
Emergency Department Pre-Arrival Info Pre-Arrival...
42
Dale of Service: 4/9/2013 19:42 PDT Authored By: Result Status: Weaver.Kassi L ( 4/912013 19:42 POT) Au1h (Verified) Documen1 Type: Emergency Departmen1 Pre-Arrival Info Emergency Department Pre-Arrival Info Pre-Arrival Summary Name: xie, jianhua Gender: Male Current Date: 4/9/2013 19:42:02 PDT Date of Birth: 9/16/2012 Age: 6 mon1hs Pre-Arrival Type: PCP-Clinic ETA: 419/201319:11 :OO PDT Chief Complaint: wz,? cardiac prob.1930.pov Pre-Arrival User: Schneider, Carol J, RN Referring Provider Search: Wen, Julie E, MD Current Time: 1 8:46 Clinic/Facility: peds assoc Location: Pre-Arrival Imaging: Yes Imaging Type: heart size big on XR Labs: No Recommendations: From Referring: worried about undiagnosed cardiac issues Mode of Arrival: Private Vehicle Mode of Arrival Comments: parents speak mandarin Call Back: After ED Evalua1ion Call Back Name: Wen, Julie Call Back Phone: 425-827-4600 Probable ICU?: No PMH: bronchiolitis for past 2 months, immunized, HP/: 6 mon1h old ill for 2 mon1hs, PCP concerned 7 heart failure, heart size large on CXR. wz for 2rnon1hs, generalized swelling no1ed by parent, whz worse now, diarrhea, 4 lb wgt gain in month Meds Today (Verify With referring provider's documentation) albuterol, results in some improvement, Vitals: 156 HR 102 temp, Sp02 96%, unable to do BP Seattle Children's Hospital PO Box 537t Seattle, Washington 98105-0371 NAME: XIE, J IANHUA DRACO DOB: MRN: 9/16/2012 1275567 Print Date: RRID: 9/2312015 13:52 PDT 25788848 186 of 2081
Transcript of Emergency Department Pre-Arrival Info Pre-Arrival...
Dale of Service: 4/9/2013 19:42 PDT Authored By: Result Status:
Weaver.Kassi L ( 4/912013 19:42 POT) Au1h (Verified)
Documen1 Type: Emergency Departmen1 Pre-Arrival Info
Emergency Department Pre-Arrival Info Pre-Arrival Summary
Name: xie, jianhua Gender: Male
Current Date: 4/9/2013 19:42:02 PDT
Date of Birth: 9/16/2012 Age: 6 mon1hs Pre-Arrival Type: PCP-Clinic ETA: 419/201319:11 :OO PDT
Chief Complaint: wz,? cardiac prob.1930.pov Pre-Arrival User: Schneider, Carol J, RN Referring Provider Search: Wen, Julie E, MD Current Time: 1 8:46 Clinic/Facility: peds assoc Location: Pre-Arrival Imaging: Yes Imaging Type: heart size big on XR Labs: No Recommendations: From Referring: worried about undiagnosed cardiac issues Mode of Arrival: Private Vehicle Mode of Arrival Comments: parents speak mandarin Call Back: After ED Evalua1ion Call Back Name: Wen, Julie Call Back Phone: 425-827-4600 Probable ICU?: No
PMH: bronchiolitis for past 2 months, immunized,
HP/: 6 mon1h old ill for 2 mon1hs, PCP concerned 7 heart failure, heart size large on CXR. wz for 2rnon1hs, generalized swelling no1ed by parent, whz worse now, diarrhea, 4 lb wgt gain in month
Meds Today (Verify With referring provider's documentation) albuterol, results in some improvement,
Vitals: 156 HR 102 temp, Sp02 96%, unable to do BP
Seattle Children's Hospital
PO Box 537t
Seattle, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
186 of 2081

Dale of Service: 4/9/2013 20:19 PDT Authored By: Result Status:
Ackley,Stanford Heath,MD,MPH (4/9/2013 20:21 PDT) Au1h (Verified)
Documen1 Type: ED Provider N o1e
General ED Note
Patient XIE, JIANHUA DRACO MRN: 1275567 FIN: 94243980 Age: 6 months Sex: Male DOB: 9/16/2012 Associated Diagnoses: Liver failure Author: Ackley, Stanford Heath, MD, MPH
Pre-Arrival Attending Attestation: I have reviewed any available pre-arrival information and/or included faxes or images.
Pre-Arrival Summary
Name: xie, jianhua Gender: Male
Current Date: 41912013 19:42:02 POT
Date of Birth: 911612012 Age: 6 months Pre-Arrival Type: PCP-Clinic ETA: 41912013 19.11.00 POT
Chief Complaint: wz, ? cardiac prob. 1930.pov Pre-Arrival User: Schneider, Carol J, RN Referring Provider Search: Wen, Julie E, MD Current Time: 18:46 Clinic/Facility: peds assoc Location: Pre-Arrival Imaging: Yes Imaging Type: heart size big on XR Labs: No Recommendations: From Referring: worried about undiagnosed cardiac issues Mode of Arrival: Private Vehicle Mode of Arrival Comments: parents speak mandarin Call Back: After ED Evaluation Call Back Name: Wen, Julie Call Back Phone: 425-827-4600 Probable ICU?: No
PMH: bronchiolitis for past 2 months, immunized,
HP/: 6 month old ill for 2 months. PCP concerned ? heart failure, heart size large on CXR, wz for 2months, generalized swelling noted by parent, whz worse now, diarrhea, 4 lb wgt gain in month Meds Today (Verify With referring provider's documentation]: albuterol, results in some improvement, Vitals: 156 HR t 02 temp, Sp02 96%, unable to do BP
Seattle Children's Hospital
PO Box 537t
Seattle, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Pnnt Date:
RRID:
9/2312015 13:52 PDT
25788848
194 of 2081
Triage
Triage Information Mode of Arrival: Tracking Acuity: 2-Emergency Respiratory Score: 6 Nursing Chief Complaint: RSV, swelling Vital Signs (04/09113 19:43): T(temporal): 39 DegC
Early Initiation
Early lni!iation Information None documented
Chief Complaint
Chief Complaint: RSV, swelling
History of Present Illness Time seen: 4/9/2013 20 19:00, Immediately upon arrival. History source: mother, father. Present in room: patient, mother, father.
P: 148 R: 60 BP: 117/63 (70) - SP02: 99 %
6 month old male with history of RSV at 3 months of life with recurrent wheezing who presents from his PC P's o11ice with concern for swelling x 3 days. Parents mention that he's had non-bloody diarrhea x 3 days; Dad also had diarrhea about 4 days ago. He has
been fussy, wheezin>i more loudly, and cou>ihin>i with some nasal con>iestion. Spitting up more frequently, always curdled milk in appearance - non-bloody, non-bilious. Has continued voiding in between stools.
Fellow Addendum Agree wrth resident history as above. Parents report 3 days of "increased swelling" of his "entire body". He also seems to have more difficulty breathing and has been spitting up his feeds, decreased oral intake.
Attending Addendum Agree with history above 6 month old male here with hx of 2 months of cough and congestion, here with diarrhea and emesis and difficulty breathing. Pt with possible 'swollen' abdomen and decreased po intake.
Allergies!Meds/lmm Allergies:.
Allergies (last reviewed on 04109113 19:45) NKA
Medications: . Home Medications (not reviewed by MIC)
No Home Medications were Recorded
Immunizations: .
Seattle Children's Hospital
PO Box 537t
NAME: XIE, J IANHUA DRACO
DOB:
Seat11e, Washington 98105-0371 MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
195 of 2081
Immunizations Not Recorded as of 04109/13 20:19
Past Medical/ Family/ Social History Medical nistory: RSV per HPI. No overnight hospitalization required .. Hospitalization nistory: None Surgical nistory: None Birtn nistory: 37 weeks, no complications. 7 lbs 2 oz at birth (3.28kg). Family nistory: Not significant. Developmental nistory: Normal per historian. Social nistory: Lives with Mother, Father, and 3 older siblings, all healthy.
Review of Systems Constitutional symptoms: Fever. ENMT symptoms: Nasal conqestion. Respiratory symptoms: Wheezing, cough, shortness of breath Cardiovascular symptoms: Edema diffusely Gastrointestinal symptoms: Vomiting, diarrhea, no rectal bleeding. Genitourinary symptoms: denies decreased urine output, no hematuria. Skin symptoms: denies rash
Physical Examination Time/Chaperone: Vital signs: 04/09113 21:14
Time documented: 4/912013 20:26:00.
T: P: R: 44 BP: 86/31 (50) -- Right arm SP02: 100 %
General: Obviously edematous male Asian infant in moderate distress, crying loudly. Head: Anterior fontanelle open and soft. Eye: Extraocular movements are intact, normal conjunctiva. Ears, nose, mouth and throat: Tympanic membranes clear, external auditory canal normal, Clear nasal discharge (also
cryin~) Mildly high palate. Neck: No adenopathy Cardiovascular: Tachycard1c, difficult exam given coarse breath sounds bilaterally; no obvious gallup, peripheral pulses
palpable, cap refill 2+ seconds, warm extremities. Respiratory: Coarse BS throughout, aeration equally, tachypneic and crying, prolonged expiratory push, harsh voice. Abdomen: Distended, difficult to perceive tenderness given fussiness, questionable hepatomegaly 2-3cm BCM. Genitourinary: Normal external genitalia for age Musculoskeletal: Moves all extrem1t1es, normal ROM, normal strength. Skin: Warm. dry. Neurological: Fussy but consoles sli~htly with mother; alert, responsive to exam, seems to sense throughout, moves all
extremities equally, no asymmetry to 1acies.
Physical Examination - Fellow Vital signs: Vital signs per triage. General: Generalized edema, moderate respiratory distress. Hoarse cry throughout exam. Head: Normocephalic and atraumatic, anterior fontanelle open and soft. Eye: Swollen lids bilaterally. Ears, nose, mouth and throat: Mucous membranes moist, oropharynx clear, Clear nasal discharge. Neck: Supple. Cardiovascular: Extremity pulses normal, capillary refill less than 2 seconds. no edema, Initial cardiac exam limited by
crying Tachycardic, no obvious gallop Bilateral femoral pulses 2+ When calm, harsh 2/6 systolic murmur appreciated. No thrill. CR< 2 seconds. Generalized edema ..
Respiratory: Tachypnea, mildly coarse breath sounds bilaterally that clear with crying. Intermittent grunting respirations, subcostal retractions ..
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
196 of 2081
Chest: No deformity Abdomen: Distended, firm to palpation. Difficult to appreciate liver edge. +BS .. Genitourinary: Normal external genitalia for age Musculoskeletal: Moves all extremities, no deformity. Lymphatics: No lymphadenopathy. Skin: Warm. dry, Small bruise right cheek. Neurological: Moves all extremities, no focal neurological deficit obseived. Psychiatric: Crying but consolable.
Physic:al Examination - Attending Vital signs: Vital signs per triage. General: Well developed, well nourished, no apparent distress. Head: Normocephalic and atraumatic. Eye: Pupils are equal, round and reactive to light Ears, nose, mouth and throat: Tonsils normal, oropharynx clear. Neck: Supple, full range of motion. Cardiovascular: Regular rate and rhythm, II/VI ejection murmur. Respiratory: Lungs are clear to auscultation bilaterally, normal chest shape Chest: No tenderness Abdomen: Soft, nontender, non-distended, no mass, no organomegaly. Genitourinary: Exam deferred. Back: Nontender. Musculoskeletal: Moves all extremities. Lymphatics: No lymphadenopathy. Skin: Warm. dry, CRT 3 seconds at feet b/I, normal fem pulses, +small bruise on R cheek. Neurological: Alert, moves all extremities.
Reexamination/ Reevaluation Re-examination/Re-evaluation: Time: 4/10/2013 02:35:00. Provider: Davis, Jeremiah Cheatham MD, MPH Vital signs 0~110/1300:32 T(temporal): 39 DegC P: R: 34.0 BP: 113169 (85)-- SP02: 100 %
Assessment: BPs stable but occasionally SBP < 80 so will repeat NS bolus 10ml/kg Breathing more comfortably, seems more consolable with Mom. Abdomen still distended, not increased in firmness, seems tender to palpation. Will draw LFTs and additional hematocrit to evaluate change ..
Medical Decision Making Lab results review:
Lab Results (three most recent resu/rs within past 24 hrs, per order) Tes! 04/09113 22:20
BUN 9
Creatinine 0.2
Magnesium Serum 2.4
Phocphorus Serum 3.4 (L)
B-type Natriuret1c Peptide
Amylase Serum
Gamma Glutamyltransferase
Lipase Level
Sodium Level
33
<30
54
dO(L)
134 (L)
9 - 6.5 mg/dL
- 120 IU/L
- 145 mEq/L
Normal Ranae
- 20 mgldl
1 - 0.4 mg/dl
.8 - 2.4 mg/dL
- 41 pg/ml
-115 IUIL
- 85 IU/L
Potassium Level 5 0 .5 - 5.5 mEq/L
Chloride Level
Seattle Children'c Hocpital
PO Box 5371
Seattle, Washington 98105-0371
110 -110mEq/L
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
197 of 2081
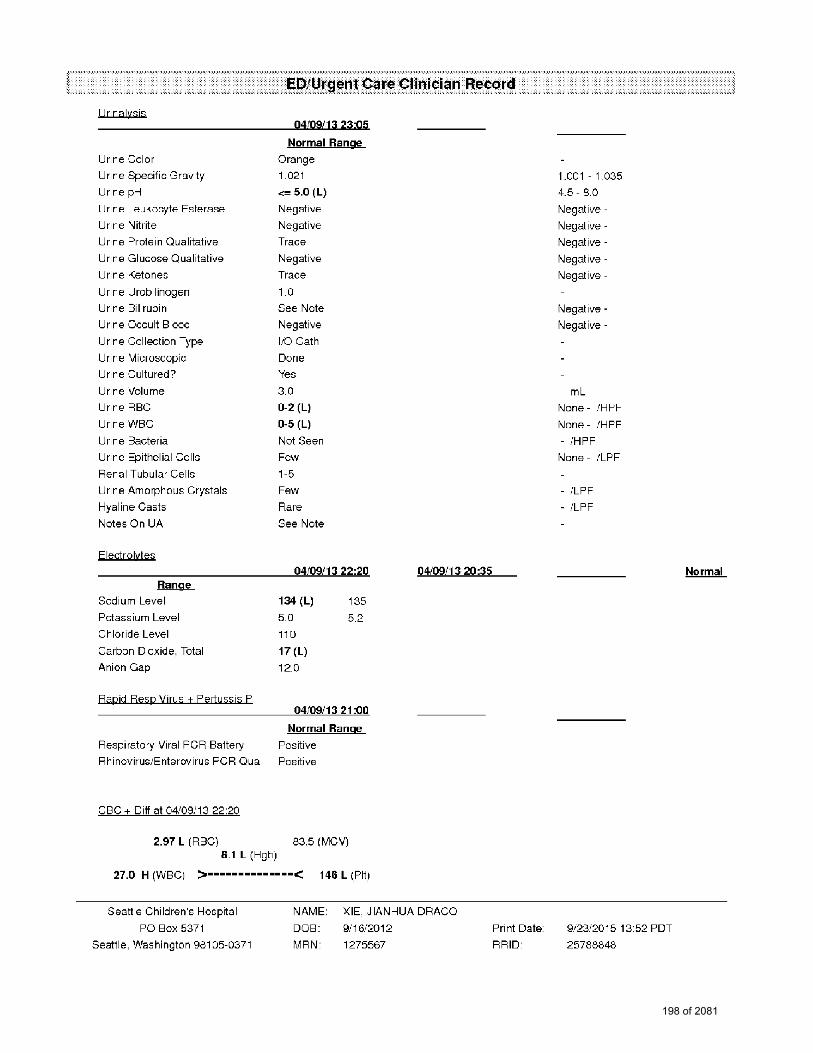
l lrjnalysis
Urine Color
Urine Specific Gravity
Urine pH
Urine Leukocyte Esterase
Urine Nitrite
Urine Protein Qualitative
Urine Glucose Qualitative
Urine Ketones
Urine Urob1linogen
Urine Bilirubin
Urine Occult Blood
Urine Collection Type
Urine Microscopic
Urine Cultured?
Urine Volume
Urine RBC
Urine WBC
Urine Bacteria
Urine Epithelial Cells
Renal Tubular Cells
Urine Amorphous Crystals
Hyaline Casts
Notes On UA
Electrolytes
Range
Sodium Level
Potassium Level
Chloride Level
Carbon Dioxide, Total
Anion Gap
Rapjd Resp yjpis + Pertussjs P
04109113 23:05
Normal Range
Orange
1.021
<= 5.0 (L)
Negative
Negative
Trace
Negative
Trace
1.0
See Note
Negative
1/0 Gath
Done
Yes
3.0
0-2 (L)
0-5 (L)
Not Seen
Few
1-5
Few
Rare
See Note
04109/13 22:20
134 (L)
5.0
11 D
17 (L)
12.0
t35
5.2
04109/13 21 :00
Normal Range
Respiratory Viral PCR Battery Positive
Rhinovirus1Enterovirus PCR Qua Positive
CBC+ Diff at 04/09/13 22:20
2.97 L (RBC) 83.5 (MCV) 8.1 L (Hgb)
27.0 H (WBC) >··············< 146 L (Pit)
04/09/13 20:35
Seattle Children"s Hocpital
PO Box 537t
NAME: XIE, J IANHUA DRACO
DOB:
Seattle, Washington 98105-0371 MRN:
9/16/2D12
1275567
Print Date:
RRID:
1.001 - 1.035
4.5- 8.0
Negative -
Negative -
Negative -
Negative -
Negative -
Negative -
Negative -
ml None - /HPF
None - /HPF
- IHPF
None - /LPF
/LPF
ILPF
9/2312015 13:52 PDT
25788848
Normal
198 of 2081
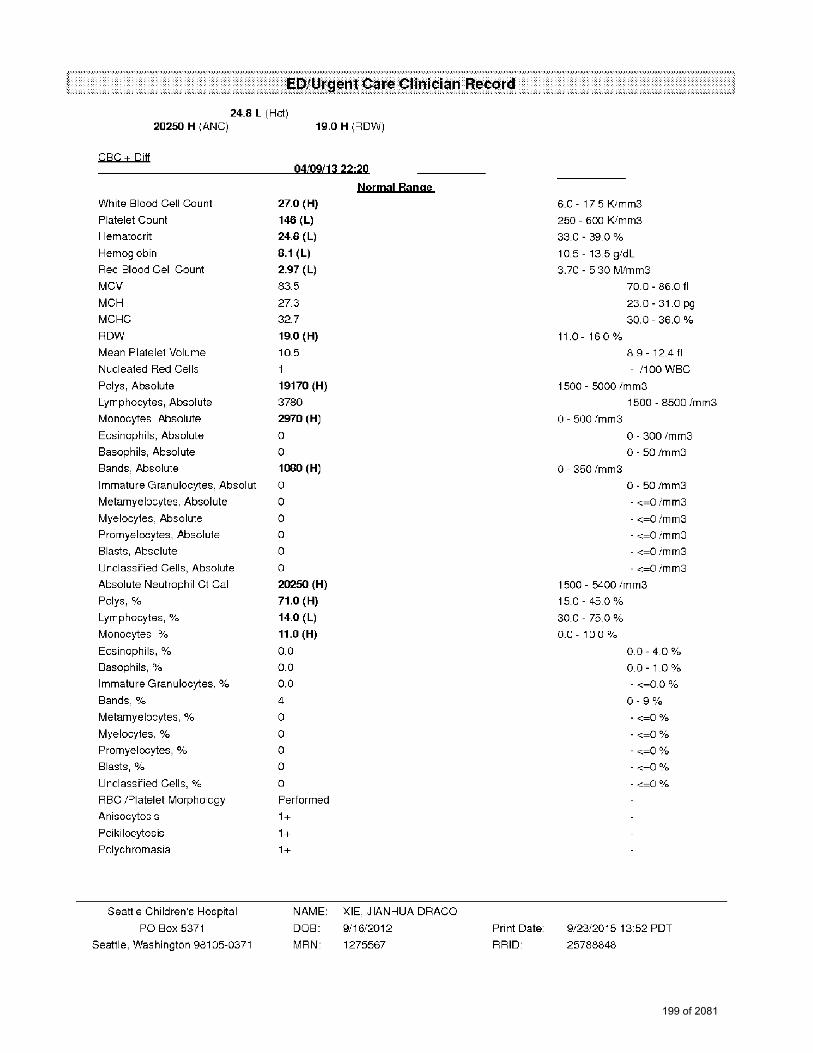
24_8 L (Hc1) 20250 H IANC) 19.0 H (RDW)
CBC+ Pit!
White Blood Cell Count
Platelet Count
Hematocrit
Hemoglobin
Red Blood Cell Count
MCV
MCH
MCHC
RDW
Mean Pla1ele1 Volume
Nucleated Red Cells
Palys, Absolute
Lymphocytes, Absolute
Monocytes, Absolute
Easinophils, Absolute
Basophils, Absolute
Bands, Absolute
Immature Granulocytes, Absolut
Metamyelocytes, Absolute
Myelocytes, Absolute
Promyelocytes, Absolute
Blasts, Absolute
Unclassified Cells, Absolute
Absolute Neutrophil Ct Cal
Polys1 ~lo
Lymphocytes, %
Monocytes, %
Eosinophils, 0/o
Basophils, %
Immature Granulocytes, %
Bands 1 °/o
Metamyelocytes, %
Myelocytes, %
Promyelocytes, %
Blasts, 0;~
Unclassified Cells, %
RSC /Platelet Morphology
Anisocytos1s
Poikilocytosis
Polychromasia
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
04109/13 22·20
27.0 (H)
146 (L)
24.S (L)
B.1 (L) 2.97 (L)
83.5
27.3
32.7
19.0 (H)
105
1
19170 (H)
3780
2970(H)
0
0
1000 (H)
0
0
0
0
0
0
20250(H)
71.0 (H)
14.0 (L)
11.0 (H)
o_o 0.0
0.0
4
0
0
0
0
0
Performed
1+
1+
1+
Normal Ranae
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
6.0 - 175 K/mm3
250 - 600 K/mm3
33.0 - 39.0 %
10.5 - 13.5 gldL
3.70 - 5.30 M/mm3
11.0- 160 %
70.0 - 86.0 fl
23.0 - 31.0 pg
30.0 - 36.0 %
89-12411
- 1100 WBC
1500 - 5000 /mm3
o - 500 /mm3
0 - 350 /mm3
1500 - 8500 Im m3
O - 300/mm3
0-50/mm3
0-50/mm3
- <=0 imm3
- <=0 imm3
- <=0 imm3
- <=0 imm3
- <=0 imm3
1500 - 5400 /mm3
15.0 - 45.0 %
30.0 - 75.0 %
o_o - 1 o.o %
00-40%
o_o- 1.0 %
- <=0.Q 0/o
0-9~/o
- <=0 °/o
- <=0 °/o
- <;=0 °/o
- <=0 O/o
- <=0 Ofo
9/2312015 13:52 PDT
25788848
199 of 2081

Radiology results: Attending statement: AXR/CXR thumbprinting of colon, intraperitoneal free fluid, paucity of bowel gas.
AR NP/Resident assessment and plan: 6 month old male with 3 days of body edema, now with fever in setting of congestion, cough, increased work of breathing and
diarrhea Rhinovirusienterovirus positive which could explain diarrhea, cough/congestion and fever, but unusual for such levels of anemia, thrombocytopen1a and body edema.
Fellow assessment and plan: 6 month old male with 3 day history of increased edema, particularly over the abdomen who now presents with increased work of
breathing, emesis, and diarrhea. Initial concern for congenital heart d1sease/myocarditis, infection, or intraabdominal process. Xray of the chest and abdomen were obtained and did not show significant pumonary edema but showed a paucity of gas in the abdomen. There was signficant difficulty obtaining labs/placing IV and parents were resistant to IV attempts. During this time, patient's WOB worsened slightly. Social work was consulted and IV access obtained. Patient given 5cclkg NS bolus. Temp at this time 40 degrees Blood and urine cultures sent, Rocephin ordered PICU evaluated patient and was most concerned about his abdominal distension. Portable abdominal US ordered. Labs concerning for 1nfect1on wrth WBC of 27K, but no clear source at this lime; antibiotics have been given. Care signed out to Dr. Ackley to follow up on US results and determine admission to PICU versus floor.
Attending assessment and plan: 6 month old male with 3 days of increasing swelling of abdomen and legs, now with increased wob, em es is and diarrhea PIV
attempted, only sm amount of blood obtained. Pt wtih anemia with a he! of 21, dehydrated with a lactate of 3.0 and bicarb of 15. Had 3 attempts to obtain IV, but had d11ficulty. Parents very resistant to continue to try, do not feel as though patient needs IVF. Called SW to be at bedside, to help discuss need for IVF with parents Parents relented for IV team to attempt and IV obtained Additional blood sent and ICU contacted as pt has paucity of gas on abdomen, and irregular respirations. Pl signed out to Dr. Ackley at 2300.
Assumed care from Dr. Slater at 2300. Patient's labs revealed fulminant liver failure of unknown etiology. Consider sepsis, biliary obstruction Pa1ient received antibiotics and IV fluids while in the ED Patient also noted to be anemic with low and blood pressure is, so a blood transfusion was begun. Anemia also has unclear etiology. A CT scan was recommended to evaluate for intra-abdomimil bleeding, however the parents refused to consent for 11 while the patient was in the ED. Case discussed with GI. Patient will be admitted to the PICU for ongoing management of liver failure.
Diagnosis and Follow Up Diagnosis
Liver failure (ICD9 572.8) Plan
Condition: Critical Disposition: Admit: to Pediatric Intensive Care Unit. Informational call to PCP: Call back for admission: Contacted by: Davis, Jeremiah Cheatham, MD, MPH.
Endorsement/Addendum
Attending Attestation I have seen and evaluated this patient, reviewed and agree with the HPl/PMHIFHISH/ROSIPE/Summary & Plan documented by the
Resident/Fellow unless otherwise indicated.
Canrributors Supervising Provider: Ackley, Stanford Heath, MD, MPH
Supervising Provider: Slater, Anne C, MD
Supervising Provider: Schuh, Abigail Marie, MD
ARNP/Residenl/Other: Davis, Jeremiah Cheatham, MD, MPH
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9116/2012
1275567
(saved on 04/1012013 06:35)
(saved on 04/0912013 23:01)
(saved on 04/1012013 00:40)
(saved on 04/1012013 02:38)
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
200 of 2081

Dale of Service: Authored By: Result Status: Documen1 Type:
Historv & Physical
HISTORY AND PHYSICAL XIE, JIANHUA DRACO
DOB: 09/16/2012 M -MR#: 01-27-55-67
DATE OF ADMISSION: 04109/2013
4/10/2013 00:00 PDT Smith,Lincoln S,MD (4124/201312:37 PDT) Modified History and Physical
DATE OF EXAMINATION: 04110/2013
CHIEF COMPLAINT: Coagulopathy, ascites, and hyperbilirubinemia.
HISTORY OF PRESENT ILLNESS: Jianhua is a 6-month-old male who was a previously healthy child aside from an episode of bronchiolitis requiring outpatient therapy for RSV (respiratory syncytial virus) at 3 months of age who presents with 3 days of loose stools in the setting of his father also having some diarrhea. He had no
fever with this illness and did not have any evidence of jaundice. In retrospect, the parents say that he has gained significant weight over the past month and they noted some edema yesterday; thus, they took him to their primary care doctor who referred them to the emergency department for evaluation, given his edema. In Seattle Children's Hospital Emergency Room, he had a fever to 39, so blood cultures were drawn and he was given a dose of ceftriaxone. His blood pressure was 117163. He had an extensive work-up in the emergency department for the etiology of his edema, which included a chest x-ray and BNP for evaluation for cardiac disease, which revealed no cardiomegaly and a normal BNP; evaluation of renal disease, which included electrolytes which were normal except a low bicarbonate at 17 but normal BUN and creatinine at 910.2, and a UA (urinalysis) significant for trace protein and trace ketones but was otherwise unremarkable. However, his labs were significant for a coagulopathy and hypoalbuminemia as well as a mixed hyperbilirubinemia. Therefore, given the concern for liver dysfunction and liver failure, he was admitted to the Pediatric Intensive Care Unit with concern for decompensation in that setting.
HOME MEDICATIONS: None. Parents deny any herbal supplements.
ALLERGIES: No known allergies.
PAST MEDICAL HISTORY: He was born at 38 weeks' gestation, and it was an uncomplicated pregnancy. He has 3 siblings. He has had some issues with loose large stools on and off; however, the parents felt like this was associated with cow's milk formula so they transitioned to soy milk-based formula at 2 months of age and they feel like this has improved. He did have an episode of RSV in January and has had some intermittent wheezing since that time.
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID: 9/2312015 13:52 PDT
25788848
201 of 2081

SOCIAL HISTORY: He lives at home with his mother, father, and 3 siblings. He is fed soy-based formula. They have recently introduced some solids in the last 3 weeks but these include typical Gerber foods without anything out of the ordinary. He has not been exposed to any other medications including even Tylenol or herbal medications. He has had his 2 and 4-month immunizations.
FAMILY HISTORY: Noncontributory.
REVIEW OF SYSTEMS: HEENT: They have not noted scleral icterus. He has had some bruising on his cheeks that they have noted in the last week. Respiratory: He has had some chronic wheezing. Cardiovascular: They have not noticed any sweating or difficulty breathing associated with feeds. GI: They have not noticed significant jaundice; however, they have noticed some swelling around his eyes and in his feet. He has had some loose stools. Neurologic: He does seem to have been more fussy over the last few weeks. Other: He was febrile today.
PHYSICAL EXAMINATION: Temperature is 38 degrees. Heart rate 160s, respiratory rate in the mid-30s, blood pressure 100/60s, saturating 100% on room air. In general, he was a bit fussy; however, calmed quite nicely with a Binky held in place by his mother. HEENT: His anterior fontanelle is open, flat, and soft. He does have evidence of ecchymosis on his left cheek. He has slight scleral icterus. His pupils equal, round, reactive to light. His mucous membranes are moist. Cardiovascular: He has normal S1, S2 with a grade 3/6 systolic ejection murmur noted at the lower left sternal border. His lungs are clear to auscultation bilaterally without appreciable wheezing or crackles. His abdomen is full but soft and nontender. His liver edge is difficult to locate; however, seems to be palpable approximately 2-3 cm below the costal margin. I did not appreciate a palpable spleen. He does not have any scrotal edema. He does not have any significant pitting edema of his lower extremities. He does have some mild periorbital edema. His extremities are warm with 2+ pulses throughout and his capillary refill is less than 2 seconds.
LABORATORY DATA: His labs are significant for a slight alkalosis with a blood gas of 7.39/28n4 in the emergency department. Electrolytes: His bicarbonate is slightly low at 17 but has normal BUN and creatinine. CBC: His hematocrit was initially 24.8 but has decreased to 20 since that time. His MCV is 83, and he has an elevated reticulocyte count; corrected reticulocyte count is 3.9. His platelets are 146, also low, and his white count is 27 with 71 % polys, 11 % monos and 4% bands. His CRP is less than 0.8. His LFTs (liver function tests) are significant for slight elevation in his transaminases, AST 107, ALT 91, but he does have a
hyperbilirubinemia, conjugated bilirubin 4, unconjugated bilirubin 10.3, alkaline phosphatase 1270. His LOH is 810. His triglycerides are 47. His albumin is 2.3. He is coagulopathic. His INR is 5.6. His PT is 48.6, PTT 75 and fibrinogen 60. His Tylenol level is less than 10.
RADIOLOGY: Chest and abdominal x-ray revealed clear lung fields and no cardiomegaly. His abdomen reveals evidence of bowel wall edema and a paucity of abdominal gas but otherwise no significant findings. A limited abdominal ultrasound in the emergency department only shows a bit of intraperitoneal free fluid and some gallbladder thickening and some mild splenomegaly but it was quite limited in the windows that they saw.
ASSESSMENT: Jianhua is a 6-month-old male presenting with acute coagulopathy and hyperbilirubinemia, mixed conjugated and unconjugated, and hypoalbuminemia in the setting of a fever and 3 days of loose stools as well as some edema. His picture is quite confusing as he does not have acute hepatitis with his liver failure. Thus, other etiologies for his coagulopathy would include causes of hemolysis or other genetic, metabolic and infectious causes of acute liver dysfunction need to be within the differential.
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
202 of 2081
PLAN BY SYSTEMS: 1. FLUIDS, ELECTROLYTES, NUTRITION: At this point, given his stable hemodynamics, it is okay for him to eat formula ad lib. We will need to keep a close eye on his fluid status and consider some diuresis if he seems to be retaining significant fluid or requires either boluses of crystalloid or blood products. 2. RESPIRATORY: He is breathing comfortably on room air at this time. 3. CARDIOVASCULAR: He has been hemodynamically stable at this time and we will continue to monitor him. 4. GASTROINTESTINAL: We have consulted our liver failure experts and appreciate their input, which is outlined in their note dated 4/10/2013. In general, our plan is to obtain a more extensive abdominal ultrasound with Doppler to look for any other abnormalities within the liver as well as evidence of portal hypertension or some sort of vascular obstruction that may explain the hyperbilirubinemia and liver dysfunction. We will send a viral hepatitis panel as well as stool alpha-1 antitrypsin and a ferritin as a 1st round look for potential etiologies of his liver dysfunction. We will give him a 1-time dose of vitamin K to determine whether this has any impact on his coagulopathy and we will recheck his coags later on today. If this does not improve his coagulopathy, we will consider correcting him with FFP (fresh frozen plasma) and cryoprecipitates.
5. HEMATOLOGIC: It appears that he has some degree of hemolysis, given his anemia and elevated reticulocytes. His LOH was normal. His hematocrit is 20. At this time we will elect not to transfuse red blood cells; however, it is likely that he will need a transfusion within the next 24 hours. We will continue to follow his hematocrit regularly to ensure that he is not having any bleeding. 6. INFECTIOUS DISEASE: It is noted that he is positive for rhinoviruslenterovirus on his FA; however, at this point he is not exhibiting significant respiratory symptoms from this virus. His other Infectious Disease work-up is outlined in the Gastrointestinal plan. We will continue him on the Zosyn at this time for a rule out, given his liver dysfunction and his fever and the possibility of infectious etiology. 7. IMMUNOLOGY: We will consider HLH (hemophagocytic lymphohistiocytosis) and send a ferritin and wait for this to come back. His triglycerides were normal.
8. SOCIAL: We will continue to support the family through this difficulty, given that their child is critically ill.
Toddler critical care, initial day.
Attending Statement: For this visit I have seen and evaluated this patient, reviewed the history, exam and plan with the resident/fellow. I agree with the note and plan of care as documented above.
Edited and Electronically Authenticated by Lincoln S Smith, MD 04124/2013 12:37 P
Lincoln S Smith, MD , Attending Physician, Critical Care Reviewed by Katie R Nielsen, MD* 04/1412013 05:56 P
Dictated By Katie R Nielsen, MD* , Critical Care Fellow
KRN/sh Doc #2932299 d: 04/1012013 07:03 P t: 04110/2013 0741 P (1554 755-)
cc:
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012 Print Date:
MRN: 1275567 RRID:
9/2312015 13:52 PDT
25788848
203 of 2081
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
204 of 2081
Dale of Service: Authored By: Result Status: Documen1 Type:
CICU I PICU Progress Note
CICU I PICU PROGRESS NOTE XIE, JIANHUA DRACO
DOB: 09/16/2012 M -MR#: 01-27-55-67
4/11/2013 00:00 PDT Smith,Lincoln S,MD (4124/201312:37 PDT) Modified Prag ress Note
DATE OF ADMISSION: 04109/2013 DATE OF REPORT: 04/11/2013
INTERVAL HISTORY: Jianhua is a 6-month-old male with liver failure of unknown etiology who remains critically ill in the Pediatric Intensive Care Unit with severe coagulopathy and fluid overload related to his liver failure. Over the last 24 hours, he had multiple tests sent to determine an etiology for his liver failure. There were many discussions with the family about the necessity for a CT scan of his abdomen to help delineate these lesions in his liver as well as look at the hepatic vasculature. However, after much discussion with the family, they were resistant to the radiation exposure, so therefore, the test was not performed overnight He also will need longer term access with a PICC (peripherally inserted central catheter) line, but that was unable to be done overnight, so we are working on scheduling that over the course of today. Clinically, he was tolerating his feeds, but now he is NPO for potential PICC line placement today. Since being made NPO, he has been quite fussy, but otherwise no acute issues.
REVIEW OF SYSTEMS: 1. FLUIDS, ELECTROLYTES, NUTRITION: He had 897 in and 700 out for a positive fluid balance of 197. He was eating Nutramigen except now he is NPO for a procedure and his electrolytes are within normal limits. 2. RESPIRATORY: He has been stable on room air. 3. CARDIOVASCULAR: He has a sinus rhythm. 4. HEMATOLOGY: His hematocrit is down to 19.4. His platelets are low at 106. His PT is 23.5, INR 2.2 and PTT of 44, and fibrinogen of 250 after receiving FFP and cryoprecipitate. His LFTs (liver function tests) remain moderately elevated with AST of 122, ALT 82, alkaline phosphatase 1204. He has hyperbilirubinemia with unconjugated bilirubin of 8.9 and a conjugated bilirubin is 6.4. 5. INFECTIOUS DISEASE: His white count is down to 23.9 with 52% polys and 2% bands. 6. RENAL: He had low urine output at 0.6 mg/kg/hr, however, had significant mixed output of 469. 7. PAIN AND SEDATION: He has been intermittently fussy but is easily consoled with a bottle.
PHYSICAL EXAMINATION: His T-max is 38.3, heart rate 11 Os-160s, respiratory rate 20s-60s, blood pressure BOs-11 Os over 30-60. I examined him just after his PICC line so he was intubated and sedated on the ventilator, waiting for his general anesthesia to wear off. HEENT: His pupils were 2 mm and reactive bilaterally. He had an endotracheal tube in place. Cardiovascular: He has normal S1 and S2 with a grade 216 systolic ejection murmur heard best at the left lower base. His lungs were clear to auscultation bilaterally. His abdomen
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID: 9/2312015 13:52 PDT
25788848
223 of 2081
is very full, but not tender. It is difficult to palpate a liver edge; however, it appears to be approximately 3 cm below the costal margin. I did not feel a spleen edge_ His extremities are warm and well perfused_
ASSESSMENT: Jianhua is a 6-month-old with liver failure of unknown etiology thus far, who remains critically ill with severe coagulopathy and volume overload in the Intensive Care Unit while undergoing diagnostic workup
for his liver failure.
PLAN BY SYSTEMS: 1. FLUIDS, ELECTROLYTES, NUTRITION: He was NPO for his PICC line placement today and was on half maintenance fluids. Now that he has had his PICC line placed, we will continue him NPO for planned extubation once the general anesthetic wears off. 2. RESPIRATORY: He was stable on room air, but is currently intubated after his PICC line and the plan would be to extubate him either later this evening or tomorrow if there are other invasive procedures that need to be done. 3. CARDIOVASCULAR: His echocardiogram was okay yesterday. 4. HEMATOLOGIC: His coagulation studies improved after the FFP and cryo transfusion yesterday. We will continue to monitor them every 12 hours given his severe coagulopathy. We will also send a second blood type that is necessary as part of his liver transplant workup.
5. INFECTIOUS DISEASE: We will send EBY (Epstein-Barr virus) and CMV (cytomegalovirus) serologies as well as an HIV (human immunodeficiency virus) test and hepatitis C serologies. Given the results of his abdominal CT that he had today that shows evidence of an infiltrative process, we will consult our ID (Infectious Disease) colleagues to help us think about other etiologies for this infiltrative process. 6. GASTROINTESTINAL: As stated above, he had an abdominal CT which shows an infiltrative process with multiple lesions in the liver, a heterogeneous spleen as well as a thickened mesentery which are all consistent with an infiltrative process or an infectious process_ We will continue to explore other etiologies of his liver failure. For now, we will monitor his liver function tests every 12 hours and we await the results of his extensive workup that has been sent thus far, and we will continue to monitor his glucoses q.12h.
7. ONCOLOGIC: We will consult our Hematology-Oncology colleagues to help us determine additional studies that should be done given the appearance of his abdominal CT. 8. SOCIAL: We will continue to support the family during this difficult time when their child is critically ill.
This is toddler critical care, subsequent day.
Attending Statement: For this visit I have seen and evaluated this patient, reviewed the history, exam and plan with the resident/fellow. I agree with the note and plan of care as documented above.
Edited and Electronically Authenticated by Lincoln S Smith, MD 0412412013 12:37 P
Lincoln S Smith, MD , Attending Physician, Critical Care Reviewed by Katie R Nielsen, MD* 04/1412013 05:56 P
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
224 of 2081

Dictated By Katie R Nielsen, MD* , Critical Care Fellow
KRN/clw Doc#2934155 d: 04111/2013 06 58 P 1: 04/11/2013 07:36 P (1555830-)
cc: cc Pediatric Assoc Redmo Julie E Wen, MD
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB:
MRN:
9/16/2012
1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
225 of 2081

Dale of Service: Authored By: Result Status: Documen1 Type:
CICU I PICU Progress Note
CICU I PICU PROGRESS NOTE XIE, JIANHUA DRACO
DOB: 09/16/2012 M -MR#: 01-27-55-67
4/12/2013 00:00 PDT Zimmerman,JerryJ,MD,PhD (4113/201315:19 PDT) Modified Prag ress Note
DATE OF ADMISSION: 04109/2013 DATE OF REPORT: 04/1212013
INTERVAL HISTORY: Jianhua is a 6-month-old male with liver failure of unknown etiology undergoing an extensive diagnostic workup to determine the etiology of his liver failure. He remains critically ill in the PICU with respiratory failure secondary to his encephalopathies following general anesthesia yesterday for a PICC line. Thus, he is being maintained on mechanical ventilation at this time. He also has severe coagulopathy associated with his liver failure. Overnight, he was slow to wake up from his anesthesia; therefore, he remained intubated. In addition, the results of his abdominal CT showed some apparent infiltrative process in his liver as well as abnormal mesentery and heterogeneous spleen. Thus, we consulted our colleagues in Infectious Disease as well as Hematology/Oncology for further evaluation. We still await the official recommendations from Hematology/Oncology but the Infectious Disease Team was concerned about fungus. Therefore, he was started on micafungin overnight.
ADDITIONAL EVENTS: He did get some packed red cells that were followed by a dose of Lasix and, of note, he was hypoglycemic this morning and required a D10 bolus.
REVIEW OF SYSTEMS: 1. FLUIDS, ELECTROLYTES, NUTRITION: He had 799 in and 518 out for a total fluid balance of +281. His electrolytes are significant for a glucose of 30; however, after a D10 bolus, it was in the 80s. His albumin is 2.2. 2. RESPIRATORY: He is on the mechanical ventilator with pressure support ventilation, a PEEP of 5, and a pressure support of 8. With that, end-tidals are in the 30s-40s and his most recent blood gas is 7.35, 41, 46. 3. CARDIOVASCULAR: He is in normal sinus rhythm. 4. GASTROINTESTINAL: He has an elevated ammonia to 50. His AFP yesterday was greaterthan 7000. He continues to have cholestasis with a total bilirubin of 11.1 and conjugated of 4.4. His LFTs are mildly elevated with AST of 109 and ALT of 90. 5. HEMATOLOGY: His INR is 2.9, PT is 29.1, PTT is 50, and fibrinogen is 157. He did not get any products yesterday. His hematocrit is 32%. 6. NEUROLOGIC: His GCS (Glasgow Coma Scale) is 11T. 7. RENAL: His urine output was 1.2 mUkg/hr. His BUN and creatinine are 11 and 0.3.
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID: 9/2312015 13:52 PDT
25788848
220 of 2081
PHYSICAL EXAMINATION: His T-max is 37.1, heart rate 80s-140s, respiratory rate 15-50s, blood pressure 60s-100 over 20s-80s. In general, Jianhua is intubated and sedated but arouses to touch during exam. HEENT: His anterior fontanelle is soft. His pupils are 2 mm and bilaterally reactive. He has an endotracheal tube in place. Cardiovascular: He has normal 51, 52 with a grade 2/6 systolic ejection murmur heard best at the left base. Respiratory: He has no retractions and his aeration is good with no wheezes noted. His abdomen is full but soft and his liver edge is palpable approximately 1 cm below the costal margin. No palpable spleen.
His extremities are warm. He does have some puffiness around his eyelids as well as in his hands and feet.
ASSESSMENT: Jianhua is a 6-month-old male with liver failure of yet unknown etiology undergoing a diagnostic workup for its etiology who remains critically ill in the PICU currently with respiratory failure secondary to medications after a procedure done under general anesthesia yesterday as well as severe coagulopathy requiring close monitoring for his high risk of bleeding. He has not required product in the last 24 hours: however, he does have a slow rise in his coagulopathy over that time.
PLAN BY SYSTEMS: 1. FLUIDS, ELECTROLYTES, NUTRITION: His hypoglycemia is concerning. Therefore, we will change his IV fluids to D10 at half maintenance and check his glucose every 2 hours after his hypoglycemia this morning. We will keep him NPO while he is intubated; however, if we end up extubating him, we may be able to restart feeds. Then we will just need to monitor his glucose prior to eating. 2. RESPIRATORY: Our plan would be to extubate him this morning as he is not going to have any more procedures today. 3. CARDIOVASCULAR: We will continue to monitor. 4. HEMATOLOGY: We will check a CBC every morning. We will add on a white count and platelets to his labs from this morning. We will also continue to follow his coags every 12 hours. 5. INFECTIOUS DISEASE: We will continue Zosyn and micafungin at this time and await further recommendations for diagnostic workup from the Infectious Disease Team. 6. GASTROINTESTINAL: We will continue to follow his coags and LFTs every 12 hours. Otherwise, we have undergone an extensive workup for his liver failure and will await the results of those tests. 7. METABOLIC: We will consult our colleagues in Metabolic Genetics to determine whether we should do further workup. In addition, we will send serum amino acids and urine organic acids, as well as an acylcarnitine profile given his hypoglycemia and his mildly elevated ammonia to delineate further etiologies of his liver
failure. B. PAIN AND SEDATION: He is only getting intermittent fentanyl as we plan to extubate him later. 9. CONSULT: We will consult Ophthalmology to evaluate his eyes for any other ophthalmologic findings that may give us an etiology for his liver failure.
PCCM Staff Addendum: I have personally examined Jianhua, reviewed his interval clinical course, laboratory data, provided oversight of morning interdisciplinary rounds regarding his care plan with the PICU Service and the Gastroenterology Service, and directly supervised Dr Katie Nielsen, the senior Pediatric Critical Care Medicine Fellow/Acting Attending PICU Staff. Dr Nielsen's progress note above has been reviewed. I agree with her findings, assessments and plans. Additional pertinent aspects of the interval history, physical exam and laboratory data include the following:
Active, ongoing investigation for cause of acute hepatic failure. Chemical coagulopathy stable, without clinical evidence of active bleeding. Ascites, but no significant restrictive lung disease.
Seattle Children's Hospital
PO Box 5371
Seat11e, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012
MRN: 1275567
Print Date:
RRID:
9/2312015 13:52 PDT
25788848
221 of 2081
Remains in viral respiratory precautions for rhinovirus infection. No abnormal retinal findings on Ophthalmology examination. Biochemical Genetics consultation pending. Increasing scleral icterus. Anxious, astute parents. Will likely need to add a continuous infusion of dextrose to avoid hypoglycemia. Not encephalopathic at this time. Discontinued from mechanical ventilation and tracheally extubated without problem.
Toddler Critical Care Services, subsequent days
Attending Statement: For this visit I have seen and evaluated this patient, reviewed the history, exam and plan with the resident/fellow. I agree with the note and plan of care as documented above.
Electronically Authenticated by Jerry J Zimmerman, MD, PhD 04/13/2013 03:19 P
Jerry J Zimmerman, MD, PhD PhD, Attending Physician, PICU
Dictated By Katie R Nielsen, MD* , Critical Care Fellow
KRN/srl Doc #2935636 d: 04/1212013 06:41 P t: 04112/201 3 07 15 P (1556808-)
cc: cc Pediatric Assoc Redmo Julie E Wen, MD
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, J IANHUA DRACO
DOB: 9/16/2012 Print Date:
MRN: 1275567 RRID:
9/2312015 13:52 PDT
25788848
222 of 2081

Consult
Date of Service: 04/11/20130:00:00 Authored By: Fong, Abraham P, MD, PhD
Hematology Consultation
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
HEMATOLOGY CONSULTATION
XIE, JIANHUA DRACO DOB: 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 04/09/2013 DATE OF CONSULTATION: 04/11/2013
IDENTIFICATION: We were asked by Dr. Lincoln Smith to evaluate this 6-month-old male, previously healthy, with regards to his most recent findings on CT of liver lesions and possible infiltrative process to evaluate for malignancy.
HISTORY OF PRESENT ILLNESS: Patient is a 6-month-old male with no significant past medical history who was healthy until approximately 1 week ago when parents noticed increasing loose stools which significantly increased on Sunday (5 days ago) and then over the following 2 days they noticed worsening generalized edema and jaundice. He presented to his pediatrician on Tuesday, 4/9, and were promptly sent to at Seattle Children's Emergency Room. In the emergency room, he was febrile, T-max of 40 degrees Celsius. Blood cultures were drawn and he was given a dose of ceftriaxone. He did have 1 episode of nonbloody, nonbilious emesis and received normal saline boluses for fluid resuscitation. Laboratory values at that time demonstrated coagulopathy with an INR of 5.6, hyperbilirubinemia, and a mild transaminitis. He was transferred to the ICU for further evaluation and treatment of his coagulopathy as well as close monitoring. He underwent ultrasound of the abdomen and CT of the chest, abdomen and pelvis today which prompted the consultation.
REVIEW OF SYSTEMS: Parents deny any weight loss or recent fevers other than the fever in the emergency room. A 5-day history of diffuse edema and jaundice and intermittent but progressively worsening loose stools was reported. Loose stools were yellow, he did have emesis in the emergency room, which was nonbloody, nonbilious. He has otherwise been active and developing well. Parents deny any unusual lymphadenopathy, skin rashes, bruising, scleral icterus, weight loss, failure to gain weight, loss of milestones.
Per her parents, patient has been otherwise well. He was diagnosed with RSV (respiratory syncytial virus) infection in January but did not require hospitalization. He has had frequent loose stools for most of his life requiring change in formulas but has continued to grow and develop well.
PAST MEDICAL HISTORY: Patient was born 10 days prior to his due date. Pregnancy was uncomplicated. His formula was converted from a milk-based formula to a soy-based formula at approximately 2 months of age. As stated, he had an RSV (respiratory syncytial virus) infection in January, not requiring hospitalization. He has been growing and developing well.
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012 MR: 1275567
Print Date 6/18/2013
I
I Consult
Date of Service: 04/11/2013 0:00:00 Authored By: Fong, Abraham P, MD, PhD
SOCIAL HISTORY: Parents live at home, mother, father, and 3 siblings, all of whom are currently healthy. He has not had recent travel exposure.
FAMILY MEDICAL HISTORY: Father does report approximately 1 week ago he did have what seemed to be gastroenteritis with diarrhea which resolved over 2 days. Mom has a history of "low platelets" though she has never had any bleeding or bruising difficulties. His older brother did have an episode of thrombocytopenia last October following a viral illness which did not require any therapies nor hospitalization and has since resolved. His other siblings are healthy. There is a history of a maternal grandfather with pancreatic cancer, developed in his 60s. No other maternal family history. Paternal family history is unknown as per dad his family lives in a small town without healthcare in China and many adult family members die young. However, there is not a history of childhood deaths.
MEDICATIONS: Albuterol as needed for wheezing Piperacillin/tazobactam 945 mg q.8h.
ALLERGIES: No known drug allergies.
ADMISSION PHYSICAL EXAMINATION: Temperature 36.3, heart rate 110, respiratory rate 34, oxygen saturations 100, blood pressure 77/30. General: Patient is in no acute distress. HEENT: Sclerae are anicteric. Moist mucous membranes. No nasal congestion. No appreciable cervical lymphadenopathy. Patient is intubated with the ET-tube in his mouth. I cannot fully examine his intraoral cavity. Chest: Clear to auscultation bilaterally. Cardiovascular: 2/6 systolic murmur heard at the left sternal border. 51, 52, regular rate and rhythm. Abdomen: Protuberant with fluid wave, reducible umbilical hernia. Liver edge approximately 3 cm below the costal margin, spleen 2-3 cm below the costal margin. Extremities are edematous. 2+ pulses throughout. Lymphatics: no appreciable lymphadenopathy
LABORATORY DATA 4/9: Blood gas pH of 7.43, C02 of 23, oxygen of 135, bicarbonate of 14.8. Sodium 135, potassium 5.2, glucose 120, ionized calcium 1.27, lactic acid 3.1 at 8:30, at 10: 15 lactic acid was 2.1, CRP less than 0.8, amylase and lipase less than 30 and less than 10, GGT 54. Rhinovirus positive. White blood count 27, hematocrit 24.8, platelets 146, ANC 20250, no blasts. 4110: PTT 48.6, INR 5.6, PTT 75, fibrinogen 60, total protein 4.1, ionized calcium 1.15, ferritin 93, conjugated bilirubin of 4.0, unconjugated 10.3, AST 107, AL T 91, alkaline phosphatase 1270, triglycerides 47, albumin 2.3, LDH 810 Hepatitis A IgM nonreactive, hepatitis A total antibody reactive, CMV (cytomegalovirus) negative, EBV (Epstein-Barr virus) negative. Parvo negative. CMV IgG positive, IgM negative, EBV IgG positive, IgM Tylenol level less than 10 Alpha-fetoprotein 7080, ammonia 40. negative.
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Print Date 6/18/2013
I
I Consult
Date of Service: 04/11/20130:00:00 Authored By: Fong, Abraham P, MD, PhD
4111: Total bilirubin 11.1, conjugated 3.5, unconjugated 6.7, AST 94, ALT 84, alkaline phosphatase 10, 67, ammonia 43, lactic acid 0.9, albumin level 2.0.
IMAGING: 419 at 11:48 p. m.: Abdominal ultrasound: Mild intraperitoneal free fluid. Mild diffuse gallbladder wall thickening with cholelithiasis and pericholecystic fluid, likely related to volume overload, third spacing, mild hepatomegaly, trace bilateral pelviectasis. Ultrasound 4110 at 10:30 in the morning: Edematous-appearing liver with interval development of multiple small echogenic foci throughout the right lobe of the liver. The latter findings suggesting a diffuse inflammatory etiology including septic emboli, persistent splenomegaly, contracted gallbladder, likely reflecting nonfasting state, trace central pelviectasis of the right kidney, small amount of anechoic fluid and peritoneal fluid, abnormally elevated resistive indices measuring 1.0 throughout the liver, recanalization patency of the umbilical vein in conjunction with splenomegaly suggestive of portal hypertension.
CT of the chest, abdomen and pelvis: Diffuse hazy mesentery which could represent edema in the setting of portal hypotension including recanalization of the paraumbilical vein, minimal gastric varices and moderate splenomegaly as well as diffuse subcutaneous edema, numerous small hypodense hepatic lesion too small to further characterize, and intermediate fatty density is seen within several lesions. Sigmoid colon and rectal wall thickening of mucosal hyperenhancement, bilateral dependent air space opacities.
ASSESSMENT AND PLAN: 6 month old male with diffuse anasarca, hyperbilirubinemia, coagulopathy, anemia, thrombocytopenia and leukocytosis suggestive of acute hepatiC failure and unlikely to be due to an underlying oncologic process.
Oncologic hepatic infiltrative processes do occur. There are cases reported in the literature of acute liver failure due to leukemia. However, I would expect that the patient would be pancytopenic and he does have a robust neutrophil count which leads us away from the diagnOSis of leukemia. Given the patient's coagulopathy and the low suspicion for leukemia we do not recommend a bone marrow evaluation at this time. Neuroblastoma can infiltrate the hepatic tissue and I would recommend sending VMNHVA labs. I am reassured that we have a CT scan of the chest, abdomen and pelvis which does not reveal any masses that would represent a primary lesion. Lymphoma can metastasize to the liver but typically presents with other mass lesions and the liver lesions develop over time (the patient's liver lesions developed over a 10 hour period early in admission). Finally, primary hepatic neoplasms, such as hepatoblastoma, are typically large masses and, again, do not develop over a period of hours. We feel the liver failure is likely due to an isolated hepatiC process and much less likely an oncologic process. We do not recommend further evaluation for a neoplasm at this time.
Thank you for the very interesting consult. Please do not hesitate to contact us with any questions or concerns.Attending Statement: For this visit I have seen and evaluated this patient, reviewed the history, exam and plan with the resident/fellow. I agree with the note and plan of care as documented above.
Edited and Electronically Authenticated by Abraham P Fang, MD, PhD 041161201310:06 P
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Print Date 6118/2013
I

f Consult
04/11/2013 0:00:00 Date of Service', Authored By: Fang, Abraham P, MD, PhD
Abraham P Fong, MD, PhD , Attending Physician, Hem-One Reviewed by Corinne N Summers, MO' 04/12/2013 06:15 P
Dictated By Corinne N Summers, MO' ,Fellow
CNSlelw Doc#2934232 d: 041111201309:44 P t: 041111201310:52 P (1555889-) ee: ec Pediatric Assoc Redmo
Julie E Wen, MD
Seattle ChHdren's Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Prmt Date 6/18/2013
I
Date of Service: 04/12/20130:00:00 Authored By: Frenkel, Lisa M, MD
Inf. Disease Consultation
Consult
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
INF. DISEASE CONSULTATION
XIE, JIANHUA DRACO DOB: 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 04/09/2013 DATE OF CONSULTATION: 04/12/2013
This consultation is requested by Dr. Lincoln Smith of the Pediatric Intensive Care Unit Service.
HISTORY OF PRESENT ILLNESS: Jianhua is a 6-month-old male with severe coagulopathy, cholestasis and mild transaminitis of unclear etiology, admitted to Seattle Children's Hospital on 4/9/2013. Per parents' report, Jianhua had a 3-day history of diarrhea, consisting of loose stools with increased volume that were non bloody without mucus. 1 day prior to admission, parents noted jaundice and periorbital edema and abdominal swelling. He was seen in the Seattle Children's Hospital Emergency Department and had a fever to 40 degrees Celsius with an elevated white blood cell count of 27 with 4% bands and 71 % polys. CRP was less than 0.8. He was found to have a severe coagulopathy with INR 5.6, elevated conjugated bilirubin of 4, mild transaminitis and hypoalbuminemia.
An abdominal ultrasound with Doppler on 4/10 demonstrated multiple echogenic foci in the right lobe of the liver. Abdominal CT with angiogram demonstrated hypodense lesions in the right low with hazy mesentery and secondary portal hypertension with bowel wall thickening. Echocardiogram did not demonstrate any evidence of vegetations. He is currently undergoing an extensive workup along with Gastroenterology, Biochemical Genetics and Hematology-Oncology teams. He was initially given a dose of ceftriaxone on 4/9 and was started on piperacillinltazobactam on 4/10. Micafungin was added on 4/11 for concern of possible fungal process, given lesions seen on his abdominal CT scan. However, he has defervesced on antibiotic therapy with a white blood cell count falling from 27 to 15.6 and is currently afebrile. He had an ophthalmology exam today which did not reveal any evidence offungal infection or metabolic abnormality.
Infectious Disease evaluation to date has included testing for viral etiologies that may cause liver failure, including CMV (cytomegalovirus), EBV (Epstein-Barr virus), HBV, and parvovirus PCR from serum, which have all been negative. There is no evidence of acute hepatitis A, B, or C. Pending labs at the time of this dictation include enterovirus, adenovirus, VZV (varicella zoster virus), HSV, HHV-6 and HIV from the blood.
PAST MEDICAL HISTORY: 1. 38 weeks' gestation. Pregnancy was complicated by an abnormal amniocentesis. The patient reportedly has a duplicated Y chromosome. 2. Mother reports normal prenatal labs including negative HIV test.
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012 MR: 1275567 Print Date 6/18/2013
I
Consult
Date of Service: 04/12/20130:00:00 Authored By: Frenkel, Lisa M, MD
3. RSV (respiratory syncytial virus) bronchiolitis, age 3 months. Mother notes that this did not seem to resolve and the patient had persistent wheezing after the initial episode. 4. History of emesis early in life which improved after transitioning to soy formula. 5. Abnormal stools. The patient's parents noted "greasy stools" since birth that the thought were notably different in consistency compared to the newborn stools of other children. 6. There is no history of recurrent infections. Jianhua has not had prior episodes of pneumonia, otitis media or cellulitis. 7. Oral intake: Jianhualnitiated solid foods 3 weeks prior to presentation, eating mostly rice cereal, as well as a variety of other fruits.
FAMILY HISTORY: The father had diarrhea 1 week prior to Jianhua's presentation. Reportedly, the mother had a history of low platelets and older brother also had a history of low platelets in the setting of an infection. There is no family history of recurrent infections or immunodeficiencies. There are no children that have died at an early age of unknown etiology.
SOCIAL HISTORY: The patient lives with his mother, father, and 3 older siblings in Redmond. Both parents are optical engineers. There are no pets in the home. The patient does not have cat exposure. Mother notes that there were mice in the home during the holidays in December when she observed mice excrement in the flour and rice bags. Jianhua did not ingest any of the affected food. Both parents are from China and immigrated to the United States in 1997. Jianhua has had no international travel and has not traveled outside of the state of Washington. There is no known TB (tuberculosis) exposure. No known ingestion of mushrooms or reheated food.
REVIEW OF SYSTEMS: A full review of systems was performed. All positives and pertinent negatives related to the current problem were noted in the History of Present Illness. All other systems were negative.
MEDICATIONS: 1. Ceftriaxone x1 on 4/9. 2. Piperacillinltazobactam on 4/10 to present. 3. Micafungin 4/11 to present.
Please see CIS (Clinic Information System) for additional medications.
ALLERGIES: No known drug allergies.
LINES: PICC line placed on 4/11.
PHYSICAL EXAMINATION: The patient had a temperature of 36.8, heart rate 103, respiratory rate 25, oxygen saturation 100% on room air and systolic blood pressure 86/40. In general, the patient is lying in bed. HEENT: Normocephalic, atraumatic. Facial edema present. Eyes have scleral icterus. Pupils are equally round and reactive to light. Oropharynx is clear, without lesions or exudate. Tympanic membranes are clear bilaterally with no infusion or injection. Neck is supple with full range of motion. Respiratory: Clear to auscultation bilaterally, no wheezes, rales, or rhonchi. Cardiac: Regular rate and rhythm, no murmurs, rubs, or gallops. Abdomen is protuberant, with evidence of ascites. Spleen is approximately 5 cm below the costal margin and
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB 09/16/2012
MR: 1275567 Print Date 6/18/2013
I

Consult
Date of Service: 04/12/2013 0:00:00 Authored By: Frenkel, Lisa M, MD
the liver is approximately 4 cm below the costal margin. Abdomen is soft and nontender. Lymphatic: No cervical, axillary, or groin lymphadenopathy. Musculoskeletal: Normal range of motion of all joints. No joint warmth, tenderness, or effusion. Genitourinary: Not performed. Neurologic: Cranial nerves II-XII intact. Patient moves all 4 extremities spontaneously. Skin: Scattered erythematous depositions on his forehead. No other lesions appreciated.
LABORATORY VALUES: White blood cell count 15.6 with 6% bands, 43% polys, 32% lymphocytes, 15% monos, and 1 % eosinophils. White blood cell count has decreased from 27 on 4/9 and 23 on 4/10. Respiratory viral PCR was positive for rhinovirus. MRSA surveillance cultures are negative. Pertussis is negative. CMV, EBV, and parvovirus PCR are negative. Hepatitis A virus serologies, IgM negative, IgG positive. Hepatitis B serologies, surface antigen negative, IgG negative. CMV IgM negative, IgG positive. EBV IgM negative, IgG positive. EBNA positive. Pending viral PCRs from serum; Enterovirus, adenovirus, VZV (varicella zoster virus), HSV, and HHV-6. HIV screening is pending. Blood cultures from 4/9 are no growth to date. Urine cultures from 4/9 growing 1-10,000 Klebsiella, 1-10,000 colonies of E. coli, pan susceptible. Stool culture from 4/10 is no growth to date. Rotavirus is negative, IgG is 479.
ASSESSMENT AND PLAN: Jianhua is a 6-month-old male with severe coagulopathy, cholestasis, hypoalbuminemia and mild transaminitis, who presents with fever and a 3-day history of diarrhea. Overall, Jianhua's process appears more consistent with an underlying chronic metabolic process leading to liver synthetic dysfunction rather than fulminant liver failure given his mild transaminitis. For example, galactosemia can present with gram negative infections, which is a consideration given his mildly abnormal reducing substances on laboratory evaluation. He presented with fever and elevated white blood cell count to 27 with a left shift and 6% bands, suggestive of bacterial process which may have complicated a more chronic underlying noninfectious process affecting liver synthetic function. Given his ascites, he would be at risk for a primary bacterial peritonitis. Other possibilities include cholangitis, though no bile duct dilation was seen on evidence of abdominal CT. Many studies have been sent that would help explain acute fulminant liver failure in this patient, though the patient has a more mild transaminitis than what would be classically seen with fulminant liver failure due to hepatic necrosis from a viral infection, such as Hepatitis A. However, we would recommend testing for hepatitis E virus with IgM and IgG serologies and sending hepatitis B DNA PCR, although would expect Hepatitis B to present later in life without such prominent coagulopathy. Reoviruses such as rotavirus may cause cholestasis and affect the liver, though stool rotavirus is negative. We would recommend sending viral cultures of the throat and stool. Regarding possible bacterial causes, Bartonella can present with a granulomatous hepatitis. Another consideration is leptospirosis which can present with jaundice and transaminitis, given the history of mice in the home. Fungal etiologies would be very unlikely with the patient's presentation, unless he had an underlying immune dysfunction. He has not had prolonged lymphopenia or neutropenia, placing him at low risk. However, we would recommend evaluation for chronic granulomatous disease with a neutrophil oxidative burst study and other primary immunodeficiencies with T and B cell subsets.
Regarding antibiotic management, given the low likelihood of fungal etiologies, we would feel comfortable discontinuing micafungin at this time. We would continue of piperacillinltazobactam for broad coverage of gram-positive and gram-negative and anaerobic organisms that would be possibly involved in peritonitiS or cholangitis, and follow blood cultures.
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME:
DOB: MR:
XIE, JIANHUA DRACO
09/16/2012
1275567 Print Date 6/18/2013
I
Date of Service: Authored By:
04/12/20130:00:00 Frenkel, Lisa M, MD
RECOMMENDATIONS: 1. Continue piperacillin/tazobactam. 2. Discontinue micafungin. 3. Stool viral culture. 4. Throat viral culture. 5. Neutrophil oxidative burst. 6. T and B cell subsets. 7. Hepatitis E IgG, IgM. 8. Hepatitis B DNA PCR. 9. Leptospirosis serologies. 10. Bartonella serologies.
Consult
Thank you very much for this interesting consultation. We will continue to follow this patient with you and provide additional recommendations as needed. Please do not hesitate to contact us with any additional questions.
Attending Statement: For this visit I have seen and evaluated this patient, reviewed the history, exam and plan with the residentlfellow. I agree with the note and plan of care as documented above.
Edited and Electronically Authenticated by Lisa M Frenkel, MD 04/16/2013 01:02 P
Lisa M Frenkel, MD , Attending Physician, Infectious Disease Reviewed by Lisa M Cranmer, MD, MPH" 04/15/2013 08:55 P
Dictated By Lisa M Cranmer, MD, MPH' ,Fellow, Infectious Disease
LMC/dma Doc #2935728 d: 0411212013 09:14 P t: 0411212013 10:45 P (1556853-) LMCldma; Doc #2935730 d: 041121201309:41 P t: 041121201310:56 P (1556858-)
cc: cc Pediatric Assoc Redmo julie E Wen, MD
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME:
DOB:
MR:
XIE, JIANHUA DRACO
0911612012
1275567
Print Date 6/1812013
I

Consult
Date of Service: 04/10/2013 0:00:00 Authored By: Hsu, Evelyn Kanyu, MD
GI Consultation
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
GI CONSULTATION
XIE, JIANHUA DRACO DOB: 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 04/09/2013 DATE OF CONSULTATION: 04/10/2013
REQUESTING PROVIDER: Lincoln Smith, MD, of the Pediatric Intensive Care Unit.
REASON FOR CONSULTATION: We are asked by Dr. Smith of the Pediatric ICU to consult on the care of Jianhua Xie regarding coagulopathy, hypoalbuminemia, ascites, fever and jaundice in a 6-month-old male.
HISTORY OF PRESENT ILLNESS: Jianhua is a 6-month-old male who was previously healthy up until several days ago, when he developed periorbital edema, jaundice and abdominal distension following 3 days of diarrhea. Also, since about a month ago, his weight has gone from the 50th percentile up to the 90th percentile. Parents noted that prior to the development of the diarrheal illness he did not have any jaundice. He was brought first to the primary care provider for evaluation, and subsequently was referred to the SCH emergency room. In the emergency room he developed a fever of 40, Blood cultures were drawn and he was given ceftriaxone. He also had 1 episode of emesis, nonbilious, non bloody. He received a total of 30 mUkg of normal saline. Upon laboratory evaluation, he was found to be coagulopathic, with an INR of 5.6, conjugated bilirubine was 4, AST and ALT only mildly elevated at 107 and 97 respectively. He was subsequently admitted to the Pediatric ICU for further workup as well as transitioned to piperacillin-tazobactam for antibiotic coverage.
In retrospect, parents felt that he has become more weak over the last week, and has definitely gained weight faster over the past month. Otherwise, they do not feel that he is any more irritable than normal.
MEDICATIONS: Home medications: None. He is currently receiving: 1. Piperacillin-tazobactam 945 mg every 8 hours. 2. Albuterol nebulizer once daily as needed for wheezing.
ALLERGIES: No known drug allergies.
PAST MEDICAL HISTORY: Patient was born 10 days early, but essentially at term. Pregnancy was uncomplicated. He is the 4th child in his family. He did have some issues with diarrhea and vomiting early on. He was switched from cow's milk-based formula to soy milk-based formula and has been on that since 2
Seattle Children's Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09116/2012
MR: 1275567 Print Date 6/1812013
I
Consult
Date of Service: 04/10/20130:00:00 Authored By: Hsu, Evelyn Kanyu, MD
months of age. He also had RSV (respiratory syncytial virus) in January, but did not require, but has had some chronic wheezing since that time. He has otherwise not had any hospitalizations or surgeries.
SOCIAL HISTORY: Patient lives at home with his mother, father, and 3 older siblings, all of whom are healthy. He has had no travel, no exposures, and he is currently at home with his grandmother, and parents deny vehemently that he has received any herbal or eastern medicine, no supplements. The only medications that he may have had access to were vitamins.
FAMILY HISTORY: Noncontributory other than that his father had had some symptoms of vomiting and diarrhea that were consistent with a rotavirus infection over the weekend. There is no other illness. His father brought up that in the last 20 days Jianhua has been taking formula that was ordered online through an independent seller through Amazon. They are concerned that this formula may have been tainted in some way, and would like for it to be examined.
REVIEW OF SYSTEMS: Positive for a history of wheezing following RSV infection. He has had relatively good weight gain. He has jaundice, coagulopathy, hypoalbuminemia, some irritability today. Parents also note that ever since birth he has had what they feel to be greasy stools. No bruising, no bleeding, no petechiae, no skin rash. A 14-element review of systems is otherwise negative except for those mentioned in the HPJ.
PHYSICAL EXAMINATION: Temperature at admission was 40. Heart rates have ranged 130-183, respiratory rate ranging 27-60, blood pressures ranging 74-135 over 20-85. His weight on admission was 9.98 kg. In general, this is a crying, vigorous infant male. He has periorbital edema and some lower extremity edema. HEENT exam: He has some mild scleral icterus. Pupils equal, round, and reactive to light. Extraocular movements intact. Cardiovascular: He has regular rate and rhythm. He does have a 2/6 systolic ejection murmur heard best at the left upper sternal border. There is no thrill, no hyperdynamicity. Respiratory exam: Clear to auscultation bilaterally, no wheezes, no rales, no increased work of breathing, no retractions. He does have intermittent coughing. Abdomen is soft, moderately distended, with an easily reducible umbilical hernia. No palpable hepatomegaly; however, I do feel a spleen down to 2 cm below the left costal margin. He does not have any increased superficial vasculature over his abdomen. GU exam does not have any scrotal edema. He is a normal Tanner I male. There is no evidence of any diaper rash. Extremities are prominent for lower extremity edema, no pitting. Neurologically, patient is moving all 4 extremities and his neurologic exam is grossly normal. He does seem irritable, but will calm when held.
LABORATORY EVALUATIONS: Labs are significant for a blood test showing a pH of 7.39, pC02 28, p02 venous of 74, bicarbonate level of 16.3. Initially on presentation his sodium level was 134, potassium 5.0, chloride 110, bicarbonate 17. Anion gap was 1. Glucose level has been normal, ranging above 80-120. BUN 9, creatinine 0.2, calcium 1.28, magnesium 2.4, phosphorus low at 3.4, lactates ranging 2.1-3.1. White blood cell count high at 27.0, platelets 146, hemoglobin 8.1, hematocrit 24.8. INR 5.6 with a prothrombin time of 48.6. Fibrinogen is 60, PTT 75. Urinalysis showed a urine specific gravity of 1.021 but a urine pH of less than 5, negative for nitrites, leukocyte esterase, and glucose, positive for trace protein, positive for trace ketones, negative for blood. Stool occult blood was negative.
Blood cultures have been drawn and are still negative. Stool cultures have also been done. Rotavirus was found to be negative. Respiratory viral PCR was positive for rhinovirus/enterovirus. Acetaminophen level was
Seattle Children's Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012 MR: 1275567 Print Date 6/18/2013
I
, Consult
Date of Service: 04/10/20130:00:00 Authored By: Hsu, Evelyn Kanyu, MD
less than 10, B natriuretic peptide was 33. Liver enzymes show AST of 107, AL T of 97, alkaline phosphatase of 1270. Uric acid 4.3, triglycerides low at 47, LDH 810 and normal, albumin level 2.3, conjugated bilirubin 4.0, un conjugated 10.3, ferritin 93, total protein low at 4.1, ionized calcium 1.15. Ammonia level 40. PTIINR following 1 dose of vitamin K showed a prothrombin time of 46.3, INR 5.3, PTT 69, fibrinogen 80, and a thrombin time of 19. Bordetella pertussis PCR was negative.
Abdominal ultrasound with Doppler study shows edematous liver exhibiting decreased through-transmission, small echogenic foci throughout the right lobe of the liver, contracted gallbladder; spleen is slightly enlarged, measuring 8.4 cm; patent IVC, hepatic veins, portal vein. There was an incidental note of recanalization of the umbilical vein. There was some small amount of anechoic free intraperitoneal fluid. Differential diagnosis for echogenic hepatic foci includes septic emboli, metastatic lesions, and the possibility of hemorrhagic infarcts.
An echocardiogram done today in the afternoon showed no intracardiac vegetation, no intracardiac shunting, normal valvular structure and function, no pericardial effusion, some mild increase in velocity across aortic, pulmonary, and mitral valves, indicating hyperdynamic or fluid overloaded status.
ASSESSMENT AND PLAN: Jianhua is a 6-month-old previously healthy male with a history of some milk protein sensitivity, who presents with of coagulopathy, jaundice, hepatitis, abdominal distention, and hypoalbuminemia in the setting of fever and diarrhea. Imaging findings, coagulopathy unresponsive to vitamin K, and lack of improvement with antibiotic treatment suggests that there is intrinsic liver dysfunction and possible acute liver failure, What remains perplexing is that his degree of transaminase elevation is not as high as we would typically see with a viral hepatitis-induced liver failure, yet the coagulopathy, jaundice and presence of portal hypertension suggests possible chronic liver disease. Also within our differential, and thinking outside of the realm of liver disease, we continue to worry about sepsis/DIC (disseminated intravascular coagulation) like picture also leading to coagulopathy and elevated un conjugated bilirubin. Hemolysis (although LDH is low) remains a concern. A haptoglobin level may help to evaluate this. ,Our differential for acute liver failure would include a viral hepatitis, metabolic disease (tyrosinemia, galactosemia, hereditary fructose intolerance, cystic fibrosis associated liver disease, alpha-1 antitrypsin liver disease), toxin induced disease, autoimmune liver disease, malignancy. Vascular obstruction or cardiac associated liver disease unlikely, as we have normal imaging of the heart and no obstruction seen on Doppler study of the liver. Within the differential for infectious causes of acute liver failure we should evaluate for hepatitis A, EBV (Epstein-Barr virus), CMV (cytomegalovirus), adenovirus, enterovirus, hepatitis B surface antigen, HSV, HHV-6, parvovirus, coxsackie, and varicella. HIV test should be done for pre-transplant work-up. With regards to possible autoimmune processes, his ferritin and triglycerides are not consistent with an HLH (hemophagocytic Iymphohistiocytosis) like picture, We will be sending factor levels as well as an alpha fetoprotein. We have an autoimmune panel which is pending. With regards to possible metabolic causes of liver disease, we have requested urine organic acids, urine reducing substances, and urine succinylacetone, as well as a galactosemia screen and serum amino acids and acylcarnitine profile. It is possible that this could be some toxicity or ingestion although extensive questioning has not yielded any untoward exposures, We will be in contact with our Toxicology colleagues regarding father's request to test the formula that he had ordered online.
Jianhua's condition is currently guarded. I spent an extensive amount of time discussing with his parents our current plan for workup and possible need for increased intervention and life-sustaining measures should his
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 0911612012
MR: 1275567
Print Date 6/18/2013
I
I Consult
Date of Service: 04/10/20130:00:00 Authored By: Hsu, Evelyn Kanyu, MD
liver failure worsen. We will need to monitor Jianhua very closely with regards to his coagulopathy and support him as needed. We would also need to be very judicious in the amount of IV fluids that he gets and allow him to take enteral intake as long as he is able. I would continue his antibiotics until our blood cultures and urine cultures are known to be negative, as the greatest risk to his life right now would be infection. We will involve the Liver Transplant Team should Jianhua's clinical status start to deteriorate. We should monitor his weights on a twice daily basis and monitor his ins and outs carefully. We should monitor liver function and coagulation panel every 12 hours.
Electronically Authenticated by Evelyn K Hsu, MD 04/11/201312:52 P
Evelyn K Hsu, MD , Attending Physician, Gastroenterology
EKH/jmc Doc#2932273 d: 04/1012013 05:46 P t: 0411012013 06:33 P (1554684-) cc: cc Pediatric Assoc Redmo
Julie E Wen, MD
Seattle Children's Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DaB: 0911612012 MR: 1275567 Print Date 6/1812013
I

Consult
Date of Service: 04/22/20130:00:00 Authored By: Hsu, Evelyn Kanyu, MD
Transplant Consultation
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
TRANSPLANT CONSULTATION
XIE, JIANHUA DRACO DOB: 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 04/09/2013 DATE OF CONSULTATION: 04/2212013
Jianhua is a 7 -month-old male with end-stage liver disease secondary to cirrhosis of unknown etiology. Liver biopsy showed irrecoverable cirrhosis and he requires listing for liver transplantation.
I discussed with the family the issues surrounding liver transplant, both listing, pretransplant wait time, the transplant stay itself, and long-term complications as well as explaining outcomes and our expectations for long-term survival. We specifically reviewed potential complications including vascular stenoses and thromboses, biliary stenoses, immunosuppression and the potential for rejection as well as infectious complications including EBV (Epstein-Barr virus) and the possibility of PTLD (posttransplant Iymphoproliferative disorder). They were given the opportunity to ask any questions. They had a good understanding of the procedure and of his need for liver transplant. He will be discussed at our multidisciplinary selection meeting once his evaluation is complete and we will then communicate with the family and the referring physicians about our recommendations, but I see no contraindications to listing for liver transplant at this stage.
Electronically Authenticated by Evelyn K Hsu, MD 04/23/201312:22 P
Evelyn K Hsu, MD , Attending Physician, Gastroenterology
EKH/sh Doc #2946987 d: 041221201301:30 P t: 04/22/201306:51 P (1563799-) cc: cc Pediatric Assoc Redmo
Julie E Wen, MD
Seattle Children'S Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567
Print Date 6/18/2013
I
Consult
Date of Service: 04/12/2013 0:00:00 Authored By: Merritt II, J Lawrence, MD
Biochem Genetic Consultation
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
BIOCHEM GENETIC CONSULTATION
XIE, JIANHUA DRACO DOB 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 04/09/2013 DATE OF CONSULTATION: 04/12/2013
REFERRING PHYSICIAN: Dr. Lincoln Smith and Dr Evelyn Hsu.
CHIEF COMPLAINT: A 6-month-old male with acute liver disease.
HISTORY OF PRESENT ILLNESS: Biochemical Genetics was asked to consult on this 6-month-old male who approximately 1 week ago developed increasing peripheral and body edema. He had been having some diarrhea and vomiting beginning for about 2 days prior to admission and then is significant edema and jaundice then developing. He was found to have profound acute liver disease with a fever of 40 degrees Fahrenheit. Blood cultures were drawn and he was given ceftriaxone. He was found to be coagulopathic with an INR of 5.6, conjugated bilirubin of 4 and mild elevations of his AST and ALT. He was admitted to the Pediatric ICU for work-up and received antibiotics for rule out infection. His parents report that other than having been maybe a little bit weak over the past week, he was not otherwise have any other problem. He had been gaining weight a little bit more over the past month. He had not been having other significant acute issues.
Here in the hospital, he was found to have mild hepatomegaly. A liver ultrasound then demonstrated a moderate amount of intraperitoneal fluid, diffuse gallbladder wall thickening and mild splenomegaly. Ultrasound with Doppler demonstrated a liver appearing edematous with portal hypertension. Liver also was found to have multiple small echogenic foci throughout the right lobe of the liver suggesting diffuse inflammatory etiology including septic emboli, metastatic lesions or possibly hemorrhagic infarcts. He then had an abdominal CT performed which reported moderate hepatomegaly. He had a diffuse hazy mesentery, possibly representing edema in the setting of the portal hypertenSion. The small hypodense hepatic lesions were otherwise too small to further characterize. They may have been consistent with fat density such as lipomas or liposarcomas, infections or metastases. There is no other obvious evidence of a primary tumor on that exam.
Echocardiogram performed demonstrated no vegetations or shunting, normal valve structure and function. No pericardial effusion.
Hematology was then consulted for possible malignancy. Their work-up to this point is currently ongoing. They currently have low suspicion for leukemia and also are working up neuroblastoma and lymphoma and other primary hepatic neoplasms such as hepatoblastoma. Today, he had an eye exam which was basically normal
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DaB: 0911612012 MR: 1275567 Print Date 6/18/2013
I
Consult
Date of Service: 04/12/20130:00:00 Authored By: Merritt II, J Lawrence, MD
except for some periorbital edema but no other eye findings and eye findings did not point to any specific infectious or metabolic disease.
On his metabolic testing, his urinalysis demonstrated trace reducing substances. He has had mild hyperammonemia ranging between 40 and 86. He had a mildly elevated lactic acid on admission of 3.1, but has been normal otherwise since then. He has had hypoalbuminemia with an albumin currently of 2.0. His triglycerides are low at 47. He has a normal GGT and uric acid. AST is currently 121, AL T of 85 and alkaline phosphatase of 1084. Unconjugated bilirubin of 8.6 and conjugated bilirubin of 6.3, currently. His glucoses have been normal with the exception of early this morning he had hypoglycemia with glucose of 30. Around that period of time, he had normal electrolytes with a bicarbonate of 23, a normal anion gap and ammonia of 50. His venous blood gas demonstrated pH of 7.35, pC02 of 41 and base excess of -3.
PAST MEDICAL HISTORY: Jianhua's mother reports her pregnancy with him was generally uncomplicated. She did have maternal serum screen that was reported as abnormal and then she had an amniocentesis which she reports demonstrated a double Y chromosome in 10 of 20 cultures. She did see a genetic counselor prior to this testing but has not seen anybody since that period of time and there has been no follow-up testing of this. He was then born full-term via vaginal delivery. He began bottle feeding immediately then was given some mixed breastfeeding with bottle feeding but then mother transitioned full bottle feeding around a month of age. His parents report that otherwise he had normal activity at birth. He did have some problems then later on over the next few weeks and then after a month of age with vomiting a lot. He was rather spitty and he was transitioned on many different formulas containing cow's milk then soy milk, eventually onto Nutramigen. He had large bowel movements, extremely large and would often blowout of his diaper. These were diarrhea like in consistency and often yellow or very pale, almost white. His parents report his stools have basically always been very oily and greasy like olive oil. Often when they would change a formula they would improve for a period of time but after a week or two, sometimes maybe up to a few weeks with certain formulas, they would then still reoccur. Most recently he did have some slightly green-tinted stools just prior to his hospitalization. He has had one previous hospitalization in January 2013 for RSV (respiratory syncytial virus) infection. Since that time he has had multiple problems with wheezing of his lungs.
His developmental skills included lifting his head and shoulders off the ground and his head to about a 45-degree angle. He could roll onto his side when he was having his diaper changed. He had good head control and would enjoy being put into a stander so he could balanced with his legs.
FAMILY HISTORY: Jianhua has 3 older siblings, an 11-year-old sister, a 9-year-old sister and a 2-year-old brother who are all otherwise healthy. Jianhua's mother reports she had a heart murmur when she was a young child and has otherwise been healthy. Maternal grandfather died of pancreatic cancer at age 64. Maternal grandmother is otherwise healthy other than having some gallbladder problems. Maternal grandmother's sister also had gallbladder problems, as well as their mother, his great-grandmother. Jianhua's father reports otherwise healthy. There are 2 paternal aunts. One paternal aunt has history of some lumbar disk problems, but is otherwise healthy. She has one daughter who is healthy. The second paternal aunt has a history of rheumatism but is otherwise healthy. She has one daughter who is otherwise healthy. A paternal grandfather died at age 62 from suicide. He had a history of depression and some medical problems after taking some natural Chinese medicines. Paternal grandmother reported to be otherwise healthy. Both families are of Chinese ancestry. There is no known consanguinity.
Seattle Children's Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME:
DOB: MR:
XIE, JIANHUA DRACO
09/16/2012
1275567 Print Date 6/18/2013
I
Consult
Date of Service: 04/12/20130:00:00 Authored By: Merritt II, J Lawrence, MD
MEDICATIONS: Please see electronic medical record.
ALLERGIES: No known drug allergies.
REVIEW OF SYSTEMS: Negative other than indicated in Past Medical History and HPI.
PHYSICAL EXAMINATION: Weight of 9.98 kg places him at the 97th percentile. Height of 66 cm places him at the 9th percentile. Head circumference of 43 cm places him at the 24th percentile. Vital signs as noted in electronic record of this date.
Generally, infant who is sleeping on exam. He wakes up during the exam, stretches, moves a[14 extremities spontaneously, and then returns back to sleep. He has profound whole body edema and puffiness in his face, his abdomen and a[[ 4 extremities and including his hands and feet. Heart: Regular rate and rhythm, S1, S2 sounds without murmurs. Lungs: Clear to auscultation bilaterally. No increased work of breathing. Abdomen is distended and full with positive ascites. Liver and spleen are nonpa[pab[e due to this profound ascites. There are a few positive bowel sounds. Facies generally appear nondysmorphic other than his significant edema. Ears are normally set, nondysmorphic. There are no ear pits or creases seen on the lobes. Nares are patent and clear. Mucous membranes appear normal. There is no visible cleft or anterior cleft palate on limited exam. Neck is supple, with normal range of motion. Back appears normal. He has some mild hyperpigmentation at the [ower lumbosacral region. Tanner stage I male genitalia with some edematous, swollen testes. Norma[appearing Tanner stage I male genitalia otherwise. Anus appears perhaps slightly retrograde in position but otherwise is norma[. Skin is otherwise clear, without other areas of hyper- or hypopigmentation than mentioned previously. No rashes are seen. Hands and feet appear generally nondysmorphic. There is no polydacty[y or syndactyly. Normal palmar creases. Cranial nerves appear symmetrical. Sensory exam appears grossly intact. He appears to have normal resting muscle bulk and tone.
[MPRESS[ON AND PLAN: 1. Acute liver disease. 2. Hepatic lesions. 3. Coagu[opathy. 4. Hypog[ycemia. 5. Abnormal karyotype with double Y chromosome on amniocentesis.
I appreciate this opportunity to meet Jianhua and his parents today. At this time, there is no specific evidence of a specific underlying metabolic or genetic disorder or genetic syndrome. He does have profound liver disease, but his hepatic lesions do not appear specific discrete nodules as there is no distortion of the hepatic architecture. As well, he has ongoing evaluations by Infectious Disease and Hematology, which are currently proceeding. His mild urine reducing substances suggested a possible association with galactosemia or hereditary fructose intolerance. He currently has testing for galactosemia currently pending. Also currently pending are urine organic acids, acylcarnitines and amino acids. He has mild hyperammonemia which I believe is likely secondary to his liver disease currently. He also has some initial lactic acidosis when he arrived but has resolved and currently has a pyruvic acid pending as well. Differential diagnosis would include various hepatic or metabolic disease as cause of hepatic adenomas which include Wi [son disease, hemochromatosis,
Seattle Children's Hospita[
PO Box 5371 Seattle, Washington 98105-0371
NAME: X[E, J[ANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Print Date 6/18/2013
I

Date of Service: Authored By:
04/12/2013 0:00:00 Merritt II, J Lawrence, MD
Consult
tyrosinemia, glycogen storage disease type I or Gaucher disease. He likely does not have hemochromatosis, given his normal ferritin level. Wilson disease would also be rather unlikely but it seems reasonable to check a copper and ceruloplasmin level. Tyrosinemia and galactosemia would both also be evaluated on his newborn screen which has been reported as normal. Currently have plasma amino acids and urine organic acids currently pending, which would be appropriate screens for tyrosinemia. Galactosemia screening is also proceeding. He does not have a firm and enlarged liver as would be expected in glycogen storage disease. His lactic acidosis has not been persistent but it certainly seems reasonable to consider this as we move forward. If he does have recurrent hypoglycemia, checking additional labs during this acute decompensation would also seem appropriate. He has no other dysmorphic features or other skin findings that would suggest more extensive genodermatosis, as could be seen if these were lipomas or hamartomas, but some dysmorphisms may be more subtle and given his significant profound edema this may be more difficult to assess and which we could do in the future if possible.
PLAN: 1. Today, I would recommend checking copper and ceruloplasmin, although this is only a very remote
chance of being Wilson disease at this age. 2. Follow up on urine organic acids, acylcarnitine, amino acids and galactosemia testing which currently
pending. 3. If he has recurrent hypoglycemia, would recommend checking a lactate, beta-hydroxybutyrate,
ammonia and urinalysis during the acute event orland a uric acid during the acute event, as well as repeating urine organic acids at that time.
4. If the above testing is normal, may consider Gaucher enzyme testing or screening for congenital disorders of glycosylation, given his significant coagulopathy, after these other labs have been normal.
We will continue to follow him while he is here in the hospital. The above plan was discussed with the primary care PICU Team.
Electronically Authenticated by J Lawrence Merritt, II, MD 04/26/2013 03:28 P
J Lawrence Merritt, II, MD , Attending PhYSician, Genetics
JLM/sh Doc #2935658 d: 0411212013 06:45 P t: 0411212013 07:52 P (1556801-) cc: Evelyn K Hsu, MD
cc Pediatric Assoc Redmo
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME: DOB:
MR:
XIE, JIANHUA DRACO
0911612012
1275567
PrintDate 6/18/2013
I
I Consult
Date of Service: 04/12/20130:00:00 Authored By: Merritt II, J Lawrence, MD
Lincoln S Smith, MD JUlie E Wen, MD
LlYING CHEN, 21743 105TH PL NE REDMOND WA 98053
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Print Date 6/18/2013
I
, Date of Service: Authored By:
Surgery Consultation
04/22/20130:00:00 Reyes, Jorge D, MD
Consult
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
SURGERY CONSULTATION
XIE, JIANHUA DRACO DOB: 0911612012 M -MR #: 01-27-55-67
DATE OF ADMISSION: 0410912013 DATE OF CONSULTATION: 0412212013
REASON FOR CONSULTATION: Acute end-stage liver disease.
PHYSICIAN REQUESTING CONSULTATION: Evelyn Hsu, MD
I was asked to see this patient by Dr. Evelyn Hsu, MD, as part of an urgent liver transplant evaluation for this patient. This baby is a 7 -month-old boy with no previous history of liver disease, but who presented about a couple weeks ago with progressive jaundice. He had some nonspecific symptoms, but was essentially referred here with rapidly increasing bilirubin and INR. He does not have any previous history of liver disease, nor does he have a history of pathology in the heart, lungs, or kidneys. He was not on any standard medications prior to becoming ill.
FAMILY HISTORY: His parents are both engineers and full caregivers.
PHYSICAL EXAMINATION: He presents awake and playful, and in no apparent distress. His mucosa is pink and the sclerae are anicteric. The neck is supple with no masses and the extremities are unremarkable. Chest shows clear breath sounds bilaterally and the heart shows a regular rhythm. The abdomen is flat with an apparent umbilical hernia; there is palpable splenomegaly at 2 fingerbreadths below the left costal margin. I could not feel his liver. Perineum laboratory functions are significant for a bilirubin of greater than 10, an INR of 2.5.
IMPRESSION: End-stage liver disease with hepatosplenomegaly. I reviewed a laparoscopic biopsy report by Dr. Healey, who visualized a small cirrhotic-appearing liver and splenomegaly. I discussed review of his liver biopsy with Dr. Hsu, who had reviewed it with Pathology; the liver shows cirrhosis and cholestasis.
IMPRESSION: End-stage liver disease of unknown origin, possible metabolic disorder. Other diagnostic possibilities are still in the workup by Hepatology, however, given this patient's synthetic function, (a prolonged INR and a high ammonia level), this patient's liver, and biopsy findings, this patient has end-stage liver disease, which will not recover.
PLAN: I believe given the patient's clinical circumstances and no immediate evidence of any contraindication, and good family support, he should be listed for liver transplantation urgently.
Seattle Children's Hospital
PO Box 5371
Seattle, Washington 98105-0371
NAME:
DOB:
MR:
XIE, JIANHUA DRACO
0911612012
1275567 Print Date 6/18/2013
I
I Consult
Date of Service: 04/22/2013 0:00:00 Authored By: Reyes, Jorge D, MD
I spent approximately 1 hour with this family explaining details of the liver transplant operation, anatomy, and the process of removing the liver in and transplanting a new one. We went over all the technical variance of liver graft, which included whole, reduced, splint, liver, and living donor. I expressed to them that at this point, our living donor program is temporarily on hold due to staffing, but he would be listed for cadaveric only. We reviewed all of the potential risks and benefits of liver transplant versus not receiving a liver transplant, as well as complications of liver transplant, which included bleeding, vascular complications, including hepatic artery thrombosis, portal vein thrombosis, biliary strictures and leaks, and also primary nonfunction of the liver. We spent some time answering questions regarding potential failure of the liver transplant, which would require retransplantation, and also situations which may result in death. I answered all their questions and stated that once we discussed him in committee today, we would be listing him. We did discuss also the specifics of brain dead donors and also deceased after cardiac death donors to which they agreed to meet with.
I spent approximately 1 hour with this family.
Electronically Authenticated by Jorge D Reyes, MD 04/24/2013 08:40 A
Jorge D Reyes, MD , Attending Physician,Transplant
JDR/pam Doc#2946527 d: 04/22/201311:37 At: 04/22/201302:24 P (1563592-) cc: cc Pediatric Assoc Redmo
Julie E Wen, MD
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME:
DOB: MR:
XIE, JIANHUA DRACO
09/16/2012
1275567 Print Date 6/18/2013
I

Date of Service: Authored By:
04/12/20130:00:00 Weiss, Avery H, MD
Ophthalmology Consultation
Consult
Document may Not be Signed/Finalized. See End of report for Electronic Authentication of Signature.
OPHTHALMOLOGY CONSULTATION
XIE, JIANHUA DRACO DOB: 09/16/2012 M -MR #: 01-27-55-67
DATE OF ADMISSION 04/09/2013 DATE OF CONSULTATION: 04/12/2013
Jianhua is a 6-month-old previously healthy child with the acute onset actually of lethargy, weight gain, hepatomegaly with splenomegaly suggestive of chronic liver disease, and coagulopathy with a serum albumin of 2 who is seen in consultation in the Pediatric Ophthalmology Service on 4/12/2013 as part of his overall evaluation, specifically to look for ocular evidence of an underlying metabolic disease. This child's history dates back a week ago when he developed lethargy, marked weight gain, increasing from 50th to the 90th percentile loose stools without icterus. He was noted to have some periorbital edema and wheezing. His T-max was 40 degrees, serum albumin 2.3, INR 5.6, bilirubin 4.0 conjugated, 10.3 unconjugated. Transaminases were baSically normal or minimally elevated, AST 107, AL T 91, alpha fetoprotein 7080. Further evaluation for infectious causes of acute hepatic failure included hepatitis A that was positive for the IgG but the IgM was negative. EBV (Epstein-Barr virus) and CMV (cytomegalovirus) were IgG positive but IgM negative. Abdominal ultrasound revealed an edematous liver with multiple echogenic foci, particularly in the right lobe of the liver. On the basis of these findings, he was thought to have either metabolic or infiltrative disease. There was mild pelviectasis of the right kidney but the creatinine is 0.3. He did then had a CT of chest, abdomen, and pelvis; abdomen shows multiple subcentimeter hypodensities predominantly in the right lobe suggestive of infiltration or infectious etiologies. The chest CT showed air space opacities in the right upper lobe but no adenopathy and abdomen showed evidence of portal hypertension with recanalization the umbilical vein and splenomegaly. All blood cultures have been negative to date. Ferritin and triglycerides were both normal, which would help to exclude hemophagocytic Iymphohistiocytosis. This child was basically normal, born at term. His growth and development have been normal. He does have a history of milk protein sensitivity and had an episode of RSV (respiratory syncytial virus) in January for which he was not hospitalized.
PHYSICAL EXAMINATION: He is a lethargic child with a very protuberant abdomen and generalized edema. When awake he seems to be very alert and oriented and his visual behaviors are very age-appropriate. Gaze holding was stable. Acquires eccentric targets with saccades. Pupils round and reactive to light. Anterior segment normal to gross inspection. Dilated fundus exam: Disks, vessels, macula, retinal periphery normal. No evidence of pigmentary retinopathy. No maculopathy. No vitreitis other than for fungal.
IMPRESSION: Acute liver failure with coagulopathy, hyperbilirubinemia, and generalized edema. This child's exam is basically normal except for his periorbital edema. This is just another manifestation of his overall third spacing due to his hypoproteinemic state. The eye findings do not pOint in the direction of any specific infectious or metabolic disease. His visual function is normal and his eye exam was completely normal. No
Seattle Children'S Hospital PO Box 5371
Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012 MR: 1275567 Print Date 6/18/2013
I
, Date of Service: Authored By:
04/12/20130:00:00 Weiss, Avery H, MD
Consult
abnormalities of the anterior segment, the lens or posterior segment that point to any specific metabolic etiology.
Electronically Authenticated by Avery H Weiss, MD 04/24/2013 08:00 A
Avery H Weiss, MD , Attending Physician, Ophthalmology
AHW/jwm Doc#2935106 d: 04/12/2013 02:02 P t: 04/12/2013 02:22 P (1556397-) cc: cc Pediatric Assoc Redmo
Julie E Wen, MD
Seattle Children's Hospital
PO Box 5371 Seattle, Washington 98105-0371
NAME: XIE, JIANHUA DRACO
DOB: 09/16/2012
MR: 1275567 Print Date 6/18/2013
I








![[pre arrival] checklist for eps](https://static.fdocuments.us/doc/165x107/568ca72c1a28ab186d944790/pre-arrival-checklist-for-eps.jpg)









