Electronic Fetal Monitoring D. Lata Sharma, MD, FRANZCOG Senior Lecturer, University Of Queensland,...
70
Electronic Fetal Monitoring D. Lata Sharma, MD, FRANZCOG Senior Lecturer, University Of Queensland, Australia
-
Upload
nathaniel-jenkins -
Category
Documents
-
view
215 -
download
0
Transcript of Electronic Fetal Monitoring D. Lata Sharma, MD, FRANZCOG Senior Lecturer, University Of Queensland,...
Electronic Fetal Monitoring
D. Lata Sharma, MD, FRANZCOGSenior Lecturer, University Of Queensland, Australia
HISTORY - EFM
1818-Francios Major in Geneva-DDx between FH and Maternal Pulse
1827- John C Ferguson –described FHR sounds. 1849-Killian indicated FHr parameters requiring interventions. 1876-Pinard produced his design for a fetal stethoscope. 1893-Winkel set normal FHR120-169 bpm. 1958-Hon in USA and Hammacher in Europe introduced first
EFM. 1964- Doppler ultrasound scan replaced phonocord. 1966- Saling in Berlin introduced FBS. 1968-Hamacher and Hewitt-Packard developed first fetal
monitor. 1985- Dublin RCT changed terminology for the CTG
interpretation.
Electronic Fetal Monitoring
Pioneered in 1958 by Hon.in USA and Hammacher in Europe
Commercially available 1968 Continues monitoring of FH in low risks
pregnant -lacks evidence Needs to be viewed in conjunction with
other assessment e.g. FBS and clinical situation.
Should be used for the right reason and with appropriate degree of skill.
EFM-ISSUES
Detect fetal hypoxia i.e reduce and avoid harm to the fetus and improve fetal and baby out-come.
Severe acidosis may result in FHR changes. Could occur in Normal physiological response in
labor. Misunderstanding the physiological and
pathphysiological CTGs will improve the Mx.
EFM Problems and Realities
Electronic Intra-partum FHR Monitoring is now considered mandatory for high-risk pregnancies.
Difficulties with interpretation include over confidence and not-only difference in opinion between practitioners but, also when the same practitioner examines the same CTG twice.
Increases CS rates 1.41%rr. Increases operative vaginal delivery 1.20%rr. And no change in incidence of C Palsy. Reduction in Neonatal seizures rates 0.51% No difference in APGAR scores. ? About the efficacy.
EFM- Facts
Reliability of interpretation-50-75% are false positive .
False positive Dx reduces to 105 with FBS. FBS 93% sensitivity, 6% false positive. PH Vs Lactate -39% Vs 2.3(rr 16.7).
Electronic Fetal Monitoring-Indications
Indications for the continuous EFM
High risk pregnancies
IOL and Augmentation of Labour.
Reduced FM. Premature
labour/TPL. APH/IPH
Oligohydramnios Hypertension. Abnormal FHR
detected. Malpresentation and in
labour. DM,Multiple Gestation. Previous CS. Abdominal Trauma. Prolonged ROM. Meconium Liq.

EFM- Interpretation
Consider : Intrapartum/antepartum trace. Stage of labour. Gestation. Fetal presentation, ?Malpresentation. Any augmentation,?IOL Medications Direct or indirect monitoring/
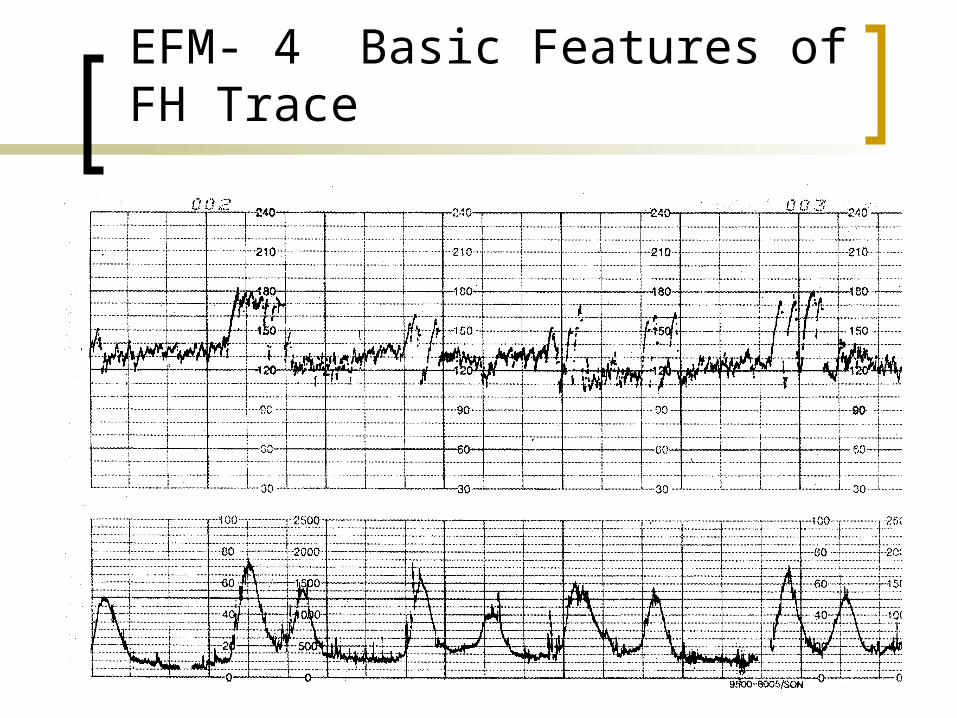
EFM- 4 Basic Features of FH Trace
EFM-4 Basic Features.
Baseline FHR - Mean level of FHR when this is stable, excluding Accelerations and Decelerations (110-160 bpm)-Tachycardia-Bradycardia
Baseline Variability-5 bpm or greater than or equal to 5bpm, between contractions-Normal-Non-reassuring-Less than 5 bpm or less but less than 30 min-Abnormal-less than 5 bpm for 90 min or more.
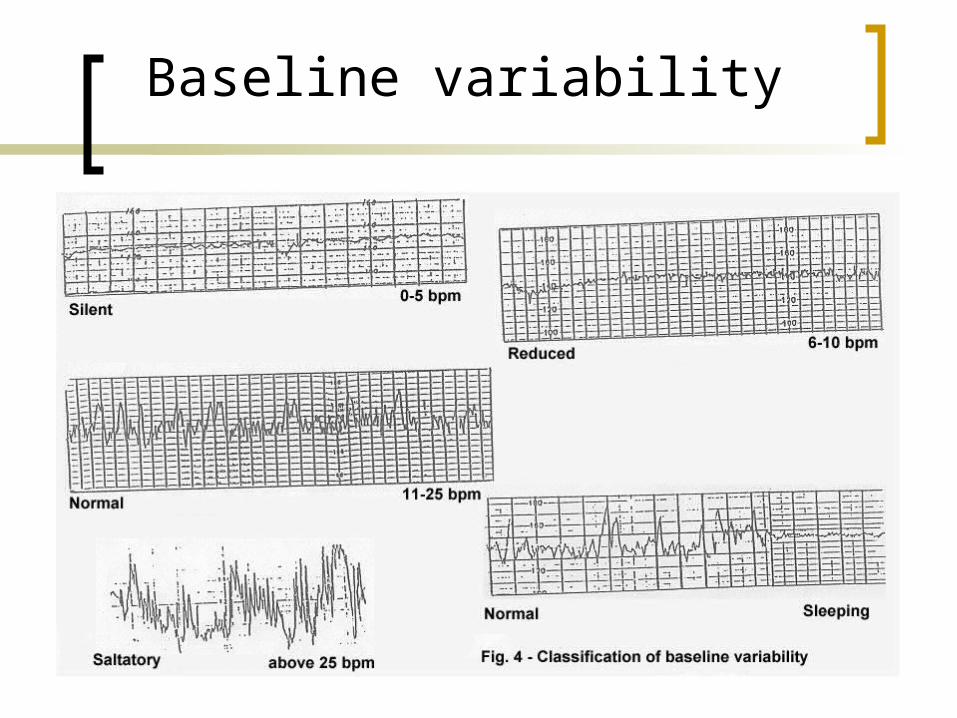
Baseline variability CTG
Baseline variability
Baseline variability
The minor fluctuations on baseline FHR at 3-5 cycles p/m produces Baseline variability.
Examine imin segment and estimate highest peak and lowest trough.
Normal is more than or equal to 5 bpm.
Factors affecting Baseline variability.
Para-Sympathetic affects short term variability whilst Long Term is more Symp.
CNS ,Drugs reduce Variability High gestation increases variability Mild Hypoxia may cause both S and
para S stimulation.
Non-reassuring Baseline variability.
NRCTGs- reduced or less than 5 bpm for 40 min or more but less than 90 mins..
B-B or short Term V is varying intervals between successive heart beats .
Long Term v is irregular waves on the CTG 3-5 bpm.
Normal is 5-25 bpm– this indicates N-CNS.
EFM-Accelerations
Accelerations- transient increase in FHR of 15 bpm or more lasting for 15 sec.
Absence of accelerations on an otherwise normal CTG remains un clear.
Presence of FHR Accelerations have Good outcome.
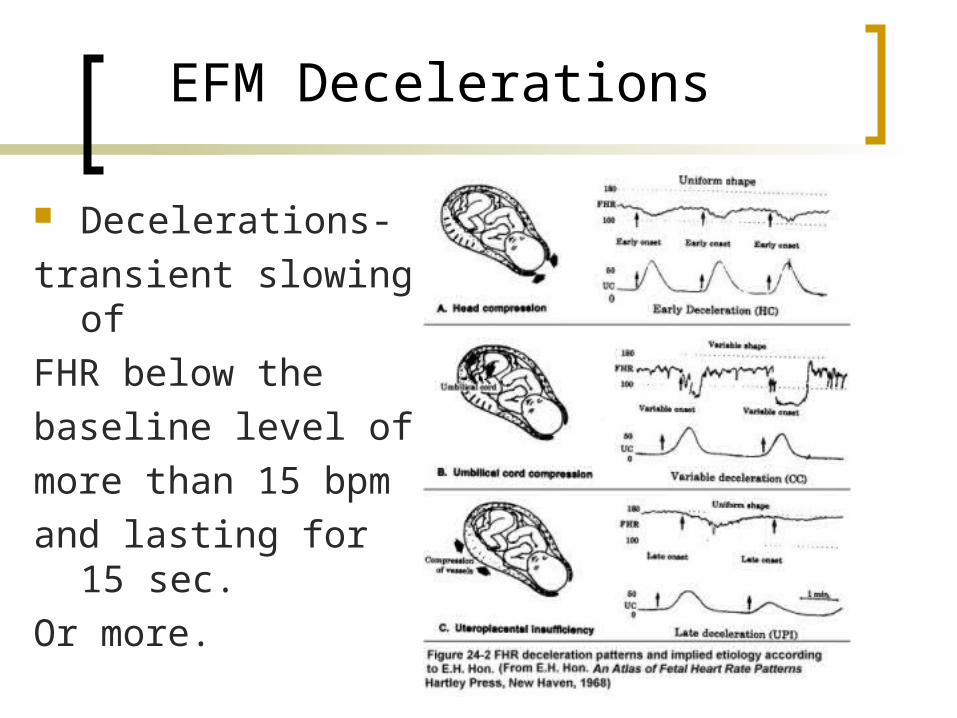
EFM Decelerations
Decelerations-
transient slowing of
FHR below the
baseline level of
more than 15 bpm
and lasting for 15 sec.
Or more.
Electronic Fetal Monitoring
a) Early Decelerations (fig 3) Head compression Begins on the onset of contraction
and returns to baseline as the contraction ends.
Should not be disregarded if they appear early in labor or Antenatal.
Clinical situation should be r/v
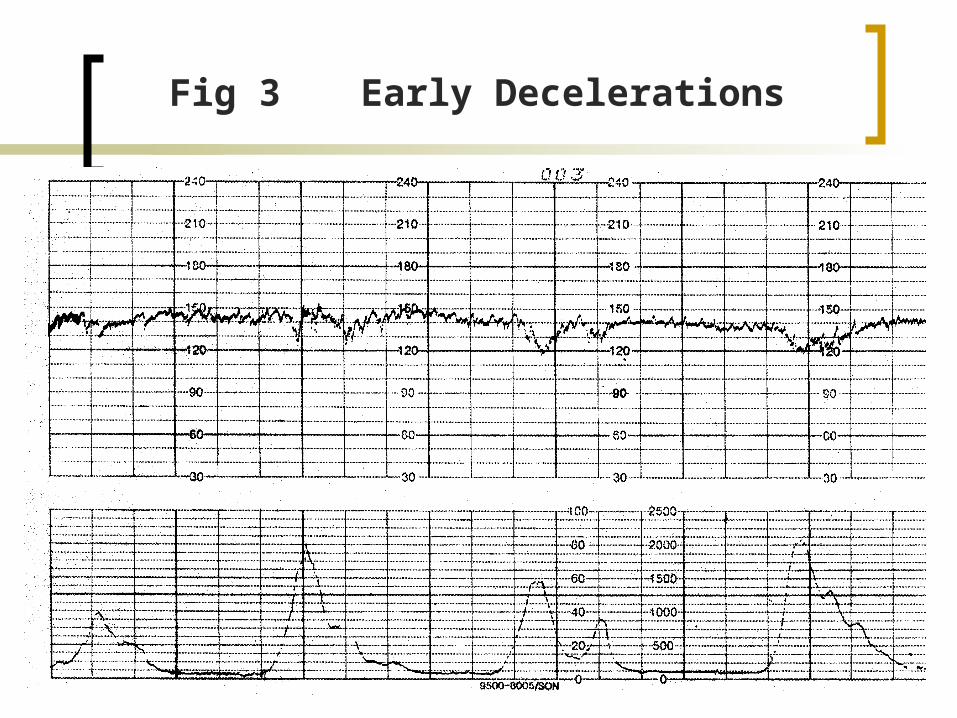
Fig 3 Early Decelerations
Late Decelerations.
Uniform periodic slowing of FHR with the on set of the contractions .
Repetitive late decels increases risk of Umbilical artery acidosis and Apgar score of less than 7 at 5 mins and Increased risk of CP.
Electronic Fetal Monitoring
b) Late Decelerations (Fig 4)• Due to acute and chronic feto-placental
vascular insufficiency Occurs after the peak and past the length of uterine
contraction, often with slow return to the baseline. Are precipitated by hypoxemia Associated with respiratory and metabolic acidosis Common in patients with PIH, DM, IUGR or other
form of placental insufficiency.
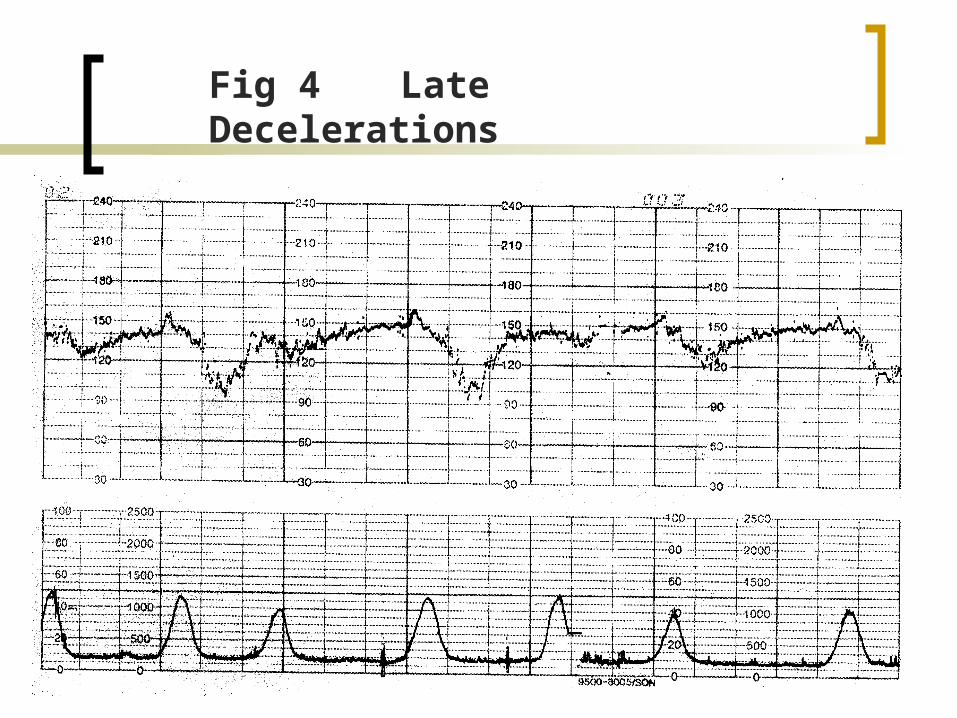
Fig 4 Late Decelerations
Late Decelerations
Reduces Baseline variability together with Late Decelerations or Variable Decelerations is associated with increased risk of CP.
EFM- Variable Decelerations
Variable intermittent periodic slowing of FHR with rapid onset recovery and isolation.
They can resemble other types of deceleration in timing and shape.
Atypical VD are associated with an increased risk of umbilical artery acidosis and Apgar score less than 7 at 5 min
Additional components: Loss of 1 degree or 2 degree rise in baseline Rate Slow return to baseline FHR after and end of contraction. Prolonged secondary rise in Base FHR Biphasic deceleration Loss of variability during deceleration Continuation of base line at a lower level.
Electronic Fetal Monitoring
c) Variable Deceleration (Vagal activity) (Fig 5) Inconsistent in configuration, No uniform temporal r-ship to the onset of contraction, are
variable and occur in isolation. Worrisome when Rule of 60 is exceeded (i.e. decrease of
60 bpm,or rate of 60 bpm and longer than 60 sec) Caused by cord compression of the umbilical cord Often associated with Oligo-hydroaminos with or without
ROM Can cause short lived RDS if they MILD Acidosis if prolonged and Recurrent.
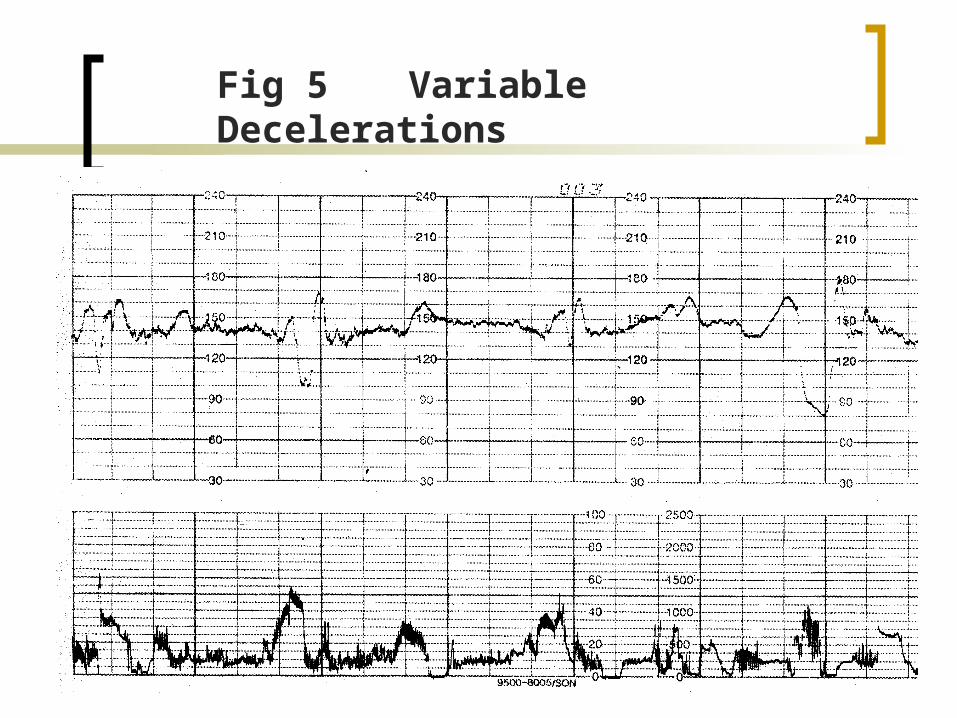
Fig 5 Variable Decelerations
EFM Prolonged deceleration
Prolonged Deceleration (Fig 6) Drop in FHR of 30 bpm or More lasting for at
least 2 min Is pathological when crosses 2 contractions i.e 3
mins. Reduction in O2 transfer to placenta. Associated with poor neonatal outcome.
EFM- Prolonged DecelerationsCAUSES
Cord prolapse. Maternal hypertension Uterine Hypertonia Followed by a VE or ARM or SROM
with High PP.
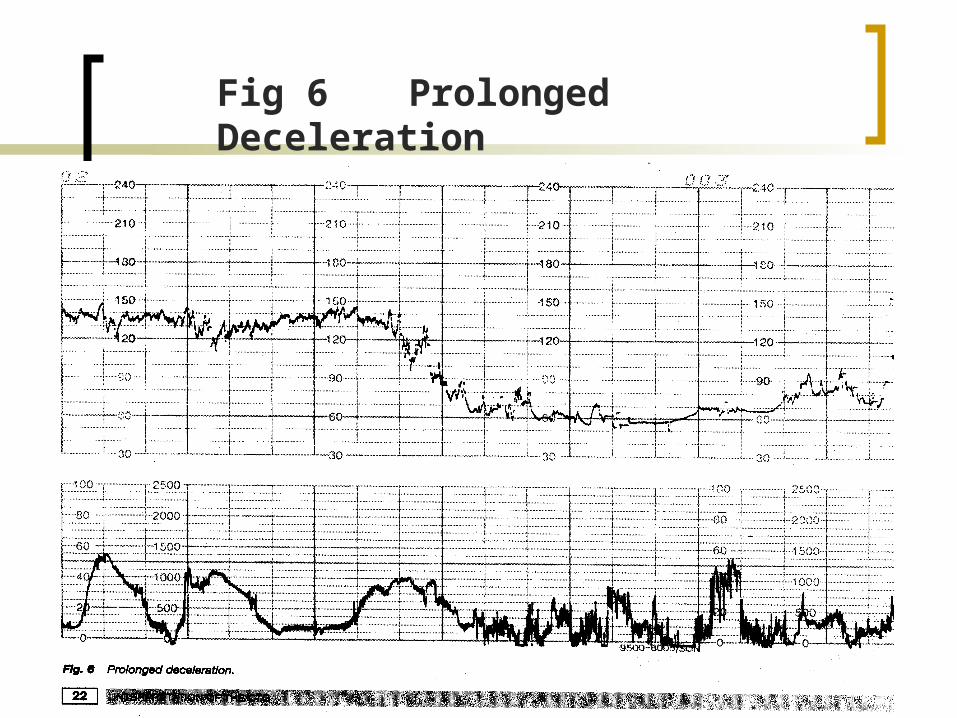
Fig 6 Prolonged Deceleration
EFM Mx Prolonged Deceleration
Maternal position IV fluids V.E to exclude cord prolapse Assess BP FBS if cx dilated and well applied PP Mx Depending on the clinical situation.
Baseline Bradycardia
FH below 110bpm(FIGO ). less than 100bpm (RANZCOG).Causes.Postdates, Drugs, Idiopathic,Arrythmias, hypothermia(increased Vagal
Tone)Cord Compression (Acute Hypoxia, congenital
H/disease and Drugs).Mx depends on the clinical situation.(FBS,VE
Observation or expedite delivery)
Types
Moderate Bradycardia 100-109 bpm Abnormal bradycardia less than
100bpm. Tachycardia 161-180 bpm Abnormal Tachycardia more than 180
bpm Ranzcog Australian more than 170
bpm
Baseline tachycardia and Bradycardia.
Uncomplicated baseline tachycardia 161-180 bpm or bradycardia 101-109 do not appear to be associated with poor NN outcome.
Causes of B Tachycardia.
Asphyxia Drugs Prematurity Maternal Fever Maternal thyrotoxicosis Maternal Anxiety Idiopathy Mx depends on the clinical situation
Electronic Fetal Monitoring
Baseline Bradycardia FH Rate below 110bpm (FIGO Recommended) Postdates Drugs Idiopathic Arrhythmia's Hypothermia.(Increased Vagal tone), Cord compression(Acute Hypoxia,Congenital
H/disease, and drugs)Mx depends on the clinical situation. (FBS, VE, Observation or expedite Delivery).
Electronic Fetal Monitoring
Baseline Tachycardia Asphyxia Drugs Prematurity Maternal fever Maternal thyrotoxicosis Maternal Anxiety Idiopathy
Mx depends on the clinical situation
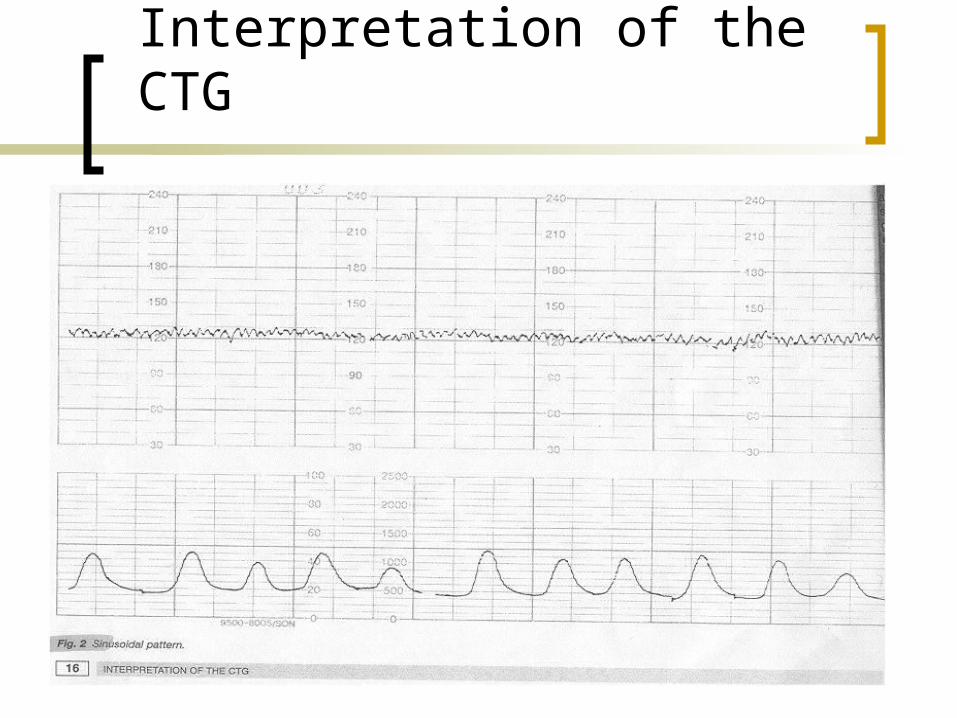
Fig 2 Sinusoidal pattern
Interpretation of the CTG
EFM-Sinusoidal Pattern
Regular Oscillation of the Baseline long-term Variability resembling a Sine wave ,with no B-b Variability (Fig 2),
Has fixed cycle of 3-5 p min. with amplitude of 5-15 bpm and above but not below the baseline.
Should be viewed with suspicion as poor outcome has been seen (eg Feto-maternal haemorrhage)
Electronic Fetal Monitoring
Sinusoidal pattern - distinctive smooth undulating Sine-wave baseline with no B-b variability ( Fig 2 ) 0.3 % (Young 1980) cord compression hypovolemia ascites idiopathic(fetal thumb sucking) Analgesics Anaemia Abruption Mx r/v clinical situation
EFM- Saltatory pattern
Seen During Fetal thumb sucking. Could be associated with Hypoxia. See slide 11.
NR CTGs
Difficult to interpretation,leads to Increased rate of C Section.
50% CTG in Labour have 1 abnormal feature
15-20% Nr CTGs (pathological). ?? To reduce CS….
F O R E M O S T Feta oximetry randomised evaluation Multi Oxygen saturation Trial
To evaluate the role of F Sats P02 Had a Multicentre Randomised trial- RWB Brisbane MMH Brisbane RWH Melbourne RWH Sydney
Endpoints
To reduce Operative deliveries for the Nr CTG by 1/3
The Sample size was 600 participants. Secondary Endpoint- Investigate the incidence of Dystocia F/up outcomes Low Umbilical arterial PH NICu admissions HIE (Enchelopathy) Maternal perception of monitoring Clinician perception of sensor placement.
NR CTG (Foremost)
Any of the following for more than 15min-Persistent Late decelerationsSinusoidal patternVariable decelsLess than 70 bpm for more than 60 secPersistent slow return to the baselineLong term variability less than 5 bpmTachycardia more than 160 bpm.Recurrent prolonged deceleration 2 or more in15 min and less
than 70bpm for 90 sec .Any on of the following for more than 60 minTachycardia with variability less than 5bpmPersistent reduced baseline variability less than 5 bpm for more
than 60min.
Inclusion Criteria
NR CTG Consent Gest age more than 36 k Early or active labour ROM or eligible for
Exclusion criteria
Multiple gestation Non-Vertex Pl Praevia APH Fetal anomaly HIV other Thrombocytopenia.
Clinical Mx Protocol
CTG Only Reassuring –continue labour unless
otherwise indicated NR CTG –Evaluate and manage NR
CTG Suspicious CTG Deliver for NR Fetal Status.
CTG and Oximetry
Reassuring CTG Continue NR CTG Continue unless otherwise
indicated( FSp02 Reassuring) If FSp02 less than 30%- Further Evaluation and MX
Suspicious CTG -Deliver
Conclusion
R/v NR CTG Mx tools & decision making
Responsibility to assess new technology before widespread introduction
Overview of Multicentre RCT Case presentation.
Reliability of CGT Interpretation
50%-75% false positive False Positive Dx is reduced to 10%
with FBS PH Vs lactate 39% Vs 2.3%(rr16.79).
Fetal Blood Sampling
information on the acid base balance Has 6%-20% false- normal 8-10% False Low valuesWhy and when to do-Persistent Abnormal CTG after reversible factors have been
corrected, Persistent late decels and 2 abnormal other features e.g baseline tachycardia or reduced B-B variability or just difficult to interpret the CTG
Rom, PP accessible and well applied Cx dilatation at least 3 cm or more
Left lateral maternal positionSterile environment and good light and equipment.Good analgesia
FBS-PH
Introduced by Sailing –fairly reliable predictor of fetal PH in presence of abnormal FHR
Has an error of 15% falsely low and 5 % falsely increased, however in presence of abnormal FHR a scalp PH of less 7.2 is pathologonomic of fetal asphyxia.
FBS-Cord PH
FBS-Arterial Normal-7.25-7.35 Normally good agreement
between Apgar,cord PH . Less than 7.20-significant asphyxia Values between 7.2 and 7.24 need further
evaluation Low –normal PH should be repeated in 30
min Less than 7.20- eminent delivery
FBS- Lactate
FBS easier to interpret, difficult to perform Anaerobic metabolism can lead to metabolic
acidosis Lactate is major end product of metabolic
acidosis Lactate levels more specific for degree of
metabolic acidosis than Ph Lactate rises quicker takes longer to resolve
than Ph.
FBS Contraindications
FetalPremature –less than 34 ksActive HerpesKnown HIV,Hep B,C positive status.Thrombocytopenia.Maternal-Unfavourable CxMobile PPMalpresentation(face etc) uncertain??Pl Praevia or APHSepsis
FBS-Sampling errors
Between decelerations if possible Avoid Excess pressure on PP reduces
perfusion Do not sample on the caput. Failure of scalp to bleed –due to
peripheral shut down.
EFM-Summary
Normal - CTG with all 4 Features Suspicious -one non reassuring category
and reminder are reassuring Pathological -2 or more non-reassuring
categories or one or more abnormal categories.
At Birth
Need to Consider
Cord PH if CTG suspicious
Preterm labour
Mec Liquor
FBS intrapartum
Flat baby at delivery
Operative or instrumental delivery.
Mx of FBS Results
If PH /Lactate normal –Observe Pre-acidotic were CTG remains to be
Suspicious –Rpt after 30 min. Acidotic-eminent delivery Instrumental or CS depending on the clinical
situation.Lactate 4.8 upper limit-average 2.8 in 1st stage–
changes in labour
Electronic Fetal Monitoring
Education and training Improves Knowledge for all staff Improves clinical skills Training should include instruction on
documenting traces and storage Training should include appropriate clinical
responses to suspicious or pathological traces Training should include local guidelines
relating to fetal monitoring both intermittent and EFM
EFM-Legal Issues
CTG in Litigation Unsatisfactory or Missing Abnormal CTG ignored or not recognized Traces not done.
Risk Mx EFM traces should be kept up to 25 years. If removed for teaching purposes or etc,
should be easily located Minimize incidence of adverse outcome
Legal Issues
In the U.K 70% of cases are due to EFM. In U S A 45.8% involve E F M,
3.8% more $1Million payouts and only17% are due to delay or failure to diagnose fetal distress.
What Influences Litigation
Consumer Expectation The profession –education The employer (policies/procedures) Legislation (duty of care/scope of
practise/ registration)
Legal issues- Consumer expectation
Are for a good outcome (healthy baby/mother)
Bad outcome Someone to blame Someone must pay
Professional Responsibility
To act within scope of practise. To seek support and guidance Work within organisational standards Duty of care to the woman and
employer Maintain knowledge and skills
(evidence Based Practise) Be prepared to defend ones practise.
When EFM is the focus of Malpractice
Comparison of consistency of documentation contained on the trace and in the chart will be made
Lapse in documentation may leave doubt about the quality of care.
Hospital policy and procedure manuals will be examined
Competency levels will be evaluated expert witness (plaintiff/defence)-to determine if acceptable standards were applied.
Major Omission in Liability
Failure to appropriately monitor the mothers and fetus status
In appropriate Syntocinon monitoring Failure to notify the physician in a
timely manner. Initiation of procedures without
adequate client information or consent
Elements of successful Malpractice Action
The clinician had a duty to the woman The clinician had committed a breach
of duty The woman suffered damages There was a casual connection
between the clinician’s actions and the woman's damage.
(MacRae,1993)
Legal issues
If you are going to use the CTG You must be able to Interpret the trace and respond accordingly-
It’s a permanent record One that is scrutinized in litigation case May be pivotal in determining liability
Legal issues
A normal CTG can be used to indicate that that were no abnormalities and no indication for intervention.
An abnormal CTG or suspicious trace may provide evidence that inappropriate or lack of treatment may give rise to litigation,whilst CTGs could be viewed as part of “defensive medicine”, litigation is reported to be on the increase but there is not enough data reporting system in Australia to support this.
References
Manual Obs and Gyn. by Niswander, MD
Fetal Monitoring RCOG UK CTGs RANZCOG Literature review articles American
Family Physician CTG Made Easy