Embarking on A New Path Bill P. Martone President WPM ... · Introduction of Parent Partners . From...
64
The Community Technical Assistance Center of New York Embarking on A New Path Bill P. Martone President WPM Consulting
Transcript of Embarking on A New Path Bill P. Martone President WPM ... · Introduction of Parent Partners . From...

The Community Technical Assistance Center of New York
Embarking on A New Path Bill P. Martone
President WPM Consulting
The Community Technical Assistance Center of New York
To obtain Continuing Education Unit credits, please 1. Please log into the webinar system via your computer, and view the
entire presentation 2. Go to http://socialwork.nyu.edu/alumni/continuing-
education/OnlinePortal.html 3. Create a profile 4. Select today’s webinar 5. Pay the $15 processing fee 6. Take the Knowledge Test* *The Knowledge Test will be made available to you within the week. You will receive an email with this information within 24 hours of this webinar.

The Community Technical Assistance Center of New York
January 15th 11am-12pm Culture- Driven Leadership
There is growing recognition of the need for organizations to infuse a performance management culture not only in residential treatment,
but in all levels of the organization. A critical component in all employees understanding and embracing a performance based
culture is defining, teaching, assessing, and monitoring the essential competencies of those who deliver behavioral health services. This webinar will outline critical skill sets and identify strategies aimed at
strengthening and supporting the workforce.

The Community Technical Assistance Center of New York
What is your role in your agency? A. Director/Administrator B. Supervisor C. Clinician D. Administrative Support E. Other

Agenda For Session 1
William P. Martone 12/18/15
1. Goals for The Series 2. Bill’s Background and Experiences 3. Emerging Trends - Top 40 Trends in Our Field 4. Reinventing the Organization 5. Assessing Where Your Organization is At 6. Q&A

Goals For The Series
William P. Martone 12/18/15
• Support you in identifying the strengths of your organization specific to achieving sustained positive outcomes for youth and families.
• Support you in increasing your understanding about your organizational
capacity for developing or expanding community based services • Hopefully increase your enthusiasm and understanding regarding specific
strategies you can go back and utilize to improve services in your own programs

Bill’s Background and Experiences
Agencies Employed At BBI Work Peer Faculty
Agencies
Freddy

So Why Consider Offering More Services in Communities

Lets Look at Some Emerging Trends

Top 40 Trends* to Expect in the next 3-5 years
William P. Martone 12/18/15
*From Tom Woll’s 40 Trends Report - to be released January 2016 – For the Alliance Residential Transformation Project and The Strategic Change Initiative
1. Expecting less money from local, state and federal governments.
2. A strong emphasis by service purchasers on reducing their costs.
3. Many are saying they only want to buy evidence-based practices.
4. Most are saying they want to buy results instead of buying services.
5. Emphasis on durable results that can be sustained for 6-12 months.
6. Movement from child-centered to family-focused service delivery.
7. Faster moves toward permanency for children not returning home.
8. Engagement is seen as the means and stability is seen as the end.
9. Re-emergence of a focus on Maslow’s hierarchy of needs for families.
10. Promoting “safe, secure, calm and well” as the results of our efforts.
Top 40 Trends to Expect in the next 3-5 years
William P. Martone 12/18/15
11. Preparing for success with a stable family is the new test to teach for.
12. Emphasis on making community connections to existing resources.
13. Emphasis on helping the working poor to get better paying jobs.
14. Emphasis on helping to build natural support networks for families.
15. Care coordination and aftercare are seen as essential for durability.
16. Movement away from “one size fits all” and toward individualization.
17. Push to re-design all existing services to ensure more durable results.
18. Emphasis on learning how to teach normal developmental processes.
19. Emphasis on using wraparound designs to help meet family needs.
20. Emphasis on identifying and addressing the impact of trauma.

Top 40 Trends to Expect in the next 3-5 years
William P. Martone 12/18/15
21. Emphasis on developing guidance for staff behaviors in their work.
22. Emphasis on shorter durations of service whenever possible.
23. Emphasis on continuing to reduce the use of out-of-home care.
24. Emphasis on using out-of-home care primarily for crisis stabilization.
25. Emphasis on developing an integrated, collaborative system of care.
26. Emphasis on change leadership as the method to adapt organizations.
27. Using strategic data analysis to inform responsive decision-making.
28. Significant efforts to begin to integrate physical and behavioral health.
29. Call for collaborative relationships with primary healthcare providers.
30. Efforts to strengthen and enforce performance-based contracts.

Top 40 Trends to Expect in the next 3-5 years
William P. Martone 12/18/15
31. Continued movement toward more risk-sharing and managed care.
32. Emphasis on developing improved training and support for line staff.
33. Emphasis on finding ways to adjust organizational identity and culture.
34. Emphasis on community-based over campus-based service delivery.
35. Need for new business plans and more sophisticated financial systems.
36. Changing public sector role, moving away from direct service delivery.
37. Public sector to focus more on defining community priorities.
38. Public sector to focus more on developing and enforcing contracts.
39. Public sector to look for solution-finding partners for systems of care.
40. Flexible, responsive, capable and collaborative are key trend words.

Reinventing the Organization Case Example From Hathaway-Sycamores
Mission
Of Hathaway-Sycamores Child and Family Services
Cultivating hope and resilience to enrich the well-being of children, adults, families and communities

In 1994 Niche 60 Bed Residential Program – DCFS/PROBATION/EDUCATION Placements
Some Beginning Family Work – Picnics/Campus Visits/Home Visits
Concerns about what Managed Care Might Mean Began Building an Array of Community Based Serv ices In 2000 Became a Wraparound Agency Hired Parent Partner (Peer to Peer Support) Began Utilizing Wraparound Philosophy Through Out All Our Programs/Serv ices Built Parent Partner Program Introduced Parent Partner Into Residential Milieu – Key Step in Transforming Values & Beliefs
In 2004 Introduced ResWrap In 2005 Merger 187 Residential Beds Added a former Parent Consumer to Board of Directors In 2010 34 Residential Beds Began Residentially Based Serv ices - (Demonstration Project)
Key Highlights
Environmental changes
Lack of fiscal resources Lawsuits Rate Reform Growth in community based services
National Accreditation – JCAHO Changed our organization Data driven decision making Performance Improvement focus 2010 began Performance Excellence Project – quest for state/national quality award
Agency-wide implementation of Wraparound Philosophy Wrap started in 2000 Strength based Families as partners Development of Child and Family Team No difference from kids in residential – getting better outcomes in community
Building Bridges Initiative Values and Principles continued to drive change Adapted by state Association Adapted into RBS in Los Angeles
Changing the Metaphor of Placement The Transformation of a Residential Program
Key Issues in Change

Introduction of Parent Partners
From 1 to 40
Res/Wrap – Homeward Bound Pilot Combining a RTF with Wraparound Philosophy – importance of Child and Family Team Implemented Res/Wrap in LA County in 2004 Four agency pilot Each model varied slightly in approach, but contained core elements Funded through agency wraparound reserves Achieved LOS of 9 months
Family Search and Engagement
Detective to identified staff
Directive Supervision Focus on precision of intervention
Created a Core Practice Model (will review later)
Eventually a County and Statewide Model Created Today County is discussing Underlying Needs
RBS Demonstration Project (see appendix for additional details) 4 Counties in CA - 3 Providers in Los Angeles 17 Bed Pilot started in 2010
Changing the Metaphor of Placement (continued) The Transformation of a Residential Program
Key Issues in Change

RBS Values (See Appendix for Details on RBS)
• Children Belong at Home in Their Community
• Families are Experts on Themselves and Their Children
• Family Culture is Acknowledged and Honored
• Planning and Treatment are Individualized and Strengths-based
• Family Involvement and Connections are Essential
• Strong Communities Make Strong Families
• Whatever It Takes
19

Fiscal Break Down In Dollars 1994 - The Sycamores – budget of $5,848,000
Residential Mental healthNPS Development
Development
NPS Residential

Fiscal Break Down in Percentages 1994 - The Sycamores – budget of $5,848,000
Residential Mental healthNPS Development
Development
NPS Residential
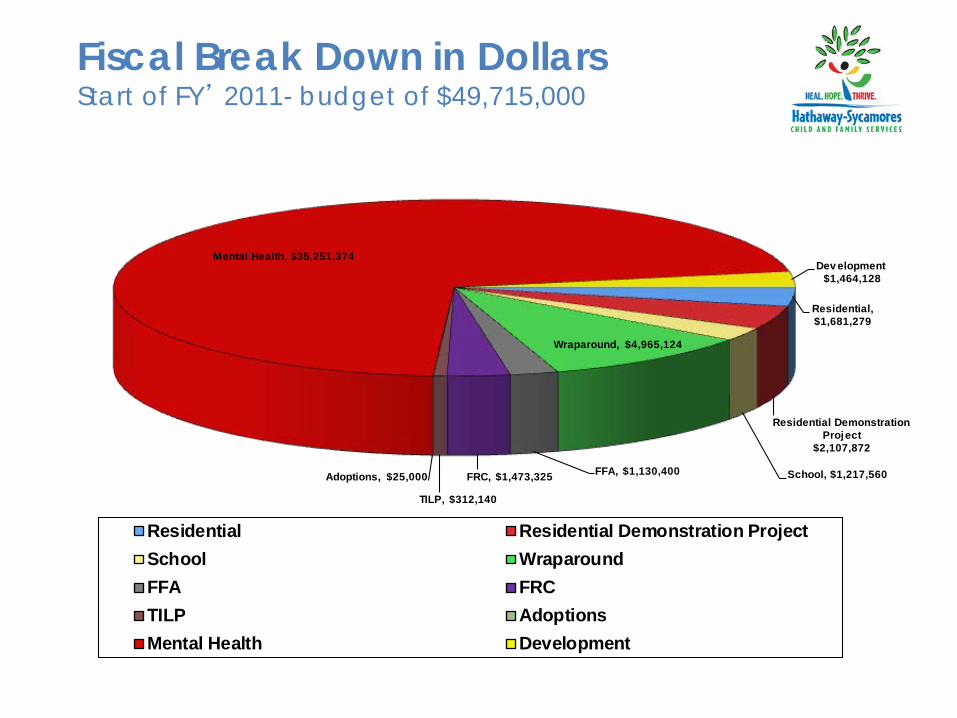
Fiscal Break Down in Dollars Start of FY’ 2011- budget of $49,715,000
Residential, $1,681,279
Residential Demonstration Project
$2,107,872
School, $1,217,560
Wraparound, $4,965,124
FFA, $1,130,400 FRC, $1,473,325
TILP, $312,140
Adoptions, $25,000
Mental Health, $35,251,374 Dev elopment $1,464,128
Residential Residential Demonstration ProjectSchool WraparoundFFA FRCTILP AdoptionsMental Health Development

Fiscal Break Down in Percentages Start of FY’ 2011- budget of $49,715,000
Residential 3.4%
Residential Demonstration Project
4.2% School 2.5%
Wraparound 10.0%
FFA 2.3%
FRC 3.0%
TILP 0.6%
Adoptions 0.1%
Mental Health 71.0% Dev elopment
3.0%
Residential Residential Demonstration ProjectSchool WraparoundFFA FRCTILP AdoptionsMental Health Development

Fiscal Position in 2015
The Hathaway-Sycamores budget at the beginning of FY’14-15 was > $55,000,00 All Growth Since 2011 has been in Community-Based services and has been >$5 Million

Assessing Where Your Organization Is At

Identify and promote practice and policy initiatives that will create strong and closely coordinated partnerships and collaborations between families, youth, community- and residentially-based treatment and service providers, advocates and policy makers to ensure that comprehensive services and supports are family-driven, youth-guided, strength-based, culturally and linguistically competent, individualized, evidence and practice-informed, and consistent with the research on sustained positive outcomes.
BBI Mission

BBI Self-Assessment Tool: Purpose
• Establish guideposts for operationalizing principles and practices of the BBI Joint Resolution.
• Provide information about:
• The degree of continuity, seamlessness and integration of services and support.
• The extent to which known promising and/or best practices are being utilized in both or either residential and community settings.
• A platform to stimulate quality improvement (QI) activities - intended to identify guidelines where there is disagreement between respondents OR where no or little activity is occurring as assessed by one or more parties (i.e. family members), so that QI work can occur.
• The SAT is NOT intended to be used for monitoring program “compliance”.
• The SAT Glossary provides a definition of terms used throughout the SAT. It is available at the BBI website (www.buildingbridges4youth.org)
27

BBI Self-Assessment Tool Framework: Assumptions
Regulatory bodies are already monitoring standards and practices in residential and community settings. Other resources (e.g. cultural competency, self assessment, wraparound fidelity) are available and do not require duplication. A high degree of mutual interdependence between all stakeholder is important to implement the values and principles of the BBI Joint Resolution. The tool is intended to spark dialogue, inclusive of community, family, youth and agency staff who are involved and familiar with the residential agency-to help structure conversations that focus collective energy on outcomes and effective practices.
28

Elements of the BBI SAT
1. Child and Family Team 2. Family Driven Practices 3. Youth Guided Practices 4. Cultural and Linguistic Competence 5. Entry Into Residential Treatment 6. During Residential Treatment 7. Post-Residential Treatment 8. Community System of Care 9. Performance and Evaluation in the System of Care
29
Who is the SAT for?
Designed to be used with groups of: • Residential staff • Community staff • Advocates • Youth • Families • Funders/ oversight agencies
Approaches to Administering the BBI SAT
Decide which is the best approach for your program and/or community; examples include, but are not limited to:
• The residential or community program lead staff completes the tool with one discipline of staff at a time, followed by discipline specific dialogues and decisions about action steps regarding improvement needs based on findings;
• The residential or community program lead staff completes the tool with groups of youth and/or families, involving them in dialogue about improvement needs; the ‘findings’ and the summation of the youth/family discussions/recommendation are then shared with executives and/or the group responsible for the BBI Improvement Project at the residential program;
• A comprehensive approach to the SAT, including staff at all levels from residential and community partner organizations, youth, families, and payers.
Often initiated by the residential provider. Consider a variety of implementation options, including pre-discussion of items w/ respective groups of stakeholders. Create opportunities for respondents to discuss the results and collaborate to identify organizational and systemic improvements.
31

Examples of BBI SAT Implementation Approaches • Use the BBI SAT for internal staff development and training • Consider adapting a SAT simulation exercise for training • Take sections of the BBI SAT and implement in staff meetings, or as part of
youth/staff community meetings • Facilitate a discussion of the ratings • Convene discussions of individual items as promising/best practices • Use the Family and Youth tool as the basis for an exit interview and present
results to staff at least annually • Use sections for QI discussions with community partners • Formalize the process internally with Board review and full implementation
and analysis of results • Establish Learning Collaborative at State or regional levels – ensure
stakeholders with BBI expertise and families/youth are partners
32

3. Youth-Guided Practices
1 2 3 4 5 Don’t Know/ Doesn’t Apply Never/
Almost Never
Rarely
Sometimes
Often Always/
Almost Always The goals of the treatment plan are based on the
youth’s own goals.
If they are able, youth guide the Child and Family Team meetings.
Youth develop full understanding of the treatment plan.
Youth are involved in everyday decision-making about their care.
Peer advocates support youth in: a. Treatment Planning b. returning to the community c. transition to post-residential placement
Youth have a voice in selecting members of their Child and Family Team.
Examples From the SAT
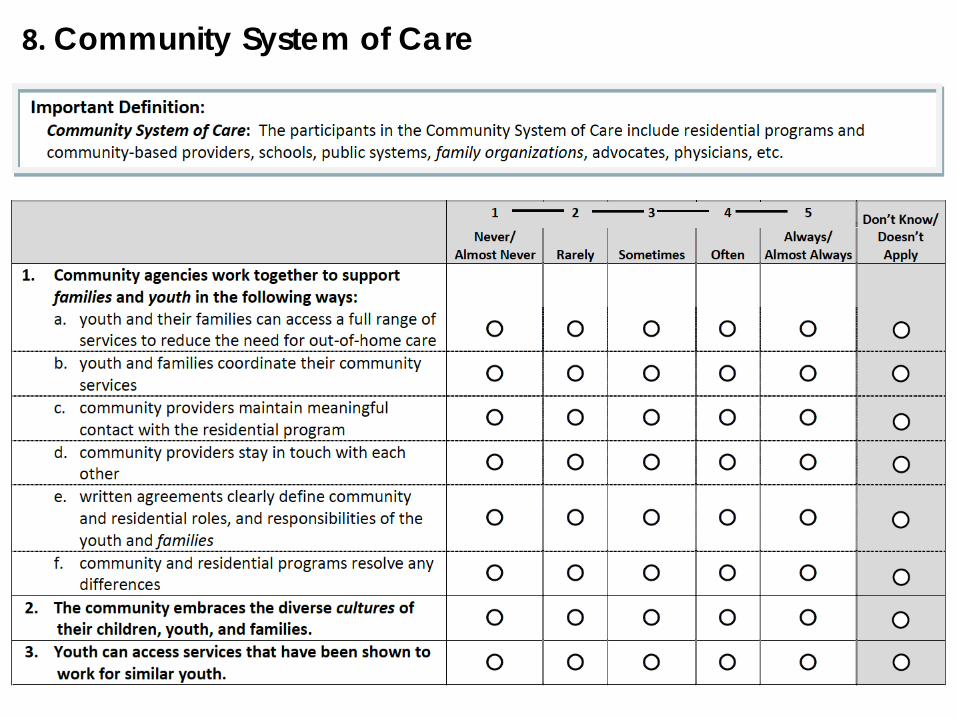
8. Community System of Care

Example of Use
LA Providers utilized the SAT Tool from Building Bridges • Administered at Start of RBS Program • Completed by All 3 Providers • Comparison of Demonstration Project and RCL Programs • Groups Completing Included: Residential staff Community staff Advocates Youth Families Funders/ oversight agencies
• To be re-administered after the first 4 years of the project
35
The SAT Glossary provides a definition of terms used throughout the SAT. It is available at the BBI website (www.buildingbridges4youth.org)

Another Tool for Organizational Assessment
http://www.createthefuture.com/CBtoolkit.htm
The Center for Public Skills Training Capacity Building Toolkit 1
1 T his Capacity Building Action Planning Toolkit was originally developed by Frank Martinelli and Shelly Schnupp for use by local associations of the Great Lakes Alliance of the YWCA as part of the GLA Capacity Building Project.
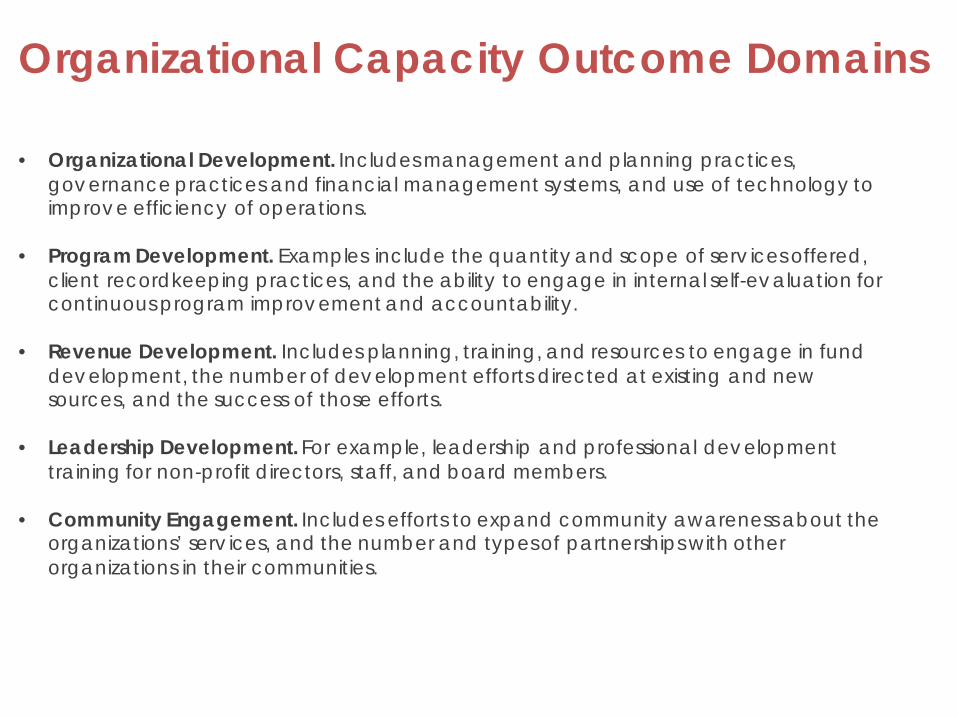
Organizational Capacity Outcome Domains • Organizational Development. Includes management and planning practices,
governance practices and financial management systems, and use of technology to improve efficiency of operations.
• Program Development. Examples include the quantity and scope of serv ices offered,
client recordkeeping practices, and the ability to engage in internal self-evaluation for continuous program improvement and accountability.
• Revenue Development. Includes planning, training, and resources to engage in fund
development, the number of development efforts directed at existing and new sources, and the success of those efforts.
• Leadership Development. For example, leadership and professional development
training for non-profit directors, staff, and board members. • Community Engagement. Includes efforts to expand community awareness about the
organizations’ serv ices, and the number and types of partnerships with other organizations in their communities.
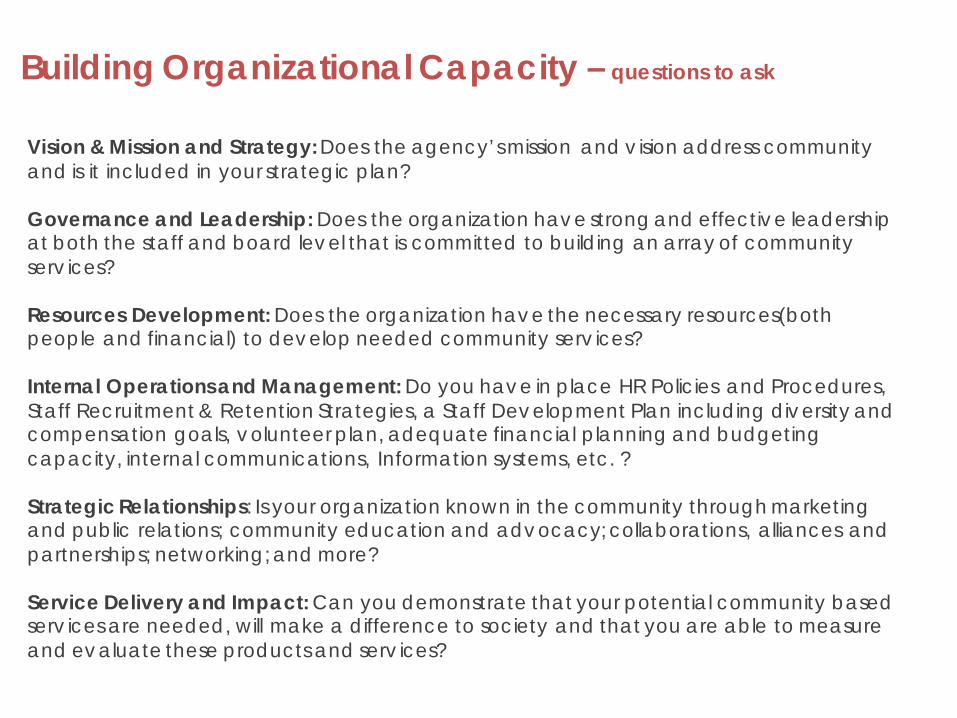
Building Organizational Capacity – questions to ask
Vision & Mission and Strategy: Does the agency’s mission and v ision address community and is it included in your strategic plan? Governance and Leadership: Does the organization have strong and effective leadership at both the staff and board level that is committed to building an array of community serv ices? Resources Development: Does the organization have the necessary resources(both people and financial) to develop needed community serv ices? Internal Operations and Management: Do you have in place HR Policies and Procedures, Staff Recruitment & Retention Strategies, a Staff Development Plan including diversity and compensation goals, volunteer plan, adequate financial planning and budgeting capacity, internal communications, Information systems, etc. ? Strategic Relationships: Is your organization known in the community through marketing and public relations; community education and advocacy; collaborations, alliances and partnerships; networking; and more? Service Delivery and Impact: Can you demonstrate that your potential community based serv ices are needed, will make a difference to society and that you are able to measure and evaluate these products and serv ices?

Capacity Building Toolkit Example – Internal Management and Operations

Capacity Building Toolkit Example – Service Delivery and Impact

Capacity Building Toolkit Example – Strategic Relationships

Examples of Community Based Services Organizations May Develop
• Co-Occurring/Addiction Prevention Services • Foster Care • Intensive Treatment Foster Care • Adoption • Transitional Independent Living • Family Resource Center • School Based Mental Health Services • School Based Educational Programs • Therapeutic Behavioral Services – In-Home • Outpatient/Psychiatric Services • Home Based Services • Youth Advocacy
• Family Finding/Search & Engagement • Family Preservation • Kinship Support Services • Parent Advocate Programs • Wraparound • Employment Services • Housing Services • Day Care/Head Start • Charter Schools • 0-5 Services • Autism Spectrum Services

Topics for Future Webinars Include
Systems Approach to Change • A systematic approach to providing community-based services
Management Infrastructure Needs • Organizational culture and how that will impact the work with families, staff retention. • Hiring for the right people to do this new kind of work and how you move along those who don’t.
The Value of Real & Effective Partnerships • Establishing connections with community providers • How to implement timely, relationship-based resources to meet needs in multiple life domains
Innovative Service Delivery Models • Short term crisis models • Intensive In-home models
Outcomes • An agencies commitment to improve the outcomes for children and families should be the
fundamental driver of system change efforts. • How do you utilize data to support these change efforts • Focus on functional skills in the community vs. in residential and also on long-term, sustained
positive outcomes. Supervision Models
• What are the critical skill sets • Family finding skills • Ongoing training & mentoring

’s

Contact Information
William P. Martone President WPM Consulting, Inc. 1516 Beech Street South Pasadena, CA 91030 Cell Phone: 626-831-6850 E-Mail: [email protected]

Appendix
Residentially Based Services Reform in California
What is RBS Reform
California's Residentially-based Services Reform initiative seeks to transform the state's group homes, currently providing long-term congregate care and treatment, to programs combining short-term residential stabilization and treatment with follow-along community-based services to quickly reconnect youth to their families, schools and communities. In 2007, with the passage of AB 1453 (Soto), support of the California Department of Social Services (CDSS), financial support from Casey Family Programs, and the creation of the RBS Reform Coalition, reform of the State's system for care and treatment of youth with challenging needs came to fruition. The legislation authorized selection of four counties or consortia of counties that, with private partners, will implement alternative program and funding models consistent with the framework document that defines and describes RBS. The lessons learned from these projects informed planning for statewide implementation of RBS reform presented to the Legislature in 2011.
Los Angeles Model
Los Angeles selected by State to participate in RBS Parallel to State reform Los Angeles also working on Group Home Reform since 2005 The ResWrap* model Hathaway-Sycamores Child and Family Services developed with three other providers in Los Angeles in 2004, and presented at previous Alliance Conferences, became the basis for the development of the Los Angeles RBS reform model *ResWrap combines Residential and Wraparound approaches

LOS ANGELES COUNTY RESIDENTIALLY BASED SERVICES DEMONSTRATION PROJECT
OPEN DOORS Los Angeles County was selected, along with three other counties (San Bernardino, Sacramento and the Bay Area Consortium) to participate in an AB 1453 “Residentially Based Services” (RBS) demonstration project to shorten timeframes to durable permanency for children who face a residential stay. LA’s plan is to infuse residential care with Wraparound principles (active family voice and choice, facilitated planning process, care coordination, family finding), and transform the traditional residential milieu to a therapeutic community without walls.
Note: CA is a IV-E Waiver State and Los Angeles County is operating as one of two IV-E Waiver Counties in CA providing it greater flexibility in funding models than other Counties
52


Key Components of Model
Target Population
Children in or at risk of RCL – 12/14 placement (high-end placements) 52 bed demonstration Approximately 160 children to be served in 2 years
The RBS Collaborative Partners
DCFS DMH Five Acres - (Boys only - Ages 6-14 - 18 beds - 2 open) Hillsides - (Co-ed - Ages 6-17 - 18 beds - 2 open) Hathaway-Sycamores - (Boys only - Ages 6-17 - 16 beds - 1 open)
Innovations
Treatment without walls Family search, engagement, preparation and support from Day 1 Flexible funding to support innovation Waiving RCL requirements

Key Components continued
Key Features
One Child and Family Team across all environments One plan of care Crisis stabilization without replacement Respite in the community
Outcomes (see resources for details)
Safety, Permanency and Well Being; Decreased length-of-stays in residential placements; Reduced re-entry Increased use of informal or “natural” community supports
Performance Measures
CAFAS School Report Card CANS WFI-4 YSS Client Demographics YSS-F Changes of Placement

Client Eligibility Criteria
Must be a Department of Child and Family Services (DCFS) Client
Would Otherwise Need RCL 12 or 14 Placement
•As Determined by Resource Management Process & CANS (Child and Adolescent Needs and Strengths) •Must Enter Residential Treatment Program
Will Need Significant Community Development Work to Achieve Permanency
Will Need Significant Family Finding and Development Work to Achieve Permanency
•Having or not having family not a criteria for admission •Bridge care available if family is not ready (foster home, relative home)
Will Need Intensive Services Post-residential to Sustain Permanency* * DCFS case must remain open throughout arc of care

Key Fiscal and Policy Challenges
Fiscal How to build a better funding model
How to creatively overcome existing methods of payment • Blending funding streams to pay for model
Determining IV-E Allowable Costs in model
Waiving the RCL System Policy
How to change current attitudes toward residential care
Using data to determine how children fare
Leadership for Reform (CA Alliance / LA County/Providers/ Casey Family Programs – $ support for reform)
How long public policy changes take to implement
How to market project to “powers that be” (County BOS/State Officials/County Social Workers etc.)
Fiscal Model for Los Angeles
The RBS providers will be paid a new RBS case rate which will fund up to ten months in residential care, a Child and Family Team, concurrent family finding engagement, preparation and support, respite, crisis stabilization, and intensive parallel community-based interventions including the development of connections. After ten months of residential care (not necessarily concurrent) have been used, the rate will convert to a lower rate to incentivize providers to reconnect children with their families and communities and return them quickly to home based settings. Waiving the RCL System for the RBS Units only; the RCL system will no longer apply so that all Open Doors beds (formerly RCL 12 or 14) represent a single level of care. The Waiver Request reflects the transformed staffing and treatment model outlined in the Voluntary Agreement and the Funding Model.

Fiscal Model for Los Angeles continued
Provider is at risk for meeting cost neutrality over a 24 month period - $147,314 Reconciliation process after 24 month period
Reconciliation Process Average cost per child defined as:
The exit cohort Children in care for 24 months during the first 24 months of the Demonstration
If average cost is over $147,314 provider pays difference back to County If average cost is less than $147,314 savings shared 50/50 between provider and County – dollars to be used for reasonable and allowable child welfare related services
Actual Residential Cost Determination Residential Rate is an estimate Actual costs to be determined at conclusion of project Provider may keep up to 10% excess over actual cost Any excess beyond 10% is returned to the County Rate to be renegotiated if project is extended beyond 24 months

Staffing Model (for a 16 bed facility) Residential Group CareResidential Director 0.40Milieu Supervisor 1.00Youth Specialists 14.00On-Call Youth Specialists 3.00
18.00
Community Services StaffProgram Director 1.00Clinical Supervisor 1.00Clinician 6.50Lead 2.00Family Facilitator 6.50Youth Specialist 6.50Family Finding & Engagement 2.00Lead Parent Partner 1.00Parent Partner 6.50Family Crisis Response Team 6.00Administrative Support 1.50
40.50Mental Health Specialty StaffPsychiatric Services 1.00Medical Services Staff 1.50TBS 6.00MHRS Staff/Youth Specialists 9.00
17.50Shared Program Support Program Oversite & Supervision QA/QI Clinician 0.50 DMH Billing & Chart Staff 1.50
2.00
Total Salaries & Wages 78.00
Initial Staffing Model for RBS including residential and community components of the model
Techniques Used to Overcome Fiscal and Policy Challenges Partnerships of Key Visionary Individuals
Including parents and youth in planning
Re-conceptualizing the use/purpose of residential treatment Significant Investment of Time Neutral Coordination by 3rd parties (consultants and Casey) Building off Wraparound Principles/Values
ResWrap Pilot Results Family Decision Making/Child &Family Team Fundamental shift in philosophy on how the family is viewed Realization that many children being successfully served in Wraparound in the community are the same children being referred to residential treatment
Developing Fiscal Creativity Creating cross-team Training and Evaluation Workgroups for the project Social Marketing to County Social Workers

Additional Resources
Information On The California RBS Reform Coalition Project And Other County Models Can Be Found At:
www.rbsreform.org
The Community Technical Assistance Center of New York
To obtain Continuing Education Unit credits, please 1. Please log into the webinar system via your computer, and view the
entire presentation 2. Go to http://socialwork.nyu.edu/alumni/continuing-
education/OnlinePortal.html 3. Create a profile 4. Select today’s webinar 5. Pay the $15 processing fee 6. Take the Knowledge Test* *The Knowledge Test will be made available to you within the week. You will receive an email with this information within 24 hours of this webinar.

The Community Technical Assistance Center of New York