Effects of dorsolateral spinal lesions on stretch reflex threshold and stiffness in awake cats
6
European Journal of Neuroscience, Vol. 11, pp. 363–368, 1999 © European Neuroscience Association SHORT COMMUNICATION Effects of dorsolateral spinal lesions on stretch reflex threshold and stiffness in awake cats Julian Taylor, John Munson and Charles Vierck, Jr Department of Neuroscience, University of Florida, Gainesville, FL 32610, Florida, USA Keywords: consciousness, ketamine, spasticity, spinal cord injury, triceps surae Abstract Measurements of threshold angle and incremental dynamic stiffness (IDS) were derived from triceps surae stretch reflexes, elicited by ramp and hold flexion at the ankle joint of four cats that were tested while awake. Stretch reflexes were assessed from trials that began from different ankle joint start positions or were matched using a post-hoc analysis for initial background force during testing sessions before and following unilateral lesions of the dorsolateral funiculus at levels ranging from T13 to L3. Unilateral lesions of the dorsolateral funiculus (DLF) produced significant ipsilateral decreases in stretch reflex threshold and increases in reflex gain, measured as incremental dynamic stiffness (IDS). ANCOVA testing indicated that the reduction in threshold, but not the increase in IDS, was dependent upon the level of background force. Reflex testing from different start angles demonstrated that DLF lesions diminished the correlation between threshold and IDS. Intravenous infusion of ketamine dose-dependently reduced IDS, compared with testing in the unanaesthetized state. Postoperative reflex testing during infusion of ketamine at 22.2 mg/kg per h, when electromyographic responses were reduced to 24% of control levels, abolished differences in IDS between the ipsilateral and contralateral hindlimbs. These and related observations suggest that the postoperative increase in IDS in awake animals was not due to an increase in passive stiffness. Introduction Stretch hyper-reflexia following central injury has been suggested to reflect either a decrease in threshold (Powers et al., 1989) or an increase in gain (Thilmann et al., 1991). However, direct evidence for these effects has not been obtained in other studies, regardless of whether the initial load (background force) for spastic human subjects was unmatched (Rack et al., 1984) or matched (Lee et al., 1987; Sinkjaer et al., 1993; Sinkjaer & Magnussen, 1994) with the load on muscles of normal subjects. In animal models of reflex pathology, changes in reflex threshold but not in the slope of the length–tension curve (gain) have been noted following decerebration (Matthews, 1959; Feldman & Orlovsky, 1972) or in reduced preparations following lateral spinal hemisection (Fujimori et al., 1966). However, small changes in the length–tension relationship have been observed in other studies when muscle stretch is combined with vestibular stimulation (Kim & Partridge, 1969), during activation of the red nucleus (Nichols & Steeves, 1986) and by activation of heterogenic reflex pathways (Nichols, 1989). Also, administration of baclofen has been demonstrated to concurrently attenuate stretch reflex gain and increase threshold in the decerebrate cat (Capaday, 1995). Dorsal spinal lesions in cats have been utilized to model spasticity (Heckman, 1994), but physiological characterizations of the lesion effect have been conducted after acute decerebration, which modifies modulatory influences on spinal reflexes. The present study utilized Correspondence: J. S. Taylor, Instituto Cajal, Avenida Doctor Arce, 37, 28002 Madrid, Spain. E-mail: [email protected] Received 5 May 1998, revised 22 September 1998, accepted 28 September 1998 a model of stretch hyper-reflexia which permits evaluation of reflex threshold and gain in awake cats, before and after dorsolateral spinal lesions (Taylor et al., 1997). An important consideration in the attempt to determine whether threshold and gain are influenced separately or alike by different experimental manipulations is that background force was evaluated, to insure that the activation level of the motoneuron pool was at a comparable level before and after injury (Hoffer et al., 1990). Moreover, some investigations have suggested that an increase in passive stiffness, but not increased reflex gain, is responsible for spasticity (Deitz et al., 1981; Sinkjaer et al., 1993; Sinkjaer & Magnussen, 1994). Accordingly, reflex measures were recorded during ketamine anaesthesia, to determine whether effects of the spinal injury on reflexes were mediated by a neural component. Materials and methods Four adult female cats were trained to accept restraint in a support harness. Both hindpaws were placed in ‘boots’ that could be oscillated by a motor and cam system, applying ramp-and-hold flexion at the ankle joint (Taylor et al., 1997). Bilateral triceps surae stretch reflex activity was monitored by force transducers located under the plantar pads, and also from chronic electromyographic (EMG) electrodes implanted previously during halothane anaesthesia into the soleus (SOL) and medial gastrocnemius (MG) muscles. Angular displace- ment was produced by a DC motor controlled by an analogue circuit, working through adjustable cogs and a flywheel that specified the initial joint angle start position and the degree of displacement (20– 43°). Reflexes were recorded following angular displacement at a velocity of 60°/s, either from a neutral foot-tibial angle of 120° or
-
Upload
julian-taylor -
Category
Documents
-
view
214 -
download
0
Transcript of Effects of dorsolateral spinal lesions on stretch reflex threshold and stiffness in awake cats

European Journal of Neuroscience, Vol. 11, pp. 363–368, 1999 © European Neuroscience Association
SHORT COMMUNICATIONEffects of dorsolateral spinal lesions on stretch reflexthreshold and stiffness in awake cats
Julian Taylor, John Munson and Charles Vierck, JrDepartment of Neuroscience, University of Florida, Gainesville, FL 32610, Florida, USA
Keywords: consciousness, ketamine, spasticity, spinal cord injury, triceps surae
Abstract
Measurements of threshold angle and incremental dynamic stiffness (IDS) were derived from triceps surae stretch reflexes, elicitedby ramp and hold flexion at the ankle joint of four cats that were tested while awake. Stretch reflexes were assessed from trialsthat began from different ankle joint start positions or were matched using a post-hoc analysis for initial background force duringtesting sessions before and following unilateral lesions of the dorsolateral funiculus at levels ranging from T13 to L3. Unilaterallesions of the dorsolateral funiculus (DLF) produced significant ipsilateral decreases in stretch reflex threshold and increases inreflex gain, measured as incremental dynamic stiffness (IDS). ANCOVA testing indicated that the reduction in threshold, but not theincrease in IDS, was dependent upon the level of background force. Reflex testing from different start angles demonstrated thatDLF lesions diminished the correlation between threshold and IDS. Intravenous infusion of ketamine dose-dependently reducedIDS, compared with testing in the unanaesthetized state. Postoperative reflex testing during infusion of ketamine at 22.2 mg/kg perh, when electromyographic responses were reduced to 24% of control levels, abolished differences in IDS between the ipsilateraland contralateral hindlimbs. These and related observations suggest that the postoperative increase in IDS in awake animals wasnot due to an increase in passive stiffness.
Introduction
Stretch hyper-reflexia following central injury has been suggested toreflect either a decrease in threshold (Powerset al., 1989) or anincrease in gain (Thilmannet al., 1991). However, direct evidencefor these effects has not been obtained in other studies, regardless ofwhether the initial load (background force) for spastic human subjectswas unmatched (Racket al., 1984) or matched (Leeet al., 1987;Sinkjaeret al., 1993; Sinkjaer & Magnussen, 1994) with the load onmuscles of normal subjects.
In animal models of reflex pathology, changes in reflex thresholdbut not in the slope of the length–tension curve (gain) have beennoted following decerebration (Matthews, 1959; Feldman & Orlovsky,1972) or in reduced preparations following lateral spinal hemisection(Fujimori et al., 1966). However, small changes in the length–tensionrelationship have been observed in other studies when muscle stretchis combined with vestibular stimulation (Kim & Partridge, 1969),during activation of the red nucleus (Nichols & Steeves, 1986) andby activation of heterogenic reflex pathways (Nichols, 1989). Also,administration of baclofen has been demonstrated to concurrentlyattenuate stretch reflex gain and increase threshold in the decerebratecat (Capaday, 1995).
Dorsal spinal lesions in cats have been utilized to model spasticity(Heckman, 1994), but physiological characterizations of the lesioneffect have been conducted after acute decerebration, which modifiesmodulatory influences on spinal reflexes. The present study utilized
Correspondence: J. S. Taylor, Instituto Cajal, Avenida Doctor Arce, 37, 28002Madrid, Spain. E-mail: [email protected]
Received 5 May 1998, revised 22 September 1998, accepted 28 September 1998
a model of stretch hyper-reflexia which permits evaluation of reflexthreshold and gain in awake cats, before and after dorsolateral spinallesions (Tayloret al., 1997). An important consideration in the attemptto determine whether threshold and gain are influenced separately oralike by different experimental manipulations is that backgroundforce was evaluated, to insure that the activation level of themotoneuron pool was at a comparable level before and after injury(Hoffer et al., 1990). Moreover, some investigations have suggestedthat an increase in passive stiffness, but not increased reflex gain, isresponsible for spasticity (Deitzet al., 1981; Sinkjaeret al., 1993;Sinkjaer & Magnussen, 1994). Accordingly, reflex measures wererecorded during ketamine anaesthesia, to determine whether effectsof the spinal injury on reflexes were mediated by a neural component.
Materials and methods
Four adult female cats were trained to accept restraint in a supportharness. Both hindpaws were placed in ‘boots’ that could be oscillatedby a motor and cam system, applying ramp-and-hold flexion at theankle joint (Tayloret al., 1997). Bilateral triceps surae stretch reflexactivity was monitored by force transducers located under the plantarpads, and also from chronic electromyographic (EMG) electrodesimplanted previously during halothane anaesthesia into the soleus(SOL) and medial gastrocnemius (MG) muscles. Angular displace-ment was produced by a DC motor controlled by an analogue circuit,working through adjustable cogs and a flywheel that specified theinitial joint angle start position and the degree of displacement (20–43°). Reflexes were recorded following angular displacement at avelocity of 60°/s, either from a neutral foot-tibial angle of 120° or

364 J. Tayloret al.
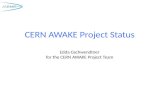
FIG. 1. (A) Stretch reflex force and EMGreflex activity from the medial gastrocnemiusmuscle of cat 3 with background forcematched for trials obtained preoperatively(control) and 4 weeks following ipsilateralspinal surgery (SCI). The responses wereevoked by an angular displacement of 25°from a foot-tibial angle of 120°. Thr., thresholdangle; Stiff., incremental dynamic stiffness;Lat., latency; Vel., velocity; Hold Lat., holdlatency of displacement ramp. (B,C)Relationships of threshold angle andincremental dynamic stiffness with backgroundforce are shown for three cats before (control)and after ipsilateral interruption of thedorsolateral column (SCI; triangles: cat 2 at9 weeks postlesion; circles: cat 3 at 3 weekspostlesion; squares: cat 4 at 7 weekspostlesion). Responses evoked by 30°displacements during single sessions in whichinitial foot–tibial angles of 143, 120 and 105°produced mean background forces of94 6 12 g and 1416 19 g pre- and postlesion.The mean values for threshold angle orstiffness are indicated on the ordinates of Band C by filled triangles for preoperativetesting or open triangles for postoperativetesting. Postoperatively, there was a significantdecrease in threshold angle and an increase inincremental dynamic stiffness.
from greater (143°) or smaller (105°) foot–tibial angles. Manualmanipulation of the angular start position facilitated an analysis ofthe relationship between initial background triceps surae muscle forceat rest and several evoked reflex parameters obtained followingcontrolled ankle joint displacement. Initial background force wasmeasured during the first 0.1 s of each trial, before reflex activitywas produced by ankle movement.Post-hocanalysis of reflex activitywas performed for each animal by utilizing trials in which the initialbackground forces overlapped for preoperative and postoperativetesting, or by matching background forces within6 10%.
At matched background force resting SOL and MG EMG activityis comparable before and after T13–L3 lesions (Tayloret al., 1997).Furthermore, the preoperative ratio of dynamic reflex force to totalEMG activity was equal to the postoperative ratio. It was thereforeunlikely that the state of triceps surae muscles at matched backgroundforces was different before and after lesion. The full range ofbackground forces that are observed in the normal state (Hofferet al.,1990) was not utilized, because postoperative hyper-reflexia was notobserved when the initial foot–tibial angle was decreased to 105°.
Recordings of EMG activity and reflex force were filtered with abandwidth of 3–500 Hz and sampled at 1.48 kHz, using an analogue-to-digital converter. The EMG signals were rectified and filteredfurther by ensemble averaging over six responses. Dynamic reflexamplitude was measured at the time at which the ramp phase ofstretch terminated. Static amplitude was measured at 1.5 s followingramp termination. EMG threshold latency (in seconds) was calculatedby deriving the time at which the EMG amplitude exceeded 50% ofthe mean 0.1 s background activity. Incremental dynamic EMG slope(µV/s) was calculated from the increment in amplitude over 10–90%of the time between threshold and the time at which the ramp phaseterminated. However, these EMG measures were highly variable ona weekly basis, and so we followed the recommendation outlined ina review by Katz & Rymer (1989) and derived threshold frommechanical measurements, which was more suitable for a longitudinalstudy. Threshold angle (the joint angle at which 50 g of force wasproduced) and incremental dynamic stiffness (the slope of the
© 1999 European Neuroscience Association,European Journal of Neuroscience, 11, 363–368
relationship between dynamic force and excursion) were also calcu-lated. The latency at which 50 g of reflex force was produced wasidentified, because all peak dynamic reflex measures well exceededthis level. Incremental dynamic stiffness was calculated over 10–90%of the time between threshold and the time at which the ramp phaseterminated. Incremental dynamic stiffness was taken as a measure ofthe length–tension relationship (Grillner, 1972) and of reflex gain(Kernell, 1993). Owing to a mechanical fault, threshold reflex datawere not available throughout the testing period for cat 4, but dataobtained at 7 weeks postlesion are presented in Fig. 1B.
Following collection of stable baseline data, the dorsolateral column(DLF) of the trained cats was interrupted (with minor damage to thedorsal column) at spinal levels ranging from T13–L3, using fullysterile procedures and deep surgical anaesthesia. The effect ofintravenous (i.v.) infusion of ketamine HCl was determined for alarger group of seven cats, including cats 2–4. Induction of anaesthesiawas implemented with ketamine (10 mg/kg, i.v.); the trachea wasintubated, and the cat was placed in the stretch reflex apparatus(Taylor et al., 1993). Reflex testing was conducted during infusionof ketamine at rates of 10 and 22.2 mg/kg per h. Terminal studieswere performed with two cats in the presence of pancuronium bromideand 10.0 mg/kg/h ketamine hydrochloride, with respiration and bodytemperature being assisted with a respirator and heat blanket,respectively.
Statistical analysis utilized a combination oft-tests,ANOVA andANCOVA. Correlation coefficients and linear regression slopes wereobtained with computer software (CSS-Statistica), and significancewas defined at the 5% level.
Results
An increase in incremental dynamic stiffness following ipsilateralinterruption of the dorsolateral column was observable on mechano-graphic records of preoperative and postoperative trials with matchedbackground force levels (e.g. Fig. 1A). Although an effect on thresholdangle was not apparent from visual inspection of reflex responses,

Stretch reflex threshold and stiffness following spinal lesions 365
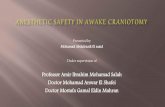
FIG. 2. Case studies of the effects of unilateralspinal lesions on reflex threshold andincremental dynamic stiffness as a function ofoverlapping background forces. Representativetransverse sections at the level of spinal injuryare presented in the left column; the lesions ofthree cats extended 1–2 mm in the rostral–caudal dimension, and the lesion for cat 4 was5 mm in length. Reflex activity was elicited by30° displacement from the neutral start angleof 120°. Ipsilateral interruption of thedorsolateral column produced a significantdecrease in threshold and an increase instiffness for each cat (threshold data for cat 4are not presented due to technical problemswith the axle potentiometer). Filled symbols,preoperative; open symbols, postoperative, asin Fig. 1. The filled and hollow triangles onthe ordinate of each scatterplot indicate themean values for preoperative and postoperativedata.
postoperative reductions of threshold angle were detected by digitalanalysis.
Preoperative and postoperative testing sessions involving 30°displacements from each of the three ankle start positions that imposeddifferent levels of background force were used to evaluate reflexresponses of three cats (Fig. 1B,C). These conditions producedoverlapping ranges of background force and were associated with anincrease in dynamic reflex amplitude from 4616 92 g preoperativelyto 6816 73 g postoperatively (pairedt 5 3.00,P 5 0.018, d.f.5 8).Also, the plots in Fig. 1B,C illustrate linear relationships betweeninitial background force and threshold and between initial back-ground force and IDS, before and after dorsolateral spinal lesions.Accordingly, there was a significant increase in IDS, from 226 4 to30 6 3 g/° (pairedt 5 2.33,P , 0.048, d.f.5 8), and threshold angledecreased from 8.06 2.2° to 3.56 1.2° (pairedt 5 2.29,P 5 0.052).Initial background force was a significant covariate of the reductionin threshold (ANCOVA, P , 0.05) but not of the increase in IDS
© 1999 European Neuroscience Association,European Journal of Neuroscience, 11, 363–368
following dorsolateral lesions. Incremental dynamic stiffness andthreshold were significantly correlated preoperatively (r 5 – 0.72,P , 0.05), but not postoperatively (r 5 – 0.50).
Using data from testing sessions conducted up to 10 monthspostoperatively, the effects of dorsolateral lesions on IDS and thresholdfor 30° displacements from an initial ankle joint of 120° were analysedfor individual animals (Fig. 2 and Table 1B) and across animals. Forindividual analyses, preoperative and postoperative background forceswere not matched, but considerable overlap was present for cats 1and 3 (Fig. 2). For the limb ipsilateral to dorsolateral spinal injury,reflex threshold was reduced postoperatively (Table 1B; postoperativedata unavailable for cat 4; overall analysis,F 5 47.28,P , 0.0001,d.f. 5 1,53), and IDS significantly increased for each cat (Table 1B;overall analysis,F 1,1005 28.31,P , 0.0001).
Post-hocexamination of data matched for background forces duringpre- and postlesion testing revealed significant effects of the lesionson IDS and reflex threshold (Table 1 A), but neither the latency of

366 J. Tayloret al.
TABLE 1. Mean threshold and stiffness, before (preoperative) and up to 10 months after ipsilateral lesions of the dorsolateral funiculus. Data obtained using 30°angular displacements from the ankle start angle of 120°, during conditions when background forces were matched or were in a comparable range (mean6 SE;*two tailed t-test,P , 0.05). Threshold data unavailable from cat 4
Initial background force (g) Threshold angle (deg) Incremental dynamic stiffness (g/deg)
Preoperative Postoperative Preoperative Postoperative Preoperative Postoperative
A. Matched background force
Total (n 5 4) 566 11 576 11 4.96 0.7 2.36 0.4* 216 3 316 4*
B. Comparable ranges of background force
Cat 1 316 6 296 2 5.36 1.3 1.66 0.3* 126 2 226 1*Cat 2 616 16 1256 5* 2.8 6 0.6 0.36 0.0* 216 3 296 2*Cat 3 496 8 526 5 4.96 0.5 1.46 0.3* 296 2 436 2*Cat 4 746 21 1036 21 — — 256 3 356 8*
peak dynamic force (0.726 0.00 to 0.736 0.01 s) nor the time fromthreshold to peak force (0.516 0.03 to 0.536 0.03 s) was changedsignificantly for comparable velocities of angular displacement(57.66 0.7 to 58.06 1.3 deg/s).
The mechanical joint angle threshold was mediated by a reflexcomponent in the unlesioned cat, because the average mechanicalthreshold latency (0.236 0.01 s) was greater than the mean SOL andMG threshold latency (0.196 0.03 s and 0.196 0.02 s) that were inturn based on the time when the level of EMG activity exceeded thebackground level by 50% following joint ankle dorsiflexion. Ananalysis of EMG threshold latency and slope before and after injuryat matched background force levels was also performed to corroboratethat changes in mechanical reflex parameters described above weremediated by a neural component. A postoperative decrease in ipsi-lateral SOL threshold latency from 0.196 0.03 s to 0.166 0.01 swas noted, but this effect was not significant (F 5 1.16; P 5 0.31;d.f. 5 1,12). Likewise an increase in SOL incremental dynamic slopefrom 1046 39 µV/s to 1526 15 µV/s following injury was also non-significant (F 5 1.31; P 5 0.29; d.f.5 1,8). Before and after T13–L3 lesions no change in MG threshold latency (0.196 0.02 s to0.206 0.05 s) nor MG incremental dynamic slope (1156 45 µV/sto 1196 44 µV/s) was observed.
Stretch reflexes were recorded after administration of ketamine, toexamine effects of anaesthesia on threshold and IDS. Preoperatively,low rates of ketamine infusion preserved EMG and force responsesto ankle flexion, although amplitudes were reduced (see insets Iand II in Fig. 3A). Ketamine dose-dependently decreased IDS andincreased reflex threshold (Fig. 3A).
The high infusion rate of 22.2 mg/kg per h of ketamine provideda test of whether an increase in passive stiffness could account forthe increased resistance to stretch following dorsolateral spinal lesions.EMG responses to static stretch were reduced by 766 11% by thisdosage. Insets I and II in Fig. 3B illustrate negligible EMG and forceresponses during the high level of ketamine anaesthesia. Ratios ofstatic reflex force for postoperative testing of the two hindlimbs(ipsilateral/contralateral) revealed no significant ipsilateral effect ofthe lesion on passive resistance for cats 2 and 3, or when these datawere combined with results from two untrained cats with unilaterallesions of the dorsolateral column. Moreover, IDS was not significantlygreater ipsilateral to the lesion during the high rate of ketamineinfusion for cats 2 and 3 (ipsilateral: 126 4 g/deg, contralateral:7 6 2 g/deg). Two further lines of evidence suggest that there wasno change in passive stiffness following spinal injury. Administrationof sufficient pancuronium bromide to totally abolish reflex EMGactivity during ketamine anaesthesia (10.0 mg/kg per h, i.v.) in twochronic-lesioned animals (including cat 4) produced an ipsilateral/
© 1999 European Neuroscience Association,European Journal of Neuroscience, 11, 363–368
contralateral static force ratio of 0.486 0.05, and IDS was the samefor both hindlimbs (26 1 g/deg).
Discussion
The effects of dorsolateral spinal lesions on stretch reflexes wereunilateral, which is an important consideration for experimentalmodels of hyper-reflexia that involve acute recording experiments,providing only comparisons between ipsilateral and contralateralreflexes (i.e. where preoperative recordings from the same animalscannot be obtained). The dorsal spinal lesions in the present studywere quite small, involving only the tip of one dorsolateral column andsparing much of the distribution of the corticospinal and rubrospinalpathways. The location of the lesions suggests that hyper-reflexiaresulted from interruption of dorsal reticulospinal pathways (Shreineret al., 1949; Nathan & Smith, 1955; Engberget al., 1968).
Although IDS is considered to be constant over normal operatingconditions (Matthews, 1959; Feldman & Orlovsky, 1972; Cragoet al.,1976; Nichols & Houk, 1976; Hoffer & Andreassen, 1981), alterationsin reflex stiffness occur following activation of supraspinal centres(Nichols & Steeves, 1986), after administration of baclofen (Capaday,1995) and during vestibular stimulation (Kim & Partridge, 1969). Inthe present study, selective interruption of dorsolateral spinal pathwaysproduced an enduring ipsilateral increase in IDS. This could haveresulted from an overall shift of background force toward the highend of the normal range (see Fig. 1C; cf. Racket al., 1984; Leeet al.,1987), reflecting an increase in resting muscular tone. However, therewere significant postoperative increases in IDS that could not beaccounted for by levels of resting resistance prior to ankle flexion.
Evidence that the lesion effect on IDS was mediated by an increasein reflex activity was provided by recording from anaesthetized cats.Following administration of doses of ketamine that greatly attenuatedor eliminated EMG responses (with or without pancuronium bromide),leaving non-reflex stiffness as the only source of resistance todorsiflexion of the ankle, the lesion effect was eliminated. Thisfinding differs from a previous suggestion that increased intrinsicmuscle stiffness is present in spastic patients (Dietzet al., 1981).Also, passive changes in stiffness of non-muscular tissue have beenshown in patients with more severe pathologies (Sinkjaeret al., 1993;Sinkjaer & Magnussen, 1994). The effect of anaesthesia indicatesthat neither intrinsic muscle stiffness nor passive tissue stiffnesscontributed to the increase in ankle extensor stiffness resulting froma dorsolateral spinal lesion.
Unilateral interruption of the dorsolateral column at T13–L3produced a significant decrease in threshold and an increase inIDS for responses elicited by passive stretch of extensor muscles.

Stretch reflex threshold and stiffness following spinal lesions 367
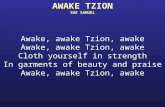
FIG. 3. (A) Threshold angle and IDS from responses evoked by 43° angulardisplacement of seven uninjured cats (including 2, 3 and 4) in conscious andketamine-anaesthetized states. Slow infusion of ketamine at 10.0 mg/kg per hpreserved reflex EMG and force responses (inset I and II; solid line: conscious;broken line: ketamine). and significantly decreased IDS (filled squares) relativeto the conscious state (**one-tailedt 5 3.77,P , 0.005, d.f.5 10). The highinfusion rate of 22.2 mg/kg per h produced a further decrease in IDS (***one-tailed t 5 6.38, P , 0.001, d.f.5 10) and an increase in reflex threshold(1: two-tailed t 5 1.84, P , 0.05, d.f.5 10). (B) The ratio of ipsilateral/contralateral static forces, before and after SCI, in deeply anaesthetized cats.During ketamine infusion at 22.2 mg/kg per h, triceps surae EMG activitywas negligible (inset I), which permitted analysis of passive force followingankle displacement (inset ll). Greater resistance to flexion ipsilateral todorsolateral lesions was not observed under deep anaesthesia, as shown bythe postoperative ratios of ipsilateral/contralateral static force for trained cats(2 and 3; left bars) or trained and untrained cats (right bars).
Previously, a reduction in threshold has been reported only for reflexeselicited by stretch during active contraction (Fujimoriet al., 1966;Powerset al., 1988, 1989) but not during passive stretch (Thilmannet al., 1991). Likewise, evidence for an increase in gain under passivetesting conditions has been demonstrated (Thilmannet al., 1991) butnot from previously activated muscles (Leeet al., 1987). Our datasupport the idea that the initial condition, passive or active, of thetested muscle would be crucial in identifying threshold and stiffnesschanges in injured patients. The reduction in reflex threshold followinglesion in this study was dependent on the background force, whiledorsiflexion of the foot at acute start angles of less than 105° failedto demonstrate hyper-reflexia (Tayloret al., 1997).
Using different starting ankle angles and therefore different levels
© 1999 European Neuroscience Association,European Journal of Neuroscience, 11, 363–368
of muscle load, the correlation between threshold and IDS wasreduced following injury, suggesting that the lesion uncoupled anormal relationship between these reflex measures. That is, reflexthreshold and gain appeared to be affected differentially by interruptionof the dorsolateral column. Changes in threshold or stiffness after aspinal lesion can be attributed to a variety of mechanisms (for adiscussion see Katz & Rymer, 1989), although it is not known towhat extent each of these would contribute to a change in eitherreflex parameter. Interruption of descending reticulospinal pathways(Shreineret al., 1949; Nathan & Smith, 1955; Engberget al., 1968)in the DLF could mediate changes in both reflex parameters, assupraspinal inputs have been suggested to modulate both threshold(Feldman & Orlovsky, 1972) and gain (Kim & Partridge, 1969;Nichols & Steeves, 1986). Disinhibition of spinal interneurons follow-ing damage to descending monoaminergic pathways has been pro-posed to mediate stretch hyper-reflexia (Nogaet al., 1992; for areview see Jankowska, 1993). Further examination of reflex thresholdand stiffness in awake animals with restricted spinal lesions is neededto examine these relationships.
AcknowledgementsThis work was supported by NIH Grants NS 27511, NS 35702 and the Brainand Spinal Cord Injury and Rehabilitation Trust Fund (BSCIRTF) of the Stateof Florida. We would like to thank an anonymous reviewer for his advice inthe preparation of this report.
AbbreviationsDLF, dorsolateral funiculus; IDS, incremental dynamic stiffness; MG, medialgastrocnemius.
ReferencesCapaday, C. (1995) The effects of baclofen on the stretch reflex parameters
of the cat.Exp. Brain Res., 104, 287–296.Crago, P.E., Houk, J.C. & Hasan, Z. (1976) Regulatory actions of human
stretch reflex.J. Neurophysiol., 39, 925–935.Dietz, V., Quintern, J. & Berger, W. (1981) Electrophysiological studies of
gait in spasticity and rigidity. Evidence that altered mechanical propertiesof muscle contribute to hypertonia.Brain, 104, 431–449.
Engberg, I., Lundberg, A. & Ryall, R.W. (1968) Reticulospinal inhibition oftransmission in reflex pathways.J. Physiol. (London), 194, 201–223.
Feldman, A.G. & Orlovsky, G.N. (1972) The influence of different descendingsystems on the tonic stretch reflex in the cat.Exp. Neurol., 37, 481–494.
Fujimori, B., Kato, M., Matsushima, S., Mori, S. & Shimamura, M. (1966)Studies on the mechanism of spasticity following spinal hemisection in thecat. In Granit, R. (ed.),Muscular Afferents and Motor Control. NobelSymposium I. Almquist and Wiskell, Uppsala, pp. 397–413.
Grillner, S. (1972) The role of muscle stiffness in meeting the changingpostural and locomotor requirements for force development by the ankleextensors.Acta Physiol. Scand., 86, 92–108.
Heckman, C.J. (1994) Alterations in synaptic input to motoneurons duringpartial spinal cord injury.Med. Sci. Sport Exer., 26, 1480–1490.
Hoffer, J.A. & Andreassen, S. (1981) Regulation of soleus muscle stiffnessin premammillary cats: intrinsic and reflex components.J. Neurophysiol.,45, 267–285.
Hoffer, J.A., Leonard, T.R., Cleland, C.L. & Sinkjaer, T. (1990) Segmentalreflex action in normal and decerebrate cats.J. Neurophysiol., 64, 1611–1624.
Jankowska, E. (1993) Monoaminergic inhibitory control. of spinal interneurons.In Thilmann, F., Burke, D.J. & Rymer, W.Z. (eds),Spasticity: Mechanismsand Management.Springer-Verlag, Berlin, pp. 193–203.
Katz, R.T. & Rymer, W.Z. (1989) Spastic hypertonia: mechanisms andmeasurement.Arch. Phys. Med. Rehabil., 70, 144–155.
Kernell, D. (1993) Functional properties of the neuromuscular system andforce gradation. In Thilmann, F., Burke, D.J. & Rymer, W.Z. (eds),Spasticity: Mechanisms and Management.Springer-Verlag, Berlin, pp.193–203.

368 J. Tayloret al.
Kim, J.H. & Partridge, L.D. (1969) Observations on types of response tocombinations of neck, vestibular, and muscle stretch signals.J.Neurophysiol., 32, 239–250.
Lee, W.A., Boughton, A. & Rymer, W.Z. (1987) Absence of stretch reflexgain enhancement in voluntarily activated spastic muscle.Exp. Neurol., 98,317–335.
Matthews, P.B.C. (1959) The dependence of tension upon extension in thestretch reflex of the soleus muscle of the decerebrate cat.J. Physiol.(London), 147, 521–546.
Nathan, P.W. & Smith, M.C. (1955) Long descending tracts in man. I. Reviewof present knowledge.Brain, 78, 248–303.
Nichols, T.R. (1989) The organization of heterogenic reflexes among musclescrossing the ankle joint in the decerebrate cat.J. Physiol. (London), 410,463–477.
Nichols, T.R. & Houk, J.C. (1976) Improvement in linearity and regulationof stiffness that results from actions of stretch reflex.J. Neurophysiol.,39,19–142.
Nichols, T.R. & Steeves, J.D. (1986) Resetting of resultant stiffness in ankleflexor and extensor muscles in the decerebrate cat.Exp. Brain Res., 62,401–410.
Noga, B.R., Bras, H. & Jankowska, E. (1992) Transmission from group IImuscle afferents is depressed by stimulation of locus coeruleus/subcoeruleus,Kolliker-Fuse and raphe nuclei in the cat.Exp. Brain Res., 88, 502–516.
Powers, R.K., Marder Meyer, J. & Rymer, W.Z. (1988) Quantitative relations
© 1999 European Neuroscience Association,European Journal of Neuroscience, 11, 363–368
between hypertonia and stretch reflex threshold in spastic hemiparesis.Ann.Neurol., 23, 115–124.
Powers, R.K., Campbell, D.L. & Rymer, W.Z. (1989) Stretch reflex dynamicsin spastic elbow flexor muscles.Ann. Neurol., 25, 32–42.
Rack, P.M., Ross, H.F. & Thilman, F. (1984) The ankle stretch reflexes innormal and spastic subjects.Brain, 107, 637–654.
Schreiner, L.M., Lindsley, D.B. & Magoun, H.W. (1949) Role of brain stemfacilitatory systems in maintenance of spasticity.J. Neurophysiol., 12,207–216.
Sinkjaer, T. & Magnussen, I. (1994) Passive, intrinsic and reflex-mediatedstiffness in the ankle extensors of hemiparetic patients.Brain, 117, 355–363.
Sinkjaer, T., Toft, E., Larsen, K., Andreassen, S. & Hansen, H.J. (1993) Non-reflex and reflex mediated ankle joint stiffness in multiple sclerosis patientswith spasticity.Muscle Nerve, 16, 69–76.
Taylor, J.S., Vierck, C.J. Jr & and Munson, J.B. (1993) Development of ananimal model for the study of spinal spasticity. In Thilmann, F., Burke,D.J. & Rymer, W.Z. (eds),Spasticity: Mechanisms and Management.Springer-Verlag, Berlin, pp. 204–221.
Taylor, J.S., Friedman, R.F., Munson, J.B. & Vierck, C.J. Jr (1997) Stretchhyperreflexia of triceps surae muscles in the conscious cat followingdorsolateral spinal lesions.J. Neurosci., 17, 5004–5015.
Thilmann, A.F., Fellows, S.J. & Garms, E. (1991) The mechanism of spasticmuscle hypertonus; variation in reflex gain over the time course of spasticity.Brain, 114, 233–244.