
Emergent Management of Pediatric Asthma: Myths & … · Cost of Asthma Pathophysiology ... “A...
26
1 Emergent Management of Pediatric Asthma: Myths & Pitfalls Dan Nguyen, MD Assistant Professor of Emergency Medicine & Pediatrics MCEP Critical Care Practice in the Emergency Department March 22 nd , 2018 Disclosures and Conflicts of Interest • I have no conflicts of interest in relation to this presentation
-
Upload
duongkhuong -
Category
Documents
-
view
223 -
download
0
Transcript of Emergent Management of Pediatric Asthma: Myths & … · Cost of Asthma Pathophysiology ... “A...
1
Emergent Management of
Pediatric Asthma: Myths & Pitfalls
Dan Nguyen, MDAssistant Professor of Emergency Medicine & Pediatrics
MCEP Critical Care Practice in the Emergency Department
March 22nd, 2018
Disclosures and Conflicts of Interest
• I have no conflicts of interest in relation to this presentation

2
Learning Objectives
• Summarize the prevalence and financial impact of asthma in the pediatric population
• Prioritize a systematic approach for acute management
• Identify advanced treatment modalities
• Evaluate common pitfalls in management
Epidemiology
• 8.4% prevalence in US children– Rate of emergency care use 2-2.5 times higher in age <18 yrs
• Minorities disproportionately affected*– Mortality 4-5 times higher in black compared to white children
– Puerto Ricans have highest prevalence
– Role of allergen exposure
– Reliance on episodic/emergent care
– Decreased medication compliance
*Mayrides M, et al. “Ethnic Disparities in the Burden and Treatment of Asthma”. AAFA/National Pharmaceutical Council. 2005.

3
Epidemiology
Wang LY, et al. “Direct and Indirect Cost of Asthma in School-age Children”. Preventing Chronic Disease. Jan 2005. Asthma Allergy Foundation of America, May 20015.The Express Scripts Lab. The 2014 Drug Trend Report. March 2015. http://lab.express-scripts.com/drug-trend/report/
• Annual health care cost for child with asthma: $1042
– Child without asthma $618
• Children with asthma miss 2.48 school days/year
$56 B$50.1 B
$5.9 B
Cost of Asthma
Pathophysiology
Reduce
Inflammation
Reverse
Obstruction
Correction of
Hypoxemia
4
Bronchodilators
• Inhaled SABA (Albuterol)
• Ipratropium bromide
• Parental beta-agonists
• Magnesium sulfate
• Ketamine
Continuous vs. Intermittent
• Cochrane Database Systematic Review, 2003
– RCTs of continuous vs. intermittent inhaled beta-agonists in ED
– 8 trials
– Continuous treatments associated with greater improvement in spirometry and reduced rates of hospital admissions
*Carmargo CA, et al. “Continuous versus intermittent beta-agonists in the treatemnt of acute asthma”. Cochrane Database Systematic review. 2003 Oct 20;(4):CD001115.
5
Inhaled SABA
• Goal = Administer 3 doses within the first hour
• Continuous vs. Intermittent– Similar outcomes and side effects
– Continuous less labor intensive
– Intermittent may be better tolerated by younger children
Recommendation
Continuous therapy for moderate to
severe asthma exacerbation
Nebulizer vs. MDI

6
Nebulizer vs. MDI
• Meter-dosed Inhaler✖ Requires patient coordination and education
✖ Requires respiratory hold
✖ Requires spacer & mask
✔ Portability
✔ Treatment Time
✔ No external power source
✔ Cost in the community
• Nebulizer✖ Required to hold treatment over patient’s face (≈60 minutes)
✖Machine sanitation
✖Machine are not portable
✔ Passive administration
✔ Supplemental humidified oxygen
✔ Co-administration of other inhaled meds (ipratropium)
*Cates CJ, et al. “Holding chambers (spacer) versus nebulizers for beta-agonist treatment of acute asthma”. Cochrane Database Systematic review. 2014 Sept 13;(9):CD000052.
Nebulizer vs. MDI
*Cates CJ, et al. “Holding chambers (spacer) versus nebulizers for beta-agonist treatment of acute asthma”. Cochrane Database Systematic review. 2014 Sept 13;(9):CD000052.
Hospitalization Admission Rates
• Cochrane Database Systematic Review, 2014
– 39 Trials, 1897 children
7
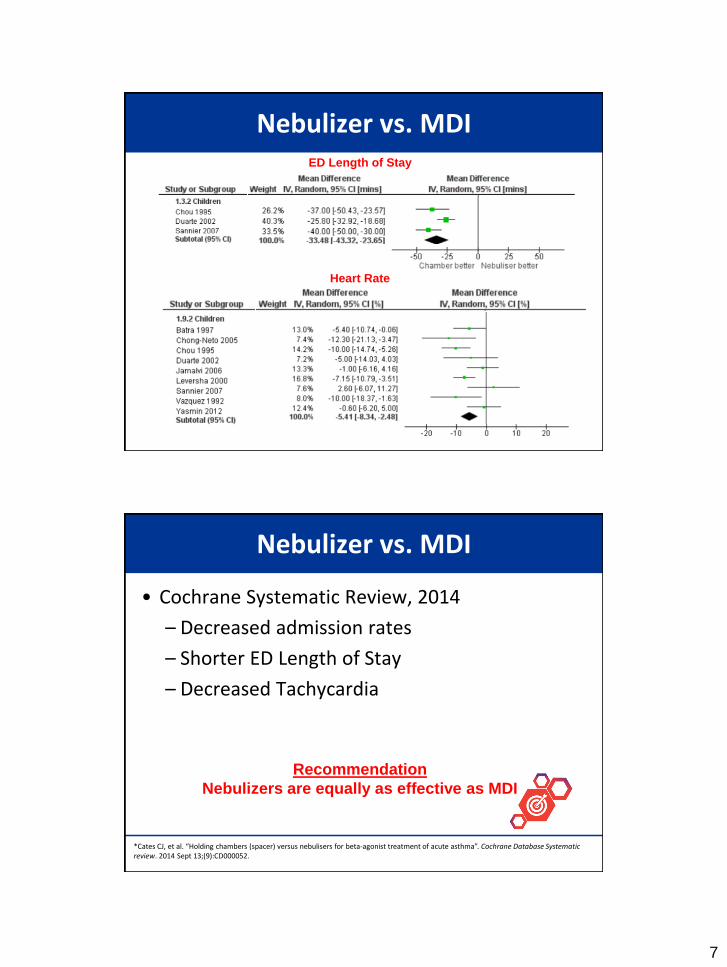
Nebulizer vs. MDIED Length of Stay
Heart Rate
Nebulizer vs. MDI
Recommendation
Nebulizers are equally as effective as MDI
*Cates CJ, et al. “Holding chambers (spacer) versus nebulisers for beta-agonist treatment of acute asthma”. Cochrane Database Systematic review. 2014 Sept 13;(9):CD000052.
• Cochrane Systematic Review, 2014
– Decreased admission rates
– Shorter ED Length of Stay
– Decreased Tachycardia
8
A Word About Spacers
• Improved outcomes in children with asthma
Recommendation
All Children Need a
Spacer & Mask
• Corrects for poor coordination/technique
• Decreases oropharyngeal deposition
Levalbuterol
• Xopenex - Pure R-albuterol
• S-albuterol thought to be a weaker bronchoconstrictor
• Is it more effective?
9
Levalbuterol
• Journal of Asthma, 2011
– 99 children, ED visits for mod/severe exacerbation
– 7.5 mg albuterol vs. 3.75 mg levalbuterol
• Further treatments given with same meds
• Standard care; Double-blinded
– After one hour, spirometry and asthma scores showed greater improvement in albuterol group
• No differences in side effects, HR, RR, SaO2
• No difference in admission rate
Wilkinson, et al. “Efficacy of Racemic Albuterol versus Levalbuterol used as a Continuous nebulization for the Treatment of Acute Asthma Exacerbations: A Randomized, Double-Blind, Clinical Trial”. Journal of Asthma. 2011 Mar; 48 (2):188-93.
Levalbuterol
• Pulmonary Pharm Therapeutics, 2013
– Large meta-analysis and systemic review
– 7 trials, 1625 patients
– Similar RR, SaO2, %ΔFEV1, Clinical Asthma Scores
– Levalbuterol should not be used over albuterol
Jat KR, et al. “Levalbuterol versus albuterol for acute asthma: a systematic review and meta-analysis”. Pulm Pharm Therapy. 2013 Apr; 26(2):239-48.
10
Decreased Tachycardia?
• Journal of Ped Pharm Therapy, 2011
– Levalbuterol vs. Racemic Albuterol x 3 doses
– 50 patients
– No clinically significant difference in HR changes
• Annals of Pharmacotherapy, 2013
– Children with CHD, cardiomyopathy, or SVT
– 192 patients
– Equivalent increases in HR
*Bio LL, et al. “Comparison of levalbuterol and racemic albuterol based on cardiac adverse effects in children”. Journal of Ped Pharm Therapy. 2011 Jul-Sep; 16(3): 191-198.**Kelly A, et al. “Comparison of heart rate changes associated with levalbuterol and racemic albuterol in pediatric cardiology patients. Annals of Pharmacotherapy. 2013 May; 47(5): 644-50
Levalbuterol
• Does it cost more?
– YES! 4-5 x more expensive for equivalent neb nose
Recommendation
Racemic albuterol with rare exception

11
Ipratropium Bromide
• Anticholinergic agent
• Impairs bronchial smooth muscle contraction
• Minimal systemic side effects
– Unable to cross from lung to systemic circulation
Ipratropium Bromide
• Additive effect with SABA*
– Improved spirometry measures
– Reduced risk of hospitalization
• No benefit to continuing as inpatient**
Recommendation
Combine ipratropium bromide (2-3 doses) with first
3 doses of albuterol given over 1st hr
*Rodrigo GJ, et al. Anticholinergic in the treatment of children and adults with acute asthma: a systematic review and meta-analysis”. Thorax. 2005 Sep; 60(9): 740-6. **Vezina K, et al. “Combined inhaled anticholinergics and short-acting beta2-agonists for initial treatment of acute asthma in children”. Cochrane Database Systematic Review. 2013 Aug 21;(8): CD000060.
12
Parental Beta-Agonists
• Subcutaneous or Intramuscular
• Poor inspiratory air flow or cooperation (i.e. AMS)
• Given within minutes of arrival
• Dosing– Terbutaline: 0.01 mg/kg/dose (Max dose 0.4 mg)
– Epinephrine: 0.01 mg/kg/dose (Max dose 0.4 mg)
– Consider auto injectable epinephrine
Parenteral Beta-Agonists
• Pediatric Emergency Care, 2007
– Prospective RCT of IV Terbutaline
– 49 children in ICU
– Trend toward improved scores and shorter ICU stay, but not statistically significant
• Cochrane Review, 2012
– 3 studies, 157 children
– Limited evidence to support use of IV beta agonists
Bogie AL, et al. “Comparison of intravenous terbutaline versus normal saline in pediatric patients on continuous high-dose nebulized albuterol for status asthmaticus”. Pediatric Emergency Care. 2007 un; 23(6): 355-61.Travers AH, et al. “Addition of intravenous beta(2)-agonists to inhaled beta(2) agonists for acute asthma”. Cochrane Database Systematic Rev. 2012. Dec 12; 12: CD10179.
13
Parental Beta-Agonists
• Increased side effects
– Dysrhythmias, myocardial ischemia, hypertension
• Reserved for critically ill, poorly responsive
• Consider repeated doses (x3) vs. infusion
• Discuss with ICU colleagues
Systemic Glucocorticoids
• Reduce airway edema and secretions
• Indicated in most children presenting to ED
– Any moderate or severe exacerbation
– Any mild exacerbation not responding to adequate home therapy
14
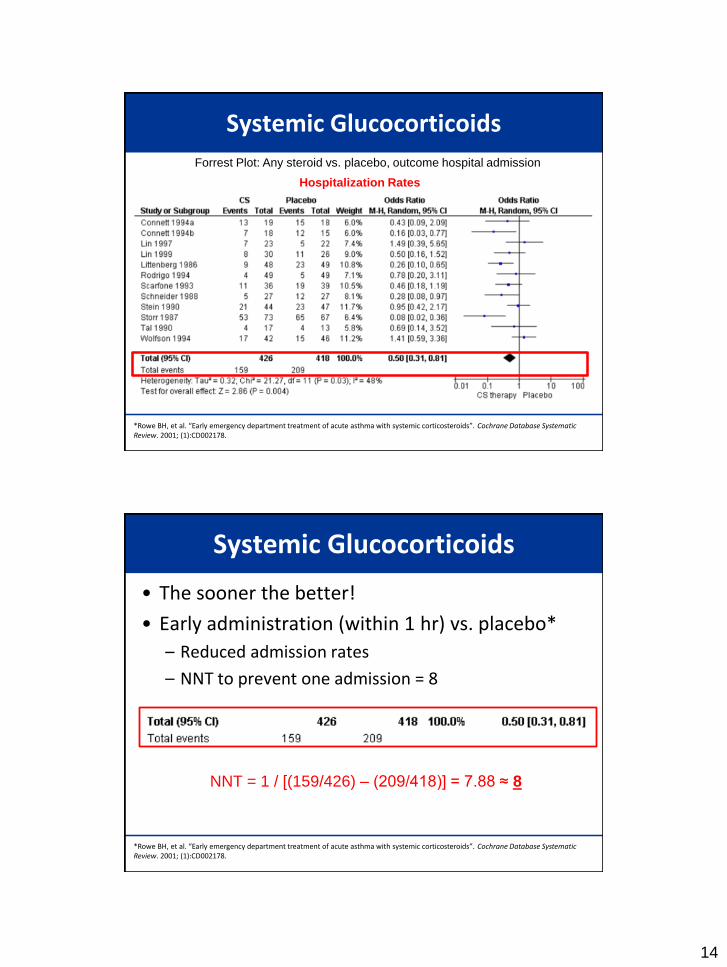
Systemic Glucocorticoids
*Rowe BH, et al. “Early emergency department treatment of acute asthma with systemic corticosteroids”. Cochrane Database Systematic Review. 2001; (1):CD002178.
Forrest Plot: Any steroid vs. placebo, outcome hospital admission
Hospitalization Rates
Systemic Glucocorticoids
• The sooner the better!
• Early administration (within 1 hr) vs. placebo*
– Reduced admission rates
– NNT to prevent one admission = 8
*Rowe BH, et al. “Early emergency department treatment of acute asthma with systemic corticosteroids”. Cochrane Database Systematic Review. 2001; (1):CD002178.
NNT = 1 / [(159/426) – (209/418)] = 7.88 ≈ 8
15
Systemic Glucocorticoids
• Prednisone vs. Dexamethasone vs. Methylprednisolone
(2mg/kg) (0.6 mg/kg) (2 mg/kg)
• Effects start in 1-3 hours, max effect at 4-8 hours
• Inhaled glucocorticoids?
– Thus far, no benefit in acute management
*Hendeles L, et al. “Are inhaled corticosteroids effective for acute exacerbation of asthma in children?”. Journal of Pediatrics. 2003; Feb; 142(2 Suppl): S26-32; discussion S32-3.Upham BD, et al. “Nebulized budesonide added to standard pediatric emergency department treatment of acute asthma: a randomized, double-blind trial. Acad Emerg Med 2011; 18:665-73.
Recommendation
Systemic steroids recommended to
non-responders to inhaled beta-agonists
Dexamethasone vs. Prednisone
• Pharmacokinetics
– 5-6 times more potent than prednisone
– 4-5 times longer half life
• Clinical
– Similar efficacy with less side effects (i.e. vomiting)*
– Single Dose or Two-Doses not inferior to predinsone**
– No increase in unscheduled medical evaluations
*Qureshi F, et al. “Comparative efficacy of oral dexamthasone versus oral prednisone in acute pediatric asthma”. Ped. Jul 2001; 139(1): 20-6.**Schwartz ES et al. “Is dexamethasone as effective as prednisone or prednisolone in the management of pediatric asthma exacerbations? ”. Annals of Emergency Medicine. Jan 2001; 65(1): 81-2.

16
Dexamethasone vs Prednisone
• Increased Compliance
– Families prefer shorter duration*
– More palatable and preferred by pediatric patients**
• Economic Cost Savings***
– Less return visits
– Less admissions
*Williams KW, et al. “Parental preference for short- versus long-course corticosteroid therapy in children with asthma presenting to the pediatric emergency department”. Clinical Pediatrics. Jan 2013; 52(1): 30-4.**Hames H et al. “A palatability study of a flavored dexamethasone preparation versus prednisolone liquid in children ”. Canadian J ClinPharmacol. Winter 2008; 15(1): e95-8.***Andrews A et al. “A cost-effectiveness analysis of dexamthasone vs prednisone in pediatrics acute asthma exacerbation”. Acad Emerg Med. Aug. 2012; 19(8): 943-8.
Kitchen Sink
• Beta Agonists (naturally)
• Inhaled anticholingerics (useful in first hour)
• IV steroids (struggling to breath ≠ PO)
• Magnesium sulfate
• Heliox
• Ketamine
17
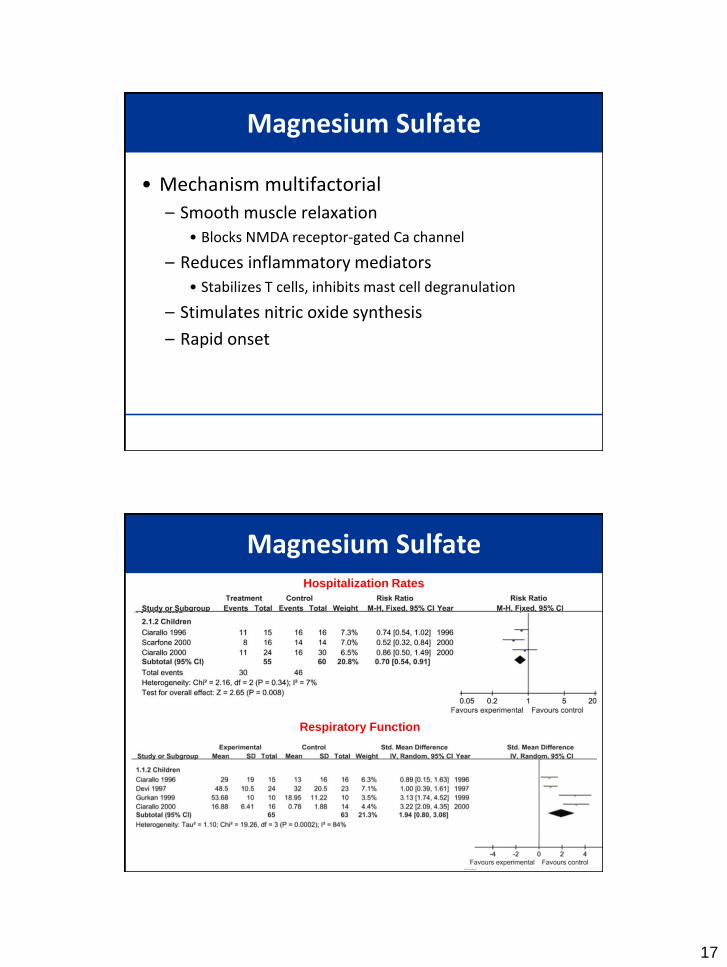
Magnesium Sulfate
• Mechanism multifactorial
– Smooth muscle relaxation
• Blocks NMDA receptor-gated Ca channel
– Reduces inflammatory mediators
• Stabilizes T cells, inhibits mast cell degranulation
– Stimulates nitric oxide synthesis
– Rapid onset
Magnesium SulfateHospitalization Rates
Respiratory Function
18
Magnesium Sulfate
• When added to SABA and steroids:– Improved pulmonary function
– Reduced inpatient hospitalization
– NO effect on SBP/DBP
• Dose: 25-75 mg/kg (max 2g) over 20 minutes
*Shan Z. et al. “Intravenous and nebulized magnesium sulfate for treating acute asthma in adults and children: a systematic review and meta-analysis” Respiratory Medicine. 2013 Mar; 107(3): 321-30.
Recommendation
Consider magnesium in severe exacerbations who
deteriorate despite initial therapy
Ketamine
• Bronchodilator effect
– Central catecholamine release
– Inhibition of vagal pathways anticholinergic effect on bronchial smooth muscle
• Medication of choice for sedation/analgesia required for endotracheal intubation in asthmatics
19
Ketamine
• Utility in non-intubated children?
• Annals of Emergency medicine, 2005
– Double-blind, randomized, placebo-controlled trial
– 68 patients with continued mod-sever symptoms after initial conventional therapy
– No benefit
Allen JY, et al. “The efficacy of ketamine in pediatric emergency department patients who present with acute severe asthma”. Annals of Emergency Medicine. 2005 Jul; 46(1): 43-50.
Heliox
• Increases efficient laminar flow
• 70:30 or 80:20 mixture
Re =
Re = Reynolds Number
ρ = density
v = velocity
R = radius
η = viscosity
ρvr/η
η
*Gupta VK, et al. “Heliox administration in the pediatric intensive care unit: an evidence-based review”. Pediatric Critical Care Med. 2005; 6(2): 204-11.
20
Heliox
• Benefits
– Better lung mechanics
– Improves albuterol delivery
– Few side effects/complications (inert gas)
• Drawback
– Expensive
– Contraindicated in hypoxia
– Few proven RCTs
– Does not treat causative issue
*Rodrigo GV, et al. “Heliox for the non-intubated acute asthma patients”. Cochrane Collaboration. 2010.
Common Pitfalls
• Intubation Risk
• Excessive IVF
• Elevated lactic acidosis
• Transient hypoxia with β-agonist
21
Endotracheal Intubation
• Goal = DON’T INTUBATE
– ¼ of children intubation develop complications
• Pneumothorax
• Impaired Preload
• Cardiovascular Collapse
– Mechanical ventilation associated with increased mortality
Endotracheal Intubation
• Indications
– Apnea/Coma
– Worsening mental status
– Exhaustion
– Refractory hypoxemia
– Significant refractory respiratory acidosis (worsening despite maximal therapy)
22
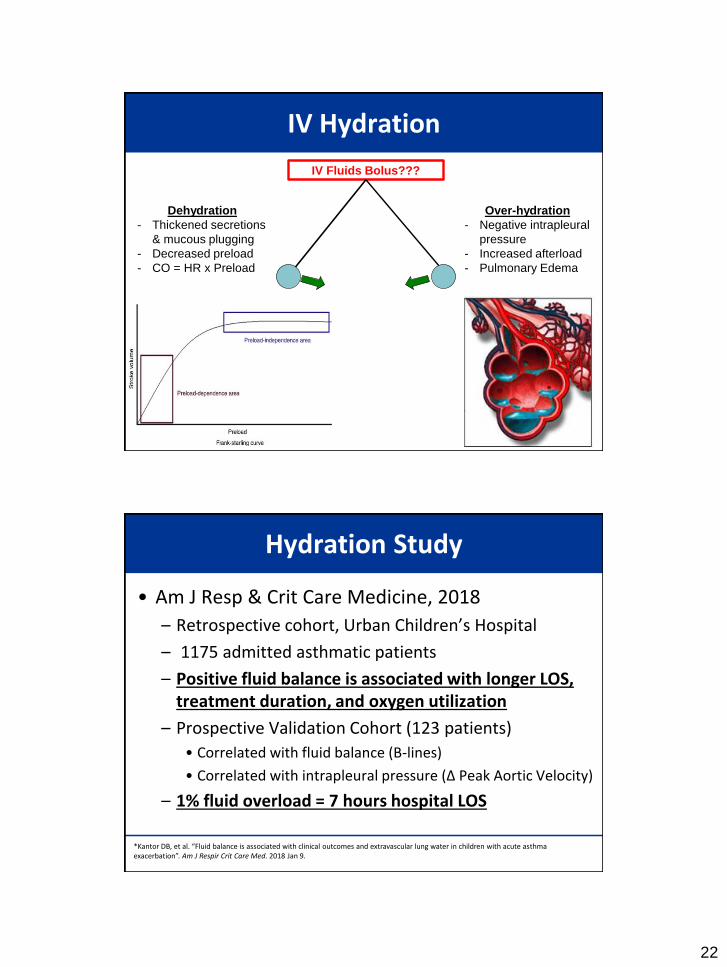
IV Hydration
IV Fluids Bolus???
Dehydration
- Thickened secretions
& mucous plugging
- Decreased preload
- CO = HR x Preload
Over-hydration
- Negative intrapleural
pressure
- Increased afterload
- Pulmonary Edema
Hydration Study
*Kantor DB, et al. “Fluid balance is associated with clinical outcomes and extravascular lung water in children with acute asthma exacerbation”. Am J Respir Crit Care Med. 2018 Jan 9.
• Am J Resp & Crit Care Medicine, 2018
– Retrospective cohort, Urban Children’s Hospital
– 1175 admitted asthmatic patients
– Positive fluid balance is associated with longer LOS, treatment duration, and oxygen utilization
– Prospective Validation Cohort (123 patients)
• Correlated with fluid balance (B-lines)
• Correlated with intrapleural pressure (Δ Peak Aortic Velocity)
– 1% fluid overload = 7 hours hospital LOS
23
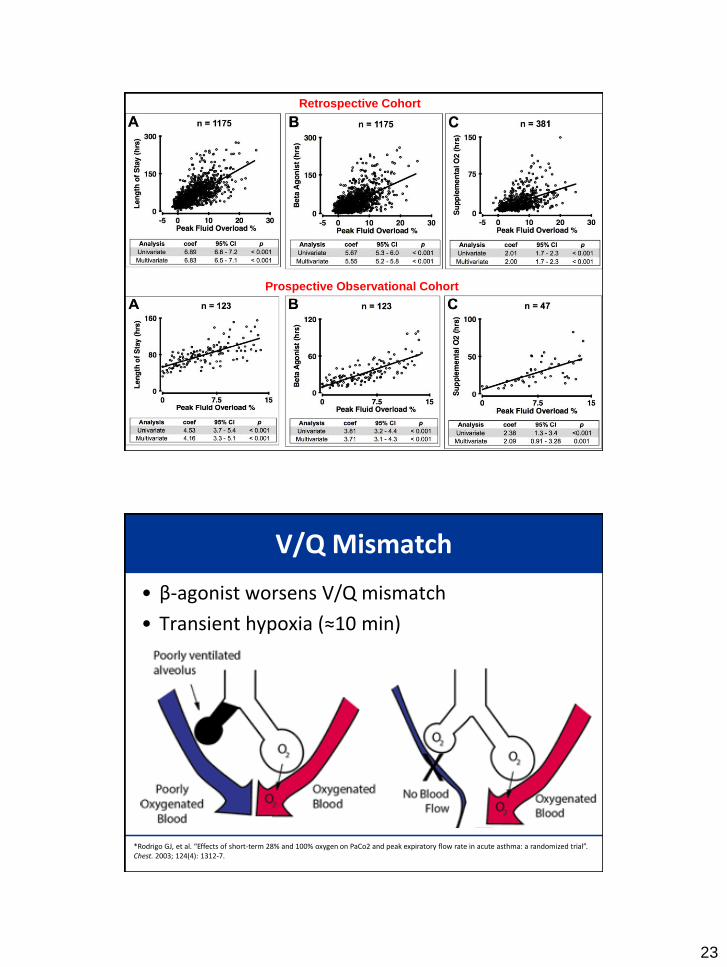
Retrospective Cohort
Prospective Observational Cohort
V/Q Mismatch
• β-agonist worsens V/Q mismatch
• Transient hypoxia (≈10 min)
*Rodrigo GJ, et al. “Effects of short-term 28% and 100% oxygen on PaCo2 and peak expiratory flow rate in acute asthma: a randomized trial”. Chest. 2003; 124(4): 1312-7.
24
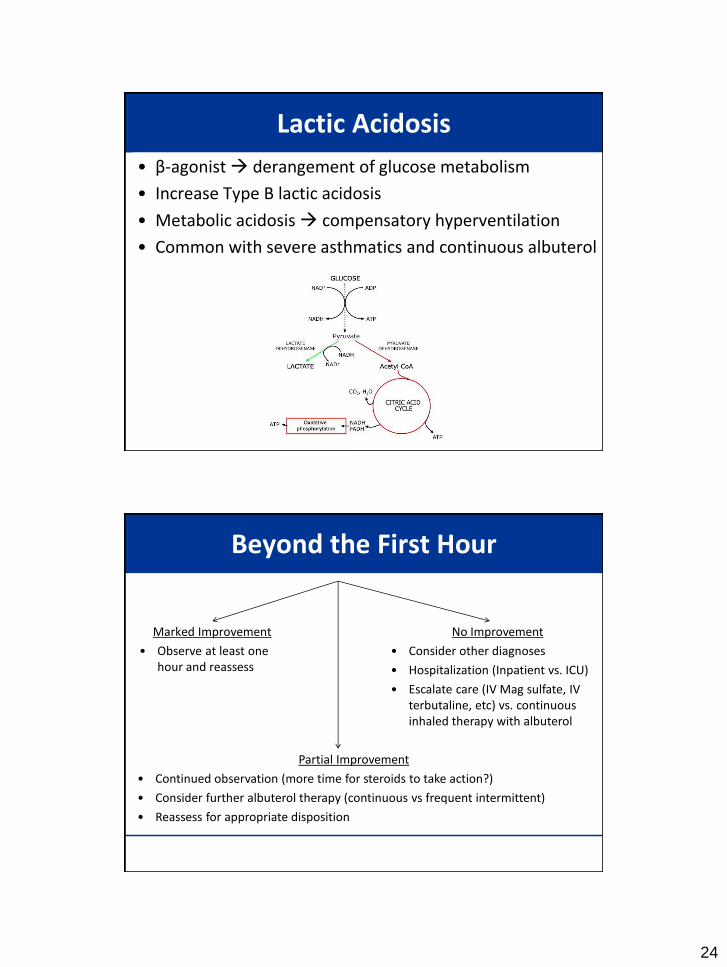
Lactic Acidosis
• β-agonist derangement of glucose metabolism
• Increase Type B lactic acidosis
• Metabolic acidosis compensatory hyperventilation
• Common with severe asthmatics and continuous albuterol
Beyond the First Hour
Marked Improvement
• Observe at least one hour and reassess
No Improvement
• Consider other diagnoses
• Hospitalization (Inpatient vs. ICU)
• Escalate care (IV Mag sulfate, IV terbutaline, etc) vs. continuous inhaled therapy with albuterol
Partial Improvement
• Continued observation (more time for steroids to take action?)
• Consider further albuterol therapy (continuous vs frequent intermittent)
• Reassess for appropriate disposition
25
Take Home Points
• Get steroids onboard early
– Decadron = Prednisone
• Duoneb x 3 in first hour
• MDI-Spacer = Nebulizer
• Advance therapies (continuous, magnesium, parental beta-agonist)
• Avoid pitfalls (V/Q mismatch, lactic acidosis, IVF)
References• Wang LY, et al. “Direct and Indirect Cost of Asthma in School-age Children”. Preventing Chronic Disease. Jan 2005.
• Mayrides M, et al. “Ethnic Disparities in the Burden and Treatment of Asthma”. AAFA/National Pharmaceutical Council. 2005.
• The Express Scripts Lab. The 2014 Drug Trend Report. March 2015. http://lab.express-scripts.com/drug-trend/report/
• Bousquet J, et al. “Uniform definition of asthma severity, control, and exacerbations: document presented for the World Health Organization Consultation on Severe Asthma”. Journal of Allergy and Clinical Immunology. Nov 2010. 126(5): 926-38.
• Singer AJ, et al. “A call for expanding the role of emergency physician in the care of patients with asthma”. Annals of Emergency Medicine. Mar 2005. 45(3): 295-8.
• Carrol CL, et al. “A modified pulmonary index score with predictive value for pediatric asthma exacerbation”. Annals of Allergy, Asthma, and Immunology. 2005 Mar; 94(3):355-9.
• Cates CJ, et al. “Holding chambers (spacer) versus nebulisers for beta-agonist treatment of acute asthma”. Cochrane Database Systematic review. 2014 Sept 13;(9):CD000052.
• Doan Q, et al. “Cost-effectiveness of meter-dose inhalers for asthma exacerbations in the pediatric emergency”. Pediatrics 2011. 127;(5): e1105-e1111.
• Castro-Rodriguez JA, et al. “Beta-agonists through meter-dose inhaler with valved holding chamber versus nebulizer for acute exacerbation of wheezing or asthma in children under 5 years of age: a systematic review with meta-analysis”. Journal of Pediatrics. 2004. 145: 172-7.
• Dolovich MB, et al. “ Device selection and outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology”. Chest. Jan. 2005. 127(1): 335-71.
• Qureshi F, et al. “Clinical efficacy of racemic albuterol vs levalbuterol for the treatment of acute pediatric asthma”. Annals of EM. 2005 Jul; 46 (1):29-36.
• Jat KR, et al. “Levalbuterol versus albuterol for acute asthma: a systematic review and meta-analysis”. Pulm Pharm Therapy. 2013 Apr; 26(2):239-48.
• Bio LL, et al. “Comparison of levalbuterol and racemic albuterol based on cardiac adverse effects in children”. Journal of Ped Pharm Therapy. 2011 Jul-Sep; 16(3): 191-198.
• Kelly A, et al. “Comparison of heart rate changes associated with levalbuterol and racemic albuterol in pediatric cardiology patients. Annals of Pharmacotherapy. 2013 May; 47(5): 644-50
• Rodrigo GJ, et al. Anticholinergic in the treatment of children and adults with acute asthma: a systematic review and meta-analysis”. Thorax. 2005 Sep; 60(9): 740-6.
• Vezina K, et al. “Combined inhaled anticholinergics and short-acting beta2-agonists for initial treatment of acute asthma in children”. Cochrane Database Systematic Review. 2013 Aug 21;(8): CD000060.
26
References• Bogie AL, et al. “Comparison of intravenous terbutaline versus normal saline in pediatric patients on continuous high-dose nebulized
albuterol for status asthmaticus”. Pediatric Emergency Care. 2007 un; 23(6): 355-61.
• Shan Z. et al. “Intravenous and nebulized magnesium sulfate for treating acute asthma in adults and children: a systematic review and meta-analysis” Respiratory Medicine. 2013 Mar; 107(3): 321-30.
• Allen JY, et al. “The efficacy of ketamine in pediatric emergency department patients who present with acute severe asthma”. Annals of Emergency Medicine. 2005 Jul; 46(1): 43-50.
• Rodrigo GV, et al. “Heliox for the non-intubated acute asthma patients”. Cochrane Collaboration. 2010.
• Rowe BH, et al. “Early emergency department treatment of acute asthma with systemic corticosteroids”. Cochrane Database Systematic Review. 2001; (1):CD002178.
• Hendeles L, et al. “Are inhaled corticosteroids effective for acute exacerbation of asthma in children?”. Journal of Pediatrics. 2003; Feb; 142(2 Suppl): S26-32; discussion S32-3.
• Qureshi F, et al. “Comparative efficacy of oral dexamthasone versus oral prednisone in acute pediatric asthma”. Ped. Jul 2001; 139(1): 20-6.
• Schwartz ES et al. “Is dexamethasone as effective as prednisone or prednisolone in the management of pediatric asthma exacerbations? ”. Annals of Emergency Medicine. Jan 2001; 65(1): 81-2.
• Williams KW, et al. “Parental preference for short- versus long-course corticosteroid therapy in children with asthma presenting to the pediatric emergency department”. Clinical Pediatrics. Jan 2013; 52(1): 30-4.
• Hames H et al. “A palatability study of a flavored dexamethasone preparation versus prednisolone liquid in children ”. Canadian J ClinPharmacol. Winter 2008; 15(1): e95-8.
• Andrews A et al. “A cost-effectiveness analysis of dexamthasone vs prednisone in pediatrics acute asthma exacerbation”. Acad EmergMed. Aug. 2012; 19(8): 943-8.
• Kantor DB, et al. “Fluid balance is associated with clinical outcomes and extravascular lung water in children with acute asthmaexacerbation”. Am J Respir Crit Care Med. 2018 Jan 9.
• Scarfone RJ, et al. “Emergency physicians’ prescribing of asthma controller medications”. Pediatrics. 2006 Mar; 117(3): 821-7.
• Lehman HK, et al. “Initiation of maintenance antiinflammatory medication in asthmatic children in pediatric emergency department. Pediatrics. 2006 Dec; 118(6): 2394-401.
Questions/Evaluation
https://survey.az1.qualtrics.com/jfe/form/SV_0cuBSHq4y5LGc3X


















