Effects of Prone Positioning on Lung Protection in … of prone positioning on lung protection in...
45
Effects of prone positioning on lung protection in patients with Acute Respiratory Distress Syndrome 1 Rodrigo A. Cornejo, 2 Juan C. Díaz, 1 Eduardo A. Tobar, 3 Alejandro R. Bruhn, 2 Cristobal A. Ramos, 1 Roberto A. González, 1 Claudia A. Repetto, 1 Carlos M. Romero, 1 Luis R. Gálvez, 1 Osvaldo Llanos 1 Daniel H. Arellano, 1 Wilson R. Neira, 1 Gonzalo A. Díaz, 1 Aníbal J. Zamorano, 2 Gonzalo L. Pereira. 1. Unidad de Pacientes Críticos, Departamento de Medicina, Hospital Clínico Universidad de Chile 2. Departamento de Radiología, Hospital Clínico Universidad de Chile 3. Departamento de Medicina Intensiva, Facultad de Medicina, Pontificia Universidad Católica de Chile Corresponding author: Rodrigo Cornejo MD, FACP. Associate Professor Universidad de Chile Address: Santos Dumont 999, Independencia, Santiago, Chile E-mail: [email protected] [email protected] Phone: +562 9788519 Mobile: +569 88399280 FAX: +562 7771373 Author's contributions to the study Authorship credit was based on: 1.1 Substantial contributions to conception and design: RC; 1.2 Acquisition of data: RC, JD, CR, RG, CR, DA, WN, GD, AZ, GP; 1.3 Analysis and interpretation of data: RC, ET, AB, CR, LG, OLl; 2 Drafting the article or revising it critically for important intellectual content: RC, JD, ET, AB, CR, RG, CR, CR, LG, OLl, DA, WN, GD, AZ, GP; 3 Final approval of the version to be published: RC, JD, ET, AB, CR, RG, CR, CR, LG, OLl, DA, WN, GD, AZ, GP Supported by FONDECYT Grant 11070156, Chile. Running head: Prone decreases instability and hyperinflation Subject Code: 4.08 Mechanical Ventilation: Physiology & Pathophysiology Scientific Knowledge on the Subject Experimental and clinical studies suggest that high levels of positive end-expiratory pressure (PEEP) and prone positioning may favor protective mechanical ventilation in patients with acute respiratory distress syndrome. High PEEP may induce lung recruitment and decrease cyclic recruitment/derecruitment; however, increasing PEEP may increase hyperinflation. Prone positioning could have synergistic effects with high PEEP by providing a more uniform recruitment and better distribution of lung stress. What This Study Adds to the Field In ARDS ventilated patients, prone positioning is able to enhance the effects of high PEEP in terms of lung recruitment and reduction of cyclic recruitment/derecruitment, while it prevents the negative impact of PEEP on tidal-hyperinflation Page 1 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
Transcript of Effects of Prone Positioning on Lung Protection in … of prone positioning on lung protection in...

Effects of prone positioning on lung protection in patients with Acute Respiratory
Distress Syndrome
1Rodrigo A. Cornejo,
2Juan C. Díaz,
1Eduardo A. Tobar,
3Alejandro R. Bruhn,
2Cristobal A. Ramos,
1Roberto A. González,
1Claudia A. Repetto,
1Carlos M. Romero,
1Luis R. Gálvez,
1Osvaldo Llanos
1Daniel H. Arellano,
1Wilson R. Neira,
1Gonzalo A.
Díaz, 1Aníbal J. Zamorano,
2Gonzalo L. Pereira.
1. Unidad de Pacientes Críticos, Departamento de Medicina, Hospital Clínico
Universidad de Chile
2. Departamento de Radiología, Hospital Clínico Universidad de Chile
3. Departamento de Medicina Intensiva, Facultad de Medicina, Pontificia Universidad
Católica de Chile
Corresponding author:
Rodrigo Cornejo MD, FACP. Associate Professor Universidad de Chile
Address: Santos Dumont 999, Independencia, Santiago, Chile
E-mail: [email protected] [email protected]
Phone: +562 9788519 Mobile: +569 88399280 FAX: +562 7771373
Author's contributions to the study
Authorship credit was based on: 1.1 Substantial contributions to conception and design:
RC; 1.2 Acquisition of data: RC, JD, CR, RG, CR, DA, WN, GD, AZ, GP; 1.3 Analysis
and interpretation of data: RC, ET, AB, CR, LG, OLl; 2 Drafting the article or revising
it critically for important intellectual content: RC, JD, ET, AB, CR, RG, CR, CR, LG,
OLl, DA, WN, GD, AZ, GP; 3 Final approval of the version to be published: RC, JD,
ET, AB, CR, RG, CR, CR, LG, OLl, DA, WN, GD, AZ, GP
Supported by FONDECYT Grant 11070156, Chile.
Running head: Prone decreases instability and hyperinflation
Subject Code: 4.08 Mechanical Ventilation: Physiology & Pathophysiology
Scientific Knowledge on the Subject
Experimental and clinical studies suggest that high levels of positive end-expiratory
pressure (PEEP) and prone positioning may favor protective mechanical ventilation in
patients with acute respiratory distress syndrome. High PEEP may induce lung
recruitment and decrease cyclic recruitment/derecruitment; however, increasing PEEP
may increase hyperinflation. Prone positioning could have synergistic effects with high
PEEP by providing a more uniform recruitment and better distribution of lung stress.
What This Study Adds to the Field
In ARDS ventilated patients, prone positioning is able to enhance the effects of high
PEEP in terms of lung recruitment and reduction of cyclic recruitment/derecruitment,
while it prevents the negative impact of PEEP on tidal-hyperinflation
Page 1 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

1
ABSTRACT
Rationale: Positive end-expiratory pressure (PEEP) and prone positioning may induce
lung recruitment and affect alveolar dynamics in acute respiratory distress syndrome
(ARDS). However, whether there is any interdependence between the effects of PEEP
and prone positioning on these variables is unknown.
Objectives: To determine the effects of high PEEP and prone positioning on lung
recruitment, cyclic recruitment/derecruitment and tidal-hyperinflation, and how these
effects are influenced by lung recruitability.
Methods: Mechanically ventilated patients (VT 6 ml/kg IBW) underwent whole-lung
computed tomography (CT) during breath-holding sessions at airway pressures of 5, 15,
and 45-cmH2O, and Cine-CTs on a fixed thoracic transverse slice at PEEP 5 and 15-
cmH2O. CT-images were repeated in supine and prone. A recruitment maneuver at 45-
cmH2O was performed before each PEEP change. Lung recruitability was defined as the
difference in percentage of non-aerated tissue between 5 and 45-cmH2O. Cyclic
recruitment/derecruitment and tidal-hyperinflation were determined as tidal changes in
percentage of non-aerated and hyperinflated tissue, respectively
Main Results: 24 ARDS patients were included. Increasing PEEP from 5 to 15-cmH2O
decreased non-aerated tissue (501±201 to 322±132grs, p<0.001) and increased tidal-
hyperinflation (0.41±0.26 to 0.57±0.30%, p=0.004) in supine. Prone positioning further
decreased non-aerated tissue (322±132 to 290±141grs, p=0.028), and reduced tidal-
hyperinflation observed at PEEP 15 in supine (0.57±0.30 to 0.41±0.22%). Cyclic
recruitment/derecruitment only decreased when high PEEP and prone were applied
together (4.1±1.9 to 2.9±0.9%, p=0.003), particularly in patients with high lung
recruitability.
Page 2 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

2
Conclusions: Prone positioning enhances lung recruitment and decreases alveolar
instability and hyperinflation observed at high PEEP in ARDS patients.
Page 3 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

3
INTRODUCTION:
Ventilator-induced lung injury (VILI) seems to play an important role in patients with
acute respiratory distress syndrome (ARDS) (1). The mechanisms by which mechanical
ventilation exerts its detrimental effect are not completely understood, but it appears
that hyperinflation of lung units and shear forces generated during cyclic
recruitment/derecruitment of unstable alveoli exacerbate, or even initiate lung injury (1).
High levels of positive end-expiratory pressure (PEEP) and prone positioning have
demonstrated to reduce VILI in experimental models of acute lung injury (ALI) (2-5).
However, analysis of several large clinical trials in ALI/ARDS patients suggests that
these interventions may be effective only in patients with severe ARDS (6-9).
Interestingly, patients who seem to benefit from prone positioning are frequently
subjected to higher levels of PEEP. Thus, there may be a potential interaction between
the effects of both interventions on the mechanisms of VILI.
Regarding VILI, PEEP may have a protective effect by favoring lung recruitment and
by reducing cyclic recruitment/derecruitment (1, 6), but other mechanisms, such as
redistribution of extravascular lung water, redistribution of pulmonary blood flow to
better aerated units or preservation of surfactant activity may also be involved.
However, PEEP may induce hyperinflation and increase the risk of VILI, especially in
patients with low recruitability or lobar ARDS (10-12). In fact, some patients exhibit
tidal-hyperinflation despite using low tidal volume and moderate PEEP levels according
to the ARDS-Net strategy (13, 14).
Prone positioning may influence mechanisms of VILI. By recruiting non-aerated tissue,
and by reducing the vertical pleural pressure gradient, prone positioning may provide a
Page 4 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

4
more uniform distribution of transpulmonary pressures during mechanical ventilation
(15-21). Therefore, prone positioning may act synergistically with high PEEP to protect
the lungs from VILI by enhancing lung recruitment and decreasing the risk of PEEP-
induced hyperinflation.
The objectives of this study were to determine the combined effects of high PEEP and
prone positioning on lung recruitment, cyclic recruitment/derecruitment and tidal-
hyperinflation, as assessed by static and dynamic computed tomography (CT) in ARDS
patients. In addition, we sought to determine whether these responses are influenced by
lung recruitability (22). Some of the results of this study have been previously reported
in the form of abstracts (23, 24).
Page 5 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

5
METHODS
Study Population
Twenty-four patients were studied in a university hospital. Institutional and
governmental ethical committees granted their approval. Informed consent was obtained
from the patients’ next of kin. Adult patients fulfilling ARDS criteria (25) and on
mechanical ventilation for 24-72 hours, who required lung CT scan for clinical
proposes, were enrolled. Patients younger than 18-years, pregnant, or for whom prone
positioning was contraindicated (26), were excluded.
Study protocol
Patients were evaluated in the ICU and CT-room (Figure 1). During the protocol they
were kept under deep sedation and neuromuscular paralysis, and ventilated in volume-
controlled mode with tidal volume (VT) of 6 ml/kg ideal body weight (IBW).
ICU assessments
Patients were ventilated with PEEP 5 and 15-cmH2O, for 20 minutes each, in supine
and prone (PEEP changes and positioning were applied in random order). Respiratory
mechanics, oxygenation and hemodynamic parameters were assessed at the end of each
setting. Before PEEP changes, a recruitment maneuver at 45-cmH20 airway pressure
was performed to standardize volume history. Quasi-static compliance of the respiratory
system (“compliance”) was calculated by dividing tidal volume by the difference
between plateau pressure and total PEEP.
CT assessments
Page 6 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

6
i) Patients underwent whole-lung CT during breath-holding sessions at three different
airway pressures: 45-cmH20 end-inspiratory airway pressure, and 5 and 15-cmH20
PEEP. CT scanning (Somaton Sensation®, Siemens, Germany) was performed under
the following protocol: Voltage 120 kVp, Current 200 mA, mAs 100, Rotation time 0.5
seconds, matrix 512x512. Lung compartments were defined according to their CT
density in hyperinflated (-901 to -1000 Hounsfield Units “HU”), well-aerated (-501 to -
900 HU), poorly-aerated (-101 to –500 HU), and non-aerated tissue (-100 to +100 HU)
(22). Lung weight for each compartment was calculated as: (1-[mean CT-number/-
1000]) x volume, where CT-number represents lung density (HU). Percentage of
potentially recruitable lung was defined as ([non-aerated tissue at 5-cmH2O - non-
aerated tissue at 45-cmH2O]/total weight) and high lung recruitability as a percentage of
potentially recruitable lung >13.9% in supine, which corresponds to the median value
observed in 49 ARDS patients in a previous study of lung recruitability (22).
Contiguous axial sections 5-mm thick were reconstructed from the volumetric data
using high definition filter.
ii) A 2.4 mm-thick supra-diaphragmatic CT slice was selected for dynamic-CT.
Respiratory rate was transiently decreased to 10/min during dynamic-CT capture. Cine-
CTs of 12 seconds were performed under the following protocol: Voltage 100 kVp,
Current 80 mA, mAs 40; 0.5 seconds-24 images; matrix 512x512. Lung compartments
were expressed as percentage of tissue weight in the transverse slice. Cyclic
recruitment/derecruitment and tidal-hyperinflation were determined as tidal changes in
percentage of non-aerated and hyperinflated tissue respectively.
Page 7 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

7
CT-images were repeated in supine and prone, and the sequence of positions and PEEP
levels was applied in random order. Images were analyzed manually by radiologists
using Pulmo® (Siemens, Germany) and MALUNA® (University of Gottingen,
Germany) software. (See additional METHODS in the online supplement).
Statistical analysis
Results are expressed as mean (±SD) or median (interquartile range). The effect of
PEEP level and position was assessed by applying a two-way analysis of variance for
repeated measurements with Sidak’s post-hoc analysis. Comparisons between patients
with low and high lung recruitability were performed with Student's t-test or Wilcoxon-
Mann-Whitney test. SPSS 20.0 software (Chicago, USA) was used for statistical
calculations. Two-sided p<0.05 was considered statistically significant.
Page 8 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

8
RESULTS:
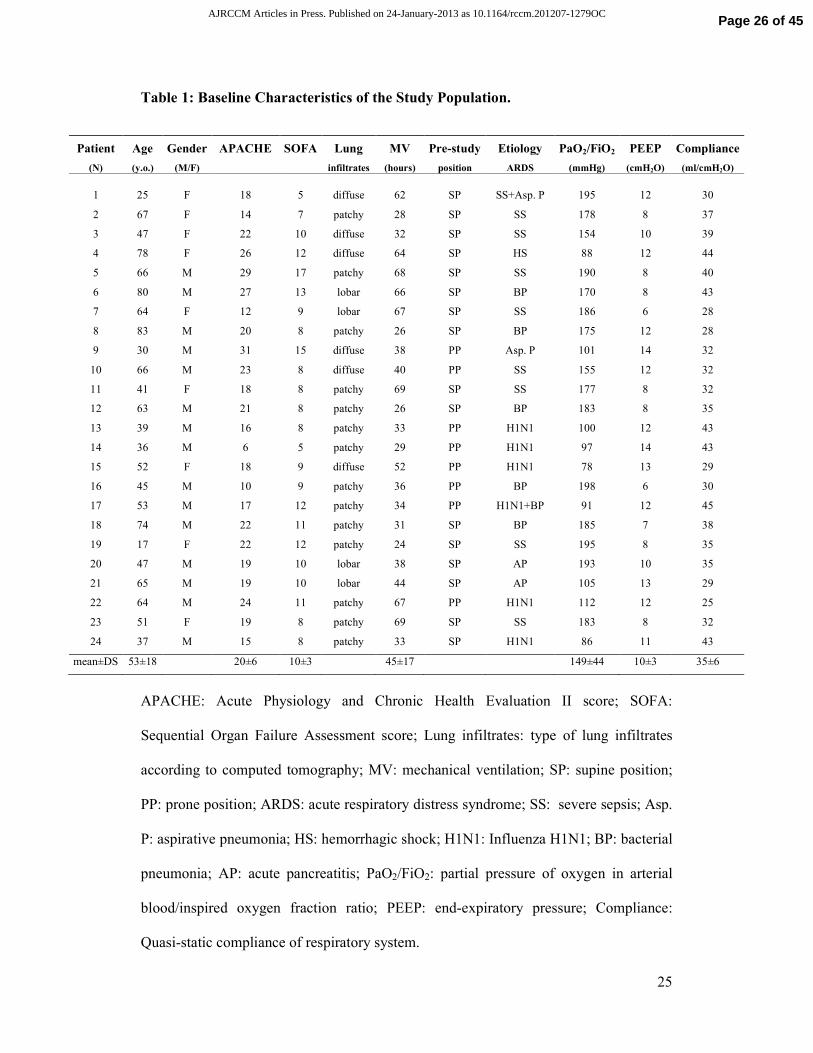
We included 24 patients (15 male, age 54±18 years) with ARDS. Fourteen patients
presented patchy, six diffuse, and four had lobar CT attenuations. Baseline
characteristics are presented in Table 1.
Prone positioning had no significant effect on gas exchange or compliance, when
compared to supine position at PEEP 5 (Table 2). However, it induced a decrease in
non-aerated tissue and an increase in well-aerated tissue (Table 3).
Increasing PEEP from 5 to 15-cmH2O increased oxygenation and compliance (Table
2), decreased non-aerated tissue, and increased well-aerated tissue (Table 3). However,
it markedly increased hyperinflation. These effects were observed both at supine and
prone positioning. Nevertheless, compared to supine, at prone positioning oxygenation
and compliance tended to be higher at PEEP 15, while non-aerated tissue and
hyperinflation were lower (Table 3 and Figure 2).
The effects of prone positioning and PEEP level on determinants of VILI, namely cyclic
recruitment/derecruitment and tidal-hyperinflation, are shown in Figure 3. Compared to
supine position at PEEP 5, neither prone positioning nor increasing PEEP had a
significant effect on cyclic recruitment/derecruitment. However, both strategies applied
together (prone positioning at PEEP 15) significantly decreased cyclic
recruitment/derecruitment (4.1±1.9 to 2.9±0.9%, p=0.003). Tidal hyperinflation was not
affected by prone positioning at PEEP 5, but it increased in response to PEEP 15 in
supine position (0.41±0.26 to 0.57±0.30%, p=0.004). Noteworthy, PEEP induced tidal-
Page 9 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
9
hyperinflation observed in supine was markedly decreased by prone positioning
(0.57±0.30 to 0.41±0.22%, p=0.01).
Potentially recruitable lung was 18.3±11% in supine and 14.9±8% in prone (p=0.036).
Figure 4 shows CT-images from representative patients obtained at airway pressures of
5 and 45-cmH20, in supine and prone positioning. According to our predefined
threshold, fourteen patients presented high lung recruitability.
Increasing PEEP to 15-cmH2O improved oxygenation and compliance only in patients
with high lung recruitability. This subgroup exhibited a 48% relative decrease in non-
aerated tissue when increasing PEEP, while this effect was only 22% in patients with
low lung recruitability (Table 4). In contrast to patients with high lung recruitability,
who showed no additional effect of prone positioning on non-aerated tissue at PEEP 15,
patients with low lung recruitability exhibited a significant decrease in non-aerated
tissue when subjected to prone positioning (20% additional relative decrease).
Cyclic recruitment/derecruitment was significantly lower at baseline in patients with
low lung recruitability (2.8±1.3% vs 5.1±1.8% in patients with high lung recruitability,
p=0.002), and neither increasing PEEP nor prone positioning had any significant effect
on this variable in the former subgroup (Figure 3). In contrast, cyclic
recruitment/derecruitment decreased in patients with high lung recruitability when
increasing PEEP to 15-cmH2O, and a significant additional effect was obtained after
prone positioning at the same PEEP level. Regarding tidal hyperinflation, patients with
low and high lung recruitability had similar values at baseline (0.39±0.25% versus
Page 10 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

10
0.45±0.24, p=0.568). The effect of high PEEP level on increasing tidal hyperinflation
was prevented by prone positioning in both subgroups of lung recruitability.
Page 11 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

11
DISCUSSION:
The main finding of the present study is that prone positioning enhances the effects of
high PEEP on lung recruitment and cyclic recruitment/derecruitment, while it prevents
the effects of high PEEP on tidal-hyperinflation. In addition, we found that lung
recruitability, assessed by CT at high airway pressures (22), does not predict lung
recruitment induced by prone positioning.
Effects of prone positioning
Although it has been reported that oxygenation improves after proning (7-9), we only
found a trend, which did not reach statistical significance. This may be explained by the
short sampling period. Data obtained from different series of prolonged prone
positioning in ARDS patients found that oxygenation improves several hours after
turning them into prone (26-30). Other possible explanation is that oxygenation
variation and lung recruitment may be dissociated, because “anatomical” lung
recruitment may differ from “functional” recruitment (22).
We observed that prone positioning was an effective recruitment strategy that, in
contrast to high PEEP, did not increase either hyperinflated tissue or plateau pressures.
This effect may be explained in part by the suppression of the compressive force of the
heart on dorsal lung regions obtained in prone (31, 32). Interestingly, patients with
predominantly basal consolidations, such as patients A and B from Figure 4, were those
who experienced higher recruitment induced by prone (data not shown), which is in line
with the findings of Galiatsu et al. (15). These observations may complement the
Page 12 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

12
concept by Rouby et al. about lung morphology as a predictor of the response to
increasing airway pressures (33), although this requires confirmation by further studies.
Noteworthy, in patients with low potentially recruitable lung prone positioning was able
to recruit a significant amount of non-aerated tissue, in addition to that already recruited
by high PEEP (Table 4). Therefore, the assessment of potentially recruitable lung
between 5 to 45 cmH2O may correctly predict lung recruitability to increasing airway
pressures, but not the response to prone. Thus, prone positioning may be considered in
severe ARDS patients, even if they have poor response to recruitment maneuvers in
supine position, as assessed by CT.
Effects of positive end-expiratory pressure
Although increasing PEEP from 5 to 15-cmH2O decreased non-aerated tissue and
increased oxygenation, it had no consistent effect on cyclic recruitment/derecruitment in
the overall population. However, in the subgroup of patients with higher lung
recruitability cyclic recruitment/derecruitment significantly decreased when increasing
PEEP to 15-cmH2O (Figure 3). Similar findings were reported in a recent study in
which cyclic recruitment/derecruitment was assessed indirectly with static CT images
(34).
As expected, in supine position high PEEP resulted in higher plateau pressures,
hyperinflated tissue, and tidal-hyperinflation. Hyperinflation is a morphologic
description of the lung areas that appear overfilled with gas in CT images, and it has
been associated to VILI (14). The low values of tidal-hyperinflation may seem
irrelevant (lower than 1%). However, fractional analysis of CT data was based on lung
Page 13 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

13
weight instead of volume, so the magnitude of real hyperinflated tissue may have been
systematically underestimated (35, 36). We used weight for fractional analysis in
dynamic-CT, because total volume is changing throughout the respiratory cycle. If the
results were expressed as percentage of volume, tidal-hyperinflation would have been
ten times greater (4-6%). PEEP-induced tidal-hyperinflation could be an important
drawback of high PEEP strategies (14), which may explain the lack of consistency in
results of recent clinical trials (6).
The fact that high PEEP levels could favor hyperinflation, without a consistent decrease
in cyclic recruitment/derecruitment, supports the notion that PEEP should be titrated
individually based not only on oxygen exchange, but considering other variables such as
lung recruitability.
Interaction of prone positioning with positive end-expiratory pressure
Few studies have addressed the issue of potential interactions between prone positioning
and PEEP (37, 38). In the present study, we found that prone positioning has a
synergistic effect with high PEEP in increasing respiratory system compliance, likely
because of an increase in well-aerated lung tissue. Previous studies have shown
contradictory data about the effects of prone positioning on respiratory system
compliance (39). These discrepancies may be due to differences in chest wall
compliance and lung recruitability of the study groups.
Prone positioning as well as high PEEP induced lung recruitment, resulting its
combination in the least amount of non-aerated tissue. Prone positioning also reinforced
the effect of high PEEP on cyclic recruitment/derecruitment, especially in patients with
Page 14 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

14
higher lung recruitability. This interaction did not seem to be a simple additive effect
because in the whole population, neither prone at low PEEP, nor high PEEP on supine,
decreased cyclic recruitment/derecruitment. Thus, prone positioning and high PEEP
together showed a synergistic effect on cyclic recruitment/derecruitment.
Prone positioning prevented the increase in hyperinflated tissue and in tidal-
hyperinflation induced by high PEEP levels in supine. Likewise, the increase in plateau
pressures induced by high PEEP was lower in prone. These findings may be related to
the effects of prone positioning in decreasing pleural pressure gradients and
homogenizing transpulmonary pressures in the ARDS lungs (15, 16, 18, 20). A regional
analysis of CT images, as performed by Grasso et al (40), would be a valuable
complement to the present study in order to assess the effects of prone positioning on
inhomogeneity and recruitment of individual lung regions.
The results of the present study suggest that a high PEEP strategy applied in prone
positioning, instead of supine, could have more benefitial and less adverse effects in
terms of respiratory mechanics and determinants of VILI. These findings are consistent
with the observations of metaanalysis, which indicate that patients with severe forms of
ARDS, who are usually ventilated with high levels of PEEP, may have a survival
benefit when treated in prone positioning (7-9).
Recruitment and cyclic recruitment/derecruitment: Methodological issues
Computed tomography has been the gold standard to assess lung recruitment, although
different definitions have been applied (10, 41). We chose the original definition of
recruitment based on the decrease of non-aerated tissue expressed in lung weight, as we
Page 15 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

15
have already used in the past (22, 42), and because it may be applied to analyze cyclic
recruitment/derecruitment in dynamic-CT. Other authors have defined recruitment as
the reaeration of the nonaerated and poorly aerated compartment (10). As we applied a
definition limited to the nonaerated compartment we acknowledge that our results for
PEEP-induced recruitment may appear as subestimated compared to studies which
include the poorly aerated compartment, as shown in a recent study using transthoracic
ultrasound (43).
The threshold of 13.9% used in the present study to classify patients as having high or
low lung recruitability in supine position was predefined arbitrarily based on the median
value of the subgroup of 49 ARDS patients from Gattinoni’s study. The original lung
recruitability threshold of Gattinoni’s study was 9%, which corresponded to the median
value of the whole ALI/ARDS population (68 patients). We are aware that by applying
a different threshold our subgroups of higher and lower lung recruitability are not
comparable to the subgroups defined in the original study of Gattinoni (22).
There is controversy whether cyclic recruitment/derecruitment, as assessed by CT,
corresponds really to intra-tidal opening and closing of lung units, or whether it
corresponds to flooded alveoli that become partially inflated during inspiration (44, 45).
Whatever the underlying phenomenon (cyclic mechanical deformation, or cyclic
recruitment/derecruitment of lung units), a reduction of instability produced by prone
positioning at high PEEP, as supported by our study, appears as theoretically positive in
terms of lung protection.
Page 16 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

16
Several approaches to assess cyclic phenomena have been used (46). A cine-CT
analysis of a fixed transverse slice allows dynamic imaging without mechanical
ventilation interruption. This method has been recently validated by experimental and
clinical studies to determine cyclic recruitment/derecruitment, tidal hyperinflation and
dynamic lung strain (18, 35, 36, 47, 48). The main limitations of this method are: a) the
more inhomogeneous the lung impairment, the less representative the slice may be (this
handicap is particularly true in patients with lobar pattern, but only four of our patients
had such pattern); b) it is impossible for dynamic-CT to scan exactly the same
anatomical structure in different settings, although the careful definition of anatomical
landmarks and fractional analysis used for dynamic-CT may avoid artifacts created by
the cranio-caudal motion, and c) the absolute amount of grams of lung tissue
undergoing either recruitment/derecruitment or tidal-hyperinflation cannot be
determined. The alternative approach of using static CT images of the whole lung after
end-expiratory and end-inspiratory breath holds (15, 16, 18-20, 22, 34) also has several
limitations, being the time dependency of the recruitment and derecruitment phenomena
the most important (49, 50). Despite limitations of both methods, a previous study
comparing them showed no major differences (48).
In conclusion, prone positioning induces lung recruitment even in patients classified as
having low potential for lung recruitment. In addition, prone positioning applied
together with high PEEP levels in ARDS patients act synergistically to decrease
mechanical determinants of VILI such as cyclic recruitment/derecruitment and tidal-
hyperinflation.
ACKNOWLEDGMENTS
Page 17 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

17
We thank Dr. Jerónimo Graf, Dr. Gastón Murias and Dr. Guillermo Bugedo for their
critical comments and suggestions for the manuscript, as well as the nurses, respiratory
therapists, medical staff and medical technologists from Hospital Clínico Universidad
de Chile for their precious support during the execution of the studies. We acknowledge
the role of Dr. Hector Gatica, for the statistical advice in the present article. We are
indebted to Daniel Castro, medical biophysics and radiation protection officer, who
assessed and adjusted the level of radiation per CT, allowing that the total dose per
patient did not exceed the equivalent of 1 coronary CT Angiography study.
Page 18 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

18
References
1. Dos Santos CC, Slutsky AS. Invited review: Mechanisms of ventilator-induced
lung injury: A perspective. J Appl Physiol 2000;89:1645-1655.
2. Argiras EP, Blakeley CR, Dunnill MS, Otremski S, Sykes MK. High peep
decreases hyaline membrane formation in surfactant deficient lungs. Br J Anaesth
1987;59:1278-1285.
3. Broccard A, Shapiro RS, Schmitz LL, Adams AB, Nahum A, Marini JJ. Prone
positioning attenuates and redistributes ventilator-induced lung injury in dogs. Crit Care
Med 2000;28:295-303.
4. Dreyfuss D, Soler P, Basset G, Saumon G. High inflation pressure pulmonary
edema. Respective effects of high airway pressure, high tidal volume, and positive end-
expiratory pressure. Am Rev Respir Dis 1988;137:1159-1164.
5. Webb HH, Tierney DF. Experimental pulmonary edema due to intermittent
positive pressure ventilation with high inflation pressures. Protection by positive end-
expiratory pressure. Am Rev Respir Dis 1974;110:556-565.
6. Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, Slutsky AS,
Pullenayegum E, Zhou Q, Cook D, et al. Higher vs lower positive end-expiratory
pressure in patients with acute lung injury and acute respiratory distress syndrome:
Systematic review and meta-analysis. JAMA 2010;303:865-873.
7. Sud S, Friedrich JO, Taccone P, Polli F, Adhikari NK, Latini R, Pesenti A,
Guerin C, Mancebo J, Curley MA, et al. Prone ventilation reduces mortality in patients
with acute respiratory failure and severe hypoxemia: Systematic review and meta-
analysis. Intensive Care Med 2010;36:585-599.
Page 19 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

19
8. Gattinoni L, Carlesso E, Taccone P, Polli F, Guerin C, Mancebo J. Prone
positioning improves survival in severe ards: A pathophysiologic review and individual
patient meta-analysis. Minerva Anestesiol 2010;76:448-454.
9. Abroug F, Ouanes-Besbes L, Dachraoui F, Ouanes I, Brochard L. An updated
study-level meta-analysis of randomised controlled trials on proning in ards and acute
lung injury. Crit Care 2011;15:R6.
10. Malbouisson LM, Muller JC, Constantin JM, Lu Q, Puybasset L, Rouby JJ.
Computed tomography assessment of positive end-expiratory pressure-induced alveolar
recruitment in patients with acute respiratory distress syndrome. Am J Respir Crit Care
Med 2001;163:1444-1450.
11. Nieszkowska A, Lu Q, Vieira S, Elman M, Fetita C, Rouby JJ. Incidence and
regional distribution of lung overinflation during mechanical ventilation with positive
end-expiratory pressure. Crit Care Med 2004;32:1496-1503.
12. Rouby JJ. Lung overinflation. The hidden face of alveolar recruitment.
Anesthesiology 2003;99:2-4.
13. Grasso S, Terragni P, Mascia L, Fanelli V, Quintel M, Herrmann P,
Hedenstierna G, Slutsky AS, Ranieri VM. Airway pressure-time curve profile (stress
index) detects tidal recruitment/hyperinflation in experimental acute lung injury. Crit
Care Med 2004;32:1018-1027.
14. Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, Gandini G,
Herrmann P, Mascia L, Quintel M, et al. Tidal hyperinflation during low tidal volume
ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med
2007;175:160-166.
Page 20 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

20
15. Galiatsou E, Kostanti E, Svarna E, Kitsakos A, Koulouras V, Efremidis SC,
Nakos G. Prone position augments recruitment and prevents alveolar overinflation in
acute lung injury. Am J Respir Crit Care Med 2006;174:187-197.
16. Mentzelopoulos SD, Roussos C, Zakynthinos SG. Prone position reduces lung
stress and strain in severe acute respiratory distress syndrome. Eur Respir J
2005;25:534-544.
17. Mure M, Domino KB, Lindahl SG, Hlastala MP, Altemeier WA, Glenny RW.
Regional ventilation-perfusion distribution is more uniform in the prone position. J Appl
Physiol 2000;88:1076-1083.
18. Perchiazzi G, Rylander C, Vena A, Derosa S, Polieri D, Fiore T, Giuliani R,
Hedenstierna G. Lung regional stress and strain as a function of posture and ventilatory
mode. J Appl Physiol 2011;110:1374-1383.
19. Richter T, Bellani G, Scott Harris R, Vidal Melo MF, Winkler T, Venegas JG,
Musch G. Effect of prone position on regional shunt, aeration, and perfusion in
experimental acute lung injury. Am J Respir Crit Care Med 2005;172:480-487.
20. Valenza F, Guglielmi M, Maffioletti M, Tedesco C, Maccagni P, Fossali T,
Aletti G, Porro GA, Irace M, Carlesso E, et al. Prone position delays the progression of
ventilator-induced lung injury in rats: Does lung strain distribution play a role? Crit
Care Med 2005;33:361-367.
21. Wiener CM, Kirk W, Albert RK. Prone position reverses gravitational
distribution of perfusion in dog lungs with oleic acid-induced injury. J Appl Physiol
1990;68:1386-1392.
22. Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M,
Russo S, Patroniti N, Cornejo R, Bugedo G. Lung recruitment in patients with the acute
respiratory distress syndrome. N Engl J Med 2006;354:1775-1786.
Page 21 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

21
23. Cornejo R, Diaz J, Repetto C, Suarez P, Bozan F, Arellano D, Rouliez K, Diaz
G, Romero C, Mezzano E, et al. Comparison of potentially recruitable lung (prl) in
supine versus prone position. Preliminary data. [abstract]. Intensive Care Med
2009;35:S126.
24. Cornejo R, Diaz J, Repetto C, Suarez P, Bozan F, Neira W, Zamorano A, Tobar
E, Castro D, Monsalve J, et al. Effect of prone position and peep on cyclic recruitment-
derecruitment (r/d), and tidal hyperinflation (th) using cine-ct. Preliminary data.
[abstract]. Intensive Care Med 2009;35:S103.
25. Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M,
Legall JR, Morris A, Spragg R. The american-european consensus conference on ards.
Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J
Respir Crit Care Med 1994;149:818-824.
26. Romero CM, Cornejo RA, Galvez LR, Llanos OP, Tobar EA, Berasain MA,
Arellano DH, Larrondo JF, Castro JS. Extended prone position ventilation in severe
acute respiratory distress syndrome: A pilot feasibility study. J Crit Care 2009;24:81-
88.
27. Chan MC, Hsu JY, Liu HH, Lee YL, Pong SC, Chang LY, Kuo BI, Wu CL.
Effects of prone position on inflammatory markers in patients with ards due to
community-acquired pneumonia. J Formos Med Assoc 2007;106:708-716.
28. Charron C, Bouferrache K, Caille V, Castro S, Aegerter P, Page B, Jardin F,
Vieillard-Baron A. Routine prone positioning in patients with severe ards: Feasibility
and impact on prognosis. Intensive Care Med 2011;37:785-790.
29. Cornejo R, Tobar E, Diaz G, Romero C, Llanos O, Galvez LR, Zamorano A,
Fabrega L, Neira W, Arellano D, et al. Systematic approach for severe respiratory
failure due to novel a (h1n1) influenza. Minerva Anestesiol 2011;77:510-521.
Page 22 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

22
30. Mancebo J, Fernandez R, Blanch L, Rialp G, Gordo F, Ferrer M, Rodriguez F,
Garro P, Ricart P, Vallverdu I, et al. A multicenter trial of prolonged prone ventilation
in severe acute respiratory distress syndrome. Am J Respir Crit Care Med
2006;173:1233-1239.
31. Malbouisson LM, Busch CJ, Puybasset L, Lu Q, Cluzel P, Rouby JJ. Role of the
heart in the loss of aeration characterizing lower lobes in acute respiratory distress
syndrome. Ct scan ards study group. Am J Respir Crit Care Med 2000;161:2005-2012.
32. Albert RK, Hubmayr RD. The prone position eliminates compression of the
lungs by the heart. Am J Respir Crit Care Med 2000;161:1660-1665.
33. Puybasset L, Cluzel P, Gusman P, Grenier P, Preteux F, Rouby JJ. Regional
distribution of gas and tissue in acute respiratory distress syndrome. I. Consequences for
lung morphology. Ct scan ards study group. Intensive Care Med 2000;26:857-869.
34. Caironi P, Cressoni M, Chiumello D, Ranieri M, Quintel M, Russo SG, Cornejo
R, Bugedo G, Carlesso E, Russo R, et al. Lung opening and closing during ventilation
of acute respiratory distress syndrome. Am J Respir Crit Care Med 2010;181:578-586.
35. Bruhn A, Bugedo D, Riquelme F, Varas J, Retamal J, Besa C, Cabrera C,
Bugedo G. Tidal volume is a major determinant of cyclic recruitment-derecruitment in
acute respiratory distress syndrome. Minerva Anestesiol 2011;77:418-426.
36. David M, Karmrodt J, Bletz C, David S, Herweling A, Kauczor HU, Markstaller
K. Analysis of atelectasis, ventilated, and hyperinflated lung during mechanical
ventilation by dynamic ct. Chest 2005;128:3757-3770.
37. Gainnier M, Michelet P, Thirion X, Arnal JM, Sainty JM, Papazian L. Prone
position and positive end-expiratory pressure in acute respiratory distress syndrome.
Crit Care Med 2003;31:2719-2726.
Page 23 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

23
38. Walther SM, Johansson MJ, Flatebo T, Nicolaysen A, Nicolaysen G. Marked
differences between prone and supine sheep in effect of peep on perfusion distribution
in zone ii lung. J Appl Physiol 2005;99:909-914.
39. Pelosi P, Brazzi L, Gattinoni L. Prone position in acute respiratory distress
syndrome. Eur Respir J 2002;20:1017-1028.
40. Grasso S, Stripoli T, Sacchi M, Trerotoli P, Staffieri F, Franchini D, De Monte
V, Valentini V, Pugliese P, Crovace A, et al. Inhomogeneity of lung parenchyma during
the open lung strategy: A computed tomography scan study. Am J Respir Crit Care Med
2009;180:415-423.
41. Gattinoni L, Pelosi P, Crotti S, Valenza F. Effects of positive end-expiratory
pressure on regional distribution of tidal volume and recruitment in adult respiratory
distress syndrome. Am J Respir Crit Care Med 1995;151:1807-1814.
42. Bugedo G, Bruhn A, Hernandez G, Rojas G, Varela C, Tapia JC, Castillo L.
Lung computed tomography during a lung recruitment maneuver in patients with acute
lung injury. Intensive Care Med 2003;29:218-225.
43. Bouhemad B, Brisson H, Le-Guen M, Arbelot C, Lu Q, Rouby JJ. Bedside
ultrasound assessment of positive end-expiratory pressure-induced lung recruitment. Am
J Respir Crit Care Med 2011;183:341-347.
44. Hubmayr RD. Perspective on lung injury and recruitment: A skeptical look at
the opening and collapse story. Am J Respir Crit Care Med 2002;165:1647-1653.
45. Tschumperlin DJ, Oswari J, Margulies AS. Deformation-induced injury of
alveolar epithelial cells. Effect of frequency, duration, and amplitude. Am J Respir Crit
Care Med 2000;162:357-362.
46. Ghadiali S, Huang Y. Role of airway recruitment and derecruitment in lung
injury. Crit Rev Biomed Eng 2011;39:297-317.
Page 24 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
24
47. Doebrich M, Markstaller K, Karmrodt J, Kauczor HU, Eberle B, Weiler N,
Thelen M, Schreiber WG. Analysis of discrete and continuous distributions of
ventilatory time constants from dynamic computed tomography. Phys Med Biol
2005;50:1659-1673.
48. Zinserling J, Wrigge H, Neumann P, Muders T, Magnusson A, Hedenstierna G,
Putensen C. Methodologic aspects of attenuation distributions from static and dynamic
thoracic ct techniques in experimental acute lung injury. Chest 2005;128:2963-2970.
49. Albert SP, DiRocco J, Allen GB, Bates JH, Lafollette R, Kubiak BD, Fischer J,
Maroney S, Nieman GF. The role of time and pressure on alveolar recruitment. J Appl
Physiol 2009;106:757-765.
50. Massa CB, Allen GB, Bates JH. Modeling the dynamics of recruitment and
derecruitment in mice with acute lung injury. J Appl Physiol 2008;105:1813-1821.
Page 25 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
25
Table 1: Baseline Characteristics of the Study Population.
Patient Age Gender APACHE SOFA Lung MV Pre-study Etiology PaO2/FiO2 PEEP Compliance
(N) (y.o.) (M/F) infiltrates (hours) position ARDS (mmHg) (cmH2O) (ml/cmH2O)
1 25 F 18 5 diffuse 62 SP SS+Asp. P 195 12 30
2 67 F 14 7 patchy 28 SP SS 178 8 37
3 47 F 22 10 diffuse 32 SP SS 154 10 39
4 78 F 26 12 diffuse 64 SP HS 88 12 44
5 66 M 29 17 patchy 68 SP SS 190 8 40
6 80 M 27 13 lobar 66 SP BP 170 8 43
7 64 F 12 9 lobar 67 SP SS 186 6 28
8 83 M 20 8 patchy 26 SP BP 175 12 28
9 30 M 31 15 diffuse 38 PP Asp. P 101 14 32
10 66 M 23 8 diffuse 40 PP SS 155 12 32
11 41 F 18 8 patchy 69 SP SS 177 8 32
12 63 M 21 8 patchy 26 SP BP 183 8 35
13 39 M 16 8 patchy 33 PP H1N1 100 12 43
14 36 M 6 5 patchy 29 PP H1N1 97 14 43
15 52 F 18 9 diffuse 52 PP H1N1 78 13 29
16 45 M 10 9 patchy 36 PP BP 198 6 30
17 53 M 17 12 patchy 34 PP H1N1+BP 91 12 45
18 74 M 22 11 patchy 31 SP BP 185 7 38
19 17 F 22 12 patchy 24 SP SS 195 8 35
20 47 M 19 10 lobar 38 SP AP 193 10 35
21 65 M 19 10 lobar 44 SP AP 105 13 29
22 64 M 24 11 patchy 67 PP H1N1 112 12 25
23 51 F 19 8 patchy 69 SP SS 183 8 32
24 37 M 15 8 patchy 33 SP H1N1 86 11 43
mean±DS 53±18 20±6 10±3 45±17 149±44 10±3 35±6
APACHE: Acute Physiology and Chronic Health Evaluation II score; SOFA:
Sequential Organ Failure Assessment score; Lung infiltrates: type of lung infiltrates
according to computed tomography; MV: mechanical ventilation; SP: supine position;
PP: prone position; ARDS: acute respiratory distress syndrome; SS: severe sepsis; Asp.
P: aspirative pneumonia; HS: hemorrhagic shock; H1N1: Influenza H1N1; BP: bacterial
pneumonia; AP: acute pancreatitis; PaO2/FiO2: partial pressure of oxygen in arterial
blood/inspired oxygen fraction ratio; PEEP: end-expiratory pressure; Compliance:
Quasi-static compliance of respiratory system.
Page 26 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

26
Table 2: Effects of PEEP levels and prone position on respiratory variables
SUPINE 5 SUPINE 15 PRONE 5 PRONE 15
PaO2:FiO2 [mmHg] 143 ± 58 235 ± 68* 170 ± 71 259 ± 63†
PaO2 [mmHg] 90 ± 34 155 ± 73* 114 ± 68 175 ± 79†
PaCO2 [mmHg] 47 ± 7 46 ± 8 46 ± 6 46 ± 7
Compliance [ml/cmH2O] 34 ± 6 40 ± 9* 35 ± 8 44 ± 10†‡
plateau pressure [cmH2O] 18 ± 3 27 ± 3* 18 ± 2 26 ± 2†‡
driving pressure [cmH2O] 13 ± 3 12 ± 3 13 ± 2 11 ± 2†‡
PaO2:FiO2: partial pressure of oxygen in arterial blood/inspired oxygen fraction ratio;
PEEP 5: Positive end-expiratory pressure 5 cmH2O; PEEP 15: Positive end-expiratory
pressure 15 cmH2O; PaCO2: partial pressure of carbon dioxide; Compliance:
compliance of the respiratory system; Driving pressure: difference between plateau
pressure and positive end-expiratory pressure; ∆: delta between parameters at PEEP 15
and PEEP 5 cmH2O
*P<0.05, between parameters at supine 5 and supine 15 cmH2O
†P<0.05, between parameters at prone 5 and prone 15 cmH2O
‡ P<0.05, between parameters at supine 15 and prone 15 cmH2O
Page 27 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

27
Table 3: Effects of PEEP levels and prone position on lung compartment
distribution
SUPINE 5 SUPINE 15 PRONE 5 PRONE 15
total lung volume [ml] 2140 ± 643 3271 ± 900 2240 ± 614 3268 ± 821
total lung weight [g] 1201 ± 307 1282 ± 316 1216 ± 341 1261 ± 321
volume of non-aerated compartment [ml] 503 ± 201 324 ± 133* 431 ± 193‡ 291 ± 143†§
weight of non-aerated tissue [g] 501 ± 201 322 ± 132* 431 ± 192‡ 290 ± 141†§
volume of poorly-aerated compartment [ml] 623 ± 210 753 ± 314 657 ± 207 724 ± 289
weight of poorly-aerated tissue [g] 446 ± 149 517 ± 216 467 ± 157 497 ± 203
volume of well-aerated compartment [ml] 872 ± 406 1767 ± 661* 1027 ± 456‡ 1893 ± 617†
weight of well-aerated tissue [g] 254 ± 103 485 ± 148* 324 ± 148‡ 535 ± 152†
volume of hyperinflated compartment [ml] 144 ± 160 434 ± 318* 125 ± 105 362 ± 220†§
weight of hyperinflated tissue [g] 5,6 ± 6 19 ± 15* 4,4 ± 4 14 ± 8†
*P<0.05, between parameters at supine 5 and supine 15 cmH2O
†P<0.05, between parameters at prone 5 and prone 15 cmH2O
‡ P<0.05, between parameters at supine 5 and prone 5 cmH2O
§ P<0.05, between parameters at supine 15 and prone 15 cmH2O
Page 28 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

28
Table 4: Comparisons between Patients with High and Low Lung Recruitability
High Lung Recruitability Low Lung Recruitability
SUPINE PRONE SUPINE PRONE
PaO2/FiO2 at PEEP 5 [mmHg] 128±61 156±62 164±49 191±80
PaO2/FiO2 at PEEP 15 [mmHg] 230±69* 272±70*§ 244±70 241±49§
PaCO2 at PEEP 5 [mmHg] 49±7 47±7 45±6 45±6
PaCO2 at PEEP 15 [mmHg] 47±8 46±8 46±6 46±5
Compliance at 5 cmH2O [ml/cmH2O] 34±6 33±8 35±6 37±9
Compliance at 15 cmH2O [ml/cmH2O] 40±7* 45±11*§ 40±12 43±10§
Total lung weight at 5 cmH2O [ml] 1307 ± 240 1312 ± 292 1052 ± 334 1083 ± 376
NAT at 5 cmH2O [g] 576 [410-797] 448 [354-646]† 372 [305-472]# 325 [181-390]#
NAT at 15 cmH2O [g] 301 [230-400]* 296 [231-329]*§ 290 [250-334]* 215 [163-330]*‡§
PAT at 5 cmH2O [gr] 454 [360-546] 443 [411-561] 387 [281-431] 457 [275-561]
PAT at 15 cmH2O [gr] 486 [422-786] 459 [410-681] 378 [241-572] 407 [263-577]
WAT at 5 cmH2O [g] 208 [163-347] 255 [191-434]† 240 [210-351] 324 [239-343]†
WAT at 15 cmH2O [g] 468 [388-593]* 534 [458-630]*ठ461 [377-581]* 483 [336-593]*
HIT at 5 cmH2O [gr] 3.6 [2.1-5.4] 2.7 [2.0-4.9] 5.8 [4.7-6.9] 6.0 [4.8-7.9]#
HIT at 15 cmH2O [gr] 15 [7.3-18]* 12 [9.0-18]* 17 [14-26]* 15 [10-24]*
Page 29 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

29
PaO2/FiO2: pressure of oxygen in arterial blood/inspired oxygen fraction ratio; PEEP 5:
Positive end-expiratory pressure 5 cmH2O; PEEP 15: Positive end-expiratory pressure
15 cmH2O; PaCO2: partial pressure of carbon dioxide; NAT: non-aerated tissue; PAT:
poorly- aerated tissue; WAT: well-aerated tissue; HIT hyperinflated tissue
*P<0.05, between parameters at 5 cmH2O (or PEEP 5) and 15 cmH2O (or PEEP 15)
†P<0.05, comparing parameters at 5 cmH2O (or PEEP 5) between supine and prone
‡ P<0.05, comparing parameters at 15 cmH2O (or PEEP 15) between supine and prone
§ P<0.05, between parameters at 5 cmH2O (or PEEP 5) in supine, and 15 cmH2O (or
PEEP 15) in prone
# P<0.05, comparing patients with high lung recruitability versus low lung recruitability
at the same level of PEEP and position
Page 30 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

30
LEGENDS
Figure 1: Study Protocol
The protocol was performed in ICU and CT room. In ICU, patients were ventilated with
PEEP 5 and then 15 cmH2O, for 20 minutes each, starting with a recruitment maneuver
at 45 cmH2O before each period. Respiratory mechanics, oxygenation and
hemodynamic parameters were assessed at the end of each setting. Thereafter, in the
CT-room, patients underwent whole-lung CT during breath-holding sessions at
consecutive airway pressures of 5, 45, and 15 cmH20; afterwards, Cine-CTs were
performed on a fixed thoracic transverse slice at PEEP 5 and 15 cmH2O. CT-images
were repeated in supine and prone, and the sequence of positions and PEEP levels was
applied in random order.
Figure 2: Distribution of lung compartments expressed in weight and volume
Proportion of total lung weight (A) and volume (B) of each compartment classified as
non-aerated (NAT), poorly-aerated (PAT), well-aerated (WAT), and hyperinflated
(HIT) tissue, at end expiration with PEEP 5 and 15-cmH2O, assessed in supine (supine
5 and supine 15) and prone positioning (prone 5 and prone 15). Data is presented for the
overall population (left, n=24), for the subgroup of patients with high lung recruitability
(center, n=14) and for the subgroup of patients with low lung recruitability (right,
n=10).
*P<0.05, between parameters at supine 5 and supine 15 cmH2O
†P<0.05, between parameters at prone 5 and prone 15 cmH2O
‡ P<0.05, between parameters at supine 5 and prone 5 cmH2O
§ P<0.05, between parameters at supine 15 and prone 15 cmH2O
Page 31 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

31
Figure 3: Effects of PEEP and prone positioning on cyclic
Recruitment/Derecruitment (R/D) and Tidal-Hyperinflation (TH).
Cyclic Recruitment/Derecruitment (R/D) and Tidal-Hyperinflation (TH) with PEEP 5
and 15-cmH2O, assessed in supine (supine 5 and supine 15) and prone positioning
(prone 5 and prone 15). Data is presented for the overall population (A; n=24), for the
subgroup of patients with high lung recruitability (B; n=14) and for the subgroup of
patients with low lung recruitability (C; n=10).
*P<0.05, between parameters at supine 5 and prone 15 cmH2O
†P<0.05, between parameters at supine 5 and supine 15 cmH2O
‡ P<0.05, between parameters at supine 15 and prone 15 cmH2O
Figure 4: Representative chest CT images obtained during breath-holding sessions.
Representative CT slices of the lungs obtained 2 cm above the diaphragm dome at
airway pressures of 5-cmH2O (left) and 45-cmH2O (right) from four patients in supine
(upper) and prone positioning (lower). The percentage of potentially recruitable lung
was defined as the proportion of non-aerated tissue in which aeration is restored when
increasing airway pressures from 5 to 45 cmH20. In patient A, percentage of potentially
recruitable lung was 24% in supine and 18% in prone; in patient B, 24% in supine and
15% in prone; in patient C, 14 % in supine and 21% in prone; and in patient C, 27% in
supine and 24% in prone.
Page 32 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Figure 1. Study Protocol
ICU CT ROOM
PEEP 5
PEEP 15
RM
1° CT 5 cmH2O 3° CT
15 cmH2O
5 min
2 cicles
(12 sec)
DYNAMIC CT
(MV unterrupted)
PEEP 25
2° CT 45 cmH2O
5 min
2 cicles
(12 sec)
RM
RM
RM
STATIC CT
(Holding sesions)
PEEP 5
PEEP 15
20 min.
20 min.
Assessment of:
-Respiratory
mechanics
-Oxygen
exchange
-Hemodynamic
parameters
ZEEP
RM 45 cmH2O
Assessment of:
-Respiratory
mechanics
-Oxygen
exchange
-Hemodynamic
parameters
RM
Page 33 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Fig 2
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% HIT
% WAT
% PAT
% NAT
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
Tis
sue W
eig
ht
(%
of
tota
l lu
ng w
eigh
)
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
Overall
population
Patients with high
lung recruitability
Patients with low
lung recruitability
∗∗∗∗ †
‡∗∗∗∗
∗∗∗∗†
‡
∗∗∗∗†
∗∗∗∗
†
‡∗∗∗∗
†∗∗∗∗
†
∗∗∗∗ †‡
∗∗∗∗ †
∗∗∗∗†
†
‡
∗∗∗∗
A
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% HIT
% WAT
% PAT
% NAT
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
Lu
ng c
om
partm
en
ts
(% o
f to
tal
lun
g v
olu
me)
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
sup
ine
5
sup
ine
15
pro
ne
5
pron
e 1
5
Overall
population
Patients with high
lung recruitability
Patients with low
lung recruitability
∗∗∗∗ †‡
∗∗∗∗
†‡
∗∗∗∗†
∗∗∗∗ †∗∗∗∗ †
‡
†
∗∗∗∗†
‡
∗∗∗∗ †
∗∗∗∗†
∗∗∗∗†
∗∗∗∗†
B
Page 34 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Figure 3. Effects of PEEP and prone position on cyclic Recruitment/Derecruitment
(R/D) and Tidal-Hyperinflation (TH).
A.- Overall population (n = 24)
R/D (%)
B.- Patients with high lung recruitability (n = 14)
R/D (%)
C.- Patients with low lung recruitability (n = 10)
supine 5 supine 15 prone 5 prone 150
2
4
6
8
supine 5 supine 15 prone 5 prone 150.0
0.5
1.0
1.5
∗∗∗∗ ‡
†
† †
‡ ∗∗∗∗
‡
†
‡
Page 35 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Figure 4. Representative chest CT images obtained during breath-holding sessions
Patient A Patient B
5 cm H2O 45 cm H2O 5 cm H2O 45 cm H2O
Patient C Patient D
5 cm H2O 45 cm H2O 5 cm H2O 45 cm H2O
Page 36 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Effects of prone positioning on lung protection in patients with Acute Respiratory
Distress Syndrome
Rodrigo A. Cornejo, Juan C. Díaz, Eduardo A. Tobar, Alejandro R. Bruhn, Cristóbal A.
Ramos, Roberto A. González, Claudia A. Repetto, Carlos M. Romero, Luis R. Gálvez,
Osvaldo Llanos, Daniel H. Arellano, Wilson R. Neira, Gonzalo A. Díaz,
Aníbal J. Zamorano, Gonzalo L. Pereira.
ONLINE DATA SUPPLEMENT
Page 37 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Additional Methods
Study population
Twenty-four patients were studied at the Hospital Clínico Universidad de Chile. This
prospective single center study was approved by the institutional review board and the
ethical committee from CONYCIT (Comisión Nacional de Investigación Científica y
Tecnológica, Gobierno de Chile). Written informed consent was obtained from the next
of kin.
Inclusion criteria included patients with i) acute respiratory distress syndrome (ARDS),
i.e., ratio of partial pressure of arterial oxygen to the fraction of inspired oxygen
(PaO2:FiO2) of less than 200 mmHg, the presence of bilateral pulmonary infiltrates on
the chest radiograph, and no clinical evidence of left atrial hypertension (defined by
pulmonary-capillary wedge pressure of 18 mmHg or less, if measured) (E1); ii) time on
mechanical ventilation more than 24 and less than 72 hours (early phase of ARDS); and,
iii) who required lung computed tomography (CT) scan for clinical proposes.
Exclusion criteria were an age below 18 years, pregnancy, haemodynamic instability,
evidence of barotrauma, history of chronic bronchitis, emphysema or pulmonary
fibrosis, and contraindications for prone positioning: intracranial hypertension,
abdominal compartment syndrome, severe septic shock, unstable spinal injury, recent
abdominal or chest surgery, open or flail chest, and inability to tolerate prone
positioning (eg, pelvic fracture, unstable long bone fracture) (E2).
Ventilatory setting
During the protocol, all patients were in volume-controlled mode, under deep sedation
(fentanyl and midazolam) and neuromuscular paralysis (rocuronium). Tidal volume
(VT) was kept constant at 6 ml/kg ideal body weight (IBW) during the protocol.
Fraction of inspired oxygen (FiO2) and respiratory rate were adjusted to maintain
Page 38 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
oxygen saturation higher than 93%, and partial pressure of arterial carbon dioxide
(PaCO2) lower than 55 mmHg. Inspiration: expiration time ratio (I:E) was set at 1:2.
Respiratory flow and airway pressures were monitored continuously using a
pneumotachometer (Hans Rudolph 3700; Kansas City, MO), and data was collected on
a personal computer-based data acquisition system (Research Pneumotach System
3.07.08, Korr Medical Technologies Inc.).
Protocol
Protocol was performed in two areas: intensive care unit (ICU) and CT room. Before
the protocol, we verified that PEEP 15 cmH2O did not induce plateau pressure higher
than 30 cmH2O nor hemodynamic instability.
In the ICU, patients were evaluated at two levels of PEEP (5 and 15), first in one
position, and later in the other one (i.e. supine and prone positioning, in random order).
Respiratory mechanics (quasi-static compliance of the respiratory system and driving
pressure), oxygenation and hemodynamic parameters (central venous pressure, heart
rate, and mean arterial pressure) were measured at the end of each 20-minute period
with PEEP 5 and PEEP 15 cmH2O, both applied in random order also. Quasi-static
compliance of the respiratory system was calculated by dividing tidal volume by the
difference between plateau pressure and total PEEP (including auto-PEEP if present).
In the CT room patients were scanned in supine and prone positioning. The sequence of
positions and PEEP levels was applied randomly. Static and dynamic CT images were
acquired at each setting after 5-min of ventilations for stabilization. Immediately before
each stabilization period, a recruitment maneuver performed at 45 cmH2O (Pressure-
controlled mode with inspiratory pressure of 25 cmH2O over PEEP 20 cmH2O, I:E ratio
1:1, respiratory rate 15 breaths/min, for 1 minute) was applied to standardize volume
history (E3). Patients remained in the CT room at least 1 hour. The delay time between
Page 39 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

ICU and CT assessments was less than two hours. Each patient was transported to the
CT room by the intensive care research team, composed by two intensivists, two nurses,
two respiratory therapists and one nursing assistant.
Static computed tomography
Lung scanning was performed from the apex to the diaphragm at an inspiratory-plateau
pressure of 45 cmH2O during an end-inspiratory pause (ranging from 15 to 20 seconds)
and thereafter at PEEP values of 5 and 15 cmH2O applied in a random sequence during
an end-expiratory pause (ranging from 15 to 20 seconds). Airway pressure was
monitored during the CT scan acquisition to ensure that the target pressures (end-
inspiratory 45 cmH2O and end-expiratory 5 and 15 cmH2O) were actually applied.
Multidetector CT scanning (Somaton Sensation®, Siemens Medical Systems Germany)
was performed as follows: tube voltage: 120 kVp, tube reference current: 200 mA,
mAs: 100, collimation: 24 x 1.2 mm, bed speed: 80.64 mm per second, rotation time:
0.5 sec, pitch: 1.4, matrix was 512x512, and pixel 0.55 mm. Contiguous axial sections
5-mm thick were reconstructed from the volumetric data using the B70 convolution
Kernel, a high definition filter (Very Sharp, Siemens®). All sections were recorded on
an optical disk for later computerized analysis
Dynamic computed tomography
During this phase respiratory rate was reduced to 10 breaths per minute. A 2.4 mm-
thick CT slice, 2 cm above the dome of the diaphragm was selected for the dynamic
protocol. Cine-CTs of 12 seconds was performed as follows: tube voltage: 100 kVp,
tube current: 80 mA, mAs: 40, collimation: 24 x 1.2 mm; 0.5 sec-24 images, 0.36
sec./rotation; matrix: 512x512, and pixel 0.55 mm.
Page 40 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

CT-scan images analysis
CT-scan images analysis was performed by three radiologists (JD, CR and GP), blinded
to the patient data and airway pressure applied, using Pulmo® (Siemens Medical
Systems Germany), and MALUNA® (University of Gottingen, Germany) software for
CT images analysis.
In the case of static CT images, analysis was performed on each one of the contiguous
axial 5-mm thick sections, from the apex to the diaphragm. The outline of each CT-slice
was established visually and delineated manually, including all lung parenchima and
excluding bones, mediastinal organs, pleaural effusions and large vessels of lung hilum.
The respective volumes of gas and tissue were measured according to a previously
described analysis (E4-E7), based on the correlation between the CT attenuation and
physical density (E8).
We used the classic definition for lung compartments according to their different CT
thresholds, identifying the following lung compartments: hyperinflated (pixels with CT
numbers between -1.000 and -900 Hounsfield units [HU]), well-aerated (between -900
and -500 HU), poorly aerated (between -500 and -100 HU), nonaerated (between -100
and +100 HU) (E4-E7).
The weight of the corresponding lung tissue in each lung compartment was calculated
as follows:
Tissue weight [compartment] = Volume [compartment]*(1- (CT[compartment] /-1000))
E4
Where “Tissue weight [compartment]” corresponds to the lung tissue weight of the
compartment, “Volume [compartment]” its entire volume, and “CT [compartment]”
corresponds to the average CT number of the compartment, expressed in HU.
The percentage of potentially recruitable lung was defined as:
Page 41 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC
([non-aerated tissue at 5 cmH2O - non-aerated tissue at 45 cmH2O] / total weight) (E5)
Patients with high lung recruitability were defined as those with a percentage of
potentially recruitable lung higher than 13.9% in supine. For sample size determinations
we defined this recruitability threshold “a priori” based on the median value of
recruitability for the subgroup of ARDS patients from Gattinoni’s study (49 of the 68
patients) (E5). The original threshold of Gattinoni’s study was 9%, which corresponded
to the median value of the whole ALI/ARDS population (68 patients). We acknowledge
that by applying a different threshold, our subgroups of higher and lower lung
recruitability are not comparable to the subgroups defined in the original study of
Gattinoni.
In the case of dynamic CT, each 2.4 mm-thick cine-CT slice was analyzed. Each lung
was manually outlined drawing ROIs in each of the 24 images (frames) that
encompassed two respiratory cycles. The weight of each tissue compartment was
divided by the total lung weight contained in the transverse slice and expressed as
percentage. Each dynamic CT captured two respiratory cycles. In each respiratory cycle
within the 12 sec-dynamic CT, maximal (max), minimal (min), and cyclic variation (∆,
with ∆=max-min) of the four density compartments were registered and averaged to
obtain the corresponding values for each level of PEEP, in supine and prone
positioning. Anatomical landmarks were carefully defined to obtain CT slices at the
same level and comparable between different levels of PEEP and positions. Cine-CT
was performed at each ventilator setting at least after 5 minutes of stable airway
pressures and pulse oximetry readings. Cyclic recruitment/derecruitment was defined as
∆ non-aerated tissue, and tidal-hyperinflation was defined as ∆ hyperinflated tissue
measured (E7) at each PEEP level (5 and 15 cmH2O) while VT was held constant.
Page 42 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

Given the potential for radiation exposure, a medical biophysics and radiation
protection officer (DC) was included in the study team to reduce the level of radiation
per CT. Finally, the total dose per patient did not exceed the equivalent of 1 coronary
CT Angiography study (1500 - 1800 mGy*cm).
Page 43 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

References
E1. Bernard, G. R., A. Artigas, K. L. Brigham, J. Carlet, K. Falke, L. Hudson, M.
Lamy, J. R. Legall, A. Morris, and R. Spragg. The American-European Consensus
Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial
coordination. Am.J.Respir.Crit Care Med. 1994; 149: 818 - 824.
E2. Messerole E, Peine P, Wittkopp S, Marini JJ, and Albert RK. The Pragmatics of
Prone Positioning. Am J Respir Crit Care Med 2002; 165: 1359 - 1363
E3. Perchiazzi G, Rylander C, Vena A, Derosa S, Polieri D, Fiore T, Giuliani R,
Hedenstierna G. Lung regional stress and strain as a function of posture and ventilatory
mode. J Appl Physiol 2011; 110: 1374 - 1383.
E4. Gattinoni, L., P. Caironi, P. Pelosi, and L. R. Goodman. What has computed
tomography taught us about the acute respiratory distress syndrome? Am.J.Respir.Crit
Care Med 2001; 164: 1701 - 1711.
E5. Gattinoni, L., P. Caironi, M. Cressoni, D. Chiumello, V. M. Ranieri, M. Quintel, S.
Russo, N. Patroniti, R. Cornejo, and G. Bugedo. Lung recruitment in patients with
the acute respiratory distress syndrome. N.Engl.J.Med. 2006; 354: 1775 - 1786.
E6. Bugedo G, Bruhn A, Hernández G, Rojas G, Varela C, Tapia JC, Castillo L. Lung
computed tomography during a lung recruitment maneuver in patients with acute lung
injury. Intensive Care Med. 2003; 29: 218 - 25.
Page 44 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC

E7. Bruhn A, Bugedo D, Riquelme F, Varas J, Retamal J, Besa C, Cabrera C, Bugedo
G. Tidal volume is a major determinant of cyclic recruitment-derecruitment in acute
respiratory distress syndrome. Minerva Anestesiol 2011; 77: 418 - 426.
E8. Mull RT. Mass estimates by computed tomography: physical density from CT
numbers. Am J Padiol 1984; 143: 1101 - 1104.
Page 45 of 45 AJRCCM Articles in Press. Published on 24-January-2013 as 10.1164/rccm.201207-1279OC