
emd166_slide_acute_coronary.pdf
40
ACUTE CORONARY SYNDROME Nizam Akbar Dept of Cardiology & Vascular medicine Universitas Sumatera Utara Adam Malik Hospital - Medan
-
Upload
uliuliaulia -
Category
Documents
-
view
217 -
download
2
Transcript of emd166_slide_acute_coronary.pdf
ACUTE CORONARY
SYNDROME
Nizam Akbar
Dept of Cardiology & Vascular medicine
Universitas Sumatera Utara
Adam Malik Hospital - Medan


Major clinical manifestations
of atherothrombosis
Transient ischemic attack
Angina:• Stable• Unstable
Ischemicstroke
Myocardial infarction
Adapted from: Drouet L. Cerebrovasc Dis 2002; 13(suppl 1): 1–6.
Peripheral arterialdisease:• Intermittent claudication• Rest Pain• Gangrene• Necrosis
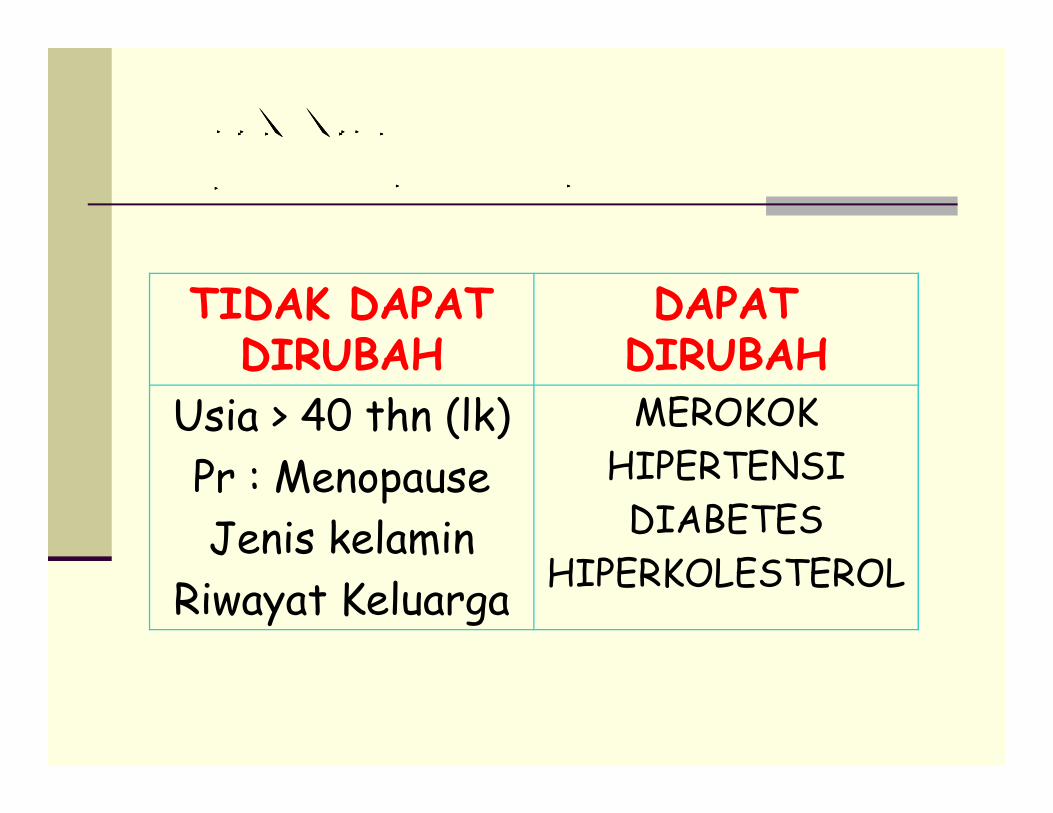
FAKTOR RESIKO FAKTOR RESIKO FAKTOR RESIKO FAKTOR RESIKO
P������� J������ K������P������� J������ K������P������� J������ K������P������� J������ K������
TIDAK DAPAT
DIRUBAH
DAPAT
DIRUBAH
Usia > 40 thn (lk) MEROKOKUsia > 40 thn (lk)
Pr : Menopause
Jenis kelamin
Riwayat Keluarga
MEROKOK
HIPERTENSI
DIABETES
HIPERKOLESTEROL

FAKTOR RESIKO PJK DI INDONESIA
INA – MONICA 1993
Merokok Hipertensi HiperkolesterolD M
What Is Atherothrombosis?
� Atherosclerosis
Thrombosis� Thrombosis
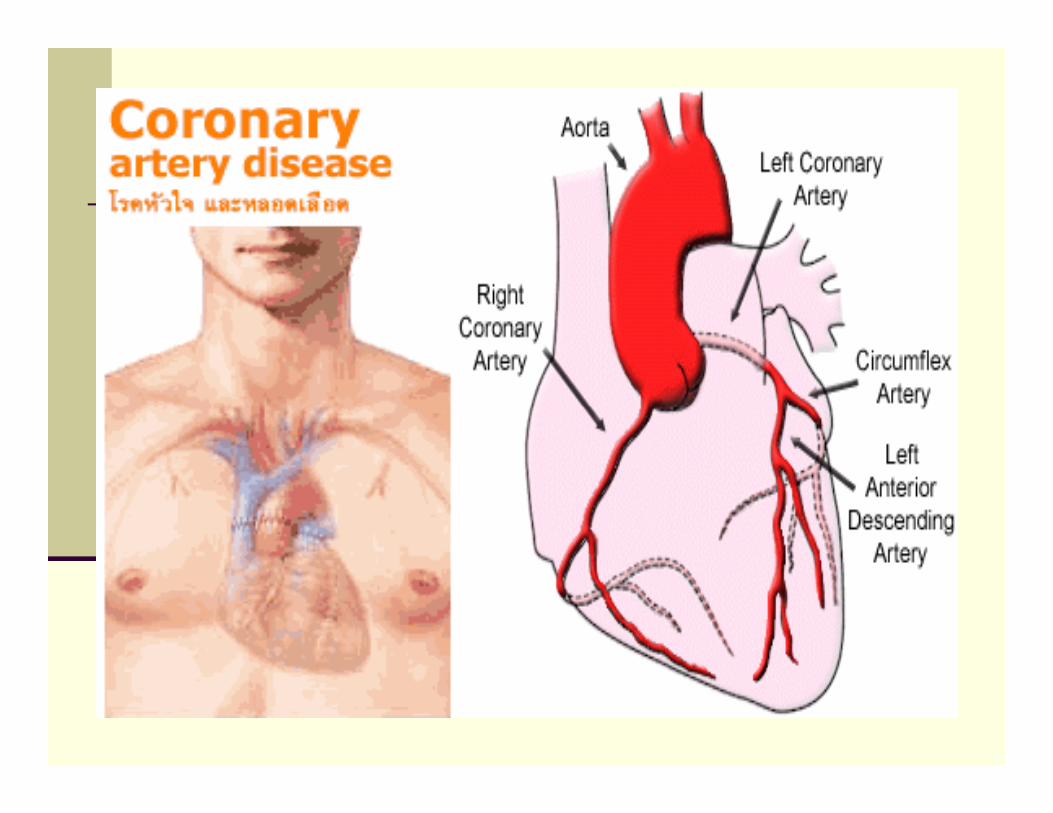
PENYAKIT JANTUNG KORONER :PENYAKIT JANTUNG KORONER :
PENYEMPITAN PEMBULUH ARTERI
KORONER JANTUNG OLEH PLAK
(TUMPUKAN ) ATEROSKLEROSIS
PLAK ATEROSKLEROSISPLAK ATEROSKLEROSIS ::
KOLESTEROL (UTAMA),KALSIUM, JARINGAN IKAT,
OTOT POLOS, KOMPONEN DARAH, FIBRIN, KARBOHIDRAT

Kapan Atherosklerosis Terjadi?
AtherosklerosisBerawal dari usia balita sampai dengan lansia
Tedjasukmana P
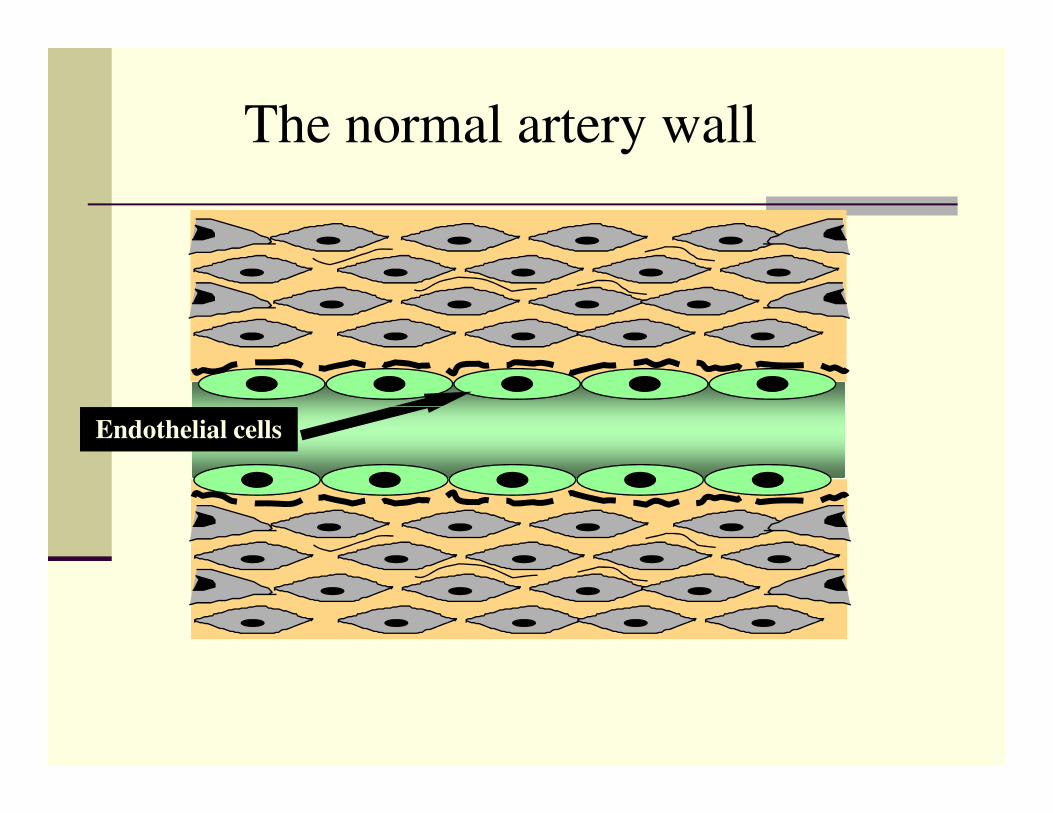
The normal artery wall
Endothelial cells

Early atherosclerosis (I) Early atherosclerosis (I) ––
Endothelial dysfunctionEndothelial dysfunction
Lipid accumulates in
the intimal space and is
associated with
abnormal endothelial
cell function
Lipid
cell function
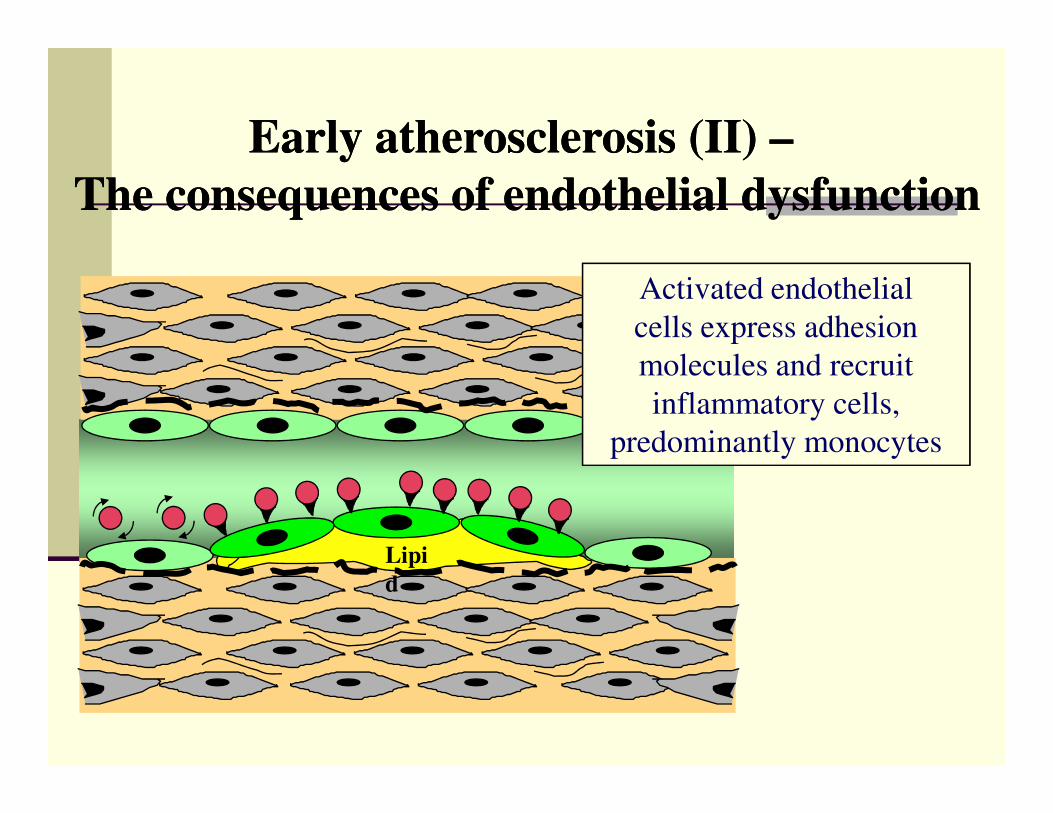
Early atherosclerosis (II) Early atherosclerosis (II) ––
The consequences of endothelial dysfunctionThe consequences of endothelial dysfunction
Activated endothelial
cells express adhesion
molecules and recruit
inflammatory cells,
Lipi
d
inflammatory cells,
predominantly monocytes
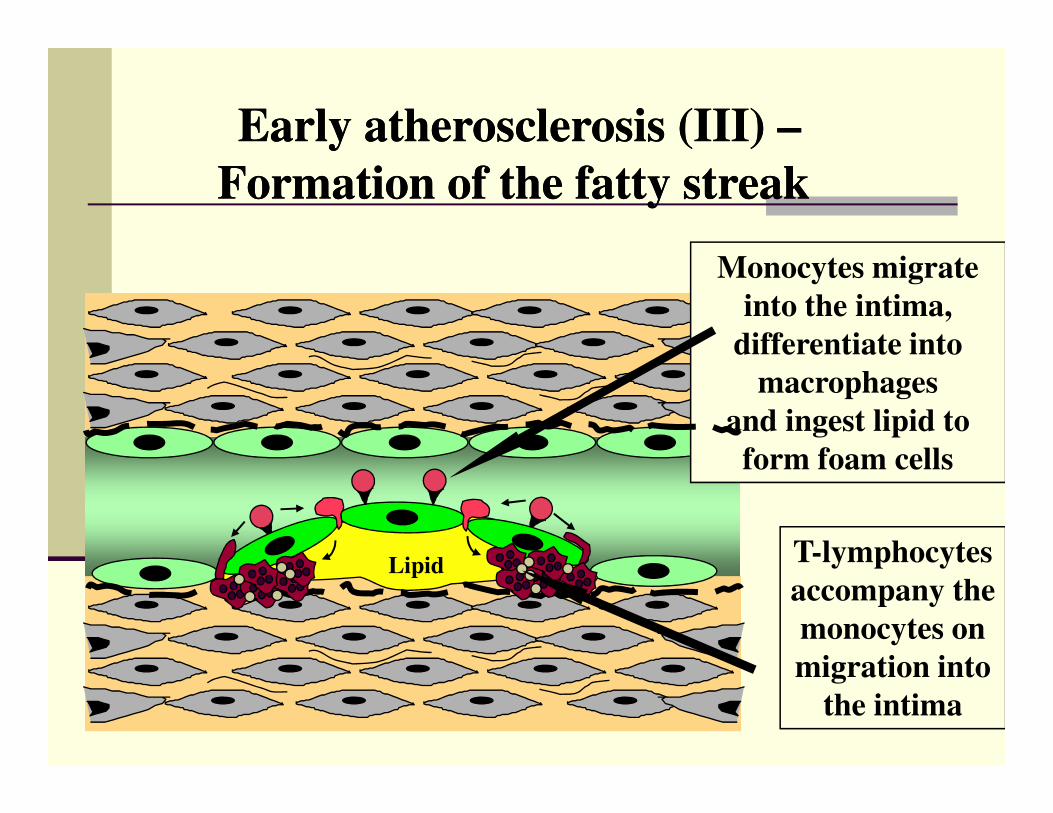
Monocytes migrate
into the intima,
differentiate into
macrophages
and ingest lipid to
Early atherosclerosis (III) Early atherosclerosis (III) ––
Formation of the fatty streakFormation of the fatty streak
Lipid
and ingest lipid to
form foam cells
T-lymphocytes
accompany the
monocytes on
migration into
the intima
Proses Terjadinya Atherosklerosis

�Nyeri dada
( Angina, Chest Pain )
�Serangan Jantung
Manifestasi KlinisPenyakit Jantung Koroner
�Serangan Jantung
( Heart Attack, Myocard Infark )
�Kematian mendadak
( Sudden Death, Cardiac Arrest )
Chronic PJK

Dimana Rasa Nyeri Dirasakan??

Adhesion
The Role of Platelets in Atherothrombosis
Aggregation1 3
Activation2

Lefkovits et al.NEJM 332:1553,1995.
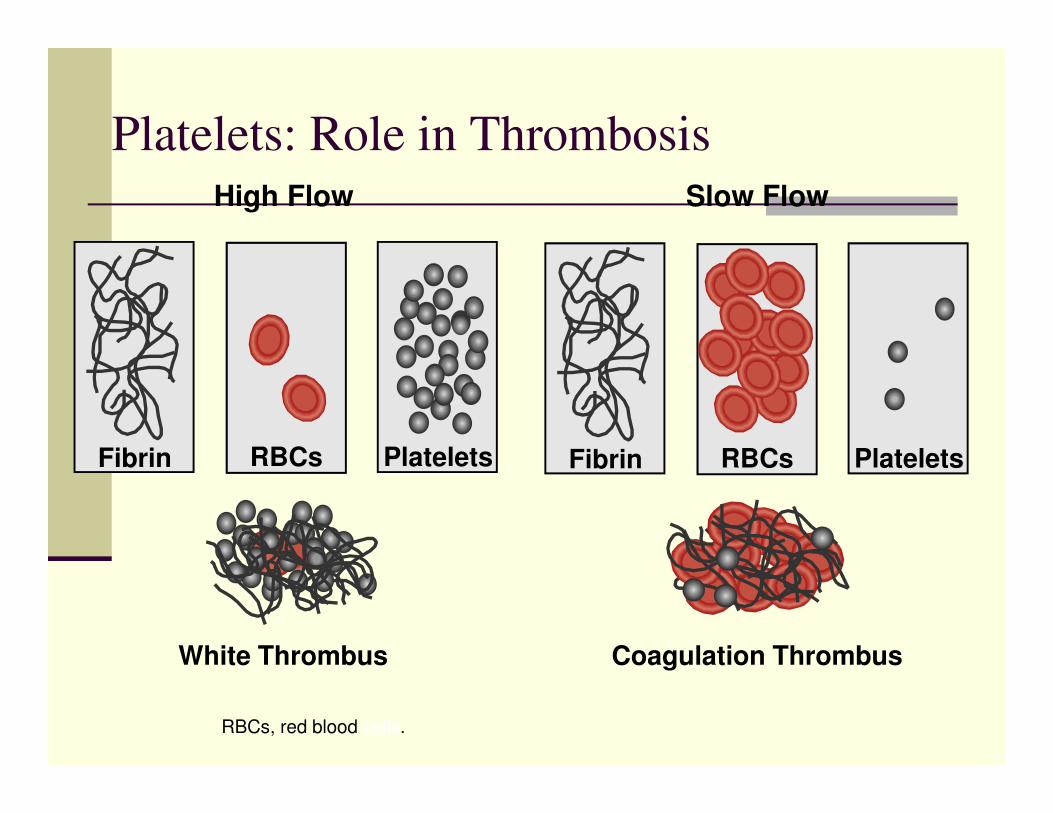
High Flow Slow Flow
Platelets: Role in Thrombosis
Fibrin PlateletsRBCs
White Thrombus
Fibrin PlateletsRBCs
Coagulation Thrombus
RBCs, red blood cells.

CLOPIDOGREL
ADP
ADP
C
ASA COX
GPllb/llla(Fibrinogen receptor)
Collagen thrombin
TXA2
Activation
TXA2
COX (cyclo-oxygenase)ADP (adenosine diphosphate)TXA2 (thromboxane A2)
1. Jarvis B, Simpson K. Drugs 2000; 60: 347–77.

Thrombin
Activated
Platelet
AspirinGp Gp IIb/IIIa
fibrinogenfibrinogen
receptorreceptor
To neighboringTo neighboring
plateletplatelet
Clopidogrel
Ticlopidine
IV Gp IIb/IIIaInhibitors Thrombin
SerotoninEpinephrineCollagen
Activation
COXCOX
Degranulationαααααααα δδδδδδδδ
Platelet agonists
ADPATPserotonincalciummagnesium
Adhesive proteinsthrombospondinfibrinogenp-selectinvWF
Coagulation factors
factor Vfactor XIPAI-1
Inflammatory factors
platelet factor 4
CD 154 (CD 40 ligand)
PDGF
Inhibitors
TXA, thromboxane; PDGF, platelet-derived growth factor.

Atherothrombosis:
The Pathologic Process
Medical Training Asia Middle East
3L
Occlusion
Acute Event
Embolism
Chronic Ischemia
AtheroscleroticPlaque
PlaqueFissure/Cracking
/ Rupture
Thrombus Incorporated
into Atheroma
Thrombus Formation
Stabilized Plaque

Atherothrombosis:
A Generalized Condition
Medical Training Asia Middle East
3R Ruptured Carotid Artery Plaque with Thrombus

Surface of a Thrombus
M 3Nilsson, 1984
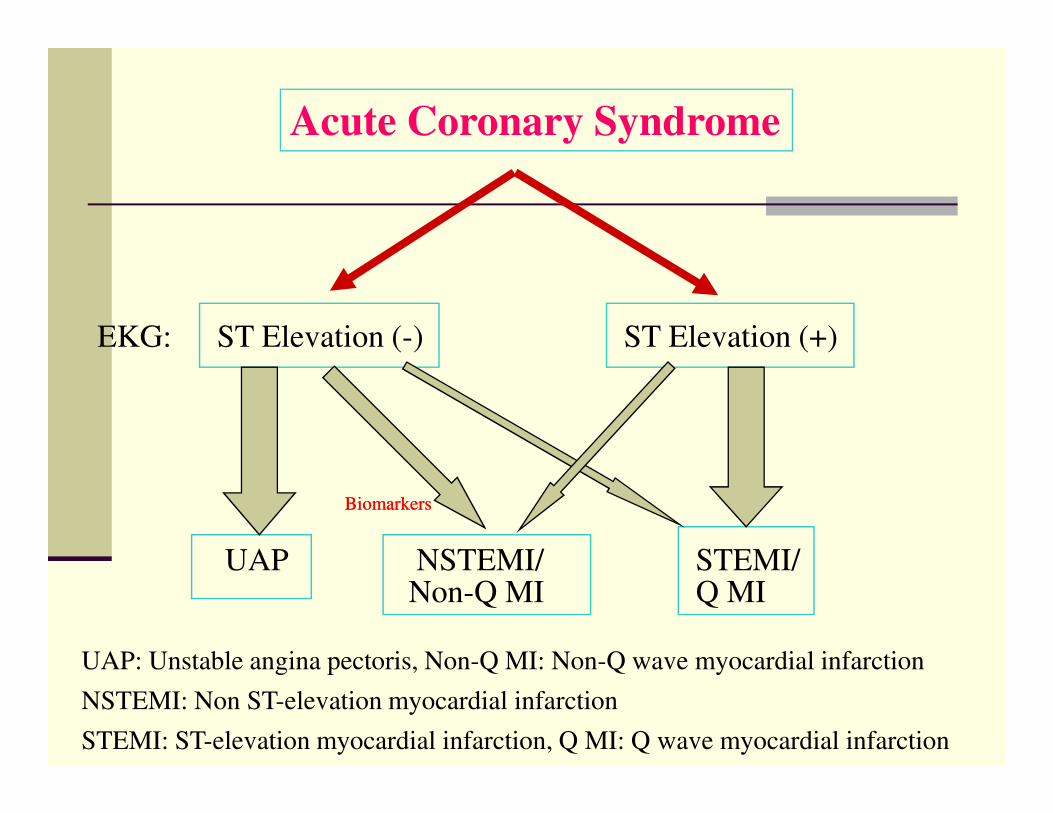
ST Elevation (-) ST Elevation (+)EKG:
Acute Coronary Syndrome
UAP NSTEMI/ STEMI/Non-Q MI Q MI
UAP: Unstable angina pectoris, Non-Q MI: Non-Q wave myocardial infarction
NSTEMI: Non ST-elevation myocardial infarction
STEMI: ST-elevation myocardial infarction, Q MI: Q wave myocardial infarction
BiomarkersBiomarkers
ANGINA PECTORIS
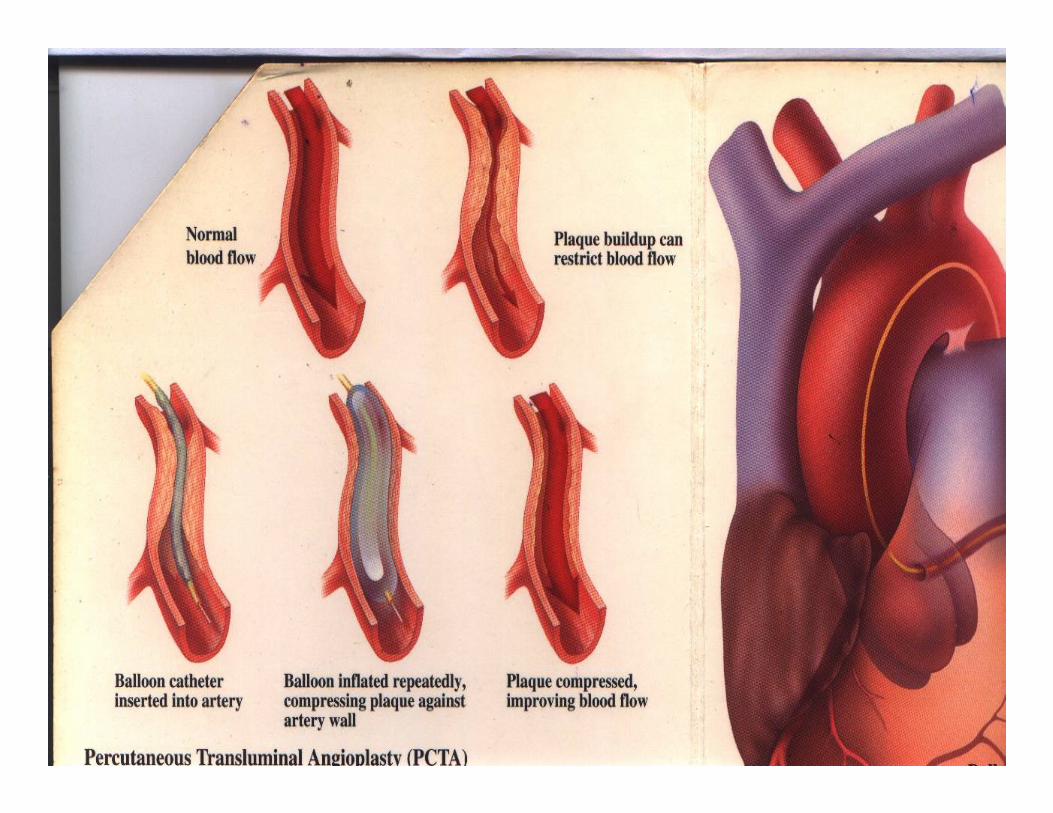
Proses Tersumbatnya Pemb. Darah
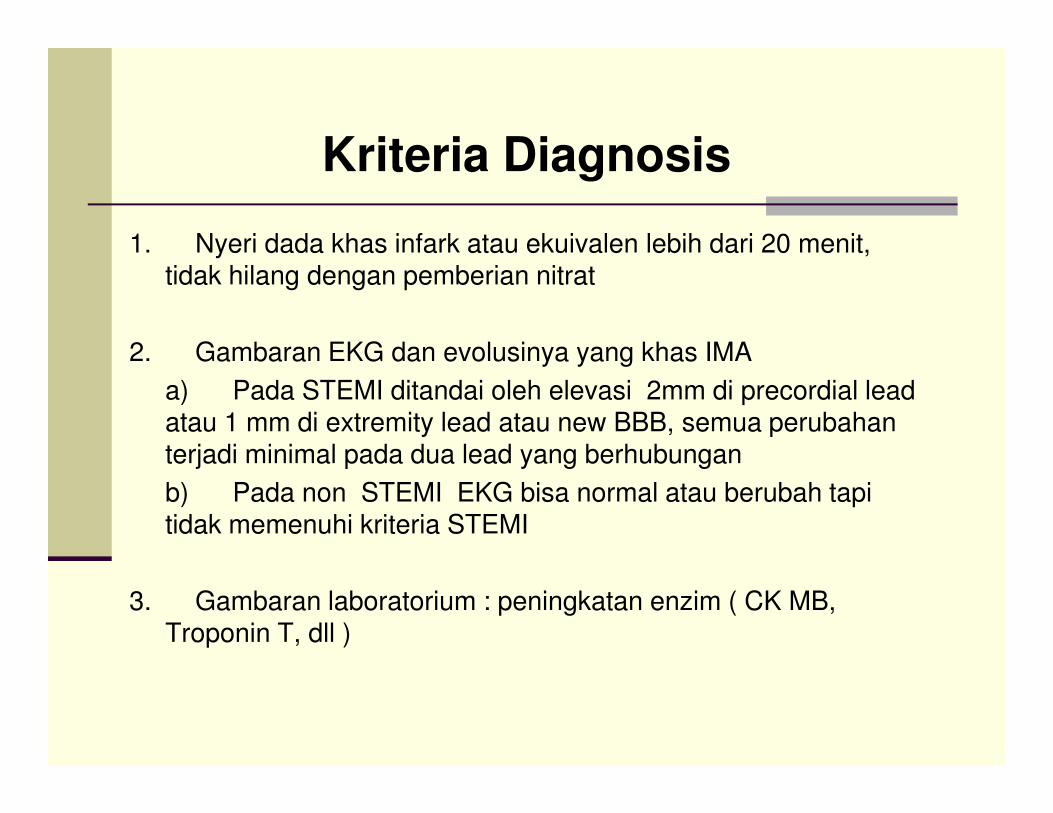
Kriteria Diagnosis
1. Nyeri dada khas infark atau ekuivalen lebih dari 20 menit, tidak hilang dengan pemberian nitrat
2. Gambaran EKG dan evolusinya yang khas IMA
a) Pada STEMI ditandai oleh elevasi 2mm di precordial lead atau 1 mm di extremity lead atau new BBB, semua perubahan terjadi minimal pada dua lead yang berhubungan
b) Pada non STEMI EKG bisa normal atau berubah tapi tidak memenuhi kriteria STEMI
3. Gambaran laboratorium : peningkatan enzim ( CK MB, Troponin T, dll )
Pertolongan Pertama :
MONA
�Morphine (M)
�Oksigen (O)�Oksigen (O)
�Nitrat (N)
�Aspirin (A)
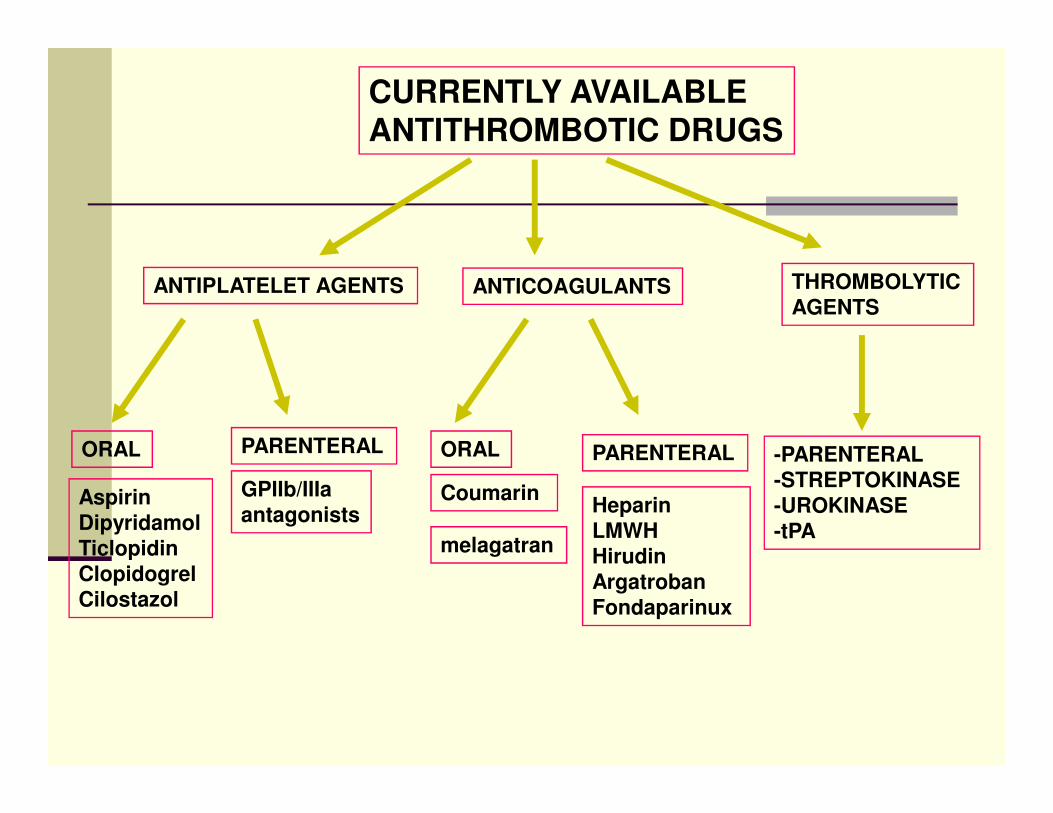
CURRENTLY AVAILABLEANTITHROMBOTIC DRUGS
ANTIPLATELET AGENTS ANTICOAGULANTS THROMBOLYTIC
AGENTS
ORAL PARENTERAL ORAL PARENTERAL
Aspirin
Dipyridamol
Ticlopidin
Clopidogrel
Cilostazol
GPIIb/IIIa
antagonistsCoumarin
Heparin
LMWH
Hirudin
Argatroban
Fondaparinux
melagatran
-PARENTERAL
-STREPTOKINASE
-UROKINASE
-tPA

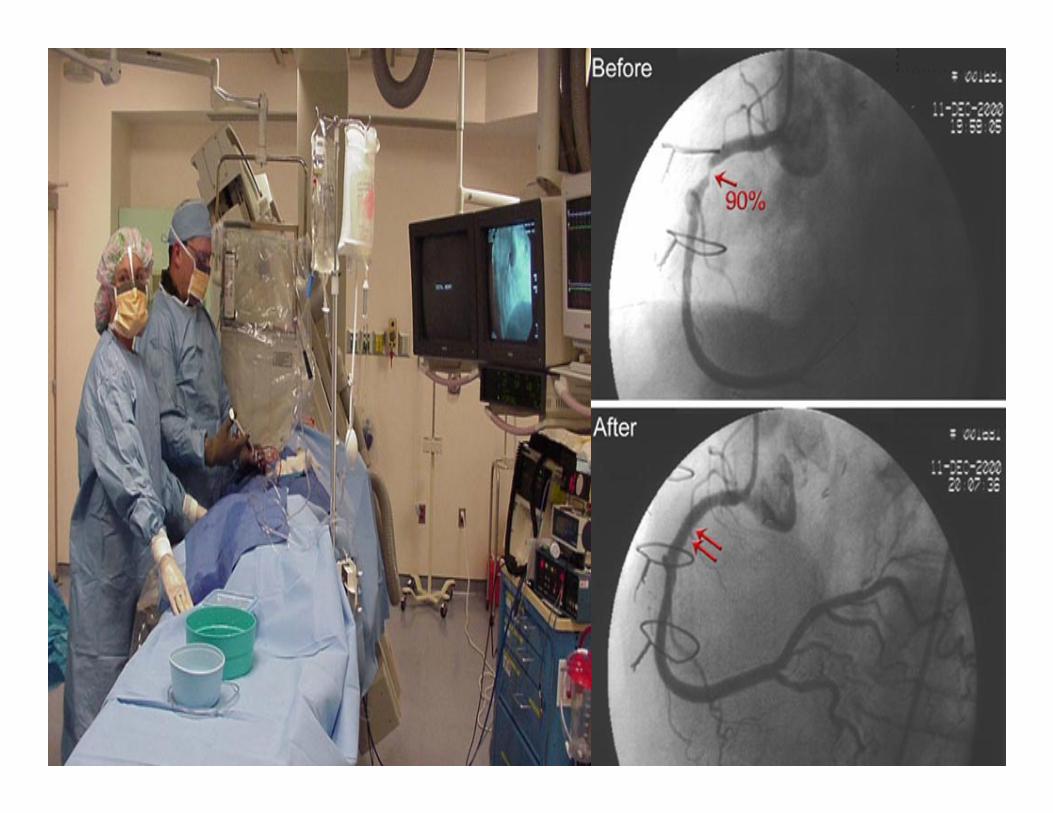
Therapy
� STEMI : Revascularisasi secepatnya
< 3 jam : PCI (Percutaneus Coronary Intervention>
<12 Jam : Thrombolytyc Therapy
� UAP / Non-STEMI :Anticoagulant dgn Heparinisasi
� Lain-lain :
Antiplatelet Agents : Aspirin and Clopidogrel
Nitrat, Betabloker, Calcium Antagonist, ACE Inhibitor
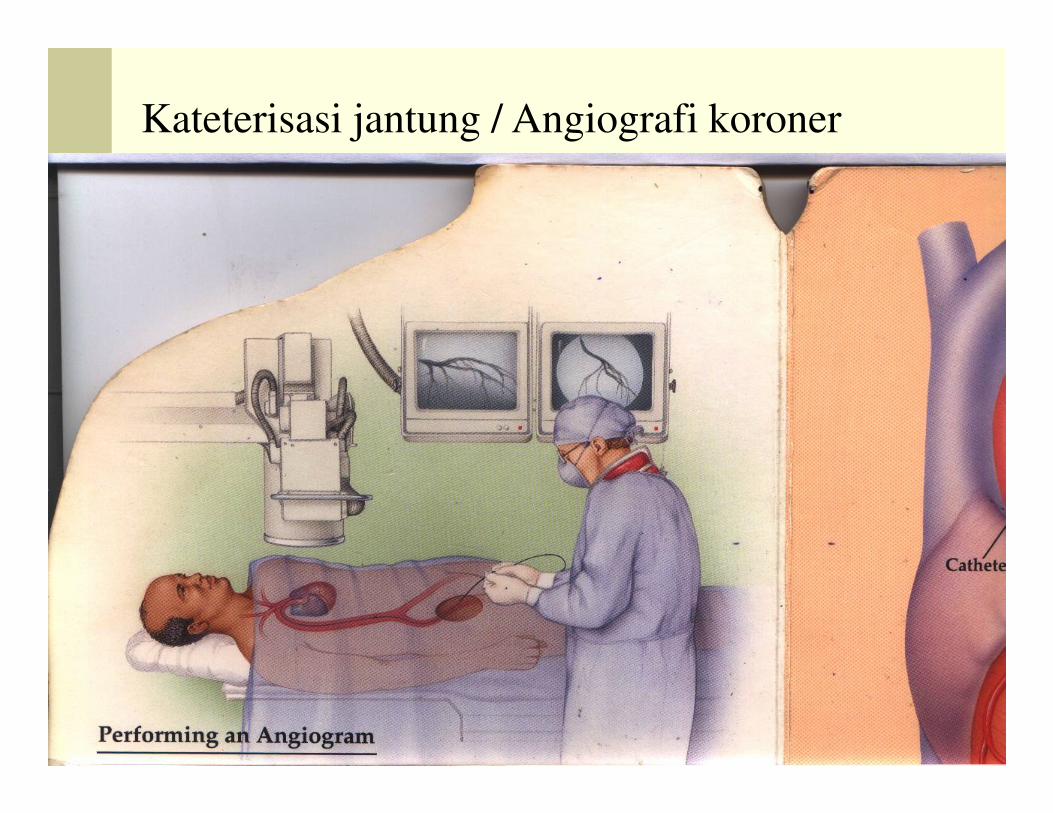
Kateterisasi jantung / Angiografi koroner

Angiografi Koroner

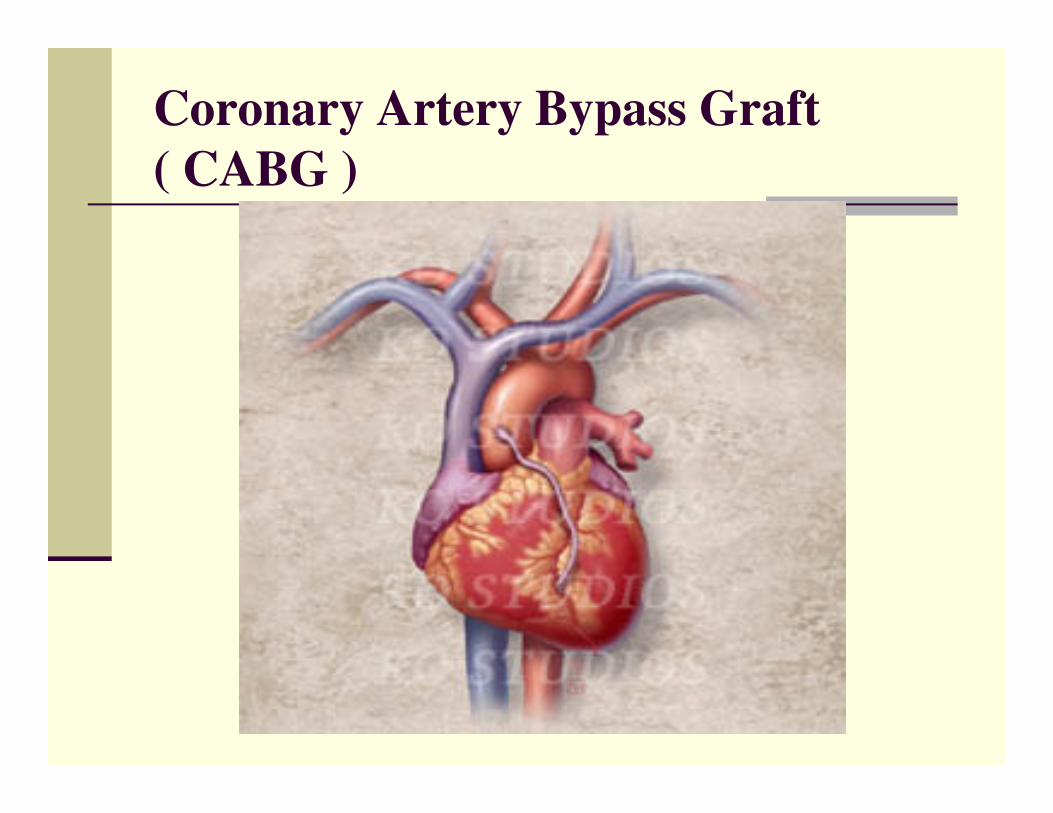
Coronary Artery Bypass Graft
( CABG )
Coronary Artery Bypass Graft


















