Eight-hourly prothrombin responses after induction dose of Coumadin (warfarin) sodium∗
4
Eight-Hourly Prothrombin Responses after Induction Dose of Coumadin (Warfarin) Sodium* HAROLD BARKER, M.D., V.A.C.C. and R. RANGEL, M.D. Cleveland, Ohio A s THE EXPERIENCE with bishydroxycoumarin (Dicumarol@) has widened, several draw- backs to its general use have come to light so that now it has, to some extent, been replaced by other anticoagulants, particularly its congener,’ warfarin (Coumadin@) sodium. One of the disadvantages of Dicumarol is its slowness of action, namely, a delay in the onset of hypopro- thrombinemia so that therapeutically effective levels may not be achieved for as long as ninety- six hours following the initial dose. Since the clinical value of an anticoagulant may be considered a reflection of its capabilities in both tlLe early establishment of protective cover as ~4 ell as its duration, we wished to assess the usefulness of Coumadin with respect to these characteristics. This report is based upon our experience with Coumadin (warfarin) sodium administered to twenty-five patients requiring anticoagulant therapy. METHODS AND MATERIAL Twenty-five patients were admitted to St. Alexis Hospital with the following diagnoses: twenty-two with acute myocardial infarction; two with acute thrombophlebitis and one with cerebral thrombosis. Each was given 75 yg: Coumadin orally after blood was first drawn for mltial prothrombin time deter- minations. The oral route of administration was utilized since our patients were not vomiting and re- tained drugs given by mouth. Coumadin is ex- tremely soluble in water and appears to be absorbed directly from stomach and intestine. M’e wished to determine how soon after the adminis- tration of this single priming dose of Coumadin the following occurred : a change in prothrombinemia (as evidenced by a change in prothrombin time), the peak level of hypoprothrombinemia, the time of entry into the therapeutic range and the duration of thera- peutic range. We wished to determine, too, the per- sistence of levels of hypoprothrombinemia which, though elevated, are below the generally accepted therapeutic range, i.e., suboptimal; the persistence of excessive levels of hypoprothrombinemia and inci- dence of bleeding. and the correlation between these latter two. In order to accomplish this we conducted pro- thrombin time determinations every eight hours by the Quick one stage methodt during the first ninety- six hours of each patient’s hospitalization. We consider therapeutic hypoprothrombinrmia to be one and one-half to two and one-half times the con- trol prothrombin time, i.e., twenty-two to thirty-five seconds with a control time of fifteen seconds. RESULW The pertinent information concerning the twenty-five patients studied is sumtnarized graphically in Figure 1. Analysis of the data revealed the following significant points : Change.r in PTothrombin Time during L‘lrst l;ortj Hours: At 8 hours: The prothrombin time (PT) in eleven pa- tients was rising; one was in lower limits of thera- peutic range. .4t 76 hours: The PT in twenty-three patients was rising; two were now in therapeutic range ; thirteen were now in suboptimal range of 19 to. but not including, 22 seconds. dl 2.1 hours: The PT in all twenty-five patients was rising; twenty-one were now in therapeutic range; two patients were in suboptimal range. 20 and 9 seconds. respectively. ,4t .?? houn: The PT in twenty-four was now in therapeutic range; in one, no significant change in PT. though rising, was yet apparent. .4/ JO hours: The PT in all twenty-five was now in therapeutic range, including one who had not responded readily earlier. One patient showed a rapid spurt in PT from 25 seconds at 32 hours to 62 seconds at 40 hours when she was given 10 mg. K I. t ISink-Shapiro modification using Simplastin.” * From the Department of Medicine, St. Alexis Hospital, Cleveland, Ohio. NOVEMBER 1960 933
-
Upload
harold-barker -
Category
Documents
-
view
215 -
download
0
Transcript of Eight-hourly prothrombin responses after induction dose of Coumadin (warfarin) sodium∗

Eight-Hourly Prothrombin Responses after
Induction Dose of Coumadin
(Warfarin) Sodium*
HAROLD BARKER, M.D., V.A.C.C. and R. RANGEL, M.D.
Cleveland, Ohio
A s THE EXPERIENCE with bishydroxycoumarin (Dicumarol@) has widened, several draw-
backs to its general use have come to light so that now it has, to some extent, been replaced by other anticoagulants, particularly its congener,’ warfarin (Coumadin@) sodium. One of the disadvantages of Dicumarol is its slowness of action, namely, a delay in the onset of hypopro- thrombinemia so that therapeutically effective levels may not be achieved for as long as ninety- six hours following the initial dose. Since the clinical value of an anticoagulant may be considered a reflection of its capabilities in both tlLe early establishment of protective cover as ~4 ell as its duration, we wished to assess the usefulness of Coumadin with respect to these characteristics.
This report is based upon our experience with Coumadin (warfarin) sodium administered to twenty-five patients requiring anticoagulant therapy.
METHODS AND MATERIAL
Twenty-five patients were admitted to St. Alexis Hospital with the following diagnoses: twenty-two with acute myocardial infarction; two with acute thrombophlebitis and one with cerebral thrombosis. Each was given 75 yg: Coumadin orally after blood was first drawn for mltial prothrombin time deter- minations. The oral route of administration was utilized since our patients were not vomiting and re- tained drugs given by mouth. Coumadin is ex- tremely soluble in water and appears to be absorbed directly from stomach and intestine.
M’e wished to determine how soon after the adminis- tration of this single priming dose of Coumadin the following occurred : a change in prothrombinemia (as evidenced by a change in prothrombin time), the peak level of hypoprothrombinemia, the time of entry into the therapeutic range and the duration of thera-
peutic range. We wished to determine, too, the per- sistence of levels of hypoprothrombinemia which, though elevated, are below the generally accepted therapeutic range, i.e., suboptimal; the persistence of excessive levels of hypoprothrombinemia and inci- dence of bleeding. and the correlation between these latter two.
In order to accomplish this we conducted pro- thrombin time determinations every eight hours by the Quick one stage methodt during the first ninety- six hours of each patient’s hospitalization.
We consider therapeutic hypoprothrombinrmia to be one and one-half to two and one-half times the con- trol prothrombin time, i.e., twenty-two to thirty-five seconds with a control time of fifteen seconds.
RESULW
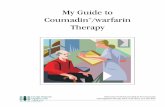
The pertinent information concerning the twenty-five patients studied is sumtnarized graphically in Figure 1. Analysis of the data revealed the following significant points :
Change.r in PTothrombin Time during L‘lrst l;ortj Hours: At 8 hours: The prothrombin time (PT) in eleven pa- tients was rising; one was in lower limits of thera- peutic range. .4t 76 hours: The PT in twenty-three patients was rising; two were now in therapeutic range ; thirteen were now in suboptimal range of 19 to. but not including, 22 seconds. dl 2.1 hours: The PT in all twenty-five patients was rising; twenty-one were now in therapeutic range; two patients were in suboptimal range. 20 and 9 seconds. respectively. ,4t .?? houn: The PT in twenty-four was now in therapeutic range; in one, no significant change in PT. though rising, was yet apparent. .4/ JO hours: The PT in all twenty-five was now in therapeutic range, including one who had not responded readily earlier. One patient showed a rapid spurt in PT from 25 seconds at 32 hours to 62 seconds at 40 hours when she was given 10 mg. K I.
t ISink-Shapiro modification using Simplastin.”
* From the Department of Medicine, St. Alexis Hospital, Cleveland, Ohio.
NOVEMBER 1960 933

934 Prothrombin Response to Coumadin
THROMBIN - 32-
- -
I-r-T-7r-r r- r ~7 1
0 16 32 46 64 60 96
HOURS POST-TREATMENT
FIG. 1. Summary of prothrombin responses in twenty-five cases.
Peak Level of Prothrombin Time: The time lag be- tween the oral administration of a single priming dose (75 mg.) of Coumadin and the attainment of maximum prothrombin time in each of twenty-five patients was as follows: At 76 hours, one patient (45 seconds); at 24 hours, one patient (30 seconds); at 32 hours, two patients (43 and 44 seconds); at 40 hours, eight patients (35, 30, 35, 32, 25, 30, 62, 38 seconds); at 48 hours, five patients (30, 29, 34, 28, 36 seconds); at 56 hours, six patients (26, 36, 38, 30, 29, 36 seconds); at 64 hours, two patients (80, 43 seconds).
Maximum prothrombin time was attained in 76 per cent of patients between 40 and 56 hours. In 16 per cent of patients this maximum was reached in from 16 to 32 hours and in 8 per cent of patients in 64 hours.
Time of Entry into Therapeutic Range: The time lag between the oral administration of a single loading dose (75 mg.) of Coumadin and the entry of each of twenty-five patients into therapeutic range (22 to 35 seconds) was as follows: 8 hours, one patient; 16 hours, one patient; 24 hours, nineteen patients; 32 hours, three patients; 40 hours, one patient.
Twenty-one patients or 84 per cent were in thera- peutic range at the end of the first 24 hours following the administration of the initial dose of Coumadin; 96 per cent at 32 hours and 100 per cent at 40 hours.
Duration of Therapeutic Range: The duration of range of therapeutic hypoprothrombinemia in each of twenty-five patients was as follows: 24 hours, one patient; 48 hours: two patients; 56 hours, one pa- tient; 64 hours, two patients; 72 hours, three pa- tients; 80 hours, fourteen patients; 88 hours, one patient; 95 hours, one patient.
In 82 per cent of patients the duration of thera- peutic range persisted for 48 to 88 hours; in 4 per cent for 24 hours and in another 4 per cent for 96 hours.
Persistence of Suboptimal Leuels: The finding of levels
of hypoprothrombinemia which, though elevated, are not within therapeutic range, i.e., suboptimal (19 to, but not including, 22 seconds) was noted in each of the twenty-five patients: At 76 hours, thirteen sub- optimal ; one in therapeutic range (4 per cent) ; eleven below suboptimal; at 24 hours, two subopti- mal; twenty-one in therapeutic range (84 per cent); two below suboptimal; at 32 hours, twenty-four in therapeutic range (96 per cent); one below sub- optimal; at 40, 48, 56 hours, all in therapeutic range; at 64 hours, one suboptimal; twenty-four in thera- peutic range (96 percent); at 72hours, twosuboptimal; twenty-three in therapeutic range (92 per cent); at 80 hours, two suboptimal; twenty-two in range (88 per cent); one below suboptimal; at 86: hours. four suboptimal; nineteen in range (76 per cent); two below suboptimal ; at 96 hours, five suboptimal ; eight- een in range (72 per cent); two below suboptimal.
Persistence of Excessiw Levels: Persistence of excessive levels of hypoprothrombinemia (i.e., over 35 seconds) was noted in seven cases (Table I).
It is well to note, however, that in five of the patients their highest prothrombin times were 45, 43, 44, 38 and 36 seconds, not excessively- high values. In the other two patients the highest levels were 80 and 62 seconds at which points vitamin Ki was administered with prompt reversal of Coumadin effect on prothrombin depression. In none of these seven patients was there any evidence of bleeding. A correlation between persistently high levels of hypopro- thrombinemia and bleeding incidents was not possible.
In order to analyze our data regarding the duration of a therapeutic hypoprothrombinemia more definitively, we took as our first figure the
THE AMERICAN JOURNAL OF CARDIOLOGY

Barker and Range1
TABLE *
Persistence of Excessive Prothrombin Time Levels at Hours after Initial Priming Dose of C:oumadin
035
Case 16 24 32 40 48 56 64 72 80 88 90
1 45 2 3 4 5 6 7
30 39 38 40 45 45 38 43 40 40 40 44 38
45 55 63 72 74 SO(K) 68 57 45 40 62 (K) SO 38 38
_ 36
(K) = Vitamin K, administered.
trst hour when the patient first exhibited thera- peutic hypoprothrombinemia and as our second figure the last time a therapeutic range showed plus eight hours (or from onset of therapeutic hypoprothrombinemia to first decline below the therapeutic range). In this manner we found that the duration of therapeutic hypopro- thrombinemia was 24 hours in one patient, 48 hours in two patients, 56 hours in one patient, 64 hours in two patients, 72 hours in three patients, 80 hours in fourteen patients, 88 hours in one patient and 96 hours in one patient. In nineteen, or 76 per cent of our patients, then, the therapeutic range lasted for three to four days once it had been attained. In the at- tainment of therapeutic hypoprothrombinemia and in the decline therefrom, our patients were none the less generally under the protective influence of Coumadin, as evidenced by sub- optimal prothrombin times.
One patient (Case 5, Table I) was given her initial dose of Coumadin for an acute myocardial infarction four days after she had underaone subtotal qastrectomy and gastrojejunostomy for peptic ulcer. The prothrombin test forty hours after the administration of the initial dose of Coutnadin was 62 seconds. There was no Ijleeding. The patient was given 10 mg. vitamin K1 intramuscularly. There was prompt and gradual recession of prothrombin time to 50, 38, 33 seconds for each of the next three suc- cessilre eight hour tests.
Another patient (Case 4, Table I) vomited shortly after she had swallowed her 75 mg. dose of Coumadin. Inadvertently, she was given another 75 mg. Coumadin sixteen hours after the first dose. A prothrombin time of 27 sec- onds at sixteen hours, i.e., the time of ad- ministration of the second 75 mg. dose, indi- cates probable complete and rapid absorption of the first dose. The prothrombin time of 80 >cconds (without bleeding) in the sixty-four
NOVEMBER 1960
hour test was followed by the intramuscular injection of 15 mg. vitamin K1, and the sub- sequent rapid and gradual recession of pro- thrombin time to 68, 57, 45, 40 seconds for each of the next four successive ei,qht hour tests.
COMMENTS
The results of this study indicate that the use of Coumadin provides early onset of therapeutic hypoprothrombinemia (84 per cent of our patients at twenty-four hours). Achievement of therapeutic hypoprothrotnbinemia (22 to 35 seconds) occurred in an additional 12 per cent at thirty-two hours, and in 4 per cent more at forty hours, so that 100 per cent of our pa- tients were in the therapeutic range at forty hours. Some degree of protective confer (sub- optimal range, 19 to 22 seconds, plus therapeutic range, 22 to 35 seconds or higher) was noted in ninety-two to one hundred of our patients frotn the twenty-four hour through the ninety-six hour test. The duration of the thc,rapeutic ranye persisted in eighty-two of our patients from forty-eight to eighty-eight after the iniGl1 loading dose.
In view of these findings, Coumadin is judged by us an excellent anticoagulant which provides maximal protective cover during the tnost critical period of disorders requiring effective anticoagulation, that is, the first ninety-six hours following their onset.
SUMMARY
The usefulness of an anticoagulant is predi- cated upon the speed of initiation of thera- peutic hypoprothrombinetnia and its duration. We have studied these two components of the response to the administration of a priming dose of Coumadin. Twenty-five patients, selected only as requiring anticoagulant therapy, were each given a single induction dose of 75 mg. Coumadin by mouth. Prothrombin time tests

936 Prothrombin Response to Coumadin
by the Link-Shapiro modification (using Sim- plastin) of the one stage method were made every eight hours for the first ninety-six hours follow- ing the administration of this dose to each patient, an initial test having been made before treatment with Coumadin was instituted.
By means of this eight hour testing, it was determined that within the first twenty-four hours following the administration of Coumadin, twenty-one patients entered the therapeutic range; three patients, eight hours later; and one patient at the forty hour test. The dura- tion of therapeutic hypoprothrombinemia was forty-eight to eighty-eight hours in twenty-three patients; twenty-four hours in one patient; and ninety-six hours in another. At the twenty- four through the ninety-six hour prothrombin time tests, the great majority of patients (72 to 100 per cent) were in the therapeutic range. There were two instances of excessively extended prothrombin time, without bleeding, which responded promptly to vitamin K1.
The predictability of action and desirable character of the response to the hypoprothrom- binemia-inducing effect of Coumadin are borne out by the objective analysis of the data.
REFERENCES
1. LINK, K. P. The Discovery of Dicoumarol and Its Sequels. Presented at the N. Y. Academy of Med., under the auspices of the Section on Medicine and
the N. Y. Heart Assn., on the Program, “The Historical and Physiological Aspects of Anti- coagulants.” Feb. 25. 1958.
2. SHAPIRO, s. Anticoagulant therapy. Clin. North .4merica, 36: 469, 1956.
3. BAER, S., YARROW, M. W., KRAVITZ, C., and MARKSON, V. Clinical experiences with warfarin (coumadin) sodium as an anticoagulant. .I.A.M.A., 167: 704, 1958.
4. FREMONT, R. E. and JAGENDORF, B. Clinical ob- servations on use of warfarin (coumadin) sodium; a new anticoagulant. J.A.M.A., 165: 1381, 1957.
5. NICHOLSON, J. H. Clinical experiences with anti- coagulants; a comparison of coumadin (warfarin) sodium and dicumarol (bishydroxy-coumarin). Angiolqy, 8 : 456, 1957.
6. NICHOLSON, J. H. and LEAVITT, T., JR. Coumadin (warfarin) sodium, a new anticoagulant. New England J. Med., 255: 491, 1956.
7. CLATANOFF, D. V., TRIGGS, P. 0. and MEYER, 0.0. Clinical experiences with warfarin and warfarin sodium. Arch. Znt. Med., 94: 213, 1954.
8. CLATANOFF, D. V. and MEYER, 0. 0. Further observations on use of warfarin sodium in anti- coagulant therapy. Arch. Int. Mtd., 97: 758, 1956.
9. PORTER, R. R., RICHARDSON, D., MAUCK, H. P., JR. Clinical experiences with the anticoagulant war- farin sodium (“coumadin sodium”). Vir,finia M. Month., 85: 465, 1958.
10. TAYLOR, F. E., CROCKETT, C. L., JR. and GLENDY, R. E. Experience with long-term anticoagulation. Virginia M. Month., 86: 630, 1959.
11. ATWOOD, W. H., JR. and MEYER, 0. 0. Manage- ment of patients receiving warfarin sodium (coumadin) therapy with prothrombin time de- terminations at 3-day intervals. Am. J. M. SC., 238: 6, 1959.
THE AMERICAN JOURNAL OF CARDIOLOGY