Electrolyte Emergencies for Pediatric Residents
21
Electrolyte Emergencies for Pediatric Residents July 2010 Jennifer Vick, MD
-
Upload
cardiacinfo -
Category
Documents
-
view
608 -
download
4
Transcript of Electrolyte Emergencies for Pediatric Residents

Electrolyte Emergencies for
Pediatric ResidentsJuly 2010
Jennifer Vick, MD

Cases 1 & 2: Serum K of 7.0
• 11 do baby presented to ED with fever but was overall well-appearing
• Sepsis work-up initiated
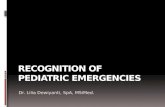
• 12 yo boy involved in MVC, 3 hours ago
• Leg was pinned between front passenger seat and door
• Foley inserted, with urine seen here:

Most Common Etiologies of True Emergent
Hyperkalemia
Body Functions Impaired by ↑ K
CARDIOVASCULAR∙Arrhythmias ( V.fib and asystole most severe)∙Decreased systemic vascular resistanceNEUROMUSCULAR∙Skeletal muscle weakness, usually begins with lower extremities and progresses caudally; rarely involves respiratory musclesRENAL∙Increased Na excretion∙Decreased renal ammonium production (thereby decreased generation of HCO3)ENDOCRINE/METABOLIC∙Aldosterone release (direct adrenal action), decreased renin secretion
• Increased K load• Acute Renal Failure• ↑ed Tissue Catabolism– Tumor Lysis Syndrome– Rhabdomyolysis– Severe hemolysis– Immediately post cardiac
surgery
• Nonoliguric hyper-kalemia of the premature infant

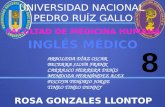
EKG Changes

Management of HyperkalemiaNo EKG Changes, Have Time
• Decrease dietary (or IVF) K• Review medications• Increase Renal excretion (if
possible)– Loop diuretic (lasix)
• Increase GI excretion– Kayexalate (1gram/kg po or
rectal)
• Dialysis if appropriate (ESKD, TLS, etc)
No Time—Gotta Treat
• IV Calcium to stabilize the myocardium– 10% Calcium gluconate
0.5-1.0ml/kg
• IV Insulin (and glucose) which drives K into cells– Glucose 0.5-1.0g/kg– Insulin 0.1 unit/kg
• Albuterol neb (if easily accessible)– <25kg give 2.5mg– >25kg give 5mg
• IV NaHCO3 causes H+ to move out of cells, and K+ to move in– 1-2mEq/kg

HYPO kalemia
• RARELY an emergency• Muscle weakness and
cramps are most common symptoms
• Symptom severity is proportional to degree
• EKG:– Depressed ST segment,
decreased T wave amp, increase U wave amp
• Consider 5 groups of causes:– Spurious, redistribution,
true depletion (usu GI), renal losses, expanded “effective” circulating volume (with HTN, due to mineralocorticoids)
• Correction can almost always be done enterally

Potassium Preparations: PO is PREFERRED ROUTE OF REPLACEMENT!
• Potassium Chloride (KCl)– Preferred for pts with metabolic acidosis due to diuretics
or vomiting– Can be given IV if deemed necessary:
• (3.0 – Measured K) x body weight in kg x 0.04 gives you the value of KCL to give in mmol
• If IV required, but not urgent, rate of infused K should not exceed 0.5-1.0mmol/kg/hr
• Potassium Citrate or Potassium Bicarbonate– Most often used for patients with RTA (low K and acidosis)
• Potassium Phosphate– Can be used in recovery from DKA, in patients at risk of
refeeding syndrome and in TPN

Disorders of Water
Metabolism

Cases 3 & 4: Serum Na 110
• 3yo girl got dehydrated during a GI illness
• Received 20cc/kg NS, then admitted overnight for IVF.
• Initial lab studies (3pm):– 144/5/110/16/28/0.6
• Called to bedside at 3am when she is not rousing
• 18 mo boy with known diagnosis of Bartter’s syndrome, appearing ill after GI illness
• Initial labs:– 110/0.9/76/32/16/0.3

Hyponatremia
Most common
electrolyte abnormality
in hospitalized
children

SIADH
• VERY common in hospitalized kids
• Sosm & Uosm for diagnosis
• Fluid restriction is primary treatment
• Often resolves with child’s recovery

Management of Hyponatremia
• Treat the underlying cause if possible – Pain, nausea, inadequate solute intake, infection, etc.
• Fluid restriction if SIADH is suspected etiology– Remember that SIADH is not a Na problem—it’s a
WATER problem.• 3% saline (0.5mEq/ml) if severely symptomatic to
get patient’s serum Na to 125 • Rule of thumb is to correct no more than 10-
12mEq/L in a 24 hour period• Calculate Na deficit: 0.6 x wt (kg) x (Desired Na –
Measured Na)

Management of Hyponatremia: Some Cautions
• Don’t be fooled by hyperglycemia.– The osmotic load of elevated serum blood glucose pulls
water out of the cells, diluting the concentration of Na (as well as K). An osmotic diuresis causes total body loss of Na & K.
– Differentiate by serum osmolality.– Final Na (mEq/L)=meas Na + 0.16 [glucose(mg/dL) – 100]
• Regardless of your calculations, you need to check the serum Na frequently to prevent overcorrection.– Why? Central pontine myelinolysis

Cases 5 & 6: Serum Na 150
• 13yo girl with severe CP and developmental delay in a group home
• Has recently not been feeling well, and has had decreased interest in taking po
• 16yo boy with recent diagnosis of ALL, who developed a hemorrhagic stroke as a complication of dialysis needed for TLS
• Water intake and UOP each exceed 10L per day

Moritz M, Ayus JC. Disorders of Water Metabolism in Children: Hyponatremia and Hypernatremia. Pediatrics in Review Vol 23, No 11, Nov 2002.
Hypernatremia
Breaks down to either 1) Loss of water, or 2) Failure to adequately replace water loss

Management of Hypernatremia
• If ECFV depletion: bolus with NS– Subsequent IVF should slowly correct fluid loss– Can calculate water deficit and/or monitor serum
Na closely– H20 deficit: TBW x (Measured Na – Desired Na)/
Desired Na. TBW is 0.6 x wt in kg• Possible complication of rapid correction:
CEREBRAL EDEMA– Generally correct 0.5-1.0mEq/L per hour, and
complete correction over 36-72 hours

Cases 7 & 8: Serum Ca 5.5
• 16yo girl with ESKD with a several year history of non-compliance
• Presented to ED complaining of leg cramping over past several days that has worsened, and now hand cramping
• 21 mo boy with FTT, weakness
• Cries when his mom changes his diaper
• X-ray of hips/legs showed severe osteopenia and fractures in various states of healing

HypocalcemiaCAUSES OF….Hypoalbuminemia HyperphosphatemiaRenal failureHypocalcemia of newborn Early or late
HypoparathyroidsimPseudohypoparathyroidismExchange transfusionVit D-deficient or dependent rickets
HypomagnesemiaPancreatitis
FEATURES OF…..
Muscle weakness, fasiculations, or both
Numbness or tingling of extremities
Cramps
Hyperreflexia
Positive Chvostek and Trousseau signs
Tetany
Seizures

Management of Hypocalcemia• Measure serum total (low is <9), and ionized
forms (low <4); full set of chemistries; albumin, Phos, Mg, PTH, alk phos. +/- Vit D
• Can see prolonged QTc on EKG• For severe symptoms (usually seizures):– Give 10-20mg/kg elemental Calcium
• IV 10% Calcium gluconate: 1ml=9mg=0.45mEq• IV 10% Calcium chloride: 1ml=27mg=1.36mEq
– IV Calcium can cause tissue necrosis if extravasates• If Magnesium is low, correct that too

Hyperphosphatemia
• Advanced chronic kidney disease– Decreased renal excretion– Minimize dietary phosphate– Phosphate binders
• Tumor lysis syndrome– Cell lysis, intracellular phosphate released into
serum– Can require hemodialysis– Rasburicase
• If normal renal function, saline diuresis helps