
1 EMS Fundamentals An Introduction to the EMS Process Roadmap AASHTO EMS Workshop.
Upload
godwin-harringtonCategory
view
216download
0
EMS Performance Targets and Travel Times
EMS Planning Conference, August 2008
Armann [email protected]
Academic DirectorCentre for Excellence in Operations
School of Business, University of Alberta
Based on joint work with S. Budge, E. Erdogan, E. Erkut, and D. Zerom
and using data from Calgary EMS and Edmonton EMS

Typical EMS Performance Targets: Coverage
• US EMS Act, 1973: 95% in 10 min.
• North America, current: 90% of urgent urban calls in 8:59 min.
• UK: – 75% of all calls in 8 min.– 95% of urban calls in 14 min.– 95% of rural calls in 19 min.
• Germany: – 95% in X min.– X varies across the country
from 10 to 15 min.
• Questions:– What are targets based on?– How can we predict
compliance to these targets, using a map?
– Are there better targets?

What are Coverage Targets Based on?
• Cardiac Arrest Survival Studies
• Focus on limiting the longest possible response time– As opposed to average response time
• Consistency: it’s what other operators do– Although the details vary widely
• Simple to interpret and compute

Let’s do this for a location in Twin Brooks, Edmonton
• Pick a location in the city• Find closest station• Predict performance for that location• Repeat for all locations in the city• Colour-code the map• Compute weighted average performance for the
whole city– Weights = call volumes
• (What we’re leaving out: ambulance availability)
Using a Map to Predict Performance

Closest Station: Terwillegar
Call location
Closest station

How Far is it? Take 1
Call location
Closest station
4.5 km
As the crow flies
“Euclidean distance”

How Far is it? Take 2
Call location
Closest station
5.8 km
North-south and east-west travel only
“Manhattan metric”
“Rectilinear distance”

How Far is it? Take 3
8.6 km
Using Google Maps
“Network distance”

OK, so I Measured the DistanceWhat’s Next?
DistanceDifferent ways to measure
Station locations
Ambulance availability
Zone sizes
Response TimeWhen to start and stop the clock
Variability
“Outcome”Less or more than 8:59?
Medical outcome?
Psychological outcome?
Transform
Transform
Traffic conditions
Driver behaviour
Construction
Pre-travel and post-travel
…
Paramedic training
Patient’s condition
…
What we’ll do next

Distance Travel Time
• 8.6 km ? min.• Google Maps says 14 min.• Better: use historical call data to compute
average speed• Even better (?)
compute different average speeds for:– Downtown vs. elsewhere– Different road types– Urgent vs. non-urgent– Rush hour vs. other times– Winter vs. summer– And so on …
Complicated!
Is there a simpler approach that is useful?

A Simpler Approach
Time
Speed
acceleration
cruising speed
deceleration
A long trip:

A Simpler Approach
Time
Speed
A short trip:

The Simpler Approach vs. RealityD
P
EN AR
0
30
60
90
0 2 4 6 8 10 12 14
Time from dispatch (min)
Spee
d (k
m/h
r)
AVL speed
K WH predictionLong trip
DP
EN AR
0
30
60
90
0 2 4 6
Time from dispatch (min)
Spee
d (k
m/h
r)
AVL speed
K WH predictionShort trip
Good enough to estimate average travel time, but lots of variability around the average

(Average) Travel Time Curve
-123456789
10
- 2 4 6 8 10
Distance (km)
Tra
vel t
ime
(m
in.)
Short trips Long trips
Estimates from Edmonton and Calgary data:
• Cruising speed: 100 kph.
• Acceleration: 5 min. (4.2 km) to reach cruising speed

Travel time Formula
• Short trips (< 4.2 km):Travel time in min.
= 2.45 × SQRT(distance in km)
• Long trips (> 4.2 km):Travel time in min.
= 2.5 + 0.6 × (distance in km)
• Twin Brooks: 2.5 + 0.6 × (8.6 km) = 7:42 min.• 8:59 min. 10.8 km• Twin Brooks is covered!

Not coveredCovered!
Is Twin Brooks Really Covered?Terwillegar station Twin Brooks
8:597:42But travel times are not always the same:
• Traffic
• Driver behaviour
• Construction
Twin Brooks may be covered on average, but it would be useful to know the probability of coverage
Terwillegar station Twin Brooks
8:597:42

Probability of Coverage Curve
8.6 km, 70%
0%10%20%30%40%50%60%70%80%90%
100%
- 5 10 15 20 25
Distance (km)
Pro
b. o
f co
vera
ge Twin Brooks:
Implications for deployment:
3 km is twice as good as 11 km
vs.
< 11 km good, > 11 km bad

Probability of Coverage Map
0%20%40%60%80%
100%
Prob. of Coverage
G
G
G
G
GG
G
G
G
G
G
G
G
G
G
G
G
G
G
GG
G
G
GG
G
G
G
G
9
8
6
5
4
32
1
94
34
32
31
30
28
26
24
23
22
21
20
19
18
1715
14
12
11
AMC
Cochrane
Created using probability of coverage curve, for all locations in a city

The Formulas
• Travel time = ((distance) + f(time of day))× exp((distance) )
• (distance) avg. travel time curve
• (distance) next slide
• f(time of day) the slide after that
• ~ t distribution with 3.3 d.f.

Coefficient of Variation: (distance)

Time-of-day Effect
~ 5 PM
Afternoon rush hour
~ 4 AM ??

How About Medical Outcomes instead of % in 8:59?
DistanceDifferent ways to measure
Station locations
Ambulance availability
Zones sizes
Response TimeWhen to start and stop the clock
Variability
“Outcome”Less or more than 8:59?
Medical outcome?
Psychological outcome?
Transform
Transform
Traffic conditions
Driver behaviour
Construction
Pre-travel and post-travel
…
Paramedic training
Patient’s condition
…

Out-of-hospital Cardiac Arrest Survival Rates
Sur
viva
l rat
e
100%
Time from cardiac arrest
10 min.
CPR
Defibrillation
Adapted from Eisenberg et al, 1979
Advanced cardiac life support

Casino Study (Valenzuela et al, 2000)
• Casino security officers trained in CPR and defibrillation
• Time of collapse from videotapes
• Response times ≈ 3 min – much shorter than most EMS calls
• Survival rates:– 74% when response time < 3 min.– 49% when response time > 3 min.

Estimated Survival Functions
• Here’s one of four that we found:
• “Response time” is nowhere to be seen!• Need to make assumptions so can
“average over” non-response-time factors• A good thing – allows calibration of a
function estimated in one city for use in another city with a different EMS system
1)0.1390.156 0.26-DefibCPR
DefibCPR1),( IIeIIs
Arrest to CPR time Arrest to defibrillation time

Calibrating Survival Functions: Assumptions
• Is collapse witnessed?61% yes, average access time = 1.2 min
39% no, average access time = 30 min
• Bystander CPR: 64%, 1 min after 911
• Response time: Average pre-travel delay = 3 min
+ Average travel time (based on distance)
• EMS arrival to defibrillation: 2 min
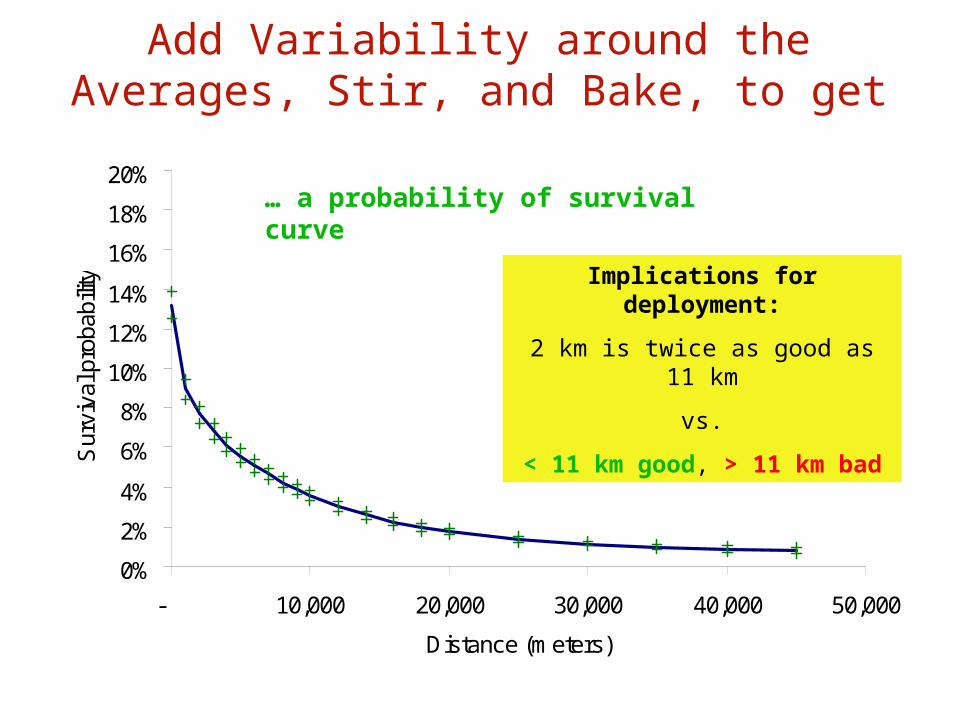
Add Variability around the Averages, Stir, and Bake, to get …
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
- 10,000 20,000 30,000 40,000 50,000
Distance (meters)
Sur
viva
l pro
babi
lity
… a probability of survival curve
Implications for deployment:
2 km is twice as good as 11 km
vs.
< 11 km good, > 11 km bad

Sensitivity Analysis: Avg. Access Time, Un-Witnessed Arrest
0%
5%
10%
15%
20%
0 10,000 20,000 30,000
Distance (m)
Su
rviv
al p
rob
ab
ility
30
5
60

“Optimal” Allocation of Ambulances to Stations
• Change target from avg. response time to coverage: save 65 lives
• Account for uncertainty about coverage: save 47 lives• Change target from coverage to survival (but ignore
uncertainty): save 47 lives
Incorporation of uncertainty
None Response times
Ambulance availability
Both
Min. avg. response time
697 745
Max. avg. coverage 762 809 809 809
Max. avg. lives saved 809 809 809 809

Observations
• Survival rates vs. response time:– Out-of-hospital cardiac arrest survival rates have
been studied extensively– These are the most “saveable lives”
• Possible to incorporate survival rates based on medical research into planning models
• Coverage is a poor proxy for survival rates …– … but consideration of uncertainty improves it

Why does Maximizing Survival Rates and Maximizing Expected Coverage give Similar Results?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
- 5 10 15 20 25
Distance (km)
Pro
b. o
f co
vera
ge
0%
2%
4%
6%
8%
10%
12%
14%
Pro
b. o
f su
rviv
al
0/1 coverage

Potential Reasons to Focus on Survival Rates instead of Coverage• Coverage is an imperfect proxy for survival rates …
– … assuming that that’s the real objective
• Abstract units– $ or lives saved get more attention than “% in 8:59”
• All of the following are arbitrary and vary among EMS systems:– The time standard– The percentage goal– When the clock starts and stops

Potential Problems (and Solutions) with a Focus on Survival Rates
• Only know survival rates for cardiac arrest– Do more studies of non-cardiac arrest patients– Use coverage target for other patients?
• Insufficient data to calibrate survival functions– Maybe the data should be collected anyway for cardiac arrest
patients?– Plans to collect the data in some cities
• “90% covered” sounds better than “8% survived”– Important to include benchmarks: 2% survival without EMS?– Focus on “lives saved” instead of “% survival”?
• ?– ?

For More Information
• Erkut, E., A. Ingolfsson, G. Erdoğan. 2008. Ambulance deployment for maximum survival. Naval Research Logistics 55 42-58
• Budge, S., A. Ingolfsson, D. Zerom. Empirical Analysis of Ambulance Travel Times (ready later this month)
• [email protected]• www.business.ualberta.ca/aingolfsson/publications.htm

Questions?


















