Emergency Room Utilization in the Navy
26
Emergency Room Utilization in the Navy C. Allison Russo Kennell and Associates, Inc. Day 3 – June 6, 2012
description
Emergency Room Utilization in the Navy. C. Allison Russo Kennell and Associates, Inc. Day 3 – June 6, 2012. Outline. Describe patterns of ER utilization in the MHS and Navy Medicine. Discuss special topics related to ER utilization analysis. - PowerPoint PPT Presentation
Transcript of Emergency Room Utilization in the Navy

Emergency Room Utilization in the Navy
C. Allison Russo
Kennell and Associates, Inc.
Day 3 – June 6, 2012

Outline
• Describe patterns of ER utilization in the MHS and Navy Medicine.
• Discuss special topics related to ER utilization analysis.
• Discuss potential reasons for high ER utilization in the MHS and Navy Medicine.
FOR OFFICIAL USE ONLY2

Why do we care?
• Indicator of poor access, lack of continuity, patient education needs
• Used by many payers as an indicator of quality
• Can be costly• Evaluated by Services and HA/TMA in
several formats for several purposes
FOR OFFICIAL USE ONLY3

Table 1a: The overall number of ER visits and network ER visits in the MHS
increased, but MTF ER visits slightly decreased, FY 2004-2011
FY 04 FY 11 % Change
Purchased Care 1.2M 1.8M 54%
Direct Care 1.2M 1.2M -1%
Total 2.4M 3.0M 26%
Note: Includes ADSMs, ADDs, and NADDs<65 in CONUS.
4
FOR OFFICIAL USE ONLY4

Table 1b: Even when adjusted for population changes, ER visit rates in the MHS increased for network care
and decreased for direct care, FY 2004-2011ER Visits/1000
FY 04 FY 09 % ChangePurchased Care 209 290 39%Direct Care 215 193 -10%Total 423 483 14%Note: Includes ADSMs, ADDs, and NADDs<65 in CONUS. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
5
FOR OFFICIAL USE ONLY5

Table 2: MHS-wide, ADDs have the highest rate of ER visits, but ADSMs experienced the
largest increase from FY 2004-2011ER Visits/1000
Beneficiary Category FY 04 FY11 % Change
ADSMs 363 452 25%
ADDs 537 663 23%
NADDs <65 359 359 0%
423 483 14%Note: Includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
6
FOR OFFICIAL USE ONLY6

Table 3: Annual ER visit rates for the Navy are lower than the Army's rates, FY 2011
ER Visits/1000Type of
Enrollees Navy Army Air Force MHS
ADSMs 378 527 430 452
ADDs 658 714 564 663
NADDs <65 363 382 327 359
Total 465 540 417 483Note: Includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
7
FOR OFFICIAL USE ONLY7

Table 4: Annual ER visit rates are highest for enrollees with a MTF PCM, FY 2011
ER Visits/1000Beneficiary
Category MTF PCM Civ PCM Not Prime Total
ADSMs 435 343 N/A 452
ADDs 674 550 888 663
NADDs <65 404 317 364 359
Total 513 412 494 483Note: Includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
8
FOR OFFICIAL USE ONLY8

Table 5: Among enrollees with a MTF PCM, Navy ER visit rates are lower than the Army's rates for
all beneficiary categories, FY 2011ER Visits/1000 (MTF PCM)
Type of Enrollees Navy Army Air Force MHS
ADSMs 369 498 422 435
ADDs 671 740 582 674
NADDs <65 400 434 380 404
Total 481 583 467 513Note: Includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
9
FOR OFFICIAL USE ONLY9

10
FOR OFFICIAL USE ONLY10
Table 6: Annual ER visit rates are higher for enrollees with a Navy MTF PCM even in inpatient catchment areas,
FY 2011ER Visits/1000
Beneficiary Location MTF PCM Civ PCM
IP catchment areas 476 449
Non-catchment areas 504 395
Prism, non-catchment area 401 383
Non-prism, non-catchment area 1311 401
Note: Includes purchased care and direct care.

Table 7a: Among Navy Prime enrollees, ADDs had higher ER utilization than NADD <65, regardless of PCM type, beneficiary
location, age, and gender, FY 2011MTF PCM Civ PCM
ER Visits/1000 ER Visits/1000
Beneficiary Characteristics ADD NADD <65 ADD NADD <65Total Prime Enrollees: 671 400 569 317Beneficiary Location:IP catchment areas 668 414 579 328Non-catchment areas 687 326 556 310Prism, non-catchment area 585 300 538 301Non-prism, non-catchment area 1793 476 565 314
Age Group:00-04 930 648 732 46105-14 417 352 350 25615-17 432 378 378 29518-24 952 456 833 38525-34 736 682 669 60635-44 520 412 466 35745-64 459 388 424 295
Gender:Females 695 453 597 359Males 623 349 515 274
Note: Includes purchased care and direct care.
11
FOR OFFICIAL USE ONLY11


Table 8: Enrollees with an Navy MTF PCM have ER visit rates that are more than 20 percent higher than
the US civilian average, FY 2011ER Visits/1000
Navy MHSU.S.
Population*
MTF PCM Civ PCM Navy Total MHS Total U.S. TotalTotal ER visits: 481 421 465 483 391Visits by age: <18 years 592 432 511 511 36218-44 years 463 525 508 548 43345-64 years 377 298 345 348 317
Visits by sex:Female 635 474 559 569 414Male 383 354 380 405 361
Note: MHS includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.* As reported in Tang N, Stein J, Hsia RY, Maselli JH, Gonzales R. Trends and characteristics of US emergency department visits, 1997-2007. JAMA. 2010 Aug 11;304(6):664-70.
13
13

Table 9: ADDs have ER visit rates that are nearly 70 percent higher than the U.S. civilian average
ER Visits/1000
NavyU.S.
Population* ADSM ADD NADD <65 Navy Total U.S. Total
Total ER visits: 378 658 363 465 391Visits by age: <18 years NA 591 326 511 36218-44 years 382 766 447 508 43345-64 years 291 528 341 345 317
Visits by sex:Female 684 689 413 559 414Male 332 597 311 380 361
Note: MHS includes purchased care and direct care. Rates have been adjusted to account for OHI use among ADDs and NADDs<65 not enrolled in TRICARE Prime.
* As reported in Tang N, Stein J, Hsia RY, Maselli JH, Gonzales R. Trends and characteristics of US emergency department visits, 1997-2007. JAMA. 2010 Aug 11;304(6):664-70.
14
FOR OFFICIAL USE ONLY14

Figure 1: MTF Prime enrollees have ER visit rates that are higher than the privately-insured and the uninsured*
15
* As reported in Tang N, Stein J, Hsia RY, Maselli JH, Gonzales R. Trends and characteristics of US emergency department visits, 1997-2007. JAMA. 2010 Aug 11;304(6):664-70.
15

Figure 2: Purchased care ER visits had higher intensity coding than MTF ER visits, FY 2011
16
FOR OFFICIAL USE ONLY16

Table 8: Top 10 ER visit diagnoses in FY11 in the Direct Care system compared to the Purchased Care system
Direct Care Rank DX Description
% of all DC ER Visits Cum %
PC Rank of this DX
% of all PC ER Visits
1 465 Acute upper respiratory infections 4.8% 5% 4 2.6%2 780 General symptoms 4.0% 9% 3 5.1%3 786 Symptoms invl respiratory sys & oth chest symp 3.9% 13% 1 5.6%4 789 Oth symptoms invl abdomen & pelvis 3.7% 16% 2 5.4%5 787 Symptoms invl digestive sys 3.2% 20% 5 2.5%6 462 Acute pharyngitis 2.8% 22% 9 1.9%7 382 Suppurative and unspecified otitis media 2.6% 25% 7 2.2%8 724 Oth unspecified dis of back 2.4% 27% 8 1.9%9 599 Oth dis of urethra and urinary tract 2.2% 30% 12 1.8%
10 079 Viral and chlamydial infection 2.1% 32% 20 1.1%
17
FOR OFFICIAL USE ONLY17

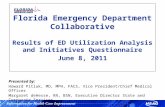
18
Total Navy ER Visits (FY11)N=2.7 million
Injury16%
Classified by Algorithm66.1%
Non-Emergent21%
Emergent/Primary Care Treatable
35%
Emergent – ED Care Needed – Preventable/Avoidable
5%
Emergent – ED Care Needed – Not Preventable/Avoidable
22%
Classified by Algorithm84%
NYU Algorithm

FOR OFFICIAL USE ONLY19
Special Topics for ER Utilization Analysis

How are ER records identified?
• Purchased Care:• TED-NI (professional services) claims
• Place of Service=23 and CPT codes 99281-99285• Limit to 1 ER visit per person per day
• Direct Care:• CAPER
• CPT codes 99281-99285 and MEPRS Code starts with “BI”
• Caution using TED-I (facility) claims• Caution using TED-NI claims without limiting
to 1 person per day (double-counts any consults)
• M2 Corporate Document available for ER visitsFOR OFFICIAL USE ONLY
20

What about Urgent Care Centers?
• Can be defined using Place of Service code• Very inaccurate; most are coded as office visits
• Apparent increases in UCC utilization is partially due to push by MCSC to code place of service better
• From cost perspective, UCC use is better: same cost as an office visit
• From quality/continuity perspective, UCC use can be a concern; however, very difficult to accurately id.
FOR OFFICIAL USE ONLY21

Potential Population and Health System Factors That
Increase ER Use
• Population changes• Demographic changes• Socioeconomic status• Multiple chronic conditions
• Outpatient capacity constraints:• Difficult for patients to obtain outpatient appointments• Longer average appointment waiting times
• HMO enrollment• Other community differences
• Regional practice variation• ER capacity• Population’s generic preferences and habits
22
FOR OFFICIAL USE ONLY22

Summary of Key Findings
• The overall number of MHS ER visits is increasing (3.0M visits in FY2011)
• When adjusted for changes in the eligible population, ER utilization increased 14% over seven years - 39% increase for purchased care and a 10% decline for direct care
• ADDs have the highest ER visit rates, regardless of enrollment type
• Annual ER visit rates for the Navy are lower than the Army's rates, averaging 465 visits per 1,000.
• MTF PCM enrollees have 25 percent higher ER utilization than civilian PCM enrollees
23
FOR OFFICIAL USE ONLY23

Key Findings (cont.)
• Prime enrolled ADDs have higher ER utilization than NADDs <65, regardless of PCM type, beneficiary location, age group, and gender.
• Navy MTF Prime ER utilization exceeds the U.S. civilian rate by 23%; 64% higher among children <18 years old and 54% higher among females.
• Non-emergent and primary care treatable conditions accounted for 56% of all ER visits in FY 2011
24
FOR OFFICIAL USE ONLY24

Key Findings (cont.)
• ER utilization among ADDs is 60% higher than U.S. civilian rates
• ER utilization rates among TRICARE Prime enrollees exceeds the rate for privately-insured and uninsured U.S. civilians
• There is an increase in the intensity of ER visits, particularly among purchased care ER visits; yet, the mix of primary diagnoses has not changed significantly over time or between purchased and MTF care
25
FOR OFFICIAL USE ONLY25