
Emergency Humanitarian Response Plan for Kenya 2009 …€¦ · Web view · 2017-09-14sample of...
149
Transcript of Emergency Humanitarian Response Plan for Kenya 2009 …€¦ · Web view · 2017-09-14sample of...

SAMPLE OF ORGANISATIONS PARTICIPATING IN CONSOLIDATED APPEALS
AARRECACFACTEDADRAAfricareAMI-FranceARCASBASIAVSICARECARITASCEMIR INTERNATIONALCESVICFACHFCHFICISVCMACONCERNConcern UniversalCOOPICORDAID
COSVCRSCWSDanchurchaidDDGDiakonie Emergency AidDRCEM-DHFAOFARFHIFinnchurchaidFSDGAAGOALGTZGVCHandicap InternationalHealthNet TPOHELPHelpAge InternationalHKIHorn Relief
HTHumedicaIAILOIMCINTERMONInternewsINTERSOSIOMIPHDIRIRCIRDIRINIRWIslamic RWJOINJRSLWFMalaria ConsortiumMalteserMercy CorpsMDA
MDMMEDAIRMENTORMERLINNCANPANRCOCHAOHCHROXFAMPA (formerly ITDG)PACTPAIPlanPMU-IPURC/GermanyRCOSamaritan's PurseSECADEVSolidaritésSUDOTEARFUND
TGHUMCORUNAIDSUNDPUNDSSUNEPUNESCOUNFPAUN-HABITATUNHCRUNICEFUNIFEMUNJLCUNMASUNOPSUNRWAVISWFPWHOWorld ConcernWorld ReliefWVZOA

TABLE OF CONTENTS
1. EXECUTIVE SUMMARY...................................................................................................................................1
Table I. Summary of Requirements - By Cluster....................................................................................2Table II. Summary of Requirements - By Appealing Organisation..........................................................3
2. 2008 IN REVIEW...............................................................................................................................................5
3. THE 2009 COMMON HUMANITARIAN ACTION PLAN..................................................................................7
3.1 THE CONTEXT AND HUMANITARIAN CONSEQUENCES.....................................................................................7
3.2 SCENARIOS...............................................................................................................................................15
3.3 STRATEGIC OBJECTIVES FOR HUMANITARIAN RESPONSE IN 2009...............................................................16
3.4 CLUSTER/SECTOR RESPONSE PLANS.........................................................................................................173.4.1 Coordination....................................................................................................................................173.4.2 Early Recovery and Food Security..................................................................................................183.4.3 Education.........................................................................................................................................203.4.4 Food Aid and Nutrition.....................................................................................................................233.4.5 Health..............................................................................................................................................253.4.6 Multi-Sector: Protection of Refugees and Asylum Seekers in Kenya..............................................283.4.7 Protection/ Human Rights/ Rule of Law...........................................................................................313.4.8 Shelter/NFI and Camp Coordination and Camp Management........................................................363.4.9 Water, Sanitation and Hygiene........................................................................................................38
4. CRITERIA FOR SELECTION OF PROJECTS...............................................................................................42
5. STRATEGIC MONITORING PLAN.................................................................................................................42
6. COMPLEMENTARITY WITH OTHER ACTORS............................................................................................42
ANNEX I: STRATEGIC FRAMEWORK FOR HUMANITARIAN RESPONSE................................................59
ANNEX II. SECTOR RESPONSE: ACHIEVEMENTS AND CHALLENGES...................................................44
ANNEX III. TABLE III. LIST OF PROJECTS – (GROUPED BY CLUSTER)...................................................77
ANNEX IV. TABLE IV. LIST OF PROJECTS – (GROUPED BY APPEALING ORGANISATION...................84
ANNEX V. TABLE V. SUMMARY OF REQUIREMENTS – (GROUPED BY IASC STANDARD SECTOR). .94
ANNEX VI. DONOR RESPONSE TO 2008 APPEAL.......................................................................................95
ANNEX VII. ACRONYMS AND ABBREVIATIONS...........................................................................................107
Please note that appeals are revised regularly. The latest version of this document is available on http://www.humanitarianappeal.net
Full project details can be viewed, downloaded and printed from www.reliefweb.int/fts
iii

iv

K E N Y A
1. EXECUTIVE SUMMARY
The crisis which followed the 2007 presidential elections in Kenya gave rise to a sudden and large-scale humanitarian emergency, the effects of which were felt far beyond Kenya’s borders. Violence in many parts of the country led to the killing of approximately 1,300 persons and the displacement of over 300,000. The disruption of livelihoods and essential services affected large numbers throughout the country and the interruption of transport hampered the delivery of humanitarian aid to neighbouring countries and economic activity in the region. Thanks to progress in political processes and the joint efforts of humanitarian stakeholders, the situation has stabilised over the course of the year with many IDPs returning to their homes and resuming their livelihood activities. The returns process was facilitated by the launch of the Government’s Operation Rudi Nyumbani (Return Home) in May. To date, the Government estimates that fewer than 10,000 people remain in IDP camps and more than 238,047 people have returned to pre-displacement areas and transit sites. Despite the many positive developments, the Government of Kenya estimates that at least 54,000 remain in transit sites and others have yet to return. Continued assistance is required to facilitate durable solutions for those who have yet to re-establish their homes and livelihoods.
Meanwhile, other multiple factors have affected livelihoods and food security throughout the country. Poor long rains, rising food and commodity prices, reduced cereal production and livestock diseases have converged to increase food insecurity among many vulnerable populations, including pastoralists in northeastern and northwestern arid and semi-arid land (ASAL) areas, coastal lowland areas and amongst the urban poor. As of September 2008, more than 1.3 million people were estimated to require food assistance. A lack of adequate water and pasture in affected parts of the ASAL regions has also contributed to an escalation in conflicts as communities compete for increasingly scarce resources. In October 2008, both Mandera and Turkana Districts were affected by substantial flooding: more than 9,600 people were displaced by floods and inter-clan conflict in Mandera and there was serious crop damage and significant loss of livestock in Turkana. Crises in other parts of the country also persist, including in Mount Elgon where activities of the Sabaot Land Defence Force (SLDF) militia and counter-insurgency efforts have led to displacements.
Regionally, Kenya’s porous borders have witnessed continued refugee flows. The deterioration in the situation in Somalia precipitated increased movements of Somalis over the border into Kenya. This influx adds to a refugee population which already far exceeds the capacity of existing refugee camps. Due to the continuing crisis in Somalia, new arrivals are expected to continue during 2009, increasing the strain on existing refugee support mechanisms.
During 2008, humanitarian actors have faced a multitude of challenges due to the changing nature of humanitarian needs in the country. Stakeholders have worked together to respond flexibly to new developments, despite the many competing priorities. Thanks to the generous support of donors, a total of $1259.8 million has been committed to humanitarian action in Kenya, of which $146.4 million was received through the 2008 Emergency Humanitarian Response Plan (EHRP).
In light of the continued need to support post-election affected populations, those affected by climatic shocks, food and livelihood insecurity, and growing numbers of refugees, partners have agreed that a coordinated multi-sector approach to humanitarian assistance in Kenya continues to be necessary. As such, it has been agreed by IASC members that a Common Humanitarian Action Plan (CHAP) and associated appeal should be developed for Kenya. The process was facilitated through a two-day consultation with stakeholders and subsequent follow up to develop response plans and projects in all relevant clusters. The EHRP comprises a harmonised multi-sector strategy for response to humanitarian and early recovery needs, as well as for preparedness measures to mitigate the impact of new crises.
The plans and projects presented in this document have been developed with the participation of over 50 organisations, including the Government of Kenya, local and international NGOs, UN agencies and the Kenya Red Cross Society (KRCS). The appeal outlines key response and preparedness requirements as well as early recovery strategies in eleven sectors. A total of $390 million is requested to meet the most urgent needs of targeted populations.
1 All dollar signs in this document denote United States dollars. Funding for this appeal should be reported to the Financial Tracking Service (FTS, [email protected]), which will display its requirements and funding on the CAP 2009 page.
1

K E N Y A
Table I. Summary of Requirements - By Cluster
2

K E N Y A
Table II. Summary of Requirements - By Appealing Organisation
3

K E N Y A
4

K E N Y A
2. 2008 IN REVIEW
The outbreak of violence that followed the disputed presidential election in December 2007 led to a large humanitarian crisis and a significant scaling up of emergency operations in Kenya. In the weeks and months that followed elections, violence led to the deaths of an estimated 1,300 persons and displaced up to 500,000 people around the country—massively disrupting the country’s basic services and economic activity. The impacts were felt throughout the East and Central Africa region as essential transport routes were disrupted, halting the supply of humanitarian goods and trade activities.
In January 2008, humanitarian partners launched the Emergency Humanitarian Response Plan in response to the post-election crisis, outlining sector response strategies in the immediate aftermath of the crisis. In April, the Plan was revised to more comprehensively reflect needs and to include early responses to drought. Within this framework more than 50 UN agencies and NGOs requested a total of $191 million for 140 projects in ten sectors2. The EHRP identified six overall strategic priorities:
Providing coordinated assistance to, and protection of, IDPs and other vulnerable populations according to their own expressed needs and preferences and in line with internationally accepted norms and the Guiding Principles on Internal Displacement;
Promoting community-based peace building and reconciliation that allows for underlying grievances to be addressed and IDPs to be peacefully resettled and re-integrated into communities;
Enhancing support for and increasing access to basic social services to IDPs and host populations, including weather-proofing displaced camps and effective service delivery;
Supporting the recovery of lost livelihoods, reducing vulnerability and strengthening coping capacities for vulnerable or food-insecure populations;
Supporting policy development and strengthening national institutions to mitigate future crises; Addressing HIV/AIDS related vulnerabilities amongst IDPs and host communities (drug
resistance, testing services, tuberculosis [TB] and access to anti-retrovirals [ARVs]).
As of 12 November, OCHA’s Financial Tracking System (FTS) had recorded a total of $259.8 million in commitments and contributions to Kenya in 2008. Of this amount, $146.4 million had been committed to activities in the EHRP, representing 71% of the total funds requested. Overall the level of funding received in 2008 is the highest since 2000 when contributions to Kenya began to be recorded. Whilst this overall picture is very positive, the disparity between sectors has been broad, with a range of funding levels between 35% for economic recovery and infrastructure and almost 94% for multi-sector assistance. Other sectors that received less than 50% of the funds requested include education, agriculture, shelter and non-food items (NFIs), and water and sanitation.
Of the total funding received for Kenya, $21.4 million (of which $15.4 was specifically for activities in the EHRF) has been contributed through the CERF in four separate allocations: three from the rapid response window and one under-funded allocation. These funds have been prioritised for needs related to the post-election crisis, under-funded sectors within the refugee response, and the impact of rising food prices.
In response to the post-election crisis, the Humanitarian Country Team put in place a number of emergency coordination mechanisms to assist with the response. These included the roll-out of the cluster approach and the formation of the Inter-Agency Standing Committee (IASC). For the Kenya context, 11 clusters3 were identified with two sub-clusters4 to ensure a more accountable and predictable response. At the same time, humanitarian partners responded quickly – and in some cases immediately - establishing field hubs in affected areas to ensure an effective on-the-ground response. The creation and operationalisation of clusters and other coordination mechanisms at national and
2 Further revisions have brought the total to $207.6 million as of mid-November.3 Camp Coordination and Camp Management, Early Recovery and Food Security, Education, Emergency Telecommunications, Food Aid, Health, Logistics, Nutrition, Protection, Shelter and NFIs, Water and Sanitation.4 Gender Based Violence and Child Protection were identified as sub-clusters under the Protection Cluster.
5
Pastoralist in Turkana. July 2008Mercy Manyala, OCHA Kenya

K E N Y A
sub-national level was undertaken rapidly and contributed to improved gap identification and minimal duplication. The coordination arrangements have further contributed to strengthening partnerships, including those with the Government of Kenya. In the coming year, these partnerships will form the cornerstone of humanitarian response, as well as preparedness and capacity-building activities.
In August, humanitarian partners reviewed current cluster / sector coordination arrangements in light of the changing contexts within the country. It was agreed that in moving ahead, the clusters would focus on support to national mechanisms for sector coordination at national and sub-national level. In addition, partners emphasised the need to include consideration of humanitarian needs beyond the post-election crisis, as well as to develop preparedness measures for conflict, drought, refugees and other humanitarian situations.
The unexpected nature and scale of the post-election crisis led to significant challenges in the early stages of response. A proliferation of actors and a highly fluid context further complicated coordination and response. A lack of flexible funding and insufficient existing capacity led, in some cases, to delays in the early phases. However, subsequent efforts have contributed to coordinated and multi-level advocacy and resource mobilisation.
The dominant focus on the post-election crisis presented challenges in responding to other humanitarian needs in Kenya. In addition to emerging drought conditions, rising food prices and virulent livestock diseases have contributed to diminished food security in predominantly pastoral ASAL areas leading to greater conflicts over resources. Whilst awareness of these is growing, capacity and resource constraints limited comprehensive early action. Similarly, the response to needs related to other displacement contexts, including refugees and pre-existing internal displacement, such as that seen in Mount Elgon, have also been constrained by the focus on the post-election displacement.
A cluster/sector breakdown of achievements and challenges is provided in the table in Annex I.
6

K E N Y A
3. THE 2009 COMMON HUMANITARIAN ACTION PLAN
3.1 THE CONTEXT AND HUMANITARIAN CONSEQUENCES PoliticalWidespread violence which followed the disputed presidential elections in December 2007 resulted in the deaths of an estimated 1,300 persons and the displacement of more than 500,000 people and signalled a serious protection crisis. Rioting and looting broke out in cities and towns, particularly in the Rift Valley, the west of the country and in and around Nairobi. Many civilians moved to their ancestral homelands and urban areas for security, despite the likelihood of insufficient services to meet the needs of the displaced in these areas.
After a power-sharing deal was signed on 28 February and a Grand Coalition Government was formed, the Kenya National Dialogue and Reconciliation Implementation Committee is now overseeing several commissions and activities to address some of the core drivers of conflict. To ensure a lasting peace and meaningful reconciliation, it is recognised that the long-term root causes of ethnic tension and violence must be addressed.
The Independent Review Commission, mandated to investigate all aspects of the December 2007 General Election in Kenya, concluded it was not possible to identify which party had genuinely won the presidential elections. The Commission has developed a set of recommendations which require urgent attention in advance of the 2012 elections, including an overhaul of the electoral system, in order to prevent a similar situation from occurring.
As a critical part of the peace-building process, the established Truth, Justice and Reconciliation Commission is expected to complete its work by 2010, while measures to address inequities and regional imbalances are planned for the next three years. District Peace Committees and NGO partners are supporting peace-building activities in the most affected areas. However, the debate over whether perpetrators of the post-election violence (PEV) should receive amnesty continues to fuel divisions and divert reconciliatory processes.
The Commission of Inquiry into the Post-Election Violence recommended that a special tribunal be set up to hold accountable those who were most responsible for crimes during the violence. The Commission report also called for the implementation of the Conflict and Disaster Early Warning and Response System to address operational and service delivery issues that emanated from the crisis period. Furthermore, in spite of evidence to the Commission from both the Police Commissioner and the Attorney General that no data existed of sexual violence during the emergency, the Commission specifically elected to hear evidence from GBV survivors, including in camera hearings.5
Recognising that land-related issues are among the primary drivers of conflict, there has been widespread demand for first National Land Policy since 1963 to be passed. The Policy is expected to address irregular allocations of land and improve equitable access to land.
EconomicThough peace and reconciliation remain at the forefront of the national agenda, many Kenyan households prioritise economic security and development as they experience the pressure of increased inflation and rising commodity prices. Inflation had risen to 27.6% in August, from 18.2% in January. In May, inflation had reached a 15-year high of 31.5% as the result of a slowdown in production due to the post-election violence, erratic rains, and global increases in commodity prices.
Poverty also continues to be a key development challenge in Kenya: 46% of the population lives below the income poverty line of $1 per day. Food poverty6 is the highest
5 The Commission of Inquiry into the Post-Election Violence (The Waki Commission), submissions by FID-K on sexual and gender-based violence, supported by the GBV subcluster.6 The Kenya Integrated Household Budget Survey (KIHBS) 2005/2006 classifies households as facing food poverty when their food consumption levels “are insufficient to meet their basic daily emergency requirements of 2,250 kilocalories per adult equivalent”. Food poverty is measured by consumption expenditure, designated as less than 988 KES (Kenyan shilling)/month for rural inhabitants and less than 1,474 KES/month for urban inhabitants.
7
Young children scavenge for valuables in a dumpsite in Nairobi, Kenya. September 2008. © Julius Mwelu/IRIN

K E N Y A
among pastoralists (71%), followed by marginal agriculturalists (54%) and agro-pastoralists (40%) in the ASALs. Furthermore, an estimated 7.6 million people reside in urban slums where communities have limited access to basic services, are dependent on markets and are consequently particularly vulnerable to fluctuations in food and commodity prices.7
Women represent 51% of the Kenyan population but their participation in post-primary education, wage employment, enterprise ownership and decision-making processes is limited. The high incidence of female-headed households in both urban (46.2%) and rural (50%) areas contributes to high poverty levels.8
Internal Displacement
Post-election displacementThe MoSSP reported that as of 28 September less than 10,000 people remained in IDP camps and a total of 238,047 IDPs had returned to pre-displacement areas and transit sites . An unknown number of IDPs are also living in communities in areas of displacement in urban slums and with host families. The returns process was accelerated in May by the government’s launch of Operation Rudi Nyumbani (return home), which included provision of transport and some start-up financial support for returning IDPs. In September the government announced that it is in the last phase of the operation and that all IDP camps were to be closed in October 2008.
A substantial proportion of displaced who left established IDP camps or host communities relocated to transit sites, which are often in close proximity to their pre-displacement homes. The MoSSP and an inter-agency assessment concluded that there were at least 54,000 IDPs in 161 transit sites as of October 2008. Other agencies estimate this figure to be as high as 138,000. Many of the transit sites lack basic services, including adequate sanitation and hygiene facilities, as well as access to schools and health facilities. Food assistance is currently being provided on a monthly basis by WFP through KRCS-run food distribution points. However, the continuous movement of IDPs and the dispersed nature of the transit sites present obstacles to food delivery and adequate service provision.
Some IDP households who are unable to return to areas they resided in prior to the election crisis are combining their resources to collectively purchase land on which to relocate, including some groups comprised of up to 2,500 individuals in areas near Nakuru town. In Mai Mahiu, Naivasha district, 150 households – including 42 female-headed households – have collectively purchased land on which to relocate. The humanitarian community has supported this process and will facilitate the delivery of services to the new sites. However, humanitarian partners have also encouraged local authorities to monitor and support relocation processes to ensure that they are sustainable and in-line with peace building and reconciliation goals and can foster effective integration with the neighbouring communities.
Many children were separated from their families during displacement, were left behind during the returns process so they could continue to attend school, or were separated as parents attempted to restore livelihoods in areas of return. The number of separated children in Kenya increased dramatically: there were approximately 1,774 cases of separated children (related to the PEV) registered in 14 districts as of 4 September. Furthermore, there were 948 children in child-headed households in Eldoret, Subukia, Ekarenyo, Kitale and Molo district (all related to the PEV), the majority of whom were in Molo district. Partners help monitor children who are currently separated and reunite them with families as quickly as possible.Sexual and gender-based violence (SGBV) was perpetrated during the PEV and displacement process; however there was limited awareness of the practice or sensitivity among state and security forces. Furthermore, current mechanisms to report SGBV are inadequate so there is no recourse for
7 Some 70% of the population are net food buyers and its food security is highly susceptible to food price fluctuations. Pastoral areas that are situation far away from surplus areas have poorly integrated markets, where cereal prices range between 70% and 120% above seasonal average. Pastoralists remain highly food-market dependent while rising cereal prices are negatively affecting pastoral terms of trade. 8 Profile of Women’s Socio-Economic Status in Kenya: Institute of Economic Affairs, Kenya 2008.
8
A view of the Eldoret IDP camp, April 2008 which hosted more than 14,000 people displaced by post-election violence. © Manoocher Deghati/IRIN

K E N Y A
survivors to hold perpetrators accountable. In order to address this gap, systems to facilitate reporting and provide support for survivors of SGBV are being developed. In addition specific incidences of SGBV have been presented to the Commission of Inquiry into the PEV. Training was conducted across affected areas on prevention and response to GBV. Issues of sexual exploitation and abuse have also been noted and an adviser from the Gender Standby Capacity Project (GenCap) has been brought in to establish coordination and reporting mechanisms.
Due to the chronic and protracted nature of displacement, particularly among the non-land owning farmers, one of the most critical areas in need of increased support is early recovery, including peace-building, reconciliation and livelihoods support. Early recovery has received approximately 35% of the funding appealed for under the EHRP. Peace-building and reconciliation urgently require increased and sustained engagement of both local and national leaders. Meanwhile, greater investment in livelihoods is essential to ensure that recovery processes take hold so returnees can lead productive lives and meet their basic needs while re-building their socioeconomic security.
To facilitate returnees in rebuilding their livelihoods, the Government has provided start-up funds of Ksh10,000 ($150) per household. The MoSSP reported that 112,900 households had received the Government assistance as of 16 September. However, there have been some complaints from urban IDPs in Nakuru and Naivasha, particularly those who owned small businesses, who claim that the start-up funds are insufficient to support their livelihoods recovery. There have also been reports that some IDPs who were not in camps were not included in the registers.
In addition, the MoSSP plans to construct 40,000 shelters for IDPs by the end of March 2009 under a joint shelter project that was launched on 10 September; partners are also providing shelter to over 3,000 households. The Government shelter project is providing Ksh 25,000 ($357) to households whose shelter was destroyed in the post-election violence. A total of Ksh 438,900,000 had been disbursed to 17,556 households by 13 October. Increased funding for this project is required to support approximately 15,000 households.
Other internally displaced populationsPrior to the 2007 elections, there were an estimated 350,000 IDPs in Kenya, owing to earlier election-related clashes, unresolved land grievances and governance issues, as well as socio-economic insecurity. In the Mount Elgon region, clashes between the SLDF militia, communities and the military has resulted in the death of over 600 people and the displacement of 45,000 persons since January 2007, some of whom remain in five IDP camps in the district. Disruption of socio-economic activities, in particular farming, has seen a decline in cultivation; schools have closed and there have been allegations of human rights violations by both the Kenyan military and SLDF.
From the 6 - 8 September, conflict over land between crop farmers and pastoralists resulted in the displacement of 200 individuals from Maela to Kongoni police station, Naivasha District. In addition, the Government is also planning to evict up to 10,000 households from the Mau Forest during 2008 to preserve a critical water catchement area. This could lead to an increased caseload of chronic IDPs and reverse the resettlement programme. On 14 October, flash floods and inter-clan conflict in Mandera town, North-eastern Province, led to the displacement of approximately 9,600 people.
RefugeesKenya hosts over 300,000 refugees mainly from Somalia and Sudan. In the course of 2008, there has been an influx of refugee arrivals into Kenya due to continued insecurity and humanitarian crisis in Somalia, despite the official closure of the border between the two countries. Further deterioration of the situation in Somalia could result in a continued or increased influx of refugees.
The capacity of the refugee camps near the Kenya-Somali border has already been greatly overstretched. Currently there are over 217,000 refugees in the Dadaab camps in northeastern Kenya, which have an intended capacity of approximately 100,000 people; there are currently over 50,000 in Kakuma refugee camp. The insufficient capacity within the existing refugee camps is of growing concern to humanitarian partners, including the potential health risks posed by overcrowding and insufficient water and sanitation facilities as well as the need to ensure there are adequate resources to meet increases in food assistance needs.
9
IDs relocating from Nakuru ASK IDP Camp to Nyahururu Relocation Site. OCHA.October 2008
K E N Y A
Drought and climatic hazards
DroughtSuccessive failed rainy seasons are causing drought conditions throughout significant portions of the ASAL areas which comprise 80% of Kenya’s livelihood zones. The short rains in late 2007 coincided with La Niña (abnormally cool ocean surface temperatures). As a result, Northern, North Western and Western Provinces, as well as northern and central Rift Valley and parts of Coast Province received depressed rainfall (below 75% of normal) that was poorly distributed both geographically and over time.
The long rains in 2008 were also projected to be below normal and sporadic in many areas, particularly in northern pastoral areas. This was anticipated to lead to a reduction in sub-surface water resources by 50% in some northern areas. As of September, it was estimated that the declining water resources are unlikely to recover sufficiently in the coming months in the northern pastoral areas, even if the October-December short rains are normal. Furthermore, a FEWSNET food security outlook projected that food security would deteriorate to an emergency level, with extreme food insecurity in some parts of the primarily pastoralist north and north-eastern regions between December 2008 and March 2009. Rains are expected
to be below normal in this zone, which is likely to exacerbate drought conditions as well as increase resource-based conflicts and related displacements. The areas currently reporting the most severe deterioration in food security include the northern, western and some eastern pastoral areas, as well as localised areas of the coastal lowlands.
In Mandera West District, water shortages are already affecting tens of thousands of people. Households are relying on three to eight litres of water per person per day. Water pans and dams have dried up in 19 centres, which now rely on costly water trucking. Global acute malnutrition (GAM) rates have soared to 28%, almost twice the emergency level. Livestock migrations have started earlier than normal in search of water and pasture; and clashes have erupted due to competition for scarce resources. The current drought emerging in Mandera and other parts of North Eastern Province is the fifth drought in the past ten years. Populations have yet to recover from the devastating effects of the 2005 drought.
Drought conditions in the Turkana area have triggered migration into neighbouring areas, including across the border into Uganda. Resultant clashes over scarce resources have pushed pastoralists into dry areas with insufficient access to water and pasture. The GAM rate in some parts of Turkana is reported to be as high as 30%.
FloodingThe risk of flooding along the country’s main river basins in 2009 is a great concern and highlights the need for preparedness and response to a multitude of climatic hazards. These risks were evident in many areas in 2008.
Multiple factors have led to the displacement of over 9,600 persons in the vicinity of Mandera Town in mid-October. While approximately two-thirds were displaced by the actual floods, 3,800 people were displaced by inter-clan violence which erupted in the wake of the floods. Competition for scarce resources (owing to successive droughts and the recent floods) and clan rivalries are fuelling the clashes, which led to at least ten deaths between 16-21 October. The floods, caused by heavy rains in the Ethiopian highlands, submerged seven wells and 350 toilets, caused the closure of three schools, washed away one kilometre of water pipeline and led to the disappearance of livestock. Contaminated water sources and disease outbreak threaten the 150,000 residents of Mandera Town.
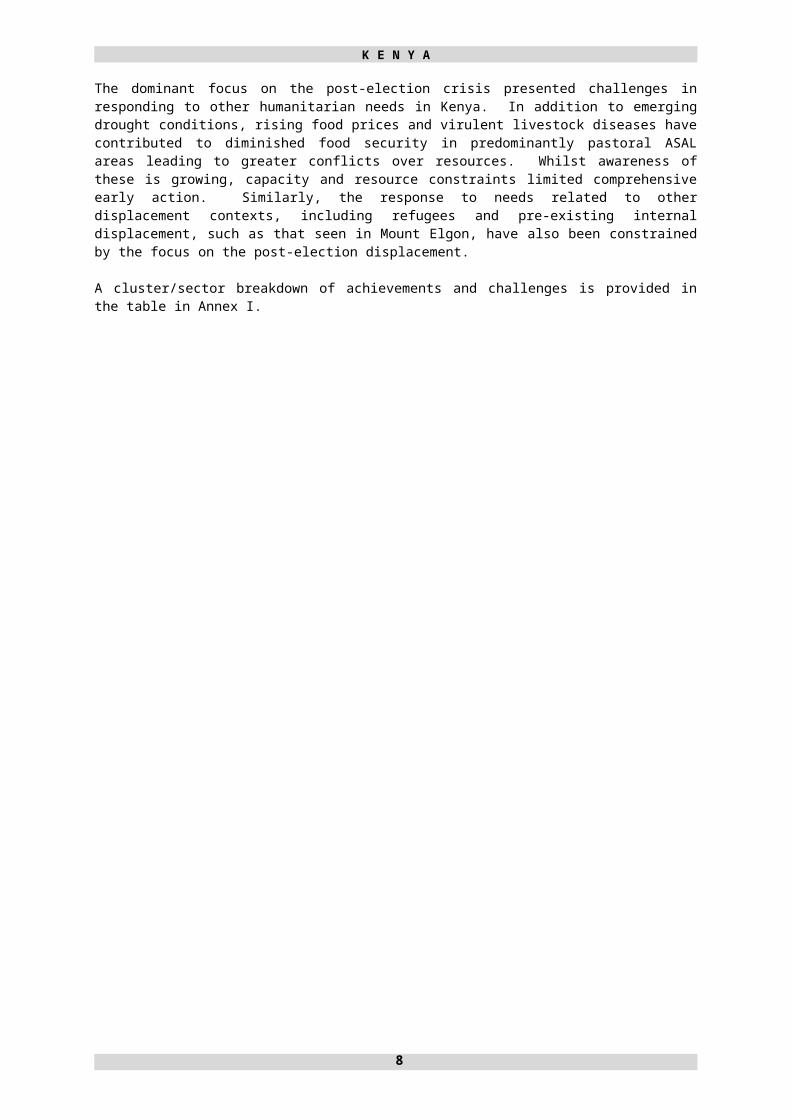
Heavy rains in parts of Turkana from 4 to 7 October caused flooding of the Turkwel River and the destruction of crops and livestock in Katilu division. An assessment undertaken by OCHA and KRCS on 15 October concluded that the floods caused serious damage to crops, and led to one confirmed death and 16 missing people. The loss of crops could worsen the food security of affected communities, which are highly dependant on crop production after insecurity/raids have impeded pastoralist livelihoods.
10
Collecting water in Tana River, 2008. © Julius Mwelu/IRIN

K E N Y A
The Tana River, which is the longest in the country, runs through Coast Province along the border with North Eastern Province. In June 2008, heavy rains caused flooding in Tana River District which resulted in the displacement of many families and submerged 3,000 acres, destroying crops and jeopardising livelihoods. In early August, the Tana River changed its course near Garsen Town after a farmer cut a channel to divert water for irrigation. The diversion is expected to cause massive flooding on the banks of the new river course during forthcoming rainy seasons. The population of the affected Tana River and Tana Delta districts is approximately 250,000, many of whom rely on fishing, irrigated farming or pastoralism, all of which have been affected by the diversion.
Nyando and Sondu Rivers in Budalangi District, Nyanza Province are also prone to periodic flooding, which affects thousands of households and could aggravate the spread of water-borne diseases in the region, including cholera outbreaks.
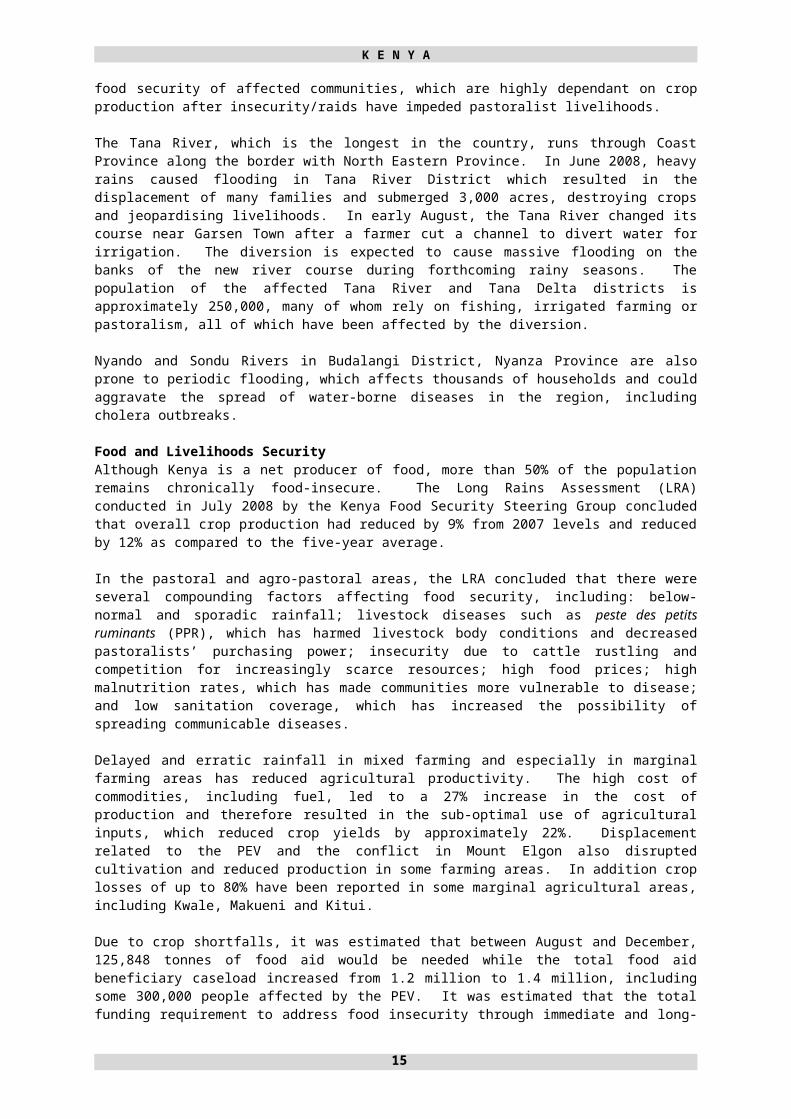
Food and Livelihoods Security Although Kenya is a net producer of food, more than 50% of the population remains chronically food-insecure. The Long Rains Assessment (LRA) conducted in July 2008 by the Kenya Food Security Steering Group concluded that overall crop production had reduced by 9% from 2007 levels and reduced by 12% as compared to the five-year average.
In the pastoral and agro-pastoral areas, the LRA concluded that there were several compounding factors affecting food security, including: below-normal and sporadic rainfall; livestock diseases such as peste des petits ruminants (PPR), which has harmed livestock body conditions and decreased pastoralists’ purchasing power; insecurity due to cattle rustling and competition for increasingly scarce resources; high food prices; high malnutrition rates, which has made communities more vulnerable to disease; and low sanitation coverage, which has increased the possibility of spreading communicable diseases.
Delayed and erratic rainfall in mixed farming and especially in marginal farming areas has reduced agricultural productivity. The high cost of commodities, including fuel, led to a 27% increase in the cost of production and therefore resulted in the sub-optimal use of agricultural inputs, which reduced crop yields by approximately 22%. Displacement related to the PEV and the conflict in Mount Elgon also disrupted cultivation and reduced production in some farming areas. In addition crop losses of up to 80% have been reported in some marginal agricultural areas, including Kwale, Makueni and Kitui.
Due to crop shortfalls, it was estimated that between August and December, 125,848 tonnes of food aid would be needed while the total food aid beneficiary caseload increased from 1.2 million to 1.4 million, including some 300,000 people affected by the PEV. It was estimated that the total funding requirement to address food insecurity through immediate and long-term solutions was $25.7 million, primarily in pastoral regions.
11

K E N Y A
FOOD SECURITY CLASSIFICATION BEFORE AND AFTER 2008 LONG RAINS
Before Long Rains
12

K E N Y A
After Long Rains
13

K E N Y A
According to the LRA, the Kenyan urban population accounts for about 13 million people, of which an estimated 7.6 million reside in slums. Overall nearly 40% of the urban sector falls into the highly insecure to extremely food-insecure category. Urban livelihoods are very diversified but the majority of income is derived from waged labour and petty business and almost all food and non-food requirements are met through the market. As a result, livelihoods are highly vulnerable to fluctuations, including price, production and labor shocks. According to analysis conducted by the Kenya Food Security Steering Group (KFSSG), rising food prices of up to 50% have led to further declines in food insecurity since wages have remained unchanged. Diet changes have been noted, with both a decline in frequency and in the quality/composition of meals.
Pastoral livelihoods and resource-based conflictsPastoral livelihoods have been affected by several factors in addition to the prevailing drought conditions. Livestock diseases, particularly PPR, have decimated small ruminant herds, including an estimated two million sheep and goats, since 2006. Because pastoralist households derive 40% of their nutrition from livestock meat and milk, declined herd sizes is jeopardising household food security. In addition, quarantine restrictions on livestock trade and movement as a result of contagious caprine pleuropneumonia (CCPP) and foot and mouth disease in Baringo and Samuburu districts have further damaged pastoral livelihoods. Livestock body conditions have deteriorated as herds have to walk further distances between water points and scarce pasture areas. Furthermore, livestock markets have declined due to the saturation of markets with distress livestock sales. Meanwhile, food and cereal prices have increased, resulting in a precipitous decline in pastoralists’ terms of trade.
A consequence of the deterioration of pastoralist livelihoods is the increasing frequency and intensity of raiding and resource-based conflicts in pastoral communities. Over 300 pastoralists have been killed in armed conflicts since January 2008 and over 15,000 people have been displaced from the Turkana districts alone. Competition for scarce resources, including water and pasture, has also led to clashes, particularly along the borders with Uganda, Southern Sudan and Somalia. The proliferation of small arms and light weapons has increased the number of casualties in clashes and has raised the stakes in retaliatory attacks.
There are over 700,000 food-insecure pastoralists and agro-pastoralists in the semi-arid Karamoja region of northeastern Uganda, which borders Kenya. The number of people in need of humanitarian assistance in Somalia is nearly 3.3 million—a 77% increase since January 2008. These highly vulnerable populations are likely to exacerbate competition for scarce resources along Kenya’s borders.
Health and NutritionKenya is prone to many diseases of epidemic potential, such as cholera, dysentery, rift valley fever, visceral leishmaniasis (Kala Azar), among others. Malaria remains the main cause of morbidity and
mortality, accounting for five percent of deaths in the country. Cases of cholera outbreak have been reported in parts of Nyanza, Western and Rift Valley Provinces and WHO reported that an outbreak of Kala Azar has affected more than 130 persons and killed nine people since April in Wajir and Isiolo districts.
Findings from recent nutritional surveys conducted between March and April 2008 in Mandera, Turkana, Marsabit, Samburu and Wajir districts indicate that the nutritional situation of the populations in the ASAL areas of Kenya is deteriorating and acute malnutrition rates are reaching entirely unacceptable levels. On average GAM is ranging between 20% and 25%. Caseloads of children being treated for severe acute malnutrition in health facilities are also rising in the urban poor areas.
There has been an overall decline in all health indicators following the PEV: vaccination coverage decreased from 77% to 66%; disease surveillance capacity declined from 74% to 35%; and many government health facilities
14
Turkana men armed with AK-47 rifles next to a water pump, northwestern Kenya, February 2007. Resource-based Conflicts are widespread and of increasing concern © Siegfried Modola/IRIN
A young child gets her weight measured in Tana River, Kenya 2008. © Julius Mwelu/IRIN

K E N Y A
are experiencing shortages of drugs, particularly anti-malarials and other essential supplies. There is also a shortage of health care workers, exacerbated by post-election displacement and insecurity.
Furthermore, a Kenya HIV/AIDS Indicator Survey concluded that the prevalence of HIV in Kenya is growing by more than a quarter percent per year and there are now nearly 1.5 million Kenyan living with HIV/AIDS, 70% of whom are in rural areas. However, the number of new cases has remained constant since July 2007. Low levels of awareness of HIV status and high risk behaviours could lead to increased numbers of infections: four out of five HIV-positive Kenyans are unaware of their status, while two thirds of Kenyans have never been tested for HIV. Frequent emergencies increase the risk of transmission and complicate prevention and treatment.
3.2 SCENARIOS Best-Case ScenarioUnder this scenario the security situation is expected to be good as a result of regional and national stability. The coalition government would remain intact and the peace building processes would continue with widespread support. These factors would therefore be expected to prompt social integration and successful return and resettlement of IDPs. In addition Kenyan citizens would participate fully in the legal reform processes that include constitutional, electoral as well as land reforms. These processes would be implemented, thereby addressing the provisions of the three agenda items of the National Accord and Reconciliation Act and Agenda Four that addresses root causes of the post-election violence.
The food security situation would improve due to better than expected climatic conditions as a result of favourable 2008 short rains and 2009 long rains. In turn, drought conditions, food insecurity and resource-based conflicts would be mitigated and regional agricultural crop and livestock production would improve. In terms of livestock, the best case scenario would see management of PPR and an improvement of livestock body condition due to a reduction in disease prevalence and improved access to water and pasture. Consequently this would lead to enhanced livelihoods and nutrition standards. Whilst some localised flooding is expected even under the best case scenario, other natural hazards such as earthquakes would not be present or would be very limited. Crop damage due to pests would be minimal while the presence of vector-borne diseases affecting livestock would not be devastating. In terms of preparedness, response plans would be drafted and humanitarian assistance would be pre-positioned. In addition, food and commodity prices would stabilise and would not contribute to further declines among vulnerable communities.
As a result of the above factors, no major new displacement would be envisioned and the humanitarian community would continue to provide support to existing IDPs. The process of developing a national IDP policy, as well as the Great Lakes IDP Protocol, would continue and a first draft of the same would be presented. In addition, the humanitarian community would draft and agree on a response framework to address needs in Mount. Elgon. In terms of refugees, under this scenario, the Kenya-Somali border would be reopened and sporadic access into Somalia would be possible. The political situation in Somalia would improve resulting in the reduced flow of refugees into the country and Dadaab camps. Humanitarian programmes in Dadaab camps would continue. Kakuma camp would continue to empty as refugees continue to return to their original countries. In addition, new adequate land for expansion of refugee sites would be allocated by the Government of Kenya to accommodate any influx of new asylum seekers/refugees and decongest existing refugee sites.
Worst-Case ScenarioUnder a worst case scenario, divisions within the coalition government would lead to political unrest and a resurgence in violence and ethnic division. None of the Commissions’ recommendations would be adopted and peace and reconciliation efforts would be poorly implemented, further aggravating the likelihood of a relapse into conflict at all levels and leading to large-scale displacement. Economically, a worst case scenario would see a downward decline in economic growth and further rapid escalations in food and commodity prices. In turn, increased unemployment would intensify poverty and vulnerability, including for the urban poor.
In terms of climatic conditions there would be a continued failure of the rains and an increased global food crisis leading to growing food insecurity and a worsening of drought conditions. The PPR outbreak would escalate, further spreading into new districts. Deterioration in livelihoods and nutritional status would be expected. The situation would be compounded by flooding in some parts of
15

K E N Y A
the country. Competition for resources would be expected to increase resource-based conflict, including at border areas. Continued conflict in Mount Elgon and Molo would result in greater loss of livelihoods while continued displacement and evictions from Mau forest would contribute to new population displacements.
A worsening in the situation in Somalia would cause an increased refugee influx into Kenya with 46,000 new Somali refugees arriving from January to September 2008, further overextending refugee camps. Additional influxes would heighten the risk of disease outbreaks such as measles and polio and cause higher mortality and morbidity within camp settings. No additional land is allocated to decongest already overcrowded camps or to accommodate new asylum seeker/refugee arrivals, causing a humanitarian crisis and leading to local community conflicts due to overflowing population and dwindling resources.
Overall this situation would be expected to be accompanied by decreasing access to basic needs and services and an attendant decrease in overall health indicators, higher HIV/AIDS prevalence and increased human rights violations and GBV.
Most Likely ScenarioUnder the most likely scenario, the political situation would be expected to remain stable with no major changes in 2009. Conditions would allow for some continued return of post-election IDPs although trends towards transit and satellite camps would be expected to persist. In addition peace and reconciliation efforts would continue although unresolved tensions would persist in some areas. Displacement and humanitarian needs would also continue in the Mount Elgon, Molo and Nakuru areas.
Regardless of the performance of the current short rains season, drought conditions would be expected to remain in some of the ASAL areas – particularly in northwestern and northeastern Kenya. A combination of drought, floods in some areas, high food and commodity prices, and a prevalence of livestock diseases, including PPR, would contribute to continued food and livelihood insecurity for some pastoral and agro-pastoral communities. The competition for already scarce resource would also be expected to contribute to continued resource-based conflicts, leading to further deaths and displacements. The effect of rising food prices would also be expected to increase vulnerability among the urban poor as access to food and other basic needs would be reduced. These factors would be expected to lead to an increase in malnutrition rates and consequently morbidity and mortality.
In relation to refugees, it would be expected that the ongoing crisis in Somalia would contribute to new refugee arrivals. This would further strain capacities within existing camps as well as within communities in neighbouring areas of northeastern Kenya. Drought conditions and declining availability of pasture and water in the region would also be expected to create continued cross-border movements. Limited, but inadequate, land would be allocated to accommodate new influxes of asylum seekers/refugees and to partially decongest existing refugee camps. Limited land allocation may lead to increased levels of resource-related conflicts amongst refugees, as well as with local communities.
3.3 STRATEGIC OBJECTIVES FOR HUMANITARIAN RESPONSE IN 2009 Humanitarian partners have worked together to develop a common humanitarian strategy based on the analysis of the context, humanitarian needs and projected scenarios for the coming year. As a basis for the specific sector response plans, overarching strategic priorities have been identified in order to support effective and timely humanitarian assistance to populations in need in Kenya.
The overall strategic objectives for 2009 are to ensure that: timely, coordinated humanitarian assistance and protection is provided to highly vulnerable
populations affected by natural and man-made disasters in accordance with internationally accepted norms and standards;
early recovery initiatives are linked with longer-term programming to reduce vulnerability and strengthen resilience among vulnerable populations;
16
A group of newly arrived Somali women and children wait to be registered at Dadaab refugee camp, Kenya, October 2008 © Manoocher Deghati/IRIN
K E N Y A
strong linkages with conflict mitigation, peace building and reconciliation initiatives are integrated within humanitarian action;
the capacity of national institutions and networks is strengthened to enhance coordination, undertake humanitarian policy development, and promote effective emergency preparedness and disaster risk reduction.
3.4 CLUSTER/SECTOR RESPONSE PLANS
3.4.1 Coordination
Cluster lead: OCHA (in support of the Humanitarian Coordinator)
Overview of priority needs and response strategyIn January 2008, humanitarian partners and government counterparts agreed to organise humanitarian activities around 11 sectors under the cluster approach. It was agreed that existing sectoral working groups would be integrated within this structure. In August, humanitarian partners met to discuss the ongoing operation of the clusters in light of the chronic nature of the post-election violence situation and the need for a more inclusive response to other humanitarian situations in the country. The subsequent recommendations highlighted the necessity for clusters to increase their focus on strengthening and transitioning to national sectoral coordination mechanisms. In some cases – such as water and sanitation and GBV – these transitions are already underway. In others, cluster members are in the initial stages of partnership building with national counterparts. The recommendations also highlighted the need to focus beyond the issues and sectors related to the post-election violence to include drought, food and livelihood insecurity, urban vulnerability and refugees.
In relation to food security, the KFSM and the KFSSG continue to take the lead role in coordination under the leadership of the Government of Kenya and UN agency and NGO participation. In the coming year humanitarian partners will continue to collaborate around the issues of food and livelihood security through the monthly KFSM meetings and participation in joint assessments and complementary programming.
Inter-sectoral coordination has continued throughout the course of 2008 at a decision making level through the IASC and the Stakeholders Meeting chaired by the MoSSP and at a technical level through inter-cluster meetings and the Kenya Humanitarian Forum. These fora will continue as the main arenas for coordination at the national level in 2009.
At the district level, operational hubs were established in Eldoret, Nakuru and Kisumu during the post-election crisis. Whilst many agencies and NGOs have now decreased their field presence in PEV-affected areas, inter-sector coordination continues with local authorities and, in the case of Eldoret and Nakuru, with the support of OCHA. In the coming year, the focus of coordination at the field level is expected to expand to ensure greater coverage of ASAL areas and other areas affected by localised conflicts or natural disasters. Priorities for coordination at the field level also include support to national coordination mechanisms.
Objectives Ensure effective and inclusive coordination at technical and decision making levels. Strengthen national coordination capacity at centralised and sub-national levels. Strengthen preparedness activities, including inter-agency contingency planning. Ensure the information needs of the humanitarian community are met. Raise awareness and mobilise effective humanitarian action.
Indicators Inter-agency coordination mechanisms continue to be effectively supported. Increasing number of clusters transition to national coordination structures. Humanitarian website maintained and regularly updated with relevant information. Regular reporting. Multi-hazard contingency plan in place and regularly reviewed. Inter-agency advocacy strategy developed and implemented. More than 60%of funds requested through the EHRP received and 100% CERF applications
approved.Activities
17

K E N Y A
Facilitate the ongoing role of the IASC. Work with clusters to ensure an effective and timely humanitarian response and the
development of preparedness plans. Provide support for national coordination mechanisms. Undertake multi-hazard inter-agency contingency planning for Kenya. Maintain and develop information products and mechanisms to meet the information
management needs of the humanitarian community. Support resource mobilisation through the development of inter-agency appeals and the
coordination of CERF applications. Explore other opportunities for resource mobilisation. Facilitate inter-agency advocacy through the advocacy working group and the development of
appropriate advocacy strategies.
Monitoring Coordination activities will be monitored through formal and informal mechanisms including through periodic reviews of the EHRP and the mid-year review process. Regular consultations will be held with humanitarian partners, including the humanitarian coordinator, cluster leads, IASC members, Government partners and donors, to identify coordination needs.
3.4.2 Early Recovery and Food Security
Cluster leads: UNDP (early recovery) and FAO (food security)
Agencies participating: UNDP (co-lead); FAO (co-lead); OCHA; ACCORD; WV Kenya; UNHCR; Agency for Cooperation and Research in Development (ACORD); International Rescue Committee (IRC); Danish Refugee Council (DRC); Action Aid; PeaceNet; Catholic Relief Services (CRS); Oxfam GB; CARE International; Save the Children; Catholic Agency for Overseas Development (CAFOD); Kenya Episcopal Conference Catholic Church Secretariat; International Medical Corp (IMC); Action Against Hunger (ACF); United Nations Industrial Development Organization (UNIDO); UNICEF; United Nations Development Fund for Women (UNIFEM); United Nations Volunteers (UNV); Caritas Kenya; Christian Aid; Concern Worldwide; CORDAID; Italian Corporation; German Agro Action (GAA); IOM; Dutch Ministry of Foreign Affairs; Ministry of State for Special Programmes; National Council of Churches of Kenya; National Empowerment of Deaf Kenya; National Steering Committee on Peace Building & Conflict Management (NSC); Pact Kenya; Safer World; Solidarités; Aide Humaine d' Urgence; World Concern; United States Agency for International Development (USAID); Engender Health; WFP; Church World Service and United Nations Population Fund (UNFPA).
Overview of priority needs and response strategyThe Early Recovery and Food Security Cluster will continue to focus on the priority areas, which were identified following the PEV, namely peace and reconciliation; governance and rule of law; access and delivery of basic services; agricultural and non-agricultural livelihoods; and mainstreaming of cross-cutting issues. These areas are still of great relevance and significance in 2009. Despite the progress made to restore some degree of normality and peace following the 2008 violence, the task of ameliorating the effects of the crisis remains enormous. As of October, the Government of Kenya estimated there were less than 10,000 people IDPs living in IDP camps and an estimated 54,000 to 75,000 IDPs living in transit camps. In addition, the impending drought in the arid and semi-arid regions has created worsening food conditions. Among the priority issues that need to be addressed by all stakeholders include: the challenges of reconciling the nation and building lasting peace; restoration of livelihoods of the affected communities and individuals; and enhancing food security.
18
IDPs relocating from Eldoret ASK IDP camp to Yamumbi Transit Site.Photo by OCHA. October 2008.

K E N Y A
Peace and ReconciliationAlthough a political settlement to end the violence was reached with the signature of the National Accord and Reconciliation Act (NARA) in February 2008, the peace has not as yet completely permeated the fabric of society at the community-level. In the absence of the National Policy on Peacebuilding and Conflict Management, there is no national framework to deal with peace and reconciliation activities in a coordinated manner. District Peace Committees (DPCs) need support to be well-established and adequately resourced to carry out their duties. Due to the critical nature of peace as a prerequisite for development as well as to reduce the likelihood of further conflict, it is critical to integrate peacebuilding and reconciliation activities into all humanitarian and reconstruction actions in communities affected by the post-election violence and also those affected by resource-based conflict.
LivelihoodsThe post-election violence had an extremely negative impact on the economy at large and, by extension, on livelihoods. The impact of the violence included: destruction of business premises; KSh 90 billion lost in micro and small enterprises; 66,515 farm families affected; destruction of the main staple, maize (estimated at 2.5 million bags) and other crops in stores; loss of seed, fertilizer and farm machinery estimated at KSh.3.4 billion; 4,000 fishers lost fishing equipment; and average asset loss per household of Kh.261,655.9 Further analysis is required to provide disaggregated data indicating numbers of affected men, women, and vulnerable groups such as people with disabilities (PWDs) and people living with HIV/AIDS, to better-tailor intervention strategies. There is also the need to adopt a strategy of livelihoods diversification, which would reduce conflict due to limited resources, and strengthen partnerships and linkages with HIV actors and community support networks for livelihoods programming. These actions need to be tailored to address both agricultural and non-agricultural livelihoods.
Food SecurityAlthough the global rise in food prices was expected to benefit households that were net sellers of agricultural produce, the post-election violence, increasing fuel prices, high input prices, the poorly distributed rainfall during the long rains of 2008 and the persistent drought have impacted negatively on agricultural production, resulting in very few net sellers. There are approximately 1.38 million people rated as highly food-insecure who, without assistance, will be unable to meet their minimum food requirements by March 2009.10 About 46% of the 35 million Kenyans live below poverty levels. Welfare monitoring reports by Kenya’s National Bureau of Statistics indicates that, on average, the rural and urban communities spend 62% and 40% of their total income on food, respectively. The prices of staple foods, especially maize and beans have increased by between 32% and 80% in the last six months in different regions, with the greatest increases in rural farming areas.11 Low production, together with increasing food prices, will result in the rural and urban vulnerable population not being able to access food, a situation which may consequently lead to hunger and malnutrition, possibly provoking food riots. Strategic actions include provision of water for both household and livestock needs; provision of fast-maturing and drought-tolerant seed crop varieties; strengthening partnerships and linkages with HIV actors and community support networks for food security programming; and addressing livelihoods incorporating peace building.
Objectives1. To support national and community-based peace and reconciliation initiatives to facilitate the
return and reintegration of displaced persons. 2. To enhance livelihood opportunities for vulnerable populations, including those in areas affected
by post-election violence and in food-insecure regions, particularly in the ASAL. 3. To provide quality and appropriate inputs to contribute to the food security of vulnerable farming
households through crop production during the long rains of March and the short rains of October 2009.
4. To harmonise disaster preparedness and disaster response plans, particularly at the community level.
Indicators Increased number of returnees returning to settle on their farms. Number of active and effective District Peace Committees.
9 Source: Tegemeo Institute of Agricultural Policy and Development (2008), Effects of Post-Election Violence in Kenya on Agriculture. 10 Source: KFFSG Long Rains Assessment Report, 2008. 11 Ibid.
19
K E N Y A
Enhanced livelihood opportunities for displaced persons and affected communities in food-insecure areas.
Community support mechanisms established to assist vulnerable persons in the rehabilitation/reconstruction of sustainable livelihoods.
Enhanced and diversified livelihoods for pastoralist and sedentary communities in ASAL. Increased productivity of food crops on farm holdings as a result of increased use of yield-
enhancing inputs, including irrigation water. Enhanced access to food. Partially stabilised food prices in project areas. Most affected farmers are able to cultivate their land. Harmonised disaster preparedness and disaster response mechanisms established at the
community level, which take into account climatic changes.
Activities Engage communities in peacebuilding and reconciliation activities and inter-communal dialogue. Training of District Peace Committee members. Creation of linkages and synergies among peace actors at the community level. Documentation and dissemination of best practices in community peacebuilding initiatives. Documentation and dissemination of best practices in livelihoods actions. Collection of qualitative and quantitative disaggregated data to enhance tailoring of livelihoods
actions. Skills development training. Facilitation of access to credit and entrepreneurial opportunities. Identification and sensitisation of households vulnerable to food insecurity. Agricultural input procurement and distribution. Provision of agricultural inputs and implements to affected communities. Training in diversified and alternative farming methods. Assistance to vulnerable households to enhance and protect livestock assets. Impact assessments. Support to disaster preparedness, mitigation and management by assisting the development of
contingency plans. Awareness-raising on disaster preparedness and climatic changes. Building the capacity of local governments to respond to disasters through provision of technical
assistance. Assisting with the establishment of disaster management sub-committees.
Monitoring As co-leads, UNDP and FAO will be responsible for early recovery and food security sector coordination and monitoring through the following methods: Monthly meetings with stakeholders to advocate and share information; Mapping of early recovery and food security activities (to be accessible online on the 3Ws
OCHA database) and creating a GIS map to facilitate the identification of gaps and duplication in programming. The findings of this exercise will be disseminated and discussed on a periodic basis at the monthly forum for enhanced coordination of activities, as well as disseminated among actors at the community level;
Quarterly peer review field visits to conduct impact assessments; Final one-day stakeholders’ annual review.
3.4.3 Education
Cluster lead: UNICEF
Agencies participating: UNICEF, MoE, The Association of Volunteers in International Service (AVSI), CISP, SC-UK, World Friends - Kenya, UNFPA, Gender Commission
Overview of priority needs and response strategyThe strategic priorities of the education cluster in 2009 are that all school-aged children (pre-primary, primary and secondary) have access to quality and relevant education opportunities, in a safe learning environment that promotes the protection and mental and emotional well-being of learners.
20

K E N Y A
The gaps identified by the Education Cluster are as follow: School feeding programme
Low attendance rates in the afternoons, especially amongst IDP children, are being reported. Reduced levels of school attendance are being linked with the lack of provision of food in schools. WFP has reported that due to increasing food prices and shortage/difficulties with supplies, there are currently problems in filling the needs.
Protection (SGBV and tracking of children). The Education Cluster set up a strong synergy with the two sub-clusters to have a common strategy to respond to this gap.
Youth There is an urgent need to address youth issues in Kenya; notably, the number of youth taking part in the violence after the 2007 general elections was alarming. Youths were perceived to have been strongly involved and their vulnerability was “used” to reinforce the violence. It is therefore important to equip these youth with life skills and other practical skills to reinforce positive development.
WASH improvement in the provision of latrines and water points at school level. Early Childhood Development (ECD) - training for the ECD teachers, provision of more
material, improve physical structures. Psychosocial support for children and teachers (above all for the teenagers that, as reported
by secondary school directors, have shown the biggest problems with post-traumatic stress disorder).
Capacity-building is needed for the district education officers, teachers, head teachers, school directors and also for the humanitarian staff, to better identify and respond to the needs of the beneficiaries.
The needs identified are the following: Tents; Educational material for primary schools; ECD kits; Educational material for secondary schools; Recreational kits; Peace and reconciliation training sessions; Textbooks and exercise books.
Proposed coverage (UNICEF in all the areas)
SITE / AREA ORGANISATIONSTana River CISPMalindi District CISPNairobi CISP, World Friends - Kenya, AVSIEast Pokot (Balpelo) AVSINyandarua AVSIYala-Siaya (Nyanza) AVSIKajiado (Rift Valley) AVSIEldoret (Koibatek) CISP, AVSINakuru (Naivasha, Molo and Nakuru) SCUKUasin Gishu/Transzoia CISP SC-UKNarok CISP, AVSIBurnt Forest SC-UKMandera SC-UKDadaab CISP, SC-UK
Objectives1. To ensure access and retention of ECD and primary school-aged children in quality and
protective learning environments.2. To provide appropriate learning opportunities to secondary school-aged children affected by
the emergency.3. To ensure equity in educational opportunities to marginalised, vulnerable and excluded
children affected by the emergency.4. To strengthen the capacity of key education stakeholders at all levels in emergency
preparedness planning and management.
21
Children in a crowded class at the Moto primary school, Molo town, Rift Valley Province, February 2008. © Allan Gichigi/IRIN

K E N Y A
5. To ensure psychosocial and emotional well-being of children through peace education, conflict management and psychosocial support.
Indicators 50% of affected ECD children and 70% of affected primary school-aged children have access to
quality education. 30% of affected secondary school-aged children are provided with appropriate learning
opportunities. School enrolment reflects the population make-up of orphans and vulnerable children (OVC)
and marginalised and excluded children. The emergency and preparedness response plan is ready and disseminated at the district level
and all the education cluster members have developed their respective contingency plans. All enrolled children benefit from peace education, conflict management and/or psychosocial
support.
Activities Rehabilitation and construction/reconstruction of learner friendly education facilities, including
adequate WASH facilities (gender appropriate). Provision of necessary NFIs for girls and vulnerable groups to increase enrolment. Provision of teaching and learning materials, as well as uniforms, ECD kits, educational kits,
and recreational kits. Provision of feeding programmes. Back-to-school campaign, including child-to-child and community support. Provision of short-term teacher training on child-centred teaching methodologies, psychosocial
issues, HIV, inclusion, gender and protection issues, subject matters, etc. Strengthening of the School Management Committees (PTAs), Administrators and Head
Teachers for ECDs, primary and secondary schools in the affected areas with a gender equity component.
Community awareness-raising and mobilisation for provision and monitoring of quality education for all to encourage inclusion of affected and excluded children and ensure the attendance of girls, vulnerable and marginalised children and children with special educational needs.
Short skills training, vocational training, and literacy and numeracy skills for youth. Establishment of recreational and social activities for youth for psychosocial and emotional well-
being and inter-community peace building. Facilitation of teacher recruitment and placement. Provision of incentives to attract quality female and male teachers. Capacity-building of local authorities and MoE representatives in emergency education planning
and management. Strengthening of Environmental Management Information System (EMIS) to include data
collection to reflect marginalised, vulnerable and excluded children. Provision of psychosocial support to children and youth. Provision of peace education activities. Establishment of strong networks between communities and schools to build support and
reporting linkages for the well-being of the child.
MonitoringThe monitoring of the activities/indicators/objectives will be ensured through the analysis of monthly reports and monthly quantitative data formats filled out by the implementing partners, as well as through systematic field visits by UNICEF and MoE partners.
Quality assessments will be conducted at the field level by UNICEF and MoE partners. In the sector of emergency education, the focus will be placed on teacher training, activities with students, utilisation of distributed materials, and in strengthening the response’s capacity of the stakeholders. A plan of regular field visits/M&E will be developed for 2009.
The monthly education cluster meeting, under the umbrella of the MoE and with the participation of NGO implementing partners and UN agencies, will provide timely feedback on education project ongoing activities.
Areas Category Affected population
Beneficiary population (school-aged children)
ASAL areas, Trans Zoia, Garissa, Wajir, Mandera,
IDPs in PEV-affected areas in camps still functioning
10,000 3,500
22

K E N Y A
Tana River, North and South rift Valley, Nairobi
IDPs still in transit camps 75,000 26,250Returnees in PEV-affected areas 238,000 83,300
IDPs in Mount Elgon 45,000 15,750Refugees from Somalia 213,000 77,000Children in flood-affected areas 250,000 87,500
Children in drought-affected areas 870,000 300,000*
Grand total 1,701,000 593,300* As per 2007
3.4.4 Food Aid and Nutrition
Sector leads: UNICEF (nutrition) and WFP (food)
Agencies participating: WHO, Action Aid, COCOP, KRCS, Oxfam, WV, Samaritans Purse (SP), Action Against Hunger (AAH), Islamic Relief (IR), Merlin, International Medical Corps (IMC), SC, Food for the Hungry (FFH) Kenya, Concern Worldwide, Path Finder, AMPATH, Family Health International.
Overview of priority needs and response strategy:The number of people living under the food poverty line has increased sharply over the last six months. It is estimated that six million people in Kenya could be at risk of not being able to meet their food consumption needs in 2008-2009. The most affected areas are the ASAL, the areas affected by the post-election crisis, and more recently, the urban poor areas (due to rising food and fuel prices).
The nutritional situation of young children and women has deteriorated in most parts of the country. Nutritional surveys conducted in the ASALs in April 2008 showed that levels of GAM have significantly risen, with rates between 20% and 25% (weight-for-height, z-scores). Turkana District has been the most affected where levels of GAM rose from 14.3% in April 2007 to 22.5% in April 2008, while severe acute malnutrition rose from 1.2% to 3.5%. Also, the Long Rain Assessment (LRA) findings indicated, in July 2008, an overall deterioration of the food and livelihood situation in ASAL with Turkana District, as well as some divisions in Marsabit and Samburu Districts, being at high risk of falling into a humanitarian crisis. Partners have reported a steady increase in the number of children being treated for severe acute malnutrition since March this year and a deterioration of households’ food consumption in urban poor areas. Finally, newly resettled populations in the PEV-affected areas are still facing great challenges in accessing basic social services which will directly affect their overall health and nutrition status.
As a result of the above, the number of Kenyans relying on food aid increased from 652,000 in 2007 to 1,028,000 in 2008. The number of children and mothers affected by acute malnutrition is expected to rise further if the current trends are not addressed with timely food and nutrition actions that are linked to other key sector actions, i.e. health, food security, water and sanitation. With malnutrition as an underlying factor in more than a third of all child deaths, substantial breakthroughs in improving child nutrition are essential.
WFP has been providing food assistance to the most affected populations (i.e. pastoralists, agro-pastoralists and marginal agriculturalists) to protect households from further deterioration and help them to recover from shocks. The food sector will continue to combine general food distribution to the most vulnerable households and food-for-assets for households with active members to create lasting assets and increase resilience to future shocks, such as natural disasters and rising food prices. This will be achieved through social, technical and capital support from partners (i.e. NGOs, CBOs, Government, FAO, private sector) and with strong links to ongoing safety-net programmes. In addition, WFP will work towards enhancing community and Government capacity to design, manage and implement programmes geared towards reducing hunger, while ensuring flexibility and preparedness to expand its operation to respond to future crises.
23
WFP food distribution at Woodley Stadium, Kibera Nairobi – January 08

K E N Y A
Targeting of food aid beneficiaries is carried out at two levels: geographical—through twice-yearly food security assessments, and beneficiary targeting by communities, following the “Community-Based Targeting Guidelines”. Targeting criteria used by communities include gender-related criteria, such as single-mother households, poor family health, poor child health, lack of assets, and income. Community-Based Targeting Guidelines promote the participation of women in relief committees (at least 50% female members) and encourage women to manage food aid both at community and household level. According to the post-distribution monitoring, some 70%-80% of beneficiary households assisted under the emergency operation (EMOP) are female-headed.
Nutrition partners have commenced comprehensive and integrated nutrition actions with an aim to address short-term needs (i.e. life-saving actions) while focusing on building preparedness capacity in crisis-prone areas. However, despite various and ongoing initiatives to strengthen the systems, the MoH’s capacity to address the growing burden of malnutrition remains very low. Therefore, the overall strategy for the nutrition sector will be to support the MoH and partners to improve their capacity to deliver essential nutrition services (i.e. growth monitoring, management of acute malnutrition, micronutrient supplementations, protection and support to infant feeding practices). In addition, partners will focus on strengthening nutrition surveillance and support coordination mechanisms. Technical and logistical support will be provided at the health facility and community levels. Scale-up of outreach activities will particularly be required in the post-election affected areas. The response will be primarily undertaken through the MoH, with full support of WFP, UNICEF and implementing partners. A common operational framework is being developed with partners to support the sector plan.
The approach will contribute to preventing and addressing acute malnutrition and avert excess associated morbidities and mortalities.
Site/Area OrganisationsASAL General Food Distribution (GFD): KRCS, Action Aid, COCOP, WV, Oxfam,
WFPFood for Asset: WV, WFP Nutrition: IR, SC-UK, Merlin, SP, Freedom from Hunger (FFH), WV, AAH, WFP
Post-election crisis areas GFD: KRCS, WFPNutrition: SP, Merlin, IMC, Concern Worldwide, Academic Model for Prevention and Treatment of HIV/AIDS (AMPATH), Family Health International (FHI), WFP
Urban Poor Nutrition: Concern Worldwide, Path Finder
Objectives1. Stabilise and reduce vulnerability to hunger resulting from shocks (e.g. climatic disasters,
rising food prices).2. Ensure that essential nutrition services are delivered to affected populations.3. Ensure that efficient coordination mechanisms are in place at national and sub-national levels.4. Maintain efficient nutrition surveillance systems.
Indicators Impact: Percentage reduction in acute malnutrition rates in affected areas. Percentage of households reporting improved dietary diversity score.
Process1. Percentage of households accessing adequate food rations, of which % female-headed. 2. Number and type of assets utilised by target beneficiaries, of which % utilised by women. 3. Percentage of health facilities offering essential nutrition services, as per standards. 4. Percentage of health facilities offering maternity services certified as baby-friendly.5. Number of districts/provinces with functioning coordination structures led by the MoH.6. Number of districts/provinces providing timely surveillance/monitoring reports.
Activities1. Distribution of food and non-food items in sufficient quantities and quality to targeted
populations.2. Food-for-assets to enhance resilience to shocks.
24

K E N Y A
3. Provision of food commodities and logistics support for GFD, food-for-assets (FFA) and school-feeding programme (SFP).
4. Capacity development for managing acute malnutrition and supporting/protecting infant and young child feeding practices.
5. Technical and logistical support for diagnosis of acute malnutrition and referrals for adequate management at health facility and community levels.
6. Technical, logistical and human resource support to ensure adequate diagnosis and management of acute malnutrition, protection and promotion of infant and young-child feeding practices as well as routine and curative micronutrient supplementation for young children and women, including those affected by HIV/AIDS.
7. Communication of key messages at health facility and community levels to promote positive caring practices.
8. Support for improved coordination mechanisms and link with other sectors at both national and sub-national levels.
9. Monitoring, surveillance and assessment of households’ food and nutrition security. 10. Provision of essential supplies, including anthropometric equipment, feeding kits, therapeutic
and supplementary foods and micronutrients.
Monitoring Monitoring of the proposed actions will essentially be ensured through: 1) regular field visits from partners’ officers and project coordinators; 2) joint monitoring and evaluation assessments with partners; 3) nutrition assessment; 4) WFP monthly distribution and post-distribution monitoring activities; 5) monthly reports from health facilities; and, 6) activity reports from implementing partners.
Areas Category Beneficiary populationASAL Drought-affected populations
(including 105,000 children under five and 33,000 pregnant and lactating women)
1,057,000
Areas of Displacement IDPs 165,750Children under-five 15,750Pregnant and lactating women 22,500
Urban poor Children under-five 21,000Pregnant and lactating women 45,000
TOTAL12 1,327,000
3.4.5 Health
Cluster lead: WHO
Agencies participating: WHO, IOM, MoH, Provincial Health Teams, District Health Teams (DHT), MERLIN, IRC, Deutsche Gesellschaft für Technische Zusammenarbeit (GTZ), Health NGO Network (HENNET) HENNET Members and faith-based organisations (FBOs), UNICEF.
Health cluster members/partnersThere are over 120 active health cluster humanitarian partners in Kenya. Members include the MoPSS, Medical Care Services, UN agencies, international and local NGOs and community based organisations (CBOs). WHO is the cluster lead for health in Kenya, and has one sub-office in Garissa, North Eastern Province, and is being called upon by the Government and partners to establish another one in the western part of the country. During emergencies, the cluster lead also collaborates with WHO Somalia and partners in Somalia.
Overview of priority needs and response strategyKenya has been experiencing various natural and human disasters such as drought, floods, civil strife and mass displacement of people, disease outbreaks (Rift Valley Fever, acute watery diarrhoea cholera, Kala Azar as well as acute flaccid paralysis), earth tremors and landslides. These situations have severe public health consequences, causing mass morbidity, mortality, disability and psychosocial trauma. The fundamental emergency life-saving infrastructure and systems, especially for provision of basic and primary health care services, are consequently also affected.
12 WFP is currently providing food assistance for some 211,000 beneficiaries who were affected by the post-election violence but expects a reduction in 2009. This figure does not include the estimated 337,000 Somali and Sudanese refugees who will receive food aid in 2009. A separate project to address their needs is included under Multi-Sector.
25

IDSR NATIONAL REPORTING RATE JAN 2006-MARCH 2008
0
10
20
30
40
50
60
70
80
90
1/8/
2006
2/8/
2006
3/8/
2006
4/8/
2006
5/8/
2006
6/8/
2006
7/8/
2006
8/8/
2006
9/8/
2006
10/8
/200
6
11/8
/200
6
12/8
/200
6
1/8/
2007
2/8/
2007
3/8/
2007
4/8/
2007
5/8/
2007
6/8/
2007
7/8/
2007
8/8/
2007
9/8/
2007
10/8
/200
7
11/8
/200
7
12/8
/200
7
1/8/
2008
2/8/
2008
3/8/
2008
WEEK ENDING
REPO
RTI
NG
RA
TE
1st Weekly reports received
1st Weekly Feedback bulletin
Post Election Violence
K E N Y A
Disease OutbreaksSince the beginning of 2008 there have been cholera outbreaks in Nyanza, western North Eastern, Rift Valley and Coast Provinces, as well as Kala Azar in North Eastern, Eastern and Rift Valley Provinces. By end of July 2008, 2,166 cases of cholera with 83 deaths (cfr = 3.8%) and 174 cases of Kala Azar and nine deaths (cfr = 5.2%) were recorded. There is a risk of meningitis outbreaks in the northern parts of the country which lie in the meningitis belt. Kenya also has a generalised HIV epidemic (prevalence rate of 7.8%), hence the impact of disasters on HIV transmission and service continuity during disasters is significant.
Effect of PEV on health sectorThe post-election violence which gripped the country for the first months of 2008 significantly disrupted most of the existing emergency primary health care structures and services. WHO and the MoH conducted rapid assessments on the health system in May 2008. This assessment showed that most of the emergency health and life-saving indicators had declined. For example, the national immunisation coverage for the fully immunised dropped to 65% by end of March 2008 from 79% reported in March 2007. The weekly disease surveillance reporting rate also fell from 80% in late 2007 to 40% by March 2008, focused ante-natal care and family planning services offered in health facilities dropped by 17% and 12%, respectively, and TB case notification rate also dropped by 12%. The fundamental emergency life-saving infrastructure and systems especially for basic and primary health care services, such as health human resources, supply and replenishment of essential drugs, reagents for laboratories and consumables, were also affected. Health care workers themselves have been displaced and many are also in need of psychosocial support. Addressing these numerous challenges requires additional logistical and other efforts.
* Integrated Disease Surveillance and Reporting.
Food crisis and healthWhile Kenya is facing problems associated with the food crisis and food insecurity, levels of acute malnutrition have significantly risen in the past few months. The population at risk for food insecurity is approximately 3.8 million - up to 95,000 children under-five and pregnant and lactating women are currently receiving food supplementation. Surveys conducted between March and April 2008 in eight districts indicated nutritional levels of between 20 and 29.8% GAM whilst severe acute malnutrition (SAM) was between 1.2% to 3.5%. The food price crisis has an important impact on health as diminished access to foods results in acute and chronic malnutrition among vulnerable groups and affects morbidity and mortality by aggravating infectious diseases. People living with HIV/AIDS or TB are especially vulnerable to the effects of diminished access to food.
Also, the capacity of partners and MoH to diagnose malnutrition is poor and most health facilities have not been trained to effectively handle severe malnutrition. Having a poor health infrastructure and
26

K E N Y A
being situated in an epidemic zone, the risk for concurrent disease outbreaks in 2009 is extremely high.
RefugeesThe humanitarian community in Kenya cannot lose sight of the needs of over 217,000 refugees in Dadaab and 50,000 in Kakuma and their host communities in the northern parts of the country. With deterioration in the security and political insecurity in Somalia, more refugees are expected before the end of the year and in 2009. The fragile health infrastructure in the camps and in host communities may collapse if resources are not made available.
Cross border health issuesCross-border emergency health issues in the Horn of Africa and Kenya in particular, have become a serious concern. All major disease outbreaks such as cholera, Rift Valley Fever, poliomyelitis and Kala Azar occur concurrently along the Kenya’s bordering neighbouring areas. Somalia, southern Ethiopia, northern Uganda and southern Sudan all have poor health infrastructures and pose serious public health challenges for cross-border cooperation and emergency health response.
Overall objectiveContribute to reducing avoidable morbidity and mortality among the vulnerable and mobile populations facing emergency situations in the country.
Specific objectives1. Provide life-saving emergency basic health care package to target vulnerable populations,
including pregnant and lactating women, in emergency settings for 30 districts and four provinces in areas with a high concentration of IDPs, refugee camps and drought-affected areas.
2. Provide life-saving emergency secondary care package, including psychosocial assistance to target vulnerable populations (HIV, TB, non-communicable diseases, reproductive health care, psychosocial for health workers and facility-based patients, etc) in emergency settings for the resettled and returning IDPs, IDPs in transit camps, those still in IDP camps, refugees and those with complications of acute malnutrition.
3. Improve early warning and response systems as well as emergency health information management systems for provincial and DHTs in 30 districts and four provinces in areas of high IDP concentration, refugee camps and drought-affected areas.
4. Train and equip existing emergency provincial and district health teams in 30 districts and four provinces in areas of high IDP concentration, refugee camps and drought-affected areas in emergency and disease outbreak investigation, surveillance, preparedness and response.
5. Improve partnerships and coordination among all health cluster/sector partners for effective emergency response in refugee camps, IDP areas, food-insecure and drought-affected regions.
Indicators Joint emergency health response plans developed for each type of disaster and for refugee
camps Reports on monthly monitoring visits to affected areas Reports of joint rapid health and nutrition assessments provided in a timely fashion 80% of basic health care service providers using standard Guidelines At least 95% of children under five immunized against measles in refugee camps Number of reported disease outbreaks investigated and responded within 48 hours 80% supervised delivery and post natal care among refugees Weekly coordination meetings held at each level (National, Provincial and District) Weekly epidemiological bulletin on vulnerable populations published and disseminated Improved mental health indicators
27
Patients at the Dadaab refugee camp nurse their children August 2008. © Allan Gichigi/IRIN

K E N Y A
Key activities Establish emergency early warning systems for disease, malnutrition and water quality
surveillance. Support 30 provincial and district teams for prompt diagnosis, disease outbreak investigation
and management of cases. Provide basic field laboratory investigation package for 30 districts and four provincial hospitals. Hire short-term local staff for disease outbreak response. Procure personal protection equipment (PPE) for haemorrhagic fevers. Procure disinfectants for cholera treatment units and other isolation wards. Train and equip district and provincial emergency health response teams in 30 districts hosting
IDPs, refugees and in the ASAL and semi-arid areas on emergency preparedness and contingency planning.
Conduct joint rapid health and nutrition assessments and emergency activities monitoring among the vulnerable populations.
Train health workers for psychosocial support. Provide psychosocial support to targeted affected populations. Provide basic health care services (drugs, emergency health kits) for identified vulnerable
populations. Provide essential secondary health care drugs, kits and services for special vulnerable groups
such as HIV, TB, patients requiring psychological support, etc. Facilitate health activities coordination and information management among IDP and refugee
camps and ASAL and semiarid areas.
Monitoring Monitoring of the proposed actions will be facilitated by the cluster lead (WHO), through: 1)
review of the existing Health Cluster Emergency Response Plan; 2) updating the existing contingency plans; 3) weekly health cluster meetings with stakeholders; 4) regular joint field visits by partners, MoH officers and project coordinators; 5) joint monitoring and evaluation with MoH and partners; 6) rapid health assessments, weekly epidemiological bulletins, weekly and monthly reports from partners and health facilities; 7) activity reports from implementing partners.
3.4.6 Multi-Sector: Protection of Refugees and Asylum Seekers in Kenya
Sector lead: UNHCR
Agencies participating: UNHCR, UNICEF, WHO, WFP, DRC, GTZ, IRC, Norwegian Refugee Council (NRC), Lutheran World Federation (LWF), National Council of Churches in Kenya (NCCK), CARE
Overview of priority needs and response strategy:Population of concernCurrently the population of concern to UNHCR is 303,89013 of whom the majority are Somali refugees. Based on current trends, UNHCR projects that by the end of 2008, there will be 322,890 including 20,000 new arrivals just in the last months of 2008, and 3,000 persons who repatriate. 14 This number could rise to between 350,000 and 400,000 refugees depending on developments in Somalia.
New arrivals from SomaliaSomalia, from 1991 to present, is cited as a real-world example of a stateless society.15 Since the fall of the Barre government in 1991 till 2006 and the capture of Mogadishu by the Islamic Courts Union, there was no permanent national government in Somalia, a situation which persists to date. The country is currently claimed as the sovereign territory of the Transitional Federal Government (TFG), a divided collection of warlords and tribal leaders. The TFG has not however been able to effectively control Mogadishu and the rest of the country. As a result of the lack of a “real” sovereign authority, Somalia continues to face widespread violence caused by fighting between the TFG and the Supreme Council of Islamic Courts (SCIC) who effectively control all the major cities in the country.16
13 UNHCR Statistics as at October 12, 2008: Nairobi (Urban Refugees) – 35,000, Dadaab Camps - 217,407 and Kakuma Camp: 51,483.14 It is anticipated that 3,000 Sudanese refugees will have voluntarily repatriated by the end of 2008. UNHCR also projects 20,000 new arrivals between October and December 2008 (Dadaab 236,317, Kakuma – 48,483 and Nairobi – 35,000). 15 MacCallum, Spencer Heath (2007-09-12). "The Rule of Law Without the State". Mises Daily Article. Ludwig von Mises Institute.
28
K E N Y A
The infighting has weakened Somalia’s socio-economic infrastructure, geopolitics, and security standing, and led to a humanitarian crisis on both sides of the border (Kenya and Somalia), which is unlikely to improve in the foreseeable future. As such, Kenya has continued to be the recipient of large numbers of asylum seekers from Somalia escaping the humanitarian catastrophe. Indeed, Kenya received nearly 58,000 Somali refugees in 2006 and 2007 (an estimated 40,000 in 2006 and 18,000 in 2007). Since the start of 2008 until September, 46,600 refugees have been received. It is estimated that the unprecedented mark of 60,000 refugees will be passed by the end of 2008. If the current situation persists, Kenya could host up to 350,000 Somali refugees and asylum seekers by the end of 2009. In keeping with its refugee protection mandate, UNHCR and partners are currently registering new asylum seekers to ensure that they receive the entitlements due to them.
Refugee protection The enactment of the Refugees Act, 2006 and its entry into force on 15 May 2007 was welcome news to UNHCR and partners. Prior to its entry into force, there was no legislative framework for the management of refugee affairs exclusively. The Act stipulates refugee rights and entitlements, and the role of the Government of Kenya in safeguarding these rights and entitlements.
As part of its core mandate of refugee protection, capacity-building has become a cornerstone of UNHCR’s programme implementation in view of government’s long term involvement with refugees. It is a strategic priority for UNHCR as it will provide a strong foundation for the implementation of the new refugee legislation and mark an important first step towards handing over full responsibility of management of refugee matters to the Government of Kenya. This initiative is aimed at bringing cognisance to the government on the Refugee Act, 2006 and the management of refugee affairs. It will emphasise a number of other areas as well, including the reception and registration of refugees, refugee status determination of individual applicants as well as camp coordination and management.
In terms of scope of implementation, the initiative has been rolled out in a holistic manner. It has targeted all officials involved in the implementation of the Refugees Act, 2006 and the management of refugee affairs, including but not limited to, DRA staff, members of the judiciary, immigration department staff, police officers and provincial authorities. It will also involve other stakeholders, including refugees, implementing partners, the legal profession and members of academia. This approach is ultimately intended to reinforce government’s and other stakeholders’ sense of responsibility and accountability in the management of refugee affairs.
Health and nutritionThe prevention and cure of disease among refugees is a fundamental principle of protection. Recent reports17 reveal that the health situation among the refugees is still far below the minimum standards and requires the action of all stakeholders. On average, there is one health facility for every 17,000 refugees. This is much lower than international standards (1:10,000 refugees). The need to close this gap is a matter of urgency. Indeed, in view of such gaps, crude mortality, maternal mortality, infant mortality and under-five mortality rates are currently far below WHO standards.
In addition, there is a high level of malnutrition resulting from the poor provision of essential goods and services. A number of surveys have indicated that the amount of food available to be consumed by refugees is seriously constrained. This is largely due to refugees having to sell some food assistance to purchase complementary foods that are in short supply as well as essential non-food items, such as wood for fuel and basic household items. Despite the injection of funds in 2008 (both UNHCR and CERF funding), the level of malnutrition among under-fives remains elevated and is below WHO standards.18 In order to mitigate the shortfalls listed above, UNHCR and partners need to provide not only the sufficient calorie intake in 2009, but also bolster the provision of NFIs.
Other areas including immunisation, micro-nutrient supplementation, de-worming of children, provision of long-lasting insecticide-treated mosquito nets, water, sanitation and personal hygiene that impact on the nutritional status of the population need to be prioritised and addressed with urgency.
16 Ethiopia and Eritrea are involved in hostilities between the TFG and the SCIC with Ethiopia sending troops to protect the TFG and Eritrea sending military supplies to the SCIC. The United States backing of the Alliance for Restoration of Peace and Counter-Terrorism (ARPCT), a warlord group, as well as the presence of Ethiopian troops have led to outrage from the SCIC, who declared jihad against Ethiopia in October 2006.17 UNHCR 2008 Annual Programme Interim Report, 24 July 2008.18 Current malnutrition levels (9% in Kakuma and 13% in Dadaab) remain below WHO standards of 5%. Anaemia and micronutrients deficiency among pregnant women and children are also acutely high at 65% in the two camps.
29

K E N Y A
UNHCR will ensure full community participation in food and nutrition planning and implementation. All nutrition actions are designed based on accurate information derived from Health Information Systems, surveys and assessments. Lastly, mechanisms will be established and maintained to ensure continuous surveillance, monitoring and evaluation of programme activities.
HIV/AIDSHIV/AIDS prevalence among refugees is high (about 15%). Refugees have neither access to institutionalised curative and preventive mechanisms, nor do they have full awareness of the issues surrounding HIV/AIDS. In addition, they are often excluded from multi-million dollar HIV/AIDS programmes.
UNHCR will strive to ensure that refugees live in dignity, free from discrimination, regardless of their HIV status, and to provide comprehensive programmes linking prevention to care by increasing awareness on causes, living positively and prevention. UNHCR will also work with the Government of Kenya and other international bodies to include refugees in national and international HIV/AIDS prevention and care programmes. UNHCR and partners also plan to increase the access of people living with HIV/AIDS to clean water and adequate sanitation and to reduce the risk of exposure to HIV/AIDS through mainstreaming.
ShelterThere are major infrastructural gaps in the Dadaab camps. This is partly due to the continued flow of asylum seekers to the camps, putting undue pressure on the already fragile infrastructure which was not initially designed for the current population. The population increase has given rise to the need for more shelter. Assessments have revealed that the Dadaab camps alone require between 25,000 and 30,000 new shelters to improve living conditions. In Kakuma, despite the ongoing repatriation of Sudanese, there is need for an additional 1,000 shelters.
In view of funding constraints, UNHCR aims to construct 7,000 new shelters in both camps, including resettlement of flood-affected refugees in Ifo camp.
WaterYet another area that has been affected by the increased camp population is the supply of safe and adequate amounts of water to refugees. In Dadaab, the existing water supply system can only deliver 17 litres per person per day (below the standard of 20 l/p/d). To bridge the supply-demand gaps in Dadaab, UNHCR plans a two-pronged approach. This will include demand management that lays emphasis on reduction of wastage on the one hand, and expanding the existing system to meet the expected standards of 20 l/p/d and emergent demands (new arrivals).
In Kakuma, refugees are currently provided with 23 l/p/d as compared to 21 l/p/d in 2007. The increase in the amount of water supplied has been due to a combination of factors, including regular maintenance of the water system and overall reduction in the refugee population as a result of the ongoing repatriation. In view of the repatriation movements, UNHCR plans to review the camp lay-out to ensure that the water supply system operates at optimum capacity.
SanitationThe sanitation conditions in the camps are very poor. Similarly, the maintenance of communal latrines in the camps and schools is also poor. The communal latrines neither offer adequate privacy for users nor are they structured in accordance with cultural and/or religious norms and practices.
The latrine-user ratio of 1:19 is below the standard of 1:14. To address this, UNHCR plans to facilitate the construction of 10,000 latrines and washing facilities by the end of 2009. In Kakuma, UNHCR plans to construct an additional 1,000 family latrines either to replace old ones or to serve new arrivals. UNHCR also plans to consolidate the camp in 2009 to enable refugees to easily access assistance and to effectively address camp security.
Floods and diseases
30
Young girls go in search of water in Dadaab refugee camp, Kenya. August 2008. © Allan Gichigi/IRIN

K E N Y A
Recurrent floods have reduced the amount of available and usable land in Ifo camp as part of the camp is flood-prone and refugees have to be relocated in the event that flooding occurs. They destroy infrastructure, expose refugees to disease and increase the need for additional shelter.
Overall objectiveMaintain internationally established standards of protection for and legal assistance to 300,000 beneficiaries in keeping with strategic policy priorities and AGDM principles.
Indicators: Please refer to the multi-sector matrix in Annex II.
Monitoring: Processes or
Events Purpose and Description Whom to Involve TimingParticipatory Review of Programme Strategy
Update the situation analysis, revise problems/visions, adjust objective hierarchy and assumptions
Representatives of intended primary stakeholders, IP staff, and UNHCR staff
Three-day workshop at beginning of the year
Development of M&E plan with Stakeholders
Assess different information needs, take stock of who is already doing what, agree on priority information areas, refine questions/indicators, decide on methods, agree on responsibilities
Representatives of intended primary stakeholders, IP staff and UNHCR staff
Two full-day meetings during first six months
Quarterly progress reviews by Programme staff
Discussion of key successes and problems
UNHCR & IP Senior staff One-day meeting every three months
Field visits Firsthand look at what is happening in the field, informal discussions about how activities are being implemented
Field staff, supervisor of field staff, Head of Sub Office
At least bi-weekly for field staff, weekly for SO staff and monthly for BO staff
Annual Project Review
Summary of key successes and problems, ideas for changing programme activities/outputs and assumptions, review of implications for the logframe, identification of lessons learned about project implementation, M&E system adjustment
Representatives of IPs, refugees, and other primary stakeholders, staff of implementing partners, UNHCR staff
Once a year
Periodic review workshops of key project components
Focused discussion about strategy and operations of key components to adjust the objective hierarchy, solve problems and identify lessons learned
Key stakeholders of the project component: intended primary stakeholders, IP, field and senior project staff
Once a year
Preparation for missions
Explain the mission purpose, agree on what the programme would like to get out of the mission, identify who needs to prepare what before the mission, organise the logistics
Small group of primary stakeholder representatives, senior staff of the implementing partners, senior UNHCR staff
Once a month prior to the mission
3.4.7 Protection/ Human Rights/ Rule of Law
Cluster lead: UNHCR
Sub-clusters/ working groups: Child Protection (UNICEF), Gender-based Violence (UNFPA)
Cluster membership: Ministry of State for Special Programmes, Ministry of Home Affairs, Children’s Affairs, Child Welfare Society, KRCS, Federation of Women Lawyers in Kenya (FIDA), NCCK, Mama na Dada, Peace-Net, Zabibu Centre, ACCORD, Action Aid, Christian Children’s Fund (CCF), DRC, CLAN, GOAL Kenya, GTZ, GDIA, Handicap International, Help Age Kenya, Help Age International, IJM, IMC, IRC, National Commission on Human Rights, Kenya Human Rights Commission, Nairobi Women’s Hospital, RCK, Save the Children Kenya, Save the Children Alliance, CARITAS, CDT, NCGD, FAO, FHOK, FAMEC, Equality Now, ECODEV, Concern Worldwide, CIDA-GESP, COVAW, CREAW, ADRA, AFH, FEMNET, Africa Woman, AMREF, ANNCPAN, Care International, Caritas
31

K E N Y A
Kenya, Sexual Offences Task Force, WFJA, WEL, World Vision, RCDA, WRAP, National Aids Control Council, MoH, Department of Reproductive Health, Ministry of Justice and Constitutional Affairs, Maendeleo ya Wanawake, Kenyan Youth Against Gender Violence, Liver Pool VCT (LVCT), LWF, IOM, USAID, UNICEF, UNFPA, Office of the High Commissioner for Human Rights (OHCHR), UNDP, OCHA, UNHCR
Overview of priority needs and response strategyThe terms of reference for the Protection Cluster, activated in January 2008, were initially limited to protection monitoring and interventions, advocacy, legal-aid and durable solutions for some 500,000 persons displaced or affected by PEV following the 27 December disputed Presidential elections. As the situation in the PEV-affected areas stabilised, albeit with many individuals and communities still struggling to achieve durable solutions, cluster members expanded their scope of work to include issues of conflict, natural disaster and displacement in other areas of Kenya. Key areas of focus include the conflict and displacement in Mount Elgon and mitigation of displacement in drought stricken areas. In addition to PEV-affected IDPs, there are an estimated 350,000 IDPs throughout Kenya in need of enhanced protection and durable solutions. Most of the displaced are living in situation of prolonged or recurrent displacement, resulting from previous events of political violence, ethnic or inter-communal conflict, natural or man-made disasters or land disputes. While the government provides humanitarian and limited financial assistance to some displaced groups, the current legislation and government policy framework on IDPs and displacement does not adequately provide for nor address root causes of displacement, peace and reconciliation, restitution for lost property, nor does it provide for sustainable and durable solutions.
Efforts are underway to ensure that by early 2009, the Protection Cluster will be transformed into a national protection forum aimed at identifying and incorporating the broader protection needs of all persons affected by humanitarian crisis and internal displacement throughout Kenya. Key and initial activities of the newly formed protection forum (Protection Working Group [PWG]) will be to establish revised terms of reference and draft a comprehensive and inclusive work plan that prioritises key areas of interests and themes as well as an advocacy and programmatic response strategy. In addition to the Nairobi based PWG, field level protection or thematic working groups may also be established with the aim of strengthening protection and human rights monitoring and establishing response networks at the field level. Linkages with key government ministries, statutory bodies and national independent and NGO protection actors will be reinforced. The Child Protection sub-cluster group will be integrated into government structures as a working group on Child Protection while the GBV sub-cluster will operate under the leadership of the National Commission for Gender and Development.
In order to enhance the accuracy of knowledge of the protection environment of persons affected by conflict, natural disaster and displacement and to better inform and improve programmatic responses, policy development and advocacy activities, the PWG and its members will undertake a broad review of conflict and displacement around Kenya. In designing and implementing actions and programme responses, PWG members will work in close collaboration with relevant government structures, national human rights and protection agencies, KRCS, local groups and communities to address the protection, human rights and/or legal/ judicial concerns of internally displaced and affected populations with a view towards mitigating, or finding durable solutions, for displacement. Further, PWG members will implement projects that are complementary to government’s efforts to strengthen physical security in all areas of displacement, including camps and affected communities and in areas of return as elaborated in the National Reconciliation Strategy document and in keeping with the Guiding Principles on Internal Displacement. Particular attention will be paid to persons with specific needs, including victims of sexual and gender-based violence, victims of ethnic-based violence, unaccompanied and separated children, elderly, persons with disabilities and people living with HIV/AIDS or other marginalised groups.
In order to create conditions conducive for sustainable return/(re) integration, emphasis will continue on community-based initiatives for conflict resolution and peace building as well as land ownership and tenancy rights, access to public/social services, attaining full protection of the law and access to national and local protection mechanisms including police and courts, and personal documentation. Systematic information collection and reporting on population movements, identification of root causes of displacement and activities will assist PWG members with advocacy activities at field and Nairobi level. PWG members will continue advocacy efforts consistent with the “IASC Steps toward Durable Solutions to Post-Election Displacement in Kenya”. The PWG will maintain close contacts with the Early Recovery and other sectors to ensure a multi-sector and non-duplicative response.
32

A young displaced boy carries his belongings January 2008. © Anthony Morland/IRIN
K E N Y A
Child ProtectionIn terms of Child Protection (CP), organisations will continue to ensure child protection prevention and response mechanisms are established in areas affected by conflict and natural disaster, including IDP and refugee populations. There will be a specific focus on capacity-building and the development of child protection in emergencies systems with input into key sectors such as education, social welfare, the judiciary, law enforcement and health. The CP sector will focus on training and the provision of technical support to partners engaged in prevention and response to unaccompanied and separated children, the development of community-based psycho-social support mechanisms, the creation of a comprehensive advocacy strategy, monitoring child rights violations, reporting and response, and provide continued support to the transition, and subsequent establishment, of a national level child protection in emergencies coordination mechanism. The Child Protection sector will also continue to work on issues of gender-based violence, including partnering with the GBV Working group, to support prevention, mitigation of impact, and child-sensitive service response.
Gender-based violence During natural disasters and armed conflict, women and girls are particularly vulnerable to GBV. Recent assessments19 conducted in Kenya indicate that perpetrators exploited the conflict and the situation of displacement by committing sexual violence with impunity. Efforts to protect or respond to the needs of women and girls in the post-conflict/development context remain remarkably insufficient. Displaced women and girls20 not only fear sexual exploitation and assault, but are experiencing other types of GBV, including abuse perpetrated by humanitarian workers and domestic violence due to shifts in traditional spousal roles, idleness among men, and stress factors associated with displaced living. Increased rates of divorce and separation have been noted—sometimes occurring along tribal lines—leaving women as the sole caretaker of their children. Other commonly reported concerns for young girls include early marriage and trafficking for domestic labour due to increased poverty and the inability of parents to provide for their children, and the withdrawal of girls from school as a result of security risks, increased domestic responsibilities, and lack of financial support. Although the GBV Working Group (GBV WG) is taking concrete steps to build a coordinated humanitarian response to GBV among IDP communities in Kenya, much still urgently needs to be done to scale-up and improve both protective and remedial mechanisms. In addressing GBV among IDP communities and communities affected by natural disasters in Kenya, actions prioritised by the GBV WG members will include: coordination at national, district and local levels; assessment and monitoring; promoting protection through humanitarian action; multi-sector GBV prevention and response. GBV WG actions will take place at the structural level through implementation of preventative measures to ensure rights are recognised and protected, at the systemic level through strategies to monitor and respond when rights are breached through statutory and traditional legal/justice, health, and social welfare systems and community mechanisms, and at the operative level through the provision of direct services to meet the health, psychosocial, legal/justice and protection needs of survivors. Particular attention will be given to the following cross-cutting issues: promoting gender equality and gender mainstreaming as key components of addressing GBV; supporting participatory approaches; engaging men and young males and females; mobilising the media, addressing GBV in schools; and conducting outreach to the most vulnerable, particularly those with disabilities.
19 Ward, J., Myrum, J., and Marsh, M. (2208). A Rapid Assessment of Gender-based Violence During the Post-election Violence in Kenya, UNFPA, UNICEF, UNIFEM and CCF.20 Response programmes should also take into account the fact that men and boys can also be victims of sexual violence.
33

K E N Y A
Objectives1. Transform the current UNHCR-led protection cluster into a national protection forum
incorporating the protection needs of all persons affected by humanitarian crisis and internal displacement.
2. Enhance the accuracy of knowledge of the protection environment of persons affected by conflict and displacement in order to better inform and improve programmatic responses, policy development and advocacy activities.
3. Create conditions conducive to achievement of durable solutions for persons affected by conflict or displaced, including the restoration and reclamation of human rights, justice/ rule of law and access to community and social services and where provided, humanitarian assistance.
4. Ensure child protection prevention and response mechanisms are established in areas affected by conflict and natural disaster, including IDP and refugee populations, with specific focus on capacity-building and CPiE systems development.
5. Deliver a set of actions to prevent and respond to GBV in line with the IASC Guidelines for GBV Actions in Humanitarian Settings and other international and national policies, resources, and guidelines in areas affected by conflict and natural disaster, including IDP and refugee populations, with specific focus on capacity-building and multi-sector systems development.
Activities Liaise with all stakeholders to build consensus on the establishment and leadership of a national
protection forum: establish a comprehensive strategy and work plan for the reformed protection forum.
Capacity of national independent and NGO protection actors is further strengthened through capacity-building measures including training and technical support.
Linkages with the Government of Kenya and statutory bodies reinforced (MoJ, MoSSP and other linked ministries and offices).
Field level or thematic protection working groups are established. Review of national legislation relevant to achievement of durable solutions and development of
and advocacy for a national IDP policy. Profiles of displaced/at risk populations established: map of protection of human rights, rule of
law needs to be established. Develop SOP for linking protection data with advocacy activities at Nairobi and field level. Make recommendation to all clusters linking protection to programmatic responses. Multi-sector assessments of conflict and displacement situations to identify and address root
causes of conflict and displacement and create conditions conductive to return. Peace and reconciliation activities and advocacy are mainstreamed into all activities. Advocacy with government at all levels, donors and national/ international agencies to ensure
timely response to the protection, human rights, legal aid/ justice and humanitarian needs of displaced persons and affected populations.
Support establishment of the ‘Child Protection in Emergencies’ national level coordination mechanism, financially, administratively, and through provision of training opportunities for government counterparts and other national child protection partners. (This will include working with other sectors, such as education, social welfare, the judiciary, law enforcement, and health).
Training of humanitarian workers, government staff and uniformed services on prevention of sexual exploitation and abuse and Code of Conduct in collaboration with food security, shelter, water/ sanitation and other sectors: HIV/AIDs awareness is mainstreamed into trainings and activities including emergency preparedness.
Support establishment of the ‘Child Protection in Emergencies’ national level coordination mechanism, financially, administratively, and through provision of training opportunities for government counterparts and other national child protection partners. (This will include working with other sectors, such as education, social welfare, the judiciary, law enforcement, and health).
Develop and disseminate standard operating procedures on prevention and response to the situation of separated and unaccompanied children, including capacity-building on identification, documentation, tracing, reunification, and mediation, including (but not limited to) continued focus on the children placed in charitable children’s institutions (CCIs) and part of child-headed households (CHHs).
Continue support to survivors (including child survivors) and service providers on prevention and response to GBV through integrated training initiatives, provision of primary education project (PEP), awareness-raising on HIV/AIDS, and dissemination of information, education, communication (IEC) materials.
34
K E N Y A
Continue training psychosocial service providers on operationalising community-based psychosocial support (PSS) actions and the concept of child-friendly spaces, with a view towards building national emergency capacity and dissemination of Kenya’s national PSS guidelines and IASC principles on the provision of PSS support.
Support the GBV sub-cluster financially, administratively, and through the provision of training opportunities for GBV partners to ensure its transition to the National Commission on Gender and Development (NCGD) as a sustainable national level coordination mechanism
Continue roll-out and operationalisation of GBV prevention and response standard operating procedures (SOPs), including capacity-building on: GBV prevention and response, community mobilisation, case management, setting up referral systems, guiding principles of working with survivors and special considerations for children.
Continued support to survivors and service providers on prevention and response to GBV through integrated training initiatives and through the dissemination of IEC materials and where to access services for GBV.
Pilot a GBV information management system in target areas to improve analysis and understanding of nature and scale of GBV.
Promote access to livelihood opportunities for vulnerable women and girls, including but not limited to, survivors of GBV
Continue efforts to institutionalise actions for prevention of sexual exploitation and abuse by humanitarian workers.
Promote access to justice for survivors of GBV. Improve capacity among first responders to integrate issues of gender, GBV and HIV/AIDS
prevention and response into all emergency actions and contingency plans.
Indicators National human rights agency assumes chair of the national protection forum, terms of
reference, areas of focus, capacity-building plan and comprehensive work plan established by March 2009.
Effective and continuous participation of focal points and agencies in the national protection forum.
General protection or thematic working groups are established as required. Map of which agency is working where (3Ws), themes and activities. Number and results of trainings on data collection, analysis and reporting. Disaggregated data by age and gender available for IDPs and affected populations. SOPs are drafted: number of times data used to develop programmes and mobilise funding and
response Number and types of situations of displacement documented. Number and locations of IDPs with enhanced access to social, legal and community services. Number of trainings and persons benefiting from peace and reconciliation skills and civic
education, including Guiding Principles trainings, Child Protection, GBV prevention and response.
Number of legal cases identified and legally assisted (legal aid, case reviews, litigation). National level CPiE coordination mechanism established. CPiE Communication strategy developed and implemented. Number of agencies engaged in child protection contingency planning process - with
corresponding information on ability to contribute insofar as technical expertise, HR and funding. Number of trainings, and number of persons trained on GBV, PSS and U/SC – with
corresponding information on how these persons/organisations are engaged in CPiE systems development.
Inter-agency GBV coordination bodies are created and supported in major sites affected by post-election violence and natural disasters.
An inter-agency plan of action is created by the GBV sub-cluster under the leadership of the NCGD.
Number of target locations that have referral mechanisms in place. GBV information management system piloted in target locations. Advocacy/awareness work plan created to ensure that people know how and where to access
services. Creation of a prevention of sexual exploitation and abuse (PSEA) focal point network. Number of agencies that have focal points and sufficient codes of conduct in place. Development of a training module for use by first responders. Number of contingency plans in place that include gender and GBV and HIV/AIDS prevention
and response.
Monitoring
35
K E N Y A
Protection Working Group/forum meetings, led by a national human rights or protection agency and co-chaired by UNHCR will meet at Nairobi level as well at field or thematic working group meetings. The fora will be used for discussions, planning and monitoring of all protection activities. The national Protection Working Group will establish a new terms of reference, work plan and response strategy during the first three months of 2009. The work plan will outline key areas of focus for 2009.
The Protection Working Group and member agencies will establish a data collection/monitoring framework during the first quarter 2009. SOPs for collection of Protection including GBV and child protection data and population movement should be established at Nairobi and field level.
Multi-sector assessments with a clear focus on protection, human rights, legal/justice and policy reviews should be conducted monitor situations and develop response strategies.
3.4.8 Shelter/NFI and Camp Coordination and Camp Management
Cluster lead: UNHCR
Agencies participating: UNHCR, UNDP, UNICEF, OCHA, UN-Habitat, MoSSP, GOAL, DRC, IOM, KRCS, CARE International, Canadian Hunger Foundation (CHF), CORDAID, Habitat for Humanity, Health Water Foundation (HWF), IRC, GAA, CRS, Shelter Forum
Overview of priority needs and response strategyThe PEV following the December 2007 disputed Presidential elections left an estimated 1,300 dead, 300,000 displaced and approximately 30,000-50,000 houses damaged or destroyed. Population movements between January – April were very fluid with IDPs moving between camps and host families, seeking safety and assistance, medical care and family tracing as well as transportation to regions considered to be ‘ancestral homes’. The fluidity of the movements made quantifying the numbers of displaced and collection of registration/profiling information a challenge: collected information was usually outdated within days. Key cluster activities in the first weeks of the crisis included mobilising through airlifts and emergency shipments, sufficient quantities of non-food and domestic items and emergency shelter materials such as plastic tarpaulins and tents for the more than 300,000 IDPs. Emergency registration (level 1) was conducted in camps to enable distributions.
Within the first days of violence, the Government of Kenya appointed the KRCS as coordinating agency for country-wide emergency response as well as IDP Camp Management: KRCS chaired the CCCM National Coordination meeting both in Nairobi and at field level, with UNHCR as co-chair providing technical support/advice. In addition to CCCM, KRCS was responsible for providing emergency food and non-food assistance, through a ‘single pipeline’ approach and negotiating with local authorities for allocation of land to establish IDP camps. In total, more than 260 camps were established either by KRCS or spontaneously. In addition to KRCS, UN agencies and local and international NGOs rapidly deployed emergency field teams. Warehouses for emergency shelter and NFI stocks were established in each region by KRCS. Within ten days of the crisis, the pipeline for NFI including plastic sheeting, tents and other domestic items was established and family kits and emergency shelter supplies channeled to KRCS. While some agencies continued unilateral distribution, the majority of items were issued through the KRCS single pipeline system by the organisation’s volunteers. Emergency shelter consisted of tarpaulins issued in combination with poles and a variety of types of tents. A key constraint of the single pipeline system was the lack of accurate and timely reporting to donor agencies on where and to whom items were distributed. The 2009 contingency planning process by all agencies should include a section on single pipeline distribution to ensure accountability and reporting.
In the absence of further displacement requiring establishment of camps and sites, the CCCM Sector will likely not be active in 2009. However, UNHCR, OCHA, WFP, UNICEF and other agencies will continue to work with Government of Kenya, KRCS, NDOC and other structures to ensure that CCCM planning and SOPs for camp establishment are included in contingency planning and future trainings in preparation for any emergency humanitarian scenarios that may warrant establishment of camps, including displacement due to conflict and natural or man-made disasters. Inclusion of CCCM issues and coordination of a multi-sector response should also be part of UN contingency planning. Additional training on CCCM can also be conducted, particularly through training of trainers initiatives.
The Shelter Cluster has transitioned to a national Shelter Working Group chaired by the MoSSP and co-chaired by UNHCR. Initial terms of reference of the Shelter Cluster were to coordinate emergency
36

K E N Y A
shelter and NFI procurement and transport, including mobilising tarpaulins and tents for emergency shelter and developing a prototype for transitional shelter (TSK) for rapid deployment during the initial phases of return. While the TSK model was initially adopted by the Shelter Cluster members and government as the first basic shelter model, it has since been upgraded to a more permanent structure in the hopes that return will be durable. In September, the MoSSP launched the Low-Cost Housing Scheme that aims to reconstruct up to 40,000 houses (for 200,000 persons), mainly in rural areas, for households with completely destroyed houses. In line with this project, Shelter Working Group members have established a common shelter design and bill of quantities as well as implementation strategy. In 2008, shelter partners will construct an estimated 4,500 low-cost houses for IDPs returning to their lands.
Other categories of IDPs that are currently at risk of continued and prolonged displacement are IDPs who did not previously own land and instead were renters of lands/houses and business properties or were squatters. This category of IDPs is still in need of durable solutions as the majority cannot return due to discrimination or insecurity. In some cases, those in the squatters group have been displaced multiple times and are in dire need of durable solutions. In the past months, a number of these IDPs have grouped together and are purchasing land as a group, with the hope of constructing homes and reestablishing their lives and livelihoods in safety and dignity with full access to services.
The Shelter Working Group partners propose to continue with implementation of the self-help, Low Cost Housing Project in 2009. To foster conditions for sustainable return and to facilitate the peace and reconciliation process, both displaced and non-displaced communities are mobilised to conduct joint housing assessments and beneficiary selection based on established criteria. Training of youth/ young men and women on shelter construction and the self-help components of the project are designed to engage all sectors of the community and strengthen reconciliation and peace building efforts. Collaboration with local government officials will foster trust-building, improve beneficiary identification, help resolve land ownership issues and facilitate access to services such as water, health and education. All Shelter and NFI related as well as CCCM initiatives will pay special attention and report on cross cutting issues such as GBV, Peace and Reconciliation initiatives, HIV/AIDS and operate with established criteria that prioritise and target the most vulnerable within communities.
In addition to PEV-affected areas, some shelter partners will work in other areas affected by conflict or natural disasters to provide NFI and/or emergency or low-cost housing. Mount Elgon region, where there has been significant destruction and ongoing displacement, is one such focus area. Emergency shelter initiatives in areas of conflict and natural disaster will also be coordinated with MoSSP, KRCS and other government and local actors.
Shelter and NFI distributions related to durable solutions will be planned in conformity with the ‘IASC Steps toward Durable Solutions to Post-Election Displacement in Kenya’ and will be closely coordinated with Early Recovery Cluster partners.
Objectives:1. Ensure access to adequate physical protection, decent living conditions and proper shelter2. Provide sufficient basic domestic, hygiene items (NFI) and emergency shelter to IDPs and
other affected persons.3. Establish and strengthen existing CCCM mechanisms as needed in preparation for
emergency humanitarian scenarios and coordination of multi-sector response in 2009.
37
Danish Refugee Council/UNHCR supported shelter project at Karirikanya Farm, Molo District. Photo by OCHA. October 2008

K E N Y A
Activities In coordination with MoSSP, local officials and communities, quantify overall shelter needs for
emergency and/or low-cost shelter in areas of operation. Construct/distribute low-cost housing kits or shelter material kits to households with damaged
destroyed houses. In conflict/return areas, ensure linkages with or undertake, and report/ address on peace and
reconciliation or legal aid needs or other protection issues to better ensure a durable return. Link with other clusters and line ministries, agencies: water/sanitation, health, education to
ensure access to services. Procure, warehouse and distribute emergency shelter materials where required: tents,
tarpaulins. SOPs for NFI distribution and beneficiary tracking are drafted and included as part of
contingency plan: train all managers and distributors on reporting requirements. Cluster agencies participate in contingency planning for emergencies in Kenya. Efficient procurement, storage and distribution mechanisms are established by each agency Guidance and training on CCCM. CCCM is included in contingency planning including pre-emergency training of staff and SOPs
for camp establishment and management. Registration/profiling and data management SOPs are pre-established between Government of
Kenya, KRCS, UN and NGOs.
Indicators Quantification of shelter needs and types in target areas established. Beneficiary databases are maintained: Number of shelters constructed/ distributed in each
location for number of persons (age/ gender disaggregated data). Number of locations benefiting from multi-sector response in addition to shelter (water/
sanitation, health, education, peace building, etc). Number of areas where peace-building and reconciliation activities are used to promote
sustainable return. SOP in place for distribution and beneficiary tracking practices. Percentage of NFI accounted for through distribution reports. Percentage of gaps identified and reported. Contingency plan for conflict/ disaster include CCCM planning. Number and locations of trainings for possible CCCM activities. SOPs for registration/ profiling, site mapping and data management are drafted and put in
place.
Monitoring Distribution monitoring and reporting format for NFI/emergency shelter to be established:
training on distribution recordkeeping and reporting should be provided to all managers. Shelter Forum will compile information on shelter, NFI distributions. Shelter Forum will continue to monitor shelter projects through visits and reviews.
3.4.9 Water, Sanitation and Hygiene
Cluster lead: UNICEF
Agencies participating: Water and Environmental Sanitation Coordinating Group (WESCOORD) Members (Line Ministries MoWI, MoPH&S, MoE, KRCS, NGO partners, FBOs, private sector organisations, UNICEF & UN agencies)
Overview of priority needs and response strategy
IDPSParnters continue to support returning IDPs through repair and rehabilitation of water supplies in returnee areas, construction of latrines in schools and hygiene promotion activities. Water and sanitation activities also continue for those few IDPs still in camps and those in so called “transitional camps.” There are many IDPs who have been integrated into communities,
38
A boy drinks water at the Eldoret IDP camp, April 2008. Manoocher Deghati/IRIN

K E N Y A
notably in Kisumu and Nairobi informal settlements, which is placing a strain on already poor existing services. Priorities are to provide water and sanitation services in returnee areas, especially schools and health centres, and to support communities hosting IDPs.
DroughtPriority need is to establish adequate, sustainable water supplies and move away from the expensive and unsustainable water trucking which has been the standard drought response. The response strategy is to include the establishment of water supplies with solar or wind powered pumps where this is feasible and to build capacity in local communities to manage the water supply schemes more effectively. Support is needed to repair and rehabilitate existing water supplies and ensure their sustainability through improved management capacity. Hygiene promotion and behavioural change is also a priority area for action to reduce the water and sanitation related disease load - this includes promotion of hand-washing with soap and training on appropriate household water treatment, storage and use.
RefugeesThe influx of Somali refugees is placing a strain on the existing water and sanitation infrastructure in the Dadaab refugee camps. Whilst current service provision is adequate, the ability of the infrastructure to cope with increased numbers of refugees is being tested. Strategies include the drilling and equipping of new boreholes and installation of new water and sanitation infrastructure, hygiene promotion and education and the training of local artisans in concrete latrine construction. One of the biggest challenges in Dadaab is the huge amounts of solid waste produced – whilst there are currently plastic recycling projects ongoing, these, as well as other solid waste management strategies need to be strengthened. Also to be considered in project planning are the needs of the host community in Dadaab since the possibility of hostility due to the unequal allocation of resources is high.
CholeraCholera outbreaks are common in Kenya and although they can happen anywhere, outbreaks tend to be found in flood-prone Western and Nyanza Provinces along the shores of Lake Victoria and in the ASAL areas most noticeably Mandera District. Nakuru and Wajir Districts also suffer as well as the Hagadera Refugee Camp in Dadaab.
A priority is to strengthen the cholera monitoring and response mechanisms. These are primarily through the MoPH&S and Ministry of Water. Strategies would include provision of water quality testing kits and training for District Officers to plan, implement and sustain a coherent water quality testing regime and to build capacity to respond early to contain outbreaks. Hygiene promotion is an essential component of cholera response and such activities would use schools as an entry point to the wider community.
Table of Proposed Coverage SITE / AREA ORGANISATIONS
Kisumu WV, Action Aid, KRCSEldoret CRS, Catholic Diocese of Eldoret, KRCSNakuru ACF, Action Aid, Diocese of Nakuru, KRCSMandera ACF, IR, KRCSTurkana Oxfam GB, Merlin, IRC, KRCS, COOPIMolo Merlin, DRC, Action Aid, ACF, KRCSNarok South Merlin, KRCSKipkelion Merlin, Action Aid, KRCSWajir Merlin, Oxfam GB, KRCS, COOPIKitale IRC, KRCSWestern/Nyanza Health & Water Foundation, New Life International, WV, CARE, Action Aid,
KRCSOther ASAL Areas KRCS, ACFDadaab, Kakuma CARE, DRC, NRC, UNHCR, IRC
Objectives Effective leadership is set-up for WASH Inter-Agency Coordination, including for provision of
children and women’s special needs regarding water, sanitation and hygiene. Children and women have safe and reliable access to sufficient water of appropriate quality for
drinking, cooking and maintaining good hygiene. Children and women have easy access to toilets and washing facilities, both day and night, that
are secure, sanitary and are user- and gender friendly.
39
K E N Y A
Children and women, including child caregivers, receive critical WASH-related information on how to protect health and well-being, especially prevention of diarrhoeal disease among young children.
Children in their learning environment/s have access to safe water, sanitation and hygiene facilities that are secure, sanitary and user and gender friendly.
Indicators
IDPs Percentage of IDPs who have access to adequate qualities of safe drinking water. Percentage of IDPs who have access to adequate and appropriate safe sanitation. Percentage of IDPs who are reached by hygiene promotion messages. District WESCOORD structures in place and functioning.
Drought Percentage of population in target area with access to adequate quantities of safe drinking
water. Percentage of population in target areas with access to improved sanitation facilities. Percentage of population in target areas practising improved hygiene behaviour. Number of households in target area which have received training on safe handling, storage
and use of water including household water treatment choices. Number of people receiving safe water from repaired or rehabilitated water supply schemes.
Refugees Quantity of water per capita per day. Water pumping capacity Reduction in waterborne disease incidence. Percentage of refugees who have access to adequate and appropriate safe sanitation. Percentage of refugees who are reached by hygiene promotion messages. Host community are aware and involved in decision making and coordination processes. Host community receive improved WASH services.
Cholera Reduction in seasonal diarrhoea outbreaks in target districts. Reduction in vulnerability to diarrhoea and other water related illnesses by adherence to safe
water treatment and usage and use of safe sanitation options. Improved access to safe drinking water and sanitation facilities. Strengthened Government of Kenya capacity to plan and implement emergency actions and
respond to cholera outbreaks.
Activities
IDPs Support construction, including training on management, of water and sanitation facilities for
vulnerable groups. Support the repair and rehabilitation of damaged water supply and sanitation facilities. Construction of latrines and water supplies in schools. Provide emergency WES supplies to affected populations. Support development of appropriate water quality testing surveillance and response systems. Conduct hygiene promotion activities to affected populations with a focus on school children. Conduct capacity mapping exercises, identify gaps and support training programmes for
Government district officers. Support Government of Kenya to coordinate WES sector emergency preparedness and
response through formation of WESCOORD secretariat.
Refugees Construction and equipping of new boreholes complete with pumps, generator sets and
overhead steel tanks. Installation/rehabilitation of water supply infrastructure. Hygiene and sanitation education projects conducted using schools as entry points to reach the
camp community. Solid waste clean-up campaigns.
40

K E N Y A
Training of local artisans on concrete latrine slab construction and creation of demand for household latrines.
Support development of water-quality surveillance system.
Drought Latrines and rainwater harvesting systems constructed in schools. Hygiene and Sanitation Education activities conducted in schools and communities. Water supply schemes repaired and rehabilitated. Water user committees mobilised and trained on management of water schemes. Community members reached by hygiene promotion messages. Local artisans trained in construction of concrete latrine slabs and latrine demand increased. Household latrines constructed. Provision of water quality testing kits and training for Government of Kenya personnel. Households equipped and using effective household water treatment techniques. Formation of permanent National WESCOORD secretariat and training for district
WESCOORDs to strengthen emergency coordination structures.
Cholera Equip MoWI and MoH personnel in target districts with portable water quality testing kits and
provide training on their use and the planning and implementation of a water quality surveillance strategy.
Support Government of Kenya personnel to plan and implement cholera response activities through distribution of emergency WES materials and hygiene promotion campaigns.
Provision of chlorine to disinfect community water points and supply schemes. Support Government of Kenya to conduct hygiene promotion campaigns to provide key hygiene
messages to populations living in the affected districts with focus on schools and surrounding communities.
Support the cleaning and disinfection of community water points, i.e. shallow wells with a focus on schools and health centres.
Monitoring The projects will be managed by UNICEF Project Officer in partnership with MoWI through the WESCOORD structure. Activities will be monitored through field reports from district WESCOORDs, partners and UNICEF field staff together with field visits by UNICEF Project Officer. Project reporting will be in line with UNICEF standards.
Areas Category Affected population Beneficiary populationASAL Areas, Dadaab and Kakuma Refugee Camps, Western and Nyanza Provinces, Rift Valley Province.
IDPs 100,000 63,300Refugees 250,577 250,577School Children 153,850Vulnerable Populations 823,000Grand total 350,577 1,290,727
41

K E N Y A
4. CRITERIA FOR SELECTION OF PROJECTS
All cluster/sector members were able to submit CAP projects that contribute to the attainment of the objectives outlined in the sector response plan. The criteria for the inclusion of projects in the 2009 CAP were: the project must be consistent with the cluster/sector strategy and must contribute towards the
attainment of the overall goal and towards the achievement of one or several of the strategic priorities agreed upon by the IASC for the humanitarian operation in 2009;
the project must present a clear target in the specified operational areas and should not duplicate activities implemented by other organisations;
the appealing agency should have a recognised capacity to implement the project; appealing organisations must be part of existing coordination structures; the implementation of the project or part thereof must be feasible within the 12 month
timeframe; the project must be cost-effective in terms of the number of beneficiaries and the needs to which
the project intends to respond.
To ensure that the projects met the criteria above, cluster/sector working groups reviewed the project submissions. The final selection of projects by the clusters was in turn been agreed by the IASC and the Humanitarian Coordinator.
5. STRATEGIC MONITORING PLAN
In order to monitor the implementation of the response plan, humanitarian partners under the leadership of the IASC will ensure regular monitoring of the sector response plans and the overall strategic objectives. Cluster/sector leads will undertake regular consultations and exchange information with partners on the resourcing and implementation of projects and the impacts on targeted beneficiaries. In addition systematic multi-sector reviews of the EHRP will take place through regular inter-cluster meetings, and the Kenya Humanitarian Forum. Updates, including information and analysis on funding will be shared with the IASC on at least a quarterly basis. A mid-year review process will also be undertaken to provide systematic feedback on the progress of the appeal and to make any relevant adjustments to the strategy and/or resource requirements outlined in the appeal.
6. COMPLEMENTARITY WITH OTHER ACTORS
In responding to humanitarian needs generated by the post-election crisis, inter-agency processes including the cluster approach, have enabled effective coordination with the Government of Kenya, with the KRCS and the ICRC21 as well as with CBOs and non-formal entities in the field. As the crisis shifted from an acute to chronic phase, clusters have expanded their focus to include other humanitarian situations in the country including emerging drought and growing food insecurity and other localised conflicts. In addition clusters have also begun to work towards supporting national coordination structures – a process that will continue into 2009.
Participation in the clusters has been broad and robust and has allowed for inclusive sectoral coordination. Members have collaborated in numerous joint initiatives including needs assessments, response programming and advocacy. Responses to the post-election violence have been harmonised with the KRCS which served as sector lead for Camp Coordination and Camp management and has actively participated in the IASC. Government partners have also played an active role in the clusters and in a number of sectors continue to act as co-chair. This has ensured regular information sharing and strategic harmonisation with government processes and activities. Since the restructuring of ministries in April 2008 cluster have successfully identified new counter-parts and continue to work in close consultation. The establishment of a twice monthly Humanitarian Stakeholders meeting organised by the MoSSP has also helped to strengthen multi-sector coordination between the Government of Kenya and the humanitarian community.
21 The ICRC has stated that its position on the cluster approach is the following: “Among the components of the Movement, the ICRC is not taking part in the cluster approach. Nevertheless, coordination between the ICRC and the UN will continue to the extent necessary to achieve efficient operational complementarity and a strengthened response for people affected by armed conflict and other situations of violence. At the global level, the ICRC participates as an observer in many of the cluster working group meetings.”
42

K E N Y A
The overall priorities and sector specific response plans outlined in the EHRP reflect the ongoing dialogue with the Government of Kenya and the KRCS at both a technical and decision making level. In relation to continued response to those affected by post-election violence an emphasis on peace and reconciliation and on livelihoods recovery is complementary to Government efforts in this area. Continued multi-sector assistance also aims to complement these efforts by helping to address the immediate needs of the most vulnerable.
In relation to the declining food security situation in many parts of Kenya, the KFSSG and KFSM have continued as the main mechanisms for the coordination of assessments and response activities. In June, the KFSSG undertook an evaluation of the impact of rising food prices on vulnerable groups throughout the country which has formed the basis of related programming among humanitarian partners. Similarly the Long Rains Assessment – again conducted by the KFSSG - has provided solid and agreed assessment data which has informed response planning to drought-affected and other food-insecure populations. The information and recommendations outlined by these joint assessments are clearly reflected in the EHRP strategy.
43
K E N Y A
ANNEX I. SECTOR RESPONSE: ACHIEVEMENTS AND CHALLENGES
Cluster 2008 Cluster / Sector Objectives
Achievements Constraints / challenges
Cam
p C
oord
inat
ion
and
Cam
p M
anag
emen
t (C
CC
M)
IDPs hosted in camps receive effective and well-coordinated humanitarian services to meet their protection and assistance needs.
IDPs hosted in camps participate in all aspects of camp life through a community and rights based approach.
Emergency IDP registration / profiling to determine numbers, protection needs and intentions of IDPs hosted in sites and host communities.
Camp Coordination and Camp Management (CCCM) Efficient CCCM and Sudden Onset Disaster meetings, Chaired by KRCS at Nairobi and field
level and attended by all stakeholders were essential for coordination and rapid response. Development and adoption of CCCM guidelines, standards, and camp rules and regulations
(to be included in contingency planning) improved overall coordination, division of labour between stakeholders and response.
KRCS camp managers appointed for each major camp location (mobile camp managers for smaller sites) leading to improved coordination and services.
Clear division of labour between KRCS and Government of Kenya on IDP registration and profiling responsibilities.
Key KRCS, National Disaster Operation Centre (NDOC), district government staff trained in multiple CCCM trainings.
Camp services profile formats and gap analysis used to better assess and coordinate camp service, identify service providers, and identify and address service gaps.
KRCS managed- IDP camps met minimum basic standards for services and infrastructure. Communities hosting IDP both in homes and camps provided significant assistance
including food and non-food and financial support. Ability of some CCCM partners to operationalise rapidly and form effective working
relationships with the Government of Kenya and KRCSRegistration and Mapping.
By mid April, all IDP camps and sites mapped by Regional Centre for Mapping of Resources for Redevelopment (RCMRD): transit sites (post Operation Rudi Nyambani) mapped in June and updated in October: maps and camp profiles used by partners for monitoring/ service provision.
Camp Registration: KRCS, International Organization for Migration (IOM) and United Nations High Commissioner for Refugees (UNHCR) conducted IDP registration in all major camps.
Technical advice, training and support provided to KRCS and partners on CCCM, registration, protection, gender-based violence (GBV), etc.
Government of Kenya IDP registration/ profiling exercise: Government of Kenya conducted registration of all post-election violence (PEV) IDPs across the country to establish a profile of the IDP and affected persons: data entry of the 130,000 households.
UNHCR Support to Government of Kenya Registration/ Profiling: Technical support and advice (March – December) to Government of Kenya, Ministry of State for Special Programmes (MoSSP) and Bureau of Statistics for development of a national, PEV IDP registration system. Design and development of the registration/ profiling forms and database, training of data collectors and Bureau of Statistics data entry staff.
Lack of contingency planning for post-election violence. Limited CCCM capacity in early days of crisis and dearth of
trained CCCM and resistance to assistance from NGO partners.
Sudden and uncoordinated start-up of Operation Rudi Nyambani disrupted all camp infrastructure and systems established to provide quality services.
Lack of peace and reconciliation and lack of proper conditions for return to pre-displacement locations led to movement of IDPs from established camps and host communities to unassisted transit sites.
Uncoordinated, rapid and unilateral decisions for closure and breakdown of camps led to loss of equipment and infrastructure materials: withdrawal of camp managers prior to departure of all IDPs led to worsening camp conditions and services.
IDPs in host families and affected communities did not receive the same level of humanitarian support as camp based IDPs, due to constant movements, limited time and resources.
Limited financial and material resources did not allow agencies to re-establish services in the more than 200 transit sites established during and post Operation Rudi Nyambani.
Fluidity of population movements did not allow for efficient registration or profiling of the population: registration while population movements ongoing may not be an efficient use of resources.
44

K E N Y A
Cam
p C
oord
inat
ion
and
Cam
p M
anag
emen
t (C
CC
M)
Support national humanitarian response through effective coordination of the international response and inter-sectoral coordination.
Maintain an overview of the humanitarian response including the needs and gaps per sector
Improve humanitarian information sharing and management.
Cluster coordination mechanism successfully implemented in response to the PEV crisis. Bi-weekly and latterly monthly IASC meetings held to support inter-agency decision making
under the guidance of the humanitarian coordinator. Bi-weekly inter-cluster meetings held for technical level coordination. Review of cluster mechanism conducted in August and recommendations made. Weekly and latterly bi-weekly Kenya Humanitarian Forum meetings held to support inclusive
information sharing and coordination. Support provided to national coordination mechanisms at national and sub national levels.
At national level, this has included secretariat support form the MoSSP stakeholders meetings and facilitation of round table discussions for the Ministry of Livestock. At sub-national level support has been provided to district and provincial level coordination structures.
Information management supported through the Office for the Coordination of Humanitarian Affairs (OCHA) Kenya website, the inter-cluster website, 3W databases and mapping initiatives.
Weekly (now bi-weekly) humanitarian updates produced reflecting the humanitarian situation, response activities and highlighting gaps.
Ad-hoc analytical reports produced. Inter-agency assessments facilitated including through the development of multi-sector
assessment tools. Opportunities for humanitarian funding supported including through four successful CERF
applications and through the EHRP mechanisms. Advocacy working group established and key advocacy messages developed. Guiding Principles on Internal Displacement widely disseminated through Government of
Kenya and humanitarian community and translated into Kiswahili.
Fluid nature of the situation and need for flexible approach to response activity.
Proliferation of actors at the onset of the post-election crisis. Limited financial and human resources for coordination at
the onset of the post-election crisis. Priority focus on post-election crisis has limited the
awareness and resources for other humanitarian needs in Kenya.
Limited knowledge of the Cluster Approach in a country that is not acclimatised to complex emergencies.
45

K E N Y A
Early
Rec
over
y an
d Fo
od S
ecur
ity Augment
ongoing emergency assistance operations in Kenya by building on humanitarian programmes to ensure that their inputs become assets for long-term development, thereby fostering the self-reliance of Kenyan populations and helping rebuild livelihoods, promoting spontaneous recovery initiatives, and establishing the foundations of longer-term recovery.
Although the articulation of early recovery is rather recent, the cluster was able to establish and achieve a common understanding of early recovery needs, gaps and priorities. In the Kenyan context, the humanitarian phase of the crisis was considered to be rather short compared to other crises. This has partly been attributed to immediate early-recovery actions at the onset of the crisis.
Development of an Early Recovery/Food Security (ER/FS) Work Plan that focused on five strategic pillars: peace and reconciliation; governance and rule of law; reviving agricultural and non-agricultural livelihoods; restoring delivery and access to basic needs and services; and mainstreaming of cross-cutting issues.
A rapid ERNA was conducted by a joint mission comprising of United Nations Development Programme (UNDP), OCHA, World Health Organization (WHO), IOM, UNOHCHR/UNON and the National Steering Committee on Peacebuilding and Conflict Management. The ERNA was conducted in the affected districts between 24 March 2008 and 5 April 2008. The specific objectives were, among others, to present an overview of the situation with regards to ER&FS, testing the relevance of the Kenya Strategic Early Recovery Framework; to contribute to the ER&FS Work Plan; to assess local capacities and identify gaps and opportunities; and to establish synergies with the Government of Kenya's recovery strategy and donors’ intentions. The ERNA continues to be relevant, and informed several actions.
A Peace and Reconciliation Task Force was formed from among cluster members. The Task Force developed a framework for durable return, resettlement and reintegration, focusing on conflict-sensitive approaches. Elements of this framework were used in conflict-sensitive workshops carried out by two cluster members. The target audience of the workshops were not only those involved directly in peace building, but also organisations in other fields, to emphasise the need for incorporating peacebuilding as a cross-cutting issue into other actions.
The framework for durable return was also used as an advocacy tool. Inter-agency coordination on early recovery was enhanced. Close liaison with donors, several of which were active members of the cluster. Information sharing was a key component of the cluster. This was done in several ways:
(i) Sharing of actions, best practices and needs during cluster meetings;(ii) The ER&FS Cluster was the first cluster to establish a “who does what where” (3Ws)
database, using the OCHA 3Ws tool. This information can be used to identify actors, avoid duplication of efforts, design complementary actions and to identify gaps that need to be addressed;
(iii) A live geographic information system (GIS) map was developed based on the information in the 3Ws database. The map provides an easy reference tool. Hard copies of this map have been distributed. The information is continually updated.
(iv) Mapping of voucher schemes used to address agricultural and non-agricultural livelihoods recovery.
Establishment of a Livelihoods Technical Group, which focused on enhancing understanding of the needs, gaps and capacities related to livelihoods recovery; and guidance in terms of dissemination of vocabulary, principles, specific needs for specific people, and coordination.
Piloting of the District Recovery Steering Group in the greater Nakuru area to coordinate early recovery and recovery activities.
Piloting of Livelihoods Recovery Group in the greater Nakuru area, which explores ways in which the community can work together to recover its socio-economic activities.
Although coordination was well established at the national level, field coordination needed improvement. There was an attempt to address this through the piloting of the District Recovery Steering Group in the greater Nakuru area.
Information sharing was a key component of the cluster. There was a constant need for data and, consequently, the continuous updating of data, which could be easily available to all stakeholders and particularly at the community level. Ways to make data more accessible at the community level are being explored.
In relation to field coordination and field implementation capacity, there were gaps in actions, particularly in addressing the restoration of non-agricultural livelihoods.
Resource mobilisation remained a major challenge to the cluster, and hindered some of the work that could have been undertaken had resource been available.
Mainstreaming of cross-cutting issues. Although data was available, it was a challenge to find
gender-disaggregated data, which is needed to then design appropriate actions.
46

K E N Y A
Educ
atio
n To ensure
continued access to education for at least 200,000 children and promote psycho-social recovery and promotion of peace and reconciliation in and through schools and/or learning spaces.
To improve quality of education building teachers’ and managers’ capacity to promote psycho-social recovery, peace and reconciliation in and through schools. Parents, School Management Committees (SMCs) and provincial education authorities included.
According to the information available, as some education partners did not provide updates, 85% of children have been reached and regularly enrolled in school, at least up the end of May, 1,250 schools were supported. The enrolment rate decreased as the resettlement exercise started and also as a lot of children, were left behind by families. As a result they have dropped out from school. The peace and reconciliation trainings (workshop and sensitisation activities and training of trainers (ToT) were done in the PEV-affected areas (in cooperation with the MoE – a manual was developed) targeting children, teachers, school administrators and the communities, as well as the psychosocial support, which is mainstreamed under the Child Protection sub-cluster.
MoE welcomed the idea of the education cluster and requested to expand the education cluster response all over the country, in other emergencies.
MoE is going to prepare the national Emergency Preparedness and Response Plan (EPRP). All the education cluster members are going to prepare the respective contingency plans,
which will be in line with the EPRP from the MoE.
No EPRP was ready for all the education partners, included the MoE.
Not enough funds available. Data collection not put in place since the beginning. Lack of teachers and reliance on “volunteer teachers” when
not paid. Stigmatisation of the IDP children when integrated in the
hosting schools. No school feeding programme. Fluidity of populations between camps and transit camps. Quality of teaching affected in the areas. Lack of infrastructures. Classrooms overcrowded, so far the ratio teacher/pupils not
respected. Ethnic tensions impacted the education and agencies’
response.
47

K E N Y A
Emer
genc
y Te
leco
mm
unic
atio
ns Provide
security telecommunications World Food Programme (WFP) and DATA support United Nations Children’s Fund (UNICEF) services to all humanitarian actors responding in Kenya.
The coordination component of the projects achieved the following:o All UN agencies were integrated into a common radio network;o Common VHF and HF frequencies licence requested thru UNON for all UN
agencies;o Common NGO frequencies requested thru UNON;o Standardised communication procedures and training materials were created for
all UN agencies;o A telecommunications information database was centralised for all UN and NGO
staff in Kenya. The deployment component of the projects in three locations,(Eldoret, Nakuru, and Kisumu)
achieved following:o A fully equipped Inter-Agency communication centre (COMCEN);o Two UN VHF repeater channels (UN Security / Call channel, UN / NGO Working
Channel); o Training of UN and NGO staff on the use of the network; o Provision of free DATA services (E-mail & Internet Access|) to all humanitarian
community. One of the main components of the projects was the standardisation of procedures, and the
subsequent development of a standard training curriculum. Radio Trainer was travelling with the deployment team to ensure that all UN and NGO staff receives training.
The training packages that have been developed included:o User Training, including all the material required by UN staff and NGOs; o Driver training, which includes extensive documentation on the use of HF and mobile
VHF radios, as well as vehicle tracking procedures;o Radio Operator Training, which is largest and most comprehensive training package,
including all aspects of radio communications. Estimated over 300 humanitarian staff will receive radio training during the project.
48
K E N Y A
Food
Aid
Malnutrition rates maintained below emergency levels in areas affected by rains failure and post-elections violence; moderate malnutrition managed and severe malnutrition prevented among children under five and pregnant and lactating women.
WFP scaled up operations in post-election crisis (areas, distributions started on 6 January from existing stocks.
Three main hubs created: Eldoret, Kisumu and Nakuru. Up to 211,000 beneficiaries reached in PEC areas on monthly basis. Distributions continued in ASAL, with a gradual scale-up of food for assets in semi-arid and
coastal districts to 220,000 beneficiaries. Total beneficiaries in ASALs increase from 883,000 to 1,027,000 based on the
recommendations of the assessment. Malnutrition prevented in post-election crisis areas and kept below emergency global acute
malnutrition (GAM) levels in at two of the arid districts. Two food security assessments undertaken jointly, with high WFP participation and support,
to review the beneficiary figures in ASAL and post-election violence areas. Another assessment planned for urban areas to establish levels of vulnerability due to high
food prices and inform future response.
In the first months of the operation in post-election crisis areas, WFP had to take on a major responsibility of providing trucking capacity for secondary transport, the role normally performed by NGO partners. At that time KRCS could only do a part of secondary transport from Extended Delivery points to final distribution points. In July, a standard field level agreement was signed with KRCS by which KRCS became responsible for secondary transport and distributions, and assigned more staff to the post-election crisis areas.
Numbers of IDPs were fluctuating and needed continuous verification by KRCS and WFP.
Communication between numerous IDP sites and WFP hubs was a challenge at the peak of the crisis.
Quick turnover of KRCS staff on the ground, lack of professional staff, and constant need to educate KRCS volunteers on food distributions was labour-intensive; the situation improved when KRCS deployed professional staff, & when the situation stabilised and a MoU with WFP was signed.
Fuel prices and insecurity contributed to higher transport rates, especially felt in the most remote arid areas; this rendered WFP operations more expensive.
49

K E N Y A
Hea
lth The main
objective is to prevent and reduce mortality and morbidity among IDPs host communities and refugees.
Improve coordination among health cluster partners.
Facilitate rapid health and nutrition assessments.
Conduct rapid disease outbreak investigation and response.
Provide minimum primary health care packages for vulnerable populations.
Provide secondary care for special vulnerable groups.
Improve management of cases by partners.
WHO increased office and field presence for three months during PEV and facilitated coordination of health partners at all levels.
National stakeholders/partners workshop held and emergency response plan developed and later same was reviewed.
Coordination forums for partners established at provincial and district levels held. Joint rapid health and nutrition assessments conducted at national, provincial and district
levels. Management and prompt dissemination of emergency health information to all stakeholders. District teams supported financially and logistically on the field to lead the emergency
response. Provided emergency and other health kits for basic health care services, including for
reproductive health. Health promotion on basic hygiene, HIV conducted in all IDP camps. Disease and water quality surveillance established in affected provinces and districts. Conducted immunisation of children under-five against measles. Threats of disease outbreaks promptly investigated and responded to. Facilitated provincial and district teams and hospitals to take prompt care of the sick
and injured during the post-election violence. Provided essential drugs and consumables to the provincial and district hospitals and
refugee camps. Patients with special health problems (HIV, TB, diabetes etc) traced and given
appropriate treatment. Financed transportation of essential drugs from Nairobi to the districts, IDP and refugee
camps (including family planning commodities). Partners provided ambulance services for referred cases from communities and
districts to referral points. Supported district and provincial hospital laboratories to diagnose diseases of epidemic
potential. Emergency trauma counselling and psychosocial support provided by the KRCS and IOM.
Many partners and local structures were weak in coordination. Poor local resources for coordination. Difficulty assessing the vulnerable populations due to
insecurity. Overwhelming basic social needs of the affected populations. Displaced or traumatised health workers who were not
motivated to carry out the emergency health services. Shortage of basic essential drugs and consumables
especially at points of need. Ineffective established local health structures.
50

K E N Y A
Logi
stic
s Support the
humanitarian community in assistance of the displaced populations in Kenya with effective logistics.
WFP as the lead of the logistics cluster launched a Special Operation (SO) “Humanitarian Air & Logistics Augmentation in Support of the Humanitarian Community in Assistance of the Displaced Population in Kenya” to fill logistics gaps. The SO was to account for the unprecedented need to transport and store relief commodities, as well as to address the challenges created by insecurity that resulted in blocked roads and delays at Mombasa port. Budget: $629,000, duration 9 January to 8 March 2008; scope: provided the humanitarian community with essential services including the provision of road transport and warehousing support to facilitate deliveries of food and NFIs, and air support.
WFP Humanitarian Air Service (UNHAS) facilitated the operation of an Mi8 helicopter to conduct an initial air assessment and air support for staff movements; however, air service was suspended after 14 January when roads became accessible through use of armed escorts and convoys.
In total, thirty-three humanitarian organisations, including the KRCS, participated on a regular basis in Nairobi and the three hubs with Logistics Cluster coordination, and six agencies used the free transport and storage services to their advantage.
Logistics coordination and secondary transport and warehouse services have been provided from the early onset of the crisis for food and NFIs and will continue until the end of May 2008.
51

K E N Y A
Prot
ectio
n A protection
monitoring system of IDP communities and affected populations is developed.
Protection concerns of displaced persons and affected populations are adequately responded to through timely government concerted actions.
Kenya Protection Cluster established with clear terms of reference: Protection Working Groups at field level were established in Eldoret (North Rift), Nakuru (South Rift), Kisumu/ Nyanza (Western) and Nairobi (Nairobi & Central) and are inclusive of key stakeholders including local agencies and responsible entitles.
Protection Cluster strategy and Plan of Action developed. “IASC Steps toward Durable Solutions to Post-elections Displacement in Kenya” drafted by
the Protection Cluster and adopted by the IASC Kenya Country Team: IASC Steps document will be reviewed and updated to include other displacement situations in Kenya.
Cluster membership reinvigorated in September and planning for transition to a national Protection Working Group ongoing: by December, a national Protection/ Human Rights agencies should be identified as Chair.
Protection Cluster members expanded scope of work to include other, non-PEV related conflict and displacement.
Nation-wide training on Guiding Principles on Internal Displacement enhanced understanding of IDP Guiding Principles including rights and responsibilities of IDPs, humanitarian agencies and responsible entities.
Protection monitoring is ongoing in IDP camps, transit sites, host communities and return areas.
Development of Relocation Framework and IOM’s participation to transport IDPs to formal camps and to areas of return.
Trafficking and other forms of irregular migration recognised as important during such periods of internal displacement and resultant mobility.
Child Protection Child Protection sub-Cluster is transitioning to a government chaired (with UNICEF co-chair)
Child Protection Working Group. Child protection database for unaccompanied children and other protection concerns
developed with the Ministry of Children’s Services. Establishment of the Inter-agency Database on Separated Children at a national level;
worked with Department of Children Services to develop a Collaborative Programme of Response to the issue of separated children that piloted a systematised process of identification, documentation, tracing, reunification and mediation (IDTR&M) for children placed in charitable children’s institutions and living in child-headed households.
Drafting and adoption of National Guidelines on Emergency Post Disaster Psychosocial principles and Response and through a number of collaborative training initiatives and programme actions; operationalise the child-friendly space concept in areas affected by post-election violence.Child Protection in Emergency (CPiE) specific Emergency Preparedness Post-election Affected Areas.
Response Planning workshop for child protection partners as a first step towards establishing a national coordination mechanism addressing coordination and capacity-building for partners engaged in both natural disaster and conflict crises in Kenya.
Cluster lead agency had limited Kenya IDP experience prior to emergency.
Initial scope of cluster was limited to post-election violence. Good NGO/ agency capacity at Nairobi/ national level but
limited implementation capacities and limited funding for projects at field level.
Need for all protection agencies, local and international, to have clear terms of reference and capacity to implement outside Nairobi.
Protection incident and monitoring reporting system should be established and reinforced.
Limited cross sectoral planning and activities with Early Recovery Cluster.
Lack of funding limited protection services at field level.
Child Protection No national level child protection in emergency coordination
body prior to the onset of post-election violence. Need for greater understanding among partners about the
differences between community-based psychosocial actions versus trauma counselling.
Human resource (HR) constraints in re: trained/experienced CPiE personnel and limited national level NGO partners with chid protection specific experience.
No standard operating procedures in place for prevention and response to separated children.
52

K E N Y A
GBV GBV sub-cluster established and GBV strategy
developed. Inter-agency rapid GBV assessment conducted
Jan/Feb by UNFPA, UNICEF, UNIFEM, and CCF in main affected areas Rift Valley, Central Province, Mombasa, Nairobi, Nyanza
Training to government, UN, INGO and NGO partners in field sites throughout Kenya on sexual exploitation & abuse; GBV prevention & response, and gender mainstreaming (based on IASC guidelines)
Development of standard operating procedures (SOPs) including data collection tools, and training of approximately 280 actors on the SOPs.
Initial development of a GBV Information Management System
Preparation and support to 75 survivors of violence from around Kenya to testify during the ‘Commission of Inquiry in Post Election Violence’: approximately 20 of whom, testified.
Gender based violence training and advocacy underway to address reported sexual exploitation and abuse in IDP camps.
Advocacy undertaken on key protection concerns, including voluntariness of movement.
GBV Lack of experienced GBV field-based staff
to ensure field level coordination and capacity-building
Gaps in the health, security and judicial sectors which make it difficult for survivors to receive comprehensive, and life-saving care based on the guiding principles
Insufficient resources for local organisations to scale-up programming
53

K E N Y A
Nut
ritio
n Support the
Ministry of Health (MoH) to deliver integrated nutritional actions for both IDP and host populations.
Support integrated nutritional actions and accelerate the re-establishment or establishment of efficient routine services.
Technical and logistical support to MoH provided by UNICEF, WFP and Partners (i.e. Samaritans Purse, World Vision [WV], IMC, Merlin, Action Against Hunger [AAH], Concern Worldwide) to scale up diagnosis and management of acute malnutrition
Training of about 150 health workers in management of acute malnutrition. As a result, 93,000 children under-five affected by moderate malnutrition and 5,000 affected by severe malnutrition were treated and levels of acute malnutrition were kept below 5%.
Training of health workers in infant and young child feeding practices (health facility and community). As a result, 65 health facilities offering maternity services will be ready for external assessment for Baby Friendly accreditation by January-February 2009.
Technical support to MoH for nutrition surveillance provided by Save the Children in five provinces. As a result, monthly situation reports, improved monthly reports from health facilities and updated response matrix were circulated to partners; a capacity assessment of health systems was conducted and recommendations shared to partners and; six nutritional surveys conducted in Rift Valley and Central Provinces.
Insecurity affected timely supplies of essential commodities and technical support.
Resettlement process affected continuation of nutrition services and follow-up of cases.
Limited nutrition partners and capacity within government affected (to some extent) interventions coverage.
Very limited capacity of MoH which affected initial response and demanded heavy technical support.
Shel
ter &
NFI
s
To provide sufficient basic domestic and hygiene items and emergency shelter to IDPs and other affected persons.
To ensure access to adequate physical cover, decent living conditions and proper shelter.
Shelter Cluster Strategy Document agreed by all Cluster members distributed in March: established beneficiary criteria, standards for implementation including minimum project elements such as community mobilisation, self help, peace and tolerance etc.
Finalised the Transitional Shelter Kit (TSK) design and project document in March: revised Shelter Project in September in line with the MoSSP/ UNDP Low Cost Shelter project aiming to construct 40,000 houses.
Revised Shelter design, bill of quantities and procurement in line with new Low Cost Housing strategy.
Construction of more than 5,700 houses for an estimated 28,500 returnees in Rift Valley by end December (GOAL, Danish Refugee Council [DRC], IOM, KRCS, Italian Cooperation).
Shelter Cluster transitioned to a Shelter Working Group in June when MoSSP assumed chairmanship with UNHCR as co-chair/ secretariat.
NFI Distribution Established and documented NFI distribution and beneficiary criteria. Common standards, content agreed for ‘family kits’ to enable agencies to distribute a
standard kit. Standardised beneficiary targeting criteria. Distribution of NFI to benefit more than 300,000 individuals (all agencies). Distribution of more than 8,000 tents benefiting 60,000 IDPs.
Reporting mechanisms for NFI distribution including beneficiary data and areas of distribution must be strengthened.
In aftermath of Operation Rudi Nyambani, donor reluctance to provide funds through UN either directly delayed or prevented shelter reconstruction.
54

K E N Y A
Wat
er, S
anita
tion
& H
ygie
ne
(WA
SH)
Ensure all IDPs have access to adequate quantities of safe drinking water.
Ensure all IDPs have access to adequate and appropriate safe sanitation.
Ensure all IDPs are reached by hygiene promotion messages.
All IDPs in established IDP camps had access to adequate quantities of safe drinking water. This was achieved by using local sources such as hand pumps, springs or municipal supplies which often involved extension of pipelines to connect the camp. Where these sources were not available water trucking was used. Where traditional sources of water such as unprotected shallow wells, rivers or unprotected springs were close to the camps IDPs often used this water in addition to safe supplies – water treatment chemicals such as PUR sachets & aquatabs (chlorine) were distributed and training given in their use to ensure water was treated & safe for consumption. Chlorine powder was supplied to Ministry of Water and Irrigation (MoWI) and was used to disinfect pumped water supplies to IDP camps & communities. MoWI and Ministry of Public Health and Sanitation (MoPH&S) officers were provided with water quality testing kits and training in their use to monitor water quality in the camps and returnee areas and to respond where water sources were found to be contaminated.
Municipal water supply schemes were repaired with connections made to IDP camps – this also assisted the local communities together with the IDPs who had integrated into them.
All IDPs in established camps were provided with adequate sanitation facilities – i.e. latrines & bathing cubicles. In the early stages of the emergency the Sphere indicators regarding latrine provision were relaxed in line with Sphere guidance notes whilst construction (and the uncertain situation with IDP movement) caught up. In larger camps a group of families were allocated their own latrine with responsibility to manage & maintain cleanliness – this proved to be a very effective method. In smaller camps for example in Police Posts or Church grounds the existing facilities were used – often with specific latrines assigned to the IDPs – this was generally adequate for the smaller numbers of IDPs housed in these situations.
There were no cases of cholera or major outbreaks of WASH related diseases reported in the IDP camps.
Hygiene promotion messages were developed and activities conducted in all established IDP camps. Hygiene Promotion activities were included in all partnership agreements. KRCS, MoPH&S, MoWI as well as NGO partners were active. Activities included placement of hygiene messages with pictures on pit latrines, hand washing places and other strategic areas in all the IDP camps as well as hygiene promotion training in schools. IDPs were briefed on how to maintain their personal cleanliness and their environment in all the IDP camps.
Each camp had a coordinated solid waste management system in place and was supplied with bins, hand washing facilities, wheel barrows, rakes, gumboots and other protective equipment to use for providing a cleaner environment in all the IDP camps. Work was conducted by volunteer IDP groups.
All camps had some form of drainage & vector control mechanisms in place, however the quality & efficiency of these tended to vary from camp to camp depending on the geographical features of the camp & strength of camp management.
The overall response of the WASH sector to the emergency was generally considered to be good in terms of coordination. The activation of the Cluster Approach and available resources especially in terms of information management, fed into the existing Government of Kenya coordination structure, WESCOORD. The participation of the WESCOORD members was very good & district WESCOORDs were established, & proved effective, in the IDP hubs. Many local NGOs and Faith-based Organisations were actively involved & made a major contribution to the response effort.
Some regions did not have reliable water supply due to government rationing – this was most evident after Rudi Nyambani (Operation “Go Home”) where municipal water supplies to larger camps were often cut – this was seen as an attempt to force remaining IDPs out of the camps.
Camps served by municipal mains experienced shortages when electricity was disconnected at the pump stations by the power company due to non payment of bills by the water service providers.
There was a lack of government exhausters to empty latrines which were filled – more latrines needed to be constructed.
Some local authorities banned the construction of new latrines to replace filled ones in some areas – this was seen as an attempt to force IDPs from the camps. Advocacy attempts at local level were usually successful to resolve this issue & lift the ban.
Some hygiene promotion materials were in small print and were not placed on visible locations – also some were too “technical” for public use being more suited to health workers. There is a need to have appropriate IDP hygiene messages & IEC materials available as part of preparedness.
There were many IDPs who did not stay in camps moving instead to integrate into communities and these were difficult to target. Some of these were assisted by the repair of municipal water supplies together with the distribution of NFIs including for example, ceramic water filters for household use.
In areas where there was no available safe proper water source, water trucking was used – this is an expensive & often unreliable task and difficult to sustain. This may have occasionally led to delays in IDPs receiving safe water & may have prompted some IDPs to resort to unsafe supplies.
The efficiency and quality of drainage & vector control mechanisms varied from camp to camp often due to the geographical features of a specific camp.
Following Rudi Nyumbani in early May the IDPs dispersed to many hundreds of “Transitional Camps” in their original home areas – it was impossible to provide the same level of WASH services in these camps due to their location, number and uncertain status and duration. WASH cluster partners assisted with emergency water and environmental sanitation (WES) provisions but levels of service were low compared to those in the established IDP camps. The movement of IDPs to transit camps marked the beginning of the early recovery phase and efforts were directed towards activities to support this such as rehabilitation of community water supplies, latrine construction in schools and hygiene promotion activities in schools & communities.
Funding proved to be a major constraint with little response to the revised Flash Appeal.
55

K E N Y A
Multi - Sector Achievements and Challenges
Sector 2008 Sector Objectives Achievements Challenges/Constraints
Wat
er, S
anita
tion
and
Hyg
iene
Pro
mot
ion
1. All refugees and asylum seekers have access to safe and adequate potable water.
2. Refugees and asylum seekers are protected from disease outbreaks through the provision of sufficient and suitably located sanitation facilities.
3. Reduce the risk of diseases through promotion of best hygiene practice and vector control within the camps.
In Dadaab, about 17 litres of safe water provided to each individual refugees and asylum seeker per day.
In Kakuma, about 23 litres of safe and clean water provided to each individual refugee and asylum seeker per day.
Current latrine ratio remains at 1:19 in Dadaab (down from 1:21 in 2007) and 1:13 in Kakuma camps. At least 30,000 more latrines required fro current population.
Limited levels of hygiene promotion conducted although more needs to be done. Two rounds of Indoor Residual Spraying (IRS) carried out in all camps. 95% of houses
sprayed. Food premises inspection regularly done at Butcheries, Hotels, Tea rooms, Shops,
Groceries, animals and around the market. Cleaning materials and supplies including wheelbarrows, brooms, rakes, gloves, and spades
and disinfectants supplied to reception centres and transit centres.
Dilapidated infrastructure and thus leakages and wastage of water. Difficulty in meeting set targets with existing resources due to
Dadaab Population increase; in addition high livestock population puts pressure on water resources.
Low community participation in water supply management. Soil texture is poor and has very poor water retention levels implying
that latrines get filled within short periods of time (on average one month as opposed six months to a year).
Due to soil texture (sandy soils) it is impossible to achieve requisite latrine depth.
Low level hygiene promotion due to inadequate funding. In Dadaab, increase in population size remains a major challenge as
it is difficult to achieve targets. Illegal slaughter slabs by the local community compromise the
quality of meat and increase sanitation and hygiene promotion problems.
56

K E N Y A
Sector 2008 Sector Objectives Achievements Challenges/Constraints
Hea
lth
1. All Refugees and asylum seekers have unfettered access to quality health care
2. There are adequate safe motherhood and reproductive facilities in all the camps.
3. Prevention, care and support mechanism for HIV/AIDS in place in all camps.
Only 40% of refugees and asylum seekers have access health facilities at a time. Condoms are available at all health and Voluntary Counselling & Testing (VCT) facilities and
usage is 0.07/person/month (below WHO standards). VCT coverage is 98%, Prevention of Mother to Child Transmission (PMTCT) coverage is
79% and 27 AIDS patients are on ARV treatment & are being monitored. Construction and equipping of theatre, maternity ward, delivery rooms and Pediatrics Ward
at Hagadera Hospital completed. Vaccination coverage for all antigens 100% in all camps. Mental Health clinics functional in camps and 80% of patients have access to treatment
including counselling. Community Mental Health Teams in place, supported and operational. TB activities integrated into the national TB Programme. Emergency Preparedness Plans for Malaria, Cholera, and Avian Flu in place.
Ratio of beneficiaries to health facilities still very high at an average of one health centre to 23,000 Beneficiaries in Dadaab and 1: 17,000 in Kakuma.
Very few medical personnel to serve refugees. Doctor to patient ratio still high (there are three doctors in Kakuma and five in Dadaab).
Rise in refugee population overstretching the existing facilities, human resources & drug requirements.
Levels of malnutrition remain below WHO standards. Maternal Mortality Ratio of 298 per 100,000 live births (still very
high). Cultural barriers to family planning hinder progress. Most health facilities are in a dilapidated state and need repair. Commercial sex work remains an obstacle to HIV/AIDS prevention
and behaviour change. No x-ray facilities in Dadaab making it difficult to treat TB patients. Insecurity and poor road network in some firewood harvesting areas.
Nut
ritio
n
1. Vulnerable refugees are provided with supplementary and therapeutic feeding.
2. Refugees and asylum seekers are provided with complementary food to cover micronutrients deficiencies in the regular food basket.
57,000 new asylum seekers provided with three meals a day at both reception centre & transit Centres as they wait registration.
653 MTs of Green Grams and 653 MTs of groundnuts distributed in Kakuma (136) and Dadaab (517).
Therapeutic Foods provided to severely malnourished children in all camps and Supplementary Foods provided to moderately malnourished children under-five, vulnerable persons, pregnant and lactating mothers and chronically ill persons.
Beneficiaries’ sell part of their food ration to buy commodities that are not provided in the WFP food basket, e. g. firewood, Sugar, milk, meat, clothes, etc.
Current complementary food need for all camps is 2,400 MTs of Green grams and 2,400 MTs of Groundnuts thus unmet gap of 1,747 MTs of green grams and 1,747 MTs of ground nuts.
57

K E N Y A
Sector 2008 Sector Objectives Achievements Challenges/Constraints
Shel
ter &
NFI
s
1. Refugees and asylum seekers have adequate and secure shelter.
2. In consonance with the refugee community, carry out camp planning exercise.
3. All refugees receive 250 gms of soap per day for personal hygiene.
4. Refugees receive adequate household supplies for cooking and water storage (kitchen sets, blankets and water containers).
Three sheds repaired and 60 tents pitched at reception centres. In Dadaab, 17 new blocks demarcated and allocated to 8,174 new arrivals. 1,849 new shelters constructed in Dadaab. 1550m of bushes cleared off the road sides in Kakuma. 400m of road repairs completed. Refugees receive 125 gms of soap per person per month in Dadaab (standard is 250
gms/p/mth) and 250 gms/persons per month in Kakuma. New arrivals registered and provided with NFIs (Blankets, water storage containers and
kitchen sets). In all camps, targeted distribution to families of five individuals or more (base year was
1992) and persons with special needs (i.e. over 50 years). 8% of total firewood requirements provided to all beneficiaries.
Host communities living around the camps interfere with camp planning, demarcation of plots and markets plots allocation.
Availability of soil for construction of houses is a major challenge. In Dadaab, increase in population has affected meeting of
targets/standards (11-13% adequate dwellings against a standard of 100%).
Camps over congested and there is no space for new arrivals. Lack of efficient substitute energy in lieu of firewood. Difficulty in identification of beneficiaries to current stock balances
of NFIs. Inadequate funding for provision of NFIs for family size 1 – 4. Firewood expensive and difficult to harvest. Beneficiaries sell their NFIs in the local market in order to purchase
other essential items e.g. clothing, meat, vegetables and education).
Educ
atio
n
1. All refugees and asylum seekers have unfettered access to quality basic education
2. All refugees receive peace education
3. All education infrastructure meets requisite standards
Construction of 16 new class-rooms in Dadaab meeting 13% of needs. Education materials purchased for all schools to cover 13% of needs. Furniture purchased to cover 13% of needs. 2309 (654 girls) for KCPE and 496 (91 girls) for KCSE were registered. 15 students with special needs are in special institutions at primary and secondary levels,
and technical training institutes. Peace education covered in all schools.
Cultural barriers and awareness on the importance of education mostly for girls.
Most school buildings are in a state of disrepair. Insufficient latrine coverage in schools. More textbooks and furniture required in schools (current
student/textbook ratio is about 1:4). Lack of and high turnover of teachers. Need to procure supplies for children with special learning needs
(e.g. hearing aids & Braille machines) and improve existing infrastructure to cater to them.
58

K E N Y A
Sector 2008 Sector Objectives Achievements Challenges/Constraints
Ref
ugee
Pro
tect
ion
and
Lega
l Ser
vice
s
1. Refugees and asylum seekers are fully involved in programme design and decision making.
2. All new arrivals benefit from a fair and efficient registration and RSD system.
3. Delivery of durable solutions for all refugees.
4. The security and safety of all refugees and their property is guaranteed.
Security improved at transit centres, reception centres and within camps. 11,000 Sudanese refugees repatriated. Community Peace and Security Team (CPST) established (30% women and nine persons
from the local community). 30% Reduction in cases of SGBV. Education on substance abuse, career guidance, reproductive health, girl child education
and Female Genital Mutilation (FGM) done. 213 (85 female) new members recruited for peer counselling. 509 cases (2,346 individuals) submitted for resettlement; 155 cases (533 individuals)
resettled in third countries; and ten cases (52 individuals) resubmitted. Magistrate mobile court in place to expedite justice to aggrieved parties. Monthly baby registration conducted and 90% birth certificates issued by civil registrar. GoK issuing movement passes assisted by UNHCR. Child-friendly spaces constructed in all camps (one per camp). All SGBV survivors provided with shelter material. Provision of material support for identified vulnerable children and foster parents (i.e. NFI)
and monitoring of foster care arrangements.
Human resource required to process new arrivals. Current capacity is 25%.
Family tracing in Somalia through International Committee of the Red Cross (ICRC) is not possible with current situation.
Resources for Verification Exercise diverted to meet demands for the registration of new arrivals, hence Verification is on hold.
Recent arrivals are not aware on the modalities to obtain Registration services (family reunification, loss/stolen cards, ration card merger/separations etc.).
Verification Exercise for entire camp population still on hold due to ongoing influx.
Police ill equipped making quick and rapid response to security issues difficult.
Insufficient female officers and inadequate daily deployment of officers at the stations.
Population too large for the present Community Police Teams coverage.
Commercial Sex Workers (CSWs) and their family members discriminated against within the community.
Uncircumcised girls face stigma and discrimination. Security in Kakuma remains a major challenge as some areas
within the refugee camps have been vacated leaving a security vacuum.
59

K E N Y A
ANNEX II. STRATEGIC FRAMEWORK FOR HUMANITARIAN RESPONSE
Strategic Priorities 1. Timely, coordinated humanitarian assistance and protection is provided to highly vulnerable populations affected by natural and man-made disasters in accordance with
internationally accepted norms and standards.2. Early recovery initiatives are linked with longer term programming to reduce vulnerability and strengthen resilience among vulnerable populations.3. Strong linkages with conflict mitigation, peace building and reconciliation initiatives are integrated within humanitarian action.4. The capacity of national institutions and networks is strengthened to enhance coordination, undertake humanitarian policy development, and promote
effective emergency preparedness and disaster risk reduction.Sector Sector Objective Strategic
priorityArea of Focus Activities Target Indicators Organisations
Coo
rdin
atio
n
Ensure effective and inclusive coordination of humanitarian assistance at a technical and decision making levels
1, 2, 3 National Facilitate coordination through support to cluster / sector working groups, the Kenya Humanitarian Forum and provide support to government partners including the MoSSP
Support the HC office in humanitarian coordination and disaster risk management including through the IASC
At least 50 organisations participate regularly in coordination fora
100% of recommendations and action points from coordination fora shared through the dissemination of minutes
OCHA, cluster, IASC members, Government of Kenya, national NGOs
Strengthen national coordination capacity at centralised and sub-national levels
4 National Support capacity development of national coordination structures including through the transition of the cluster approach
Participate in and support district level coordination structures
At least 50% of clusters transition into national structures
OCHA, cluster, IASC members, Government of Kenya, national NGOs
Strengthen preparedness activities, including inter-agency contingency planning
4 National Provide support on early warning to national and district level partners
Review early warning and preparedness capacities in relation to sudden onset disasters
Provide learning opportunities and technical capacity-building for disaster managers
Facilitate the development and inter-agency strategies for humanitarian response and disaster risk management
Number of early warning SOPs developed for select districts
Workshop held on disaster risk management
Inter-agency multi-hazard contingency plan developed and agreed
OCHA, cluster, IASC members, Government of Kenya, national NGOs
Ensure the information needs of the humanitarian community are met
1,2,3 National Prepare and disseminate reports including situation updates, analytical reports and 3 W information
Raise awareness on emerging or under-reported issues
Map vulnerabilities and capacities Maintain humanitarian website as a platform for
sharing analytical information Facilitate the development of inter-agency tools Facilitate regular consultative and information
sharing meetings Support the establishment and function of the Kenya
Humanitarian Information Management network
At least 15 analytical reports produced or presentation made to humanitarian community
3 Ws in place for all clusters / sectors Website maintained and regularly updated At least 12 maps produced KHIMN established and functioning
OCHA, cluster, IASC members, Government of Kenya, national NGOs
60

K E N Y A
Raise awareness and mobilise effective humanitarian action
1 National Produce and disseminate advocacy materials to identified target audiences
Analytical briefings developed on key humanitarian issues
Engage partners, including media to raise awareness on key issues of concern
Ensure regular consultation through the advocacy working group
Advocate for resources including through the EHRP
Advocacy materials produced and disseminated on key issues
Increased coverage of humanitarian issues in local media
At least four consultations held through the advocacy working group
At least 60% of funding requirements met
OCHA, cluster, IASC members, Government of Kenya, national NGOs
Early
Rec
over
y an
d Fo
od S
ecur
ity
To provide quality and appropriate inputs to contribute to the food security of vulnerable farming households through crop and livestock production during the long rains of March and the short rains of October 2009
1 Areas affected by post-election violence
ASAL
Identification and sensitisation of households vulnerable to food insecurity
Agricultural input procurement and distribution Provision of agricultural inputs and implements to
affected communities Training on diversified and alternative farming
methods Assistance to vulnerable households to enhance
and protect livestock assets Development of protocols and guidelines for
livelihood support for People Living with HIV/AIDS (PLHIVA), affected families and other vulnerable groups, including People Living with Disabilities (PWDs)
Enhance linkages between HIV community-support groups and humanitarian actors
Impact assessments
Increased productivity of food crops on farm holdings
Enhanced access to food for affected families and vulnerable groups, such as PLHIVA
Stabilised food prices in the project areas Acreage cultivated
FAO WV
To enhance livelihood opportunities for vulnerable populations
2 PEV-affected areas
ASALS
Collection of qualitative and quantitative disaggregated data to enhance tailoring of livelihoods actions
Skills development training Facilitation of access to credit and entrepreneurial
opportunities Development of protocols and guidelines for
livelihoods support for PLHIV, affected families and other vulnerable groups including PWDs
Documentation and dissemination of best practices in livelihoods actions
Number of men and women engaged in livelihood activities
Number of men and women trained Community support mechanisms
established and operational assisting vulnerable persons, such as PLHIV in the rehabilitation/reconstruction of sustainable livelihoods
Increase in diversification of livelihoods
IRC
DRC
UNDP
61

K E N Y A
To support national and community-based peace and reconciliation initiatives to facilitate return and reintegration of displaced persons
3 PEV-affected areas
Resettlement areas
Engage communities in peace building and reconciliation activities
Training of District Peace Committee members Creation of linkages and synergies among peace
actors at the community level Facilitate effective linkages for newly created district
peace committees through influencing existing local development authorities to incorporate conflict sensitivity planning
Inclusion of HIV programming for demobilised forces including men, women, boys and girls
Strengthening on-going reconciliation efforts between communities through providing localised structures and mechanisms for mediation
Documentation and dissemination of best practices in community peace building initiatives
Number of returnees returning to settle on their farms
Number of active and effective District Peace Committees
Number of arms collected Number of rehabilitated militia Number of localised community social
contracts between communities at site level in areas affected by the PEV
Linkages established within the newly established District Peace Committees to support implementation of the social contracts
UNDP
ACORD
PeaceNet
To harmonise disaster preparedness and disaster response plans, particularly at the community-level
4 National, provincial, district
Support disaster preparedness, mitigation and management by assisting development of contingency plans
Awareness rising on disaster preparedness and climatic changes
Building capacity of local government and communities to respond to disasters through technical assistance
Assisting with the establishment of disaster management sub-committees
Number of districts with harmonised disaster preparedness and disaster response mechanism plans available
Number of districts targeted for community awareness-raising campaigns
Food
aid
and
Nut
ritio
n
Stabilise and reduce vulnerability to hunger resulting from shocks (e.g climatic disasters, rising food prices)
1 ASAL areas, Post-election violence affected and urban poor
Distribution of food and non-food items in sufficient quantities and quality to targeted populations
Food for assets and voucher schemes Provision of essential supplies including
anthropometric equipments, feeding kits, therapeutic and supplementary foods and micronutrients
Overall: Levels of acute malnutrition reduced to 10%
% households accessing adequate food rations
100% of affected districts received timely and adequate supplies
WFP
WFP and UNICEF
Ensure that essential nutrition services are delivered to affected populations
1 ASAL areas, PEV-affected and urban poor
Capacity development in management of acute malnutrition and infant and young children practices
Technical and logistical support for diagnosis of acute malnutrition and referrals for adequate management at health facility and community levels
Technical, logistical and human resources support in management of acute malnutrition, protection and promotion of infant and young child feeding practices, routine and curative micronutrient supplementation
Communication of key messages at health facility and community levels
# of health workers trained in management of acute malnutrition
50% children affected by acute malnutrition are diagnosed and referred for adequate treatment
60% health facilities offering essential nutrition services in affected areas as per standards
60% health facilities offering maternity services certified baby friendly in targeted areas
UNICEF, NGO partners and MoH
62
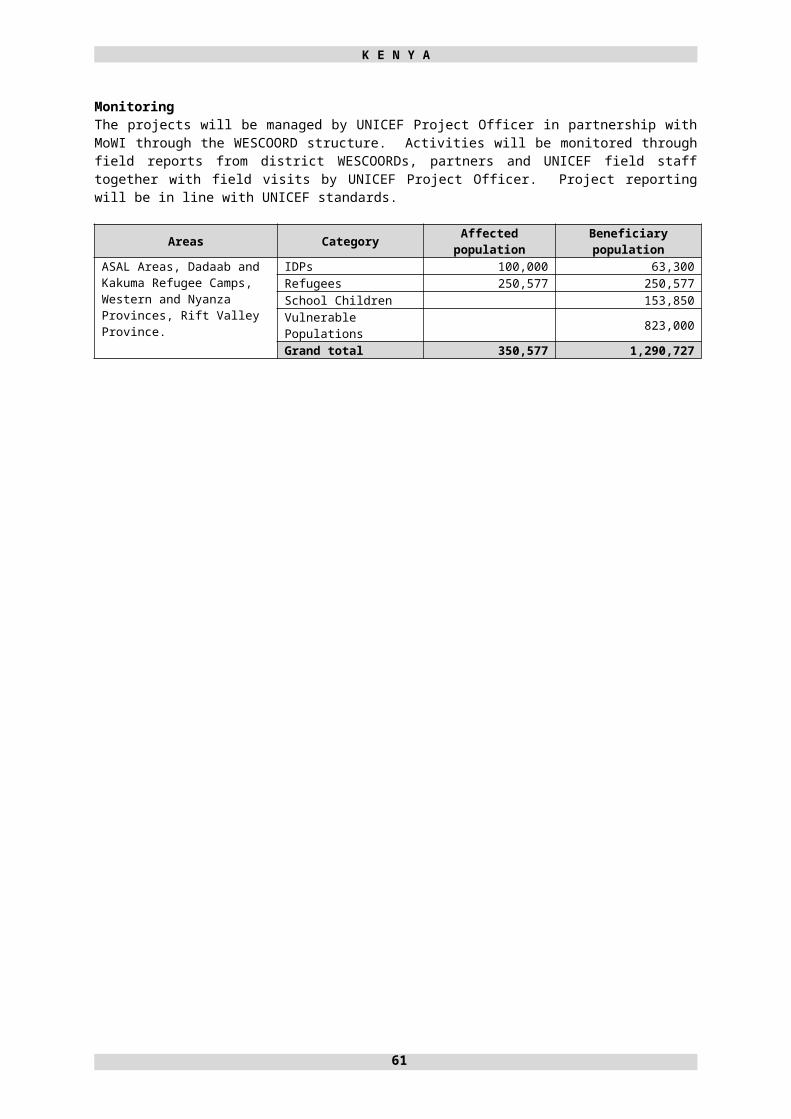
K E N Y A
Ensure that efficient coordination mechanisms are in place at national and sub-national levels
4 ASAL areas, PEV-affected areas and urban poor
Support for improved coordination mechanisms and linkages with other sectors at national and sub-nation levels
# of districts / provinces with functioning coordination structures led by MoH
UNICEF, NGO partners and MoH
Maintain efficient nutrition surveillance systems
4 ASAL areas, PEV- affected areas and urban poor
Monitoring, surveillance and assessment of household food security and nutrition
# of districts / provinces providing timely surveillance / monitoring reports
UNICEF, NGO partners and MoH
Hea
lth
To reduce avoidable morbidity and mortality among: refugees; IDP;, severely
malnourished vulnerable groups
especially children under-five and lactating and pregnant women in the camps and their host communities and the drought stricken areas
1 PEV-affected areas
ASALS
Areas hosting IDPs and refugees (local population)
Establish emergency early warning systems for (disease, malnutrition and water quality surveillance) in refugee camps and districts affected by drought and disease epidemics
Provide basic field laboratory investigation package for 30 districts and four provincial hospitals for diseases of epidemic potential
Training for partners on diagnosis and management for diseases of epidemic potential, special conditions for vulnerable groups
Hire short-term local staff for disease outbreak response
Procure PPE for haemorrhagic fever Procure disinfectants for cholera treatment units and
other isolation wards Train and equip district and provincial emergency
health response teams in 30 districts hosting IDPs, refugees and in the ASAL areas on emergency preparedness and contingency planning
Conduct joint rapid health and nutrition assessments and emergency activities monitoring among the vulnerable populations
Training of health workers for psychosocial support for themselves and hospital patients
Provide basic health care services Provide essential secondary health care drugs, kits
and services for special vulnerable groups such as HIV, TB, psychosocial
Facilitate health activities coordination and information management among IDPs and refugee camps and ASAL areas
Joint emergency health response plans developed for each disaster and refugee camps
Monthly monitoring visits to affected areas reports
Reports of joint rapid health and nutrition assessments conducted timely
80% of basic health care service providers using standard Guidelines
At least 95% of children less than five years immunised against measles in the refugee camps
Number of reported disease outbreaks investigated and responded to within 48 hours
80% supervised delivery and post natal care among refugees
Weekly coordination meetings held at each level (National, provincial and district)
Weekly epidemiological bulletin on vulnerable populations published and disseminated
WHO, IOM, MoH, Provincial Health Teams, DHTs, MERLIN, IRC, GTZ, Health NGO Network HENNET Members and FBOs
63
K E N Y A
Mul
ti Se
ctor
ass
ista
nce
for r
efug
ees
All refugee families have access to adequate feeding
GAM and SAM levels < 10% and <3% in all camps
1 Nairobi (Urban refugees) Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
Provision of incentives to increase attendance in growth monitoring
Conduct regular nutrition trainings among refugee community and incentive staff
Procure complementary foods for special high risk children and other highly vulnerable groups
Provide nutritional support and care to the chronically ill and people living with HIV/AIDS
Support kitchen gardening. Community mobilisation and trainings on prevention of
micro-nutrient deficiencies Enhance community based care for severely
malnourished children Provide adequate and appropriate Ready-to-Use
Therapeutic Foods, such as Plumpy Nuts Promote best infant and maternal feeding practices,
such as breast feeding and weaning practices Conduct two cross-sectional nutrition surveys to
monitor malnutrition trends and morbidity in each camp
Conduct three vitamin A and two de-worming campaigns in all camps
SFP recovery rate=>92%, death rate=0%; defaulter rate<6%; SFP coverage for under fives>72%; PLP coverage>82%.
TFP coverage>50%; recovery rates>66%; death rate<4 %; defaulter rate<5%
GAM<10% and SAM<2%. Provide for alternative feeding options for
children born to HIV+ mothers
GTZ, IRC, NCCK, UNHCR
Refugees receive adequate (at least 20 l/p/d) and safe potable water
Refugees have access to safe water
Refugees’ water storage is safe and free from contamination
Reduction of HIV/AIDS prevalence and increase awareness through HIV/AIDS mainstreaming in the water sector
1 Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
Upgrade water system efficiency through acquisition of service materials, standby equipment and construction of buffer tanks to forestall failures in the system and meet demand requirements
Conduct monthly hygiene promotion/awareness campaigns on safe water storage
Install additional water distribution points Increase number of water pans available for livestock Build refugee water management capacity Extend water supply system to new sites Acquire suitable equipment for emergency water
supply, e.g. water bladders, water tanks, pillow tanks, water bowlers, etc
Regular maintenance of water systems (at least once every month)
Increase water supply system efficiency by phased replacement of ageing equipment22
Connect water to schools’ latrines, blocks and hand washing facilities
Drilling and commissioning of two additional boreholes Support to host community (boreholes and water
pans) Refugee communities and PLWA are involved in
planning, designing and implementation of water systems and water systems management
SFP recovery rate=>92%, death rate=0%; defaulter rate<6%; SFP coverage for under fives>72%; PLP coverage>82%.
TFP coverage>50%; recovery rates>66%; death rate<4 %; defaulter rate<5%
GAM<10% and SAM<2%. Provide for alternative feeding options for
children born to HIV+ mothers
DRC, GTZ, IRC, NCCK, UNHCR
22 Generators and pumps
64

K E N Y A
Ensure that refugees have access to adequate and safe sanitation facilities
Reduction of HIV/AIDS prevalence and increase awareness through an integrated approach to HIV/AIDS mainstreaming in the sanitation sector
Refugees are aware of best hygiene practice
Refugees and host communities live in a health and sanitary environment
Refugees have means of safe waste disposal
All meat and food consumed is of the highest health standards
1 Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps)
One hygiene promotion campaign conducted every month
11,000 latrines constructed One bathing shelter per refugee family constructed One communal garbage pit for four refugee families
dug Undertake two camp wide residual spraying cycles
targeting at least 90% of all camps Daily inspection of all food premises within the
camps All slaughter slabs within camps well maintained Quarterly disinfections of at least 95% of latrines Support Public Health Department in sanitation and
solid waste management in host community Involvement of refugee communities and PLWA in
the planning, designing and implementation of sanitation and hygiene promotion programmes
The latrine/user ratio is 1:14 11,000 latrines constructed in Dadaab and Kakuma camps At least 12 hygiene promotion campaigns
conducted (one per month) All dilapidated sanitation facilities
rehabilitated No incidences of communicable diseases No incidences of violence or security
breaches at sanitation facilities
NRC, IRC, DRC CARE, UNHCR
65

K E N Y A
All refugees have access to primary health care
Strengthen Reproductive Health (RH), Family Planning and HIV/AIDS awareness
Voluntary Counselling and Testing (VCT), PMTC) services among refugees fully utilised
Reduce levels of anaemia
1 Nairobi (Urban refugees) Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
Maintain antenatal care coverage at 90% and increase post natal care coverage to 60%
Increase number of skilled deliveries One additional midwife per camp hired Three additional female health workers hired per
camp 25 traditional birth attendants (TBAs) are hired One RH community sensitisation activity held per
month on RH issues At least one night ambulance provided at camp level 24 hour communication system established within
camps Provide hospital inpatients with a balanced diet Provide nutritional support and care to the chronically
ill and people living with HIV/AIDS Provide 50,000 LLITNs Retreat about 25,000 (5,000 in Kakuma and 20,000 in
Dadaab) existing nets that have lost their protective efficacy
Procure adequate Rapid Diagnostic Test kits for 2009 Maintain Intermittent preventive treatment for all
pregnant mothers attending ANC clinics
Increase number of primary health facilities MMR<2/1,000; CMR<3/1,000;
IMR23<60/1,000 births; Crude MR<1.5/1,000 ANC coverage>90% and PNC
coverage>60% Ratio of TBA: population=<1:3500 (25 TBAs
are hired) Four female midwives hired 45% hospital deliveries 12 RH sensitisation workshops conducted Night duty ambulances in place in all camps 24-hour duty roster in place in RH units Reduction in HIV/AIDS prevalence Reduction in mother to child transmission of
HIV/AIDS No incidences of stigma and discrimination
among those affected and infected by HIV Increased number of primary health facilities Anaemia among children and women<45% Reduction in prevalence of substance abuse
among refugees and host community 100% identified pregnant mothers receive
community based ANC services 85% of the community access health
education messages on HIV/AIDS 30% Increase in VCT candidates 30% increase in access to RH services and
facilities 100% mothers who visit for ANC receive
PMTCT services Provide for alternative feeding options for
children born to HIV+ mothers Sensitize community on HIV/AIDS trans-
mission, control and availability of HIV/ AIDS services with various partners.
Increase in number of skilled deliveries to over 50%
GTZ, IRC, NCCK, UNHCR
23 MMR is Maternal Mortality Rate, CMR is Child Mortality Rate and IMR is Infant Mortality Rate.
66

K E N Y A
All refugees have access to adequate shelter
All refugees are equipped with construction and maintenance skills
Kakuma airstrip is in good working/usable condition
1 Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
Implementation and enforcement of compliance with site plans being honoured
Community structures for site planning put in place Access roads being marked for rehabilitation and
maintenance Repair 500 metres of Kakuma airstrip and regular
maintenance of airstrip Construct 7,000 new shelters (6,000 in Dadaab and
1,000 in Kakuma) and rehabilitate dilapidated shelters (10–15% of shelters for persons with special needs)
Consolidate Kakuma camp as part of rationalisation of programme implementation and security management
7,000 new shelters constructed Refugees construct and, or repair their own
houses/shelters All refugees live in safe and well constructed
houses of at least 3.5 m2 per person Transport to and from Kakuma by air is safer
and without undue delays All access roads are well maintained and
functional in keeping with standards No security incidences No dilapidated structures in camps Kakuma infrastructure rationalised and
operating at optimum level
NRC, NCCK, UNHCR
All refugees and asylum seekers of school going age have access to education (100% school enrolment)
100% refugees and asylum seekers who enrol in education programmes graduate (100% school retention)
Refugee schools are efficiently and effectively managed
1 Nairobi (Urban refugees) Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
At least three parents-teachers meetings held per year per school
Three new primary schools constructed in Dadaab camps
55 new classrooms constructed across Dadaab camps Student intake increased at secondary school level Online secondary education established through the
Research Experience for Teachers (RET) Programme and the MoE
Textbooks, teacher guides, furniture and other requisite education materials procured and used
Peace education conducted among refugees Increased participation and performance in co-
curricular activities within the camp to stimulate better academic performance
Four pre-schools to be fully run and managed by community in Kakuma
Maintain 13 primary schools and one secondary school at cost free basis
Maintain average classroom to pupils ratio at 1:45 Increase enrolment of girls by 80% Repair 20 classrooms in Kakuma to improve learning
environment
All planned materials and textbooks procured 100% refugees and asylum seekers of
school going age in school Refugees live in peace and harmony with
each other (refugee co-existence enhanced Learners to classroom ratio<1:45 Improved learning environment in order to
make it child and learning friendly for better performance
Community based school management system established; Committees making decisions over school general management and plans for improvement of standards
Desk to learner ratio=1:3 (primary) & 1:2 in secondary
Book to learner ratio in core subject=1:3 10% improvement in performance of learners
in national examinations Gender parity in all schools and transition to
next education level Average daily attendance of learners>85% Increase performance of girls: boys at
50% :70%, respectively Four pre schools fully managed by
community 13 primary schools and one secondary
school cost free Girls enrolment increased by 80% 85% retention of girls in school Average daily attendance of learners is 95% Community participation/ contribution in
running of schools is 50%
NRC, CARE, LWF, UNHCR
67

K E N Y A
Refugees and asylum seekers are fully protected as per the Refugee Act, 2006, international laws, conventions and protocols
Government has capacity to protect refugees through systematic and accurate implementation of the Refugee Act, 2006
Registration and RSD procedures are consistent with international standards of quality and fairness
All refugees have access to durable solutions as a means to alleviating their suffering
Refugees are free to move within and outside of camps for work or personal reasons
1 Nairobi (Urban refugees) Dadaab (Ifo, Dagahaley and Hagadera) and Kakuma refugee camps
200 refugees integrated locally (in Kenya) as part of implementation of Refugees Act, 2006
5,000 refugees resettled in third countries 20,000 Sudanese voluntarily repatriated (both UNHCR
assisted and spontaneous) to their country of origin UNHCR will advocate for the opening of the Kenyan-
Somalia border to enable Somali refugees to safely seek asylum in Kenya
One verification exercise of refugee population conducted in all camps
Request Government of Kenya to issue identity documents to refugees
Administrative and logistical support provided to mobile courts
Training of humanitarian workers, government officials and uniformed services on protection of sexual exploitation and abuse (SEA) in code of conduct as well as mainstreaming of HIV/AIDS trainings an activities in collaboration with food security and other sector
Registration of refugees and asylum seekers completed on the same day or not more than 15 days from day of first approach to the BO Nairobi
Biometrics of all refugees and asylum seekers captured
Exchange of biometrics between UNHCR and GoK done bi-monthly
DRA responds to detention of asylum seekers and refugees within 48 hours
Eight training for police and immigration officers done.
Brochures with information on access to rights, entitlements and services distributed to refugees and asylum-seekers.
Training of the national paralegal network done (to give refugees and asylum-seekers access to low-cost, locally-available legal services).
Asylum claims of UAMs handled expeditiously in line with guidelines and procedures.
Asylum seekers from central and south Somalia have unfettered access to Kenya.
Kenyan government adheres to its obligations on international refugee law and the Refugee Act, 2006.
Mobile courts capacity to deliver justice in a timely manner increased by 50%
100% refugees move freely within and outside the camps
UNHCR, OCHA, GTZ, IRC, NRC, LWF, NCCK, CARE, DRC, RCK
68
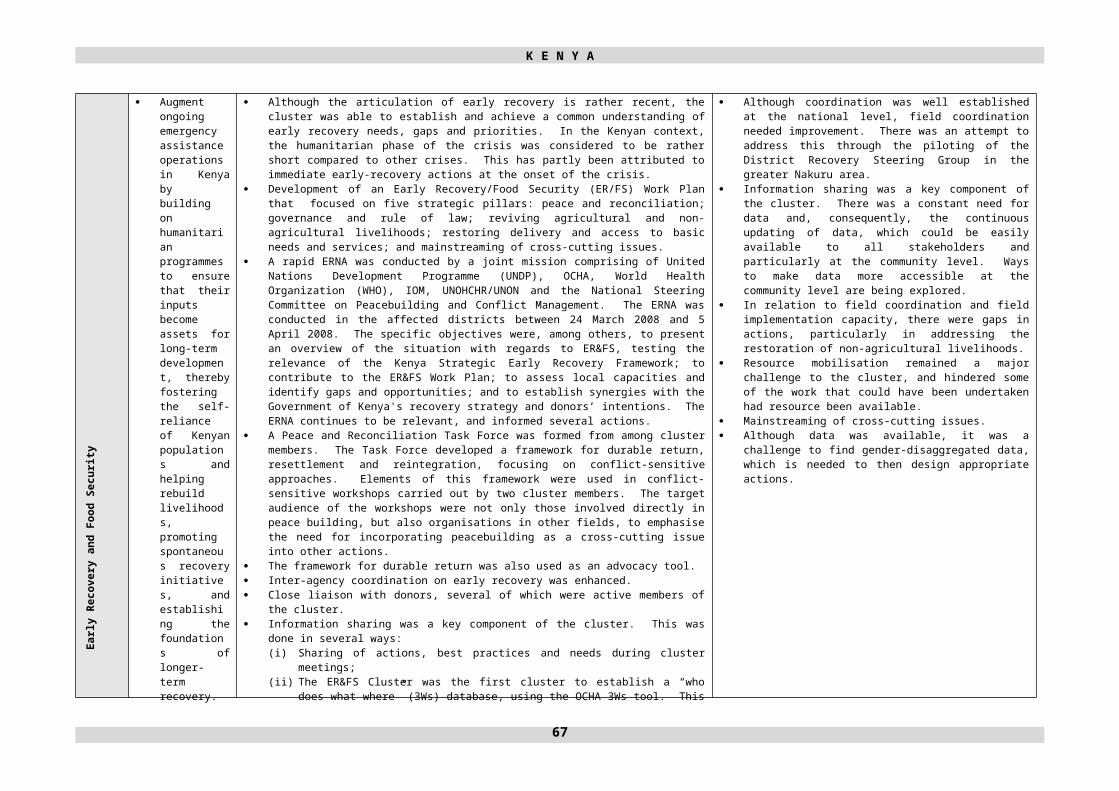
K E N Y A
200 refugees integrated locally (in Kenya) as part of implementation of Refugees Act, 2006
5,000 refugees resettled in third countries 20,000 Sudanese voluntarily repatriated (both UNHCR
assisted and spontaneous) to their country of origin UNHCR will advocate for the opening of the Kenyan-
Somalia border to enable Somali refugees to safely seek asylum in Kenya
One verification exercise of refugee population conducted in all camps
Request Government of Kenya to issue identity documents to refugees
Administrative and logistical support provided to mobile courts
Training of humanitarian workers, government officials and uniformed services on protection of sexual exploitation and abuse (SEA) in code of conduct as well as mainstreaming of HIV/AIDS trainings an activities in collaboration with food security and other sector
Registration of refugees and asylum seekers completed on the same day or not more than 15 days from day of first approach to the BO Nairobi
Biometrics of all refugees and asylum seekers captured
Exchange of biometrics between UNHCR and GoK done bi-monthly
DRA responds to detention of asylum seekers and refugees within 48 hours
Eight training for police and immigration officers done.
Brochures with information on access to rights, entitlements and services distributed to refugees and asylum-seekers.
Training of the national paralegal network done (to give refugees and asylum-seekers access to low-cost, locally-available legal services).
Asylum claims of UAMs handled expeditiously in line with guidelines and procedures.
Asylum seekers from central and south Somalia have unfettered access to Kenya.
Kenyan government adheres to its obligations on international refugee law and the Refugee Act, 2006.
Mobile courts capacity to deliver justice in a timely manner increased by 50%
100% refugees move freely within and outside the camps
69

K E N Y A
Prot
ectio
n
Current UNHCR-led protection cluster is transformed into a national protection forum incorporating the protection needs of all persons affected by humanitarian crisis and internal displacement
4 National and field levels throughout Kenya
Liaise with all stakeholders to build consensus on the establishment and leadership of a national protection forum: establish a comprehensive strategy and work plan for the reformed protection forum
Capacity of national independent and NGO protection actors is further strengthened through a variety of capacity-building measures including training and technical support
Linkages with the Government of Kenya and statutory bodies reinforced (MoJ, MoSSP and other linked ministries and offices)
Field level or thematic protection working groups are established
Review of national legislation relevant to achievement of durable solutions and development of and advocacy for a National IDP policy
Ensure that cross cutting issues such as GBV, HIV/AIDS, women’s and children’s issues are mainstreamed into protection activities
National human rights agency assumes chair of the national protection forum, terms of reference, areas of focus, capacity-building plan and comprehensive work plan established by March 2009
Effective and continuous participation of focal points and agencies in the national protection forum
General protection or thematic working groups are established as required
Protection cluster members, national and international protection and human rights NGOs, bodies and agencies KNCHR, UNHCR, OHCHR, UNICEF, UNDP, OCHA, Government of Kenya
To enhance the accuracy of knowledge of the protection environment of persons affected by conflict and displacement in order to better inform and improve programmatic responses, policy development and advocacy activities
4 National, provincial, district, community levels
Profiles of displaced / at risk populations established: Map of protection human rights, rule of law needs established
Strengthen protection and human rights monitoring and response networks through training on data collection, verification, analysis and reporting
Develop SOP for linking protection data with advocacy activities at Nairobi and field level
Make recommendation to all cluster linking protection to programmatic responses
Map of which agency is working where (3Ws), themes and activities
Number and results of trainings on data collection, analysis and reporting
Disaggregated data by age and gender available for IDPs and affected populations
SOPs are drafted: number times data used to develop programmes and mobilise funding and response
Protection cluster members, national and international protection and human rights NGOs. Bodies and agencies KNCHR, UNHCR, OHCHR, UNICEF, UNDP, UNOCHA, Government of Kenya
70

K E N Y A
Create conditions conducive to achievement of durable solutions for persons affected by or displaced including the restoration and reclamation of human rights, justice/ rule of law and access to community and social services and where provided, humanitarian assistance
3 National, Provincial, District, Community
Multi-sector assessments of conflict and displacement situations to identify and address root causes of conflict and displacement and create conditions conductive to return
Peace and reconciliation activities and advocacy are mainstreamed into all activities
Advocacy with government at all levels, donors and national/ international agencies to ensure timely response to the protection, human rights, legal aid/ justice and humanitarian needs of displaced persons and affected populations
Strengthen the capacity of communities to reduce vulnerability and increase protection
Identify and address legal obstacles to individual and group enjoyment of human rights and access to services
Strong linkages with Early Recovery Cluster as well as other assistance agencies and line ministries in areas of displacement
Training of humanitarian workers, government staff and uniformed services on prevention of sexual exploitation and abuse and Code of Conduct in collaboration with food security, shelter, water/ sanitation and other sectors: HIV/AIDS awareness is mainstreamed into trainings and activities including emergency preparedness
Number and types of situations of displacement documented
Number IDPs with enhanced access to social, legal and community services
Number of trainings and persons benefiting from peace and reconciliation skills and civic education, including Guiding Principles trainings
Number of legal cases identified and legally assisted (legal aid, case reviews, litigation)
Protection Cluster Members,National and International protection and human rights NGOs, bodies and agenciesKNCHRUNHCR UNOHCHR UNICEFUNDPUNOCHA Government of Kenya
71

K E N Y A
To ensure child protection prevention and response mechanisms are established in areas affected by conflict and natural disaster, including IDP and refugee populations, with specific focus on capacity-building and CPiE systems development
4 National, Provincial, District, Community
Support establishment of the ‘Child Protection in Emergencies’ national level coordination mechanism, financially, administratively, and through provision of training opportunities for government counterparts and other national child protection partners. (This will include working with other sectors, such as education, social welfare, the judiciary, law enforcement, and health)
Develop and disseminate standard operating procedures on prevention and response to the situation of separated and unaccompanied children, including capacity-building on identification, documentation, tracing, reunification, and mediation, including (but not limited to) continued focus on the children placed in CCIs and part of CHHs
Continue support to child survivors and service providers on prevention and response to GBV through integrated training initiatives, provision of PEP, awareness-raising on HIV+/AIDS, and dissemination of IEC materials
Continue training psychosocial service providers on operationalising community based PSS actions and the concept of child-friendly spaces, with a view towards building national emergency capacity and dissemination of Kenya’s national PSS guidelines and IASC principles on the provision of PSS support
Develop and implement a ‘Child Protection in Emergencies’ advocacy initiative to disseminate information on how to prepare children for, and keep children safe during emergencies
Continue child rights violation monitoring, reporting, and response, including commensurate human right and CRC advocacy activities
National level CPiE coordination mechanism established
CPiE Communication strategy developed and implemented
SOPs are developed and disseminated Number of agencies engaged in child
protection contingency planning process – with corresponding information on ability to contribute insofar as technical expertise, HR and funding
Number of trainings, and number of persons trained on GBV, PSS and U/SC – with corresponding information on how these persons/organisations are engaged in CPiE systems development
Department of Children’s Services/National Council of Children’s Services, KRCS, Children’s Legal Advocacy Network, the CRADLE, NCCK, Child Welfare Society of Kenya, LVCT, The Girl Child Network, ActionAid, RCK, SCA, CCF, IRC, CARE, IOM, UNICEF, WV, DRC
72

K E N Y A
Deliver a set of actions to prevent and respond to GBV in line with the IASC Guidelines for GBV Actions in Humanitarian Settings and other international and national policies, resources, and guidelines in areas affected by conflict and natural disaster, including IDP and refugee populations, with specific focus on capacity-building and multi-sectoral systems development
4 All levels, ie., national, provincial, district and community
Support the GBV Sub-cluster in its transition to the NCGD to ensure a sustainable national level coordination mechanism financially, administratively, and through the provision of training opportunities for GBV partners
Continue roll-out and operationalisation of GBV prevention and response SOPs, including capacity-building on: GBV prevention and response, community mobilisation, case management, setting up referral systems, guiding principles of working with survivors and special considerations for children
Continued support to survivors and service providers on prevention and response to GBV through integrated training initiatives and through the dissemination of IEC materials
Pilot a GBV Information Management System in target areas to improve analysis and understanding of nature and scale of GBV
Develop and implement advocacy/awareness initiatives to disseminate information on ensuring that people know how and where to access services for GBV
Promote access to livelihood opportunities for vulnerable women and girls, including but not limited to, survivors of GBV
Continue efforts to institutionalise actions for prevention of sexual exploitation and abuse by humanitarian workers
Promote access to justice for survivors of GBV Improve capacity among first responders
(emergency actors such as the KRCS) to integrate issues of gender, GBV and HIV/AIDS prevention and response into all emergency actions and contingency plans
GBV sub-cluster, under the leadership of the NCGD continues to map out who is doing what and where
Inter-agency GBV coordination bodies are created and supported in major sites affected by post-election violence and natural disasters
An inter-agency plan of action is created by the GBV sub-cluster under the leadership of the NCGD
Number of persons trained on SOPs, and GBV prevention and response
Number of target locations that have referral mechanisms in place
GBV Information Management System piloted in target locations
Advocacy/awareness workplan created to ensure that people know how and where to access services
Creation of a PSEA focal point network Number of agencies that have focal points
and sufficient Codes of Conduct in place Development of a training module for use
by first responders Number of contingency plans in place that
include gender and GBV and HIV/AIDS prevention and response
NCGD, MoH, MoJ, Police Commission, Department of Children’s Services, KRCS, Children’s Legal Advocacy Network, the CRADLE, LVCT, The Girl Child Network, ActionAid, SCA, RCK, CCF, CARE, IOM, Population Council, COVAW, WEL, UNICEF, UNHCR, DRC
73

K E N Y A
Shel
ter,
NFI
and
CC
CM
Ensure access to adequate physical protection, decent living conditions and proper shelter
1 PEV-affected areas, Mount Elgon, areas of conflict or natural disaster with shelter damage or areas with assessed humanitarian needs
In coordination with MoSSP, local officials and communities, quantify overall shelter needs for emergency and/or low-cost shelter
Construct/ distribute low-cost housing kits to households with damaged destroyed houses.
In conflict/ return areas, ensure linkages with or undertake, and report/ address on peace and reconciliation or legal aid needs or other protection issues to better ensure a durable return
Link with other clusters and line ministries, agencies: water/ sanitation, health, education to ensure access to services
Quantification of shelter needs and types in target areas established
Beneficiary databases are maintained # shelters constructed/ distributed in each
location for # persons (age/ gender disaggregated data)
# of locations benefiting from multi-sector response in addition to shelter (water/ sanitation, health, education, peace building etc)
# areas where peace building and reconciliation activities are used to promote sustainable return
# of persons (age/ gender disaggregated) benefiting from emergency shelter due to displacement by conflict or natural disaster
MoSSP, Government of Kenya including national and local line ministries and provincial/ district officials, KRCS, DRC, GOAL Ireland, Habitat for Humanity, ACCORD, CORDAID, HWF, CCF, IOM, UN Habitat, local and international NGOs, UN-Habitat, UNDP, UNHCR
Provide sufficient basic domestic, hygiene items (NFIs) and emergency shelter to IDPs and other affected persons
1 Conflict and natural disasters areas
Procure, warehouse and distribute emergency shelter materials where required: tents, tarpaulins
SOPs for NFI distribution and beneficiary tracking are drafted and included as part of contingency plan: train all managers and distributors on reporting requirements
Cluster agencies participate in contingency planning for emergencies in Kenya
Efficient procurement, storage and distribution mechanisms are established by each agency
SOP in place for distribution and beneficiary tracking practices
(reporting on locations, # persons + age/gender disaggregated data)
# distribution agents/ partners trained in distribution tracking and reporting
% of NFI accounted for through distribution reports
% of gaps identified and reported
Government of Kenya, MoSSP, KRCS, IOM, CARE, IRC, DRC, International/ National NGOs, Logistics/ Transport Clusters (if activated), UNICEF, UNHCR
Establish and strengthen existing CCCM mechanisms in preparation for emergency humanitarian scenarios and coordination of mult-sector response in 2009
4 Agencies responsible for CCCM, local, district, provincial and national agencies, All affected populations in camp or camp-like situations
Guidance and training on CCCM CCCM is included in Contingency planning including
pre-emergency training of staff and SOPs for camp establishment and management
Registration/ profiling and data management SOPs are pre-established between Government of Kenya, KRCS, UN and NGOs
Contingency plan for conflict/ disaster include CCCM planning
# and locations of trainings for possible CCCM activities
SOPs for registration/ profiling, site mapping and data management are drafted and put in place
MoSSP, NDOC, other Ministries, KRCS, IOM, UNHCR, UN agencies (through contingency planning processes)
74

K E N Y A
WA
SHEffective and efficient WES emergency preparedness and response plans are in place and operational
1 ASAL areas, IDP affected areas of Rift Valley, Cholera affected areas of Western and Nyanza Provinces
Formation and training of WESCOORDs Technical training of cluster members
No of WESCOORDs trained Number of partners receiving technical
training Coherent sector response plan and
strategic operating framework in place
MoWI, MoPHandS, WESCOORD members
Community water supplies effectively & sustainably managed
2 ASAL areas, IDP affected areas of Rift Valley, Cholera affected areas of Western and Nyanza Provinces
Formation and training of Community Water Committees
No of CWCs trained No of water supplies with strong and
sustainable management structures in place
No of water supply schemes operating six months after completion
MoWI, MoPH&S, WESCOORD members
Reduction in ethnic conflict due to scarce or inequitable WES resources
3 ASAL areas, IDP affected areas of Rift Valley, Cholera affected areas of Western and Nyanza Provinces
Training of WESCOORDsand Cluster members
Inclusion of peace building and reconciliation aspects in all project proposals
No of participants reached by trainings Peace building and reconciliation aspects
included in all project proposals Reduction in community conflict over WES
resources
MoWI, MoPH&S, WESCOORD members
Effective and efficient preparedness, coordination and response strategy in place and operational
4 ASAL areas, IDP affected areas of Rift Valley, Cholera affected areas of Western and Nyanza Provinces
Support to MoWI to strengthen coordination mechanisms
Provision of services
No. of District WESCOORDs formed and trained
No. of affected population with improved access to water and sanitation
MoWI, MoPH&S, WESCOORD members
75

K E N Y A
ANNEX III. TABLE III. LIST OF PROJECTS – (GROUPED BY CLUSTER)
77
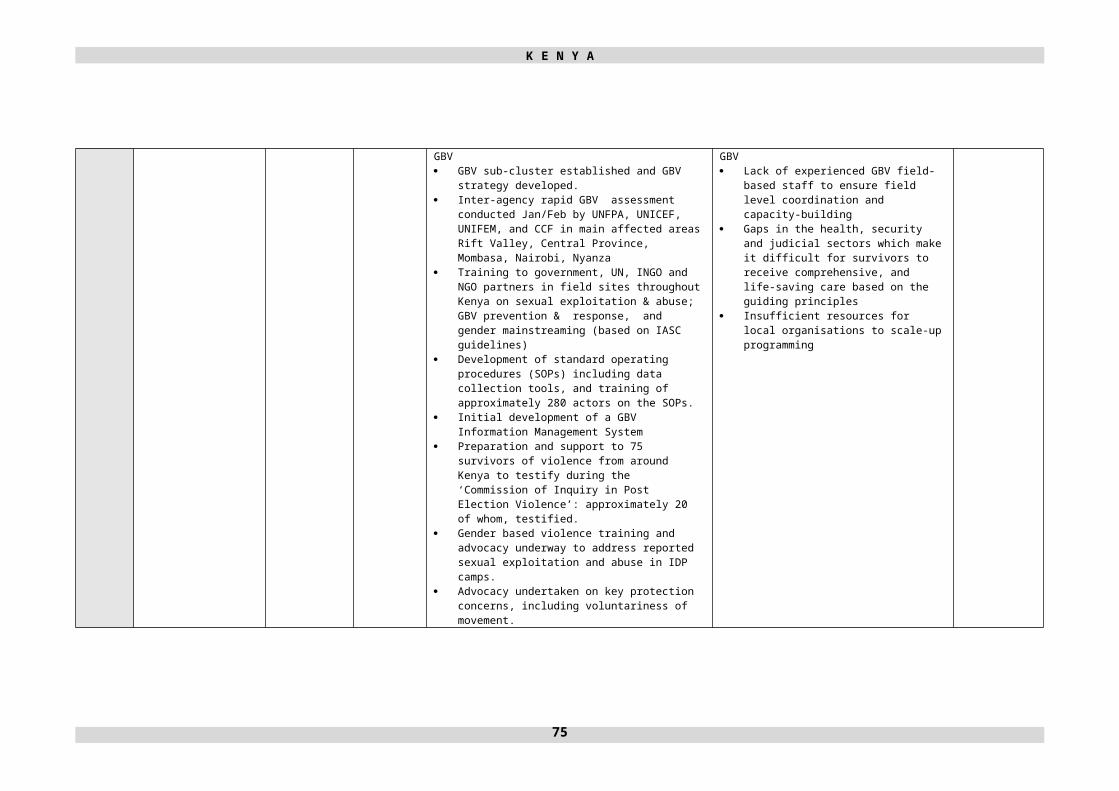
K E N Y A
78
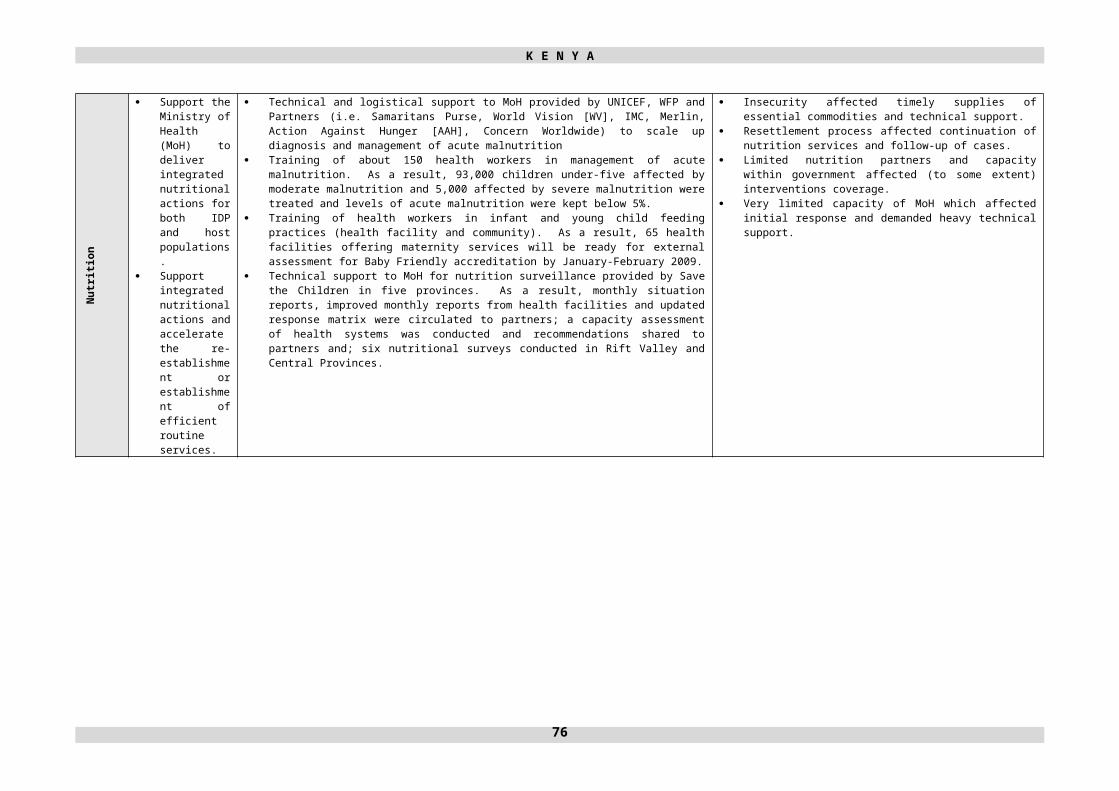
K E N Y A
79

K E N Y A
80

K E N Y A
81

K E N Y A
82

K E N Y A
83

K E N Y A
ANNEX IV. TABLE IV. LIST OF PROJECTS – (GROUPED BY APPEALING ORGANISATION
84

K E N Y A
85

K E N Y A
86

K E N Y A
87

K E N Y A
88

K E N Y A
89

K E N Y A
90
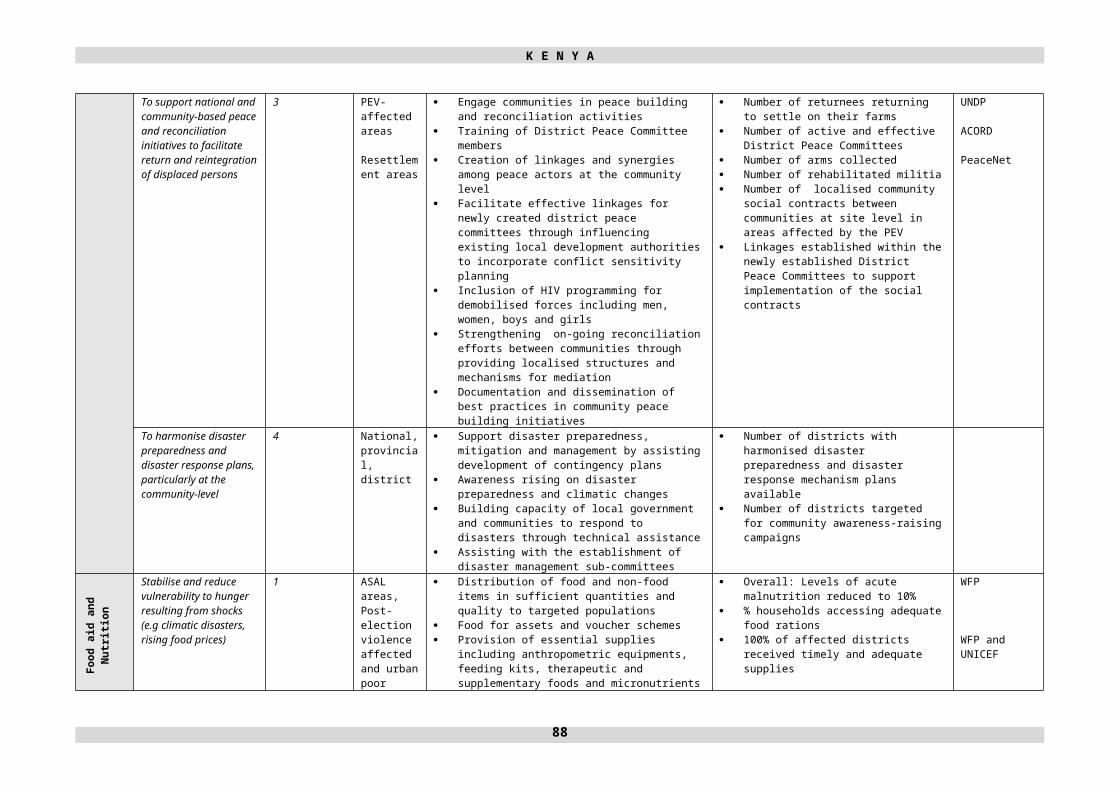
K E N Y A
91

K E N Y A
92
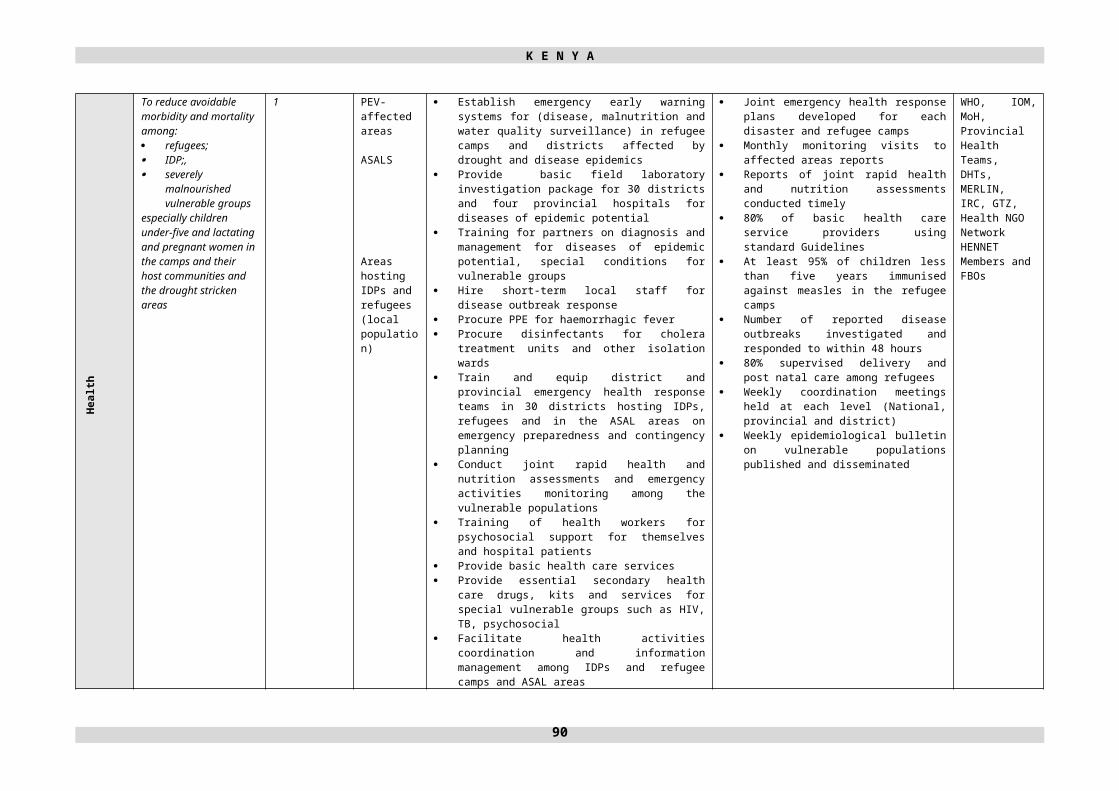
K E N Y A
93

K E N Y A
ANNEX V. TABLE V. SUMMARY OF REQUIREMENTS – (GROUPED BY IASC STANDARD SECTOR)
94

K E N Y A
ANNEX VI. DONOR RESPONSE TO 2008 APPEAL
95

K E N Y A
96

K E N Y A
97

K E N Y A
98

K E N Y A
99

K E N Y A
100

K E N Y A
101

K E N Y A
102
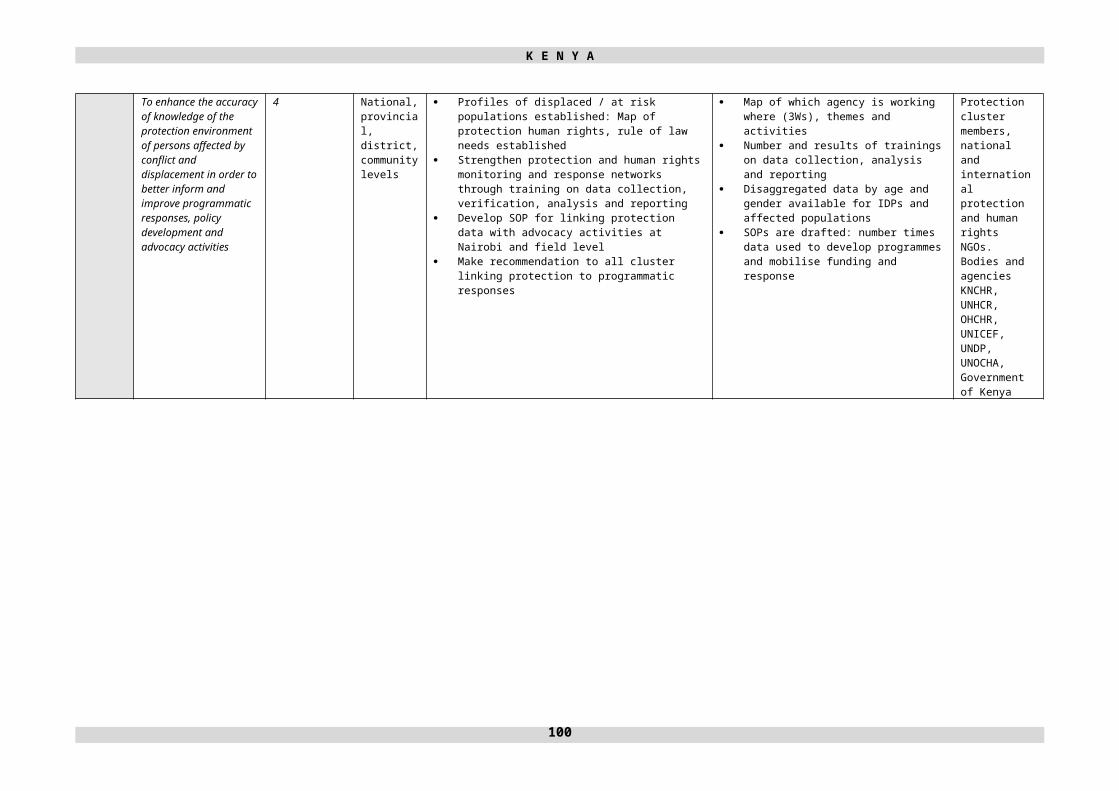
K E N Y A
103
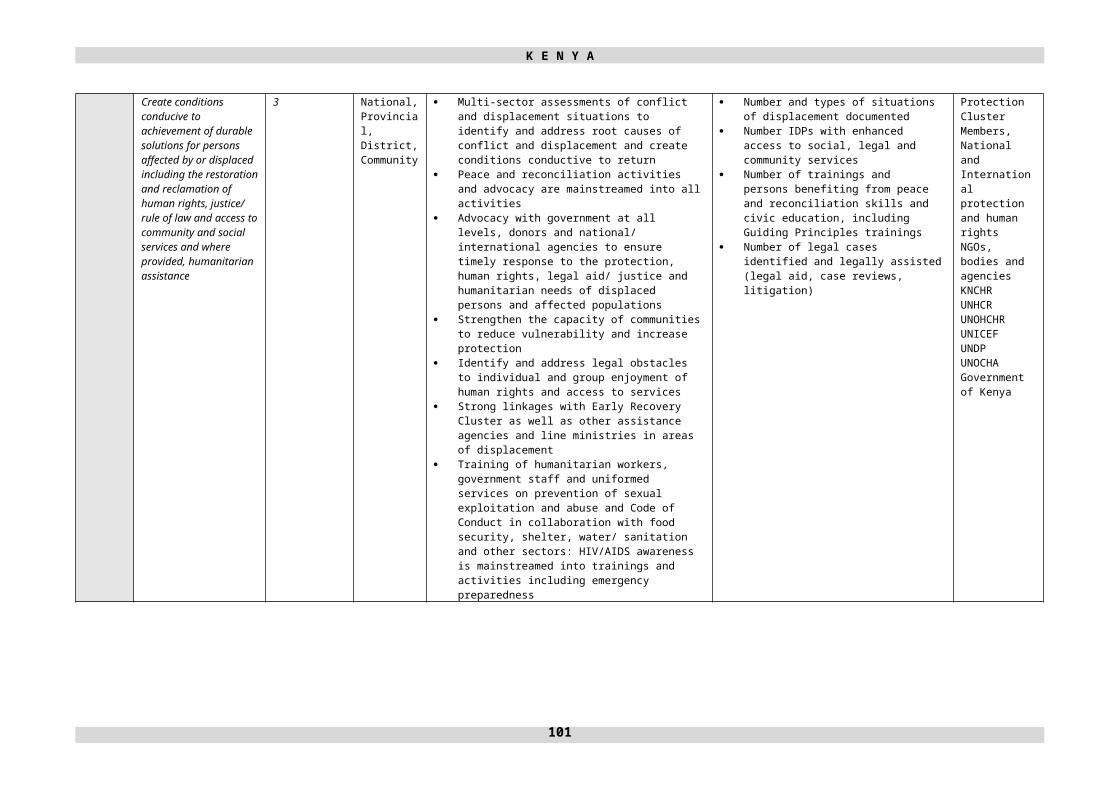
K E N Y A
104
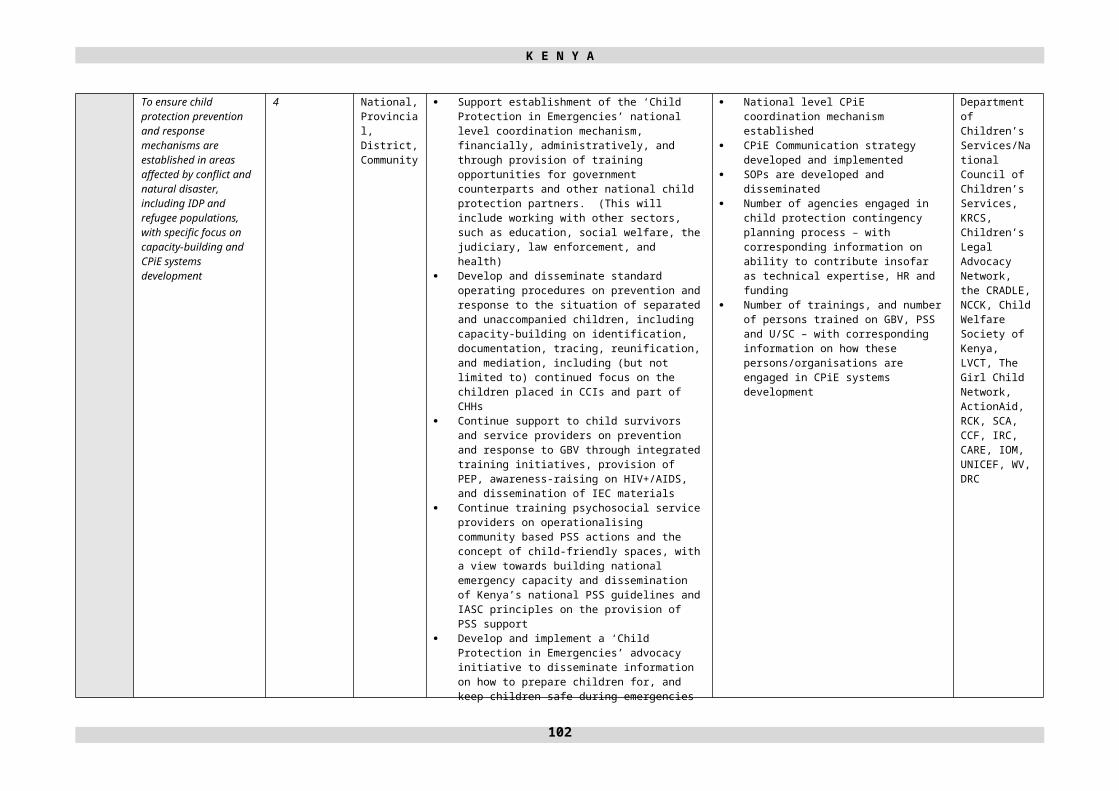
K E N Y A
105
K E N Y A
106

K E N Y A
ANNEX VII. ACRONYMS AND ABBREVIATIONS
AAH Action Against HungerACORD Agency for Cooperation and Research in DevelopmentAGDM Age, Gender, Diversity MainstreamingAIDS Acquired Immuno-deficiency SyndromeAMPATH Academic Model for Prevention and Treatment of HIV/AIDSANC Ante-natal Care ARPCT Alliance for Restoration of Peace and Counter-Terrorism ARV Anti-retrovirusASAL Arid and Semi-arid LandAVSI The Association of Volunteers in International Service
CAFOD Catholic Agency for Overseas Development CARE International Cooperation and Assistance for Relief EverywhereCBO Community Based OrganisationCCCM Camp Coordination and Camp ManagementCCF Christian Children’s FundCCPP Contagious Caprine Pleuro-pneumonia CCI Charitable Children’s InstituteCERF Central Emergency Response Fund CHAP Common Humanitarian Action PlanCHF Canadian Hunger FoundationCHH Child-headed HouseholdCISP Comitato Internazionale per lo Sviluppo dei PopoliCOCOP Coordinating Committee for CooperationCOMCEN Communication CentreCORDAID Catholic Organisation for Relief and DevelopmentCOVAW Coalition on Violence Against WomenCPiE Child Protection in EmergencyCPST Community Peace and Security Team CRC Committee on the Rights of the ChildCRS Catholic Relief Services CSW Commercial Sex Worker
DHT District Health TeamDPC District Peace CommitteeDRADRC Danish Refugee Council
ECD Early Child DevelopmentEHRP Emergency Humanitarian Response Plan EMIS Environmental Management Information SystemEMOP Emergency OperationEPRP Emergency Preparedness and Response PlanER&FS Early Recovery and Food Security Work PlanERNA Early Recovery Needs Assessment
FBO Faith-based OrganisationFFA Food for AssetFFH Freedom from HungerFGM Female Genital MutilationFIDA The Federation of Women Lawyers, KenyaFTS Financial Tracking Service
GAA German Agro-ActionGAM Global Acute MalnutritionGBV Gender-based ViolenceGBVWG Gender-based Violence Working GroupGenCap Gender Standby Capacity ProjectGFD General Food DistributionGIS Geographic Information SystemGOAL GoalGoK Government of KenyaGTZ Deutsche Gesellschaft für Technische Zusammenarbeit
HENNET Health NGO NetworkHF High FrequencyHIV Human Immuno-deficiency Virus
107

K E N Y A
HWF Health and Water Foundation
IASC Inter-Agency Standing CommitteeICRC International Committee of the Red CrossIDP Internally Displaced PersonsIDTR&M Identification, Documentation, Tracing, Reunification and MediationIEC Information, Education, and CommunicationIMC International Medical CorpsIOM International Organization for MigrationIP Implementing PartnersIRC International Rescue CommitteeIRS Indoor Residual Spraying
KES Kenyan ShillingKFSM Kenya Food Security MeetingKFSSG Kenya Food Security Steering GroupKHIMN Kenya Human-Development Information Management NetworkKIHBS Kenya Integrated Household Budget Survey KNCHR Kenya National Commission on Human RightsKRCS Kenya Red Cross Society
LLITNs Long Lasting Insecticide Treated NetsLRA Long Rain AssessmentLVCT Liverpool Voluntary Counselling and TestingLWF Lutheran World Federation
M&E Monitoring and EvaluationMERLIN Medical Emergency Relief InternationalMoE Ministry of EducationMoH Ministry of HealthMoPH&S Ministry of Public Health & SanitationMoSSP Ministry of State for Special ProgrammesMoU Memorandum of UnderstandingMoWI Ministry of Water & Irrigation
NARA National Accord and Reconciliation Act NBO NairobiNCCK National Council of Churches in KenyaNCGD National Commission on Gender and DevelopmentNDOC National Disaster Operation CentreNFI Non-Food ItemNGO Non-Governmental OrganisationNRC Norwegian Refugee CouncilNSC National Steering Committee on Peace Building and Conflict Management
OCHA Office for the Coordination of Humanitarian AffairsODM Orange Democratic MovementOVC Orphans and Vulnerable ChildrenOVM Orphans and Vulnerable Children
PEC Post –Election CrisisPEP Primary Education ProjectPEV Post-Election ViolencePLHIVA People Living with HIV/AIDSPLWA People Living with AIDSPPE Personal Protection EquipmentPPR Peste des Petits Ruminants PMTCT Prevention of Mother to Child TransmissionPSEA Prevention of Sexual Exploitation and AbusePSS Psychosocial SupportPTA Parent Teacher AssociationPU Première UrgencePUR for water purification (chlorine)PWD People with DisabilitiesPWG Protection Working Group
RCMRD Regional Centre for Mapping of Resources for RedevelopmentRET Research Experience for TeachersRH Reproductive HealthRSD Refugee Status Determination
108

K E N Y A
SAM Severe Acute MalnutritionSC Save the ChildrenSC-UK Save the Children – United KingdomSCIC Supreme Council of Islamic CourtsSEA Sexual Exploitation and AbuseSFP Supplementary Feeding ProgrammeSGBV Sexual and Gender-based ViolenceSLDF Sabaot Land Defence ForceSMC School Management CommitteeSO Special OperationSP Samaritan’s Purse
TB TuberculosisTBA Traditional Birth AttendantTFG Transitional Federal GovernmentTFP Therapeutic Feeding ProgrammeToT Training of TrainerTSK Transitional Shelter Kit
UAM Un-accompanied MinorUNDP United Nations Development Programme UNFPA United Nations Population FundUNHAS United Nations Humanitarian Air Service UNHCR United Nations High Commissioner for RefugeesUNICEF United Nations Children’s FundUNIDO The United Nations Industrial Development Organization UNIFEM United Nations Development Fund for WomenUNON United Nations Office in NairobiUNOHCHR United Nations Office of the High Commissioner for Human RightsUSAID United States Agency for International Development
VCT Voluntary Counselling and TestingVHF Very High Frequency
WASH Water, Sanitation, and HygieneWES Water and Environmental SanitationWESCOORD Water and Environmental Sanitation Coordination CommitteeWFP World Food ProgrammeWHO World Health OrganizationWV World Vision
109

Consolidated Appeal Process (CAP)
The CAP is a tool for aid organisations to jointly plan, coordinate, implement and monitor their response to disasters and emergencies, and to appeal for funds together instead of competitively.
It is the forum for developing a strategic approach to humanitarian action, focusing on close cooperation between host governments, donors, non-governmental organisations (NGOs), the International Red Cross and Red Crescent Movement, International Organization for Migration (IOM), and United Nations agencies. As such, it presents a snapshot of the situation and response plans, and is an inclusive and coordinated programme cycle of:
Strategic planning leading to a Common Humanitarian Action Plan (CHAP); Resource mobilisation leading to a Consolidated Appeal or a Flash Appeal; Coordinated programme implementation; Joint monitoring and evaluation; Revision, if necessary; Reporting on results.
The CHAP is the core of the CAP – a strategic plan for humanitarian response in a given country or region, including the following elements:
A common analysis of the context in which humanitarian action takes place; An assessment of needs; Best, worst, and most likely scenarios; A clear statement of longer-term objectives and goals; Prioritised response plans, including a detailed mapping of projects to cover all needs; A framework for monitoring the strategy and revising it if necessary.
The CHAP is the core of a Consolidated Appeal or, when crises break out or natural disasters strike, a Flash Appeal. Under the leadership of the Humanitarian Coordinator, and in consultation with host Governments and donors, the CHAP is developed at the field level by the Humanitarian Country Team. This team includes IASC members and standing invitees (UN agencies, the International Organisation for Migration, the International Red Cross and Red Crescent Movement, and NGOs that belong to ICVA, Interaction, or SCHR), but non-IASC members, such as national NGOs, can also be included.
The Humanitarian Coordinator is responsible for the annual preparation of the consolidated appeal document. The document is launched globally near the end of each year to enhance advocacy and resource mobilisation. An update, known as the Mid-Year Review, is presented to donors the following July.
Donors generally fund appealing agencies directly in response to project proposals listed in appeals. The Financial Tracking Service (FTS), managed by the United Nations Office for the Coordination of Humanitarian Affairs (OCHA), is a database of appeal funding needs and worldwide donor contributions, and can be found on www.reliefweb.int/fts.
In sum, the CAP is how aid agencies join forces to provide people in need the best available protection and assistance, on time.

OFFICE FOR THE COORDINATION OF HUMANITARIAN AFFAIRS(OCHA)
UNITED NATIONS PALAIS DES NATIONSNEW YORK, NY 10017 1211 GENEVA 10
USA SWITZERLAND


















