cont.

L-8
Appendix L – SkillsProvider level:
Bleeding Control
L-9
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications:
hyperventilating
Contraindications: Colormetric devices are not used to monitor non-intubated patients who have spontaneous respirations
Equipment:
2 measuring device® or Nonin®)
Preparation: Assemble necessary equipment
Procedure:
2 in a patient who is in cardiac arrest is not itself an indication for extubation but should cause the paramedic to further investigate the placement of the ETT
Pediatric considerations:
Colormetric devices must be specified for pediatric size and are not used with spontaneously breathing patients
Capnography
L-10
Appendix L – SkillsProvider level: Paramedic
Indications:techniques are not effective
Contraindications: Ventilation possible by less invasive means
Equipment:
Povidone-iodineScalpelTracheal hook
Endotracheal or tracheostomy tubeEschmann styletteMelker Kit
Preparation: Prep neck with Providone-iodineProcedure: Melker approach:
incision in membrane with scapel
angled toward feet, draw back on syringe plunger until air easily aspirated
“floppy” end first
is through skin
against skin
correct placement
Cricothyrotomy

L-11
Appe
ndix
L –
Ski
llsProcedure:
the membrane
and expose membrane
the membrane
handle of scalpel
tracheal hook
stylette into trachea
using Eschmann
and auscultate breath sounds to confirm placement
Pediatric considerations:
Cricothyrotomy Continued

L-12
Appendix L – SkillsProvider level: Paramedic
Indications:orotracheal intubation unlikely to be successful
by each of two providers)
Contraindications: None in the setting of patients needing positive airway control
Equipment:
Catheter Set
Preparation: Gather and prepare proper equipment
Procedure:with or without prism, for situations where cords cannot be visualized
tube using Eschmann stylette
situations where orotracheal intubation or use
Pediatricconsiderations:
Size-appropriate equipment should be used
Difficult Airway Management

L-13
Appe
ndix
L –
Ski
llsProvider level: ParamedicIndications:
Contraindica-tions: needed if heart rate is less than or equal to 150
Equipment:
Preparation:
(sternum/apex)
Procedure:not unconscious
“sync” control button
the patient
clinical condition is critical, go immediately to
according to the tachycardia algorithm (Appendix A)
Pediatric considerations:
Electrical Cardioversion
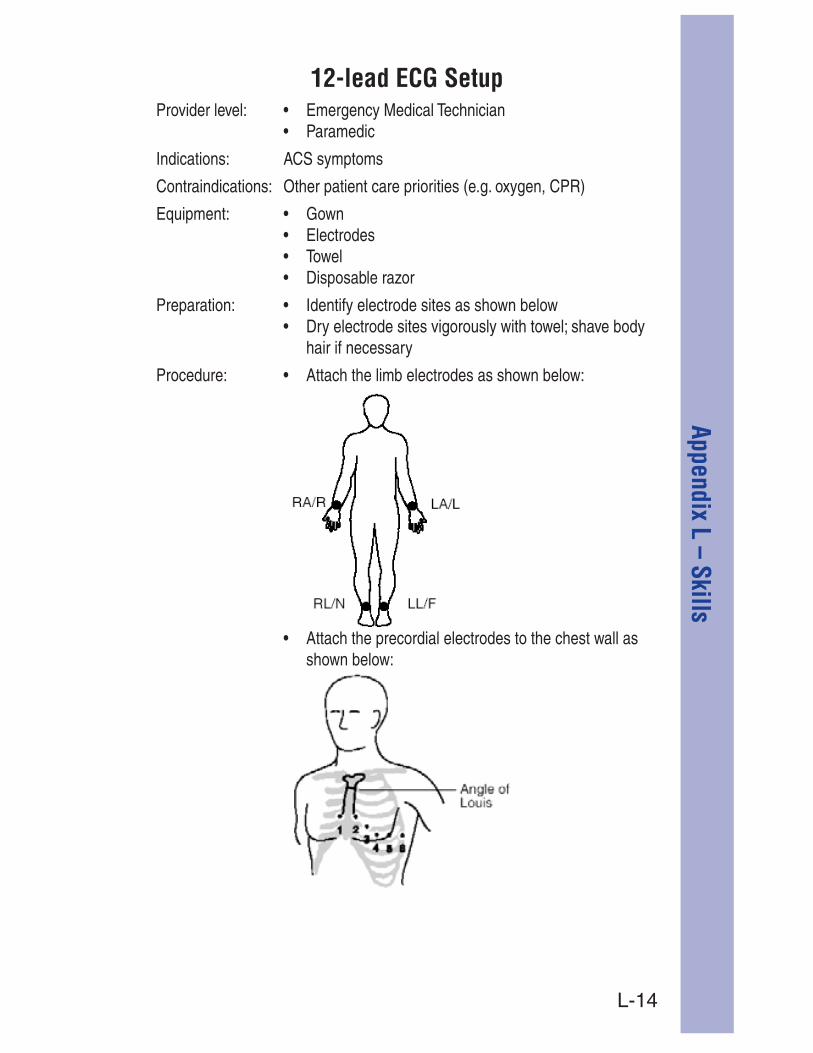
L-14
Appendix L – SkillsProvider level:
12-lead ECG Setup

L-15
Appe
ndix
L –
Ski
llsProvider level:
Epi-Pen® Administration
L-16
Appendix L – SkillsProvider level: Paramedic
Indications: Emergency venous access when peripheral access is not available in the setting of: - Shock - Cardiac arrest
Contraindications:
Equipment:
Preparation:flush tubing
Procedure:
to ensure the catheter is patent
dressing
of attempts and fluid given in the patient care report
Femoral Intravenous Cannulation
L-17
Appe
ndix
L –
Ski
llsPediatric considerations: pediatric patients
be used to administer fluid in infants requiring fluid resuscitation
Volutrol) to prevent unintentional fluid boluses
Femoral Intravenous Cannulation Cont.
L-18
Appendix L – SkillsGlucometery
Provider level:
*Note: Glucometry is a tool that should be used to supplement an ALS assessment; although it can safely be performed by ALS or EMTs. It is not a decision point in determining either upgrade or method of transport. BLS units should not carry glucometers, nor base any decision to upgrade or downgrade a patient based on a blood sugar reading. This skill should be performed under ALS supervision.
L-19
Appe
ndix
L –
Ski
llsProvider level:
Helmet Removal
L-20
Appendix L – SkillsProvider level: ParamedicIndications:
movement after 2 minutesContraindications:
to withhold or terminate resuscitative measuresoC)
Equipment: oC) saline
Preparation: Establish and secure IV if not already established
Procedure: open bolus
measures per protocol
as possible
Pediatric Considerations:
Hypothermia (Therapeutic)

L-21
Appe
ndix
L –
Ski
llsProvider level: ParamedicIndications: Emergency venous access when peripheral access is
not available in the setting of:
Contraindications:Equipment:
Preparation:flush tubing
Procedure:
being cannulated
sternocleidomastoid and clavicle
triangle, lateral to the palpated carotid artery, and advance toward the ipsilateral nipple
the plunger on the syringe until blood is freely aspirated
ensure the catheter is patent
over site
attempts and fluid given in the patient care report
Internal Jugular Intravenous Cannulation
L-22
Appendix L – SkillsPediatricconsiderations: pediatric patients
used to administer fluid in infants requiring fluid resuscitation
Volutrol) to prevent unintentional fluid boluses
Internal Jugular Intravenous Cannulation Cont.
L-23
Appe
ndix
L –
Ski
llsProvider Level: ParamedicIndications: Emergency circulatory access when peripheral access is
not available in the setting of:- Shock- Cardiac Arrest
Contraindications: RELATIVE- Peripheral access is available
Equipment: ®
® ® Needle Set
® or Standard Extension Set
Preparation:
flush tubing
Procedure:® driver and appropriate needle set
® driver from needle set while stabilizing catheter hub
or approved sharps container
®
® catheter with the
continuous infusions where applicable
as directed® site and patient condition
Introsseous Infusion EZ-10®

L-24
Appendix L – SkillsIntrosseous Infusion Cont.
Pediatric Considerations: pediatric patients
be used to administer fluid in infants requiring fluid resuscitation
to prevent unintentional fluid boluses

L-25
Appe
ndix
L –
Ski
llsProvider level:
IV Line Setup
L-26
Appendix L – SkillsProvider level:
Joint Immobilization

L-27
Appe
ndix
L –
Ski
llsProvider level:
Long Bone Immobilization

L-28
Appendix L – SkillsProvider level: ParamedicIndications:
Contraindications:
Equipment:
Preparation: on the patient (sternum-apex)
Procedure:
(through leads or paddles)
charge the defibrillator
the patient
Pediatric considerations:
Manual Defibrillation

L-29
Appe
ndix
L –
Ski
llsProvider level:
Metered Dose Inhaler (MDI) Assist

L-30
Appendix L – SkillsProvider level:
Mouth-to-Mask Ventilation with Supplemental Oxygen

L-31
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications:
activated charcoal
Contraindications:suspected skull fracture
during insertion
Equipment:
Preparation: Gather equipment
Procedure:the ear and then to a midpoint between the xiphoid and the umbilicus
soluble lubricant
continue to insert until the measured depth is reached
air while auscultating over the epigastrium
stomach contents
Pediatric considerations:
In the pediatric patient, use the length-based tape
Nasogastric Tube Insertion (NG Tube)

L-32
Appendix L – SkillsProvider level:
Nasopharyngeal Airway
L-33
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications: Tension pneumothorax
Contraindications: None in setting of tension pneumothorax
Equipment:
Preparation:iodine solution
Procedure:catheter in the mid-clavicular line at the second intercostal space at a 90-degree angle by walking the needle over the top of the third rib
air is freely aspirated, do not advance needle
in place
the catheter
Needle Thoracentesis
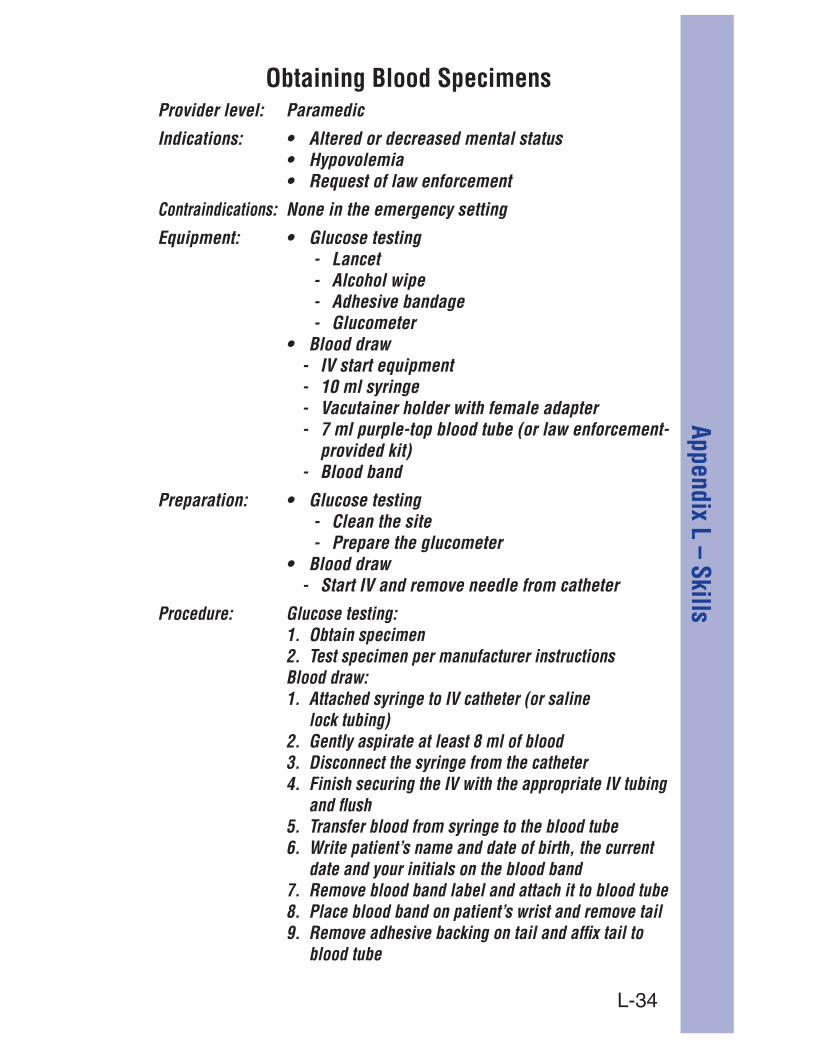
L-34
Appendix L – SkillsProvider level: Paramedic
Indications:
Contraindications: None in the emergency setting
Equipment: - Lancet
- Alcohol wipe - Adhesive bandage - Glucometer
- IV start equipment - 10 ml syringe - Vacutainer holder with female adapter - 7 ml purple-top blood tube (or law enforcement-
provided kit)
Preparation: - Clean the site - Prepare the glucometer
- Start IV and remove needle from catheter
Procedure: Glucose testing:
lock tubing)
and flush
date and your initials on the blood band
blood tube
Obtaining Blood Specimens
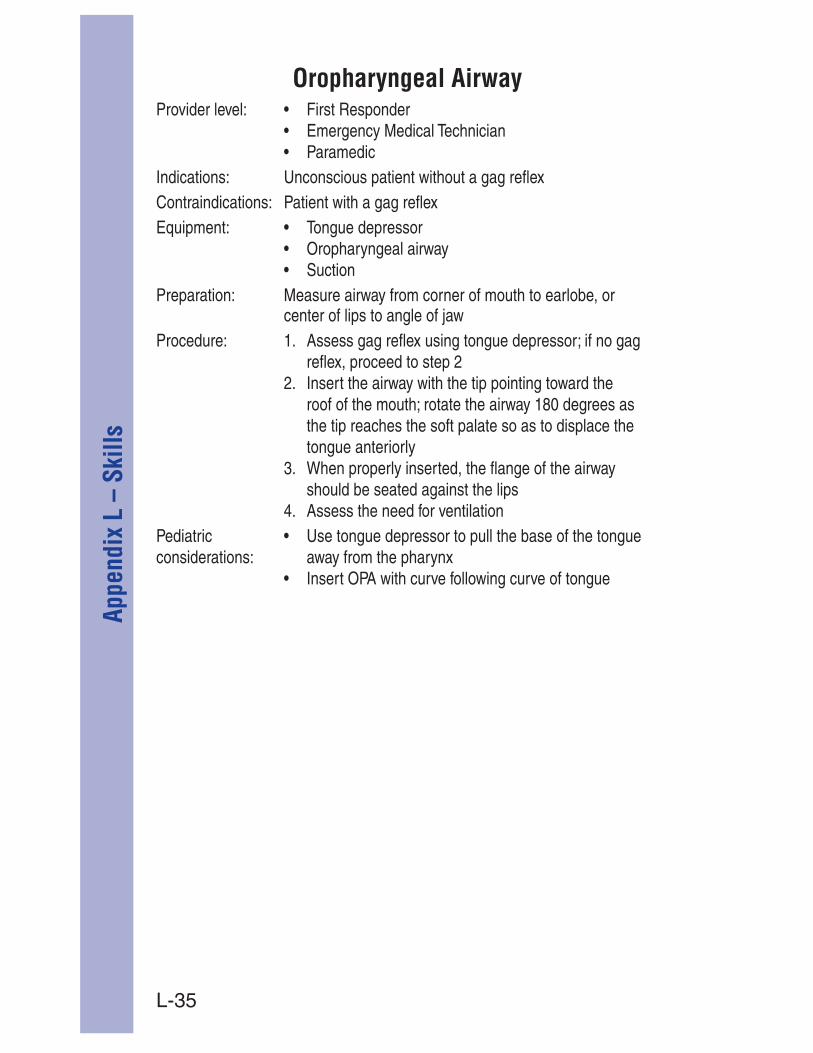
L-35
Appe
ndix
L –
Ski
llsProvider level:
Oropharyngeal Airway

L-36
Appendix L – SkillsProvider level: ParamedicIndications:
Contraindications:
Appendix L)
Equipment:
tube holder
2 monitoring equipment/device
Preparation: Assemble and check required equipment
Procedure:
30 seconds, with re-oxygenation between attempts
(total of four attempts) before implementing alternative
2 monitoring
(every 5 minutes) measurement by the defibrillator
Pediatricconsiderations:
equipment sizes
2 monitoring
Orotracheal Intubation
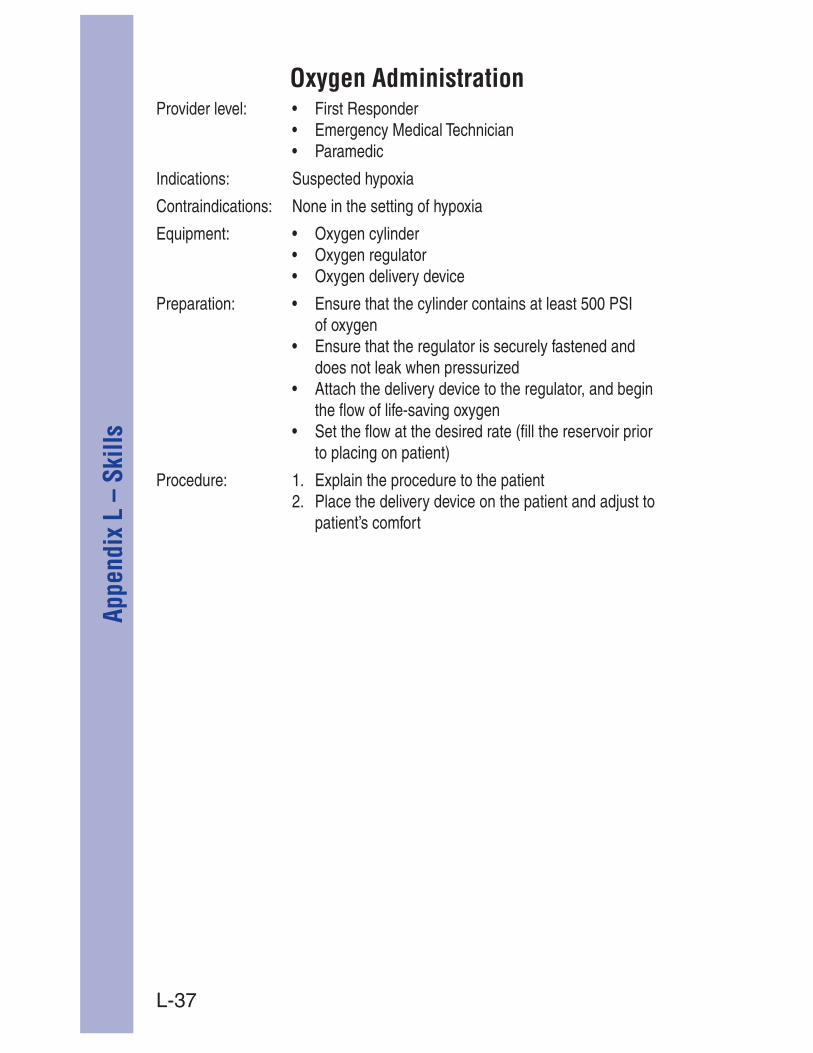
L-37
Appe
ndix
L –
Ski
llsProvider level:
Oxygen Administration
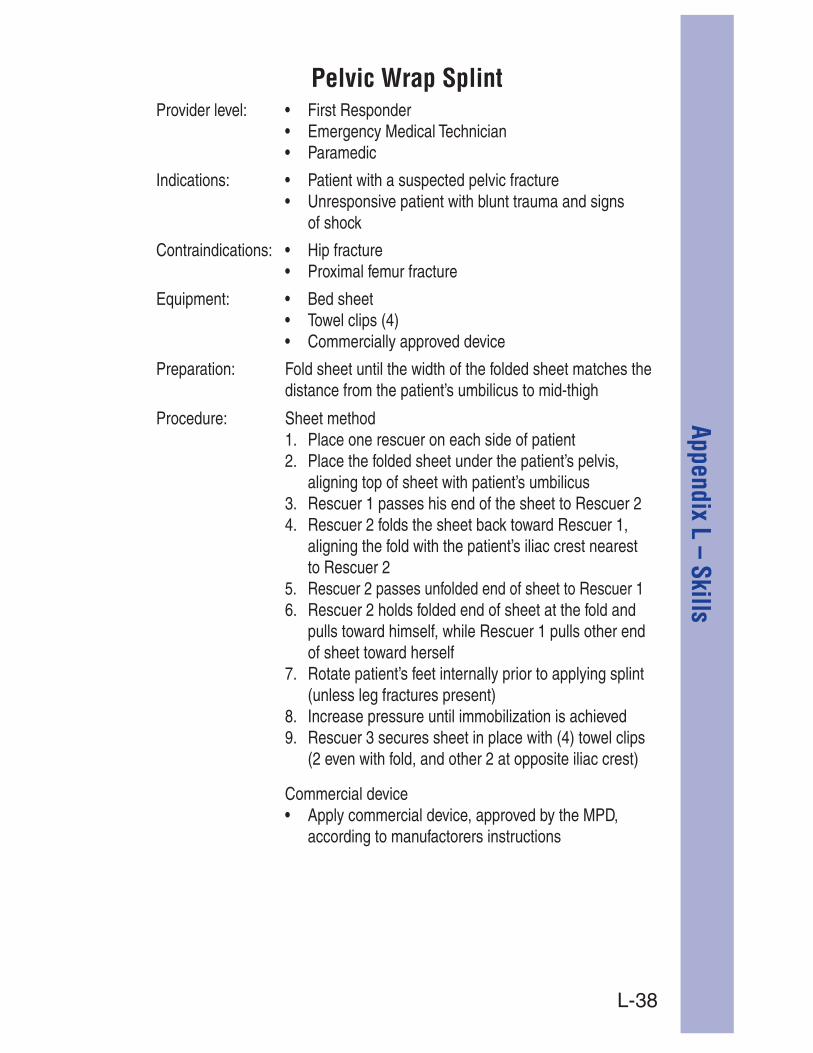
L-38
Appendix L – SkillsProvider level:
Pelvic Wrap Splint
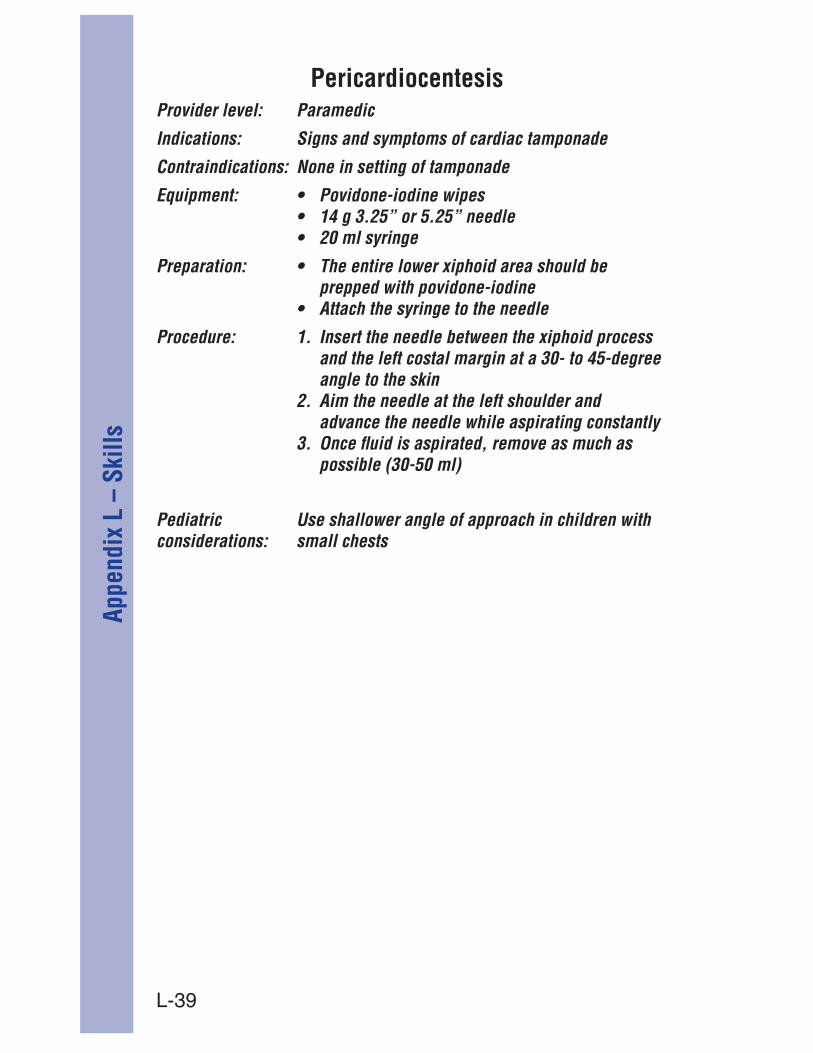
L-39
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications: Signs and symptoms of cardiac tamponade
Contraindications: None in setting of tamponade
Equipment:
Preparation:prepped with povidone-iodine
Procedure:and the left costal margin at a 30- to 45-degree angle to the skin
advance the needle while aspirating constantly
possible (30-50 ml)
Pediatric considerations:
Use shallower angle of approach in children with small chests
Pericardiocentesis

L-40
Appendix L – SkillsProvider level: Paramedic
Indications:
administration
Contraindications: None in emergent setting
Equipment:
or 1,000 ml)
Preparation:saline solution and flush tubing
Procedure:
sample, release the tourniquet
or IV fluid bag
occlusive dressing over the site
receive ALS transport
Pediatricconsiderations: Volutrol) to prevent unintentional fluid boluses
Peripheral Intravenous Cannulation

L-41
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications: Patients with signs of respiratory distress or dyspnea
Contraindications:
Equipment:
Preparation:
Procedure:
reading must correlate with heart rate)
Pediatric considerations: possible (ear lobe, toes, foot, hand)
Pulse Oximetry
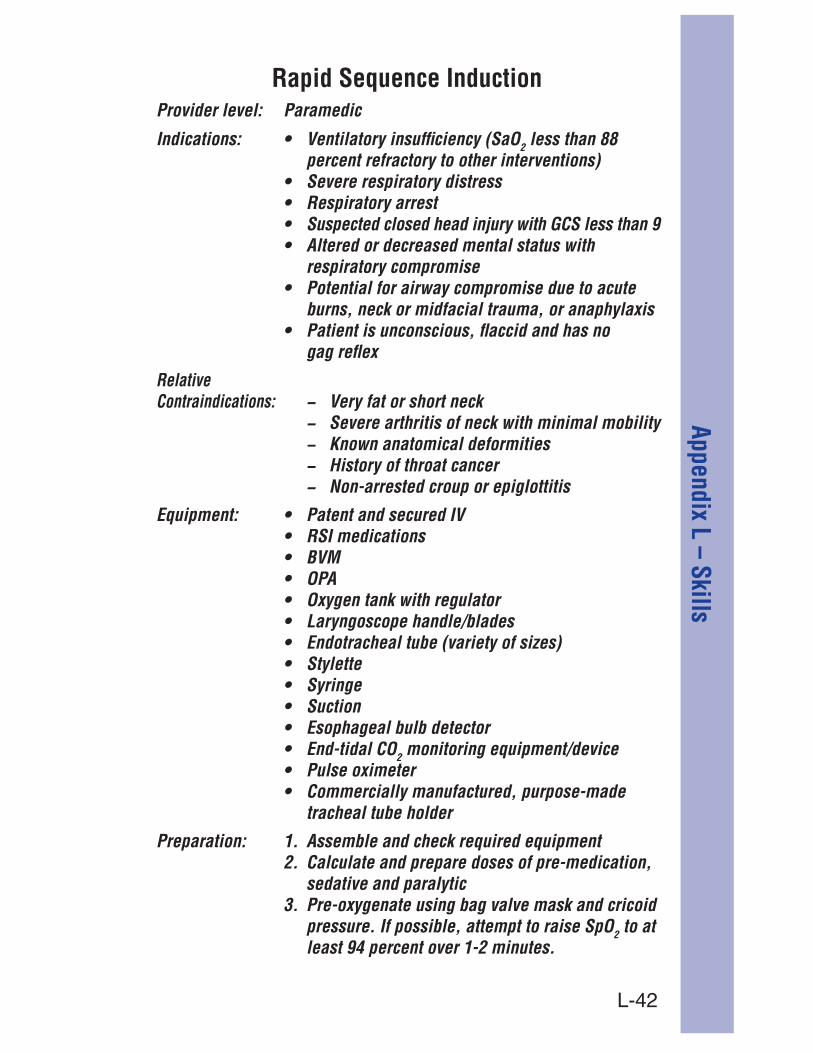
L-42
Appendix L – SkillsRapid Sequence Induction
Provider level: Paramedic
Indications: 2 less than 88 percent refractory to other interventions)
respiratory compromise
burns, neck or midfacial trauma, or anaphylaxis
gag reflex
Contraindications: − Very fat or short neck− Severe arthritis of neck with minimal mobility− Known anatomical deformities
− Non-arrested croup or epiglottitis
Equipment:
2 monitoring equipment/device
tracheal tube holder
Preparation:
sedative and paralytic
2 to at

L-43
Appe
ndix
L –
Ski
llsProcedure:
mg/kg
attempt(s)
immediately following intubation2 monitoring
tracheal tube holder
administer midazolam 5 mg IV, 2 mg IV prn Notify supervising physician as soon as possible
is necessary following intubation, contact the supervising physician to discuss administering
Pediatric considerations:
important as in adults
equipment sizes and calculate drug doses
Rapid Sequence Induction Cont.

L-44
Appendix L – SkillsProvider level:
Restraint Guidelines for Patients with Altered LOC
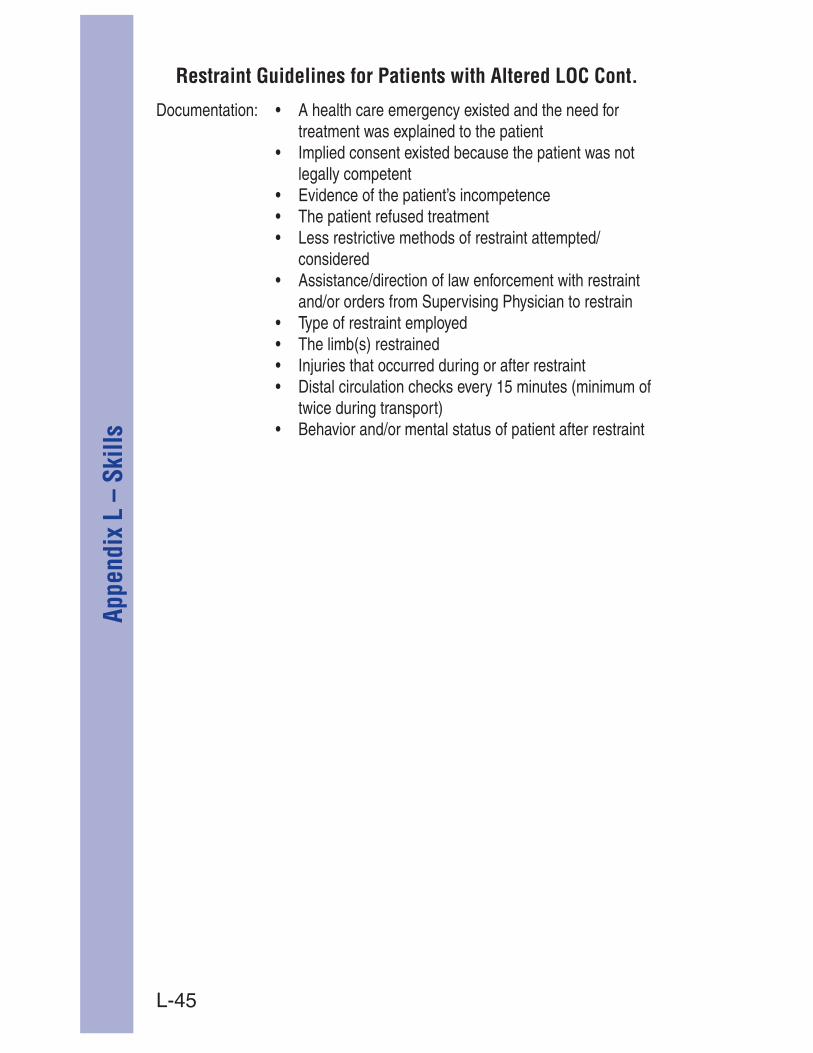
L-45
Appe
ndix
L –
Ski
llsRestraint Guidelines for Patients with Altered LOC Cont.

L-46
Appendix L – SkillsProvider level:
Restraint Guidelines for Violent/Combative Patients

L-47
Appe
ndix
L –
Ski
lls
Chemical restraint:
Indications:– Patients who are so violent and combative that
they cannot reasonably be placed in medical restraint without causing physical injury to the patient or EMS providers, OR
– Patients who continue to struggle after placed in full body medical restraint
IF SITUATION ALLOWS, contact supervising physician for orders for midazolam 10 mg IN or IM
Restraint Guidelines for Violent/Combative Patients Cont.
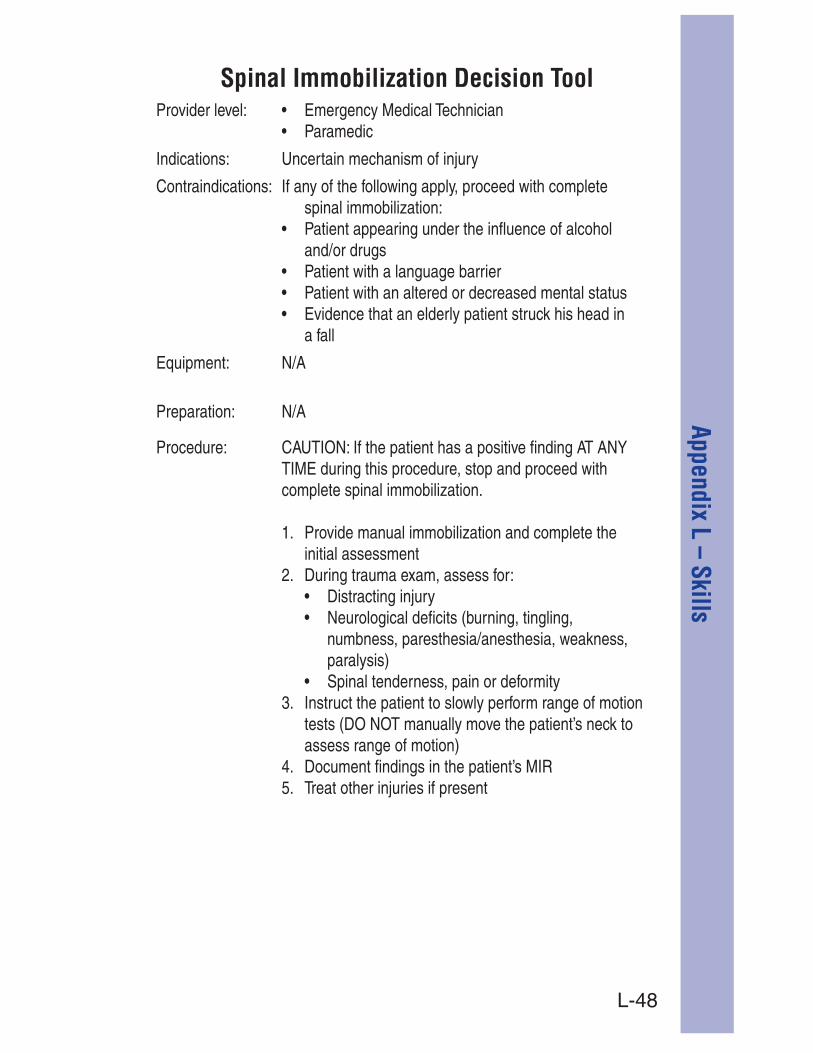
L-48
Appendix L – SkillsProvider level:
Spinal Immobilization Decision Tool
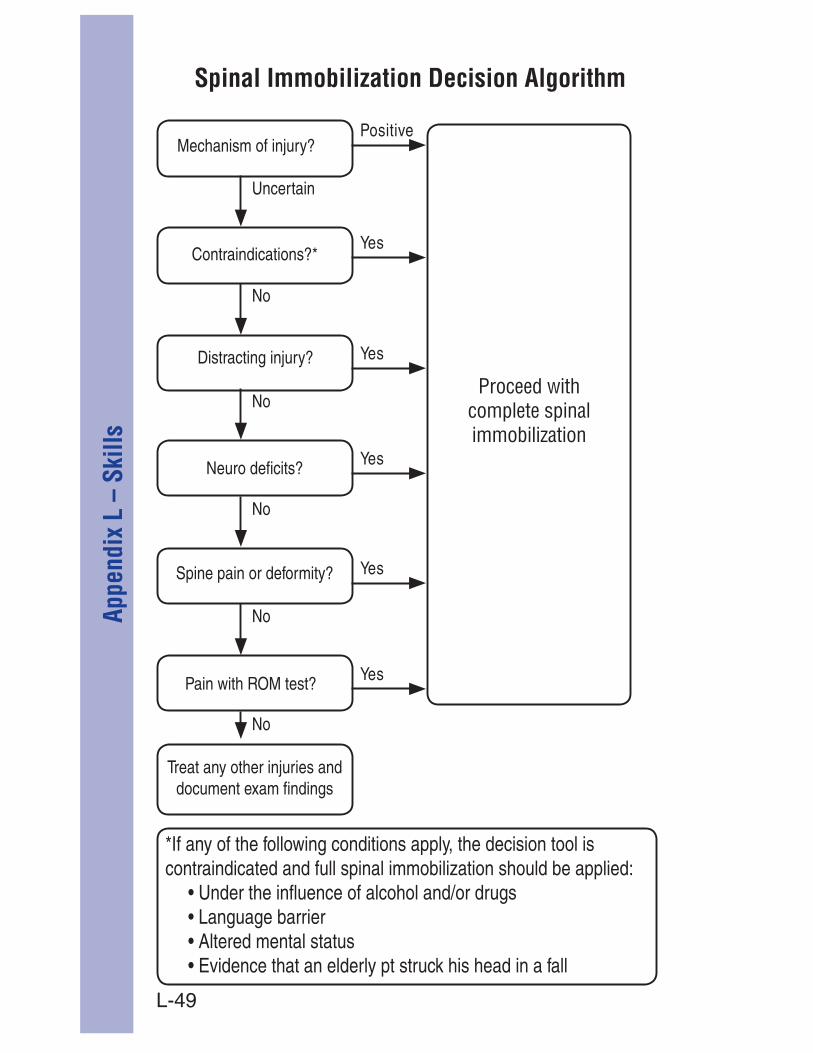
L-49
Appe
ndix
L –
Ski
lls Spinal Immobilization Decision Algorithm
Proceed with complete spinal immobilization
L-50
Appendix L – SkillsSpinal Immobilization
Provider level:

L-51
Appe
ndix
L –
Ski
llsSpinal Immobilization Cont.
L-52
Appendix L – SkillsSubclavian Intravenous Cannulation (Infraclavicular Approach)Provider level: ParamedicIndications: Emergency venous access when peripheral access is not
available in the setting of:
Contraindications:Equipment:
Preparation:flush tubing
Procedure:
the clavicle
advancing the needle toward the suprasternal notch
on the syringe until blood is aspirated
the catheter is patent
dressing over the site
and fluid given in the patient care reportPediatric considerations: pediatric patients
to administer fluid in infants requiring fluid resuscitation
prevent unintentional fluid boluses

L-53
Appe
ndix
L –
Ski
llsProvider level:
Endotracheal (paramedics only)
endotracheal tube
endotracheal tube to moisten secretions as necessary to facilitate suctioning
*Note: if patient is in cardiac arrest you may suction airway while performing chest compressions.
Suctioning

L-54
Appendix L – SkillsProvider level:
Traction Device

L-55
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications:cardiac output that is unresponsive to atropine
who has a transplanted heart
Contraindications:
Equipment:
Preparation:
(sternum/apex) fashion
Procedure:rhythm
capture is obtained
lowest effective level
Pediatric considerations:
Use pediatric pacing pads
Transcutaneous Pacing

L-56
Appendix L – SkillsProvider level: Paramedic
Indications:
Contraindications: None
Equipment:
Preparation:
Mode: CMV - Assist
Trigger [L/min] 52] 5
Tplat
VtPmax 2 2
Procedure:
Auto-PEEP
Pediatric considerations:
Contraindicated in patients requiring
Ventilation Mechanical

L-57
Appe
ndix
L –
Ski
llsProvider level: Paramedic
Indications:
Contraindications: Patient is unconscious/obtunded/absent gag reflexPatient is suspected/potential upper airway
or burns
Equipment:
Preparation:
®”)
Trigger [L/min] 52] 5
PS 10
Vt
Pmax 2 2
Procedure:
Pediatric considerations:
Contraindicated in patients less than 10 years
Ventilation Non-Invasive (“BiPAP®”)

M-1
Appendix M – SOAP W
ritten Report Format
The narrative section of the Medical Incident Report should provide a comprehensive yet as brief as possible “snapshot” of
In Thurston County, the narrative section of a pre-hospital MIR is organized using the SOAP format. SOAP stands for Subjective, Objective, Assessment and Plan.
Subjective (hx present, past): This is information told to the examiner that he or she could not directly observe. The information required in this section is easily remembered by two mnemonics: SAMPLE (Signs and symptoms, Allergies, Medications, Pertinent past medical history, Last oral intake, and Events leading to the 911 call) and OPQRST (Onset, Provokers, Quality, Radiation, Severity and Time).
Objective (findings): The objective portion of the narrative section contains details the examiner observed directly. This is where the patient assessment is documented.
Assessment (findings):
not a diagnosis. The assessment should be written as a two-part statement. The first part should state simply whatever the examiner found wrong with the patient: “Chest discomfort,” for example. The second part of the assessment is the “Rule Out” section, which is written in a
problem should be preceded by the abbreviation “R/O” (“Rule Out”). For example, the assessment of a patient with chest discomfort and shortness of breath might look like this: A/Chest Discomfort 1) R/O ACS 2) R/O CHF.
Plan (care events): This section of the narrative should detail the care the patient received and his or her response to the treatment. This Washington state-approved tool is designed to help emergency medical service providers prioritize treatment and transport during a mass casualty incident.
Appendix M – SOAP Written Report Format
M-2
Appe
ndix
M –
SOA
P W
ritte
n Re
port
Form
atPatients have the right to participate in and guide their medical care including the ability to refuse any given treatment or transport. However, in order to exercise this right a patient must demonstrate to the EMS provider that they have ‘decision making
person is able to stand trial, and is not a relevant term in medical
provider determining that a patient has the ability to understand his/her choices and the possible outcomes of their decisions.
A patient with decision making capacity must:
1. Have fluency in English2. Be over the age of 183. Be oriented to person, place and time and not show any
obvious cognitive deficit4. Be free of the influence of alcohol, drugs, or any mind
altering substances5. Not have any injury or medical condition affecting their
judgement6. Not have threatened or attempted suicide during this episode7. Demonstrate the ability to explain the decision they are
making and the possible negative outcomes including death and devastating disability
If a patient that meets these standards wishes to refuse any aspect of medical care or transport, the Thurston County EMS provider will use the following procedure:
intoxicant, medical condition, or injury that may impair their judgement
to accept
Refusal of Care

M-3
Appendix M – SOAP W
ritten Report Format
death or devastating disability due to current, subsequent or undiagnosed conditions, or deterioration of their condition caused by deviation from Thurston County standards and protocols
negative outcomes that may entail
have the patient sign the “Against Medical Advice” form
encourage the patient to seek medical attention or call 911 if conditions change or they decide they would like evaluation and care
Refusal of Care

N-1
Appe
ndix
N –
STA
RT T
ool
Notbreathing
Positionairway
Notbreathing
Breathing
Approach patient
AirRespirations
Normal
Assessradial Pulse
Present
AssessMentation
FollowsCommands
Tag Yellow,save end
Tag Black,save end
Give 5rescue
breaths; ifstill not
breathing, tag black.
Tag Red,save end
Tag Red,save end
Absent
Tag Red,save end
Fast, slow or noisyFast, slow or noisy
Breathing
Pediatricnot breathing
Appendix N – START Tool
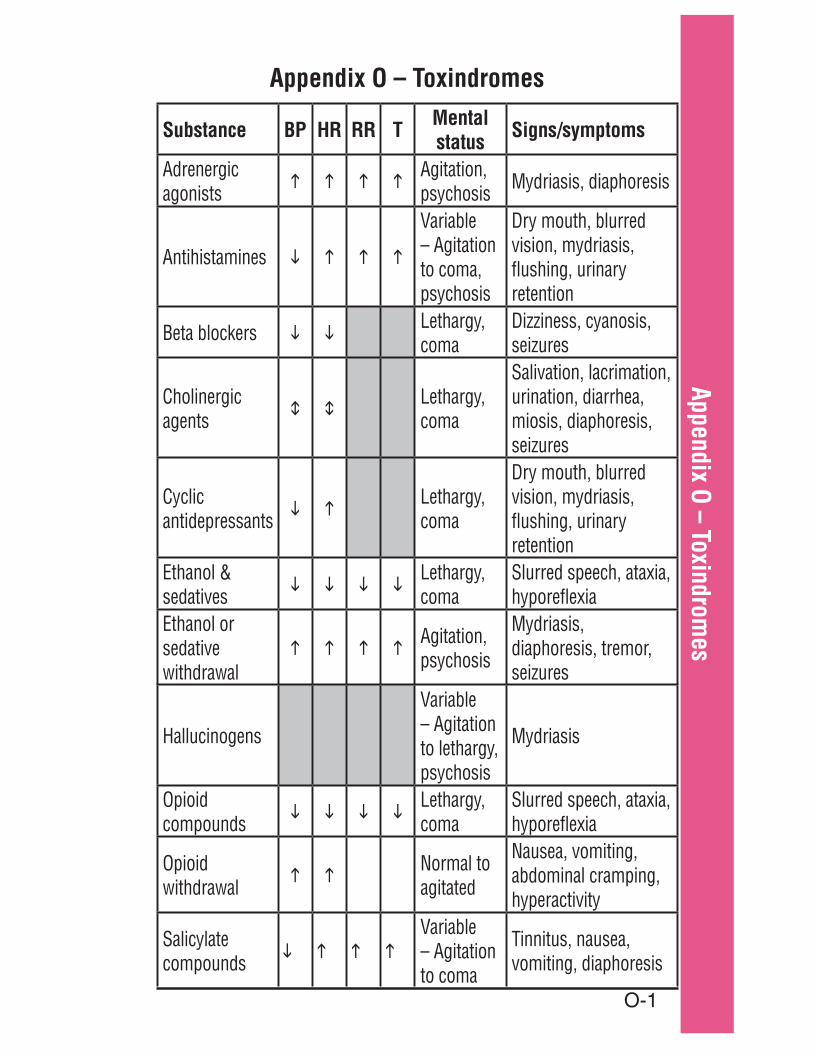
O-1
Appendix O – Toxindromes
Substance BP HR RR T Mental status Signs/symptoms
Adrenergic agonists
Agitation, psychosis Mydriasis, diaphoresis
Antihistamines
Variable – Agitation to coma, psychosis
Dry mouth, blurred vision, mydriasis, flushing, urinary retention
Beta blockers Lethargy, coma
Dizziness, cyanosis, seizures
Cholinergic agents
Lethargy, coma
Salivation, lacrimation, urination, diarrhea, miosis, diaphoresis, seizures
Cyclic antidepressants
Lethargy, coma
Dry mouth, blurred vision, mydriasis, flushing, urinary retention
Ethanol & sedatives
Lethargy, coma
Slurred speech, ataxia, hyporeflexia
Ethanol or sedative withdrawal
Agitation, psychosis
Mydriasis, diaphoresis, tremor, seizures
Hallucinogens
Variable – Agitation to lethargy, psychosis
Mydriasis
Opioid compounds
Lethargy, coma
Slurred speech, ataxia, hyporeflexia
Opioid withdrawal
Normal to agitated
Nausea, vomiting, abdominal cramping, hyperactivity
Salicylate compounds
Variable – Agitation to coma
Tinnitus, nausea, vomiting, diaphoresis
Appendix O – Toxindromes

P-1
Appe
ndix
P –
Was
hing
ton
Stat
e Tr
aum
a Tr
iage
Too
l
Appendix P – Washington State Trauma Triage Tool
Measure vital signs and level of consciousness
Access anatomy of injury
Access mechanism of injury and evidence of high-energy impact
Falls
High-Risk Auto Crash
Auto v. Pedestrian/Bicyclist Thrown, Run Over, or with Significant (> 20 mph) Impact Motorcycle Crash > 20 mph
Age
Anticoagulation and Bleeding Disorders Burns
Time Sensitive Extremity Injury End-Stage Renal Disease Requiring Dialysis Pregnancy > 20 Weeks EMS Provider Judgement
NO
NO
Access special patient or system considerations
NO
Transport according to protocol
NO
When in doubt, transport to a trauma center.For more information on the Decision Scheme, visit: www.cdc.gov/FieldTriage
1
2
3
4
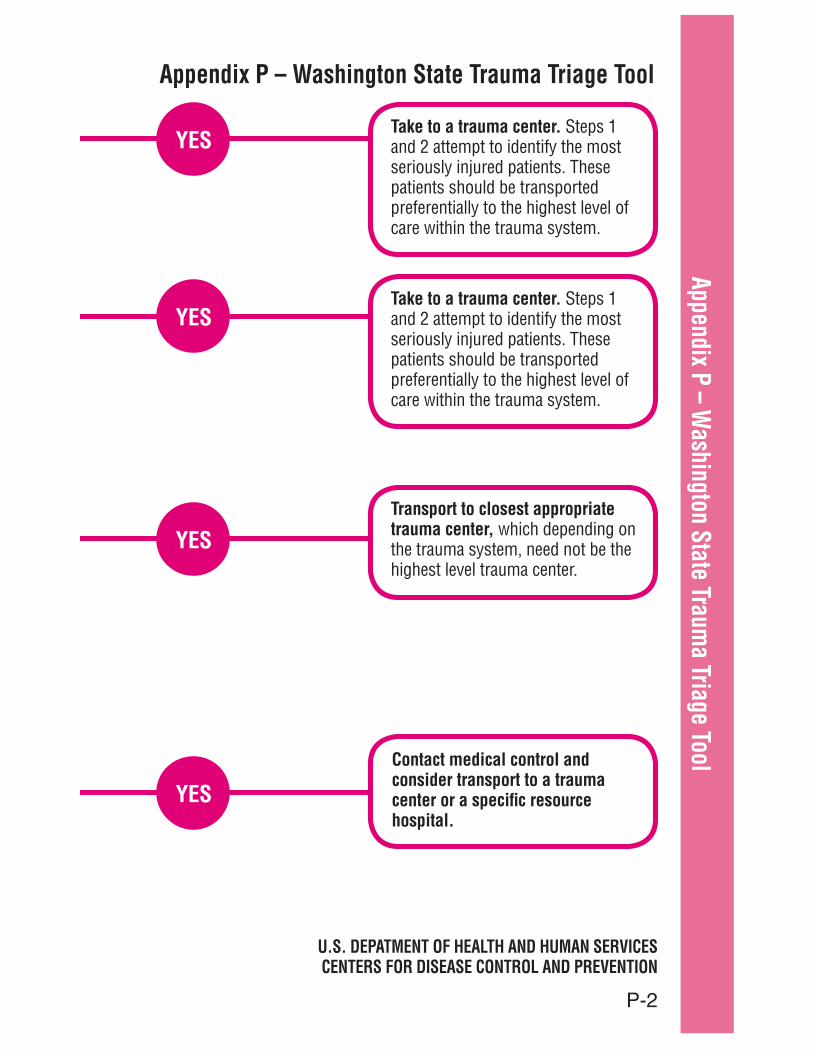
P-2
Appendix P – Washington State Traum
a Triage ToolAppendix P – Washington State Trauma Triage Tool
Take to a trauma center. Steps 1 and 2 attempt to identify the most seriously injured patients. These patients should be transported preferentially to the highest level of care within the trauma system.
YES
Take to a trauma center. Steps 1 and 2 attempt to identify the most seriously injured patients. These patients should be transported preferentially to the highest level of care within the trauma system.
YES
Transport to closest appropriate trauma center, which depending on the trauma system, need not be the highest level trauma center.
YES
Contact medical control and consider transport to a trauma center or a specific resource hospital.
YES
U.S. DEPATMENT OF HEALTH AND HUMAN SERVICESCENTERS FOR DISEASE CONTROL AND PREVENTION

P-3
Appe
ndix
P –
Was
hing
ton
Stat
e Tr
aum
a Tr
iage
Too
lSt. Peter Hospital
Full Trauma Team Activation (FTT) Requirement
2<90% with associated chest injury
pelvic fracture
Trauma Surgeon must be called in to see these patients
*Neurosurgeon may be called in place of general surgeon for isolated penetrating head injuries ONLY*
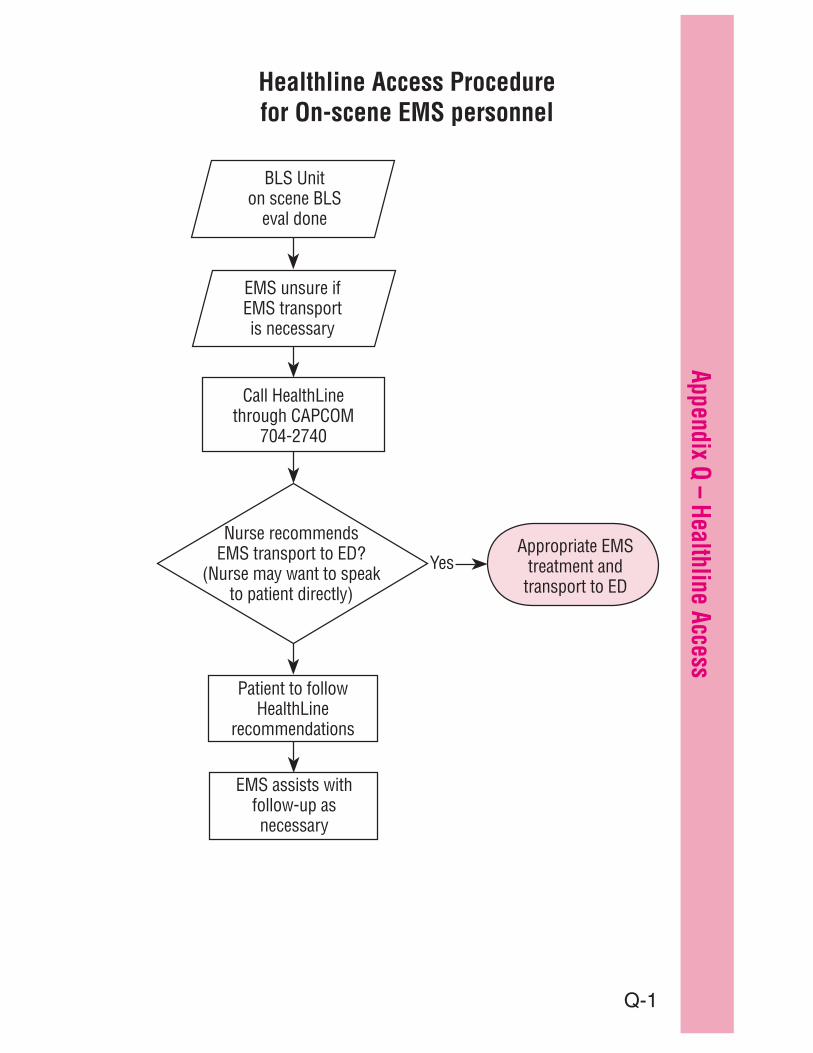
Q-1
Appendix Q – Healthline Access
BLS Uniton scene BLS
eval done
Call HealthLinethrough CAPCOM
704-2740
Nurse recommends EMS transport to ED?
(Nurse may want to speak to patient directly)
Patient to followHealthLine
recommendations
Appropriate EMS treatment and
transport to ED
EMS unsure ifEMS transportis necessary
EMS assists with follow-up asnecessary
Yes
Healthline Access Procedure for On-scene EMS personnel

Q-2
Appe
ndix
Q –
Hea
lthlin
e Ac
cess

1
GLOSSARYACS acute coronary syndrome – refers to any
group of clinical symptoms caused by acute myocardial ischemia
adrenergic resembling adrenaline, especially in physiological action
akisthesia a feeling of restlessness and an urgent need of movement, side effect of phenothiazines
antegrade forward (e.g. from the time of injury)
anticoagulant substance that hinders the clotting of blood; a blood thinner
aphasia absence or impairment of the ability to communicate through speech, writing, or signs due to dysfunction of brain centers
barotrauma any injury caused by a change in atmospheric pressure between a potentially closed space and the surrounding area
Bell’s palsy paralysis of the facial nerve producing distortion on one side of the face
carbonaceous sputum
sputum tinged black or charcoal secondary to exposure to fire and or a smoky environment
carpopedal spasms
involuntary flexion of the hands and feet, usually secondary to carbon dioxide deficiency
cholinergic liberating, activated by or involving acetylcholine; resembling acetylcholine, especially in physiologic action
CID cervical immobilization device
clonic reflexes rhythmic, involuntary muscle contractions
colormetric devices
end-tidal carbon dioxide detectors that rely on a litmus type paper to change color in the presence of carbon dioxide
consent definitions
expressed consent means the patient was advised of the treatment being offered and has given permission; implied consent means consent is assumed to exist (i.e., the patient has not refused)
cricoid pressure application of digital pressure to cricoid cartilage in neck of an unconscious patient to permit visualization of the glottic opening during endotracheal intubation
Glossary
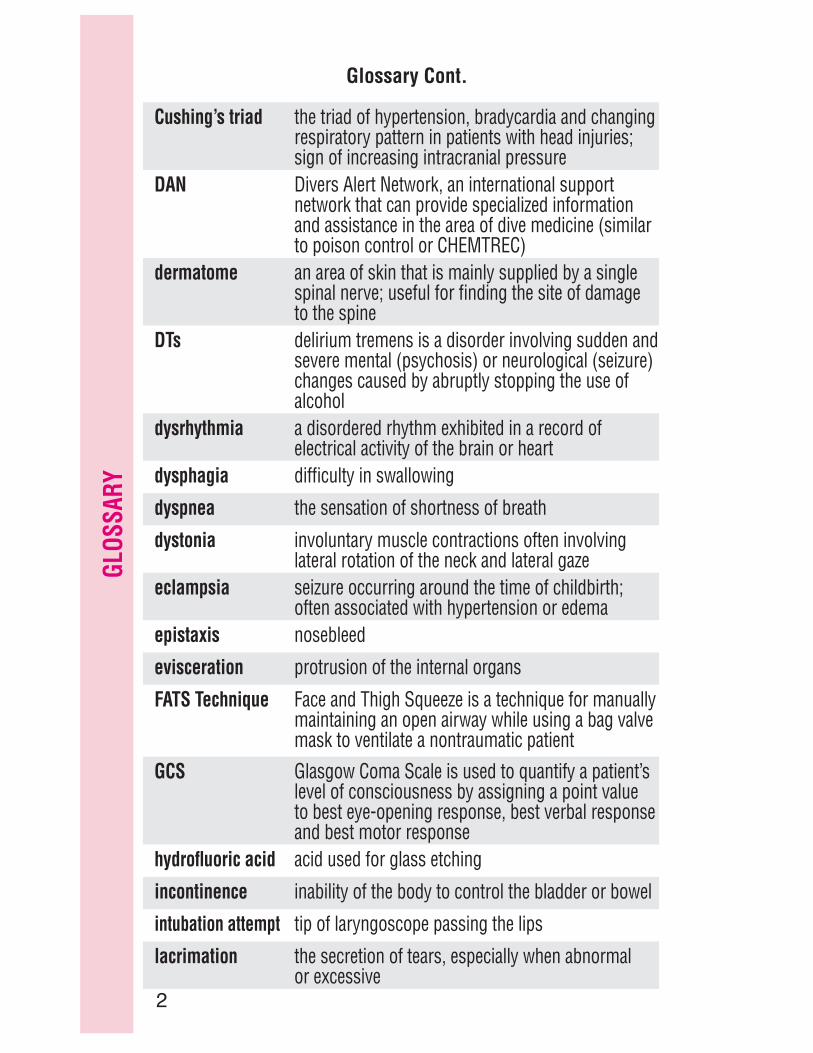
2
GLOS
SARY
Cushing’s triad the triad of hypertension, bradycardia and changing respiratory pattern in patients with head injuries; sign of increasing intracranial pressure
DAN Divers Alert Network, an international support network that can provide specialized information and assistance in the area of dive medicine (similar to poison control or CHEMTREC)
dermatome an area of skin that is mainly supplied by a single spinal nerve; useful for finding the site of damage to the spine
DTs delirium tremens is a disorder involving sudden and severe mental (psychosis) or neurological (seizure) changes caused by abruptly stopping the use of alcohol
dysrhythmia a disordered rhythm exhibited in a record of electrical activity of the brain or heart
dysphagia difficulty in swallowing
dyspnea the sensation of shortness of breath
dystonia involuntary muscle contractions often involving lateral rotation of the neck and lateral gaze
eclampsia seizure occurring around the time of childbirth; often associated with hypertension or edema
epistaxis nosebleed
evisceration protrusion of the internal organs
FATS Technique Face and Thigh Squeeze is a technique for manually maintaining an open airway while using a bag valve mask to ventilate a nontraumatic patient
GCSlevel of consciousness by assigning a point value to best eye-opening response, best verbal response and best motor response
hydrofluoric acid acid used for glass etching
incontinence inability of the body to control the bladder or bowel
intubation attempt tip of laryngoscope passing the lips
lacrimation the secretion of tears, especially when abnormal or excessive
Glossary Cont.

3
GLOSSARYlateralizing signs signs that occur on one side of the body
miosis very small pupils
mydriasis pronounced or abnormal dilation of the pupil
normothermic normal body temperature
nuchal of or relating to the region of the neck
pallor deficiency of color, especially of the face
palpitations a sensation of an unduly rapid or irregular heart beat
paresthesia sensation of numbness, prickling or tingling
petechial hemorrhaging
small, purplish hemorrhagic spots on the skin
polypharmacy ingestion of more than 1 drug together
POLST Physician Ordered Life Sustaining Treatment, or end-of-life treatment documentation
postictal period that follows the clonic phase of a generalized seizure
pre-syncope signs and symptoms experienced by a patient prior to having a syncopal event
priapism persistent, abnormal erection of the penis accompanied by pain and tenderness
procedure describes the sequence of actions in medical protocols or policies
prodrome symptom(s) that may indicate the onset of a disease
protocol defines field treatments, or the order and type of medical interventions for specific illness and injury conditions
pseudoseizure seizurelike behavior that may or may not be voluntary
retrograde going backward (i.e., loss of memory before injury)
Glossary Cont.
4
GLOS
SARY
rule of palm method used to measure the body surface area of a burn patient: the palm of the person who is burned (not fingers or wrist area) is about 1 percent of the
surface area burnedsalicylate a group of aspirin-like compounds (i.e., Pepto
Bismol, Alka Seltzer)sclera the white part of the eyeball
semi-Fowler’s position for patient, with the back raised 45 degrees from horizontal
sonorous respirations
snoring respirations
sublingual beneath the tonguestatus seizure multiple seizure without return to baseline level of
sublingual consciousness
subcutaneous emphysema
the presence of a gas and especially air in the subcutaneous tissue
tachypnea abnormally rapid breathing (36-40 breaths per minute for an adult)
Torsades de Pointes
ventricular tachycardia that is characterized by rhythmic fluctuation in amplitude of the QRS complexes
tonic involuntary muscular contraction
toxindrome a syndrome associated with a certain toxic substance
trismus total contraction of the muscles of the jaw
unilateral affecting only one side
vertigo the sensation that the environment is moving
WPW Wolff-Parkinson-White syndrome is an autonomic defect of the heart that is associated with severe or difficult-to-control tachycardias
Glossary Cont.

Phone/Fax Contacts for EMS Providers CONTACT AC NUMBER MAIN NUMBER FAX
Capital Medical Center ER 360 956‐2596 754‐5858 956‐2564
Providence Centralia ER 360 330‐8515 877‐736‐2803 330‐8684
Childrens Seattle ER 206 987‐8899 866‐987‐2000 987‐3945
Divers Alert Network (DAN) 919 684‐9111
Harborview Med Ctr “Trauma Doc” 206 731‐3074 731‐3000 731‐2655
Madigan Army Medical Center 253 968‐1396 968‐1110 968‐3190
Madigan Gate for Entrance 253 968‐1396
Mary Bridge Childrens ER 253 403‐1476 403‐1400 403‐1406
Providence St. Peter Hospital ER 360 491‐8888 491‐9480 493‐7663
Tacoma General ER 253 627‐8500 403‐1000 403‐1517
Virginia Mason ER & Hyperbaric 206 583‐6450 624‐1144 223‐6677
END HARM Reporting 866 363‐4276 END‐HARM
Area Agency on Aging 360 664‐2168 664‐2168 664‐0791
Thurston County Coroner 360 586‐2091 586‐2091 357‐2485
Washington Poison Center 800 709‐0911 800‐222‐1222
Washington State Patrol 360 586‐1999 586‐4443 (Tacoma
24hrs)
OTHER IMPORTANT RESOURCES
Red Cross (24 hrs) 360 352‐8575 352‐0861
Safeplace (Emergency Shelter) 360 754‐6300
(Will return voice mail within 20
minutes)
Salvation Army (Emergency Shelter) 360 352‐8596
CYS Shelter Project (11‐17 yrs) 360 943‐0780
Crisis Clinic 360 586‐2800 800‐627‐2211
Domestic Violence Hotline 800 562‐6025
Haven House Youth Shelter (24hrs) 360 754‐1151


















