Emerging Treatment Options for the Reversal of Oral ... · Emerging Treatment Options for the...
61
Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy Presented as a Midday Symposium at the 47 th ASHP Midyear Clinical Meeting and Exhibition Monday, December 3, 2012 Las Vegas, Nevada Remind Me Tool Planned and conducted by ASHP Advantage and supported by an educational grant from CSL Behring
Transcript of Emerging Treatment Options for the Reversal of Oral ... · Emerging Treatment Options for the...

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
Presented as a Midday Symposium at the
47th ASHP Midyear Clinical Meeting and Exhibition
Monday, December 3, 2012 Las Vegas, Nevada
Remind Me Tool
Planned and conducted by ASHP Advantage and supported by an educational grant from CSL Behring

Please be advised that this activity is being audio and/or video recorded for archival purposes and, in some cases, for repurposing of the content for enduring materials.
2
Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
A G E N D A
11:30 a.m. – 11:40 a.m. Welcome and Introductions Edith A. Nutescu, Pharm.D., FCCP
11:40 a.m. – 12:00 p.m. Oral Anticoagulant Therapies: A Balancing Act
Edith A. Nutescu, Pharm.D., FCCP 12:00 p.m. – 12:40 p.m. Options for Reversing the Effects of Oral
Anticoagulants James S. Kalus, Pharm.D., BCPS (AQ-Cardiology)
12:40 p.m. – 1:10 p.m. Practical Issues in Developing an Oral Anticoagulant
Reversal Strategy William E. Dager, Pharm.D., BCPS (AQ-Cardiology)
1:10 p.m. – 1:30 p.m. Faculty Discussion and Audience Questions
All Faculty F A C U L T Y
Edith A. Nutescu, Pharm.D., FCCP Activity Chair and Moderator Clinical Professor The University of Illinois at Chicago College of Pharmacy Director, Antithrombosis Center The University of Illinois Hospital and Health Sciences System Chicago, Illinois James S. Kalus, Pharm.D., BCPS (AQ-Cardiology) Senior Manager, Patient Care Services Department of Pharmacy Services Henry Ford Hospital Detroit, Michigan William E. Dager, Pharm.D., BCPS (AQ-Cardiology) Pharmacist Specialist UC Davis Medical Center Sacramento, California
3
Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
D I S C L O S U R E S T A T E M E N T
In accordance with the Accreditation Council for Continuing Medical Education’s Standards for Commercial Support and the Accreditation Council for Pharmacy Education’s Guidelines for Standards for Commercial Support, ASHP Advantage requires that all individuals involved in the development of activity content disclose their relevant financial relationships. A person has a relevant financial relationship if the individual or his or her spouse/partner has a financial relationship (e.g., employee, consultant, research grant recipient, speakers bureau, or stockholder) in any amount occurring in the last 12 months with a commercial interest whose products or services may be discussed in the educational activity content over which the individual has control. The existence of these relationships is provided for the information of participants and should not be assumed to have an adverse impact on presentations. All faculty and planners for ASHP Advantage education activities are qualified and selected by ASHP Advantage and required to disclose any relevant financial relationships with commercial interests. ASHP Advantage identifies and resolves conflicts of interest prior to an individual’s participation in development of content for an educational activity. The faculty and planners report the following relationships: Edith A. Nutescu, Pharm.D., FCCP, Activity Chair Dr. Nutescu declares that she has has served as a consultant for Daiichi-Sankyo Inc. and received a research grant and served as a consultant for Janssen Pharmaceuticals, Inc. James S. Kalus, Pharm.D., BCPS (AQ-Cardiology) Dr. Kalus declares that he has no relationships pertinent to this activity. William E. Dager, Pharm.D., BCPS (AQ-Cardiology) Dr. Dager declares that he has no relationships pertinent to this activity. Susan R. Dombrowski, M.S., B.S.Pharm. Ms. Dombrowski declares that she has no relationships pertinent to this activity. Carla J. Brink, M.S., B.S.Pharm. Ms. Brink declares that she has no relationships pertinent to this activity. ASHP staff has no relevant financial relationships to disclose.
4
Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
A C T I V I T Y O V E R V I E W
As the armamentarium of oral agents for prevention and treatment of thrombosis expands, practitioners must develop strategies to deal with the proper management of anticoagulant-related bleeding complications. Patients on oral anticoagulants who are at high risk of bleeding, are actively bleeding, or require emergency invasive procedures will need adjunct therapies that reverse or remove anticoagulant effects sooner than withholding the drug. This activity will provide an overview of the challenges associated with oral anticoagulant therapies, including risks for developing bleeding complications. Therapeutic options for reversing the effects of oral anticoagulants will be described, focusing on new and emerging options for reversal. Using different patient scenarios, the faculty will explore practical issues in developing a reversal strategy for oral anticoagulant therapy. A C T I V I T Y O B J E C T I V E S
After attending this application-based educational activity, participants should be able to
Identify risk factors for bleeding complications with oral anticoagulant agents.
Apply strategies for minimizing the risk of bleeding with oral anticoagulant agents.
Describe the relative benefits and limitations of emergent anticoagulant reversal strategies.
Discuss the clinical evidence supporting the use of emergent anticoagulant reversal strategies.
Explain patient-specific treatment options for reversing the effects of oral anticoagulants using laboratory observations.
Develop an approach to managing major bleeding in a patient on oral anticoagulation therapy.
5

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
C O N T I N U I N G E D U C A T I O N A C C R E D I T A T I O N
The American Society of Health-System Pharmacists is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. This activity provides 2.0 hours (0.2 CEUs) of continuing pharmacy education credit (ACPE activity #0204-0000-12-438-L01-P).
Attendees must complete a Continuing Pharmacy Education Request online and may immediately print their official statements of continuing pharmacy education credit at the ASHP CE Center at http://ce.ashp.org following the activity. Complete instructions for receiving your statement of continuing pharmacy education online are on the next page. Be sure to record the session code beginning with “A” announced during the activity.
N e w ! P R A C T I C E R E M I N D E R E M A I L During this educational activity, we encourage you to jot down points about
what YOU want to remember to do as a result of what you are learning. Use your smart device to link directly to the reminder tool and type in
your ideas.
Next month, we will send you an email as a reminder from YOURSELF about what YOU want to do after attending this activity.
Do it more than once...multiple entries for this activity from the same email address will be combined into one email.
If you do not have a smart device, go to the reminder tool on the activity website. http://www.ashpadvantage.com/reversal/?remindme=1
6

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
Instructions for Processing CPE online at http://ce.ashp.org
The ASHP CE Center allows participants to obtain statements of continuing pharmacy education (CPE) conveniently and immediately using any computer with an internet connection. To obtain CPE statements for ASHP Advantage activities, please visit
http://ce.ashp.org 1. Log in to the ASHP CE Center using your e-mail address and password.
If you have not logged in to the ASHP CE Center (launched August 2008) and are not a member of ASHP, you will need to set up an account by clicking on “Become a user” and follow the instructions.
2. Once logged in to the site, click on Process Meeting CE.
3. If you are a registered attendee at the ASHP Midyear Clinical Meeting, click on the start button to the right of ASHP Midyear Clinical Meeting 2012.
If you are not registered to attend the ASHP Midyear Clinical Meeting, click on the start link to the right of the activity title. If this activity title does not appear in your meeting list, enter the 5-digit activity code in the box above the list and click submit. The activity code is noted below. Click submit when prompted and then click on the start link to the right of the activity title. Do not click on “remove" next to an activity title unless you did not attend that activity.
4. Click on the click here link to view sessions associated with the day of the activity.
5. Enter the session code announced during the activity (e.g., A12XXX and note that the letter is case sensitive) and select the number of hours equal to your participation in the activity.
6. Click submit to receive the attestation page.
7. Confirm your participation and click submit.
8. Complete the overall Midyear evaluation and click the finish button. You will then be able to view and print your transcript.
Date of Activity Activity Code Session Code
(announced during the live activity)
CPE credit hours
December 3, 2012
12438 A12_____ 2
NEED HELP? Contact ASHP Advantage at [email protected].
7

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
Your educational opportunities related to the reversal of anticoagulant therapy extend beyond today’s symposium…
A live Ask the Experts webinar on March 20, 2013, during which faculty will
explore issues raised by participant questions in today’s symposium (1 hour CPE)
Informational podcasts featuring the faculty in a roundtable discussion about important issues related to reversal of anticoagulant therapy
e-Newsletters featuring tips for incorporating information from this symposium into practice, as well as updates on emerging information on anticoagulant therapy reversal
Web-based activity based on today’s live symposium (2 hours of CPE, but please note that individuals who claim CPE credit for the live symposium or webcast are ineligible to claim credit for the web-based activity)
Supplement to the American Journal of Health-System Pharmacy (CPE hours to be determined)
For more information and to sign up to receive e-mail updates about this educational series, go to
www.ashpadvantage.com/reversal
8

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
Edith A. Nutescu, Pharm.D., FCCP Activity Chair and Moderator Clinical Professor The University of Illinois at Chicago College of Pharmacy Director, Antithrombosis Center The University of Illinois Hospital and Health Sciences System Chicago, Illinois Edith A. Nutescu, Pharm.D., FCCP, is Clinical Professor in the Department of Pharmacy Practice, Department of Pharmacy Administration, and Center for Pharmacoeconomic Research at University of Illinois at Chicago College of Pharmacy. She also is Director of the Antithrombosis Center at the University of Illinois at Chicago Medical Center. Dr. Nutescu earned her Doctor of Pharmacy degree with high honors at the University of Illinois at Chicago College of Pharmacy. After graduation, she went on to complete a pharmacy practice residency at Lutheran General Hospital–Advocate Health Care in Park Ridge, Illinois, and a primary care specialty residency at the University of Illinois at Chicago Medical Center, both accredited by the American Society of Health-System Pharmacists (ASHP). Dr. Nutescu maintains an active clinical practice and research program. Her research and practice interests are in the areas of comparative effectiveness, health services, and outcomes, with emphasis in cardiovascular diseases, stroke, thrombosis, and antithrombotic therapies. She has authored over 100 scientific articles and book chapters, and she coauthored “Anticoagulation Therapy: A Point-of-care Guide” published by ASHP in 2011. Her research has been funded by the Department of Health and Human Services, Agency for Healthcare Research and Quality, and National Center for Research Resources. She is a recipient of the Ruth L. Kirchstein National Research Service Award for 2010-2012. She has lectured extensively both nationally and internationally on topics related to thrombosis, antithrombotic therapies, cardiovascular diseases, and stroke. Dr. Nutescu serves on the editorial boards for Pharmacotherapy, Annals of Pharmacotherapy, and Thrombosis, and she previously was on the editorial board for the American Journal of Health-System Pharmacy. Dr. Nutescu is active in several professional organizations, and she currently is a member of the Board of Regents for the American College of Clinical Pharmacy (ACCP), Board of Directors for Pharmacotherapy, and Board of Directors of the Anticoagulation Forum. She has served on the Oral Anticoagulant National Advisory Board of the National Consumers League Senior Outpatient Medication Safety Coalition and was the only pharmacist member nominated to serve on the steering committee of the National Quality Forum and The Joint Commission that developed “National Consensus Standards for the Prevention and Care of Venous Thrombosis.” Dr. Nutescu has been recognized as a fellow of ACCP and is the recipient of the ACCP 2009 Clinical Practice Award and ASHP Section of Home and Ambulatory Care Practitioners 2010 Distinguished Service Award.
9

Oral Anticoagulant Therapies:A Balancing Act
Edith A. Nutescu, Pharm.D., FCCPClinical Professor
The University of Illinois at Chicago College of Pharmacy
Director, Antithrombosis Center
The University of Illinois Hospital and Health Sciences System
Chicago, Illinois
Learning Objectives
At the conclusion of this presentation,
participants will be able to
• Identify risk factors for bleeding y gcomplications with oral anticoagulant agents
• Discuss strategies for minimizing the risk of bleeding with oral anticoagulant agents
Background
• Due to increase in the U.S. elderly population, prevalence of thrombosis related complications and bleeding associated with anticoagulants isassociated with anticoagulants is constantly rising
• Various tools exist to assess thrombotic risk but assessment of bleeding risk is often ignored
Roger VL et al. Circulation. 2012; 125:e2-e220.
10
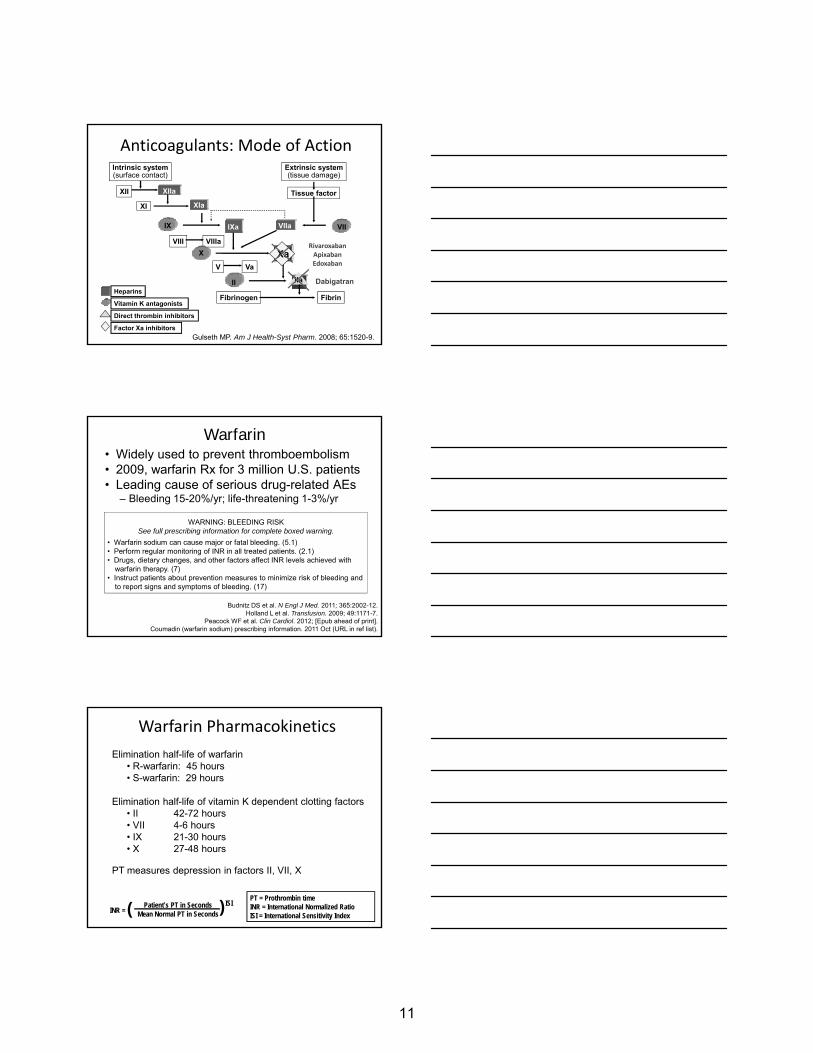
Anticoagulants: Mode of Action
XIIa
Intrinsic system(surface contact)
XII
XI XIaTissue factor
IX IXa VIIa VII
Extrinsic system(tissue damage)
Gulseth MP. Am J Health-Syst Pharm. 2008; 65:1520-9.
Xa
IIa
Factor Xa inhibitors
Direct thrombin inhibitors
Vitamin K antagonists
Heparins
VIII VIIIaX Xa
V Va
II
Fibrinogen Fibrin
DabigatranIIa
RivaroxabanApixabanEdoxaban
Warfarin Pharmacokinetics
Elimination half-life of warfarin• R-warfarin: 45 hours• S-warfarin: 29 hours
Elimination half-life of vitamin K dependent clotting factors• II 42-72 hours• VII 4-6 hours• IX 21-30 hours• X 27-48 hours
PT measures depression in factors II, VII, X
( )Patient’s PT in SecondsMean Normal PT in SecondsINR =
ISIPT = Prothrombin timeINR = International Normalized RatioISI = International Sensitivity Index
Warfarin• Widely used to prevent thromboembolism• 2009, warfarin Rx for 3 million U.S. patients• Leading cause of serious drug-related AEs
– Bleeding 15-20%/yr; life-threatening 1-3%/yr
WARNING: BLEEDING RISK
Budnitz DS et al. N Engl J Med. 2011; 365:2002-12.Holland L et al. Transfusion. 2009; 49:1171-7.
Peacock WF et al. Clin Cardiol. 2012; [Epub ahead of print].Coumadin (warfarin sodium) prescribing information. 2011 Oct (URL in ref list).
See full prescribing information for complete boxed warning.
• Warfarin sodium can cause major or fatal bleeding. (5.1)• Perform regular monitoring of INR in all treated patients. (2.1)• Drugs, dietary changes, and other factors affect INR levels achieved with
warfarin therapy. (7)• Instruct patients about prevention measures to minimize risk of bleeding and
to report signs and symptoms of bleeding. (17)
11

Kinetics of Warfarin and Clotting Factors
60
70
80
90
100
60
70
80
90
100
Warfarin steady c
once
ntra
tion
ing
fact
ors
(%)
II VII IX X Warfarin
Warfarin steady-stateconcentration achieved
0
10
20
30
40
50
0
10
20
30
40
50
y-state achieved (%)
Norm
al
of c
lott
Time (hours)
concentration achieved
Eckhoff CD et al. Ann Pharmacother. 2004; 38:2115-21.
Clinical Predictors of Prolonged Delay in Return of INR to Therapeutic Range
N 633 patients with INR > 6.0/various indicationsOutcome % patients with INR > 4.0 after holding warfarin x 2 daysAge 69 (25-95) [36% > 75 years]
INR > 4 after holding 2 doses 37%
Hylek EM et al. Ann Intern Med. 2001; 135:393-400.
OR p valueAge, per decade of life 1.18 0.04Index INR, per unit 1.25 <0.001Clinical CHF 2.79 0.009Active malignancy 2.48 0.03Weekly warfarin dose 0.87 0.009
per 10 mg increase
Properties of Novel Oral AnticoagulantsApixaban Dabigatran Rivaroxaban Edoxaban
Direct factor inhibition Xa IIa Xa Xa
Renal clearance 25% 80% 33% 40%
t½ in hours by CrCl (mL/min)
CrCl > 80 8‐15 14‐17 5‐9h 9‐11
Adapted from Kaatz S et al. Am J Hematol. 2012; 87(suppl 1):S141–5; Wittkowsky AK. Pharmacotherapy. 2011; 31:1175–91.
CrCl > 80 8‐15 14‐17 5‐9h 9‐11
CrCl 50 – 79 14.6 16.6 8.7 NA
CrCl 30 – 49 17.6 18.7 9.0 NA
CrCl < 30 17.3 27.5 9.5 NA
Dialyzable Unlikely Yes Unlikely Unlikely
Decreased renal function is associated with an increase in anticoagulant effect
NA = not available
12
See page 20 for enlarged view

Novel Anticoagulants for SPAFSafety Endpoint: Major Bleeding
2.5
3
3.5
4
4.5RELY ROCKET-AF ARISTOTLE
p<0.01GI bleed: p<0.001
ICH: p<0.001
GI bleed: p<0.001
ICH: p=0.02
0
0.5
1
1.5
2
Dabi 110 Dabi 150 Warfarin Riva Warfarin Apix WarfarinOther ICH GI bleed
Connolly SJ et al. N Engl J Med. 2009; 361:1139-51; Patel MR et al. N Engl J Med. 2011; 365:883-91; Granger CB et al. N Engl J Med. 2011; 365:981-92.
Institute for Safe Medication Practices: Serious Bleeding with Dabigatran
• ISMP QuarterWatch Report 2011
• Dabigatran linked to– 3781 serious adverse events
– 2367 cases of hemorrhage
– 542 patient deaths
http://www.ismp.org/QuarterWatch/pdfs/2011Q4.pdf
Ying – Yang Principle:Thrombosis vs. Bleeding
• With every approach to reduce thrombosis, there is an accompanying risk of increasing bleeding complications
• Conversely reducing bleeding complicationsConversely, reducing bleeding complications may increase thrombotic events– Both increase morbidity and mortality
• Balancing both ends of the spectrum is essential, and an individualized approach to therapy is advocated
13

Patient Case
• 69-year-old African American woman• HTN (uncontrolled 165/95), DM, CRI (CrCl 35
mL/min) and HLD• Presents to ER with dizziness and palpitations
EKG A i l fib ill i f 110 b• EKG: Atrial fibrillation, rate of 110 bpm• Exam: normal, Labs: WNL, Cr 1.5• Meds: lisinopril, simvastatin, glipizide• SH: ETOH (+), 2-3 drinks/day• Patient started on oral diltiazem XR 120 mg daily
Q1: This patient’s risk of a cardioembolic stroke is
a. Low
b. Moderate
c. High
d Super high ticking time bombd. Super high…ticking time bomb
Stroke Prevention in Atrial Fibrillation:Assessing Stroke Risk
CHADS2 ScoreRisk Factor ScoreCongestive heart failure 1
Hypertension 1
CHA2DS2-Vasc ScoreRisk Factor ScoreCongestive heart failure /
LV dysfunction1
H t i 1Age ≥ 75 years 1
Diabetes 1
Stroke or TIA history 2MAXIMUM 6
Hypertension 1
Age ≥ 75 years 2Diabetes 1
Stroke/TIA/TE history 2Vascular disease 1
Age 65 – 74 years 1
Sex category, female 1
MAXIMUM 9Gage BF et al. JAMA. 2001; 285:2864-70.Lip GY et al. Chest. 2010; 137:263-72.
14

CHADS2 score Chest (Grade of rec)
ACCF/AHA/HRS (Class of rec)
0 (low) No therapy (2B) Aspirin (I)
1(moderate) OAC (1B)Dabi > warfarin*
OAC or aspirin (IIa)Dabi alt to warfarin†
Stroke Prevention in Atrial Fibrillation:Guideline Recommendations
Dabi > warfarin* Dabi alt to warfarin†
≥ 2 (high) OAC (1A)Dabi > warfarin*
OAC (I)Dabi alt to warfarin†
You JJ et al. Chest. 2012;141(suppl 2):e531S-75S.Fuster V et al. Circulation. 2011; 123:e269-367. Wann SL et al. Circulation. 2011; 123:1144-50.
*Except in patients with CrCl < 30 mL/min, mitral stenosis, stable CAD, recent ACS, or s/p intracoronary stent†Except in patients with prosthetic heart valves, hemodynamically significant valvular heart disease, CrCl < 15 mL/min, or advanced liver disease
Rivaroxaban and apixaban not approved at time of guideline publication; not included
Q2: This patient’s risk of bleeding is
a. Low
b. Moderate
c. High
d Super high ticking time bombd. Super high…ticking time bomb
Q3: What is this patient’s HAS-BLED score?a. 1
b. 2
c. 3
d 4d. 4
15

Stroke Prevention in Atrial FibrillationBalancing Stroke and Bleeding Risk
HEMORR2HAGES ScoreRisk Factor ScoreHepatic or renal disease 1 ea
Ethanol use 1
Malignancy 1
Old > 75 1
HAS-BLED ScoreRisk Factor ScoreHypertension, SBP > 160 mmHg 1
Abnormal renal or liver function 1 ea
Stroke 2Older age: > 75 years 1
Reduced platelet count or Fxn 1 ea
Re-bleeding 2Hypertension, uncontrolled 1
Anemia 1
Genetic factors 1
Elevated fall risk ±neuropsychiatric disease
1
Stroke 1
MAXIMUM 14
Bleeding history or predisposition 1
Labile INRs 2Elderly: age > 65 years 1
Drugs or alcoholAntiplatelet or NSAID
Alcohol use: > 8 servings/week11
MAXIMUM 11
Gage BF et al. Am Heart J. 2006; 151:713-9.Pisters R et al. Chest. 2010; 138:1093-100.
Lip GY et al. J Am Coll Cardiol. 2011; 57:173-80.
Stroke Prevention in Atrial Fibrillation:ESC 2012 Guidelines
Camm AJ et al. Eur Heart J. 2012 Aug 24 [Epub ahead of print].
BleedingSURGERY / INVASIVE PROCEDURE
Perioperative Management Considerations
Thrombosis
SURGERY / INVASIVE PROCEDURE
See page 20 for enlarged view
16

Perioperative Management Considerations
• PRE-operative– Timing of when AC
is stopped is anchored on agent PK characteristics
• POST-operative– Consider the effect
of surgery, risk of bleeding, and bowel motility
and half-life– Aim to stop AC
agent before surgery so there is minimal or NO residual AC effect at the time of surgery
motility
– Resume once adequate hemostasis has been achieved
PRE-operative Management Considerations
• Minor surgery– Low bleeding risk
– Can have some residual AC effect at
• Major surgery– High bleeding risk
– Spinal anesthesia
– Aim to have time of surgery minimum or NO
residual AC effect at time of surgery
PRE-Operative Management Considerations
Number ofhalf-lives elapsed
% of Drug EffectRemaining
1 50
2 25
3 12 53 12.5
4 6.25
5 3.125
Allow longer period of time before surgery• Elderly• Known impaired renal function• Known clinical factors to cause delay in INR drop or
drug elimination for novel oral anticoagulants
17

Recommendations for Timing of Warfarin around Invasive Procedures
Discontinuation 5 days before scheduled procedure
Resumption “12 24 hours after surgery and whenResumption 12-24 hours after surgery and whenthere is adequate hemostasis”
(To minimize bleeding risk, use patient’s pre-operative dose rather than reloading)
Douketis JD et al. Chest. 2012; 141(suppl 2):e326S-50S.
Interruption of Novel Oral Anticoagulant Therapy for Invasive
Procedures and Surgerya
Drug(Renal Function)
No. of Doses to Skip before Minor Procedureb
No. of Doses to Skip before Major
Surgeryb
Dabigatran (CrCl > 50 mL/min) 1 or 2 4
Dabigatran (CrCl 50 mL/min) 3 or 4 6-8
Rivaroxaban (CrCl > 50 mL/min) 1 or 2 3 or 4
Apixaban 1 or 2 3 or 4
aResume therapy 24-48 hr after minor procedure, 48-72 hr after major surgery. If UFH or LMWH is used as bridging therapy in patients with atrial fibrillation, mechanical heart valve, or venous thromboembolism who are at high risk for thromboembolism, oral anticoagulant therapy should be resumed at least 1 hr after UFH infusion is discontinued and at least 10 hr after last dose of LMWH.bAssuming dabigatran is taken twice daily, rivaroxaban is taken once daily, and apixaban is taken twice daily.
Viles-Gonzalez JF et al. J Cardiovasc Electrophysiol. 2011; 22:948-55.
Measurement of Anticoagulation Effect
• Under- or overdosing
• Drug interactions
• Invasive procedures, surgery
• Thrombolytic therapy
• Progressive renal insufficiency
• Adherence assessment
y py
• Triple antithrombotic therapy
• Extremes of age, weight
18

Hematology Testing:Novel Oral AnticoagulantsUsefulness of Lab Test Dabigatran Rivaroxaban Apixaban
Lab tests Strong ECT Chromogenic anti-Xa
Chromogenic anti-Xa
TT aPTT, PT
aPTT
Weak PT/INR
Palladino M et al. Am J Hematol. 2012; 87(suppl 1):s127-32.
Summary• Assessment of bleeding risk must be objective with
the use of bleeding risk scores
• Health care providers must maintain a fine balance between thrombosis and bleeding in choosing and managing oral anticoagulant therapy
• Novel agents with multiple doses and indications
– Special attention to half-life and renal function
– Various agents will require different algorithms for managing invasive procedures and reversal approaches
19

Kinetics of Warfarin and Clotting Factors
100100
W
II VII IX X Warfarin
20
30
40
50
60
70
80
90
20
30
40
50
60
70
80
90
Warfarin steady-state achieved
Norm
al c
once
ntra
tion
of c
lotti
ng fa
ctor
s (%
)
Warfarin steady-stateconcentration achieved
0
10
0
10
d (%)
Time (hours)
Eckhoff CD et al. Ann Pharmacother. 2004; 38:2115-21.
Stroke Prevention in Atrial Fibrillation:ESC 2012 Guidelines
Camm AJ et al. Eur Heart J. 2012 Aug 24 [Epub ahead of print].
20

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
C L O T T I N G A S S A Y S Prothrombin time (PT)
Time in seconds for a clot to form after addition of calcium and thromboplastin to plasma
Thrombin time (TT) Measures the activity of thrombin in plasma
Ecarin clotting time (ECT) Directly measures thrombin generation
Activated partial thromboplastin time (aPTT) Measure of the intrinsic and final common pathway
Chromogenic anti-FXa assays Measure of coagulation during rivaroxaban and apixaban therapy
Others in development
Dilute prothrombin time (dPT) Heptest (American Diagnostica, Stamford, CT) Prothrombinase-induced clotting time (PiCT) Chromogenic anti-factor IIa assays
Miyares MA et al. Am J Health-Syst Pharm. 2012; 69:1473-84.
21

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L E C T E D R E F E R E N C E S
1. Budnitz DS, Lovegrove MC, Shehab N et al. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med. 2011; 365:2002-12.
2. Camm AJ, Lip GY, De Caterina R et al. 2012 focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation. Eur Heart J. 2012 Aug 24 [Epub ahead of print]. http://www.escardio.org/guidelines-surveys/esc-guidelines/GuidelinesDocuments/Guidelines_Focused_Update_Atrial_Fib_FT.pdf (accessed 2012 Sept 29).
3. Connolly SJ, Ezekowitz MD, Yusuf S et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009; 361:1139-51.
4. Coumadin (warfarin sodium) prescribing information. Princeton, NJ; Bristol-Myers Squibb; 2011 Oct. http://packageinserts.bms.com/pi/pi_coumadin.pdf (accessed 2012 Nov 9).
5. Douketis JD, Johnson JA, Turpie AG. Low-molecular-weight heparin as bridging anticoagulation during interruption of warfarin: assessment of a standardized periprocedural anticoagulation regimen. Arch Intern Med. 2004; 164:1319-26.
6. Douketis JD, Spyropoulos AC, Spencer FA et al. Perioperative management of antithrombotic therapy: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012; 141(suppl 2):e326S-50S.
7. Eckhoff CD, Didomenico RJ, Shapiro NL. Initiating warfarin therapy: 5 mg versus 10 mg. Ann Pharmacother. 2004; 38:2115-21.
8. Fuster V, Rydén LE, Cannom DS et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011; 123:e269-367.
9. Gage BF, Waterman AD, Shannon W et al. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001; 285:2864-70.
10. Gage BF, Yan Y, Milligan PE et al. Clinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF). Am Heart J. 2006; 151:713-9.
11. Granger CB, Alexander JH, McMurray JJ et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365:981-92.
12. Gulseth MP, Michaud J, Nutescu EA. Rivaroxaban: an oral direct inhibitor of factor Xa. Am J Health-Syst Pharm. 2008; 65:1520-9.
13. Holland L, Warkentin TE, Refaai M et al. Suboptimal effect of a three-factor prothrombin complex concentrate (Profilnine-SD) in correcting supratherapeutic international normalized ratio due to warfarin overdose. Transfusion. 2009; 49:1171-7.
22

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
14. Hylek EM, Regan S, Go AS et al. Clinical predictors of prolonged delay in return of
the international normalized ratio to within the therapeutic range after excessive anticoagulation with warfarin. Ann Intern Med. 2001; 135:393-400.
15. Institute for Safe Medication Practices. QuarterWatch monitoring FDA MedWatch reports: anticoagulants the leading reported drug risk in 2011. May 31, 2012. http://www.ismp.org/QuarterWatch/pdfs/2011Q4.pdf (accessed 2012 Sep 29).
16. Kaatz S, Kouides PA, Garcia DA et al. Guidance on the emergent reversal of oral thrombin and factor Xa inhibitors. Am J Hematol. 2012; 87(suppl 1):S141-5.
17. Lip GY, Frison L, Halperin JL et al. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. J Am Coll Cardiol. 2011; 57:173-80.
18. Lip GY, Nieuwlaat R, Pisters R et al. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on atrial fibrillation. Chest. 2010; 137:263-72.
19. Miyares MA, Davis K. Newer oral anticoagulants: a review of laboratory monitoring options and reversal agents in the hemorrhagic patient. Am J Health-Syst Pharm. 2012; 69:1473-84.
20. Palladino M, Thomson L, Swift B et al. Implementing the new oral anticoagulants into the hospital formulary. Am J Hematol. 2012; 87(suppl 1):S127-32.
21. Patel MR, Mahaffey KW, Garg J et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011; 365:883-91.
22. Peacock WF, Gearhart MM, Mills RM. Emergency management of bleeding associated with old and new oral anticoagulants. Clin Cardiol. 2012 Jul 18. [Epub ahead of print].
23. Pisters R, Lane DA, Nieuwlaat R et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010; 138:1093-100.
24. Roger VL, Go AS, Lloyd-Jones DM et al. Heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation. 2012; 125:e2-220.
25. Spyropoulos AC, Turpie AG, Dunn AS et al. Clinical outcomes with unfractionated heparin or low-molecular-weight heparin as bridging therapy in patients on long-term oral anticoagulants: the REGIMEN registry. J Thromb Haemost. 2006; 4:1246-52.
26. Viles-Gonzalez JF, Fuster V, Halperin JL. New anticoagulants for prevention of stroke in patients with atrial fibrillation. J Cardiovasc Electrophysiol. 2011; 22:948-55.
27. Wann SL, Curtis AB, Ellenbogen KA et al. 2011 ACCF/AHA/HRS focused update on the management of patients with atrial fibrillation (update on dabigatran): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011; 123:1144-50. [also available at J Am Coll Cardiol. 2011; 57:1330-7. http://content.onlinejacc.org/cgi/content/full/57/11/1330 (accessed 2012 Sept 29)].
23

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
28. Wittkowsky AK. Novel oral anticoagulants and their role in clinical practice.
Pharmacotherapy. 2011; 31:1175-91.
29. You JJ, Singer DE, Howard PA et al. Antithrombotic therapy for atrial fibrillation: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012; 141(suppl 2): e531S-75S.
24

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L F – A S S E S S M E N T Q U E S T I O N S
1. Which of the following scoring systems for bleeding risk assessment in patients with atrial fibrillation (AF) receiving oral anticoagulant therapy is recommended by the European Society of Cardiology?
a. CHADS2. b. CHA2DS2-Vasc. c. HAS-BLED. d. HEMORR2HAGES.
2. CB is a 75-year-old woman with decompensated congestive heart failure, breast
cancer, a creatinine clearance of 45 mL/min, and a new diagnosis of AF in whom stroke prophylaxis with a novel oral anticoagulant is contemplated. Which of these patient characteristics is most likely to affect the pharmacokinetics of novel oral anticoagulants and increase the risk for bleeding?
a. Decompensated congestive heart failure. b. Advanced age. c. Renal impairment. d. Active cancer.
3. CB’s CHA2DS2-Vasc score and risk for stroke is
a. 3, very high. b. 2, high. c. 1, intermediate. d. 0, low.
4. LM is a 57-year-old woman receiving rivaroxaban for AF who has a creatinine
clearance of 95 mL/min and plans to undergo elective coronary artery bypass graft surgery. How many doses should be withheld to prevent perioperative bleeding?
a. None. b. 1 or 2. c. 3 or 4. d. 6-8.
Answers
1. c 2. c 3. b 4. c
25

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
26

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
James S. Kalus, Pharm.D., BCPS (AQ-Cardiology) Senior Manager, Patient Care Services Department of Pharmacy Services Henry Ford Hospital Detroit, Michigan James S. Kalus, Pharm.D., BCPS (AQ-Cardiology), is Senior Manager of Patient Care Services in the Department of Pharmacy Services at Henry Ford Hospital in Detroit, Michigan. In this position, Dr. Kalus is responsible for planning, implementing, and managing all pharmacy services related to patient care. He also is responsible for formulary management, evaluation, and control. In addition, he oversees staff training and development, as well as pharmacy research. He is Program Director for the postgraduate year one (PGY-1) residency at Henry Ford Hospital and precepts a general inpatient cardiology rotation for pharmacy students and residents. Dr. Kalus earned both his Bachelor of Science in Pharmacy and Doctor of Pharmacy degrees at the University of Toledo in Toledo, Ohio. After completing a residency at the Medical University of South Carolina in Charleston, he did a two-year cardiovascular research fellowship through Hartford Hospital and the University of Connecticut in Hartford, Connecticut. Dr. Kalus was honored with the Outstanding Young Alumnus Award from the University of Toledo in 2009. Before assuming his current position, Dr. Kalus served as Assistant Professor at the Eugene Applebaum College of Pharmacy and Health Sciences at Wayne State University in Detroit, Michigan. He is board certified as a pharmacotherapy specialist with added qualifications in cardiology. In his research, Dr. Kalus focuses on cardiovascular disease, including the pathophysiology of atrial fibrillation (AF) occurring after cardiac surgery, novel strategies for the treatment and prevention of AF, and practice-based research related to anticoagulation. He has authored several textbook chapters and many articles published in peer-reviewed journals, including the American Journal of Health-System Pharmacy, Annals of Pharmacotherapy, Annals of Thoracic Surgery, Circulation, Journal of Electrocardiology, Journal of Hospital Medicine, Pharmacoeconomics, and Pharmacotherapy. He also serves on the editorial board of The Annals of Pharmacotherapy, Cardiology Panel. Complementing the practice and research interests of Dr. Kalus is his involvement in professional associations. An active member of the American Society of Health-System Pharmacists (ASHP), he regularly speaks at educational sessions at the ASHP Midyear Clinical Meeting. As a member of the 2007 Research Affairs Committee of the American College of Clinical Pharmacy, he co-authored the report, “Recommended Education for Pharmacists as Competitive Clinical Scientists,” published in March 2009. The Southeastern Michigan Society of Health-System Pharmacists honored him with the 2008 Preceptor of the Year Award and the 2006 Innovative Practice Award. He also has received the Drug Therapy Research Award from the ASHP Research and Education Foundation, and, in 2009, Dr. Kalus and his colleagues were finalists for the Foundation's Excellence in Medication Use Safety Award.
27
Options for Reversing the Effects of Oral Anticoagulants
James S. Kalus, Pharm.D., BCPS (AQ-Cardiology)Senior Manager, Patient Care Services
Henry Ford HospitalDetroit, Michigan
Learning Objectives
At the conclusion of this presentation,
participants will be able to
• Describe the relative benefits and li it ti f t ti l tlimitations of emergent anticoagulant reversal strategies
• Discuss the clinical evidence supporting the use of emergent anticoagulant reversal strategies
WARFARINWARFARIN
28

Q4: Which of the following patients taking warfarin would require pharmacologic reversal of anticoagulation? Select all that apply.
a. INR of 4, presenting to ED with complaints of hematemesis
b INR f 12 d i t f bl dib. INR of 12 and no signs or symptoms of bleeding
c. INR of 2.2, requiring emergent coronary artery bypass graft surgery
d. INR of 7 and no signs or symptoms of bleeding
Oral anticoagulation
Urgent procedure or bleeding
INR elevated
Clinical Scenarios for Reversal
INR < 10 INR > 10
Reversal of anticoagulation
INR < 10 INR > 10
Reversal of anticoagulation
Pharmacologic reversal not
indicated
Basis for Understanding Reversal
XIIa
XIa
IXa
Intrinsic Pathway Extrinsic Pathway
Tissue Factor
VIIaXI
XII
IX
VII
Xa
Thrombin (IIa)
Clot Stabilization
Fibrinogen
Fibrin
Platelet Activation
II
X X
LIVER
29

Vitamin K Dependent Factor Formation
Vitamin K Dependent Factor
Precursor
Vitamin K Dependent Factor
Oxidized Vitamin KReduced Vitamin K
Vitamin K Oxide Reductase
WARFARIN
Basis for Understanding Reversal
XIIa
XIa
IXa
Intrinsic Pathway Extrinsic Pathway
Tissue Factor
VIIaXI
XII
IX
VII
XX X
XXa
Thrombin (IIa)
Clot Stabilization
Fibrinogen
Fibrin
Platelet Activation
II
X XXX
XX
X
Reversal with Vitamin K
XIIa
XIa
IXa
Intrinsic Pathway Extrinsic Pathway
Tissue Factor
VIIaXI
XII
IX
VII
Xa
Thrombin (IIa)
Clot Stabilization
Fibrinogen
Fibrin
Platelet Activation
II
X X
LIVER
Exogenous vitamin K allows liver to
produce more II, VII, IX, X…
30
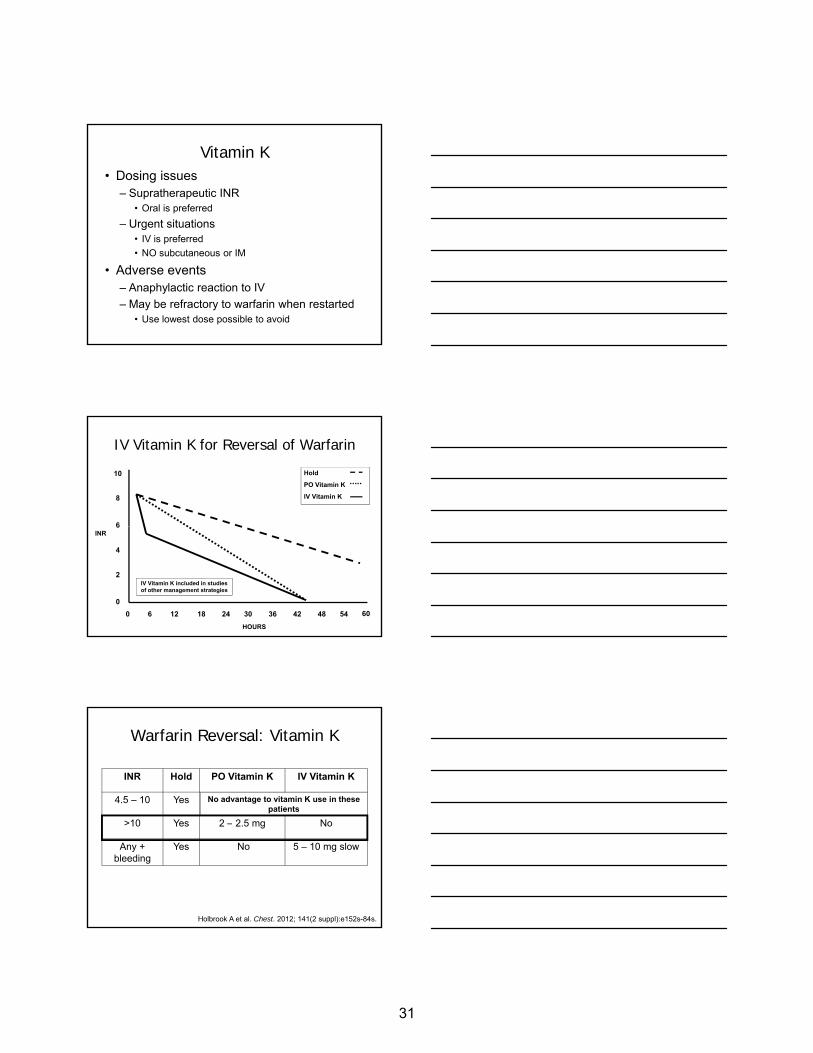
Vitamin K• Dosing issues
– Supratherapeutic INR • Oral is preferred
– Urgent situations• IV is preferred
• NO subcutaneous or IM
• Adverse events– Anaphylactic reaction to IV
– May be refractory to warfarin when restarted• Use lowest dose possible to avoid
IV Vitamin K for Reversal of Warfarin
10
8
6
Hold
PO Vitamin K
IV Vitamin K
6
4
2
00 6 12 18 24 30 36 42 48 54 60
INR
HOURS
IV Vitamin K included in studies of other management strategies
Warfarin Reversal: Vitamin K
INR Hold PO Vitamin K IV Vitamin K
4.5 – 10 Yes No NoNo advantage to vitamin K use in these patients
>10 Yes 2 – 2.5 mg No
Any + bleeding
Yes No 5 – 10 mg slow
Holbrook A et al. Chest. 2012; 141(2 suppl):e152s-84s.
31

Evidence: INR > 10 and No Bleeding
nOral Vitamin
K DoseAny Bleeding
(n)
Major Bleeding
(n)
Gunther 2004 89 2 mg Vitamin K = 0a
No vitamin K = 3a
n/a
Gunther KE et al. Thromb Res. 2004; 113:205-9.Crowther MA et al. Thromb Haemost. 2010; 104:118-21.
Crowther 2010 107 2.5 mg 16b 1b
Low rate of bleeding with oral vitamin K
No patients refractory to warfarin with oral vitamin K
aDay 3bDay 7
Reversal of Warfarin: Bleeding or Need for Emergent Surgery
Options• IV vitamin K
PLUS• Fresh frozen plasma (FFP)
OROR• Prothrombin complex concentrate (PCC)
OR• Recombinant factor VIIa (rFVIIa)
OR• Activated PCC (aPCC)
Fresh Frozen Plasma• How does it work?
– Contains all blood factors found in plasma
• Dosing– 1 unit ~ 200 – 250 mL
• Weight basedWeight based – 10 – 20 mL/kg 20 – 30% increase in any factor level
• “2 units FFP”
• Disadvantages– Volume of fluid administration – 400 mL or more!– Thawing may delay therapy– Infectious disease concerns– Hemolytic transfusion reactions and hypersensitivity
DomBourian M et al. J Infusion Nursing. 2012; 35:28-32.
32

Concentrated Blood Factor Products
rFVIIa 3-factor PCC
4-factor PCC
aPCC
Brand Names
Novo-Seven®
Bebulin VH®
Profilnine SD®
Octaplex®
Beriplex P/N®
Cofact®
FEIBA®
Kanokad®
U.S. Availability
Yes Yes No Yes
Factors Provided
VII II, IX, X II, VII, IX, X II, VII, IX, X
Activated? Yes No No Yes
Samama CM. Eur J Anaesthesiol. 2008; 25:784-9.
Prothrombin Complex Concentrates (PCCs)
Factor Profilnine SD® Beriplex P/N® Octaplex® Cofact®
II < 35-40 31 38 14-35
VII < 10 16 24 7-20
Approximate Factor Concentrations in Available PCCsa,b
VII < 10 16 24 7-20
IX 25 29 25 25
X < 25 41 30 14-35
aConcentration expressed as units/mL. bActual concentrations vary from lot to lot.
Profilnine SD (factor IX complex) prescribing information. 2010 Aug (URL in ref list).Samama CM. Eur J Anaesthesiol. 2008; 25:784-9.
Concentrated Blood Factors
• Dosing issues– Fixed dosing vs. weight based
– Extrapolating results reported in literature• Variability in factor concentrations by PCC product
• Adverse events– Prothrombotic potential
• Especially with “activated” products– rFVIIa, aPCC
• Anticipated benefit must outweigh prothrombotic risk– WHO should be reversed will be discussed in the next
presentation
33

Warfarin Reversal with a 3-Factor PCCStudy Holland and Colleagues
n 40 PCC/42 Controls
Patients INR > 5 with bleeding or at risk for bleeding
ICH excluded
Control group: historical controls
Holland L et al. Transfusion. 2009; 49:1171-7.
Dosing PCC low: profilnine 25 units/kg; High: profilnine 50 units/kg
FFP ~ 2 units per prescriber; Vitamin K 1 - 10 mg
Findings Target INR < 3 within 24 hours
Baseline INR: 8.6 – 9.4
Low and high dose had similar effect on INR
PCC alone: 43 – 55% achieved INR target
FFP alone: 62% achieved INR target
PCC + FFP: 89 – 93% achieved INR target
ICH = intracranial hemorrhage
p < 0.01
p < 0.01
Warfarin Reversal with 3-Factor PCC
Summary of Evidence
• Shortened time to reduction in INR– Faster than FFP alone
– Data limited by nonstandard monitoring after PCC
3 f t PCC tl t di d i dditi t FFP• 3-factor PCCs mostly studied in addition to FFP– Reduced FFP requirements
• Dose is typically 25 – 50 units/kg (IX)
• Lack of clinical outcome data
Boulis NM et al. Neurosurgery. 1999; 45:1113-8.Chapman SA et al. Ann Pharmacother. 2011; 45:869-75.
Holland L et al. Transfusion. 2009; 49:1171-7.Joseph B et al. J Trauma Acute Care Surg. 2012; 72:828-34.
10.4
8
10
12
Warfarin Reversal with a 4-Factor PCC
• Case series– 85 doses/82 patients
• Reversal strategy– Octaplex
• 1792 ± 601 units
– Vitamin K (69/85 doses)
5.83
3.01
1.43
5.08
0
2
4
6
Pre Post
Bleeding (n=36) Surgery (n=40) High INR (n=8) Mean
• 4.9 ± 5.5 mg
– FFP – not used
• Results– Mean INR ↓
• 3.98 ± 5.86
– Thrombosis: 3– Death: 7
• 4 surgical• 3 bleeding
P<0.0001
Song MM et al. Thromb Res. 2012; 129:526-9.
INR
34

Warfarin Reversal with a 4-Factor PCC:Impact on Outcomes
• Reversal due to bleeding– n = 212
• Randomized, open-label– 4-factor PCC (25 – 50 units/kg, based on INR)( g, )
– FFP (10 – 15 mL/kg, based on INR)
KEY FINDINGS
• Bleeding: similar at 24 hours
• INR correction: faster with 4-factor PCC
• Fluid overload: less with 4-factor PCCSarode R et al. Thrombosis and
Hemostasis Summit of North America, Chicago, IL: May 3-5, 2012.
Summary of Evidence• INR “normalized” in minutes to hours
– May normalize in as little as 15 – 20 minutes• 4-Factor PCCs effective for reducing INR without
FFPEff t bl di i il t FFP
Warfarin Reversal with a 4-Factor PCC
– Effect on bleeding similar to FFP• Dosing is often 25 – 50 units/kg (IX)
– Maybe fixed doses or INR-specific doses• Thromboembolic complications
– Infrequent, but have occurred• Surrogate endpoints Khorsand N et al. Transfus Med. 2011; 21:116-23.
Lubetsky A et al. Thromb Res. 2004;113:371-8.Pabinger I et al. J Thromb Haemost . 2008; 6:622-31.
Preston FE et al. Br J Haematol. 2002; 116:619-24.Song MM et al. Thromb Res. 2012; 129:526-9.
Warfarin Reversal with Factor VIIaRetrospective, Observational Study
> 18 y/o + traumatic ICH + warfarin use w/ INR > 1.3
Nishijima DK et al. Acad Emerg Med. 2010; 17:244-51.
Standard Management (n = 20)
FFP ± vitamin K
Other supportive measures or surgical interventions
Factor VIIa Management (n = 20)Factor VIIa (mean = 17.7 ± 6.2 mcg/kg)
FFP ± vitamin KOther supportive measures or surgical
interventions
35

Standard (n=20)
FVIIa (n=20) p-value
Initial INR 2.51 2.87 >0.05
FFP (units) 4.6 2.3 0.001
Vitamin K 800% 95.0% >0.05
Warfarin Reversal with Factor VIIa
Nishijima DK et al. Acad Emerg Med. 2010; 17:244-51.
Time to surgery 74.6 5.6 0.30
In-hospital mortality 35.0% 35.0% 1.0
Thromboembolism 5.0% 20.0% 0.15
INR < 1.3 68.4% 100% 0.02
Time to INR < 1.3 (hr) 17.5 4.8 <0.001
Factor VIIa(n = 15)
PCC* (n = 9)
Design: Retrospective cohort
Patients: Adult patients presenting with ICH, taking warfarin
Warfarin Reversal: 3-Factor PCC vs. Factor VIIa
Pinner NA et al. World Neurosurg. 2010; 74:631-5.
Baseline INR 6.1# 2.3^
1-hour INR 1.1# 1.48^
Treatment dose 53.4 mcg/kg 27.8 units/kg
Vitamin K dose 17.8 ± 14.6 mg 17.1 ± 12.9 mg
FFP 1025 ± 828 mL 778 ± 484 mL
*Bebulin VH, 3-factor PCC
#n = 6; ^n = 5
Warfarin Reversal: 3-Factor PCC vs. Factor VIIa
60% 60%
83%
93%
50%50%60%70%80%90%
100%
%
Pinner NA et al. World Neurosurg. 2010; 74:631-5.
Unexpected response to PCC due to low use of FFP ± vitamin K?
17%
33%
20%
0%10%20%30%40%
Vitamin K Use FFP Use INR </= 1.3 (1 hr) INR </= 1.3 (6 hrs)
Factor VIIa PCC
36
vyarborough
Line

“Building” a 4-Factor PCCPatients
• Warfarin related ICH, INR ≥ 1.6 (46)
• Historical controls (12)
Reversal strategy
• IV Vitamin K 5 mg slow IV
• PCC 4000 units
Factor VIIa 1 mg
2.5
3
3.5
Reversal Agent Impact on INR
Complications
2 NSTEMI
• 1 occurred 8 hours post PCC+FVIIa
• 1 occurred 3 days later
Mortality
24 hours – 5/46
72 hours – 8/46
Sarode R et al. J Neurosurg. 2012; 116:491-7.
*
• Factor VIIa 1 mg
*
*PCC+VIIa less than FFP and PCC+FFP (p<0.05)
0
0.5
1
1.5
2INR
Baseline Post-Infusion 24 hours
PCC+VIIa (46) FFP (3) PCC+FFP (9)
* *
Warfarin Reversal: aPCCPatients
• Patients requiring reversal (n = 72)
• Historical controls receiving FFP (n = 69)
Reversal strategy
• IV Vitamin K 10 mg slow IV
• aPCC 500 units if INR < 58
10
12
14
Impact on INR
• aPCC 1000 units if INR ≥ 5
• FFP dosing in control patients
- Discretion of prescriber (~2 units)
Other results
• Time to INR < 1.4
- 2 hr vs. 25 hr (p = 0.006)
Thromboembolic complications
• 1 venous thromboembolism
• 3 possible episodes of cardiac ischemia
Wojcik et al. Int J Emerg Med. 2009; 2:217-25.
0
2
4
6
8INR
aPCC(<5)
aPCC(>5)
aPCC(ALL)
FFP(<5)
FFP(I>5)
FFP(ALL)
Baseline Post-Reversal
Options for Reversal of Warfarin
10
8
6
Hold
PO Vitamin K
IV Vitamin K
Factors*
6
4
2
00 6 12 18 24 30 36 42 48 54 60
INR
HOURS*Generally reflects co-administration of vitamin K ± FFP
37

Urgent Warfarin Reversal:Bleeding or Surgery
Clinical Scenario Reversal ApproachBleeding Vitamin K 5 – 10 mg slow IV + 4-factor PCC†
Surgery in < 24 hours IV vitamin K 5 – 10 mg slow IV
+
Either 4-factor PCC#, factor VIIa or aPCC‡
Cartmill M et al. Br J Neurosurg. 2000; 14:458-61; Fredriksson K et al. Stroke. 1992; 23:972-7; Holbrook A et al. Chest. 2012; 141(Suppl):e152s-184s; Huttner HB et al. Stroke. 2006; 37:1465-70;
Makris M et al. Thromb Haemost. 1997; 77:477-80; Nishijima DK et al. Acad Emerg Med. 2010; 17:244-51; Wojcik C et al. Int J Emerg Med. 2009; 2:217-25.
,
Surgery in > 24 hours May have time to use IV vitamin K alone‡
†Recommendation based on CHEST Guidelines (2C).‡Recommendation based on published literature and pharmacodynamics of vitamin K.#Note: 4 factor PCC not yet available in the United States, FFP or factor VIIa may be needed in addition to a 3-factor PCC to achieve desired effect on INR.
What can we do in the United States?
• Add FFP to either 3-factor PCC or factor VIIa– FFP may not be tolerated by all
3 factor PCC + Factor VIIa• 3-factor PCC + Factor VIIa
• aPCC alone
4-factor PCC approval soon?
Cost Implications of ReversalAgent FFP +
PCCPCC +
VIIaaPCC
FFP (15 mL/kg) $300
3-factor PCC (25 units/kg) $1932 $1932
Factor VIIa (20 mcg/kg) $2820
aPCC (1000 units) $1800
Cost/reversal regimen $2232 $4752 $1800
• Assumes 80-kg patient and rounding to nearest vial size.• Acquisition cost (average wholesale price) for FFP = $60 per unit,
PCC = $0.97/unit, factor VIIa = $1410/1-mg vial, aPCC = $1800/1056 units.
38

Q5: 75-year-old patient presents with new onset loss of consciousness and is found to have ICH. She takes warfarin 2.5 mg daily, and her INR is 3.2 today.Which of the following could be used alone to lower her INR?
a. Oral vitamin Kb. An activated PCC c. A 3-factor PCCd. IV vitamin K
DABIGATRAN and RIVAROXABAN
How do we reverse them?
• Not really sure
• Largely theoretical
• Based on very limited data– Animal models
– Healthy volunteer studies
– Case reports
39
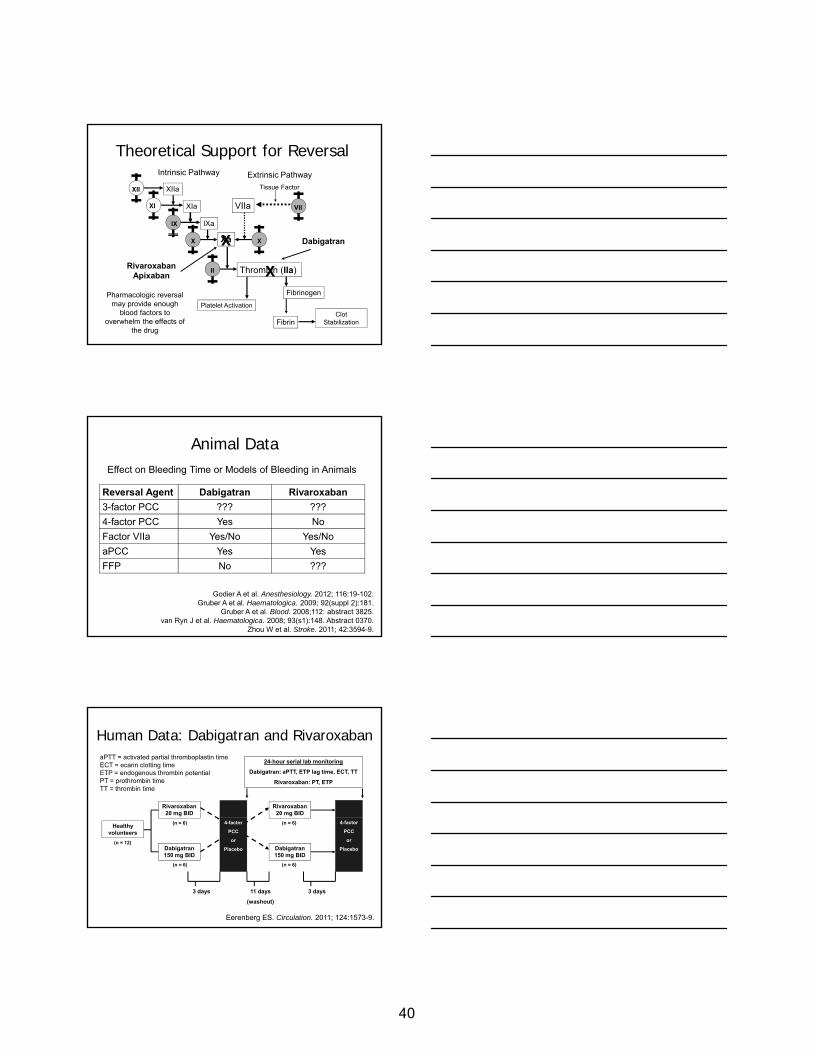
Theoretical Support for Reversal
XIIa
XIa
IXa
Intrinsic Pathway Extrinsic Pathway
Tissue Factor
VIIaXI
XII
IX
VII
Xa
Thrombin (IIa)
Clot Stabilization
Fibrinogen
Fibrin
Platelet Activation
II
X X
RivaroxabanApixaban
X Dabigatran
XPharmacologic reversal
may provide enough blood factors to
overwhelm the effects of the drug
Animal Data
Reversal Agent Dabigatran Rivaroxaban3-factor PCC ??? ???
4-factor PCC Yes No
Effect on Bleeding Time or Models of Bleeding in Animals
Godier A et al. Anesthesiology. 2012; 116:19-102.Gruber A et al. Haematologica. 2009; 92(suppl 2):181.
Gruber A et al. Blood. 2008;112: abstract 3825.van Ryn J et al. Haematologica. 2008; 93(s1):148. Abstract 0370.
Zhou W et al. Stroke. 2011; 42:3594-9.
Factor VIIa Yes/No Yes/No
aPCC Yes Yes
FFP No ???
Human Data: Dabigatran and Rivaroxaban
Rivaroxaban 20 mg BID
Rivaroxaban 20 mg BID
24-hour serial lab monitoring
Dabigatran: aPTT, ETP lag time, ECT, TT
Rivaroxaban: PT, ETP
aPTT = activated partial thromboplastin timeECT = ecarin clotting timeETP = endogenous thrombin potentialPT = prothrombin timeTT = thrombin time
Eerenberg ES. Circulation. 2011; 124:1573-9.
Dabigatran 150 mg BID
Healthy volunteers
Dabigatran 150 mg BID
(n = 12)
(n = 6)
(n = 6)
(n = 6)
(n = 6)
4-factor
PCC
or
Placebo
4-factor
PCC
or
Placebo
3 days 3 days11 days
(washout)
40

Dabigatran
• No effect of PCC on ANY measure of coagulation
Ri b
Human Data: Dabigatran and Rivaroxaban
Rivaroxaban
• PT– Normalized within 15 minutes (p<0.001)
• ETP– Normalized within 15 minutes (p<0.001)
Eerenberg ES. Circulation. 2011; 124:1573-9.
Ex Vivo Study:Dabigatran and Rivaroxaban
Dabigatran 150-mg single
dose
OR2 hours
Blood Drawn• Endogenous thrombin
potential (ETP)
• Peak thrombin
Blood Exposed to
aPCC
Factor VIIa
Marlu R et al. Thromb Haemost. 2012; 108:217-24.
OR
Rivaroxaban 20-mg single
dose
generation (PEAK)
• Lag time (LT)
• Time to peak thrombin (TTP)
4-factor PCC
3 different concentrations of
each
Measures of thrombin generation
Ex Vivo Study:Dabigatran and Rivaroxaban
Summary of Findings• 4-factor PCC and factor VIIa
– Inconsistent impact on thrombin generation• Dabigatran patient blood• Rivaroxaban patient blood
Marlu R et al. Thromb Haemost. 2012; 108:217-24.
• Rivaroxaban patient blood
• aPCC – Consistent impact on thrombin generation
• Rivaroxaban patient blood
– Less consistent impact on thrombin generation• Dabigatran
– Still better than PCC and factor VIIa
41

Dabigatran: Factor VIIa and Hemodialysis
• 79-year-old man, CrCl = 36 mL/min• Dabigatran 150 mg twice daily• Required aortic valve replacement/CABG
– Dabigatran held x 2 days prior to surgery
• Massive bleeding postoperatively– Managed with 5 doses of factor VIIa
• 2.4 mg/dose x 3 dose + 7.2 mg/dose x 2 doses
– Hemodialysis x 6 hours
• Supports previous pharmacokinetics study data suggesting 60 – 70% removal of dabigatran dose
Warkentin TE et al. Blood. 2012; 119:2172-4.Stangier J et al. Clin Pharmacokinet. 2010; 49:259-68.
Dabigatran: Perioperative Management
Renal function (CrCl, mL/min)
Half-life (hours) Time of last dabigatran dose before surgery
Standard bleeding risk
High bleeding risk
> 80 13 24 hours 2 – 4 days
DABIGATRAN
van Ryn J et al. Thromb Haemost. 2010; 103:1116–27.
> 50 to 80 15 24 hours 2 – 4 days
> 30 to 50 18 At least 48 hours
4 days
< 30 27 2 – 5 days > 5 days
A high bleeding risk is associated with cardiac surgery, neurosurgery, abdominal surgery, and surgeries involving a major organ, advanced age, spinal anesthesia and other procedures in which complete hemostatic function is required, comorbid conditions (e.g., major cardiac, respiratory, or liver disease) and concomitant use of antiplatelet therapy.
Rivaroxaban: Perioperative Management
CrCl (mL/min)
>80(n = 8)
50 – 79(n = 8)
30 – 49(n = 8)
<30(n = 8)
Half-life (hr) 8.3 8.7 9.0 9.5
RIVAROXABAN
• AUC ↑ as CrCl ↓• Most rivaroxaban clearance
– Non-renal (hepatic)– Renal secretion
• High protein binding• Limited clearance by glomerular filtration
Kubitza D et al. Br J Clin Pharmacol. 2010; 70:703-12.
42

Urgent Reversal of Novel Anticoagulants:Bleeding or Surgery
Possible strategies
• aPCC– Supported by animal and limited human data
• 3-factor PCC plus factor VIIa– Mimic effects of aPCC
• Maybe a 4-factor PCC– Conflicting animal data, limited human data
Urgent Reversal of Novel Anticoagulants:Practical Considerations
Dabigatran• Charcoal after recent ingestion• Renal impairment complicates reversal
– Role for hemodialysisRivaroxabanRivaroxaban• Less reliance on renal clearanceDosing• Very little guidance
– Higher doses than usual?Patient selection• Risk vs. benefit
Conclusions
Warfarin reversal• Concentrated blood factors > FFP alone
– All studies have some methodologic limitations
Reversal of dabigatran and rivaroxaban• Concentrated blood factors may have a role
– aPCC or 4-factor PCCs may be best approach– Extremely limited data– Human data lacking
Lack of clear benefit + risk of blood factor products• Proper patient selection is critical
43

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L E C T E D R E F E R E N C E S
1. Bebulin (factor IX complex) prescribing information. Westlake Village, CA: Baxter Healthcare Corporation; 2011 Apr. http://www.baxter.com/downloads/healthcare_professionals/products/bebulin-vh_pi.pdf (accessed 2012 Nov 9).
2. Beriplex P/N summary of product characteristics. Marburg, Germany: CSL Behring; 2011 Jul. http://www.medicines.org.uk/EMC/medicine/21147/SPC/Beriplex+P+N+250+%26+500+IU/ (accessed 2012 Nov 9).
3. Boulis NM, Bobek MP, Schmaier A et al. Use of factor IX complex in warfarin-related intracranial hemorrhage. Neurosurgery. 1999; 45:1113-8.
4. Cartmill M, Dolan G, Byrne JL et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000; 14:458-61.
5. Chapman SA, Irwin ED, Beal AL et al. Prothrombin complex concentrate versus standard therapies for INR reversal in trauma patients receiving warfarin. Ann Pharmacother. 2011; 45:869-75.
6. Crowther MA, Garcia D, Ageno W et al. Oral vitamin K effectively treats international normalized ratio (INR) values in excess of 10: results of a prospective cohort study. Thromb Haemost. 2010; 104:118-21.
7. DomBourian M, Holland L. Optimal use of fresh frozen plasma. J Infus Nurs. 2012; 35:28-32.
8. Eerenberg ES, Kamphuisen PW, Sijpkens MK et al. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011; 124:1573-9
9. FEIBA NF (anti-inhibitor coagulant complex) prescribing information. Westlake Village, CA: Baxter Healthcare Corporation; 2011 Feb. http://www.baxter.com/downloads/healthcare_professionals/products/feiba-nf-pi.pdf (accessed 2012 Nov 9).
10. Fredriksson K, Norrving B, Stromblad LG. Emergency reversal of anticoagulation after intracerebral hemorrhage. Stroke. 1992; 23:972-7.
11. Godier A, Miclot A, Le Bonniec B et al. Evaluation of prothrombin complex concentrate and recombinant activated factor VII to reverse rivaroxaban in a rabbit model. Anesthesiology. 2012; 116:94-102.
12. Gruber A, Marzek UM, Buetehorn U et al. Potential of activated complex concentrate and activated factor VII to reverse the anticoagulant effects of rivaroxaban in primates. Blood. 2008; 112:abstract 3825. http://abstracts.hematologylibrary.org/cgi/content/abstract/112/11/3825?maxtoshow=&hits=10&RESULTFORMAT=&fulltext=gruber&searchid=1&FIRSTINDEX=0&volume=112&issue=11&resourcetype=HWCIT (accessed 2012 Oct 8).
13. Gruber A, Marzek UM, Buetehorn U et al. Potential of activated complex concentrate and activate factor VII to reverse the anticoagulant effects of rivaroxaban in primates. Haematologica. 2009; 92(suppl 2):181.
44

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
14. Gunther KE, Conway G, Leibach L et al. Low-dose oral vitamin K is safe and
effective for outpatient management of patients with an INR>10. Thromb Res. 2004; 113:205-9.
15. Holbrook A, Schulman S, Witt DM et al. Evidence-based management of anticoagulant therapy. Antithrombotic therapy and prevention of thrombosis, 9th edition: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012; 141(2 suppl):e152s-84s.
16. Holland L, Warkentin TE, Refaai M et al. Suboptimal effect of a three-factor prothrombin complex concentrate (Profilnine-SD) in correcting supratherapeutic international normalized ratio due to warfarin overdose. Transfusion. 2009; 49:1171-7.
17. Huttner HB, Schellinger PD, Hartmann M et al. Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy: comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates. Stroke. 2006; 37:1465-70.
18. Joseph B, Amini A, Friese RS et al. Factor IX complex for the correction of traumatic coagulopathy. J Trauma Acute Care Surg. 2012 ;72:828-34.
19. Kanokad summary of product characteristics. Paris, France: LFB-Biomedicaments; 2009 Feb. http://www.has-sante.fr/portail/upload/docs/application/pdf/2011-03/kanokad_ct_6278.pdf (accessed 2012 Oct 17).
20. Khorsand N, Veeger NJ, Muller M et al. Fixed versus variable dose of prothrombin complex concentrate for counteracting vitamin K antagonist therapy. Transfus Med. 2011; 21:116-23.
21. Kubitza D, Becka M, Mueck W et al. Effects of renal impairment on the pharmacokinetics, pharmacodynamics and safety of rivaroxaban, an oral, direct Factor Xa inhibitor. Br J Clin Pharmacol. 2010; 70:703-12.
22. Lubetsky A, Hoffman R, Zimlichman R et al. Efficacy and safety of a prothrombin complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004; 113:371-8.
23. Makris M, Greaves M, Phillips WS et al. Emergency oral anticoagulant reversal: the relative efficacy of infusions of fresh frozen plasma and clotting factor concentrate on correction of the coagulopathy. Thromb Haemost. 1997; 77:477-80.
24. Marlu R, Hodaj E, Paris A et al. Effect of non-specific reversal agents on anticoagulant activity of dabigatran and rivaroxaban: a randomised crossover ex vivo study in healthy volunteers. Thromb Haemost. 2012; 108:217-24.
25. Nishijima DK, Dager WE, Schrot RJ et al. The efficacy of factor VIIa in emergency department patients with warfarin use and traumatic intracranial hemorrhage. Acad Emerg Med. 2010; 17:244-51.
26. NovoSeven RT (coagulation factor VIIa, recombinant, room temperature stable) prescribing information. Princeton, NJ: Novo Nordisk Inc; 2012 Jan. http://www.novo-pi.com/novosevenrt.pdf (accessed 2012 Nov 9).
27. Pabinger I, Brenner B, Kalina U et al. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008; 6:622-31.
45

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
28. Pinner NA, Hurdle AC, Oliphant C et al. Treatment of warfarin-related intracranial
hemorrhage: a comparison of prothrombin complex concentrate and recombinant activated factor VII. World Neurosurg. 2010; 74:631-5.
29. Preston FE, Laidlaw ST, Sampson B et al. Rapid reversal of oral anticoagulation with warfarin by a prothrombin complex concentrate (Beriplex): efficacy and safety in 42 patients. Br J Haematol. 2002; 116:619-24.
30. Profilnine SD (factor IX complex) prescribing information. Los Angeles: Grifols Biologicals Inc.; 2011 Aug. http://www.grifols.com/Controller?_fb=pfch&pAction=_factory&file=profil9-ft.pdf&_fp=0&idPortlet=15341&idval=385714 (accessed 2012 Nov 9).
31. Samama CM. Prothrombin complex concentrates: a brief review. Eur J Anaesthesiol. 2008; 25:784-9
32. Sarode R, Matevosyan K, Bhagat R et al. Rapid warfarin reversal: a 3-factor prothrombin complex concentrate and recombinant factor VIIa cocktail for intracerebral hemorrhage. J Neurosurg. 2012; 116:491-7.
33. Sarode R, Milling TJ, Refaai MA et al. Integrated safety analysis of a 4-factor prothrombin complex concentrate versus plasma in phase III clinical trials. Poster presented at Thrombosis and Hemostasis Summit of North America, Chicago, IL: May 3-5, 2012. http://cdn.f1000.com/posters/docs/249931755 (accessed 2012 Oct 1).
34. Song MM, Warne CP, Crowther MA. Prothrombin complex concentrate (PCC, Octoplex) in patients requiring immediate reversal of vitamin K antagonist anticoagulation. Thromb Res. 2012; 129:526-9.
35. Stangier J, Rathen K, Stahle H et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate. An open-label, parallel-group, single-center study. Clin Pharmacokinet. 2010; 49:259-68.
36. van Ryn J, Ruehl D, Priepke H et al. Reversibility of the anticoagulant effect of high doses of the direct thrombin inhibitor dabigatran, by recombinant factor VIIa or activated prothrombin complex concentrate. Haematologica. 2008; 93(s1):148. Abstract 0370. http://online.haematologica.org/eha13/browserecord.php?-action=browse&-recid=1923 (accessed 2012 Oct 1).
37. van Ryn J, Stangier J, Haertter S et al. Dabigatran etexilate--a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010; 103:1116–27.
38. Warkentin TE, Margetts, P, Connolly S et al. Recombinant factor VIIa (rFVIIa) and hemodialysis to manage massive dabigatran-associated postcardiac surgery bleeding. Blood. 2012; 119:2172-4.
39. Wojcik C, Schymik ML, Cure EG. Activated prothrombin complex concentrate factor VIII inhibitor bypassing activity (FEIBA) for the reversal of warfarin-induced coagulopathy. Int J Emerg Med. 2009; 2:217-25.
40. Zhou W, Schwarting S, Illanes S et al. Hemostatic therapy in experimental intracerebral hemorrhage associated with the direct thrombin inhibitor dabigatran. Stroke. 2011; 42:3594-9.
46

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L F – A S S E S S M E N T Q U E S T I O N S
1. DB is an 85-year-old woman who underwent hip fracture surgery 2 weeks ago, receives warfarin for venous thromboembolism prophylaxis, and comes to the clinic for a checkup. Her INR is 8, but she has no signs or symptoms of bleeding. Which of the following interventions is indicated for DB?
a. Vitamin K. b. Fresh frozen plasma (FFP). c. Three-factor prothrombin complex concentrate (PCC) + recombinant factor VIIa
(rFVIIa). d. No intervention is needed.
2. Which of the following vitamin K doses should be given to DB if she returns a week
later with confusion about what medications to take, an INR of 11, and no signs of bleeding?
a. 2-2.5 mg orally. b. 5-10 mg orally. c. 2-2.5 mg by slow intravenous (i.v.) injection. d. 5-10 mg slow i.v. injection.
3. All of the following concentrated blood factor products could be added for DB if she
requires additional surgery on an emergent basis, EXCEPT a. Four-factor PCC. b. Activated PCC (aPCC). c. rFVIIa. d. 3-factor PCC.
4. Which of the following concentrated blood factor products have been used in
combination to build a four-factor PCC product for urgent reversal in patients with warfarin-related intracranial hemorrhage (ICH) and elevated INR values in the United States where four-factor PCC products currently are not available?
a. FFP + aPCC. b. FFP + rFVIIa. c. rFVIIa + three-factor PCC. d. aPCC + rFVIIa.
Answers
1. d 2. a 3. d 4. c
47

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
48

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
William E. Dager, Pharm.D., BCPS (AQ-Cardiology) Pharmacist Specialist UC Davis Medical Center Sacramento, California William E. Dager, Pharm.D., BCPS (AQ-Cardiology), is a pharmacist specialist at UC Davis Medical Center in Sacramento, California, where he is responsible for managing challenging cases in anticoagulation, pharmacokinetics, and critical care. He also is clinically active with the cardiology service and serves as the director of the postgraduate year two (PGY-2) residency in cardiology at UC Davis. In addition, Dr. Dager holds three academic positions. He is Clinical Professor of Pharmacy at the University of California, San Francisco (UCSF) School of Pharmacy and Clinical Professor of Medicine at the University of California, Davis (UC Davis) School of Medicine. He also serves as Clinical Professor at the Touro School of Pharmacy in Vallejo, California. Dr. Dager earned his Doctor of Pharmacy degree at UCSF and completed a residency at the UC Davis Medical Center in Sacramento. In addition, he completed the University of Pittsburgh Nephrology Pharmaceutical Care Preceptorship. He is a board-certified pharmacotherapy specialist and fellow of the American College of Clinical Pharmacy (ACCP), American Society of Health-System Pharmacists (ASHP), California Society of Hospital Pharmacists, and Society of Critical Care Medicine (SCCM). Dr. Dager's research interests focus on anticoagulation, critical care medicine, cardiovascular disease, and pharmacokinetics and pharmacodynamics. He has authored numerous articles, book chapters, and scientific reviews, and he coauthored “Anticoagulation Therapy: A Point-of-care Guide” published by ASHP in 2011. He also regularly makes presentations at national and international educational conferences. Dr. Dager serves as a reviewer and editorial board member for several medical journals, and he currently is chair of the Editorial Advisory Board Panel on Anticoagulation for The Annals of Pharmacotherapy. He has served as a site coordinator for the ASHP Research and Education Foundation Antithrombotic Pharmacotherapy Traineeship. Dr. Dager has received multiple teaching and professional awards, including the 2008 ACCP Best Practice Award.
49

Practical Issues in Developing an Oral AnticoagulantReversal Strategy
William E. Dager, Pharm.D., BCPS (AQ-Cardiology)
Pharmacist Specialist
UC Davis Medical Center
Sacramento, California
Learning Objectives
At the conclusion of this presentation,
participants will be able to• Explain patient-specific treatment options for
reversing the effects of oral anticoagulants usingreversing the effects of oral anticoagulants using laboratory observations
• Develop an approach to managing major bleeding in a patient on oral anticoagulation therapy
• 75 yo with AF, CKD V, heart failure, and CVA on warfarin 1 mg/day and has a GI bleed. INR = 12
• 56 yo with mechanical MVR brought into ED after
Warfarin Situations
crashing his motorcycle. Had notable abdominal injuries with hemorrhage apparent. INR = 3.0
• 27 yo with PE 1 year ago being assessed for colonoscopy. Warfarin 15 mg/day. INR = 2.5
50

• Bleeding?• Site: risk of a complication
• Level of anticoagulationLaboratory assay
Skill: Assess the Situation
– Laboratory assay
– Antiplatelet agents?
• Hold anticoagulant
• Mechanical intervention
• Pharmacologic intervention• Intensity of anticoagulation (prior and post)
• Goal or need for re initiating therapy
Skill: Explore Options
• Goal or need for re-initiating therapy
• Neutralize the drug
• Reverse the effects of the drug independently
• Replace losses
• Optimize management of co-morbid situations
Skill: Consider the Entire Needs of the Patient
• Create a plan and request necessary follow up
• Evaluate thrombosis risks
51

Reversing Warfarin
Vitamin K (IV or PO) – 0.25 – 10 mg
Fresh frozen plasma (FFP)
Prothrombin complex concentrate (PCC)PCC3 s PCC4 s acti ated PCC• PCC3 vs. PCC4 vs. activated PCC
• 25-50 units/kg depending on patient’s weight, INR, and bleeding
Recombinant activated factor VII (rFVIIa)• Low (1-2 mg) vs. high dose
Dougherty J. In Dager WE et al. Anticoagulation therapy. 2011:123-54.Dager WE. Ann Pharmacotherapy. 2011; 45:1016-20.
IVHow Reliable Is the Laboratory
Information?• Single value?• Rapidly rising vs falling• INR: What is the difference between
6 and 12?
WarfarinINR assay (How High) • Rising vs. falling INR (? 1.8 > 2.2)
– Not reliable in first days (factor VII driven)
• False DTI, UFH elevation– UFH (neutralization step in Lab?)
Hylek et al: INR > 6 Risk Factors - INR 4 post 2-day hold
• Age per decade of life
• Initial INR (per 1.0 unit)
• Heart failure
• Weekly warfarin dose (per 10-mg increase)
• Active cancer
Hylek EM et al. Ann Intern Med. 2001; 135:393-400.
52
Using Vitamin K• What dose?
– How fast do we need a response
• What route?
– PO or IV (avoid SC or IM)
• Are other more rapid therapies planned (PCC, rFVIIa, FFP)
• Administration
– Infusion rate – Max 1 mg/min (over ~15 – 20 min)
– Light sensitive (~50 mL, avoid delay using large volumes)
– Anaphylaxis concerns (3:10,000 risk)
Riegert-Johnson DL et al. Ann Allergy Asthma Immunol. 2002; 89:400-6.
Vitamin K for Reversing WarfarinVit K IV: doses > 2 mg IV• Did not increase rate of reversal• ↑ dose → prolonged periods of bridging therapy
5
6
7
Tsu LV et al. Annals Pharmacother. In press.
0
1
2
3
4
0.25‐0.5 1‐1.25 2‐2.5 3‐5 10
INR
Vitamin K dose (mg)
BL
12 hours
24 hours
48 hours
n=22 n=39 n=10 n=23 n=6
Reversing Warfarin
rFVIIaPCC
53

What Improves Outcomes in Warfarin-related ICH?
• A good stitch– STICH Trial: ? Any impact of neurosurgery on improved outcomes
• Dowlatshahi et al. Stroke. 2012 – PCC rapidly reversed the INR, but did not change mortality and
morbiditymorbidity
• PCC shorten time to surgical procedures– Surgery may improve ICU-related outcomes
• Caution rebound
• Effects rapid – Retrospective studies may not have control on INR times
Mendelow AD et al. Lancet. 2005; 365:387-97; Dowlatshahi D et al. Stroke. 2012; 43:1812-7; Demeyere R et al. Vox Sang. 2010; 99:251-60; Chong CT et al. AnaesthIntensive Care. 2010; 38:474-80; Dager WE. Ann Pharmacother. 2011; 45:1016-20.
Hemostatic Agents and Thrombosis:After all… the patient was being anticoagulated!After all… the patient was being anticoagulated!
Hsia et al: Retrospective, single center analysis of off-label use (n=69)Mean dose = 8.2 mg rFVIIa
•36 thrombotic events, mean 8.8 days post rFVIIa•MD questioner: Not aware of any thrombotic events in these patients
rFVIIa or PCC Tissue Factor Expression ThrombosisTF
rFVIIa or PCC
TF also expressed on monocytes
rFVIIa or PCC
Thromboembolism:Thromboembolism: PCC4 (~1.8%) vs. PCC3 (0.7%)PCC4 (~1.8%) vs. PCC3 (0.7%)
Hsia CC et al. Transfus Med. 2009;19:43-9.Dentali F et al. Thromb Haemost. 2011; 106:429-38.
PCC Considerations• INR > 4.5 may not have sufficient rFVIIa (needs confirmation)
• UFH in PCC may increase risk for HIT
• Not recommended if AT deficiency
• Balanced PCC may be advantage in VKA reversal to decrease complications (needs confirmation)p ( )– ↓ Regulatory anticoagulant proteins C and S → ↑ thrombogenicity
• PCCs reduce the INR within 10 minutes
• PCC 4 in the USA soon?
Rodgers GM. Am J Hematol. 2012; 87:898-902.
54

• 75 yo with AF, CKD V, heart failure, and CVA on warfarin 1 mg/day and has a GI bleed. INR = 12
• 56 yo with mechanical MVR brought into ED after
Warfarin Situations
crashing his motorcycle. Had notable abdominal injuries with hemorrhage apparent. INR = 3.0
• 27 yo with PE 1 year ago being assessed for colonoscopy. Warfarin 15 mg/day. INR = 2.5
Dabigatran Reversal Case
AC Jr. is a 85 yo man with acute decompensated heart failure and receiving dabigatran 150 mg PO BID for AF. He has fallen and hit his head and is being admitted to the ED.
Q6: Which of the following tests would you NOT request?a. PT/INR
b. Antifactor Xa activity
c. Thrombin time
d. Serum creatinine
55

Dabigatran Reversal Case
AC Jr. is a 85 yo man with acute decompensated heart failure and receiving dabigatran 150 mg PO BID for AF. He has fallen and hit his head and is being admitted to the ED.
B li INR i ED 2 0– Baseline INR in ED = 2.0
– Thrombin time = > 200 seconds
– Scr = 2.0 mg/dL
MD orders Vit K 10 mg IV and FFP
Q7: Will you process this order?
a. Yes
b. No
c. I’m not sure
Is There a Way to Reverse these Agents?ETP = endogenous thrombin potential
Dabigatran T ½ 14-17 hr
RivaroxabanT ½ 5-9hr; Elderly 11-13 hr
Hemodialysis Yes ~2/3 in 2 hr Not expected (> 90% bound)(Apixaban: 87% bound)
Antidote In development
Hemostatic Agents
PCC4 - Did not restore aPTT, ECT, TT PT reversed, normalized ETP CC(50 units/kg)
d ot esto e a , C ,- rFVIIa alt. ETP lag time - PCC corrected ETP responsive > rFVIIa
e e sed, o a ed(114% Normal)PCC corrected ETP
Activated PCC (aPCC)(25-50 units/kg)
Altered ETP lag timeEffective – single case
Corrected all parameters
rFVIIa(high dose)
CABG: Limited effect high dose single case
Corrected lag time
van Ryn J et al. Thromb Haemost. 2010; 103:1116-27; Eerenberg ES et al. Circulation.2011; 124:1573-9; Dager WE et al. Crit Care Med. 2011; 39:243 (Abstract 867);
Warkentin TE et al. Blood. 2012; 119:2172-4; Marlu R et al. Thromb Haemost. 2012; 108:217-24.
56

Assessing Intensity of Anticoagulation EffectsDabigatran Rivaroxaban/Apixaban
Drug present Thrombin time ? Chromogenic anti-factor XaHigh sensitive INR
Quantitative test
? Dilute thrombin time or Chromogenic ECT
Chromogenic anti-factor Xa
Sensitivity:PT vs. aPTT
aPTT > PT(Point-of-care INR > central lab)
PT > aPTT
No or limited ECT TT
- INR/aPTT - Potential for normal values at trough/active levelsWhat does a value mean?
• Is there a safe level to operate?
• Is it too high where the dose should be lowered?
No or limited effect
ECT, TT
Lindhoff-Last E et al. Ther Drug Monit. 2010; 32:673-9.Lindahl TL et al. Thromb Haemost. 2011; 105:371-8.
van Ryn J et al. Am J Med. 2012; 125:417-20.van Ryn J et al. Thromb Haemost. 2010; 103:1116-27.
Dialysis of Dabigatran
Stangier et al: Clin Pharmacokinet 2010; 49:259-68
• Design: Dabigatran 50 mg x 1 + 2 HD sessions; CKD V
– Not 150 mg multiple doses or AKI
• Result: Hemodialysis ~2/3rds removed
2 h C A t i l 12 5 / L C V 4 4 / L– 2 hr Cp Arterial 12.5 ng/mL > Cp Venous 4.4 ng/mL
Wanek et al: Case report. 2.5 hr HD (BFR 500 mL/hr): TT 90 – 60 sec
Stangier J et al. Clin Pharmacokinet. 2010; 49:259-68. Wanek MR et al. Ann Pharmacother. 2012 ;46:e21.
51015202530354045
Hemodialysis of Patients on Dabigatran
HD
UCDMC experience• Chromogenic dabigatran assay
available
• Delays in initiating dialysis noted
• Plasma Cp rebound occurs
0
50
100
150
200
250
300
Time
0Time
0
20
40
60
80
100
120
140
Time
HD
HD
HD
57

Reversing Dabigatran: A Case Experience
Setting: AF and undergoing ablation, on dabigatran
Situation: Transeptal perforation, pericardial window, and > 3L blood loss
Action: FFP protamine PRBCs with limited to no effect onAction: FFP, protamine, PRBCs with limited to no effect on bleeding
• aPCC: 25 units/kg over 15 minutes • Bleeding slows in first few minutes and has stopped
before infusion completed
• Limited impact on TT, ECT, INR, or aPTT• Low dose effective• Single case report – Use caution
Dager WE et al. Crit Care Med. 2011; 39:243 (Abstract 867).
Dabigatran Reversal Case AC Jr. is a 85 yo man with acute decompensated heart failure and receiving dabigatran 150mg PO BID for AF. He has fallen and hit his head and is being admitted to the ED.
– Baseline INR in ED = 2.0
– Thrombin time = > 200 seconds
S 2 0 /dL– Scr = 2.0 mg/dL
• CT scan to assess damage
• Arrange management options (dialysis, hemostatic agent, calcium if blood given)
• Check time of last dose
• Assess bleeding
• Consider anticoagulation options
• Patient and physician education
Systems Support
• 24-hour process
• Correct labs available
• Guidelines on how to use the available agents– Easy for clinicians to locate
• Rapid ability to implement management options
58

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L E C T E D R E F E R E N C E S
1. Chong CT, Lew TW, Kuperan P et al. Rapid reversal of coagulopathy in warfarin-related intracranial haemorrhages with prothrombin complex concentrates. Anaesth Intensive Care. 2010; 38:474-80.
2. Dager WE. Using prothrombin complex concentrates to rapidly reverse oral anticoagulant effects. Ann Pharmacother. 2011; 45:1016-20.
3. Dager WE, Gosselin RC, Roberts AJ. Reversing dabigatran in a life threatening bleed occurring during cardiac ablation with FEIBA®. Crit Care Med. 2011; 39: 243. Abstract 867.
4. Demeyere R, Gillardin S, Arnout J et al. Comparison of fresh frozen plasma and prothrombin complex concentrate for the reversal of oral anticoagulants in patients undergoing cardiopulmonary bypass surgery: a randomized study. Vox Sang. 2010; 99:251-60.
5. Dentali F, Marchesi C, Pierfranceschi MG et al. Safety of prothrombin complex concentrates for rapid anticoagulation reversal of vitamin K antagonists: a meta-analysis. Thromb Haemost. 2011; 106:429-38.
6. Dougherty J. Anticoagulation reversal. In: Dager WE, Gulseth MP, Nutescu EA, eds. Anticoagulation therapy: a point-of-care guide. Bethesda, MD: American Society of Health-System Pharmacists; 2011:123-54.
7. Dowlatshahi D, Butcher KS, Asdaghi N et al. Poor prognosis in warfarin-associated intracranial hemorrhage despite anticoagulation reversal. Stroke. 2012; 43:1812-7.
8. Eerenberg ES, Kamphuisen PW, Sijpkens MK et al. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation. 2011; 124:1573-9.
9. Hsia CC, Zurawska JH, Tong MZ et al. Recombinant activated factor VII in the treatment of non-haemophilia patients: physician under-reporting of thromboembolic adverse events. Transfus Med. 2009; 19:43-9.
10. Hylek EM, Regan S, Go AS et al. Clinical predictors of prolonged delay in return of the international normalized ratio to within the therapeutic range after excessive anticoagulation with warfarin. Ann Intern Med. 2001; 135:393-400.
11. Lindahl TL, Baghaei F, Blixter IF et al. Effects of the oral, direct thrombin inhibitor dabigatran on five common coagulation assays. Thromb Haemost. 2011; 105:371-8.
12. Lindhoff-Last E, Samama MM, Ortel TL et al. Assays for measuring rivaroxaban: their suitability and limitations. Ther Drug Monit. 2010; 32:673-9.
13. Marlu R, Hodaj E, Paris A et al. Effect of non-specific reversal agents on anticoagulant activity of dabigatran and rivaroxaban: a randomised crossover ex vivo study in healthy volunteers. Thromb Haemost. 2012; 108:217-24.
14. Mendelow AD, Gregson BA, Fernandes HM et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005; 365:387-97. 2005; 365:387-97.
59
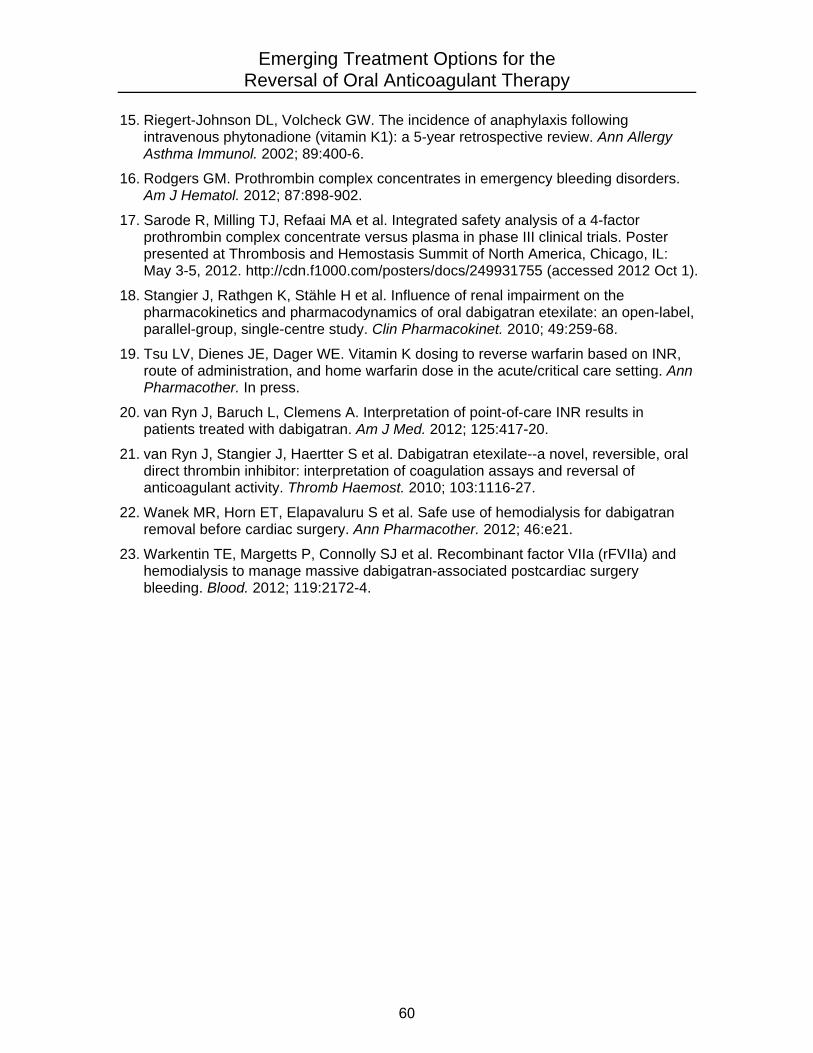
Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
15. Riegert-Johnson DL, Volcheck GW. The incidence of anaphylaxis following
intravenous phytonadione (vitamin K1): a 5-year retrospective review. Ann Allergy Asthma Immunol. 2002; 89:400-6.
16. Rodgers GM. Prothrombin complex concentrates in emergency bleeding disorders. Am J Hematol. 2012; 87:898-902.
17. Sarode R, Milling TJ, Refaai MA et al. Integrated safety analysis of a 4-factor prothrombin complex concentrate versus plasma in phase III clinical trials. Poster presented at Thrombosis and Hemostasis Summit of North America, Chicago, IL: May 3-5, 2012. http://cdn.f1000.com/posters/docs/249931755 (accessed 2012 Oct 1).
18. Stangier J, Rathgen K, Stähle H et al. Influence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre study. Clin Pharmacokinet. 2010; 49:259-68.
19. Tsu LV, Dienes JE, Dager WE. Vitamin K dosing to reverse warfarin based on INR, route of administration, and home warfarin dose in the acute/critical care setting. Ann Pharmacother. In press.
20. van Ryn J, Baruch L, Clemens A. Interpretation of point-of-care INR results in patients treated with dabigatran. Am J Med. 2012; 125:417-20.
21. van Ryn J, Stangier J, Haertter S et al. Dabigatran etexilate--a novel, reversible, oral direct thrombin inhibitor: interpretation of coagulation assays and reversal of anticoagulant activity. Thromb Haemost. 2010; 103:1116-27.
22. Wanek MR, Horn ET, Elapavaluru S et al. Safe use of hemodialysis for dabigatran removal before cardiac surgery. Ann Pharmacother. 2012; 46:e21.
23. Warkentin TE, Margetts P, Connolly SJ et al. Recombinant factor VIIa (rFVIIa) and hemodialysis to manage massive dabigatran-associated postcardiac surgery bleeding. Blood. 2012; 119:2172-4.
60

Emerging Treatment Options for the Reversal of Oral Anticoagulant Therapy
S E L F – A S S E S S M E N T Q U E S T I O N S
1. Adding rFVIIa to three-factor PCC in warfarin-treated patients with elevated INR values has been proposed to
a. Enhance the rate of INR reduction. b. Reduce the risk for thromboembolism. c. Reduce costs. d. Reduce the risk for hypersensitivity reactions.
2. RD is a 66-year-old man with AF and a creatinine clearance of 28 mL/min who
receives dabigatran 75 mg orally twice daily for stroke prevention. He comes to the clinic for a routine checkup and has no overt signs or symptoms of bleeding. Which of the following statements about the process for detecting bleeding in RD is correct?
a. The absence of overt signs and symptoms of bleeding suffices to exclude the
possibility of bleeding. b. Complete blood counts should be monitored for decreases reflecting blood loss. c. Laboratory coagulation assays are not needed because they do not provide
useful information. d. Formal monitoring for bleeding is not needed because this complication is rare.
3. RD develops bleeding, and hemodialysis is used to remove dabigatran and reverse
its anticoagulant effect. However, a rebound increase in plasma dabigatran concentration is observed after the end of the hemodialysis session. This rebound probably reflects
a. The limited renal clearance of the drug. b. The small volume of distribution. c. The large volume of distribution and distribution of the drug into tissues. d. The large volume of distribution and redistribution of the drug from tissues to
plasma.
4. Which of the following coagulation tests would be most useful as a qualitative test for the presence of dabigatran in RD after the drug is discontinued?
a. TT. b. ECT. c. Point-of-care INR. d. A chromogenic anti-factor Xa assay.
Answers
1. a 2. b 3. d 4. a
61