Emerging experimental therapeutics for bipolar disorder: clues
21
FEATURE REVIEW Emerging experimental therapeutics for bipolar disorder: clues from the molecular pathophysiology JA Quiroz, J Singh, TD Gould, KD Denicoff, CA Zarate Jr and HK Manji Laboratory of Molecular Pathophysiology, National Institute of Mental Health, Bethesda, MD, USA Bipolar affective disorder (manic-depressive illness) is a common, severe, chronic, and often life-threatening illness, associated with significant comorbidity. The recognition of the significant morbidity and mortality of patients with bipolar disorder, as well as the growing appreciation that a high percentage of patients respond poorly to existing treatments, has made the task of discovering new therapeutic agents, that are both efficacious and have few side effects increasingly more important. Most recent agents introduced into the pharmaco- peia for the treatment of bipolar disorder have been anticonvulsants and atypical antipsychotics. We propose that novel treatments developed specifically for bipolar disorder will arise from (1) understanding more precisely the molecular mechanisms of treatments that are clearly efficacious or (2) developing medications based on the knowledge obtained of the underlying pathophysiology of bipolar disorder. Knowledge with regard to the underlying pathophysiology of bipolar disorder is increasing at a rapid pace, including alterations in intracellular signaling cascades as well as impairments of cellular plasticity and resilience in critical neuronal circuits. We propose that therapeutics designed to enhance cellular plasticity and resilience and that counter maladaptive stress-responsive systems may have consider- able utility for the treatment of bipolar disorder. Therapeutic strategies designed to address cellular resilience and plasticity include the regulation of neurotrophic pathways, glucocorti- coid signaling, phosphodiesterase activity, and glutamatergic throughput and mitochondrial function. While the task of developing novel medications for bipolar disorder is truly daunting, these and similar approaches will ultimately lead to better medications for the millions who suffer from this devastating illness. Molecular Psychiatry (2004) 9, 756–776. doi:10.1038/sj.mp.4001521 Published online 11 May 2004 Keywords: depression; mania; NMDA; glutamate; memantine; riluzole; felbamate; zinc; corticotropin-releasing factor; glucocorticoids; neuroplasticity; mitochondria Bipolar disorder (manic-depressive illness) is a common, severe, chronic, and often life-threatening illness, associated with significant comorbidity. 1 It has historically been assumed that—in contrast to dementia praecox (schizophrenia)—bipolar disorder is an episodic illness with full recovery between episodes. However, studies that are more recent have clearly shown that this may only represent the situation for a minority of subjects. A number of studies and analyses have indicated that for a large percentage of patients, the outcome is quite poor, with high rates of relapse, chronicity, lingering residual symptoms, subsyndromes, cognitive and functional impairment, and psychosocial disability. Further- more, suicide is estimated to be the cause of death in up to 15% of individuals with mood disorders, and, in addition to suicide, many other deleterious health-related effects are increasingly being recog- nized. Indeed, there is a growing appreciation that, far from being diseases with purely psychological man- ifestations, mood disorders are systemic diseases with deleterious effects on multiple organ systems. The recognition of the significant morbidity and mortality of patients with bipolar disorder, as well as the growing appreciation that a significant percentage of patients respond poorly to existing treatments, has made the task of discovering new therapeutic agents, that are both efficacious and have few side effects, increasingly more important. In recent years, there has been an explosion in the number of options available for the treatment of bipolar disorder with a parallel and unprecedented increase in the interest in the treatment of bipolar disorder by pharmaceutical companies, clinicians, researchers, and indeed the public. There are a number of newer pharmacological agents that are rapidly being introduced into the market and used by clinicians for the management of bipolar patients. However, largely, these simply represent agents developed for other disorders (no- tably epilepsy or schizophrenia), following which their utility is investigated for the treatment of bipolar Received 27 February 2004; accepted 17 March 2004 Correspondence: HK Manji, Laboratory of Molecular Pathophy- siology, Bldg 49, Room B1EE16, NIMH, NIH, HHS, Bethesda, MD 20892, USA. E-mail: [email protected] Molecular Psychiatry (2004) 9, 756–776 & 2004 Nature Publishing Group All rights reserved 1359-4184/04 $30.00 www.nature.com/mp
Transcript of Emerging experimental therapeutics for bipolar disorder: clues

FEATURE REVIEW
Emerging experimental therapeutics for bipolar disorder:clues from the molecular pathophysiologyJA Quiroz, J Singh, TD Gould, KD Denicoff, CA Zarate Jr and HK Manji
Laboratory of Molecular Pathophysiology, National Institute of Mental Health, Bethesda, MD, USA
Bipolar affective disorder (manic-depressive illness) is a common, severe, chronic, and oftenlife-threatening illness, associated with significant comorbidity. The recognition of thesignificant morbidity and mortality of patients with bipolar disorder, as well as the growingappreciation that a high percentage of patients respond poorly to existing treatments, hasmade the task of discovering new therapeutic agents, that are both efficacious and have fewside effects increasingly more important. Most recent agents introduced into the pharmaco-peia for the treatment of bipolar disorder have been anticonvulsants and atypicalantipsychotics. We propose that novel treatments developed specifically for bipolar disorderwill arise from (1) understanding more precisely the molecular mechanisms of treatments thatare clearly efficacious or (2) developing medications based on the knowledge obtained of theunderlying pathophysiology of bipolar disorder. Knowledge with regard to the underlyingpathophysiology of bipolar disorder is increasing at a rapid pace, including alterations inintracellular signaling cascades as well as impairments of cellular plasticity and resilience incritical neuronal circuits. We propose that therapeutics designed to enhance cellular plasticityand resilience and that counter maladaptive stress-responsive systems may have consider-able utility for the treatment of bipolar disorder. Therapeutic strategies designed to addresscellular resilience and plasticity include the regulation of neurotrophic pathways, glucocorti-coid signaling, phosphodiesterase activity, and glutamatergic throughput and mitochondrialfunction. While the task of developing novel medications for bipolar disorder is truly daunting,these and similar approaches will ultimately lead to better medications for the millions whosuffer from this devastating illness.Molecular Psychiatry (2004) 9, 756–776. doi:10.1038/sj.mp.4001521Published online 11 May 2004
Keywords: depression; mania; NMDA; glutamate; memantine; riluzole; felbamate; zinc;corticotropin-releasing factor; glucocorticoids; neuroplasticity; mitochondria
Bipolar disorder (manic-depressive illness) is acommon, severe, chronic, and often life-threateningillness, associated with significant comorbidity.1 Ithas historically been assumed that—in contrast todementia praecox (schizophrenia)—bipolar disorderis an episodic illness with full recovery betweenepisodes. However, studies that are more recent haveclearly shown that this may only represent thesituation for a minority of subjects. A number ofstudies and analyses have indicated that for a largepercentage of patients, the outcome is quite poor, withhigh rates of relapse, chronicity, lingering residualsymptoms, subsyndromes, cognitive and functionalimpairment, and psychosocial disability. Further-more, suicide is estimated to be the cause of deathin up to 15% of individuals with mood disorders,and, in addition to suicide, many other deleterioushealth-related effects are increasingly being recog-
nized. Indeed, there is a growing appreciation that, farfrom being diseases with purely psychological man-ifestations, mood disorders are systemic diseases withdeleterious effects on multiple organ systems. Therecognition of the significant morbidity and mortalityof patients with bipolar disorder, as well as thegrowing appreciation that a significant percentage ofpatients respond poorly to existing treatments, hasmade the task of discovering new therapeutic agents,that are both efficacious and have few side effects,increasingly more important. In recent years, therehas been an explosion in the number of optionsavailable for the treatment of bipolar disorder with aparallel and unprecedented increase in the interest inthe treatment of bipolar disorder by pharmaceuticalcompanies, clinicians, researchers, and indeed thepublic. There are a number of newer pharmacologicalagents that are rapidly being introduced into themarket and used by clinicians for the management ofbipolar patients. However, largely, these simplyrepresent agents developed for other disorders (no-tably epilepsy or schizophrenia), following whichtheir utility is investigated for the treatment of bipolarReceived 27 February 2004; accepted 17 March 2004
Correspondence: HK Manji, Laboratory of Molecular Pathophy-siology, Bldg 49, Room B1EE16, NIMH, NIH, HHS, Bethesda,MD 20892, USA. E-mail: [email protected]
Molecular Psychiatry (2004) 9, 756–776& 2004 Nature Publishing Group All rights reserved 1359-4184/04 $30.00
www.nature.com/mp

disorder. Thus, the two categories of drugs that havereceived much attention by clinicians and researchersalike as putative treatments for bipolar disorder areanticonvulsant and antipsychotic medications. Sig-nificant advances were achieved with the develop-ment of the atypical antipsychotic drugs compared tothe typical antipsychotic drugs. They are associatedwith lower rates of extrapyramidal symptoms andtardive dyskinesia, and are more efficacious both inthe treatment of negative symptoms of schizophreniaand in improving the quality of life. The atypicalantipsychotic drugs were also noted to have signifi-cant thymoleptic properties early on in their devel-opment.
As a consequence, almost as rapidly as antic-onvulsants are being introduced into the market forthe management of epilepsy and atypical antipsycho-tic drugs for the treatment of schizophrenia, thesedrugs are being used by clinicians for the treatment ofbipolar disorder. This practice undoubtedly hasresulted in large part from the appalling dearth ofpharmacologic agents specifically developed for thetreatment of bipolar disorder. In this perspectivespaper, we outline approaches that are currentlyunderway for the development of novel therapeuticsspecifically for the treatment of bipolar disorder.
Approaches for developing novel therapeutics for acomplex disorder such as bipolar illness might occurin one of two ways:
(1) Understanding the precise biochemical targets(both direct and long- term) of antimanic/moodstabilizers currently in use and using the knowl-edge gained to design drugs that are more specificto those biochemical target(s).
(2) Understand the pathophysiology of the illnessand utilize that knowledge to design therapeuticsthat control core bipolar symptomatology andeither attenuate or prevent the deleterious sys-temic effects of the illness.
Here, we focus on the second approach; in anaccompanying article within this issue, we discussmedication development approaches utilizing thefirst approach.2 Knowledge regarding the underlyingpathophysiology of bipolar disorder is increasing at arapid pace, with most theories suggesting that anunderlying genetic diathesis interacts with environ-mental factors. Extensive genetic studies are under-way3 and it is likely that their fruition combined withthe knowledge obtained in other fields such asepidemiology, neuroimaging, and neuropathologywill allow for a more precise understanding of thedisease process(s) involved.
A number of neurobiological mechanisms havebeen proposed to explain the etiology of bipolardisorder, with monoamines traditionally receiving thegreatest interest. Herein, we focus on more recenthypotheses, describing how impairments of neuro-plasticity and cellular resilience may contribute to theunderlying pathophysiology. While traditionallyviewed exclusively as a neurochemical disorder,
recent evidence suggests the possibility that theunderlying primary pathophysiology of bipolar dis-order may involve alterations in intracellular signal-ing cascades that produce not only functional but alsoneuromorphological impairments, rather than speci-fic alterations in isolated neurochemicals per se. Inthis regard, it is worth noting that increasing numberof neuroimaging, neuropathological, and biochemicalstudies consistently suggest that impairments inneuroplasticity and cellular resilience are present inpatients who suffer from severe, recurrent mooddisorders. In the following sections, we describestudies identifying possible structural, functional,and cellular abnormalities associated with bipolardisorder and discuss the potential cellular under-pinnings of these micro- and macro morphologicalbrain changes. We suggest that therapeutics designedto enhance cellular plasticity and resilience and thatcounter maladaptive stress-responsive systems mayhave considerable utility for the treatment of severemood disorders.
Evidence for impairments of structural plasticityand cellular resilience in mood disorders
Methodologies to investigate structural and func-tional deficits within the human brain have exponen-tially increased in recent years allowing for a morecomplete and intensive analysis of potential deficien-cies in the brains of patients suffering from neurop-sychiatric disorders. Thus, it is now possible todiscern relatively subtle differences in cerebral bloodflow, receptor density, or in macroscopic brainstructure. Likewise, post-mortem studies of the brainare enhanced with technological advances that allowfor relatively unbiased observations of cell density,morphology, and size. The functional and morpho-metric findings in bipolar disorder have been exten-sively reviewed elsewhere;4–13 here we provide a briefoverview of these findings.
In toto, positron emission tomography (PET) ima-ging studies have revealed multiple alterations ofregional cerebral blood flow (CBF) and glucosemetabolism in limbic and prefrontal cortical (PFC)structures in patients with mood disorders. Overall,most of these studies implicate the limbic-thalamic-cortical and limbic-cortical-striatal-pallidal-thalamiccircuits, involving the amygdala, orbital and medialPFC, and anatomically related parts of the striatumand thalamus in the pathophysiology of mooddisorders (see Sheline,4 Drevets,5 Manji et al,6
Drevets7 for a review). Recent morphometric magneticresonance imaging (MRI) and post-mortem investiga-tions have also demonstrated abnormalities of brainstructure that correspond to the abnormalities ofmetabolic activity (discussed in Manji et al,6 Drevets,7
Manji and Duman8). Structural imaging studiesdemonstrate reduced gray matter volumes in areasof the orbital and medial PFC, temporal lobe, andenlargement of third ventricle in subjects with mooddisorders compared to healthy controls (reviewed in
Experimental treatments BPD IIJA Quiroz et al
757
Molecular Psychiatry

Drevets,9, Strakowski et al,10 Beyer and Krishnan11).Also consistent is the increased presence of whitematter hyperintensities (WMH) in the brains ofelderly depressed patients, and both young andelderly patients with bipolar disorder (reviewed inLenox et al14). While there is a growing awareness ofthe genetic influences on WMH, and their possibleimpact on neuropsychological functioning,15 there aremultiple other causes including cerebrovascularaccidents, demyelination, loss of axons, dilatedperivascular space, minute brain cysts, and necrosis(see Lenox et al14 for a review). Diffusion tensorimaging (DTI) of brain tissue has been utilized tostudy possible white matter tract disruption in mooddisorders.16 This procedure measures the apparentdiffusion coefficient (ADC), or isotropic diffusion,and anisotropy, or diffusion as influenced by tissuestructure. Taylor and co-workers found that WMHshowed higher ADC and lower anisotropy thannormal regions, with gray matter showing similartrends. Recent evidence suggests that subcorticalhyperintensities are correlative with cortical graymatter changes.17,18 Together, these results supportthe contention that WMH damage the structure ofbrain tissue and likely disrupt the neuronal connec-tivity necessary for normal affective functioning.Although the cause of WMH in mood disorders isunknown, their presence—particularly in the brainsof young bipolar patients—suggests importance in thepathophysiology of the disorder.14,19
Relatively recent post-mortem neuropathologicalstudies are complementary, showing reductions incortex volume, and region- and layer-specific reduc-tions in number, density, and/or size of neurons andglial cells in the subgenual PFC, orbital cortex, dorsalanterolateral PFC, amygdala, and in basal ganglia anddorsal raphe nuclei in individuals with bipolardisorder and other severe mood disorders comparedto controls (reviewed in Manji and Duman,8 Cotteret al12 Rajkowska13). It is important to note, however,that it is not currently known if these alterations—whether they be functional and structural imaging orpost-mortem—constitute developmental abnormal-ities conferring vulnerability to severe mood epi-sodes, compensatory changes to other pathogenicprocesses, the sequelae of recurrent affective epi-sodes, comorbidity, pharmacological treatments, orsolely epiphenomenon that lack real significance inthe acute signs and symptoms of these disorders(although they very likely do contribute to the long-term functional deterioration observed in manypatients). Understanding these issues will partlydepend on experiments that delineate the onset ofsuch abnormalities within the illness course anddetermine whether they antedate mood episodes inhigh-risk individuals. Furthermore, there is no totalreproducibility among either the neuroimaging orpost-mortem studies. This may be representative ofvariations of experimental design (including medica-tion effects), an effect of low sample size, or difficultyin clearly defining disease phenotypes within a
heterogeneous group of disorders. Thus, further studyis required in order to understand if more rigorouslydefined subtypes of bipolar disorder and other mooddisorders are associated with any particular orspecific biological alteration.14
Stress and glucocorticoids modulate neural plasti-city: implications for mood disorders and thedevelopment of improved therapeutics
In developing hypotheses with regard to the patho-genesis of these histopathological changes in mooddisorders, the alterations in cellular morphologyresulting from various stressors have been the focusof considerable recent research (reviewed in D’sa andDuman20). Thus, although mood disorders have astrong genetic basis, considerable evidence hasshown that severe stressors are associated with asubstantial increase in risk for the onset of mooddisorders in susceptible individuals. The hypothala-mus–pituitary–adrenal (HPA) axis is a major pathwayby which stress exerts its effects on the brain andother organ systems. This pathway represents theprimary ‘stress’ pathway in humans and othermammals, whereas the lateral ventricular nucleus ofthe hypothalamus releases corticotropin-releasinghormone/factor (CRH/F), which stimulates the pro-duction of adrenocorticotropin-releasing hormone(ACTH) by the pituitary. This latter hormone stimu-lates the production of glucocorticoids by the adrenalgland. Cortisol is considered a primary stress hor-mone of the body, having varied effects on metabo-lism, neurovegetative behaviors of organisms, and amultitude of effects on the functions of neurons andneuronal systems (Figure 1).
Most studies of atrophy and survival of neurons inresponse to stress, as well as hormones of the HPA,have focused on the hippocampus. This is due, inpart, to the well-defined and easily studied neuronalpopulations of this limbic brain region, including thedentate gyrus granule cell layer and the CA1 and CA3pyramidal cell layers. Another major reason is thatthe highest levels of glucocorticoid receptors areexpressed in this brain region.21 However, it is clearthat stress and glucocorticoids also influence thesurvival and atrophy of neurons in other brain regions(eg PFC; see below) that have not yet been studied inthe same detail as the hippocampus.
One of the most consistent effects of stress oncellular morphology in preclinical models is atrophyof hippocampal neurons (for reviews, see Sapolsky,22
McEwen.23) This atrophy is observed in the CA3pyramidal neurons, but not in other hippocampal cellgroups (ie CA1 pyramidal and dentate gyrus granuleneurons). The stress-induced atrophy of CA3 neurons(ie, decreased number and length of the apicaldendritic branches) occurs after 2–3 weeks of ex-posure to restraint stress or more long-term socialstress, and has been observed in different speciesincluding rodents and tree shrews.22,23 Atrophy ofCA3 pyramidal neurons also occurs upon exposure
Experimental treatments BPD IIJA Quiroz et al
758
Molecular Psychiatry

to high levels of glucocorticoids, suggesting thatactivation of the HPA axis likely plays a major rolein mediating the stress-induced atrophy.23–25
Neurogenesis in the adult brain is also the target ofmajor research on the role of stress and the HPA axis.The localization of pluripotent progenitor cells andneurogenesis occurs in restricted brain regions, withthe greatest density of new cell birth observed in thesubventricular zone and the subgranular layer of thehippocampus. Neurogenesis in the hippocampus isincreased by enriched environments, exercise, andhippocampal-dependent learning.26–28 Up-regulationof neurogenesis in response to these behavioralstimuli and the localization of this process to thehippocampus has led to the proposal that new cellbirth is involved in learning and memory.26
Studies have shown that decreased neurogenesisoccurs in response to both acute and chronic stress(see Gould et al.26). Furthermore, it has been shownthat removal of adrenal steroids (i.e. adrenalectomy)increases neurogenesis, and that treatment with highlevels of glucocorticoids reproduces the downregula-tion of neurogenesis that occurs in response to stress.
Lowering glucocorticoid levels in aged animalsrestores neurogenesis to levels observed in youngeranimals, indicating that the population of progenitorcells remains stable but that it is inhibited byglucocorticoids.29
Antidepressants30 and lithium31 increase neurogen-esis in the hippocampus. However, while the im-portance of neurogenesis in mood disorder treatmentand pathophysiology is still a matter of importantdebate, Santarelli et al.32 recently conducted a seriesof very critical experiments. Mice were given oralfluoxetine, imipramine, desipramine, haloperidol, orvehicle for 28 days, applying the novelty-suppressedfeeding test as a model for antidepressant efficacy.This group noted a 35% improvement in speed forretrieving food or water in mice taking antidepres-sants (fluoxetine, imipramine, or desipramine). In asecond experiment, they found a 60% increase inBrdU-positive cells in the dentate gyrus after 11–28days of treatment with fluoxetine. To test whetherhippocampal neurogenesis is necessary for the anti-depressants effect, they exposed mice to X-raysdirected at the hippocampus, leading to an 85%reduction in BrdU-positive cells in the subgranularzone. These mice were then treated with fluoxetine,imipramine, or vehicle for 28 days. The previouslynoted effect of antidepressants on the novelty-sup-pressed feeding test was not seen in irradiated mice,suggesting that behavioral effects of chronic use ofantidepressants may be mediated by new neurons inthe hippocampus.32 However, several lines of evi-dence suggest that it may be premature to concludethat hippocampal neurogenesis is causally linked tothe etiology and treatment of depression. Thus,Vollmayr et al.33 have undertaken a series of studiesto determine if the inescapable foot shock learnedhelpnessness model is associated with reducedhippocampal proliferation in a temporal time frameconsistent with the behavioral deficits. They did notfind a significant reduction in cell proliferation at atime when the helpless behavior was first observed.In follow-up studies, they utilized restraint stress todecrease the rate of cell proliferation 40%; subse-quent investigation showed that these animals did notdevelop learned helplessness at a higher rate than thecontrol animals. Most recently, large-scale clinicalstudies have shown lack of antidepressant efficacy ofan NK1 antagonist; these results argue against asimple ‘neurogenesis hypothesis’ somewhat sinceboth NK1 antagonists, and NK1 knockout mice showincreased neurogenesis.34,35 It may therefore be moreappropriate to consider the changes in the context ofbroader impairments of cellular plasticity and resi-lience, rather than a limited neurogenesis hypothesismodel. These series of preclinical findings in thehippocampus are consistent with the clinical findingsshowing that subjects with depression of longerillness duration and multiple hospitalizations(associated with prolonged hypercortisolemia22)have smaller hippocampal volumes.36,37 Antidepres-sant treatment may offer some protection against
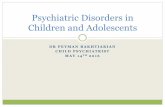
Figure 1 Harmful effects of stress, HPA axis activation, andglutamate on neurons. Depicted here are multiple mechan-isms by which stress, and potentially affective episodes,may attenuate cellular resiliency, thereby resulting inatrophy, death, and endangerment of hippocampal neurons.Three primary mechanisms appear to be: (1) excessiveNMDA and non-NMDA glutamatergic throughput; (2)downregulation of cell surface glucose transporters, whichare involved in bringing glucose into the cell. Reducedlevels of glucose transporters thus reduce the neuron’senergetic reservoir, making them susceptible to energyfailure when faced with excessive demands; (3) reductionin the levels of neurotrophic factors such as BDNF, which isessential for the neuron’s normal trophic support andsynaptic plasticity; (4) a reduction in glial cells maycontribute to impairments of neuronal structural plasticityby reducing the neuron’s energy supply and reduced glial-mediated clearing of excessive synaptic glutamate. NMDA,N-methyl-aspartate glutamate receptor; CRF, corticotropin-releasing factor; GR, glucocorticoid receptor; BDNF, brain-derived neurotrophic factor. Modified, and reproduced,with permission from.228
Experimental treatments BPD IIJA Quiroz et al
759
Molecular Psychiatry

hippocampal volume loss.38,39 It is important to note,however, that some studies suggest that small hippo-campi are—at least in part—an inherited character-istic of the brain and predisposes to (rather thanrepresents the sequelae of) psychiatric disorders.40,41
These observations highlight the need for caution inattribution of causality in the cross-sectional humanmorphometric studies of the hippocampus discussedabove and the preclinical data on the effects ofstress.
Although not as extensively studied as the hippo-campus, preclinical research has also demonstratedhistopathological changes in rat PFC after corticoster-one administration.42 Wellman investigated pyrami-dal neurons in layers II–III of medial PFC, andquantified dendritic morphology in three dimensions.This study demonstrated a significant redistributionof apical dendrites in corticosterone-treated animals,with the amount of dendritic material proximal to thesoma increased and distal dendritic material de-creased. These findings suggest that stress mayproduce a significant reorganization of the apicaldendritic arbor from medial PFC in rats. Morerecently, Lyons et al43 demonstrated that 4 years aftera brief stressor (intermittent postnatal separationsfrom maternal availability) young adult squirrelmonkeys showed significantly larger right ventralmedial prefrontal volumes.43 Neither overall brainvolumes nor left prefrontal measures were altered,suggesting selective (rather than nonspecific) effects.It is interesting to speculate that these preclinicalfindings are related to the clinical observations ofreduced size of PFC regions, gray matter changes, andpost-mortem alterations of neurons and glial cells inpatients with mood disorders.
Evidence for impairment of HPA axis in mooddisorders
Evidence of HPA axis activation in bipolar disorder issuggested by multiple lines of evidence. Cushing’ssyndrome secondary to chronic high levels of en-dogenous glucocorticoids is associated with a numberof psychiatric and psychological disturbances, regard-less of its etiology. Major depression, mania, anxietydisorders and cognitive dysfunction/delirium, andhippocampal atrophy have commonly been re-ported.44,45 For example, in a prospective study 81%of subjects diagnosed with Cushing’s developed apsychiatric disorder, most frequently a mood dis-order.46 Interestingly, treatment with antiglucocorti-coid therapeutics has been reported to result in animprovement in mood/cognitive dysfunction,46 aswell as an increase of hippocampal volume inproportion to the treatment-associated decrement inurinary-free cortisol after corrective surgery.47,48
In noncushingoid subjects, multiple case reports, aswell pharmacoepidemiological studies, have reportedthe effects of exogenous steroids on mood (reviewedin Brown et al49). In a recent review, Sirois50 foundthat 75% of patients treated with exogenous
corticosteroids exhibited affective symptoms, includ-ing mania and depression. At least one report foundthat mania or hypomania was reported to occur on theday of treatment with corticosteroids and depressionwas seen on alternate days of treatment.51
Measurements of HPA activity in patients are alsooverwhelmingly supportive. Indeed, overactivity ofthe HPA axis in depression (either unipolar orbipolar) is among the most consistently replicatedbiological findings in psychiatry. These include lackof dexamethasone suppression of endogenous cortisollevels, increased ACTH response to CRF, and alteredresponses to the combined dexamethasone/cortico-tropin release hormone (DEX/CRF) challenge test.While we do not describe this well-defined phenom-enon extensively here, we refer the interested readerto an excellent review in Plotsky et al.52
Detailed studies of glucocorticoid receptor (GR) andmineralocorticoid receptor (MR) in subjects withmood disorders are still ongoing. However, postmor-tem studies in patients have shown significantlylower glucorticoid receptor (GR), mineralocorticoidreceptor (MR) protein, and mRNA levels in the PFCcompared to controls.53 GR mRNA levels werereported to be decreased in layers III and VI in theentorhinal cortex in patients with mood disorders.54
Nemeroff et al55 have additionally shown a markeddecrease in CRF binding sites in the frontal cortex ofsuicide victims. In an in vivo study of MR function insubjects with depression using spirinolactone (an MRantagonist), Young et al56 found that subjects withdepression had higher functional activity of the MRsystem, with an increased secretion of cortisol inresponse to spirinolactone in comparison to matchedcontrols.56
Animal models using knockout genes or antisenseprobes have been extremely valuable in understand-ing the HPA axis, and support its relevance in thepathophysiology and treatment of mood and anxietydisorders. See Gould et al57 for a complete descriptionof these studies.
Is targeting the HPA axis a relevant strategy for thetreatment for severe mood disorders?
Owing to the evidence reviewed above, there is agrowing appreciation that abnormalities of the HPAaxis may play a role in mediating the phenotypicexpression of certain affective states,58 and, notsurprisingly, there is increasing interest in targetingthis system for the development of novel therapeu-tics. Published double-blind, placebo-controlled clin-ical studies to modulate the HPA axis have employedinhibitors of glucocorticoid synthesis,59,60 antagonistsof the GR,61,62 hydrocortisone to downregulate theHPA axis (as a proof of concept study in DeBattistaet al63) and dehydroepiandrosterone.64,65 See Table 1for a summary of these and additional open-labelstudies, including a CRF 1R antagonist trial. Some ofthese drugs have been investigated for proof ofconcept, and it is expected that modified and
Experimental treatments BPD IIJA Quiroz et al
760
Molecular Psychiatry

Table 1 Examples of clinical studies where HPA axis modulation was studied as a primary therapya
Study Population Study design Agent Results
Inhibitors of GCsynthesisMurphy et al232 20 Refractory
depression (1 BP)Open label, 8weeks
Aminogluthethimide 1000 mg/day
17 completers: 11 fullresponders þ 3 partialresponders
Ghadirian etal233b
Ketoconazole up to 1200 mg/day
Either one plusMetyrapone 250–1000 mg/day
Wolkowitz et al234 8 UP, 2 BP, 7completers
Open label, 3weeks
Ketoconazole 400–800 mg/day 7/7 completers had gradualimprovement in mood
O’Dwyer et al235 8 inpatient UP SB PC CO, 2weeks
Metyrapone 1000–2000 mg/day Six responders
Thakore andDinan236
4 UP inpatient 4women infollicular phase
Open label, 4weeks
Ketoconazole 400–600 mg/day Five responders, three partialresponders
Iizuka et al237 3 UP Open label, 4weeks
Metyrapone 2000 mg/day Three achieved remission,partial response
3 BPRaven et al238 6 UP Open label, 2
weeksMetyrapone 2000–4000 mg/day Six responded. Reduction in
MADRS was correlated todecrease in 11-deoxycortisolmetabolites
Sovner andFogelman239
2 AtypicalDepression
Open label, 52weeks
Ketoconazole 200–400 mg/day Remission achieved at the 1stmonth and at 1 year
Wolkowitz et al59 20 UP DB PC, 4weeks
Ketoconazole 800 mg/day/PBO Only hypercortisolemicpatients (8) showed 48% ofreduction in HAMD
Malison et al60 16 UP treatmentresistant
DB PC, 6weeks
Ketoconazole 1200 mg/day/PBO 2/8 responded onKetoconazole and none (0/8)on placebo
Brown et al240 6 BP I or II Open label,add-on, 4weeks
Ketoconazole up to 800 mg/day All three completersresponded on HAMD
GR II antagonistMurphy et al81 4 UP Open label, 8
weeksMifepristone 200 mg/day Three improved
Belanoff et al61 5 MDD withpsychosis
DB PC, 4 day Mifepristone/PBO Five showed significantdecrease in HAMD and BPRS
Belanoff et al82 30 MDD withpsychosis
Open label, 7day
Mifepristone 50 mg, 600 mg,1200 mg
42% improved HAMD in600–1200 mg group68% improved with decreasein BPRS
Hoyberg et al87c 142 UP DB RCduration notspecified
ORG 34517/Paroxetine Prelim results suggest efficacy
Young et al62 20 BP, add-on DB PC CO, 1week
Mifepristone 600 mg/PBO Statistically significantimprovement in MADRS andcognition
Hydrocortisone/oCRFDebattista et al63 22 UP DB PC, 2 days 15 mg Hydrocortisone or 1 mg/kg
oCRF or PBOGreater decrease (37%) inHAMD with hydrocortisone
DHEAWolkowitz et al80 6 UP Open label, 4
weeksDHEA 30–90 mg Improvement correlated with
DHEA levelsBloch et al65 17 MOD DB PC CO, 6
weeks onDHEA
DHEA 90 mg and 450 mg 60% responded to DHEA,20% to placebo
Experimental treatments BPD IIJA Quiroz et al
761
Molecular Psychiatry

improved medications would lack some of the limit-ing side effects observed with these compounds. Wedescribe some of the drugs currently under investiga-tion in clinical and/or preclinical trials.
CRF1 receptor antagonistsA number of small molecule CRF 1R antagonists havebeen evaluated using in vivo paradigms in animalmodels to attenuate CRF-induced ACTH release.66
Several classes of CRF 1R inhibitors have beenidentified, including peptides (astressin, a-helCRF)and small molecule nonpeptides (CP-154526, anta-larmin, DMP-695, DMP-696, CRA-1000, R-121919,SSR-125543, NBI 35965, NBI 27914) (see Soundersand Williams,66 Holmes et al67 for a review). Pre-clinical studies have shown that CRF 1 antagonistsreduce CRF-induced ACTH release and CRF-inducedcAMP production.
Antalarmin, a novel pyrrolopyrimidine com-pound,68 in oral doses of 20 mg/kg in primatessignificantly diminished the CRF-stimulated ACTHrelease, and the pituitary–adrenal, sympathetic, andadrenal medullary responses to stress and alsoreversed stress-induced inhibition of exploratoryand sexual behaviors.69 Using the chronic stressmodel in mice, both antalarmin (10 mg/kg) andfluoxetine (10 mg/kg) were found to improve mea-sures of physical state, weight gain, and emotionalresponse in the light–dark test compared to stressed,untreated animals.70
CP-154,526, developed by Pfizer, has been evalu-ated in animal paradigms for anxiety. It has a highpenetrability similar to antalarmin.71 Mansbach et al72
have shown its efficacy in the learned helplessnessmodel of depression in rats. SSR125543A, a 2-aminothiazole derivative, which displays highaffinities for human CRF R1 receptors, hasshown efficacy in the forced swim test model and inchronic mild stress model in rats in a studycomparing it to antalarmin and fluoxetine.73 Inother studies, CRA 1000, a nonpeptide pyrimidineCRF 1 antagonist being developed by TaishoPharmaceuticals,74 reduced immobility in the learnedhelplessness paradigm in male Wistar rats whengiven by intraperitoneal injection.75 DMP696, devel-oped by Dupont, is a selective, potent, and highlybioavailable nonpeptide CRF 1R antagonist. It hasbeen tested in behavioral models of anxiety andis being tested in behavioral paradigms fordepression.76
Interestingly, R-121919 reduced anxiety and de-pressive symptoms in patients with major depressionin an open-label clinical trial.77 The clinical develop-ment of the compound was discontinued probablybecause of two healthy volunteers developed elevatedliver enzymes after receiving a high dose ofR-121919.78 Recently, however, in an extended datareport of the clinical study in major depressionpatients, no serious side effects were noted in thehypothalamic-pituitary–gonadal system, the hypotha-lamic-pituitary–thyroid axis, the renin–angiotensinsystem, and prolactin or vasopressin secretion. Inaddition, no effects on clinical laboratory parameters(including liver enzymes) were observed, encouragingthe development of CRF 1R antagonists as antide-pressant medications.78
Wolkowitz et al64 20 UP, 2 BP DB PC, 6weeksmonotherapy/add-on
DHEA max 90 mg/day PBO 5/11 on DHEA and none (0/11) on placebo
CRF 1RAntagonistZobel et al77 24 UP Open label, 30
daysR121919 5–40 mg (1)or 40–80 mg (2)
20 completers, 5/10responded in group 1; 8/10responded in group 2; ACTHresponse to CRF stimulationpredicted responders
aCase reports are not included.bExtension of the original study by Murphy et al.232 Total data presented.cFrom proceedings of CINP Meeting, 2002.ACTH: adrenocorticotropin hormone, AE: adverse effects, BP: bipolar disorder, BPRS: brief psychiatric rating scale, CO:crossover, CRF: corticotropin release hormone, DB: double blind, DHEA: dehydroepiandrosterone, GC: glucocorticoid, GR:glucocorticoid receptor, HAMD: Hamilton rating scale for depression, MADRS: Montgomery Asberg depression rating scale,MDD: major depressive disorder, MOD: midlife-onset dysthymia, oCRF: ovine CRF, PBO: placebo, PC: placebo controlled,SB: single blind, UP: unipolar depression.
Table 1 continued
Study Population Study design Agent Results
Experimental treatments BPD IIJA Quiroz et al
762
Molecular Psychiatry

DehydroepiandrosteroneDehydroepiandrosterone (DHEA) serves as a precur-sor for both androgenic and estrogenic steroids andtogether with its sulfated form (DHEA-S) are secretedby the adrenal gland and also produced in the CNS.Thus, DHEA and DHEA-S are neuroactive steroidsthat have a number of effects that can be described as‘functional antagonism’ of the actions of glucocorti-coids (DHEA does not directly interact with theglucocorticoid receptor, and there is no knownreceptor for DHEA in any tissue).79 Among its effects,DHEA counteracts the actions of glucocorticoids toinhibit memory and primed-burst potentiation (a formof long-term potentiation), and antagonizes oxidativedamage in the brain (and in other organs) produced byacute hyperglycemia. Although mediated by anunknown cellular and molecular mechanism, DHEAalso interacts with neurotransmitters (serotonin,gamma amino butyric acid, excitatory amino acids,and dopamine), in addition to its glucocorticoidantagonism (reviewed in McEwen79). Its antidepres-sant efficacy has been suggested by clinical trials indysthymic and depressed patients. Wolkowitz and co-workers reported a case series comprising of sixmiddle-aged and elderly major depression patientswith low basal plasma DHEA and/or DHEA-S levelswho received DHEA 30–90 mg/day for 4 weeks. Adecrease in depression ratings and an improvement inmemory performance correlated to increases inplasma levels of DHEA and DHEA-S, were observed.80
The effects of DHEA were also investigated in adouble-blind, placebo-controlled, randomized cross-over treatment study with 90 and 450 mg of DHEA, inpatients with midlife-onset dysthymia (a total of 6weeks on medication and 6 weeks on placebo). Of 17patients, 15 completed the study and 60% of thepatients responded to DHEA compared with 20% onplacebo.65 Finally, a double-blind, placebo-controlledstudy was conducted in 22 patients with majordepression (medication-free or on stabilized antide-pressant regimens). Utilizing DHEA at a maximumdose of 90 mg/day or placebo for 6 weeks, 45% of thepatients showed a decrease of 50% or greater indepressive symptoms, while none in the placebogroup.64
GR antagonistMifepristone (RU-486) is a nonselective antagonist ofthe GR receptor that has shown efficacy in psychoticdepression61,81,82 and on which there are ongoingtrials in bipolar disorder (reviewed in Manji et al83).Preliminary data with mifepristone (600 mg) com-pared to placebo in 19 subjects with bipolar depres-sion were recently presented.84 This group found abeneficial effect on mood and neurocognitive func-tioning. In a separate study not yet published, 208patients were randomized to receive 7 days ofmifepristone or placebo in addition to their ongoingtreatment for psychotic mayor depression. Althoughboth groups improved significantly, with no statisticaldifference among them, a post hoc analysis revealed
that mifepristone patients improved more rapidlythan the placebo group.85
Other GR antagonists being developed are ORG34517 (Organon), AL082D06 (Abbott), and Cyproter-one Acetate (Schering). Bachman et al86 have reportedsynthesizing three derivatives of mifepristone, withhigher selectivity for binding to GR, secondary todecreased binding to progesterone receptors (ORG34517, ORG 34850, and ORG 34116). Among theseagents, ORG 34517 is highly potent at the GR.Preliminary data for its antidepressant efficacy werepresented at the 2002 CINP meeting by Hoyberg et al87
This compound is now in phase III trials.Miner et al88 have reported a new compound,
AL082D06 (D06), discovered by screening compoundlibraries, that binds specifically to GR with nomeasurable binding affinity to the progesteronereceptor. This compound was found to antagonizeglucocorticoid-mediated transcriptional regulationin vitro cell-based models of transcriptional activation.
Cyproterone Acetate is available outside the US asan antiandrogen approved for paraphilias. It is usedas a contraceptive agent added to estradiol, combina-tion that is also widely used for hair growth. Honeret al89 have recently reported its GR antagonismproperties and while it could be tested in depression,it is unlikely to be clinically useful because of itsantiandrogenic properties and risk of severe liverdamage.
Inhibition of glucocorticoid synthesis has also beeninvestigated as an antidepressant strategy (consider-ing the risk for hypoadrenalism) in unipolar andbipolar patients and it has included the compoundsketoconazole (that possesses risk for hepatotoxicityand drug interaction), metyrapone, and amino-gluthethimide. See a review of relevant findings inTable 1.
Modulation of glutamate receptors may regulateneuroplasticity and cellular resilience: therapeuticimplications
One major neurotransmitter system regulated byglucocorticoids is the glutamatergic system. Regu-lated either via glucocorticoids or through alternativemechanisms, abnormal activity of the glutamatergicsystem represents a likely contributor to impairmentsin brain neuroplasticity and cellular resilience ob-served in patients with bipolar disorder. Glutamate isthe major excitatory synaptic neurotransmitter in thebrain and has several important roles includingmediating neurotransmission across excitatory sy-napses and regulating numerous physiological func-tions in the mammalian central nervous system(CNS), such as synaptic plasticity, learning, andmemory.90–93 Several treatment strategies have beenimplemented to reduce glutamate-mediated excito-toxicity, which results in robust neuroprotectiveeffects in a variety of preclinical paradigms; however,the data in humans with neurodegenerative diseaseare more equivocal. The same antiglutamatergic
Experimental treatments BPD IIJA Quiroz et al
763
Molecular Psychiatry

neuroprotective strategies used for these neurodegen-erative disorders may have an important role inpatients with mood disorders and are currently beingtested in ‘proof-of-concept’ studies in patients withmood disorders (see below). Glutamate levels mayrise to excitotoxic levels within minutes of suddeninsults such as cerebral trauma or ischemia, addingstress to the normal compensatory processes byoverloading the capacity of the glutamate transpor-ters.94 Glutamate then binds the receptor complex andunder certain conditions may further add to thisinsult by triggering a series of downstream toxicitypathways (Figure 1).
Noting the findings of the dysregulation of the HPAaxis in mood disorders, it is worth noting thatglucocorticoids have been demonstrated to exacerbateneuronal damage in models of excitotoxicity due toincreased glutamatergic transmission.95 Microdialysisstudies have shown that stress increases extracellularlevels of glutamate in hippocampus, and N-methyl-D-aspartate (NMDA) glutamate receptor antagonistsattenuate stress-induced atrophy of CA3 pyramidalneurons (for a review, see McEwen,23 Sapolsky95).Furthermore, subsets of hippocampal neurons thatshow damage after kainate-induced seizures show thehighest expression of GRs, with very high colocaliza-tion of GR immunoreactivity with AMPA receptors(AMPARs),96 suggesting that the survival of neuronswith high glutamatergic input may be particularlyregulated by GC. GCs can also directly prolong NMDAresponses, causing significantly more calcium entry,97
with higher calcium levels being a possible means ofendangering neurons to subsequent injury. In addi-tion, GC can alter expression patterns of glutamatereceptors to induce possibly dramatic changes inglutamatergic signaling in the CNS.98,99 Endogenousactivation of group II/III metabotropic glutamatereceptors has recently been shown to inhibit theHPA axis,100 and human studies has suggested that atleast some NMDA antagonists can increase cortisollevels.101 Therefore, the overlap between the HPA axisand glutamatergic systems may indicate that patho-logic changes in one parameter might induce mala-daptive states of the other and that treatmentsimproving one parameter might also provide bene-ficial effects to the other.
Owing to the role of glutamate in neuronalplasticity, and independent of interactions with theHPA axis, modulation of the glutamatergic system isbeing investigated as an antidepressant strategy in anumber of ongoing clinical studies by our group andothers (see Zarate et al102 for review). Glutamate exertsits action at the presynaptic and postsynaptic levelthrough the stimulation of specific receptors that canbe classified by structural characteristics (Figure 2):the first group, ‘ionotropic glutamate receptors’, areion channels that when stimulated open the channelpore allowing sodium, potassium, or calcium to flowfreely into the cell. This opening of the pore changesthe polarization of the neuronal surface and oftenactivates intracellular signaling pathways. The sec-
ond group, ‘metabotropic receptors’, are G-protein-coupled receptors that exert their actions throughsecond messenger pathways. Therapeutics can targetthese receptors; it is additionally possible to alsotarget the release of glutamate before it binds to eitherthe ionotropic or metabotropic receptors. Therapeu-tics directed at these different targets may result in themodulation of the glutamatergic system and ulti-mately to mood-enhancing effects (see Figure 2 forfurther information with regard to classification ofglutamate receptors). In the following sections, wefurther discuss inhibition of glutamate release, in-hibition of ionotropic glutamate receptors, and mod-ulation of metabotropic glutamate receptors as generalmechanisms to adjust the function of the glutamater-gic system. We follow with a discussion of someglutamatergic modulators that may possibly have arole in the treatment of mood disorders. These agentsinclude riluzole, memantine, felbamate, and zinc,glutamatergic modulators that appear to have neuro-protective properties in preclinical models with anapparently low risk of inducing psychotomimeticsymptoms compared to certain types of NMDAantagonists (such as PCP and ketamine). Testingdifferent glutamate-modulating agents that affectdifferent components of glutamatergic neurotransmis-sion may help discern what aspects of this system aremost relevant.
Inhibition of glutamate release
Clinical evidence that modulation of glutamate levelsmay be important in the treatment of mood disorderscomes from the clinical use of the anticonvulsantlamotrigine.103,104 Lamotrigine is FDA approved asadjunctive therapy for adults with partial seizuresand as adjunctive therapy in the generalized seizureof Lennox–Gastaut syndrome in pediatric and adultpatients. Lamotrigine has recently received FDAapproval for long-term maintenance treatment ofbipolar disorder, and appears to be most useful forthe treatment of bipolar depression and in preventingmood episode relapse.103,105 While lamotrigine hasmultiple cellular effects, an inhibition of an excessiverelease of glutamate appears to be important to itsmechanism of action.106–108 Lamotrigine reduces thehyperglutamatergic consequences of NMDA receptordysfunction (cognitive dysfunction learning andmemory impairment and psychomimetic effects)caused by ketamine in healthy volunteers.109 Thereis now evidence that another drug that inhibits therelease of glutamate (riluzole) also has antidepres-sants properties (see Zarate et al126 and the discussionbelow).
RiluzoleRiluzole is a neuroprotective agent with anticonvul-sant properties. Chemically, riluzole is 2-amino-6-(trifluoromethoxy) benzothiazole, and can easilycross the blood–brain barrier.110 Riluzole is the onlydrug currently approved (by the FDA in US, CPMP in
Experimental treatments BPD IIJA Quiroz et al
764
Molecular Psychiatry

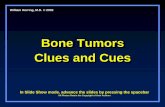
Figure 2 The glutamatergic system as a target of novel medications. Glutamate is synthesized in neuron from a-ketoglutaratethrough the tricarboxylic acid (TCA) cycle. After released, glutamate is reuptaken by glutamate transporters, shown in glia(GTg) and a presynaptic neuron (GTn). In the glia, glutamate is catabolized to glutamine (through the enzyme glutaminesynthetase), diffuses to the neurons, and is then metabolized back to glutamate (through the enzyme glutaminase). Thedifferent glutamate receptors and the presumed antiglutamatergic drug site of action are presented in the figure. Glutamate(Glu) exerts its action at the presynaptic and postsynaptic level through the stimulation of specific receptors that can beclassified by structural characteristics: the first group, ‘ionotropic glutamate receptors’ are ion channels that when stimulatedopen the channel pore allowing sodium, potassium, and calcium to flow freely into the cell. This opening of the pore changesthe polarization of the neuronal surface and activates intracellular signaling. NMDA and AMPA are ionotrophic glutamatereceptors. Activation of these receptors allows the entry into the cell of primarily calcium and sodium, respectively. Thesecond group metabotropic glutamate receptors’, mGluR are G-protein-coupled receptors, which directly act through secondmessenger pathways. Riluzole is a glutamate release inhibitor (acting through blockade of Naþ voltage dependent channels),a GABAA agonist, and probably an AMPA and Kainate antagonist. Lamotrigine has a number of biological effects (eginhibition of Naþ voltage-depend channels), including the inhibition of glutamate release. Memantine is a noncompetitiveantagonist NMDA receptor. Felbamate is a noncompetitive NMDA receptor antagonist (at glycine NR1 and glutamate NR2Bsubunits), an AMPA receptor antagonist, a mGlu group I receptor antagonist, and a glutamate release inhibitor (actingthrough blockade of Ca2þ and Naþ voltage-dependant channels). Ketamine is a high-affinity NMDA receptor antagonist. D-cycloserine is a partial agonist at the NMDA receptor glycine (Gly) site. At high does amantadine reduces NMDA receptorfunction by approximately 50%, an effect attributed to its instability within the NMDA receptor channel.229,230 Zinc is apotent inhibitor of the NMDA receptor complex. See text and102,195 for thorough description. AMPAkines allostericallyproduce positive modulation of AMPA receptors and have actively been studied in the treatment of schizophrenia.177 Studieshave shown that the biarylpropylsulfonamide AMPA receptor potentiators (LY392098 and LY451616) have antidepressanteffects in animal models of depression.126
Experimental treatments BPD IIJA Quiroz et al
765
Molecular Psychiatry

Europe, and MHW in Japan) for the treatment of ALS.Evidence from a variety of studies with experimentalanimals and with humans indicate that riluzole isdevoid of the psychotomimetic or other behavioralside effects commonly associated with excitatoryamino-acid antagonists.111,112 In contrast to meman-tine (discussed below), riluzole does not act directlyon the NMDA receptor.113 The mechanism of actionby which riluzole exerts its glutamatergic effect hasbeen reported to be through the inhibition of voltage-dependent sodium channels in mammalian CNSneurons114,115 and the reduction of glutamate re-lease.116 However, tetrodotoxin, a sodium channelblocking agent, failed to block the inhibitory effect ofriluzole on glutamate, suggesting that the effects ofthe drug are not exclusively mediated by its action onsodium channels.117 The anticonvulsant activity ofriluzole may also be due to its effect on neurotrans-mission mediated by the AMPA/KA receptors,113,118–121
however, the mechanism by which riluzole interactswith these receptors remains unclear. Recent studieshave shown that riluzole stimulates the synthesis ofgrowth factors including BDNF in cultured mouseastrocytes.122 This finding is of interest in thatprevious studies demonstrated that antidepressantand mood stabilizer treatments increase the expres-sion of BDNF in rat hippocampus and that infusion ofBDNF into the dentate gyrus of hippocampus pro-duces antidepressant effects in behavioral models ofdepression.123
Recent case reports,124–125 and an open label clinicaltrial,126 support the efficacy of riluzole in treatment-resistant depression. In the latter, 19 treatment-resistant patients with unipolar depression receivedriluzole monotherapy for up to 6 weeks. Patientstaking riluzole showed significant improvement onMADRS, CGI-S, and HAM-A scales.126 Larger, con-trolled trials are needed to confirm these interestingpreliminary findings.
Ionotropic glutamate receptors
Three different subgroups of glutamatergic ion chan-nels have been identified utilizing their pharmacolo-gical ability to bind different synthetic ligands, eachcomposed of a different set of subunits: N-methyl-D-Aspartate receptor (NMDA R), a-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptor (AMPAR), and kainate receptor (KA R). The latter two groupsare often referred to together as the ‘non-NMDA’receptors (Figure 2).
NMDA receptorA growing body of preclinical and clinical researchsuggests that the NMDA receptor complex may beinvolved in the pathophysiology of mood disordersand the mechanism of action of antidepressants andpossibly mood stabilizers (reviewed in Zarate et al102).NMDA receptor antagonists such as MK-801 and AP-7and an AMPA receptor potentiator have been shownto have antidepressant properties in animal models of
depression, including the forced swim test, theapplication of inescapable stressors, and tail suspen-sion immobility tests, in animals exposed to chronicmild stress, and in the learned helplessness models ofdepression, effects that are comparable to the tricyclicantidepressants.127–132 MK-801 increases neurogen-esis in the brains of rats.133 There is evidence thatthe NMDA receptor antagonist, ketamine, has efficacyin the treatment of depression. Berman et al134
reported the first placebo-controlled, double-blindtrial assessing the treatment effects of a single dose ofthe NMDA receptor antagonist, ketamine, in sevenpatients with depression. The authors reported thatsubjects with depression experienced a significantimprovement in depressive symptoms within a shortperiod of time (72 h) after receiving ketamine but notafter taking placebo. In addition, the ketamine-induced mood improvement persisted for 1–2 weeksafter the infusion.
Additional evidence of the role of the glutamatergicsystem in mood disorders comes from associations ofD-cycloserine and amantadine with affective symp-toms (Figure 2). In the 1950s, D-cycloserine (DCS), apartial agonist at the NMDA receptor glycine site usedas a part of multidrug antituberculosis treatment, wasreported to have mood-elevating effects.135–137 DCShas also been demonstrated to have antidepressantproperties in animal models of depression.138 Caseseries and blinded trials conducted with the non-competitive NMDA antagonist amantadine addition-ally are supportive. At a high dose, amantadinereduces NMDA receptor function by approximately50%, an effect attributed to its instability within theNMDA receptor channel.139–141 Amantadine has beenshown to have antidepressant effects in patients withParkinson’s disease and in unipolar and bipolarpatients142–144 but unlike its related compound,memantine, appears to have significant dopaminergiceffects. Studies in progress are examining the possibletherapeutic value of other NMDA receptor antagonistsincluding memantine, Felbamate, and Zinc.
MemantineMemantine has anticonvulsant and neuroprotectiveproperties and has been shown in double-blindplacebo-controlled studies to be effective in reducingclinical deterioration in Alzheimer’s, vascular, andmixed dementia of all severities.145–147 Chemically,memantine is a 1-amino-3,5-dimethyladamantane ofthe adamantine class, a compound that can easilycross the blood–brain barrier. Memantine is a potentnoncompetitive voltage-dependent NMDA antagonistwith a receptor effect comparable to MK-801148 andhas been demonstrated to inhibit [3H]MK-801 bindingto human hippocampal NMDA receptors.149 Meman-tine appears to block the NMDA receptor-associatedion channel only when it is open for long periods,thus promoting the view that it may be specific forblockade of pathological glutamate release. Owingto this mechanism of action, the untoward effectsof pathological concentrations of glutamate are
Experimental treatments BPD IIJA Quiroz et al
766
Molecular Psychiatry

prevented to a greater extent than the effects ofphysiological concentrations, which are relativelyspared.150,151
Memantine has been safely used in humans inmany clinical studies145–147 and has been recentlyapproved by the FDA for the treatment of Alzheimer’sdisorder. In preclinical studies, Moryl et al152 de-scribed a dose-dependent decrease in the immobilitytime in the forced swim test in rats followingadministration of memantine. A synergistic effectwas seen when imipramine and fluoxetine were givenjointly with memantine in the forced swim test inrats.153 Compared to the other NMDA antagonists,memantine has been reported to have the greatesteffective potency for binding at the MK-801 receptorsite in mouse brain as demonstrated by 18fluorine-PET154 and in human brain tissue. Memantine bindsto the MK-801 binding site of the NMDA receptor inpost-mortem human frontal cortex at therapeuticconcentrations,155 and reduces membrane currents.148
Memantine is well tolerated and only a few isolatedcases of psychosis (an effect of other NMDA antago-nists such as ketamine) and cognitive deficits havebeen reported. In summary, memantine is one of thefew NMDA antagonists available for use in humansand is ideal for testing in mood disorders, as it hasbeen in clinical use for many years with minimal sideeffects and has a very favorable pharmacologicalprofile.
FelbamateFelbamate (2-phenyl-1, 3-propanediol dicarbamate) isa unique broad-spectrum anticonvulsant chemicallyrelated to the anxiolytic, meprobamate.156 Felbamateexhibits neuroprotective properties in hypoxia–ische-mia models, hippocampal traumatic injury models,and in excitotoxic insult in cell cultures.157,158 Ketteret al159 reported stimulant-like effects with felbamatein patients with epilepsy and noted that half of thepatients who received chronic open felbamate dis-played modest psychiatric improvement compared tobaseline. The authors summarized some of thesepositive reports with felbamate describing ‘improvedalertness, attention and concentration, as well asimproved social, intellectual, mnestic and globalfunction’ and suggested that this drug may haveantidepressant properties.160 Gay et al161 have re-ported improved attention, alertness, and initiative inchildren taking felbamate.
The therapeutic action of felbamate in refractoryepilepsy may be related to novel noncompetitiveantagonism (relative to NMDA and glycine) specifi-cally at the NMDA NR1 and NR2B subunit. Felbamateappears to inhibit the function of the NMDA receptorcomplex through an interaction with the strychnine-insensitive glycine recognition site. Felbamate, butnot carbamazepine or valproic acid, increased [3H]5,7DCKA glycine binding in rat brain and sections ofhuman post-mortem brain.162 Notably, the binding inhuman post-mortem brain increased by as much as41% in CA2 region of the hippocampus163 in
comparison to carbamazepine and valproic acid.Thus, the anticonvulsant and neuroprotective effectsof felbamate may act through the inhibition of NMDAreceptor function via an allosteric modulation of theglycine site.162,164 In addition, felbamate has a four- to10-fold preference for the NR2B-containing recep-tors165 (Figure 2) and at high concentrations, felba-mate also enhances GABAA activity, inhibits AMPA/kainite receptors, and inhibits dihydropyridine-sen-sitive calcium channels.156 The use of felbamate hasbeen limited by the unexpected increased risk ofaplastic anemia and toxic hepatitis.166 Despite thesepotentially life-threatening side effects, considerationshould be given to the exploration of the use offelbamate in treatment-resistant mood disorders.
ZincZinc is a potent inhibitor of the NMDA receptor, playsan important role in a wide range of biochemicalprocesses,167 and could have a role in the treatment ofmood disorders. Chronic electroconvulsive shocktreatment of rats was reported to be associated withan increase in the zinc concentration in the hippo-campus.168 Recently, zinc has been reported to haveantidepressant-like properties in forced swim test andolfactory bulbectomy model in rats.169–171 In humans,although an indirect indication of CNS zinc levels,lower zinc blood concentrations were found indepressed patients, which normalized after success-ful antidepressant therapy.168,172,173 In a placebo-controlled study, adjunctive treatment with zinc hasrecently been shown to have antidepressant effects.174
Interestingly, zinc, like lithium, inhibits the enzymeglycogen synthase kinase-3 (GSK-3).175 Thus, futurestudies will need to differentiate between the NMDAand GSK-3 effects of zinc.
AMPA receptorAMPA receptors are a subfamily of ionotropicglutamate receptors that mediate the fast componentof excitatory neurotransmission, which, like NMDAreceptors, are involved in learning and memory.Several classes of compounds can allostericallymodulate AMPA receptors. These compounds (theso-called AMPA receptor positive modulators orAMPA receptor potentiators, ARPs) do not activateAMPA receptors themselves but slow the rate ofreceptor desensitization and/or deactivation in thepresence of an agonist (eg glutamate and AMPA) (seeBorges and Dingledinc,176 Bleakman and Lodge177 fora review). AMPAkines, a subclass of ARPs, are smallbenzamide compounds that allosterically producepositive modulation of AMPA receptors that haveactively been studied in the treatment of schizophre-nia.178 Studies have shown that the biarylpropylsul-fonamide AMPA receptor potentiators (LY392098 andLY451616) have antidepressant effects in animalmodels of depression (including the application ofinescapable stressors, forced swim test, and tail-suspension-induced immobility tests), in learnedhelplessness models of depression, and in animals
Experimental treatments BPD IIJA Quiroz et al
767
Molecular Psychiatry

exposed to chronic mild stress procedure.127 In one ofthese preclinical studies, the AMPAkine, Ampalexwas reported to have a more rapid effect (during thefirst week of treatment) than fluoxetine (after 2weeks).179 In contrast to traditional antidepressants,this group of compounds does not appear to affect theextracellular concentration of monoamines.180 How-ever, they can enhance the neurotrophic actions ofbrain-derived neurotrophic factor (BDNF) mRNA andprotein in primary neuronal cultures.181 Modulationof neurotrophic factor expression and altering the rateof neurogenesis may be critical factors in under-standing the therapeutic effects of antidepressantsand mood stabilizers in mood disorders. In support,chronic treatment with the AMPA receptor potentia-tor LY451646 increased progenitor cell proliferationin the dentate gyrus in a dose-dependent manner. Theantidepressant-like activity of ARPs in animals maybe attributed, at least in part, to the regulation of cellproliferation in the hippocampus.182 (Figure 2).
Metabotropic glutamate receptors
In addition to the ionotropic receptors, three groupscompromised of eight G-protein-coupled metabotro-pic glutamate receptors (mGluR) mediate slowermodulatory actions of glutamate on neurotransmitterrelease and cell excitability (Figure 2). Activation ofmGluR leads to a variety of cellular responses,including the inhibition of calcium and potassiumcurrents, presynaptic modulation of synaptic trans-mission, and postsynaptic interaction with ionotropicglutamate receptors.183–185 The mGluR are involved inthe early phase of memory formation and themechanism of long-term depression.186–188 Group ImGluRs have been found to exhibit potential ther-apeutic effects in CNS disorders related to excessexcitatory neurotransmission such as epilepsy, pain,and ischemia (see Nicoletti et al189 for a review).Preclinical studies suggest that mGlu 2/3 agonistshave antianxiety, antipsychotic, and neuroprotectiveproperties.190,191 However, selective activation/antag-onism of various mGluRs can lead to either anxioly-tic- and/or antidepressant-like effects192–195 andspecific interactions of each receptor subtype are anintensive area of investigation (see Zarate et al102 for areview). Taking into account that every group ofmGluR (see Figure 2) can simultaneously couple withdifferent subgroups of G-protein subunits, and thatinteractions with glutamate ionotropic receptors andother ion channels have been described, this complexsystem offers a tremendous potential in the search fornovel therapeutic strategies in CNS disorders (includ-ing mood disorders).
In conclusion, there is ample evidence frompreclinical and clinical research that the glutamater-gic system is involved in the pathophysiology ofmood disorders and that testing of glutamate-mod-ulating agents in ‘proof-of-concept’ studies mayprovide an insight into the pathophysiology of mooddisorders and may help open a new pathway for drug
development. It should be acknowledged that manyof the drugs reviewed here have effects on the otherneurotransmitter systems in addition to their often,indirect effects on glutamate function.
Strategies to potentiate neurotrophic cascades forthe treatment of bipolar disorder
There is a growing body of data suggesting that agentsthat directly modulate neurotrophic cascades, such asthe CREB/BDNF/bcl-2 cascade, may have utility forthe treatment of mood disorders (see Figure 3 and D’saand Duman20 for a review). Specifically, they mayrepresent a mechanism to attenuate or reverse thedeficits in neuroplasticity and cellular resilienceobserved in patients with bipolar disorder describedearlier in this article. One approach to increase CREBactivity, and thus neurotrophic signaling (Figure 3),utilizes inhibition of phosphodiesterase (PDE), theenzymes responsible for the breakdown of cAMP.Adenylate cyclase-mediated production of cAMP
Figure 3 Cyclic AMP signaling pathway. Extracellularreceptors can be both positively (eg b-adrenergic, D1) ornegatively (eg 5-HT1A, D2) coupled to adenylyl cyclase toregulate cyclic AMP (cAMP) levels. The effects of cAMP aremediated largely by activation of protein kinase A (PKA).One major downstream target of PKA is CREB (cAMPresponse element binding protein). After activation, phos-phorylated CREB binds to the cAMP response element(CRE), a gene sequence found in the promoter of certaingenes (including BDNF and bcl-2); recent data suggest thatantidepressants196 and also mood-stabilizing drugs231 mayactivate CREB, thereby bringing about increased expressionof a major target gene, BDNF. Phosphodiesterase is anenzyme that breaks down cAMP to AMP. Drugs likerolipram, which inhibit phosphodiesterase, may be usefulas adjunct treatments for depression. Thus, it is hypothe-sized that phosphodiesterase inhibitors may represent adistinct class of treatments for mood disorders, perhapsacting by increasing the activity of neurotrophic signalingpathways and attenuating impairments in neuroplasticityand cellular resilience associated with these illnesses.
Experimental treatments BPD IIJA Quiroz et al
768
Molecular Psychiatry

leads to the activation of protein kinase A andsubsequent phosphorylation-mediated activation ofCREB. CREB, in turn, increases transcription of manygenes including BDNF and bcl-2 (see Duman196 for areview). In this context, Takahashi et al.197 demon-strated that chronic antidepressant administrationincreases the expression of cAMP-specific phospho-diesterase (PDE) 4A and 4B isoforms; these effectslikely represent a compensatory ‘counter-regulatory’response to the chronic antidepressant administra-tion.198 These data suggest that PDE4A and PDE4Bmay be relevant targets for the development of agentsthat possess antidepressant effects either as mono-therapy, or in combination with agents that increaseintrasynaptic monoamine levels, due to the possiblesynergism of effects on the cAMP cascade. Preclinicalstudies conducted to date do support the potentialutility of PDE4 inhibitors in the treatment of depres-sive disorders. Thus, long-term administration ofPDE4 inhibitors increases the expression of CREBand BDNF in the hippocampus of rats,199,200 and PDEinhibitors likewise have antidepressant-like effects inbehavioral models.201–203
Indeed, the idea that PDE inhibitors may havepotential antidepressant activity is not a new one, andwas initially proposed by Wachtel in the early1980s.203 In the 1980s and early 1990s, a number ofopen204 and controlled clinical trials205–208 demon-strated that rolipram, a specific inhibitor of the high-affinity cAMP PDE4, may have antidepressant effi-cacy in depressed patients. In addition, there isevidence that rolipram may have a faster onset ofresponse compared to the standard antidepressants.In a clinical study by Horowski et al,209 a rapidantidepressant effect to rolipram was reported tooccur within the first 12 h to 10 days, and anotherstudy204 reported an antidepressant effect only after 2to 4 days of treatment. However, a randomizeddouble-blind comparative trial of rolipram vs imipra-mine carried out by Hebenstreit et al207 found thatimipramine was more effective than rolipram,although both were beneficial. Further, in a controlledstudy by Scott et al,210 they concluded that amitripty-line was more effective than rolipram in the treatmentof depressed inpatients. Although the overall litera-ture on the use of rolipram is suggestive that PDEinhibitors may have antidepressant efficacy and mayhave a faster onset of action, the potential use ofrolipram for depression was limited because of sideeffects such as nausea and emesis.
Recent studies demonstrating that PDE4 is ex-pressed in inflammatory cells such as eosinophilsand that inhibition of PDE4 downregulates theinflammatory response, has generated renewed ex-citement about the possible utility of this class ofagents in the treatment of diseases such as asthma,chronic obstructive pulmonary disease (COPD), rheu-matoid arthritis, Crohn’s disease, and multiplesclerosis (MS).211,212 Second-generation compoundswith markedly improved tolerability are rapidly beingdeveloped,211,212 and it is anticipated that the avail-
ability of CNS-penetrant PDE4 inhibitors may lead tothe development of a novel class of antidepressants.Importantly, some mood stabilizers may attenuateadenylate cyclase mediated signaling—and that thisrepresents a putative mechanism of action (see Gouldet al2 for a review). Thus, future preclinical studieswill likely discern region and cell specificity of thesefindings.
Human phase I/II trials of recombinant methionylhuman brain-derived neurotrophic factor have al-ready been undertaken, wherein the BDNF wasadministered by intrathecal infusion to patients withamyotrophic lateral sclerosis.213 Unfortunately, sideeffects such as sensory symptoms, including par-esthesias or a sense of warmth, sleep disturbance, drymouth, agitation, and other behavioral effects wereencountered at higher doses, precluding furtherstudy.
An increasing number of strategies are beinginvestigated to develop small molecule switches forprotein–protein interactions, which have the poten-tial to regulate the activity of growth factors, MAPkinases cascades, and interactions between homo-and heterodimers of the bcl-2 family of proteins. Inview of the robust effects of bcl-2 on neuritesprouting, neurite outgrowth and axonal regenera-tion,214–218 and protection against the deleterious CNSeffects of severe stress,219 it is quite possible that bcl-2enhancers will have utility in the treatment of bipolardisorder. Indeed, lithium’s ability to upregulate bcl-2robustly may play a role in many of its therapeuticeffects. It is also worth noting that pramipexole alsoupregulates bcl-2 in several brain areas,220 and hasbeen shown to exert antidepressant effects.221 Whilethe dopamine agonistic effects of pramipexole mayclearly also contribute to its purported antidepressanteffects, its robust neurotrophic effects suggest that itmay have broader utility as an antidepressant poten-tiator. In this context, recent studies at the NIMH221
and elsewhere222 have found pramipexole to be moreeffective than placebo in treating bipolar depression;ongoing longitudinal studies at the NIMH are furtherexploring putative neurotrophic effects with the useof serial MRS measurements of NAA, and volumetricMRIs.
Conclusions
Bipolar disorder is a devastating disorder, whichexerts a major toll on millions of sufferers worldwide.While recent years have seen the introduction of alarge number of agents into the pharmacopeia andundoubtedly provides the clinician with many morechoices, there has been little progress in developingtruly novel drugs specifically for the illness. Currentlyavailable medications have—by and large—beendeveloped for the treatment of other disorders likeepilepsy or schizophrenia, and therefore are notoptimal in the treatment of bipolar disorder, preven-tion of relapses, improving functioning, or treatingthe deleterious effects of this illness on other organ
Experimental treatments BPD IIJA Quiroz et al
769
Molecular Psychiatry

systems. We propose that new medications will likelyderive from both understanding mechanisms ofcurrent drug actions and by directing medications atcritical ‘signaling nodes’ determined to be at thenexus of interacting intracellular cascades.
Evolving theories of bipolar disorder neurobiologyare attempted to elucidate the complex interaction ofmultiple susceptibility (and protective) genes andenvironmental factors that regulate cellular plasticity.These interactions result in the phenotypic expres-sion of a disease that includes not only episodic andoften profound mood disturbance but also a con-stellation of cognitive, motoric, autonomic, endo-crine, sleep/wake abnormalities,223 and possiblyother systemic manifestations. Numerous genetic locihave been associated with bipolar disorder and it islikely that specific gene mutations associated with theillness will soon be identified. This endeavor willundoubtedly uncover reproducible susceptibilitygenes; however, the next task will involve placingthe complex picture together—using molecular, cel-lular, circuit, and behavioral neuroscience—withpathophysiological theories of the origins of bipolardisorder. Modulation of the HPA axis through inhibi-tion of CRH receptors, glucocorticoid receptors, orother means such as glucocorticoid synthesis maydesignate a novel class of medications that directlytarget pathophysiological processes involved in mooddisorders. As we discussed, there is a growing body ofdata suggesting that agents that modulate the gluta-matergic system may have utility in the long-termtreatment of severe mood disorders. In general,glutamatergic ‘plasticity-enhancing’ strategies includeinhibitors of glutamate release agents, NMDA antago-nists, AMPA potentiators, and metabotropic receptoragonists/antagonists. Thus, neuroprotective strategiesused for the treatment of neurodegenerative disordersmay have an important role in the treatment of mooddisorders, and are currently being tested in ‘proof-of-concept’ studies in patients. Phosphodiesterase in-hibitors may additionally be advantageous as amechanism to increase the levels of neurotrophicmolecules such as BDNF and bcl-2, which areresponsive to increases in CREB. Such studies mayultimately lead to a better understanding of thepathophysiology of recurrent unipolar depressionand bipolar disorder, and result in the developmentof improved therapeutics. It is critical to rememberthat while theories abound, ultimate validation(especially considering available animal models ofbipolar disorder224,225) will rest in the results ofclinical trials. This is not likely to be a simpleprocess, and indeed numerous methodological andstudy design issues have emerged from both con-trolled randomized trials and various longitudinalobservations of bipolar disorder patients followed forup to 20 years. Some of these methodologicalconcerns, which have been eloquently articulatedelsewhere,225,227 include the following: (i) there aremultiple subtypes of clinical presentation embeddedin current diagnosis; (ii) multiple response possibi-
lities are present; (iii) there appear to be changingresponse patterns over time; (iv) inadequate attentionis paid to combination treatments; and (v) there arehigh drop out and noncompliance rates. Whenconsidering the complexity, morbidity, and mortalityof bipolar disorder, it has been suggested that thedesired attribute of ideal new agents for the treatmentof bipolar disorder should include as many of thefollowing attributes as possible:226,227 (i) efficacy inthe treatment of acute hypomania/mania; (ii) efficacyin the treatment of acute depression; (iii) efficacy inthe acute treatment of mixed states; (iv) efficacy in thetreatment of acute episodes associated with rapidcycling bipolar disorder; (v) reducing subsyndromesor residual mood symptoms; (vi) efficacy in thetreatment of psychotic symptoms that frequentlyaccompany depressive or manic episodes; (v) abilityto prevent both relapses and recurrences; (vi) redu-cing the need for concomitant medications; (vii)preventing suicide; (viii) decreasing time-ill; (ix)decreasing substance abuse and other comorbidities;(x) preventing/reducing chronicity; (xi) improvingcognition and preventing cognitive decline; (xii)restoring full social and occupational functioningand quality of life; (xiii) rapidly acting; (xiv) few sideeffects; and (xv) preventing the systematic manifesta-tions resulting from mood episodes.
It is clear that we will never develop such idealmagic bullets; however, as we have outlined here,evidence derived from neuroimaging, post-mortembrain, biochemical and pharmacologic studies allsupport the contention that impairments of cellularplasticity and resilience are integral to the pathophy-siology of bipolar disorder. Furthermore, a growingbody of data suggest that although bipolar disorder isnot a classical mitochondrial disorder, many of theupstream abnormalities (likely nuclear genomecoded) converge to regulate mitochondrial fun-ction implicated both in abnormalities of neurotrans-mitter synaptic plasticity and long-term cellularresilience. 240–243 There is growing apprecition thatneuronal mitochondria participate not only in oxida-tive phosphorylation and —in networks with ER— incalcium uptake, but also in cellular resilience andneurotransmitter synaptic function. Thus, agentscapable of reversing the mitochondrial-driven impair-ments of cellular plasticity and resilience in biplolardisorder have the potential of becoming new ther-apeutic classes of mood-stabilizing drugs. Agentscapable actively being investigated include pramipex-ole (a bcl-2 enhancer), coenzyme Q10 and carnitine(respirtory chain enhancers). 221–245,246 It is ourcontention that targeting these cellular plasticitycascades will lead to truly novel (and hopefullyimproved) treatements for these devastating illnesses.
Acknowledgements
We acknowledge the support of the IntramuralResearch Program of the National Institute of MentalHeath and the Stanley Medical Research Institute.
Experimental treatments BPD IIJA Quiroz et al
770
Molecular Psychiatry

TDG is supported by Foundation for NIH Fellowship.JAQ and TDG are supported by NARSAD YoungInvestigators Awards. Owing to space limitations, weoften cited review papers and apologize to thoseauthors whose original data could not be included.
References
1 Goodwin FK, Ghaemi SN. The course of bipolar disorder andthe nature of agitated depression. Am J Psychiatry 2003; 160:2077–2079.
2 Gould TD, Quiroz J, Singh J, Zarate Jr CA, Manji HK. Emergingexperimental therapeutics for bipolar disorder: insights from themolecular and cellular actions of current mood stabilizers. MolPsychiatry 2004.
3 Schulze TG, McMahon FJ. Genetic linkage and associationstudies in bipolar affective disorder: a time for optimism. Am JMed Genet 2003; 123C: 36–47.
4 Sheline YI. Neuroimaging studies of mood disorder effects on thebrain. Biol Psychiatry 2003; 54: 338–352.
5 Drevets WC. Functional anatomical abnormalities in limbic andprefrontal cortical structures in major depression. Prog Brain Res2000; 126: 413–431.
6 Manji HK, Drevets WC, Charney DS. The cellular neurobiology ofdepression. Nat Med 2001; 7: 541–547.
7 Drevets WC. Neuroimaging abnormalities in the amygdala inmood disorders. Ann NY Acad Sci 2003; 985: 420–444.
8 Manji H, Duman R. Impairments of neuroplasticity and cellularresilience in severe mood disorder: implications for the devel-opment of novel therapeutics. Psychopharmacol Bull 2001; 35:5–49.
9 Drevets WC. Neuroimaging and neuropathological studies ofdepression: implications for the cognitive–emotional features ofmood disorders. Curr Opin Neurobiol 2001; 11: 240–249.
10 Strakowski SM, Adler CM, DelBello MP. Volumetric MRI studiesof mood disorders: do they distinguish unipolar and bipolardisorder? Bipolar Disord 2002; 4: 80–88.
11 Beyer JL, Krishnan KR. Volumetric brain imaging findings inmood disorders. Bipolar Disord 2002; 4: 89–104.
12 Cotter D, Mackay D, Landau S, Kerwin R, Everall I. Reduced glialcell density and neuronal size in the anterior cingulate cortexin major depressive disorder. Arch Gen Psychiatry 2001; 58:545–553.
13 Rajkowska G. Cell pathology in bipolar disorder. Bipolar Disord2002; 4: 105–116.
14 Lenox RH, Gould TD, Manji HK. Endophenotypes in bipolardisorder. Am J Med Genet 2002; 114: 391–406.
15 Carmelli D, Reed T, DeCarli C. A bivariate genetic analysis ofcerebral white matter hyperintensities and cognitive performancein elderly male twins. Neurobiol Aging 2002; 23: 413–420.
16 Taylor WD, Payne ME, Krishnan KR, Wagner HR, Provenzale JM,Steffens DC et al. Evidence of white matter tract disruption inMRI hyperintensities. Biol Psychiatry 2001; 50: 179–183.
17 Lee SH, Payne ME, Steffens DC, McQuoid DR, Lai TJ, ProvenzaleJM et al. Subcortical lesion severity and orbitofrontal cortexvolume in geriatric depression. Biol Psychiatry 2003; 54:529–533.
18 Mezzapesa DM, Rocca MA, Pagani E, Comi G, Filippi M.Evidence of subtle gray-matter pathologic changes in healthyelderly individuals with nonspecific white-matter hyperintensi-ties. Arch Neurol 2003; 60: 1109–1112.
19 Stoll AL, Renshaw PF, Yurgelun-Todd DA, Cohen BM. Neuroi-maging in bipolar disorder: what have we learned? BiolPsychiatry 2000; 48: 505–517.
20 D’Sa C, Duman R. Antidepressants and neuroplasticity. BipolarDisorder 2002; 4: 183.
21 Lopez JF, Chalmers DT, Little KY, Watson SJ. AE BennettResearch Award. Regulation of serotonin1A, glucocorticoid, andmineralocorticoid receptor in rat and human hippocampus:implications for the neurobiology of depression. Biol Psychiatry1998; 43: 547–573.
22 Sapolsky RM. Glucocorticoids and hippocampal atrophy inneuropsychiatric disorders. Arch Gen Psychiatry 2000; 57:925–935.
23 McEwen BS. Stress and hippocampal plasticity. Annu RevNeurosci 1999; 22: 105–122.
24 Sapolsky RM, Romero LM, Munck AU. How do glucocorticoidsinfluence stress responses? Integrating permissive, suppressive,stimulatory, and preparative actions. Endocr Rev 2000; 21:55–89.
25 Sapolsky RM. Stress, glucocorticoids, and damage to the nervoussystem: the current state of confusion. Stress 1996; 1: 1–19.
26 Gould E, Tanapat P, Rydel T, Hastings N. Regulation ofhippocampal neurogenesis in adulthood. Biol Psychiatry 2000;48: 715–720.
27 Kempermann G, Kuhn HG, Gage FH. More hippocampal neuronsin adult mice living in an enriched environment. Nature 1997;386: 493–495.
28 van Praag H, Kempermann G, Gage FH. Running increases cellproliferation and neurogenesis in the adult mouse dentate gyrus.Nat Neurosci 1999; 2: 266–270.
29 Cameron HA, McKay RD. Restoring production of hippocampalneurons in old age. Nat Neurosci 1999; 2: 894–897.
30 Malberg JE, Eisch AJ, Nestler EJ, Duman RS. Chronic antidepres-sant treatment increases neurogenesis in adult rat hippocampus.J Neurosci 2000; 20: 9104–9110.
31 Chen G, Rajkowska G, Du F, Seraji-Bozorgzad N, Manji HK.Enhancement of hippocampal neurogenesis by lithium. J Neu-rochem 2000; 75: 1729–1734.
32 Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, Dulawa S etal. Requirement of hippocampal neurogenesis for the behavioraleffects of antidepressants. Science 2003; 301: 805–809.
33 Vollmayr B, Simonis C, Weber S, Gass P, Henn F. Reduced cellproliferation in the dentate gyrus is not correlated with thedevelopment of learned helplessness. Biol Psychiatry 2003; 54:1035–1040.
34 Rupniak NM. Elucidating the antidepressant actions of substanceP (NK1 receptor) antagonists. Curr Opin Invest Drugs 2002; 3:257–261.
35 Morcuende S, Gadd CA, Peters M, Moss A, Harris EA, Sheasby Aet al. Increased neurogenesis and brain-derived neurotrophicfactor in neurokinin-1 receptor gene knockout mice. Eur JNeurosci 2003; 18: 1828–1836.
36 Sheline YI, Sanghavi M, Mintun MA, Gado MH. Depressionduration but not age predicts hippocampal volume loss inmedically healthy women with recurrent major depression.J Neurosci 1999; 19: 5034–5043.
37 MacQueen GM, Campbell S, McEwen BS, Macdonald K, AmanoS, Joffe RT et al. Course of illness, hippocampal function, andhippocampal volume in major depression. Proc Natl Acad SciUSA 2003; 100: 1387–1392.
38 Sheline YI, Gado MH, Kraemer HC. Untreated depressionand hippocampal volume loss. Am J Psychiatry 2003; 160:1516–1518.
39 Vermetten E, Vythilingam M, Southwick SM, Charney DS,Bremner JD. Long-term treatment with paroxetine increasesverbal declarative memory and hippocampal volume in posttrau-matic stress disorder. Biol Psychiatry 2003; 54: 693–702.
40 Lyons DM, Yang C, Sawyer-Glover AM, Moseley ME, SchatzbergAF. Early life stress and inherited variation in monkeyhippocampal volumes. Arch Gen Psychiatry 2001; 58:1145–1151.
41 Gilbertson MW, Shenton ME, Ciszewski A, Kasai K, Lasko NB,Orr SP et al. Smaller hippocampal volume predicts pathologicvulnerability to psychological trauma. Nat Neurosci 2002; 5:1242–1247.
42 Wellman CL. Dendritic reorganization in pyramidal neurons inmedial prefrontal cortex after chronic corticosterone administra-tion. J Neurobiol 2001; 49: 245–253.
43 Lyons DM. Stress, depression, and inherited variation in primatehippocampal and prefrontal brain development. Psychopharma-col Bull 2002; 36: 27–43.
44 Sonino N, Fava GA. Psychiatric disorders associated withCushing’s syndrome. Epidemiology, pathophysiology and treat-ment. CNS Drugs 2001; 15: 361–373.
Experimental treatments BPD IIJA Quiroz et al
771
Molecular Psychiatry

45 Krystal A, Krishnan KR, Raitiere M, Poland R, Ritchie JC,Dunnick NR et al. Differential diagnosis and pathophysiologyof Cushing’s syndrome and primary affective disorder. J Neurop-sychiatry Clin Neurosci 1990; 2: 34–43.
46 Kelly WF, Kelly MJ, Faragher B. A prospective study ofpsychiatric and psychological aspects of Cushing’s syndrome.Clin Endocrinol (Oxf) 1996; 45: 715–720.
47 Starkman MN, Giordani B, Gebarski SS, Berent S, Schork MA,Schteingart DE. Decrease in cortisol reverses human hippocam-pal atrophy following treatment of Cushing’s disease. BiolPsychiatry 1999; 46: 1595–1602.
48 Simmons NE, Alden TD, Thorner MO, Laws Jr ER. Serum cortisolresponse to transsphenoidal surgery for Cushing disease.J Neurosurg 2001; 95: 1–8.
49 Brown ES, Khan DA, Nejtek VA. The psychiatric side effects ofcorticosteroids. Ann Allergy Asthma Immunol 1999; 83: 495–503,quiz 503–494.
50 Sirois F. Steroid psychosis: a review. Gen Hosp Psychiatry 2003;25: 27–33.
51 Sharfstein SS, Sack DS, Fauci AS. Relationship between alter-nate-day corticosteroid therapy and behavioral abnormalities.JAMA 1982; 248: 2987–2989.
52 Plotsky PM, Owens MJ, Nemeroff CB. Psychoneuroendocrinologyof depression. Hypothalamic–pituitary–adrenal axis. PsychiatrClin North Am 1998; 21: 293–307.
53 Lopez JF, Little KY, Lopez-Figueroa AL, Lopez-Figueroa MO,Watson SJ In: Charney DS (ed) Society of Biological PsychiatryAnnual Meeting, Vol 9s Elsevier Science Inc.: San Francisco,2003.
54 Webster MJ, Knable MB, O’Grady J, Orthmann J, Weickert CS.Regional specificity of brain glucocorticoid receptor mRNAalterations in subjects with schizophrenia and mood disorders.Mol Psychiatry 2002; 7: 985–994, 924.
55 Nemeroff CB, Owens MJ, Bissette G, Andorn AC, Stanley M.Reduced corticotropin releasing factor binding sites in the frontalcortex of suicide victims. Arch Gen Psychiatry 1988; 45: 577–579.
56 Young EA, Lopez JF, Murphy-Weinberg V, Watson SJ, Akil H.Mineralocorticoid receptor function in major depression. ArchGen Psychiatry 2003; 60: 24–28.
57 Gould TD, Gray NA, Manji HK. The cellular neurobiology ofsevere mood and anxiety disorders: implications for the devel-opment of novel therapeutics. In: DS Charney (ed) MolecularNeurobiology for the Clinician. American Psychiatric Press, Inc.:Washington, 2003 pp 123–227.
58 Gold PW, Chrousos GP. Organization of the stress system and itsdysregulation in melancholic and atypical depression: high vslow CRH/NE states. Mol Psychiatry 2002; 7: 254–275.
59 Wolkowitz OM, Reus VI, Chan T, Manfredi F, Raum W, Johnson Ret al. Antiglucocorticoid treatment of depression: double-blindketoconazole. Biol Psychiatry 1999; 45: 1070–1074.
60 Malison RT, Anand A, Pelton GH, Kirwin P, Carpenter L,McDougle CJ et al. Limited efficacy of ketoconazole in treat-ment-refractory major depression. J Clin Psychopharmacol 1999;19: 466–470.
61 Belanoff JK, Flores BH, Kalezhan M, Sund B, Schatzberg AF.Rapid reversal of psychotic depression using mifepristone. J ClinPsychopharmacol 2001; 21: 516–521.
62 Young AH, Gallagher P, Watson S, Del-Estal D, Owen BM, FerrierNI. Improvements in neurocognitive function and mood follow-ing adjunctive treatment with mifepristone (RU-486) in bipolardisorder. Neuropsychopharmacology, (in press).
63 DeBattista C, Posener JA, Kalehzan BM, Schatzberg AF. Acuteantidepressant effects of intravenous hydrocortisone and CRH indepressed patients: a double-blind, placebo-controlled study. AmJ Psychiatry 2000; 157: 1334–1337.
64 Wolkowitz OM, Reus VI, Keebler A, Nelson N, Friedland M,Brizendine L et al. Double-blind treatment of major depressionwith dehydroepiandrosterone. Am J Psychiatry 1999; 156:646–649.
65 Bloch M, Schmidt P, Danaceau MLA, Rubinow D. Dehydroepian-drosterone treatment of midlife dysthymia. Biol Psychiatry 1999;45: 1533–1541.
66 Saunders J, Williams J. Antagonists of the corticotropin releasingfactor receptor. Prog Med Chem 2003; 41: 195–247.
67 Holmes A, Heilig M, Rupniak NM, Steckler T, Griebel G.Neuropeptide system as novel therapeutic targets for depressionand anxiety disorders. Trends Pharmacol Sci 2003; 24: 580–588.
68 Webster EL, Lewis DB, Torpy DJ, Zachman EK, Rice KC, ChrousosGP. In vivo and in vitro characterization of antalarmin, anonpeptide corticotropin-releasing hormone (CRH) receptorantagonist: suppression of pituitary ACTH release and peripheralinflammation. Endocrinology 1996; 137: 5747–5750.
69 Habib KE, Weld KP, Rice KC, Pushkas J, Champoux M, Listwak Set al. Oral administration of a corticotropin-releasing hormonereceptor antagonist significantly attenuates behavioral, neuroen-docrine and autonomic responses to stress in primates. Proc NatlAcad Sci USA 2000; 97: 6079–6084.
70 Ducottet C, Griebel G, Belzung C. Effects of the selectivenonpeptide corticotropin-releasing factor receptor 1 antagonistantalarmin in the chronic mild stress model of depression inmice. Prog Neuropsychopharmacol Biol Psychiatry 2003; 27:625–631.
71 Seymour PA, Schmidt AW, Schulz DW. The pharmacology of CP-154,526, a non-peptide antagonist of the CRH1 receptor: a review.CNS Drug Rev 2003; 9: 57–96.
72 Mansbach RS, Brooks EN, Chen YL. Antidepressant-like effects ofCP-154,526, a selective CRF1 receptor antagonist. Eur J Pharma-col 1997; 323: 21–26.
73 Griebel G, Simiand J, Steinberg R, Jung M, Gully D, Roger P et al.4-(2-Chloro-4-methoxy-5-methylphenyl)-N-[(1S)-2-cyclopropyl-1-(3-fluoro-4-methylphenyl)ethyl]5-methyl-N-(2-propynyl)-1, 3-thiazol-2-amine hydrochloride (SSR125543A), a potent andselective corticotrophin-releasing factor1 receptor antagonist. II.Characterization in rodent models of stress-related disorders.J Pharmacol Exp Ther 2002; 301: 333–345.
74 Okuyama S, Chaki S, Kawashima N, Suzuki Y, Ogawa S,Nakazato A et al. Receptor binding, behavioral, and electro-physiological profiles of nonpeptide corticotropin-releasingfactor subtype 1 receptor antagonists CRA1000 and CRA1001.J Pharmacol Exp Ther 1999; 289: 926–935.
75 Harro J, Tonissaar M, Eller M. The effects of CRA 1000, a non-peptide antagonist of corticotropin-releasing factor receptor type1, on adaptive behaviour in therat. Neuropeptides 2001; 35:100–109.
76 Li, Y-W, Hill G, Wong H, Kelly N, Ward K, Pierdomenico M et al.Receptor occupancy of nonpeptide corticotropin-releasingfactor 1 antagonist DMP696: correlation with drug exposureand anxiolytic efficacy. J Pharmacol Exp Ther 2003; 305:86–96.
77 Zobel AW, Nickel T, Kunzel HE, Ackl N, Sonntag A, Ising M et al.Effects of the high-affinity corticotropin-releasing hormonereceptor 1 antagonist R121919 in major depression: the first 20patients treated. J Psychiatr Res 2000; 34: 171–181.
78 Kunzel HE, Zobel AW, Nickel T, Ackl N, Uhr M, Sonntag A et al.Treatment of depression with the CRH-1-receptor antagonistR121919: endocrine changes and side effects. J Psychiatri Res2003; 37: 525–533.
79 McEwen BS. Interacting mediators of allostasis and allostaticload: towards an understanding of resilience in aging. Metabo-lism 2003; 52: 10–16.
80 Wolkowitz OM, Reus VI, Roberts E, Manfredi F, Chan T, Raum WJet al. Dehydroepiandrosterone (DHEA) treatment of depression.Biol Psychiatry 1997; 41: 311–318.
81 Murphy BE, Filipini D, Ghadirian AM. Possible use of gluco-corticoid receptor antagonists in the treatment of major depres-sion: preliminary results using RU 486. J Psychiatry Neurosci1993; 18: 209–213.
82 Belanoff JK, Rothschild AJ, Cassidy F, DeBattista C, Baulieu EE,Schold C et al. An open label trial of C-1073 (mifepristone)for psychotic major depression. Biol Psychiatry 2002; 52:386–392.
83 Manji HK, Quiroz JA, Sporn J, Payne JL, Denicoff K, Gray NA etal. Enhancing neuronal plasticity and cellular resilience todevelop novel, improved therapeutics for difficult-to-treat de-pression. Biol Psychiatry 2003; 53: 707–742.
84 Young AH, Watson S, Gallagher P, Smith MS, Del-Estal D, OwenBM et al. Mifepristone (RU-486) in the treatment of bipolardisorder and schizophrenia. Biol Psychiatry 2003; 53: 406.
Experimental treatments BPD IIJA Quiroz et al
772
Molecular Psychiatry

85 DeBattista C. C-1073 (Mifepristone) vs. placebo add-on totreatment as usual in patients with psychotic major depression.In: Difficult to Treat Mood and Anxiety Disorders. WashingtonDC, October 2003.
86 Bachmann CG, Linthorst AC, Holsboer F, Reul JM. Effect ofchronic administration of selective glucocorticoid receptorantagonists on the rat hypothalamic-pituitary-adrenocorticalaxis. Neuropsychopharmacology 2003; 28: 1056–1067.
87 Hoyberg OJ, Wik G, Mehtonen OP, Peeters BWMM, Sennef C.ORG 34517, a selective glucocorticoid receptor antagonist withpotent antidepressant activity: first clinical results. Int J Neu-ropsychopharmacol 2002; 5: 148.
88 Miner JN, Tyree C, Hu J, Berger E, Marschke K, Nakane M et al. Anonsteroidal glucocorticoid receptor antagonist. Mol Endocrinol2003; 17: 117–127.
89 Honer C, Nam K, Fink C, Marshall P, Ksander G, Chatelain RE etal. Glucocorticoid receptor antagonism by cyproterone acetateand RU486. Mol Pharmacol 2003; 63: 1012–1020.
90 Bannerman DM, Good MA, Butcher SP, Ramsay M, Morris RG.Distinct components of spatial learning revealed by prior trainingand NMDA receptor blockade. Nature 1995; 378: 182–186.
91 Collingridge GL. Long-term potentiation. A question of reliability.Nature 1994; 371: 652–653.
92 Collingridge GL, Bliss TV. Memories of NMDA receptors and LTP.Trends Neurosci 1995; 18: 54–56.
93 Watkins J, Collingridge G. Phenylglycine derivatives as antago-nists of metabotropic glutamate receptors. Trends Pharmacol Sci1994; 15: 333–342.
94 Faden AI, Demediuk P, Panter SS, Vink R. The role of excitatoryamino acids and NMDA receptors in traumatic brain injury.Science 1989; 244: 798–800.
95 Sapolsky RM. The possibility of neurotoxicity in the hippocam-pus in major depression: a primer on neuron death. BiolPsychiatry 2000; 48: 755–765.
96 Patel M, Li QY. Age dependence of seizure-induced oxidativestress. Neuroscience 2003; 118: 431–437.
97 Takahashi T, Kimoto T, Tanabe N, Hattori TA, Yasumatsu N,Kawato S. Corticosterone acutely prolonged N-methyl-D-aspartatereceptor-mediated Ca2þ elevation in cultured rat hippocampalneurons. J Neurochem 2002; 83: 1441–1451.
98 Nair SM, Werkman TR, Craig J, Finnell R, Joels M, Eberwine JH.Corticosteroid regulation of ion channel conductances andmRNA levels in individual hippocampal CA1 neurons.J Neurosci 1998; 18: 2685–2696.
99 Weiland NG, Orchinik M, Tanapat P. Chronic corticosteronetreatment induces parallel changes in N-methyl-D-aspartatereceptor subunit messenger RNA levels and antagonist bindingsites in the hippocampus. Neuroscience 1997; 78: 653–662.
100 Scaccianoce S, Matrisciano F, Del Bianco P, Caricasole A, DiGiorgi Gerevini V, Cappuccio I et al. Endogenous activation ofgroup-II metabotropic glutamate receptors inhibits the hypotha-lamic-pituitary-adrenocortical axis. Neuropharmacology 2003;44: 555–561.
101 Hergovich N, Singer E, Agneter E, Eichler HG, Graselli U,Simhandl C et al. Comparison of the effects of ketamine andmemantine on prolactin and cortisol release in men. a rando-mized, double-blind, placebo-controlled trial. Neuropsychophar-macology 2001; 24: 590–593.
102 Zarate CA, Quiroz J, Payne J, Manji HK. Modulators of theglutamatergic system: implications for the development ofimproved therapeutics in mood disorders. PsychopharmacolBull 2002; 36: 35–83.
103 Calabrese JR, Bowden CL, Sachs GS, Ascher JA, Monaghan E,Rudd GD. A double-blind placebo-controlled study oflamotrigine monotherapy in outpatients with bipolar I depres-sion. Lamictal 602 Study Group. J Clin Psychiatry 1999; 60:79–88.
104 Frye MA, Ketter TA, Kimbrell TA, Dunn RT, Speer AM, OsuchEA et al. A placebo-controlled study of lamotrigine andgabapentin monotherapy in refractory mood disorders. J ClinPsychopharmacol 2000; 20: 607–614.
105 Bowden CL, Calabrese JR, Sachs G, Yatham LN, Asghar SA,Hompland M et al. A placebo-controlled 18-month trial oflamotrigine and lithium maintenance treatment in recently
manic or hypomanic patients with bipolar I disorder. Arch GenPsychiatry 2003; 60: 392–400.
106 Leach MJ, Marden CM, Miller AA. Pharmacological studies onlamotrigine, a novel potential antiepileptic drug: II. Neuro-chemical studies on the mechanism of action. Epilepsia 1986;27: 490–497.
107 Calabresi P, Siniscalchi A, Pisani A, Stefani A, Mercuri NB,Bernardi G. A field potential analysis on the effects oflamotrigine, GP 47779, and felbamate in neocortical slices.Neurology 1996; 47: 557–562.
108 Wang SJ, Huang CC, Hsu KS, Tsai JJ, Gean PW. Presynapticinhibition of excitatory neurotransmission by lamotrigine in therat amygdalar neurons. Synapse 1996; 24: 248–255.
109 Anand A, Charney DS, Oren DA, Berman RM, Hu XS, CappielloA et al. Attenuation of the neuropsychiatric effects of ketaminewith lamotrigine: support for hyperglutamatergic effects ofN-methyl-D-aspartate receptor antagonists. Arch Gen Psychiatry2000; 57: 270–276.
110 Benavides J, Camelin JC, Mitrani N, Flamand F, Uzan A, LegrandJJ et al. 2-Amino-6-trifluoromethoxy benzothiazole, a possibleantagonist of excitatory amino acid neurotransmission–II.Biochemical properties. Neuropharmacology 1985; 24:1085–1092.
111 Kretschmer BD, Kratzer U, Schmidt WJ. Riluzole, a glutamaterelease inhibitor, and motor behavior. Naunyn SchmiedebergsArch Pharmacol 1998; 358: 181–190.
112 Doble A. The pharmacology and mechanism of action of riluzole.Neurology 1996; 47: S233–241.
113 Debono MW, Le Guern J, Canton T, Doble A, Pradier L. Inhibitionby riluzole of electrophysiological responses mediated by ratkainate and NMDA receptors expressed in Xenopus oocytes. EurJ Pharmacol 1993; 235: 283–289.
114 Urbani A, Belluzzi O. Riluzole inhibits the persistent sodiumcurrent in mammalian CNS neurons. Eur J Neurosci 2000; 12:3567–3574.
115 Benoit E, Escande D. Riluzole specifically blocks inactivated Nachannels in myelinated nerve fibre. Pflugers Arch 1991; 419:603–609.
116 Cheramy A, Barbeito L, Godeheu G, Glowinski J. Riluzoleinhibits the release of glutamate in the caudate nucleus of thecat in vivo. Neurosci Lett 1992; 147: 209–212.
117 Martin D, Thompson MA, Nadler JV. The neuroprotective agentriluzole inhibits release of glutamate and aspartate from slices ofhippocampal area CA1. Eur J Pharmacol 1993; 250: 473–476.
118 Siniscalchi A, Bonci A, Mercuri NB, Bernardi G. Effects ofriluzole on rat cortical neurones: an in vitro electrophysiologicalstudy. Br J Pharmacol 1997; 120: 225–230.
119 De Sarro G, Siniscalchi A, Ferreri G, Gallelli L, De Sarro A.NMDA and AMPA/kainate receptors are involved in the antic-onvulsant activity of riluzole in DBA/2 mice. Eur J Pharmacol2000; 408: 25–34.
120 Hubert JP, Burgevin MC, Terro F, Hugon J, Doble A. Effects ofdepolarizing stimuli on calcium homeostasis in cultured ratmotoneurones. Br J Pharmacol 1998; 125: 1421–1428.
121 Keita H, Lepouse C, Henzel D, Desmonts JM, Mantz J. Riluzoleblocks dopamine release evoked by N-methyl-D-aspartate, kai-nate, and veratridine in the rat striatum. Anesthesiology 1997; 87:1164–1171.
122 Mizuta I, Ohta M, Ohta K, Nishimura M, Mizuta E, Kuno S.Riluzole stimulates nerve growth factor, brain-derived neuro-trophic factor and glial cell line-derived neurotrophic factorsynthesis in cultured mouse astrocytes. Neurosci Lett 2001; 310:117–120.
123 Shirayama Y, Chen AC, Nakagawa S, Russell DS, Duman RS.Brain-derived neurotrophic factor produces antidepressant ef-fects in behavioral models of depression. J Neurosci 2002; 22:3251–3261.
124 Coric V, Milanovic S, Wasylink S, Patel P, Malison R, Krystal JH.Beneficial effects of the antiglutamatergic agent riluzolein a patient diagnosed with obsessive-compulsive disorderand major depressive disorder. Psychopharmacology 2003; 167:219–22 0.
125 Singh J, Zarate CA, Krystal AD. Successful riluzole augmentationtherapy in treatment-resistant bipolar depression following the
Experimental treatments BPD IIJA Quiroz et al
773
Molecular Psychiatry

development of rush with lamotrigine. Psychopharmacology2004 (in press).
126 Zarate CAJ, Payne JL, Quiroz J, Sporn J, Denicoff KK, Luck-enbaugh D et al. An open-label trial of riluzole in treatment-resistant major depression. Am J Psychiatry 2004; 161: 171–174.
127 Li X, Tizzano JP, Griffey K, Clay M, Lindstrom T, Skolnick P.Antidepressant-like actions of an AMPA receptor potentiator(LY392098). Neuropharmacology 2001; 40: 1028–1033.
128 Reynolds IJ, Miller RJ. Tricyclic antidepressants block N-methyl-D-aspartate receptors: similarities to the action of zinc. Br JPharmacol 1988; 95: 95–102.
129 Trullas R, Skolnick P. Functional antagonists at the NMDAreceptor complex exhibit antidepressant actions. Eur J Pharmacol1990; 185: 1–10.
130 Paul IA, Trullas R, Skolnick P, Nowak G. Down-regulation ofcortical beta-adrenoceptors by chronic treatment with functionalNMDA antagonists. Psychopharmacology (Berl) 1992; 106:285–287.
131 Skolnick P, Layer RT, Popik P, Nowak G, Paul IA, Trullas R.Adaptation of N-methyl-D-aspartate (NMDA) receptors followingantidepressant treatment: implications for the pharmacotherapyof depression. Pharmacopsychiatry 1996; 29: 23–26.
132 Papp M, Moryl E, Maccecchini ML. Differential effects of agentsacting at various sites of the NMDA receptor complex in a placepreference conditioning model. Eur J Pharmacol 1996; 317:191–196.
133 Cameron HA, McEwen BS, Gould E. Regulation of adultneurogenesis by excitatory input and NMDA receptor activationin the dentate gyrus. J Neurosci 1995; 15: 4687–4692.
134 Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR,Charney DS et al. Antidepressant effects of ketamine indepressed patients. Biol Psychiatry 2000; 47: 351–354.
135 Heresco-Levy U, Javitt DC. The role of N-methyl-D-aspartate(NMDA) receptor-mediated neurotransmission in the pathophy-siology and therapeutics of psychiatric syndromes. Eur Neurop-sychopharmacol 1998; 8: 141–152.
136 Crane G. The psychotropic effect of cycloserine: a new use of anantibiotic. Compr Psychiatry 1961; 2: 51–59.
137 Crane G. Cycloserine as an antidepressant agent. Am J Psychiatry1959; 115: 1025–1026.
138 Vamvakides A. D-cycloserine is active in the adult mouse andinactive in the aged mouse, in the forced swim test. Ann PharmFr 1998; 56: 209–212.
139 Kornhuber J, Bormann J, Hubers M, Rusche K, Riederer P. Effectsof the 1-amino-adamantanes at the MK-801-binding site of theNMDA-receptor-gated ion channel: a human postmortem brainstudy. Eur J Pharmacol 1991; 206: 297–300.
140 Kornhuber J, Weller M, Schoppmeyer K, Riederer P. Amantadineand memantine are NMDA receptor antagonists with neuropro-tective properties. J Neural Transm Suppl 1994; 43: 91–104.
141 Parsons CG, Quack G, Bresink I, Baran L, Przegalinski E,Kostowski W et al. Comparison of the potency, kinetics andvoltage-dependency of a series of uncompetitive NMDA receptorantagonists in vitro with anticonvulsive and motor impairmentactivity in vivo. Neuropharmacology 1995; 34: 1239–1258.
142 Parkes JD, Calver DM, Zilkha KJ, Knill-Jones RP. Controlled trialof amantadine hydrochloride in Parkinson’s disease. Lancet1970; 1: 259–262.
143 Vale S, Espejel MA, Dominguez JC. Amantadine in depression.Lancet 1971; 2: 437.
144 Rizzo M, Morselli PL. Amantadine-induced aggressiveness. BMJ1972; 3: 50.
145 Areosa SA, Sherriff F. Memantine for dementia. CochraneDatabase Syst Rev 2003 CD003154.
146 Orgogozo JM, Rigaud AS, Stoffler A, Mobius HJ, Forette F.Efficacy and safety of memantine in patients with mild tomoderate vascular dementia: a randomized, placebo-controlledtrial (MMM 300). Stroke 2002; 33: 1834–1839.
147 Reisberg B, Doody R, Stoffer A, Schmitt F, Ferris S, Mobius HJ.Memantine in moderate-to-severe Alzheimer’s disease. N Engl JMed 2003; 348: 1333–1341.
148 Bormann J. Memantine is a potent blocker of N-methyl-D-aspartate (NMDA) receptor channels. Eur J Pharmacol 1989;166: 591–592.
149 Berger W, Deckert J, Hartmann J, Krotzer C, Kornhuber J,Ransmayr G et al. Memantine inhibits [3H]MK-801 binding tohuman hippocampal NMDA receptors. Neuroreport 1994; 5:1237–1240.
150 Chen HS, Wang YF, Rayudu PV, Edgecomb P, Neill JC, Segal MMet al. Neuroprotective concentrations of the N-methyl-D-aspartateopen-channel blocker memantine are effective without cytoplas-mic vacuolation following post-ischemic administration and donot block maze learning or long-term potentiation. Neuroscience1998; 86: 1121–1132.
151 Chen HS, Lipton SA. Mechanism of memantine block of NMDA-activated channels in rat retinal ganglion cells: uncompetitiveantagonism. J Physiol 1997; 499(Part 1): 27–46.
152 Moryl E, Danysz W, Quack G. Potential antidepressive propertiesof amantadine memantine and bifemelane. Pharmacol Toxicol1993; 72: 394–397.
153 Rogoz Z, Skuza G, Maj J, Danysz W. Synergistic effect ofuncompetitive NMDA receptor antagonists and antidepressantdrugs in the forced swimming test in rats. Neuropharmacology2002; 42: 1024–1030.
154 Ametamey SM, Samnick S, Leenders KL, Vontobel P, Quack G,Parsons CG et al. Fluorine-18 radiolabelling, biodistributionstudies and preliminary PET evaluation of a new memantinederivative for imaging the NMDA receptor. J Recept SignalTransduct Res 1999; 19: 129–141.
155 Kornhuber J, Bormann J, Retz W, Hubers M, Riederer P.Memantine displaces [3H]MK-801 at therapeutic concentrationsin postmortem human frontal cortex. Eur J Pharmacol 1989; 166:589–590.
156 Brown WM, Aiken SP. Felbamate: clinical and molecular aspectsof a unique antiepileptic drug. Crit Rev Neurobiol 1998; 12:205–222.
157 Wallis RA, Panizzon KL. Felbamate neuroprotection againstCA1 traumatic neuronal injury. Eur J Pharmacol 1995; 294:475–482.
158 Wallis RA, Panizzon KL, Fairchild MD, Wasterlain CG. Protectiveeffects of felbamate against hypoxia in the rat hippocampal slice.Stroke 1992; 23: 547–551.
159 Ketter TA, Malow BA, Flamini R, Ko D, White SR, Post RM et al.Felbamate monotherapy has stimulant-like effects in patientswith epilepsy. Epilepsy Res 1996; 23: 129–137.
160 Ketter TA, Post RM, Theodore WH. Positive and negativepsychiatric effects of antiepileptic drugs in patients with seizuredisorders. Neurology 1999; 53: S53–67.
161 Gay PE, Mecham GF, Coskey JS, Sadler T, Thompson JA.Behavioral effects of felbamate in childhood epileptic encephalo-pathy (Lennox–Gastaut syndrome). Psychol Rep 1995; 77:1208–1210.
162 McCabe RT, Sofia RD, Layer RT, Leiner KA, Faull RL, Narang N etal. Felbamate increases [3H]glycine binding in rat brain andsections of human postmortem brain. J Pharmacol Exp Ther1998; 286: 991–999.
163 Wamsley JK, Sofia RD, Faull RL, Narang N, Ary T, Gan XD et al.Felbamate: interaction with glycine receptors in human cerebralcortex. Proc West Pharmacol Soc 1994; 37: 81–83.
164 Coffin V, Cohen-Williams M, Barnett A. Selective antagonism ofthe anticonvulsant effects of felbamate by glycine. Eur JPharmacol 1994; 256: R9–10.
165 Subramaniam S, Rho JM, Penix L, Donevan SD, Fielding RP,Rogawski MA. Felbamate block of the N-methyl-D-aspartatereceptor. J Pharmacol Exp Ther 1995; 273: 878–886.
166 Kaufman DW, Kelly JP, Anderson T, Harmon DC, Shapiro S.Evaluation of case reports of aplastic anemia amongpatients treated with felbamate. Epilepsia 1997; 38:1265–1269.
167 Harrison NL, Gibbons SJ. Zn2þ : an endogenous modulator ofligand- and voltage-gated ion channels. Neuropharmacology1994; 33: 935–952.
168 Nowak G, Schlegel-Zawadzka M. Alterations in serum and braintrace element levels after antidepressant treatment: part I. Zinc.Biol Trace Elem Res 1999; 67: 85–92.
169 Kroczka B, Branski P, Palucha A, Pilc A, Nowak G. Antidepres-sant-like properties of zinc in rodent forced swim test. Brain ResBull 2001; 55: 297–300.
Experimental treatments BPD IIJA Quiroz et al
774
Molecular Psychiatry

170 Szewczyk B, Branski P, Wieronska JM, Palucha A, Pilc A, NowakG. Interaction of zinc with antidepressants in the forcedswimming test in mice. Pol J Pharmacol 2002; 54: 681–685.
171 Nowak G, Szewczyk B, Wieronska JM, Branski P, Palucha A, PilcA et al. Antidepressant-like effects of acute and chronictreatment with zinc in forced swim test and olfactory bulbectomymodel in rats. Brain Res Bull 2003; 61: 159–164.
172 McLoughlin IJ, Hodge JS. Zinc in depressive disorder. ActaPsychiatr Scand 1990; 82: 451–453.
173 Maes M, Vandoolaeghe E, Neels H, Demedts P, Wauters A,Meltzer HY et al. Lower serum zinc in major depression is asensitive marker of treatment resistance and of the immune/inflammatory response in that illness. Biol Psychiatry 1997; 42:349–358.
174 Nowak G, Siwek M, Dudek D, Zieba A, Pilc A. Effect of zincsupplementation on antidepressant therapy in unipolar depres-sion: a preliminary placebo-controlled study. Pol J Pharmacol2003; 55: 1143–1147.
175 Ilouz R, Kaidanovich O, Gurwitz D, Eldar-Finkelman H. Inhibi-tion of glycogen synthase kinase-3beta by bivalent zinc ions:insight into the insulin-mimetic action of zinc. Biochem BiophysRes Commun 2002; 295: 102–106.
176 Borges K, Dingledine R. AMPA receptors: molecular andfunctional diversity. Prog Brain Res 1998; 116: 153–170.
177 Bleakman D, Lodge D. Neuropharmacology of AMPA and kainatereceptors. Neuropharmacology 1998; 37: 1187–1204.
178 Goff DC, Leahy L, Berman I, Posever T, Herz L, Leon AC et al. Aplacebo-controlled pilot study of the ampakine CX516 added toclozapine in schizophrenia. J Clin Psychopharmacol 2001; 21:484–487.
179 Knapp RJ, Goldenberg R, Shuck C, Cecil A, Watkins J, Miller Cet al. Antidepressant activity of memory-enhancing drugs in thereduction of submissive behavior model. Eur J Pharmacol 2002;440: 27–35.
180 Skolnick P, Legutko B, Li X, Bymaster FP. Current perspectives onthe development of non-biogenic amine-based antidepressants.Pharmacol Res 2001; 43: 411–423.
181 Lauterborn JC, Lynch G, Vanderklish P, Arai A, Gall CM. Positivemodulation of AMPA receptors increases neurotrophin expres-sion by hippocampal and cortical neurons. J Neurosci 2000; 20:8–21.
182 Bai F, Bergeron M, Nelson DL. Chronic AMPA receptorpotentiator (LY451646) treatment increases cell proliferationin adult rat hippocampus. Neuropharmacology 2003; 44:1013–1021.
183 Anwyl R. Metabotropic glutamate receptors: electrophysiologicalproperties and role in plasticity. Brain Res Brain Res Rev 1999;29: 83–120.
184 Baskys A, Bernstein NK, Barolet AW, Carlen PL. NMDA andquisqualate reduce a Ca-dependent Kþ current by a proteinkinase-mediated mechanism. Neurosci Lett 1990; 112: 76–81.
185 Ikeda SR, Lovinger DM, McCool BA, Lewis DL. Heterologousexpression of metabotropic glutamate receptors in adult ratsympathetic neurons: subtype-specific coupling to ion channels.Neuron 1995; 14: 1029–1038.
186 Salinska E, Stafiej A. Metabotropic glutamate receptors (mGluRs)are involved in early phase of memory formation: possible role ofmodulation of glutamate release. Neurochem Int 2003; 43:469–474.
187 Tan Y, Hori N, Carpenter DO. The mechanism of presynapticlong-term depression mediated by group I metabotropic gluta-mate receptors. Cell Mol Neurobiol 2003; 23: 187–203.
188 Riedel G, Platt B, Micheau J. Glutamate receptor function inlearning and memory. Behav Brain Res 2003; 140: 1–47.
189 Nicoletti F, Bruno V, Copani A, Casabona G, Knopfel T.Metabotropic glutamate receptors: a new target for the therapyof neurodegenerative disorders? Trends Neurosci 1996; 19:267–271.
190 Schoepp DD. Unveiling the functions of presynaptic metabo-tropic glutamate receptors in the central nervous system.J Pharmacol Exp Ther 2001; 299: 12–20.
191 Maiese K, Vincent A, Lin SH, Shaw T. Group I and group IIImetabotropic glutamate receptor subtypes provide enhancedneuroprotection. J Neurosci Res 2000; 62: 257–272.
192 Spooren WP, Vassout A, Neijt HC, Kuhn R, Gasparini F, Roux S etal. Anxiolytic-like effects of the prototypical metabotropicglutamate receptor 5 antagonist 2-methyl-6-(phenylethynyl)-pyridine in rodents. J Pharmacol Exp Ther 2000; 295:1267–1275.
193 Tatarczynska E, Klodzinska A, Chojnacka-Wojcik E, Palucha A,Gasparini F, Kuhn R et al. Potential anxiolytic- and antidepres-sant-like effects of MPEP, a potent, selective and systemicallyactive mGlu5 receptor antagonist. Br J Pharmacol 2001; 132:1423–1430.
194 Tatarczynska E, Klodzinska A, Kroczka B, Chojnacka-Wojcik E,Pilc A. The antianxiety-like effects of antagonists of group I andagonists of group II and III metabotropic glutamate receptors afterintrahippocampal administration. Psychopharmacology (Berl)2001; 158: 94–99.
195 Chojnacka-Wojcik E, Klodzinska A, Pilc A. Glutamate receptorligands as anxiolytics. Curr Opin Invest Drugs 2001; 2:1112–1119.
196 Duman RS. Synaptic plasticity and mood disorders. MolPsychiatry 2002; 7(Suppl 1): S29–S34.
197 Takahashi M, Terwilliger R, Lane C, Mezes PS, Conti M, DumanRS. Chronic antidepressant administration increases the expres-sion of cAMP-specific phosphodiesterase 4A and 4B isoforms.J Neurosci 1999; 19: 610–618.
198 Nibuya M, Nestler EJ, Duman RS. Chronic antidepressantadministration increases the expression of cAMP responseelement binding protein (CREB) in rat hippocampus. J Neurosci1996; 16: 2365–2372.
199 Asanuma M, Nishibayashi S, Iwata E, Kondo Y, Nakanishi T,Vargas MG et al. Alterations of cAMP response element-bindingactivity in the aged rat brain in response to administration ofrolipram, a cAMP-specific phosphodiesterase inhibitor. BrainRes Mol Brain Res 1996; 41: 210–215.
200 Fujimaki K, Morinobu S, Duman RS. Administration of a cAMPphosphodiesterase 4 inhibitor enhances antidepressant-induc-tion of BDNF mRNA in rat hippocampus. Neuropsychopharma-cology 2000; 22: 42–51.
201 O’Donnell JM. Antidepressant-like effects of rolipram and otherinhibitors of cyclic adenosine monophosphate phosphodiester-ase on behavior maintained by differential reinforcement of lowresponse rate. J Pharmacol Exp Ther 1993; 264: 1168–1178.
202 Griebel G, Misslin R, Vogel E, Bourguignon JJ. Behavioral effectsof rolipram and structurally related compounds in mice:behavioral sedation of cAMP phosphodiesterase inhibitors.Pharmacol Biochem Behav 1991; 39: 321–323.
203 Wachtel H, Schneider HH. Rolipram, a novel antidepressantdrug, reverses the hypothermia and hypokinesia of monoamine-depleted mice by an action beyond postsynaptic monoaminereceptors. Neuropharmacology 1986; 25: 1119–1126.
204 Zeller E, Stief HJ, Pflug B, Sastre-y-Hernandez M. Results of aphase II study of the antidepressant effect of rolipram. Pharma-copsychiatry 1984; 17: 188–190.
205 Bobon D, Breulet M, Gerard-Vandenhove MA, Guiot-Goffioul F,Plomteux G, Sastre-y-Hernandez M et al. Is phosphodiesteraseinhibition a new mechanism of antidepressant action? A doubleblind double-dummy study between rolipram and desipraminein hospitalized major and/or endogenous depressives. Eur ArchPsychiatry Neurol Sci 1988; 238: 2–6.
206 Fleischhacker WW, Hinterhuber H, Bauer H, Pflug B, Berner P,Simhandl C et al. A multicenter double-blind study of threedifferent doses of the new cAMP-phosphodiesterase inhibitorrolipram in patients with major depressive disorder. Neuropsy-chobiology 1992; 26: 59–64.
207 Hebenstreit GF, Fellerer K, Fichte K, Fischer G, Geyer N, Meya Uet al. Rolipram in major depressive disorder: results of a double-blind comparative study with imipramine. Pharmacopsychiatry1989; 22: 156–160.
208 Bertolino A, Crippa D, di Dio S, Fichte K, Musmeci G, Porro Vet al. Rolipram versus imipramine in inpatients with major,‘minor’ or atypical depressive disorder: a double-blind double-dummy study aimed at testing a novel therapeutic approach. IntClin Psychopharmacol 1988; 3: 245–253.
209 Horowski R, Sastre-Y-Hernandez M. Clinical effects of theneurotropic selective cAMP phosphodiesterase inhibitor
Experimental treatments BPD IIJA Quiroz et al
775
Molecular Psychiatry

rolipram in depressed patients: global evaluation of the pre-liminary reports. Curr Ther Res 1985; 38: 23–29.
210 Scott AI, Perini AF, Shering PA, Whalley LJ. In-patient majordepression: is rolipram as effective as amitriptyline? Eur J ClinPharmacol 1991; 40: 127–129.
211 Huang Z, Ducharme Y, Macdonald D, Robichaud A. The nextgeneration of PDE4 inhibitors. Curr Opin Chem Biol 2001; 5:432–438.
212 Dyke HJ, Montana JG. Update on the therapeutic potential ofPDE4 inhibitors. Expert Opin Invest Drugs 2002; 11: 1–13.
213 Ochs G, Penn RD, York M, Giess R, Beck M, Tonn J et al. A phaseI/II trial of recombinant methionyl human brain derivedneurotrophic factor administered by intrathecal infusion topatients with amyotrophic lateral sclerosis. Amyotroph LateralScler Other Motor Neuron Disord 2000; 1: 201–206.
214 Chen DF, Tonegawa S. Why do mature CNS neurons of mammalsfail to re-establish connections following injury—functions ofbcl-2. Cell Death Differ 1998; 5: 816–822.
215 Chen DF, Schneider GE, Martinou JC, Tonegawa S. Bcl-2promotes regeneration of severed axons in mammalian CNS.Nature 1997; 385: 434–439.
216 Holm KH, Cicchetti F, Bjorklund L, Boonman Z, Tandon P,Costantini LC et al. Enhanced axonal growth from fetal humanbcl-2 transgenic mouse dopamine neurons transplanted to theadult rat striatum. Neuroscience 2001; 104: 397–405.
217 Oh YJ, Swarzenski BC, O’Malley KL. Overexpression of Bcl-2 in amurine dopaminergic neuronal cell line leads to neurite out-growth. Neurosci Lett 1996; 202: 161–164.
218 Chierzi S, Strettoi E, Cenni MC, Maffei L. Optic nerve crush:axonal responses in wild-type and bcl-2 transgenic mice.J Neurosci 1999; 19: 8367–8376.
219 DeVries AC, Joh HD, Bernard O, Hattori K, Hurn PD, TraystmanRJ et al. Social stress exacerbates stroke outcome by suppressingBcl-2 expression. Proc Natl Acad Sci USA 2001; 98:11824–11828.
220 Takata K, Kitamura Y, Kakimura J, Kohno Y, Taniguchi T. Increaseof bcl-2 protein in neuronal dendritic processes of cerebral cortexand hippocampus by the antiparkinsonian drugs, talipexole andpramipexole. Brain Res 2000; 236–241.
221 Zarate Jr CA, Payne JL, Singh J, Quiroz J, Luckenbaugh, DenicoffKD et al. Pramipexole for bipolar II depression: a placebo-controlled proof of concept study. Biol Psych 2004 (in press).
222 Goldberg JF, Burdick KE, Endick CJ. A preliminary randomized,double-blind, placebo-controlled trial of primapexole added tomood stabilizers for treatment-resistant bipolar depression. Am JPsychiatry 2004; 161: 564–566.
223 Manji HK, Gottesman II, Gould TD. Signal transduction andgenes-to-behaviors pathways in psychiatric diseases. Sci STKE2003; 207, pe49.
224 Einat H, Belmaker RH, Manji HK. New aproaches to modelingbipolar disorder. Psychopharm Bul 2003; 37: 47–63.
225 Nestler EJ, Gould E, Manji HK, Buncan M, Duman RS,Greshenfeld HK et al. Preclinical models: status of basic researchin depression. Biol Psychiatry 2002; 52: 503–528.
226 Potter WZ, Ozcan ME. Methodological considerations for thedevelopment of new treatments for bipolar disorder. Aust NZJPsychiatry 1999; 33(Suppl): S84–98.
227 Manji HK, Zarate CA. Molecular and cellular mechanismsunderlying mood stabilization in bipolar disorder: implicationsfor the development of improved therapeutics. Mol Psychiatry2002; 7(Suppl 1): S1–S7.
228 Charney DS, Manji HK. Life stress, genes, and depression:multiple pathways lead to increased risk and new opportunitiesfor intervention. Sci STKE. 2004; RE5.
229 Danysz W, Parsons CG, Kornhuber J, Schmidt WJ, Quack G.Aminoadamantanes as NMDA receptor antagonists and antipar-kinsonian agents–preclinical studies. Neurosci Biobehav Rev1997; 21: 455–468.
230 Parsons CG, Panchenko VA, Pinchenko VO, Tsyndrenko AY,Krishtal OA. Comparative patch-clamp studies with freshlydissociated rat hippocampal and striatal neurons on the NMDAreceptor antagonistic effects of amantadine and memantine. Eur JNeurosci 1996; 8: 446–454.
231 Einat H, Yuan P, Gould TD, Li J, Du J, Zhang L et al. The role ofthe extracellular signal-regulated kinase signaling pathway inmood modulation. J Neurosci 2003; 23: 7311–7316.
232 Murphy BE. Treatment of major depression with steroidsuppressive drugs. J Steroid Biochem Mol Biol 1991; 39: 239–244.
233 Ghadirian AM, Engelsmann F, Dhar V, Filipini D, Keller R,Chouinard G et al. The psychotropic effects of inhibitors ofsteroid biosynthesis in depressed patients refractory to treatment.Biol Psychiatry 1995; 37: 369–375.
234 Wolkowitz OM, Reus VI, Manfredi F, Ingbar J, Brizendine L,Weingartner H. Ketoconazole administration in hypercortisole-mic depression. Am J Psychiatry 1993; 150: 810–812.
235 O’Dwyer AM, Lightman SL, Marks MN, Checkley SA. Treatmentof major depression with metyrapone and hydrocortisone.J Affect Disord 1995; 33: 123–128.
236 Thakore JH, Dinan TG. Cortisol synthesis inhibition: a newtreatment strategy for the clinical and endocrine manifestationsof depression. Biol Psychiatry 1995; 37: 364–368.
237 Iizuka H, Kishimoto A, Nakamura J, Mizukawa R. Clinical effectsof cortisol synthesis inhibition on treatment-resistant depression.Nihon Shinkei Seishin Yakurigaku Zasshi 1996; 16: 33–36.
238 Raven PW, O’Dwyer AM, Taylor NF, Checkley SA. The relation-ship between the effects of metyrapone treatment on depressedmood and urinary steroid profiles. Psychoneuroendocrinology1996; 21: 277–286.
239 Sovner R, Fogelman S. Ketoconazole therapy for atypicaldepression. J Clin Psychiatry 1996; 57: 227–228.
240 Brown ES, Bobadilla L, Rush AJ. Ketoconazole in bipolar patientswith depressive symptoms: a case series and literature review.Bipolar Disord 2001; 3: 23–29.
241 Konradi C, Eaton M, MacDonald ML, Walsh J, Benes FM, HeckersS. Molecular evidence for mitochondrial dysfunction in bipolardisorder. Arch Gen Psychitary 2004; 61: 300–308.
242 Kato T, Kato N. Mitochondrial dysfunction in bipolar disoder.Bipolar Disord 2000; 2: 180–190.
243 Modica-Napolitano JS, Renshaw PF. Ethanolamine phosphoetha-nolamine inhibit mitochondrial function in vitro: implicationsfor mitochondrial dysfunction hypothesis in depression andbipolar disorder. Biol Psychiatry 2004; 55: 273–277.
244 Gray NA, Quiroz JA, Kato T, Manji HK. Critical roles for themitochondrial-ER network in the pathophysiology and treate-ment of bipolar disorder. 2004 Submitted.
245 Baker SK, Tarnopolsky MA. Targeting celluar energy productionin neurological disorders. Expert Opin Invest Drugs 2003; 12:1655–1679.
246 Pettegrew JW, Levine J, McClure RJ. Acetyl-L-carnitine physical–chemical, metabolic, and therapeutic properties: relevance for itsmode of action in Alzheimer’s disease geriatric depression. MolPsychiarty 2000; 5: 616–632.
Experimental treatments BPD IIJA Quiroz et al
776
Molecular Psychiatry