Effects of Immunosuppressive Agents on Glucose Metabolism
21
ADVERSE EFFECTS AND INTERACTIONS Clin. Immunother. 4 (2): 103-123, 1995 1172-7039/95/CXXl8-01 03/S 1 0.5010 © Adis International Limited. All rights reserved. Effects of Immunosuppressive Agents on Glucose Metabolism Implications for the Development of Post-Transplant Diabetes Mellitus Andrew J. Krentz} Jan Dmitrewski,2 David Mayer 2 and Malcolm Nattrass 1 1 Diabetes Resource Centre, The General Hospital, Birmingham, England 2 Liver Unit, Queen Elizabeth Hospital, Birmingham, England Contents Summary . . . . . . . . . . . . . .. . ...... . 1. Immunosuppressant Drugs and Glucose Homeostasis 1.1 Historical Perspectives . . . . . . . . . . . . . . . . 1.2 Limitations of Metabolic Studies in Human Organ Transplant Recipients 2. Corticosteroids .............. . 2.1 Metabolic Effects in Humans . . . . . . 2.2 Studies in Human Transplant Recipients 3. Azathioprine ...... ........... . 4. Cyclosporin . . . . . . . . . . . . . . . . . . . 4.1 Studies in Human Transplant Recipients 4.2 Animal Studies. . . . .......... . 4.3 Metabolic Studies in Non-Transplant Patients. 5. Tacrolimus . . . . . . . . . . . ..... 5.1 Studies in Human Transplant Recipients 5.2 Insulin Secretion and Insulin Action . . . 5.3 Animal Studies ..... 6. Molecular Actions of Cyclosporin and Tacrolimus 6.1 Immunophilins and Intracellular Calcium Metabolism . 6.2 Physiology of Insulin Secretion. . . . . . . . . . . . . . . 6.3 Effects of Immunosuppressive Agents on P Cell Calcium Metabolism . 6.4 Immunosuppressive Agents and Insulin Action 7. Conclusions and Recommendations . . . .. . ............. . 103 104 104 105 107 107 107 108 108 108 111 III 112 112 116 116 117 117 117 118 118 119 Summary Diabetogenic effects have been ascribed to several drugs currently used for immunosuppression following organ transplantations, including corticosteroids, cyclosporin and tacrolimus (FK-506). Azathioprine appears to be devoid of ad- verse effects on carbohydrate metabolism. The pathogenesis of immunosuppression-associated diabetes mellitus has not been clearly defined, and may be multifactorial in organ transplant recipients. Metabolic similarities between post-transplant diabetes and non-insulin-dependent diabetes mellitus include defective insulin secretion and impaired insulin action in target tissues. The predominant effect of corticosteroids is induction of a state
-
Upload
david-mayer -
Category
Documents
-
view
214 -
download
0
Transcript of Effects of Immunosuppressive Agents on Glucose Metabolism

ADVERSE EFFECTS AND INTERACTIONS Clin. Immunother. 4 (2): 103-123, 1995 1172-7039/95/CXXl8-01 03/S 1 0.5010
© Adis International Limited. All rights reserved.
Effects of Immunosuppressive Agents on Glucose Metabolism Implications for the Development of Post-Transplant Diabetes Mellitus
Andrew J. Krentz} Jan Dmitrewski,2 David Mayer2 and Malcolm Nattrass1
1 Diabetes Resource Centre, The General Hospital, Birmingham, England 2 Liver Unit, Queen Elizabeth Hospital, Birmingham, England
Contents Summary . . . . . . . . . . . . . .. . ...... . 1. Immunosuppressant Drugs and Glucose Homeostasis
1.1 Historical Perspectives . . . . . . . . . . . . . . . . 1.2 Limitations of Metabolic Studies in Human Organ Transplant Recipients
2. Corticosteroids .............. . 2.1 Metabolic Effects in Humans . . . . . . 2.2 Studies in Human Transplant Recipients
3. Azathioprine ...... ........... . 4. Cyclosporin . . . . . . . . . . . . . . . . . . .
4.1 Studies in Human Transplant Recipients 4.2 Animal Studies. . . . .......... . 4.3 Metabolic Studies in Non-Transplant Patients.
5. Tacrolimus . . . . . . . . . . . ..... 5.1 Studies in Human Transplant Recipients 5.2 Insulin Secretion and Insulin Action . . . 5.3 Animal Studies .....
6. Molecular Actions of Cyclosporin and Tacrolimus 6.1 Immunophilins and Intracellular Calcium Metabolism . 6.2 Physiology of Insulin Secretion. . . . . . . . . . . . . . . 6.3 Effects of Immunosuppressive Agents on P Cell Calcium Metabolism . 6.4 Immunosuppressive Agents and Insulin Action
7. Conclusions and Recommendations . . . .. . ............. .
103 104 104 105 107 107 107 108 108 108 111 III 112 112 116 116 117 117 117 118 118 119
Summary Diabetogenic effects have been ascribed to several drugs currently used for immunosuppression following organ transplantations, including corticosteroids, cyclosporin and tacrolimus (FK-506). Azathioprine appears to be devoid of adverse effects on carbohydrate metabolism.
The pathogenesis of immunosuppression-associated diabetes mellitus has not been clearly defined, and may be multifactorial in organ transplant recipients. Metabolic similarities between post-transplant diabetes and non-insulin-dependent diabetes mellitus include defective insulin secretion and impaired insulin action in target tissues. The predominant effect of corticosteroids is induction of a state

104 Krentz et al.
of insulin resistance. Cyclosporin and tacrolimus have been shown to inhibit endogenous insulin secretion and may also have adverse effects on tissue sensitivity to insulin.
Postoperative diabetes mellitus developing de novo is a frequent complication of organ transplantation. Treatment with diet, oral antidiabetic agents or insulin may be necessary. Postoperative diabetes may be a transient phenomenon in some patients, whereas others may require long term insulin treatment. Although clinically overt diabetes is readily diagnosed, the prevalence of subclinical degrees of glucose intolerance may be higher than is currently recognised.
The long term clinical implications of immunosuppression-associated glucose intolerance and diabetes are uncertain and rely on extrapolations from studies in non-transplant populations. Patients with impaired glucose tolerance may have an increased probability of progression to diabetes mellitus, whereas long term diabetes carries the risk of tissue damage from specific microvascular complications, i.e. diabetic retinopathy, neuropathy and nephropathy. Epidemiological and experimental studies have implicated glucose intolerance and hyperinsulinaemia as risk factors for atherosclerosis. Hypertension and atherogenic plasma lipid profiles are also frequently encountered in transplant recipients treated with cyclosporin, tacrolimus and corticosteroids. Thus, patients treated with these drugs, particularly in combination, may possess a multiplicity of risk factors for macro vascular disease. These factors may be relevant to the development of accelerated atherosclerosis that occurs in renal and cardiac transplant recipients. However, their contribution to post-transplant macrovascular disease is uncertain at present.
Carefully designed prospective studies will be necessary to determine the natural history of postoperative diabetes in organ transplant recipients. We recommend that future clinical studies of immunosuppressive agents should avoid arbitrary diagnostic criteria for diabetes and should incorporate rigorous methods for the assessment of glucose tolerance, insulin secretion and insulin action. Modifications of existing immunosuppressive drug regimens may reduce the incidence or severity of postoperative diabetes. Elucidation of the molecular mechanisms responsible for this metabolic complication should provide a more logical basis for prevention and treatment.
1. Immunosuppressant Drugs and Glucose Homeostasis
1.1 Historical Perspectives
Postoperative diabetes in the pre-cyclosporin era of organ transplantation was ascribed to the well-recognised diabetogenic effects of prednisolone. [1-3] Diabetes mellitus developing de novo following transplantation was first reported by Starzl in 1964.[1] Insulin treatment (up to 120 U/day, 30 to 50 U/day in most instances) was required in l3 of the first 42 renal transplant recipients. This figure probably underestimates the incidence of lesser
degrees of hyperglycaemia. In most cases, hyperglycaemia developed insidiously over several
weeks, although diabetes presented with more dra
matic symptoms of weight loss and ketosis in some
patients. Starzl emphasised the apparent relationship between postoperative diabetes and the dosage of
corticosteroids employed as immunosuppressive therapy.l'] Reductions in steroid dosage below 30
mg/day subsequently allowed discontinuation of
insulin in all but 2 of the l3 patients in this series. It has subsequently become clear that cyclo
sporin has independent adverse effects on carbohydrate metabolism in organ transplant recipients)4]
© Adis International Limited. All rights reserved. Clin.lmmunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
Furthermore, clinical and experimental evidence indicates that the recently introduced macrolide immunosuppressant tacrolimus (FK-506) also has significant diabetogenic effects,[S] which at currently employed dosages may be more pronounced than those of cyclosporin.
Corticosteroids, azathioprine and cyclosporin have well established roles in renal, liver, and heartlung transplantation,[4,6] and a therapeutic niche for tacrolimus seems likely to emerge. The clinical application of these agents extends beyond organ transplantation into diseases such as rheumatoid arthritis, psoriasis and inflammatory liver and bowel disease)7,8] Interestingly, awareness of the adverse effect of cyclosporin and tacrolimus on glucose tolerance has not deterred clinical investigators from administering these agents to newly presenting patients with insulin-dependent diabetes with the aim of inducing disease remission)9,1O] Moreover, despite its diabetogenic potential, cyc1osporin is routinely included in the triple immunosuppressive regimen employed in whole or segmental pancreatic transplantation,lll] and has been used with long term success in trials of human islet transplantation. [12]
In this article we review the metabolic effects of immunosuppressive agents, focusing on corticosteroids, azathioprine, cyclosporin and tacrolimus. Particular reference will be made to disturbances of glucose metabolism that are known to be of clinical relevance in non-transplant populations. Druginduced hypertension and adverse changes in lipid metabolism may also be clinically important, particularly in patients with glucose intolerance or diabetes. However, detailed discussion of these factors is beyond the remit of this article. The limitations of the available data concerning the frequency, pathogenesis, management and long term clinical implications of postoperative diabetes will be considered. In addition, we will discuss some data from our own ongoing studies and explore theoretical links between the molecular actions of cyclosporin and tacrolimus with insulin secretion and insulin action. Finally, we will present our proposals for the evaluation of the diabetogenic ef-
© Adis International Limited. All rights reserved.
105
Table I. Limitations of published data concerning metabolic effects of immunosuppressive agents in human transplant recipients
Few data from prospective randomised clinical trials
Confounding effects of concomitant diabetogenic drug therapy
Confounding effects of hormonal stress response to surgery
Arbitrary and inconsistent diagnostic criteria for diabetes
Influence of other recipient characteristics predisposing to diabetes mellitus, e.g. family history, ethnic origin
Glucose intolerance and insulin resistance are features of renal failure and cirrhosis per se
fects of immunosuppressive drugs in future clinical trials.
1,2 Limitations of Metabolic Studies in Human Organ Transplant Recipients
Interpretation of the literature concerning the effects of immunosuppressive agents on glucose metabolism in organ transplant recipients is hindered by limitations in the design and execution of many clinical studies. These are summarised in table I, and discussed in more detail in this section.
(a) Few data are available from prospective studies with adequate statistical power in which patients of similar pretransplant status have been assigned to different immunosuppressive drugs on the basis of random allocation. This rigorous approach is essential to minimise potentials for bias in clinical trials of new therapies)13]
(b) Immunosuppressive drugs are rarely given as monotherapy to transplant recipients. For example, cyclosporin is usually combined with glucocorticoids and azathioprine in order to reduce the incidence of the dosage-related adverse drug effects associated with each agent.[4] Furthermore, the complex multisystem problems of organ transplant patients frequently necessitate the use of other drugs that may exert adverse effects on glucose homeostasisP.3] Inevitably, such therapeutic combinations tend to obscure the metabolic effects attributable to each drug.
(c) The hormonal stress response associated with major surgery has profound effects on the regulation of carbohydrate metabolism.[l4] Elevated circulating levels of counter-regulatory hormones
Clin. Immunother. 4 (2) 1995

106
(glucagon, cortisol and growth hormone) act in concert with the sympatho-adrenal system to stimulate hepatic glycogenolysis and gluconeogenesis; hepatic glucose production therefore increases. Simultaneously, the cellular actions of insulin on the liver and in peripheral tissues are impaired, while compensatory increases in endogenous insulin secretion are restrained by sympatho-adrenal activation. Thus, increased delivery of hepatic ally derived glucose into the systemic circulation is compounded by a state of insulin resistance in which the ability of insulin to stimulate glucose uptake into skeletal muscle and adipose tissue is reduced.[15] The resulting hyperglycaemia leads to glycosuria and hence to an osmotic diuresis when the renal threshold for reabsorption of glucose is exceeded. Dehydration further exacerbates the counter-regulatory hormonal response, and a vicious cycle of worsening metabolic decompensation ensues. Moreover, acute hyperglycaemia in the immediate postoperative period may be aggravated by the effects of high-dosage steroids and dextrosecontaining intravenous fluids. For these reasons, assessments of carbohydrate metabolism in the early postoperative period may be difficult to interpret, and caution is required in ascribing metabolic changes to individual drugs.
(d) Since postoperative diabetes may be asymptomatic, frequent biochemical assessment is necessary to detect its development, which may be insidious. However, for reasons that are unclear, many centres continue to use arbitrary and inconsistent diagnostic criteria. Moreover, the use of insensitive methods may underestimate the true prevalence of glucose intolerance. Studies performed prior to the 1980s antedate the reclassification of diabetes in which the intermediate diagnostic category of impaired glucose tolerance (IGT) was introduced.[l6,17] This category can only be diagnosed using a 75g oral glucose tolerance test following an overnight fast.[17] Thus, patients with IGT will not be identified in studies that rely on measurements of random or fasting plasma glucose concentrations. Studies in non-transplant populations indicate that patients with IGT are not at significant risk of developing
© Adis International Limited. All rights reserved.
Krentz et al.
the chronic microvascular complications associated with diabetes, i.e. retinopathy, nephropathy and neuropathy)18] Nonetheless, the diagnosis of IGT may be of clinical importance in organ transplant recipients. First, prospective population-based studies indicate that the probability of progression to diabetes is increased in individuals with IGT,P8] and secondly IGT confers an increased risk of atheromatous disease, which is the leading cause of premature mortality in patients with non-insulindependent diabetes and in organ transplant recipients.
(e) The frequency of postoperative diabetes following organ transplantation may be influenced by variables such as the age and ethnic origin of the recipient and the presence or absence of a family history of diabetes in first degree relatives. It is of interest that these factors have been identified as important determinants of non-insulin-dependent diabetes in non-transplant populations)19]
(f) Disturbances of carbohydrate metabolism are commonly observed in patients with chronic renal failure[20] or chronic parenchymal liver diseasePI] Both of these conditions are associated with tissue insulin resistance and abnormalities of ~ cell function.[20,21] Glucose tolerance remains normal in approximately 50% of patients with moderate to severe renal insufficiency.[20] In these patients the islet ~ cells are able to compensate for impaired insulin action through hypersecretion of the hormone. Elevated plasma immunoreactive insulin concentrations are also frequently seen in patients with chronic liver disease such as cirrhosis, although abnormalities of glucose intolerance occur in up to 80% of these patientsPI,22] Thus, compromised graft function in kidney and liver transplant recipients may produce abnormalities of glucose metabolism independently of any drug-induced effects. However, graft dysfunction rarely leads to clinically significant hyperglycaemia unless associated with severe rejection requiring high dosage corticosteroids. Nonetheless, minor degrees of glucose intolerance might result from impaired graft function. In addition, portosystemic anastomoses may contribute to postoperative hyperinsulinaemia in pa-
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
tients receiving liver transplants for cirrhosis.l231 In vivo dose-response studies of insulin action are therefore required to confirm the presence of insulin resistance in patients in whom glucose intolerance coexists with hyperinsulinaemia. In addition to steroid-treated kidney transplant recipients,[241 decreased insulin-mediated glucose disposal has been demonstrated in patients with chronic renal failure[201 or cirrhosisp21
Because of the complex and potentially confounding metabolic effects of organ transplantation in patients with chronic renal and liver disease, studies of the effects of cyclosporin and tacrolimus in non-transplant recipients are of particular interest.
2. Corticosteroids
2.1 Metabolic Effects in Humans
Despite their potential to induce adverse clinical effects, including prominent deleterious actions on glucose homeostasis, corticosteroids have been the mainstay of pharmacological immunosuppression since the earliest days of clinical organ transplantation.[ll It has long been recognised that corticosteroids in therapeutic doses are potent initiators of glucose intolerance and diabetes mellitus.[2.31 Glucocorticoids such as prednisolone exert their influence on glucose metabolism principally by inducing insulin resistance in hepatic and peripheral tissues through as yet unidentified intracellular biochemical effects distal to the interaction between insulin and its membrane receptor.l251 Insulin resistance in target tissues of insulin action is reflected by increased plasma immunoreactive insulin concentrations indicative of compensatory increases in islet ~ cell secretionP6,271 Corticosteroids also accelerate adipose tissue lipolysis and hepatic ketogenesis,[281 although these effects are usually only evident in the presence of marked insulin deficiency.l291
2.2 Studies in Human Transplant Recipients
The diabetogenic potential of corticosteroids in organ transplant recipients is well documented.l',30-381 Insulin therapy is frequently required to control
© Adis International Limited. All rights reserved.
107
hyperglycaemia, and occasionally these agents produce major metabolic disturbances such as the hyperosmolar nonketotic syndrome or diabetic ketoacidosis.l30-32,351 These acute life-threatening complications require emergency therapy with intravenous fluids and insulin,l391
Ethnic origin appears to influence the risk of developing postoperative steroid-induced diabetes. Two studies from the US indicate that Black organ transplant recipients are at higher risk of developing this complication than patients of White Caucasian ethnicity,l36,381 In addition, a family history of diabetes!33,371 in a first-degree relative has been shown to be positively associated with the risk of steroid-induced diabetes in some retrospective analyses. Reports of associations between steroidinduced diabetes and certain human leucocyte (HLA) antigens have been inconsistent, possibly reflecting the limited size and heterogeneity of the populations studied as well as differences in the definition of diabetes between these studies,l36,37,401
The precise incidence of postoperative steroidinduced diabetes in organ transplant recipients is uncertain. In the pre-cyclosporin era the reported incidence of postoperative diabetes ranged from approximately 6 to 47%, reflecting differences in the definition and ascertainment of diabetes between studies as discussed above.[30,32-38]
The adverse metabolic effects of corticosteroids are dosage-related[41 1 and can, therefore, be minimised by maintaining the steroid dosage as low as possible. Dosages below prednisolone 7.5 mg/day are rarely associated with clinically significant effects on glucose metabolism. However, large bolus doses of methylprednisolone (e.g. 500 mg/day for 3 to 5 days) are still employed in the management of acute organ rejection episodes.!421 The advent of immunosuppressive agents with steroid-sparing effects, for example azathioprine and cyclosporin, has led to an increasing trend towards a reduction in the maintenance dosage or complete withdrawal of steroids.l411 Experience in liver[431 and renal[44,451 transplantation suggests that maintenance immunosuppressive monotherapy with cyclosporin or complete long term withdrawal of steroids may be
Clin. Immunother. 4 (2) 1995

108
feasible, with little compromise of graft function or survival.
3. Azathioprine
Azathioprine, a derivative of 6-mercaptopurine, has played a key role in the development of modem clinical organ transplantation.
Despite extensive clinical experience and a well documented toxicity profile both in organ transplant recipients and in patients with other disorders, azathioprine has not been identified as having significant diabetogenic effects. However, concomitant corticosteroid therapy may have confounded interpretation of data concerning the metabolic effects of azathioprine in organ transplantation. It is therefore difficult to categorically exclude a diabetogenic effect of this drug on the basis of clinical observations.
4. Cyclosporin
4.1 Studies in Human Transplant Recipients
4. 1. 1 Clinical Observations The diabetogenic effect of cyclosporin was
first reported by Gunnarsson et aU46] in 4 insulindependent diabetic patients with nephropathy who had received combined renal and segmental pancreas grafts. A deterioration in intravenous glucose tolerance tests was observed when cyclosporin was substituted for azathioprine while maintaining a constant dosage (15 to 40 mg/day) of prednisolone. All patients also received rabbit antithymocyte globulin. Minor increments in fasting blood glucose were noted and a concomitant rise in plasma C-peptide concentrations, a marker of endogenous insulin secretion, was interpreted as evidence of insulin resistance.l46] These observations were subsequently confirmed in an extension of the study.l47] Reversing the sequence of drug administration, Harris et al,[48] observed a fall in the area under the curve during glucose tolerance tests in 13 nondiabetic renal transplant recipients converted from cyclosporin to azathioprine while prednisolone (30 mg/day on alternate days) was continued. Fasting glucose and immunoreactive insulin concentration
© Adis International Limited. All rights reserved.
Krentz et al.
did not alter significantly in these patients. In these studies, serum creatinine concentration was generally higher during the phase of cyclosporin treatment and this may be of relevance when considering both glucose tolerance[20] and plasma C-peptide concentrations, since C-peptide levels are inversely correlated with creatinine clearance.l49] Reports of decreased plasma clearance of prednisolone by cyclosporin are of interest,[50] since steroids were continued after conversion from cyclosporin to azathioprine or vice versa in each of these studies.
Most of the data that has been published subsequently on the metabolic effects of cyclosporin in transplant recipients is subject to the limitations associated with retrospective nonrandomised studies.[5I-65] Several reports have compared the frequency of post-transplant diabetes in patients treated with either azathioprine or cyclosporin, usually combined with prednisolone (table 2). In general, these studies have found higher rates of post-transplant diabetes with cyclosporin,[51,52,55-58,60] even when the dose of prednisolone was lower when compared with azathioprine and steroid-treated patients.[55,56,60] Roth et aU58] reported fasting hyperglycaemia, defined as 3 glucose concentrations >7.8 mmol/L, in 9.1 and 18.6% of initially nondiabetic renal transplant recipients who were treated with either azathioprine plus prednisolone or cyclosporin plus prednisolone, respectively. Post-transplant diabetes developed mainly during the first 2 months postoperatively, and insulin therapy was instituted in the majority of cases. The overall dosage of prednisolone received during the first 2 postoperative months was somewhat lower in the cyclosporintreated patients, although it is unclear whether the difference in prednisolone dosage was significantly different between the groups. In this particular study, post-transplant diabetes was associated with a significant decrease in graft survival at 3 years, although actuarial patient survival was unaffected.
Retrospective analyses of risk factors for posttransplant diabetes in cyclosporin-treated patients may have been subject to the influences of patient selection criteria and the ethnic mix of the popula-
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes 109
Table II. Clinical studies comparing incidence rates of diabetes in renal transplant recipients receiving maintenance immunosuppression with azathioprine- or cyclosporin-based regimens. None of these studies were randomised or prospective in design. See the text for discussion
Azathioprine Cyclosporin Reference
no. of patients diabetic' (%) steroidsb no. of patients diabetic' (%) steroidsb
160 5.0 Yes 193
47 6.4 Yes 58
180 21.1 Yes 118
180 12.8 Yes 105
276 3.3 Yes 187
99 9.1 Yes 215
53 7.5 Yes 20
a The diagnostic criteria for diabetes varies between studies.
b The patients were also receiving corticosteroids.
c Some patients were also receiving azathioprine (i.e. 'triple' therapy).
tion from which recipients were drawn. Nonetheless, increasing age of transplant recipient[52.58,61,62,65] has emerged as a characteristic that is associated with a greater risk of post-transplant diabetes in patients treated with cyclosporin. In 2 studies from the US, recipients of Black and Hispanic origin were at higher risk of developing postoperative diabetes than White recipientsJ61 ,65] This observation is of interest from an aetiological perspective, since it is in accordance with the higher prevalence of non-insulin-dependent diabetes that exists in these ethnic groupsJ66] By contrast, an association between postoperative cyclosporinassociated diabetes and a family history of diabetes mellitus has been documented only infrequently,[58,61] with other studies finding no association.
4. 1.2 Insulin Secretion Data from animal and human studies of cyclo
sporin-associated diabetes point to defects in both endogenous insulin secretion and insulin action at tissue level. Higher fasting concentrations of immunoreactive insulin and/or C-peptide have been reported in renal transplant recipients treated with cyclosporin plus corticosteroids than in the same or similar patients treated with azathioprine plus steroids, suggesting insulin resistance in basal glucose metabolism.[46,47,60,67] In addition, abnormalities of the dynamics of insulin secretion have been documented, with absence of the normal early (first phase) insulin response and late relative hyperinsulinaemia following an oral glucose challenge
© Adis International Limited. All rights reserved.
7.8 Yes 51
19.1 Yese 52
32.2 Yes 55
17.1 Yes 56
11.2 Yese 57
18.6 Yes 58
30.0 Yes 60
in renal transplant recipients with postoperative diabetesJ6o,67] Immunoreactive insulin responses to an oral glucose challenge[60,67] or a hyperglycaemic clamp[67] have been found to be lower in patients with postoperative diabetes compared with healthy controls or patients with normal glucose tolerance. Yamasaki et al. l68] found that the ratio of the change in immunoreactive insulin: blood glucose 30 minutes after oral glucose 75g was lower in postoperative renal transplant recipients who developed impaired glucose tolerance or diabetes compared with patients who maintained normal glucose tolerance.
The relative defect in endogenous insulin secretion induced by cyclosporin may sometimes be marked. Bending et aI.l69] reported a nondiabetic renal transplant recipient in whom plasma C-peptide concentrations became severely suppressed, necessitating temporary insulin treatment. The close temporal relationship between cyclosporin therapy and the suppression of C-peptide in this patient who exhibited other features of cyclosporin toxicity provides convincing support for an acute drug-related effect. Yoshimura et al.[56] reported a suppression of early immunoreactive insulin secretion in renal transplant recipients treated with cyclosporin plus steroids, which improved following reduction in cyclosporin dosage or conversion to azathioprine.
By contrast, however, in a study principally of pancreas transplant recipients, Blackman et aI.l70] concluded that an immunosuppressive regimen of cyclosporin, azathioprine and prednisolone did not
Clin. Immunother. 4 (2) 1995

110
impair insulin secretion in a group of 6 nondiabetic patients who had received kidney transplants. Aspects of this study are considered in more detail in section 4.1.3.
4. 1.3 Insulin Action Defects in insulin action in cyclosporin-treated
human transplant recipients have been quantitated in a study by Ekstrand et aLl67J These investigators studied 10 renal transplant recipients (7 cyclosporintreated) with normal postoperative glucose tolerance and 14 patients (9 cyclosporin-treated) with postoperative diabetes with the euglycaemic-hyperinsulinaemic clamp technique combined with indirect calorimetry. Both groups received similar dosages of corticosteroids (approximately 0.4 mg/kg/day methylprednisolone). Despite fasting hyperinsulinaemia, basal blood glucose concentration was significantly raised in patients with postoperative diabetes compared with healthy controls (6.1 ± 0.3 versus 4.8 ± 0.1 mmol/L). During insulin-induced hyperinsulinaemia, a 34% reduction in glucose utilisation, primarily storage as glycogen in skeletal muscle, was observed in the patients with normal glucose tolerance compared with matched healthy control individuals. In this group of patients with normal glucose tolerance, increased endogenous insulin secretion appeared to be sufficient to compensate for postoperative insulin resistance. Patients with postoperative diabetes showed only a slightly greater degree of insulin resistance. However, first and second phase insulin responses to oral glucose and glucagon-stimulated insulin secretion were reduced.
Thus, in this study, postoperative diabetes in patients treated with prednisolone and cyclosporin was associated with defects in both endogenous insulin secretion and in the action of insulin on skeletal muscle.l67] It is unfortunate that the patients were not clearly separated into cyclosporin-treated and non-cyclosporin-treated groups in order to distinguish the relative contributions of prednisolone and cyclosporin to the observed metabolic defects. The inclusion of patients treated with cyclosporin alone would have been of considerable interest.
© Adis International Limited. All rights reserved.
Krentz et al.
In addition to renal transplant recipients, insulin resistance in glucose metabolism has also been reported in pancreatic transplant patients treated with cyclosporin and corticosteroids.[7I] Although the kinetics of glucose metabolism are normalised by pancreas transplantation in diabetic patients, concomitant fasting and postprandial hyperinsulinaemia is a consistent finding.[72] In part, the insulin resistance and hyperinsulinaemia may arise from systemic delivery of insulin from the pancreatic graft.l73 ) However, an additional contribution from immunosuppressive drugs appears plausible. The detailed studies of insulin secretion performed by Blackman et aLl70] provide some evidence in support of this hypothesis. In 6 nondiabetic kidney transplant recipients treated with cyclosporin, azathioprine and prednisolone, basal insulin concentrations were increased compared with a control group of 10 healthy volunteers (21.8 ± 1.0 versus 9.7 ± 0.3 mUlL). Basal C-peptide levels were also increased in the transplant recipients, although clearance of this molecule was found to be reduced. While absolute insulin secretion rate was higher in the kidney transplant recipients, the ratio of insulin secreted in the basal and postprandial states was similar to that calculated for the control group. Blackman et al. concluded that the elevated ratio of basal to postprandial insulin secretion observed in a group of diabetic patients with combined pancreas and kidney grafts (treated with a similar immunosuppressant regimen) was therefore not attributable to an inhibitory effect of immunosuppressant drugs on the ~ cellsPO] In fact, the finding of increased immunoreactive insulin concentrations in concert with normal glucose levels in the transplant recipients provides prima facie evidence of insulin resistance, although this was not assessed directly.
4. 1.4 Metabolic Similarities with Non-Insulin-Dependent Diabetes Mellitus
The studies described in sections 4.1.2 and 4.1.3 suggest similarities between the metabolic abnormalities observed in organ transplant recipients treated with cyclosporin plus corticosteroids and patients with non-insulin-dependent diabetes mel-
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
litus. Insulin resistance in glucose metabolism has been identified as a cardinal metabolic abnormality of patients with non-insulin-dependent diabetes,[74,75] although impaired endogenous insulin secretion is also necessary for the development of significant hyperglycaemia. Impaired insulin-mediated glucose disposal during experimental hyperinsulinaemia is mainly accounted for by decreased nonoxidative glucose metabolism.[75] This in tum has been shown to be predominantly due to decreased glycogen formation and is associated with impaired activation of the skeletal muscle enzyme glycogen synthase.
Although fasting and postprandial plasma immunoreactive insulin concentrations may be raised in absolute terms in overt non-insulin-dependent diabetes, the levels are inappropriately low in the face of the prevailing hyperglycaemia. Loss of first phase insulin release is a characteristic feature of impaired glucose tolerance and non-insulindependent diabetes. Moreover, in most radioimmunoassays for insulin, crossreactivity with proinsulin and partially processed proinsulin intermediates is significant. [76] These molecules have considerably lower biological activity than insulin. The proportion of these molecules relative to insulin has been found to be raised both in patients with non-insulin-dependent diabetes[76] and in patients with lesser degrees of glucose intolerance. Whether the apparent hyperinsulinaemia observed in some renal transplant recipients treated with prednisolone and/or cyclosporin[77] is partially accounted for by proinsulin-like molecules has not been determined. However, corticosteroids have been shown to cause a disproportionate increase in proinsulin concentrations in individuals with experimentally induced insulin resistance.[7S]
4.2 Animal Studies
Studies in cyclosporin-treated animals have identified defects in insulin secretion[79-S5] and insulin action[SO,S4] that are independent ofthe influence of corticosteroids. Yale et al.[SO] in a study of cyclosporin-treated rats noted a reversible defect in insulin secretion which appeared to follow the induc-
© Adis Intematianal Limited. All rights reserved.
111
tion of a state of relative insulin resistance. In dogs, Wahlstrom et aI.!S4] showed that treatment with cyclosporin (in the absence of corticosteroids) was associated with a reversible decrease in peripheral insulin action and impairment of insulin secretion in glucose clamp studies.
In vitro studies support a direct toxic effect of cyclosporin on rodent and human islet p cells. [S7-92] Robertson[S7] reported a dose-related inhibition by cyclosporin of glucose-stimulated insulin secretion in isolated rat islets and in a glucose-responsive clonal p cell line. Nielsen et aI.!90] reported that therapeutically relevant doses of cyclosporin reduced insulin secretion from, and increased the residual insulin content of, isolated human islets. In vitro studies of rat pancreas by Gillison et aI.!93] suggested that the effects of cyclosporin on islet endocrine function may be confined to insulinproducing p cells; cyclosporin had no effect on arginine-stimulated glucagon release.[93]
Interactions with other drugs have been demonstrated, with a synergistic effect of cyclosporin on streptozocin (streptozotocin)-induced diabetes in mice[94] and inhibition of sulphonylurea-induced insulin secretion,!95] The toxic effect of cyclosporin on islet p cell function may be enhanced by prostaglandin inhibitors,[96] whereas administration of a prostaglandin analogue has been shown to partially protect against cyclosporin-induced p cell toxicity,!97]
4.3 Metabolic Studies in Non-Transplant Patients
The effects of cyclosporin on carbohydrate metabolism have also been examined in non-transplant patients, albeit in relatively few patients and a limited number of conditions. Robertson et al.[9S] studied patients with multiple sclerosis treated with cyclosporin in a placebo-controlled trial. After 2 years of follow-up no statistically significant alterations were observed in fasting levels of glucose, immunoreactive insulin or C-peptide, nor was there any deterioration in intravenous glucose tolerance tests. It is noteworthy that the
Clin. Immunother. 4 (2) 1995

112
patients in this study were not receiving corticosteroids.f98]
Luzi et al.[7I] studied 6 patients with uveitis who
were receiving long term therapy with cyclosporin at a mean (± SEM) dosage of 6.0 ± 1.4 mg/kg/day. There were no significant differences in fasting concentrations of glucose, immunoreactive insulin, nonesterified fatty acids or glucagon between
these patients and a control group of 9 healthy volunteers. During hyperinsulinaemic (plasma insulin concentrations approximately 65 mUlL) euglycaemic clamps there were no statistically significant
differences in glucose oxidation or nonoxidative glucose disposal. As in the study of Robertson et al.,[98] these patients were not receiving steroids.
In another study from Robertson's group, Teuscher et al.[99] found reduced maximal acute insulin re
sponses (assessed as glucose potentiation of argi
nine-stimulated insulin secretion) in 3 nondiabetic psoriasis patients treated with long term cyclosporin
(383 ± 72 mg/day) relative to a control group of 3 matched individuals. During intravenous glucose tolerance tests, the rate of glucose disappearance (Kg) was similar between the psoriasis patients and the control group. The magnitude of the reduction in maximal insulin response in the cyclosporintreated psoriasis patients was comparable to that observed in a group of 12 nondiabetic kidney transplant recipients treated with a similar dosage of
cyclosporin (260 ± 32 mg/day), together with aza
thioprine and prednisolone, relative to the matched
control group. Although the small sample sizes ofthese studies
limits their interpretation, cyclosporin, in the ab
sence of corticosteroids, has not been shown to have
any significant effects on glucose metabolism in
non-transplant patients. However, the diminished
~ cell secretory reserve in the psoriasis patients noted by Teuscher et aU99] led these investigators to con
clude that the reduced insulin response in the kid
ney transplant recipients was caused, at least in part,
by cyclosporin.
© Adis International limited. All rights reserved.
Krentz et al.
5. Tacrolimus
5.1 Studies in Human Transplant ReCipients
Although the therapeutic role of tacrolimus has yet to be clearly defined, the efficacy of the drug in renal, liver and cardiac transplantation,[lOO,IOI] combined with its ability to reverse ongoing rejection, appear to augur well for its future in clinical transplantation. Although early reports of the use of tacrolimus in humans did not reveal serious adverse effects,[100] with greater clinical experience a significant diabetogenic effect of the drug has emerged.f5,6.101-109] The reported frequency of postoperative diabetes developing de novo in organ transplant recipients treated with tacrolimus is higher than in cyclosporin-treated renal or liver transplant recipients. [5,6,110] However, as is the case for clinical studies of cyclosporin, problems of variable and arbitrary definitions of diabetes, absence of data from control individuals, heterogeneity of patient populations and concomitant corticosteroid therapy hinder interpretation of the metabolic effects of tacrolimus in human transplant recipients. Comparisons between studies must therefore be made with caution.
However, Fung et aLl6] reported postoperative hyperglycaemia which necessitated insulin treatment in 151 of 370 (36%) liver transplant recipients treated with tacrolimus and corticosteroids, whereas O'Grady et aU"O] reported postoperative diabetes in only 6 of 73 (8%) liver transplant recipients treated with cyclosporin plus corticosteroids. To date, studies in tacrolimus-treated non-transplant patients have been confined to very few individuals.[8]
In a randomised open multicentre trial comparing tacrolimus and cyclosporin in 545 liver transplant recipients (the European FK 506 Multicentre Liver Study Group), postoperative hyperglycaemia and diabetes mellitus were more frequent in the tacrolimus-treated group.[108,109] Unfortunately, this major trial contained deficiencies in its design with regard to the evaluation of glucose metabolism. First, although designed as a prospective study, there were no agreed criteria for the ascertainment, diagnosis
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
or treatment of postoperative diabetes mellitus between centres. Thus, the reported frequencies of 'hyperglycaemia' of 30.7 versus 20.5% (p < 0.01) and of 'diabetes' of 17.2 versus 9.5% (p <0.05) for the tacrolimus- and cyclosporin-based regimens, respectively, must be interpreted with a degree of caution.[I08] Interestingly, the higher frequency of diabetes in the tacrolimus-treated patients was observed despite a lower total cumulative dose of corticosteroids. It should also be noted that maintenance or withdrawal of corticosteroids was at the discretion of individual centres.
The study raises several questions. Could the difference in rate of diabetes indicate, at least in part, that patients treated with tacrolimus were monitored more frequently or with more sensitive diagnostic tests than patients treated with the cyclosporin-based regimen? Does the higher proportion of patients receiving insulin at 6 months in the tacrolimus-treated group ( 12 versus 5 %) indicate a more severe metabolic defect in these patients, or might it instead partly reflect a greater awareness of tacrolimus-associated diabetes among investigators sensitised by reports in the literature? Such a possibility is alluded to by the authors of the paper. Another intriguing aspect of this trial is the apparent decline in the incidence of diabetes following the reduction in tacrolimus dosage. The initial intravenous dosage of tacrolimus in the early phase of the study was 80% higher than that for the main phase.l 109] There was also a progressive reduction in the total daily dosage at 12 months from a median of 0.10 mg/kg (early phase) to 0.08 mg/kg (main treatment phase). Following the reduction in dosage, the incidence of diabetes fell from 23.9 to 10.5% in the tacrolimus-treated group (p < 0.0 I), whereas the incidence in the cyclosporin-based group did not change significantly (l0.4 versus 8.7%).[108] In contrast, however, no change in the incidence of hyperglycaemia, as defined by individual centres, was noted in the tacrolimus-treated patients after reduction in dosage (33 versus 29%).
At the Queen Elizabeth Hospital in Birmingham, UK (a participating centre in the trial) we also noted a higher incidence of postoperative diabetes
© Adis International Limited. All rights reserved.
113
6
5
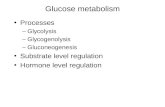
o~--~----~---Control Cyclosporln Tacrollmus
Fig. 1. Fasting venous whole blood glucose concentrations (means ± SEM) in healthy controls and in liver transplant recipients receiving maintenance treatment with cyclosporin ± azathioprine or tacrolimus (10 individuals in each group). There was no significant difference (p = 0.1) between the 3 groups by analysis of variance.
mellitus in patients randomised to tacrolimus. In an endeavour to quantify our observations and to gain some insight into the biochemical mechanisms of postoperative glucose intolerance, we performed 75g oral glucose tolerance tests in consecutive clinically stable trial participants.l lll ] Of 35 patients considered for glucose tolerance tests, only 20 (10 treated with cyclosporin ± azathioprine and 10 randomised to tacrolimus) proved to be suitable. This was for various reasons, the 2 most common being early postoperative deaths and withdrawals from the trial because of chronic rejection or drug toxicity. In contrast to many other transplant centres, it is the policy of the Queen Elizabeth Unit to taper off corticosteroids, discontinuing prednisolone completely by the end of the third postoperative month.l43] The glucose tolerance tests were performed a median of 8 months postoperatively (range 5 to 9 months) and no patient had received prednisolone for at least 6 weeks. Although hyperglycaemia had developed in several patients in the early postoperative period, none was receiving insulin treatment or oral antidiabetic drugs at the time of their glucose tolerance tests. Renal and hepatic function were comparable between the 2 transplant groups.
Clin. Immunother. 4 (2) 1995

114
12
10
4
o Control o Cyclosporin ± azathioprine • Tacrolimus
o 30 60 90 120 150 180 210 240 270 300 Time (minutes)
Fig. 2. Venous whole blood glucose concentrations (means ± SEM) after oral glucose 75g in healthy controls and liver transplant recipients receiving maintenance treatment with cyclosporin ± azathioprine or tacrolimus (10 individuals in each group). Overall trend differences between the 3 groups by 2-way analysis of variance were variance ratio (F) = 3.6 and p < 0.05. Significant differences were apparent in overall glucose concentrations between the healthy controls and the cyclosporintreated patients (p < 0.005) and the healthy controls and the tacrolimus-treated patients (p < 0.001) [reproduced from Krentz et al.,[111[ with permission].
Fasting blood glucose concentrations were similar between the 3 groups (fig. 1). However, significant postglucose hyperglycaemia was observed in the tacrolimus- and cyclosporin-treated patients compared with the healthy controls (fig. 2). We classi-
Krentz et al.
fied our patients' glucose tolerance according to World Health Organization criteria,[17] and found impaired glucose tolerance in 4 of each of the 10 cyclosporin- or tacrolimus-treated patients (table III). In addition, another 2 of the 10 tacrolimustreated patients had 120 min blood glucose concentrations diagnostic of diabetes mellitus (table III). Concomitant fasting (fig. 3) and post-glucose (fig. 4) hyperinsulinaemia, together with elevated plasma Cpeptide concentrations, were suggestive of tissue insulin resistance. However, it is clear from our study that corticosteroids were not responsible for these metabolic abnormalities.
In a follow-up study we re-examined the original cohort 23 months postoperatively)112] At this time, the frequency of glucose intolerance remained higher in the tacrolimus-treated patients, although there was a modest overall improvement in glucose tolerance in each patient group. When glycated haemoglobin concentrations were measured at 23 months we found that the concentrations were all within the nondiabetic range, indicating satisfactory glycaemic control. We believe that it is noteworthy that none of our cohort required antidiabetic drugs or insulin following the withdrawal of corticosteroids. Other investigators have reported improvements in glucose metabolism following withdrawal
Table III. Individual fasting and 120-min venous whole blood glucose concentrations in healthy controls and liver transplant recipients receiving either cyclosporin A ± azathioprine or tacrolimus (reproduced from Krentz et al.,[111] with permission)
Individual Venous whole blood glucose concentration (mmoI/L) controls cyclosporin (± azathioprine) o 120 min 0 120 min 4.8 4.4 4.7 4.5
2 5.1 5.3 4.0 6.6
3 4.6 4.8 5.0 4 4.8 5.5 4.9
5 4.6 5.2 4.9
6 4.6 5.2 4.5
7 3.7 6.3 5.0
8 4.5 5.9 5.2
9 5.4 5.9 4.2
10 4.0 3.9 5.6 Mean ±SEM 4.6±0.2 5.2 ±0.2 4.8 ± 0.2 a Impaired glucose tolerance (World Health Organization, 1985). b Diabetes mellitus (World Health Organization, 1985). c p < 0.05 versus healthy controls. d p < 0.01 versus healthy controls.
© Adis International Limited. All rights reserved.
7.7a
6.0 5.7 6.5 9.0a
4.2 7.6a
7.8a
6.6 ± 0.5e
tacrolimus o 6.2 4.6 5.6 5.3 4.6 6.0 4.5 4.5 5.1 5.0 5.1 ±0.2
120 min 7.2a
13.4b
5.8 12.0b
9.4a
11.8b
8.8a
5.6 7.4a
6.2 8.8 ±0.9d
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
10
;J' 8 ::J S c ~ 6 .5
'" ~ ~ 4 g :l E .§ 2
o ....1....._--'---_--.J'--_
Control Cyclosporin Tacrollmus
Fig. 3. Fasting plasma immunoreactive insulin concentrations (means ± SEM) in healthy controls and liver transplant recipients receiving maintenance treatment with cyclosporin ± azathioprine or tacrolimus (10 individuals in each group). Insulin concentrations were significantly increased in the tacrolimus-treated (p < 0.02) and cyclosporin-treated (p < 0.01) patients compared with the controls. There was an overall difference between the 3 groups by analysis of variance (p < 0.001).
of steroids in cyclosporin-treated renal transplant recipients sufficient to allow cessation of antidiabetic agents or insulin therapy.[113)
Jindal et aLll14) also studied liver transplant recipients randomly allocated to cyclosporin or tacrolimus. In contrast with our study, prednisolone was coadministered to both groups, although the total steroid dosage (for induction, rejection and maintenance) was significantly lower in the tacrolimus-treated group. Jindal et al.[114) used arbitrary criteria to diagnose postoperative diabetes mellitus, i.e. a single fasting blood glucose >22.2 mmollL or fasting levels> 11.1 mmollL for 2 weeks or insulin treatment for 2 weeks. Clearly, these criteria will have identified only more marked degrees of hyperglycaemia; it is uncertain whether the overall magnitude of the metabolic defects in this study was greater than in our patients, who were studied 8 months postoperatively. Jindal et al. [114] commented that the appearance of diabetes
was often temporally associated with the administration of high dosage steroids for treatment of rejection. The incidence of post-transplant diabetes was slightly (but not significantly) higher in the
© Adis International Limited. All rights reserved.
115
cyclosporin-treated group (42.4 versus 30%). This
is at variance with our observations in steroid-free
patients, none of whom had experienced recent
episodes of rejection. The findings of the US Multicenter FK 506 Liver
Study Group[115) were similar to those of the Eu
ropean FK 506 Multicentre Liver Study Group.[I09\
As for the European study, in the US trial the definition of hyperglycaemia as an adverse event was
defined by each centre according to their own particular laboratory criteria'! 115] The incidence of hyper
glycaemia in the tacrolimus treatment group was 47/263 (18%) versus 38/266 (14%), a difference
which did not reach statistical significance (p = 0.07).
The higher incidence of other adverse effects such as nephrotoxicity and neurotoxicity observed with
tacrolimus therapy, in concert with the apparent superiority of tacrolimus over cyclosporin in terms of the incidence of rejection, led to the suggestion
that the adverse event profile of tacrolimus might be diminished by dosage reduction.l 116]
80
::J 70 :; .s 60 c 'S 50 <J)
.50 g! 40 'u ~ 30 o § 20 E E 10
o Control o Cyclosporin ± azathioprine • Tacrolimus
O~-.--r-.--.--r-.--.--r--r~~r-,
o 30 60 90 120 150 180 210 240 270 300
Time (minutes)
Fig. 4. Plasma immunoreactive insulin concentrations (means ± SEM) after oral glucose 75g in healthy controls and liver transplant recipients receiving maintenance treatment with cyclosporin ± azathioprine or tacrolimus (10 individuals in each group). Overall trend differences between the 3 groups by 2-way analysis of variance were variance ratio (F) = 5.5 and p = 0.01. Significant differences were evident in overall immunoreactive insulin concentrations between the healthy controls and the cyclosporin-treated patients (p < 0.05) and the healthy controls and the tacrolimus-treated patients (p < 0.01) [reproduced from Krentz et al.,ln11 with permission].
Clin. lmmunother. 4 (2) 1995

116
5.2 Insulin Secretion and Insulin Action
Few data are available on plasma insulin or Cpeptide concentrations in tacrolimus-treated patients. Elevated C-peptide concentrations were reported in 3 children who developed diabetes following rescue therapy with tacrolimus.[105] The absence of ketonuria in the face of significant hyperglycaemia also argues against marked insulin deficiency in these children.
In parentheses, it should be pointed out that potential confusion has been introduced by rather loose application of diagnostic criteria by clinical investigators. According to the current classification of diabetes, insulin treatment is not necessarily synonymous with insulin-dependent (type 1) diabetes mellitusJI6.17] For example, the significance of the term 'insulin dependence' as employed by Jindal et aLl I 14] is difficult to interpret. No data are presented about the presence or absence of ketonuria, the severity and duration of diabetic symptoms, bodyweight loss, etc. and we therefore assume that Jindal et aLl114] use the term to indicate that it was felt that insulin therapy could not be withdrawn from certain patients during the period of follow-up. However, no information is presented concerning the biochemical criteria by which the decision was made to continue insulin in some patients but not in others. The application of a term with well accepted pathophysiological connotations is potentially confusing, since it carries the implication that the patients who remained on insulin had the particular subtype of diabetes mellitus known as type 1 or insulin-dependent diabetes. Patients with insulin-dependent diabetes require insulin therapy in order to sustain life by preventing diabetic ketoacidosis,l39] rather than to maintain degrees of glycaemic control that would be considered suboptimal on oral antidiabetic agents. Indeed, from knowledge of the protective effects of cyclosporin[l17] and tacrolimus[1l8] on animal models characterised by the spontaneous development of type 1 diabetes, such a mechanism would seem inherently improbable. This is not to suggest that the insulin-treated patients of Jindal et alJ114] may not have had more severe degrees of insulinopenia (although these
© Adis International Limited. All rights reserved.
Krentz et al.
data are not available), but we caution against using the term 'insulin-dependent' when the expression 'insulin-treated' is perhaps more appropriate in the absence of confirmatory biochemical data. More detailed characterisation of the biochemical features of patients with postoperative diabetes, particularly aspects of lipid and ketone body metabolism and quantitative assessments of ~ cell function, may identify subgroups with more marked insulin deficiency who will require long term insulin treatment.
We have recently found increased fasting and glucose-stimulated C-peptide concentrations in adult renal (1. Dmitrewski et aI., unpublished work) and liver[lII.112] allograft recipients treated with tacrolimus, suggesting increased insulin secretion in response to tissue insulin resistance. Confirmation of this inference is currently under investigation with insulin dose-response studies. As in the case of cyclosporin, normal or increased plasma levels of immunoreactive insulin imply insulin resistance. However, it can be argued that these insulin levels are inappropriately low when the prevailing hyperglycaemia is considered. It follows, therefore, that if the presence of insulin resistance is confirmed this will not necessarily exclude a significant coexisting ~ cell defect in glucose-intolerant or diabetic patients. Indeed, concomitant defects in insulin secretion would also be expected, and data from animal studies provide experimental evidence in support of this possibility.
5.3 Animal Studies
Studies in animals support a suppressive effect of tacrolimus on insulin secretion. Tacrolimus was first shown to have adverse effects on glucose metabolism in vivo in a primate transplant modeI.[l19] Elevated circulating immunoreactive insulin concentrations and the presence of insulin in pancreatic islets on immunohistochemical staining were suggestive of peripheral insulin resistance, and a dose-response effect was evident.[l19] In dogs, however, the same initial dosage of tacrolimus (lmg/kg/day) induced a vasculitisJ1l9] The authors of this study speculated that tacrolimus might be acting as a sympathomimetic agent and that this
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
effect was manifested in different ways in the baboon and the dog. Although no data were presented to support this speculation, it is interesting to note that increased sympathetic neuronal discharges have been reported in heart transplant patients with cyclosporin-associated hypertension. [120) Vascular resistance is increased, although plasma and urinary noradrenaline (norepinephrine) levels are normalJ120)
Strasser et alJ 121) performed glucagon stimulation tests in normal beagles. In contrast to the findings in baboons,D19) a decrease in glucose clearance was accompanied by suppression of insulin secretion after 2 weeks of tacrolimus 1 mg/kg/day which persisted, at least partially, for 4 weeks after the drug was discontinued. Oral and intravenous glucose tolerance were reversibly impaired by tacrolimus in non-transplanted cynomolgus monkeys,D22) although plasma insulin levels were not measured in this study.
In vitro, at low concentrations, tacrolimus does not produce significant impairment of insulin or C-peptide release from rat[123,124) or human[l25,126)
islets. Higher concentrations of the drug decrease glucose-stimulated insulin or C-peptide release from rodent,[124,126,127) canine[l28) and human[l23,125)
islets, and this is associated with impaired intravenous and oral glucose tolerance. Decreased pancreatic insulin content and vacuolation of the islets were observed at high dosages of tacrolimus (10 mg/kg/day),[l29) whereas lower dosages have not been associated with histological changes in rat[130) or human[l23) islets.
To summarise, studies in animals have shown that tacrolimus produces dosage-dependent toxic effects on islet P cells, accompanied by histological changes in some studies, which are partially[l21) or completely[l22,129) reversible on dosage reduc
tion or withdrawal of the drug. However, it should be noted that the inhibition of P cell secretion documented in these animal models has occurred at high concentrations of tacrolimus, greatly exceeding those expected to be achieved in humans at clinically relevant dosages.
© Adls Intemational Umlted. All rights reserved.
6. Molecular Actions of Cyclosporin and Tacrolimus
6.1 Immunophilins and Intracellular Calcium Metabolism
117
Cyclosporin and tacrolimus differ considerably in structure and potency, yet there are striking similarities between the drugs in their biochemical actions within cells,ll3l,132) Although the molecular mechanisms by which cyclosporin and tacrolimus exert their effects on insulin secretion, and possibly insulin action, remain uncertain, theoretical links exist between drug-induced events in T lymphocytes and toxic effects in other tissues. A role for drug-mediated inhibition of the serine-threonine protein phosphatase calcineurin has been proposed,l132) Calcineurin is a component of the signal transduction pathway which results in transcription of the gene encoding the lymphokine interleukin-2.
In T lymphocytes, antigen presentation leads to the generation of inositol trisphosphate and diacylglycerol. Generation of inositol trisphosphate leads to an increase in intracellular calcium (Ca2+) concentration and activation of the Ca2+ - and calmodulindependent regulatory phosphatase calcineurin,l131) It is now known that the phosphatase activity of calcineurin is inhibited by cyclosporin and tacrolimus following intracellular interactions between the drugs and specific binding proteins.
After entering the cell, each drug binds to a specific binding protein known as an immunophilin (the cyclophilin family and FK-506 binding proteins, respectively). The drug/immunophilin complex then binds to calcineurin, thereby inhibiting its phosphatase activity and inhibiting the critical dephosphorylation events required for early lymphokine gene expression.
6.2 Physiology of Insulin Secretion
Insulin secretion from the islet P cell is also a Ca2+ -dependent process, and interference with intracellular Ca2+ metabolism by immunosuppressive agents therefore has theoretical implications for insulin secretion. A rise in intracellular Ca2+ plays a crucial role in stimulus-secretion coupling by
Clln. Immunother. 4 (2) 1995

118
stimulating calmodulin-dependent protein kinases. This results in the phosphorylation of cellular proteins that mediate the initial secretory phase of stored insulin.[l33,134] Hydrolysis of phosphoinositide leads to generation of inositol trisphosphate, which contributes to the rise in intracellular Ca2+
concentration. Concomitant formation of diacylglycerol contributes to the sustained phase of insulin secretion.[l34] Cyclic AMP also plays an important role in regulating the states of phosphorylation of proteins within the ~ cell, acting as a potentiator of nutrient-induced insulin secretion)134] The processing of the insulin precursor proinsulin within the ~ cell is also a Ca2+ -dependent process. The enzyme that catalyses the conversion of proinsulin to its intermediate des-3I ,32-proinsulin requires a local Ca2+ concentration >0.5 mmollL)135]
6,3 Effects of Immunosuppressive Agents on ~ Cell Calcium Metabolism
The literature contains conflicting reports concerning the effect of immunosuppressive agents on ~ cell Ca2+ metabolism. Examining the effects of cyclosporin on ~ cells, Draznin et al.[l36] measured cytosolic Ca2+ changes in isolated islets and found that cyclosporin I mglL decreased Ca2+ influx in the presence of hyper glycaemia (16.7 mmollL). This was accompanied by a significant reduction in insulin release.
Martin and Bedoya[137] provided evidence from in vivo and in vitro studies that cyclosporin inhibits insulin secretion in rats, not by modifying intracellular Ca2+ but via actions on Ca2+ -calmodulindependent phosphodiesterase (reducing cyclic AMP levels) and possibly on regulatory G-proteins (guanine nucleotide binding proteins). These investigators also found an inhibitory effect of cyclosporin on glucagon secretion.
Bartlett et al)138] found no effect of increasing extracellular Ca2+ concentration to nearly 5 mmollL on cyclosporin-induced suppression of ~ cell insulin secretion in vitro. Sulphonylureas such as tolbutamide cause membrane depolarisation, thereby increasing Ca2+ influx into ~ cells. However, no effect was seen from the addition of tolbutamide to
© Adls International Limited. All rights reserved.
Krentz et al.
the perfusate. Decreased pancreatic insulin content and reductions in both phases of insulin secretion led these investigators to conclude that the primary effect of cyclosporin on the ~ cell is inhibition of insulin secretion. Using the inhibitory effect of somatostatin on insulin secretion as an indirect indicator of the glucose-induced rise in intracellular Ca2+ in rat ~ cells, the same investigators[93] found that the response to somatostatin was enhanced by cyclosporin, although glucose-stimulated insulin secretion was reduced. As noted previously, no effect of cyclosporin on arginine-stimulated glucagon secretion was observed.
6,4 Immunosuppressive Agents and Insulin Action
Insulin action in target tissues such as skeletal muscle and liver may also, in part, be mediated by changes in Ca2+ -dependent intracellular processes)139] Diacylglycerol and inositol trisphosphate are generated by the action of a specific phospholipase C bound to the plasma membrane, a process that also might involve G protein signalling. However, the role of phosphoinositol glycan release in the generation of the intracellular actions of insulin remains uncertain. The effects, if any, of cyclosporin and tacrolimus on this putative signalling pathway are unknown. Even for corticosteroids, which have been extensively studied in humans, the molecular mechanisms responsible for tissue insulin resistance remain unclear.
The inhibitory effect of cyclosporin on the production of tumour necrosis factor-a in B lymphocytes (which, incidentally, is another Ca2+
dependent process)[131] is also of interest since this cytokine has been implicated in the pathogenesis of insulin resistance in patients with non-insulindependent diabetes.[140] Tumour necrosis factor-a is a potent inhibitor of insulin-stimulated tyrosine phosphorylations on the ~ chain of the insulin receptor and insulin receptor substrate-I. Accordingly, however, it is increased, rather than decreased, expression of tumour necrosis factor-a that has been implicated in the pathogenesis of insulin resistance.
Clin. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
7. Conclusions and Recommendations
In this article, we have reviewed the evidence that implicates corticosteroids, cyclosporin and tacrolimus in the aetiology of post-transplant diabetes mellitus. However, while the theoretical risks of developing diabetes post-transplantation are now appreciated,P41) the impact of this iatrogenic metabolic syndrome, apart from the occasional development of severe hyperglycaemia and the need for long term insulin therapy in a minority of patients, are uncertain. Since the immunosuppressive drugs that appear to be largely responsible for post-transplant diabetes are modifiable factors, the search for less toxic alternatives should carefully address the metabolic effects of new drugs.
We believe that clinical trials of new immunosuppressive drugs, such as sirolimus (rapamycin) and gusperimus (deoxyspergualin),1141) should incorporate clinically relevant, standardised methods for detecting and categorising abnormalities of glucose tolerance. We have argued elsewhere that the 7Sg oral glucose tolerance test is the most appropriate investigation for this purpose at presentJ142) In addition, further studies are required to determine the pathogenesis of immunosuppressionassociated disturbances of glucose metabolism, and we are currently performing in vivo insulin doseresponse studies in liver transplant recipients treated with tacrolimus or cyclosporin.
Although there are metabolic similarities with IGT and non-insulin-dependent diabetes in nontransplant patients, we have noted intriguing differences in aspects of intermediary metabolism in cyclosporin- and tacrolimus-treated patients. For example, we found that fasting lactate concentrations, which are modestly elevated in nontransplanted patients with IGT[143) or diabetes, were significantly lower than normal in liver transplant patients treated with cyclosporin or tacrolimusJ111) Possibly, liver transplantation per se is associated with unique metabolic abnormalities, and further studies are required in recipients of other organ transplants and non-transplant patients treated with these drugs.
© Adis International limited. All rights reserved.
119
Careful metabolic characterisation and long term follow-up studies will be necessary to determine the clinical implications of glucose intolerance and, in particular, diabetes mellitus in organ transplant recipients, since these patients may be at risk of complications that may reduce postoperative survival.[144,145) The high prevalence of atherosclerotic disease in renal(146) and cardiac(147) transplant patients is a cause for concern and it is, therefore, noteworthy that insulin resistance has been implicated in the pathogenesis of macrovascular disease in nontransplant populations.1148, 149) Moreover, both cyclosporin and tacrolimus are associated with hypertension,1109,1l5,150) and renal(151) and cardiacl l52) transplant patients often have abnormal plasma lipid profiles which are considered to be atherogenic. Increased plasma low density lipoprotein cholesterol concentrations have also been reported in nontransplant patients during cyclosporin therapyJ153)
Thus, organ transplant recipients may have multiple risk factors for atherosclerosis, several of which may be induced or potentiated by immunosuppressive drugs. Although adverse lipid profiles have not invariably been found in cyclosporin- and tacrolimus-treated patients,1154,155) the impact of multiple risk factors for atheroma, including glucose intolerance and hyperinsulinaemia, on long term survival of organ transplant recipients merits further investigation.
More studies of current immunosuppressive agents are required in order to determine dose-response relationships that will maximise beneficial effects while minimising drug-related adverse metabolic effects,c41,156,157) In this regard it should be noted that the optimal dosage for tacrolimus, which has recently become available for clinical use in a number of countries, is presently uncertain.[I09,115,158) Carefully controlled studies will be necessary to achieve these objectives, although it is clear that such studies pose considerable challenges to clinical investigatorsJ159)
Acknowledgements
We wish to thank Paul McMaster, John Buckels, Bertrand Dousset, Janet Smith and Robert Cramb for their collabora-
Clin. Immunother. 4 (2) 1995

120
tion in the studies cited from Binningham. Expert technical assistance was provided by Janet Sherwell. The financial support of Fujisawa GmbH and The Bicentenary Fund of the General Hospital, Birmingham, UK, is gratefully acknowledged.
References I. Starzl TE. Experience in renal transplantation. Philadelphia:
WB Saunders, 1964: II6-7 2. Taylor R. Drugs and diabetes mellitus. In: Williams G, Pickup
JC, editors. Textbook of diabetes. Oxford: Blackwell Scientific Publications, 199 I: 803-8
3. Ferner RE. Drug-induced diabetes. Baillieres Clin Endocrinol Metab 1992; 6: 849-66
4. Kahan BD. Cyclosporine. N Engl J Med 1989; 321: 1725-38 5. Scantlebury V, Shapiro R, Fung J, et al. New onset of diabetes
in FK 506 vs. cyclosporine-treated kidney transplant recipients. Transplant Proc 1991; 23: 3169-70
6. Fung JJ, Alessiani M, Abu-Elmagd K, et al. Adverse effects associated with use of FK 506. Transplant Proc 199 I; 23: 3105-8
7. Thomson AW, Nield GH. CycIosporin: use outside transplantation. BMJ 1991; 302: 4-5
8. Nikolaidis NL, Abu-Elmagd K, Thomson AW, et al. Metabolic effects of FK 506 in patients with severe psoriasis: short term follow-up of seven cases. Transplant Proc 1991; 23: 3325-7
9. Herold KC, Rubenstein AH. Immunosuppression for insulindependent diabetes N Engl J Med 1988; 318: 701-3
10. Carroll PB, Tzakis AG, Ricordi C, et al. The use of FK 506 in new-onset type I diabetes in man. Transplant Proc 1991; 23: 3351-3
I I. Sutherland DER. Pancreatic transplantation: an update. Diabetes Rev 1993; I: 152-65
12. Warnock GL, Kneteman NM, Ryan EA, et ai. Long-term follow-up after transplantation of insulin-producing pancreatic islets into patients with type I (insulin-dependent) diabetes mellitus. Diabetologia 1992; 35: 89-95
13. Krentz AJ, Nattrass M. An introduction to human research. London: The Newbourne Group, 1988: 23-7
14. Elliott MJ, Alberti KGMM. Carbohydrate metabolism - effects of pre-operative starvation and trauma. Clin Anaesthesiol 1983; I: 527-50
15. Brandi LS, Frediani M, Oleggini M, et al. Insulin resistance after surgery: normalization by insulin treatment. Clin Sci 1990; 79: 443-50
16. National Diabetes Data Group. Classification and diagnosis of diabetes mellitus and other categories of glucose intolerance. Diabetes 1979; 28: 1039-57
17. World Health Organization Expert Committee on diabetes mellitus. Technical report series 646. Geneva: World Health Organization, 1980
18. Yudkin JS, Alberti KGMM, McLarty DG, et al. Impaired glucose tolerance. BMJ 1990; 301; 397-402
19. Alford FP, Best JD. The aetiology of type 2 diabetes. In: Nattrass M, editor. Recent advances in diabetes 2. Edinburgh: Churchill Livingtone, 1986: 1-22
20. Mak RHK. Renal disease, insulin resistance, and glucose intolerance. Diabetes Rev 1994; 2: 19-28
2 I. Megyesi C, Samols E, Marks V. Glucose tolerance and diabetes in chronic liver disease. Lancet 1967; 2: 105 1-6
22. Shnueli E, Record Co, Alberti KGMM. Liver disease, carbohydrate metabolism and diabetes. Baillieres Clin Endocrinol Metab 1992; 6: 719-43
© Adis International Um~ed. All rights reserved.
Krentz et al.
23. Johnston DG, Alberti KGMM, Faber OK, et ai. Hyperinsulinism of hepatic cirrhosis: diminished degradation or hypersecretion? Lancet 1977; I: 10-13
24. Ekstrand A, Ahonen J, Gronhagen-Riska C, et al. Mechanisms of insulin resistance after kidney transplantation. Transplantation 1989; 48: 563-8
25. Rizza RA, Mandarino LJ, Gerich JE. Cortisol-induced insulin resistance in man: impaired suppression of glucose production and stimulation of glucose utilization due to a post receptor defect of insulin action. J Clin Endocrinol Metab 1982; 54: 131-8
26. Perley M, Kipnis DM. Effect of glucocorticooids on plasma insulin. N Engl J Med 1966; 274: 1237-41
27. Pagano G, Cavallo-Perin P, Cassader M, et ai. An in vivo and in vitro study of the mechanism of prednisone-induced insulin resistance in healthy subjects. J Clin Invest 1983; 72: 1814-20
28. Boyle PJ. Cushing's disease, glucocorticoid excess, glucocorticoid deficiency, and diabetes. Diabetes Rev 1993; I: 30 1-8
29. Johnston DG, Pernet A, Nattrass M. Hormonal regulation of fatty acid mobilization in normal and diabetic man. In: Nattrass M, Santiago JV, editors. Recent advances in diabetes I. Edinburgh: Churchill Livingstone, 1984: 91-106
30. Ruiz JO, Simmons RL, Callender CO, et ai. Steroid diabetes in renal transplant recipients: pathogenic factors and prognosis. Surgery 1973; 73: 759-65
3 I. Hill CM, Douglas JF, Rajkumar KV, et al. Glycosuria and hyperglycaemia after kidney transplantation. Lancet 1974; 2: 490-2
32. Woods JE, Zincke H, Palumbo PJ, et ai. Hyperosmolar nonketotic syndrome and steroid diabetes: occurrence after renal transplantation. JAMA 1975; 231: 1261-3
33. Gunnarsson R, Arner P, Lundgren G, et ai. Steroid diabetes after renal transplantation - a preliminary report. Scand J Urol Nephrol 1977; 432: 191-4
34. Gunnarsson R, Arner P, Lundgren G, et al. Diabetes mellitus -a more common than believed complication of renal transplantation. Transplant Proc 1979; II: 1280- I
35. McGeown M, Douglas F, Brown W, et aI. Advantages of lowdose steroid from the day after renal transplantation. Transplantation 1980; 229: 287-9
36. David DS, Cheigh JS, Braun DW, et al. HLA-A28 and steroidinduced diabetes in renal transplant recipients. JAMA 1980; 243: 532-3
37. Arner P, Gunnarsson R, Blomdahl S, et aI. Some characteristics of steroid diabetes: a study in renal-transplant recipients receiving high-dose corticosteroid therapy. Diabetes Care 1983; 6: 23-25
38. Friedman EA, Shyh T, Beyer MM, et ai. Posttransplant diabetes in kidney transplant recipients. Am J Nephrol 1985; 5: 196-202
39. Krentz AJ. Diabetic ketoacidosis, hyperosmolarnon-ketotic coma and lactic acidosis. In: Foex P, Garrad C, Westaby S, editors. Principles and practice of critical care. Oxford: Blackwell Scientific. In press
40. D' Apice AJF, Mathews JD, Tait BD, et ai. Association ofHLAantigens with glucose tolerance following renal transplantation. Tissue Antigens 1978; II: 423-6
4 I. Hricik DE, Almawi WY, Strom TB. Trends in the use of corticosteroids in renal transplantation. Transplantation 1994; 57: 979-89
42. Collier StJ, Caine R. Practical problems in immunosuppression: kidney and liver transplants. Prescribers J 1991; 31: 122-7
43. Padbury RTA, Gunnson BK, Dousset B, et ai. Steroid withdrawal from long-term immunosuppression in liver allograft recipients. Transplantation 1993; 55: 789-94
Clln. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
44. Ratcliffe PJ, Firth JD, Higgins RM, et al. Randomized controlled trial of complete steroid withdrawal in renal transplant patients receiving triple immunosuppression. Transplant Proc 1993;25: 590
45. European Multicentre Trial Group. European multicentre trial of cyclosporin in renal transplantation: lO-year follow-up. Transplant Proc 1993; 25: 527-9
46. Gunnarson R, Klintmalm G, Lundgren G, et al. Deterioration in glucose metabolism in pancreatic transplant patients given cyclosporine [letter]. Lancet 1983; 2: 571-2
47. Engfeldt P, Tyden G, Gunnarson R, et al. Impaired glucose tolerance with cyclosporine. Transplant Proc 1986; 18: 65-6
48. Harris KPG, Russell, Parvin SD, et al. Alterations in lipid and carbohydrate metabolism attributable to cyc\osporin A in renal transplant recipients. BMJ 1986; 292: 16
49. Binder C. C-peptide and B-cell function. In: Williams G, Pickup JC, editors. Textbook of diabetes. Oxford: Blackwell Scientific, 1991: 348-54
50. Ost L. Effects of cyclosporin on prednisolone metabolism [letter]. Lancet 1984; I: 451
51. Yagisawa T, Takahashi K, Teraoka S, et al. Deterioration in glucose metabolism in cyclosporine treated kidney transplant recipients and rats. Transplant Proc 1986; 18: 1548-51
52. Boudreaux JP, McHugh L, Canafax DM, et al. The impact of cyclosporine and combination immunosuppression on the incidence of posttransplant diabetes in renal allograft recipients. Transplantation 1987; 44: 376-81
53. Kahan BD, Flechner SM, Lorber MI, et al. Complications of cyclosporine-prednisolone immunosuppression in 402 renal allograft recipients exclusively followed at a single center for from one to five years. Transplantation 1987; 43: 197-204
54. Ost L, Tynden G, Fehrman I. Impaired glucose tolerance in cyclosporin-prednisolone-treated renal graft recipients. Transplantation 1988; 46: 370-2
55. Nakai I, Omori Y, Aikawa I, et al. Effects of cyclosporine on glucose metabolism in kidney transplant recipients. Transplant Proc 1988; 20 Suppl. 3: 969-78
56. Yoshimura N, Nakai I, Ohmori Y, et aI. Effect of cyclosporine on the endocrine and exocrine pancreas in kidney transplant recipients. Am J Kidney Dis 1988; 12: 11-7
57. Mejia G, Arbelaez M, Henao JE, et al. Cyclosporine-associated diabetes mellitus in renal transplants. Clin Transpl 1989; 3: 260-3
58. Roth D, Milgrom M, Esqeunazi V, et aI. Posttransplant hyperglycemia: increased incidence in cyclosporine-treated renal allograft recipients. Transplantation 1989; 47: 278-81
59. Von Kiparksi A, Frei D, Uhlschmid G, et al. Post-transplant diabetes mellitus in renal allograft recipients: a matched pair control study. Nephrol Dial Transplant 1990; 5: 220-5
60. Yamamoto H, Akazawa S, Yagamuchi Y, et al. Effects of cyclosporin A and low dosages of steroid on post-transplantation diabetes in kidney transplant recipients. Diabetes Care 1991; 14: 867-70
61. Surnrani NB, Delany V, Ding Z, et al. Diabetes mellitus after renal transplantation in the cyclosporine era - an analysis of risk factors. Transplantation 1991; 51: 343-7
62. Rao M, Jacob CK, Shastry JCM. Post-renal transplant diabetes mellitus - a retrospective study. Nephrol Dial Transplant 1992; 7: 1039-42
63. Basri N, Aman H, Adiku W, et al. Diabetes mellitus after renal transplantation. Transplant Proc 1992; 24: \780-1
64. Prasad TN, Prakash BS, Subramanyam K, et al. Post-renal transplant diabetes in conventional and cyclosporine regimes. Transplant Proc 1992; 24: 1728
© Adis International Limited. All rights reserved.
121
65. Fryer JP, Granger DK, Leventhal JR, et aI. Steroid-related complications in the cyclosporine era. Clin Transplantation 1994; 8: 224-9
66. Harris MI. Diabetes in Hispanics, Whites and Blacks in the US population: epidemiologic correlates. Diabetes Care 1991; 14 Suppl. 3: 39-48
67. Ekstrand AV, Eriksson JG, Gronhagen-Riska C, et al. Insulin resistance and insulin deficiency in the pathogenesis of posttransplantation diabetes in man. Transplantation 1992; 53: 563-9
68. Yamasaki Y, Takahashi K, Yagisawa T, et al. Alterations in glucose tolerance and insulin release in renal transplant recipients receiving cyclosporine and corticosteroids. Transplant Proc 1988; 20 Suppl. I: 158-9
69. Bending JJ, Ogg CS, Viberti GC. Diabetogenic effect of cyclosporine. BMJ 1987; 294: 410-1
70. Blackman JD, Polonsky KS, Jaspan JB, et al. Insulin secretory profiles and C-peptide clearance kinetics at 6 months and 2 years after kidney-pancreas transplantation. Diabetes 1992; 41: 1346-52
71. Luzi L, Secchi A, Facchini F, et al. Reduction of insulin resistance by combined kidney-pancreas transplantation in type I (insulin-dependent) diabetic patients. Diabetologia 1990; 33: 549-56
72. Robertson RP. Pancreas transplantation in humans with diabetes mellitus. Diabetes 1991; 40: 1085-9
73. Radziuk J, Barron P, Najm H, et al. The effect of systemic venous drainage of the pancreas on insulin sensitivity in dogs. J Clin Invest 1993; 93: \713-21
74. Yki-Jarvinen H. Pathogenesis of non-insulin-dependent diabetes. Lancet 1994; 343: 91-5
75. Dinneen S, Gerich J, Rizza R. Carbohydrate metabolism in noninsulin-dependent diabetes mellitus. N Engl J Med 1993; 327: 707-13
76. Temple R, Clark PMS, Hales CN. Measurement of insulin secretion in type 2 diabetes. Problems and pitfalls. Diabetic Med 1992; 9: 503-12
77. Esmatjes E, Ricart MJ, Ferrer JP, et al. Cyclosporin's effect on insulin secretion in patients with kidney transplants. Transplantation 1991; 52: 500-3
78. Ward WK, LaCava EC, Paquette TL, et al. Disproportionate elevation of immunoreactive proinsulin in type 2 (non-insulindependent) diabetes mellitus and in experimental insulin resistance. Diabetologia 1987; 30: 698-702
79. Garvin PJ, Niehoff M, Staggenborg J. Cyclosporine's effect on canine pancreatic endocrine function. Transplantation 1988; 45: 1027-31
80. Yale J-F, Chamelian M, Courschesne S, et al. Peripheral insulin resistance and decreased insulin secretion after cyclosporine treatment. Transplant Proc 1988; 20 Suppl. 3: 985-8
81. Alejandro R, Feldman EC, Bloom AD, et al. Effects of cyclosporin on insulin and C-peptide secretion in healthy beagles. Diabetes 1989; 38: 698-703
82. Dresner LS, Andersen DK, Kahng KU, et aI. Effects of cyclosporine on glucose metabolism. Surgery 1989; 106: 163-70
83. Riegel W, Brehmer D, Thaiss F, et al. Effect of cyclosporin A on carbohydrate metabolism in the rat. Transpl Int 1989; 2: 8-12
84. Wahlstrom HE, Akimoto R, Endres D, et al. Recovery and hypersecretion of insulin and reversal of insulin resistance after withdrawal of short term cyclosporin treatment. Transplantation 1992; 53: 1190-5
Clin. Immunother. 4 (2) 1995

122
85. Helmchen U, Schmidt WE, Siegel EG, et al. Morphological and functional changes of pancreatic B cells in cyclosporin Atreated rats. Diabetologia 1984; 27: 416-8
86. Andersson A, Borg H, Hallberg A, et al. Long-term effects of cyclosporin A on cultured mouse pancreatic islets. Diabetologia 1984; 27: 66-9
87. Robertson RP. Cyclosporin-induced inhibition of insulin secretion in isolated rat islets and HIT cells. Diabetes 1986; 35: 1016-9
88. Hahn HJ, Dunger A, Laube F, et al. Reversibility of the acute toxic effect of cyclosporin A on pancreatic B cells of Wistar rats. Diabetologia 1986; 29: 489-94
89. Eun H-M, Pak C-Y, Kim C-J, et al. Role of cyclosporin A in macromolecular synthesis of B-cells. Diabetes 1987; 36: 952-8
90. Nielsen JH, Mandrup-Poulsen T, Nerup 1. Direct effects of cyclosporin A on human pancreatic beta-cells. Diabetes 1986; 35: 1049-52
91. Chandrasekar B, Mukherjee SK. Effect of prolonged administration of cyclosporin A on (pro )insulin biosynthesis and insulin release by rat islets of Langerhans. Biochem Pharmacol 1988; 37: 3609-11
92. Gillison SL, Bartlett ST, Curry DL. Synthesis-secretion coupling of insulin: effect of cyclosporin. Diabetes 1989; 38: 465-70
93. Gillison SL, Bartlett ST, Curry DL. Inhibition by cyclosporine of insulin secretion - a beta cell-specific alteration of islet tissue function. Transplantation 1991; 52: 890-5
94. Sestior C, Odert-Pogo S, Bonneville M, et al. Cyclosporin enhances diabetes induced by low-dose streptozotocin treatment in mice. Immunol Lett 1985; 10: 57-60
95. Pollock SM, Reichbaum MI, Collies BM, et al. Inhibitory effect of cyclosporin A on the activity of oral hypoglycemic agents in rats. J Pharmacol Exp Ther 1991; 258: 8-12
96. Runzi M, Peskar BM, von Schonfield S, et al. Importance of endogenous prostaglandins for the toxicity of cyclosporin A to rat endocrine and exocrine pancreas. Gut 1992; 33: 1572-7
97. Muller MK, Wojzck M, Runzi M, et al. Cytoprotection and dose-dependent inhibitory effects of prostaglandin E I on rat pancreas treated with cyclosporin A. Digestion 1991; 50: 29-36
98. Robertson RP, Franklin G, Nelson L. Intravenous glucose tolerance and pancreatic islet beta-cell function in patients with multiple sclerosis during 2-yr treatment with cyclosporin. Diabetes 1989; 38: 58-64
99. Teuscher AU, Sequist ER, Robertson RP. Diminished secretory reserve in diabetic pancreas transplant and nondiabetic kidney transplant recipients. Diabetes 1994; 43: 593-8
100. Starzl TE, Todo S, Fung T, et al. FK506 for liver, kidney, and pancreatic transplantation. Lancet 1989; 2: 1000-4
101. Todo S, Fung JJ, Starzl TE, et al. Liver, kidney, and thoracic organ transplantation under FK 506. Ann Surg 1990; 212: 295-305
102. Starzl TE, Fung J, Jordan M, et al. Kidney transplantation under FK 506. JAMA 1990; 264: 63-7
103. Mieles L, Todo S, Fung JJ, et al. Oral glucose tolerance test in liver recipients treated with FK 506. Transplant Proc 1990; 22: 41-3
104. Mieles L, Gordon RD, Mintz D, et al. Glycemia and insulin need following FK 506 rescue therapy in liver transplant recipients. Tranplant Proc 1991; 23: 949-53
105. Carroll PB, Rilo H, Reyes J, et al. FK 506-associated diabetes in the pediatric population is a rare complication. Transplant Proc 1991; 23: 3171-2
© Adls International Limited. All rights reserved.
Krentz et al.
106. Tabasco-Minguillan J, Mieles L, Carroll P, et al. Long-term insulin requirement after liver transplantation in American veterans. Transplant Proc 1993; 25: 677-8
107. Tabasco-Minguillan J, Mieles L, Carroll P, et al. Insulin requirements after liver transplantation and FK-506 immunosuppression. Transplantation 1993; 56: 862-7
108. Ericzon B, Groth C, Bismuth H, et al. Glucose metabolism in liver transplant recipients treated with FK 506 or cyclosporin in the European multicentre study. Transpl Int 1994; 7 Suppl. I: Sl1-4
109. European FK506 Multicentre Liver Study Group. Randomised trial comparing tacrolimus (FK506) and cyclosporin in prevention of liver allograft rejection. Lancet 1994; 344: 423-8
110. O'Grady JG, Forbes A, Rolles K, et al. An analysis of cyclosporine efficacy and toxicity after liver transplantation. Transplantation 1988; 45: 575-9
111. Krentz AJ, Dousset B, Mayer D, et al. Metabolic effects of cyclosporin A and FK 506 in liver transplant recipients. Diabetes 1993; 42: 1753-9
112. Krentz AJ, Dmitrewski J, Mayer AD, et al. Postoperative glucose metabolism in liver transplant recipients: a two year randomized prospective study of cyclosporine versus FK 506. Transplantation 1994; 57: 1666-9
113. Hricik DE, Bartucci MR, Moir EJ, et al. Effects of steroid withdrawal on posttransplant diabetes mellitus in cyclosporinetreated transplant recipients. Transplantation 1991; 51: 374-7
114. Jindal RM, Popescu I, Schwartz ME, et al. Diabetogenicity of FK506 versus cyclosporin in liver transplant recipients. Transplantation 1994; 58: 370-2
115. The US Multicenter FK 506 Liver Study Group. A comparison of tacrolimus (FK 506) and cyclosporine for immunosuppression in liver transplantation. N Engl J Med 1994; 331: 1110-5
116. Collins RH. Tacrolimus (FK 506) versus cyclosporin in prevention of liver allograft rejection [letter]. Lancet 1994; 344: 949
117. Bone AJ, Walker R, Varey A-M, et al. Effect of cyclosporin on pancreatic events and development of diabetes in BBI Edinburgh rats. Diabetes 1990; 39: 508-14
118. Murase N, Lieberman I. Nalesnik MA, et al. Effect of FK506 on spontaneous diabetes in BB rats. Diabetes 1990; 39: 1584-6
119. Collier DStJ, CaIne R, Thiru S, et al. FK-506 in experimental renal allografts. Transplant Proc 1987; 19: 3975-7
120. Scherrer U, Vissing SF, Morgan BJ, et al. Cyclosporine-induced sympathetic activation and hypertension after heart transplantation. N Engl J Med 1990; 323: 693-9
121. Strasser S, Alejandro R, Ricordi C, et al. The effect of FK 506 on canine pancreatic islet function in beagle dogs. Transplant Proc 1991; 23: 756-7
122. Ericzon B-G, Wijnen RMH, Kubota K, et al. FK 506-induced impairment of glucose metabolism in the primate - studies in pancreatic transplant recipients and non-transplanted animals. Transplantation 1992; 54: 615-20
123. Tze WJ, Tai J, Cheung S. In vitro effects of FK-506 on human and rat islets. Transplantation 1990; 49: 1172-4
124. Carroll PB, Boschero AC, Li M-Y, et al. Effect of the immunosuppressant FK 506 on glucose-induced insulin secretion from adult rat islets oflangerhans. Transplantation 1991; 51: 275-8
125. Ricordi C, Zeng Y, Alejandro R, et al. In vivo effect of FK 506 on human pancreatic islets. Transplantation 1991; 52: 519-22
126. Rilo HLR, Zeng R, Alejandro R, et al. Effect of FK 506 on function of human islets oflangerhans. Transplant Proc 1991; 23: 3164-5
127. Tze WJ, Tai J, Murase N, et al. Effect of FK 506 on glucose metabolism and insulin secretion in normal rats. Transplant Proc 1991; 23: 3158-60
Clln. Immunother. 4 (2) 1995

Immunosuppressants and Post-Transplant Diabetes
128. Ishizuki J, Gugliuzza KK, Wassmuth Z, et al. Effects ofFK506 and cyclosporine on dynamic insulin secretion from isolated dog pancreatic islets. Transplantation 1993; 56: 1486-90
129. Hirano Y, Fujihira S, Ohara K, et al. Morphological and functional changes of islets of langerhans in FK506-treated rats. Transplantation 1992; 53: 889-94
130. Haba T, Hachisuka T, Ohtsuka S, et al. Pathological and immunohistochemical examination in the rat treated with FK 506. Transplant Proc 1991; 23: 2229-32
131. Schreiber SL, Crabtree GR. The mechanism of action of cyclosporin A and FK 506. Immunol Today 1992; 13: 136-42
132. Wiederrecht G, Lam E, Hung S, et al. The mechanism of action ofFK 506 and cyclosporin. Ann NY Acad Sci 1993; 696: 9-19
133. Howell SL. Insulin biosynthesis and secretion. In: Williams G, Pickup JC, editors. Textbook of diabetes. Oxford: Blackwell Scientific, 1991: 72-83
134. Rasmussen H, Zawalich KC, Ganesan S, et al. Physiology and pathophysiology of insulin secretion. Diabetes Care 1990; 13: 655-66
135. Rhodes CJ, Alarcon C. What beta-cell defect could lead to hyperproinsulinemia in NIDDM? Diabetes 1994; 43: 511-7
136. Draznin B, Metz SA, Sussman KE, et al. Cyclosporin-induced inhibition of isnulin release: possible role of voltage-dependent calcium transport channels. Biochem Pharmacol 1988; 37: 3941-5
137. Martin F, Bedoya FJ. Mechanisms of action of cyclosporin A on islet alpha- and beta-cells. Effects of cAMP- and calciumdependent pathways. Life Sci 1991; 39: 1915-21
138. Bartlett ST, Gillison SL, Curry DL. Cyclosporine inhibition of insulin secretion: effect of tolbutamide and extracellular calcium concentration. Transplant Proc 1990; 22: 749-53
139. Saltiel AR. Second messengers of insulin action. Diabetes Care 1990; 13: 244-56
140. Hotamisligil GS, Spiegelman BM. Tumour necrosis factor-a: a key component of the obesity-diabetes link. Diabetes 1994; 43: 1271-8
141. Jindal RM. Posttransplant diabetes mellitus - a review. Transplantation 1994; 58: 1289-98
142. Krentz AJ, Dmitrewski J, Mayer D, et al. Tacrolimus (FK 506) versus cyclosporin in prevention of liver allograft rejection [letter]. Lancet 1994; 344: 948-9
143. Krentz AJ, Singh BM, Hale PJ, et al. Basal intermediary metabolism in impaired glucose tolerance and morbid obesity. Diabetes Res 1992; 20: 51-60
144. Nathan DM. Long-term complications of diabetes mellitus. N Engl J Med 1993; 328: 1676-85
145. Panzram G. Mortality and survival in type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia 1987; 30: 123-31
© Adis International Limited. All rights reserved.
123
146. Suthanthiran M, Strom TB. Renal transplantation. N Engl J Med 1994; 331: 365-76
147. Uretsky BF, Murali S, Reddy PS, et al. Development of coronary artery disease in cardiac transplant patients receiving immunosuppressive therapy with cyclosporin and precfnisolone. Circulation 1987; 76: 827-34
148. Reaven GM. Role of insulin resistance in human disease. Diabetes 1988; 37: 1595-607
149. DeFronzo RA, Ferrannini E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care 1991; 14: \73-94
150. Bennett WM, Porter GA. Cyclosporine-associated hypertension. AmJ Med 1988; 85: 131-3
151. Editorial. Hyperlipidaemia after renal transplantation. Lancet 1988; 1: 919-20
152. Barbir M, Kushwaha S, Hunt B, et al. Lipoprotein(a) and accelerated coronary artery disease in cardiac transplant patients. Lancet 1992; 340: 1500-2
153. Ballantyne CM, Podet EJ, Patsch Wp, et al. Effects of cyclosporine therapy on plasma lipoprotein levels. JAMA 1989; 262: 53-6
154. Krentz AJ, Cramb R, Douset B, et al. Serum lipids and apolipoproteins in liver transplant recipients: a comparative study of cyclosporin A and FK 506. J Lab Clin Med 1994; 124: 381-5
155. Jindal RM, Popescu I, Emre S, et al. Serum lipid changes in liver transplant recipients in a prospective trial of cyclosporin versus FK506. Transplantation 1994; 57: 1395-8
156. Oplez G. Effect of the maintenance immunosuppressive drug regimen on kidney transplant outcome. Transplantation 1994; 58: 443-6
157. Hollander AAMJ, van Saase JLCM, Kootte AMM, et al. Beneficial effects of conversion from cyclosporin to azathioprine after kidney transplantation. Lancet 1995; 345: 610-4
158. Schleibner S, Krauss M, Wagner K, et al. FK 506 versus cyclosporin in the prevention of renal allograft rejection - European pilot study: six week results. Transpl Int 1995; 8: 86-90
159. Schlitt HJ, Pilchmayr R. Increasing the long-term success of renal transplantation. Lancet 1995; 345: 600-1
Correspondence and reprints: Dr Andrew J. Krentz, Royal South Hants Hospital, Brintons Terrace, Southampton S014 OYG, England.
Clln. Immunother. 4 (2) 1995







![Glucose Metabolism Is Required for Platelet ... · Glucose Metabolism To determine glucose uptake, washed platelets in 1 mmol/L glucose DMEM were incubated with 10 mmol/L [3H]2-deoxy-D-glucose](https://static.fdocuments.us/doc/165x107/5f7630d406ba0e330e387389/glucose-metabolism-is-required-for-platelet-glucose-metabolism-to-determine.jpg)