
The Anti-Cancer Property of Proteins Extracted from Gynura procumbens (Lour.) Merr.

Phytomedicine Vol. 3 (1), pp. 1-10, 1996© 1996 by GustavFischer Verlag, Stuttgart· Jena . New York
Effectiveness of Harpagophytum procumbensin treatment of acute low back pain
S. CHRUBASIK, CH. ZIMPFER, U. SCHOn, R. ZIEGLER
Departmentof Internal Medicine I, University Hospital, Bergheimerstr. 58, 69115 Heidelberg
Summary
In a study that indicates more definitive investigation is needed, 118 patients with chronic backproblems seeking treatment for acute attacks of pain were included in a 4-week randomised double-blinded study on the safety and effectiveness of an extract of Harpagophytum procumbens.Both, the treatment and the placebo were administered in the form of two tablets taken threetimes per day; the treatment group had a daily consumption equal to 6,000 mg of crude preparation (50 mg harpagoside, the putative active ingredient). The treatment and placebo groups werewell matched in physical characteristics; in the severity, duration, nature and accompaniments oftheir pain; and in laboratory indices of organ system function. 109 patients completed the study.
The study was originally designed to measure Harpagophytum's effectiveness by measuring theuse of supplementary pain-killer Tramadol over its final 3 weeks. However, this did not differbetween the Harpagophytum and placebo groups nor was the consumption closely related to theamount of pain. Further analysis, though, revealed that 9 out of 51 patients who received the extract were pain free at the end of treatment compared to only lout of 54 patients who receivedplacebo. A modification of the Arhus index was used as an additional measure, covering the moreglobal impact. The percentage change was greater in those patients who received Harpagophytum extract than in those who received placebo, but inferential testing (Mann Whitney) allowedonly 94% degree of confidence that this had not arisen by chance. The Arhus index reduction wasbased on improvement in pain.
This indication of effectiveness, and the absence of demonstrable adverse effects show thatmore definite clinical studies of Harpagophytum extract will be worthwhile.
Key words: Harpagophytum procumbens, Devil's claw, acute low back pain, randomised double-blinded study, Arhus index
Introduction
Some herbal remedies that predated the need for randomized clinical trial have become established pillars of contemporary therapeutics, but others of more recent popularity are regarded with condescension by the medical establishment because they have not yet been put to the conventionally approved test. If herbal medicine is to continue tocontribute respectably to advances in therapeutics, it mustdo so by embracing the formalities, technicalities and niceties of the randomized controlled clinical trial.
Sufferers of low back pain are prominent clients at pain
clinics (Hildebrandt et aI., 1993 a). Some cases have recognizable causes but others do not (Hildebrandt, 1993 b), andare attributed to things as weak back muscles or reducedflexibility of the spine (Frymoyer, 1988). Though some authorities recommend opioids for symptomatic treatment ofacute attacks or exacerbation of low back pain (Portenoyand Foley, 1986; Zimmermann, 1990), treatment generallyconsists of nonopioid analgesics (Chrubasik and Ziegler,1996 a). However, these can cause side effects, particularlyon the gastrointestinal tract in the case of the nonsteroidalanti-inflammatory agents.
Disappointment with, or intolerance of, conventional

2 S. Chrubasik et al,
medical remedies have led many to pursue alternatives,among them extracts of the root of Devil's Claw (Harpagophytum procumbens) that have become popular for degenerative conditions of the musculoskeletal system (Chrubasik et al., 1995).
The principal active ingredient is believed to be the iridoid harpagoside (see formula). Evidence of the analgesicand antiinflammatory properties of extracts from Harpagophytum procumbens have been derived from animal experiments; however, this has not so far been strongly supported in humans with subacute or chronic pain (Belaiche1982; Grahame and Robinson, 1981; Lecomte and Costa,1992; Pinget and Lecomte, 1990; Zimmermann 1977).Whatever the effect may be on pain itself, there are no dataat all on Harpagophytum's wider impact on quality of lifewhich, for low back pain, is materially affected by physical,psychological and social disability (Vallfors, 1985; Waddel,1984 a). The plant extract does, however seem remarkablyfree of side-effects.
The objective of this study was to initiate the randomizedcontrolled testing of Harpagopbytum extract as a symptomatic treatment for acute exacerbations of chronic backpain. Because it was a starting point, the planning of thestudy trial lacked much of what was needed in study design, particularly in the related matters of choice of outcome measures and the numbers needed to insure a reasonable chance of detecting a clinically important change in anoutcome measure.
Paucity of information at the design stage is sometimesinevitable early on and can prevent definitive conclusionsfrom being drawn. This study illustrates this fact, but alsoprovides data that indicate effectiveness and safe use.
HO OH
Ci""amOYI-O~O-Glue
Harpagoside
Methods
General plan of the study
The study was approved by the Human Ethics Committee of the University of Heidelberg. The plan was as follows: (i) to randomly allocate an appropriately selectedsample of back pain sufferers into a treatment group (groupH, to receive extract of Harpagophytum procumbens forfour weeks) and a control group (group P, to receive theplacebo for the same time); (ii) to formally record of a set ofbaseline measures for pain and clinical and laboratory indications of general health; (iii) to keep the patients and investigators unaware of which the group the patients were
in; (iv) to have the patients take their allocated substancesfor the 4 week study period, keeping track on the severityof their pain with daily telephone calls; (v) to record thepatients' cumulative requirement for Tramadol, the onlysupplementary analgesic allowed during the study; (vi) torepeat the assessments made at baseline at the end of thefour weeks treatment; (vii) to have the cumulative requirement for Tramadol over the last three weeks of the studyperiod be the principal measure of effectiveness; (viii) tohave the numbers of totally pain-free patients at the end oftreatment and the change in the Arhus index relative to itsbaseline be the subsidiary measures of effectiveness;(ix) and to screen for adverse effects by comparison of thebaseline and final clinical examination and by laboratoryinvestigations.
Selection of patients
An account of the plan and invitations to participatewere given to patients between 18 and 75 years old whohad experienced at least six months of low back pain thatwas not attributable to identifiable causes (e. g. disc prolaps, hip disease, spondylolisthesis, osteomalacia or inflammatory arthritis), who were suffering from acute increasesof pain that affected both rest and movement, and whowere expected to require at least four weeks of symptomatic treatment (the proposed duration of the study). Theywere not invited if they were participating in other clinicalstudies, or had done so within 30 days; additional exclusion criteria were pregnancy, lactation or insufficient contraceptive methods, difficulties with language or co-operation, known allergy to any of the proposed trial medications, a history of drug or alcohol abuse or requirement forpsychotherapeutic agents, and serious organic illness affecting any of the organ systems.
Group sizes and outcome measures
Of those who were eligible, 118 consented in writing toparticipate. They were recruited to provide a treatmentgroup (H) and a control (placebo) group (P), each withmore than 50 patients. The numbers selected for eachgroup (n=50) were based on conventional calculations ofrequirements for 90% power of detecting a reduction froman expected average cumulative requirement for 4000 mgof Tramadol over the last 3 weeks of the study in the placebo group (P) to 2000 mg or less in the treatment group (H),when 95% confidence was required to reject the null hypothesis that there was no difference in effect. The cumulative requirement for Tramadol over the last three weeks ofthe study period was taken as the principal outcome measure, for simplicity and lack of any better information at thetime. The patients were placed in the two groups by a random number allocation.
For the first of the subsidiary measures of effectiveness,
Effectiveness of Harpagopbytum procumbens in treatment of acute low back pain 3
II"0
(,l
aOJIIIa.LIIII
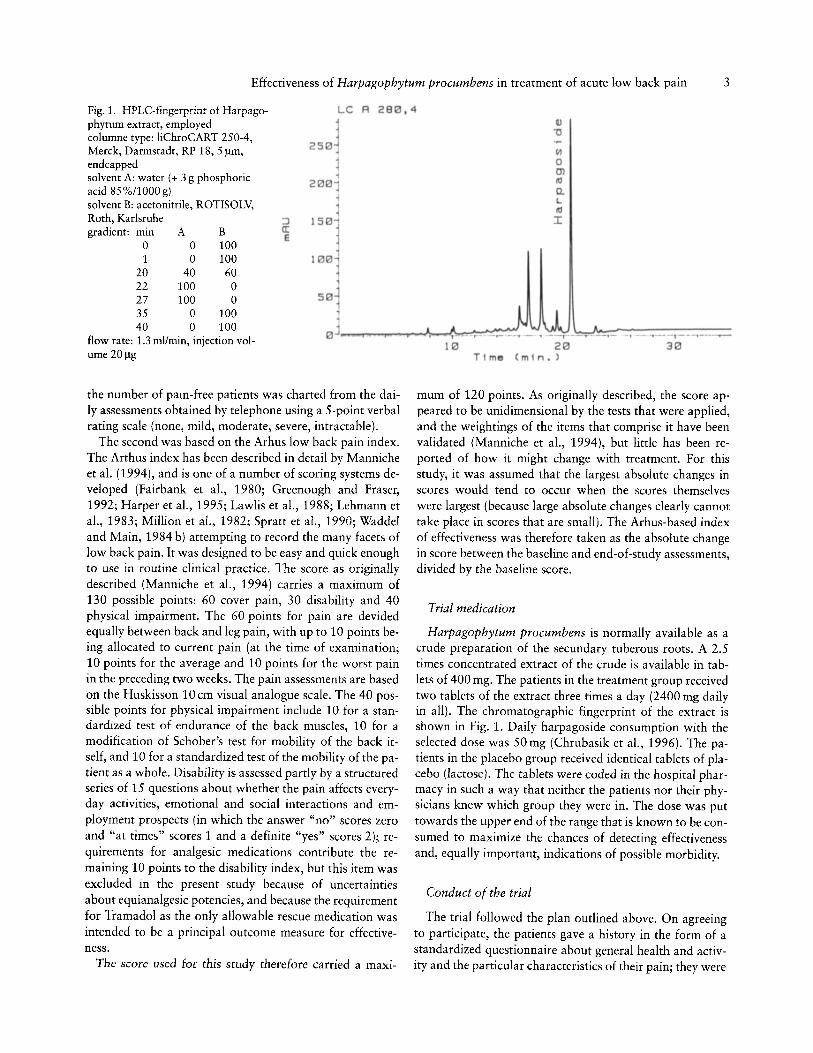
Fig. 1. HPLC-fingerprinr of Harpago- LC A 2 80 , 4
phytum extract, employed
2 S 0~columne type: liChroCART 250-4,Merck, Darmstadt, RP 18, 5 urn,endcapped ~solvent A: water (+ 3 g phosphoric 1
acid 85%/1000 g)2 0 0 1
solvent B: acetonitrile , ROTISOLV,Roth, Karlsruhe :J 150"]gradient: A B a:rmn E
0 0 1001 0 100 100
20 40 60 122 100 0
,27 100 0 S0 j
35 0 10040 0 100
0 Jflow rate: 1.3 ml/min, injection vol-ume 20Jlg
10 20T im (m in . )
- ., -- -- I - - - ,-_.-.....-
30
the number of pain-free patients was charted from the daily assessments obtained by telephone using a 5-point verbalrating scale (none, mild, modera te, severe, intrac tab le).
The second was based on the Arhus low back pain index.The Arthus index has been described in detai l by Mannicheet a!' (1994), and is one of a number of scoring systems developed (Fairbank et aI., 1980; Greenough and Fraser,1992; Harper et al., 1995; Lawlis et aI., 1988; Lehmann eta!., 1983; Million et aI., 1982; Spratt et a!., 1990; Waddeland Main, 1984 b) attempting to record the many facets oflow back pain . It was designed to be easy and quick enoughto use in routine clinical practice. The score as originallydescribed (Manniche et aI., 1994) carries a maximum of130 possible points: 60 cover pain, 30 disability and 40physical impairment. The 60 points for pain are devidedequally between back and leg pain, with up to 10 points being allocated to current pain (at the time of examination;10 points for the average and 10 points for the wors t painin the preceding two weeks. The pain assessments are basedon the Huskisson 10 em visual analogue scale. The 40 possible points for physical impairment include 10 for a standardized test of endurance of the back muscles, 10 for amodification of Schober's test for mobility of the back itself, and 10 for a standardized test of the mobility of the patient as a whole. Disability is assessed partly by a structuredseries of 15 questions about whether the pain affects everyday activities, emotional and social interactions and employment prospects (in which the answer "no" scores zeroand "at times" scores 1 and a definite "yes" scores 2); requirements for analgesic medications contribute the remaining 10 points to the disability index, but this item wasexcluded in the present study because of uncertaintiesabout equiana lgesic potencies, and because the requirementfor Tramadol as the only allowab le rescue medication wasintended to be a principal outcome measure for effectiveness.
The score used for this study therefo re carried a maxi-
mum of 120 points. As originally described, the score appeared to be unidimensional by the tests tha t were applied,and the weightings of the items that comprise it have beenvalidated (Manniche et al., 1994), but little has been reported of how it might change with treatment. For thisstudy, it was assumed that the largest absolute changes inscores would tend to occur when the scores themselveswere largest (because large absolute changes clearly cannottake place in scores that are small). The Arhus-based indexof effectiveness was therefore taken as the absolute changein score between the baseline and end-of-stu dy assessments,divided by the baseline score.
Trial medication
Harpagophytum procumbens is normally available as acrude preparation of the secundary tuberous roots. A 2.5times concentrated extract of the crude is available in tablets of 400 mg. The patients in the treatment group receivedtwo tablets of the extract three times a day (2400 mg dailyin all). The chromatographic fingerprint of the extract isshown in Fig. 1. Daily harpagoside consumption with theselected dose was 50 mg (Chrubasik et al., 1996) . The patients in the placebo group received identica l tablets of placebo (lactose). The tablets were coded in the hospital pharmacy in such a way that neither the patients nor their physicians knew which group they were in. The dose was puttowards the upper end of the range that is know n to be consumed to maximize the chances of detecting effectivenessand, equally important, indications of possible morbidity.
Conduct of the trial
The trial followed the plan outlined above. On agreeingto participate, the patients gave a history in the form of astandardized questionnaire about general health and activity and the particular characteristics of their pain; they were

4 S. Chrubasik et aI.
also examined, had their vital signs recorded, went throughthe procedure for completing the Arhus score, and gave avenous blood sample for baseline measurements of the conventional biochemical and hematological indices of organsystem function. They received their coded medication totake as directed during the four weeks of the study. Theywere contacted daily by telephone to get verbal ratings oftheir pain, to encourage their compliance with taking thestudy medication, and to record their need to take Trarnadol for supplementary analgesia. At the end of the fourweek study period, Arhus scoring, the vital signs and laboratory measurements were repeated in the same format as atbaseline.
Statistical analysis
This used the procedures available in the package of Statistical Analysis System Software (SAS Institute Inc., Cary,NC) . Categorical data were examined in contingency tables, with inferential testing by Chi square or Fisher's exacttest. Ordinal or abnormally distributed interval data weresummarised as median and quartiles, with inferential testing by Mann-Whitney-Wilcoxon (paired as appropriate fordifferences between baseline and end of study), and normally distributed interval data were displayed as means andstandard deviation and subjected, where appropriate, to
"t" -testing, Spearman Rank correlation was used to relateverbal rating scores with verbal rating of pain. The confidence level for rejecting a null hypothesis was taken as 95%(p < 0.05).
Results
Characteristics on entry to study
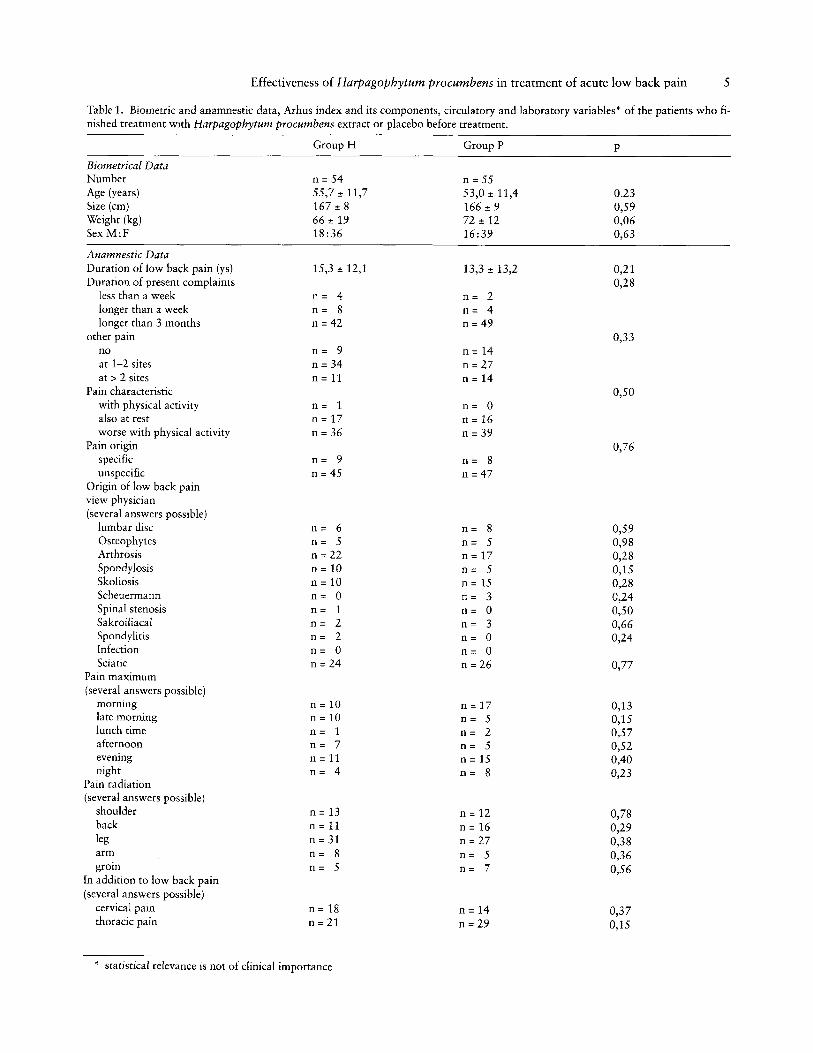
Of the 118 patients who entered into the trial, 109 completed it. There were five failures (n=4 did not attend the final examination, ne l suffered from tachycardia) ingroup H and four failures in group P (they did not attendthe final examination). The remaining 54 patients ingroup Hand 55 in group P were clearly matched (Table 1)for physical characteristics, general medical health, professional and employment status, participation in sporting activity and the Arhus low back pain index (overall, and in itsseveral components). Of an additional 50 or so possiblecomparisons of laboratory measurements and more detailed aspects of the low back pain (Table 1) there were only four in which the observed differences would havereached "significance" in single isolated comparisons. In atotal of nearly 100 comparisons this merely confirms thatthe randomization had been effective.
The 109 patients (Table 1) had been suffering bouts oflow back pain for about 15 years, and more than 83% ofthem had acute attacks longer than 3 months that had sentthem for treatment. Furthermore, 89% of them had suf-
fered physical impairment for more than 14 days in the previous six months, and their condition had affected theirwork in 46% of cases. Eighty percent of them had had painin at least one other site (upper back, shoulder, arm, neck ,groin, leg) that in 68 % of the cases was exacerbated byphysical activity. Specific causes were identified in only16% of patients, though a variety of possible causes wereadvanced by the attending physicians, the most commonbeing "arthrosis" and "sciatica" . The pain was at its worstin the morning and evening.
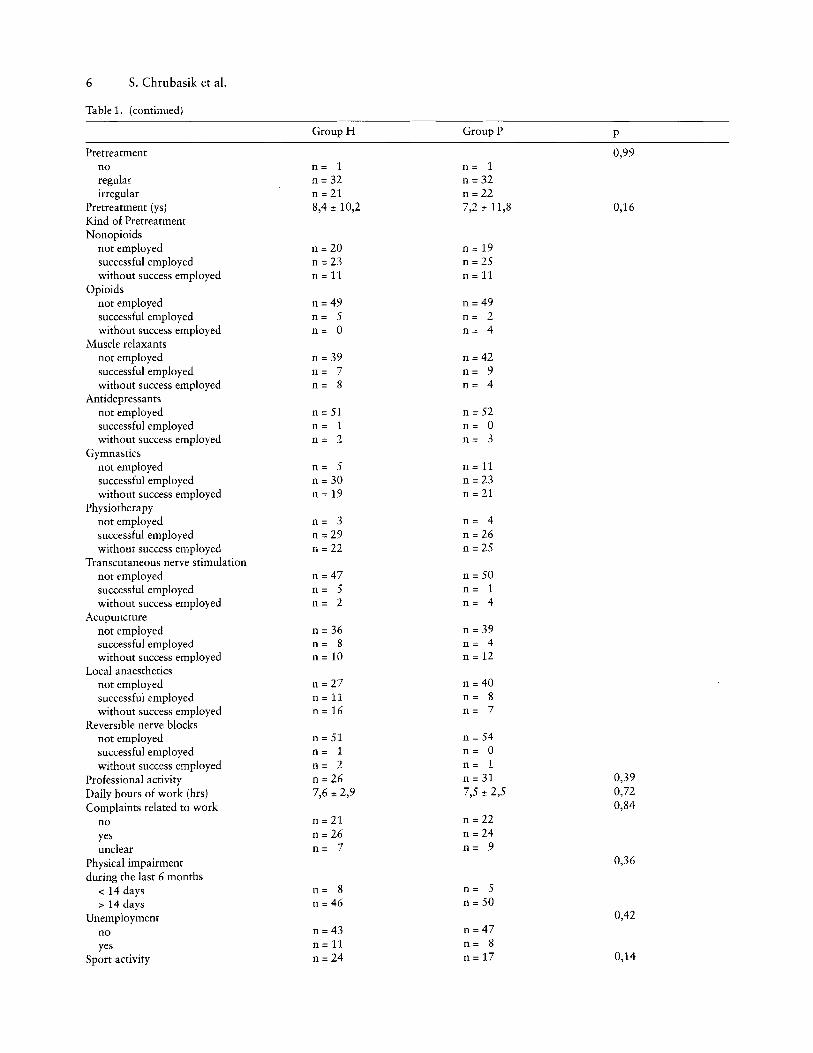
Almost all patients had previously resorted to some treatment for the chronic condition either regularly (59%) or irregularly (39%), and the average duration of treatment wasabout eight years. Exercise and physiotherapy had beentried in about 90% of patients, with success reported inabout half of the cases. Non-opioid analgesics were themost common drug treatment having been used in about64% of cases with about 68 % success. Centrally actingmuscle relaxants, opioids and antidepressants had beenused in about 26%, 10% and 5% of cases, respectively,with a success rate of about 50 %. Local anaesthetics hadbeen used in about 38% of cases for neural therapy andhad been successfully in about half of them, but they hadrarely been used for specific nerve blocks. Acupuncture hadbeen used in 31 % of the patients with success reported35 % of the times, and transcutaneous nerve stimulationdone only 11%, of whom about half claimed success.
Measures of effectiveness and safety
Tramadol consumption
During the last three weeks of treatment patients consumed a total of 99 ± 208 mg Tramadol (group H 95 ±
157mg, n=54; group P 102:to250mg, n=55, p=0.44). Average pain scores of the last three weeks did not correlatewith average Tramadol consumption (r=0.39). MedianTramadol consumption on days with none or mild, moderate or severe and intractable pain revealed that Tramadolconsumption was the same (range differed slightly) (Table 2).
Numbers of pain-free patients
The number of pain-free patients increased in group Hfrom 0 at the end of the first week to two, four and nine atthe end of the next three weeks; in group P, one patient became pain-free by the end of the second week, and there remained only one at the end of the fourth week. Had the difference between nine out of 54 and one out of 55 been thesale and principal measure of effectiveness, this would havebeen a highly significant finding (p=0.008, Fisher's exacttest).
Effectiveness of Harpagopbytum procumbens in treatment of acute low back pain 5
Table 1. Biometric and anamnestic data, Arhus index and its components, circulatory and laboratory variables ' of the patients who finished treatment with Harpagophytum procumbens extract or placebo before treatment.
n= 6 n= 8 0,59n = 5 n = 5 0,98n =22 n = 17 0,28n = 10 n= 5 0,15n = 10 n = 15 0,28n= 0 n= 3 0,14n = 1 n = 0 0,50n = 2 n= 3 0,66n= 2 n= 0 0,24n= 0 n= 0n = 24 n = 26 0,77
n = 10 n = 17 0,13n = 10 n = 5 0,15n= 1 n= 2 0,57n = 7 n= 5 0,52n = 11 n = 15 0,40n= 4 n= 8 0,13
n = 13 n = 12 0,78n = 11 n = 16 0,19n = 31 n = 27 0,38n = 8 n = 5 0,36n = 5 n = 7 0,56
n = 18 n = 14 0,37n = 21 n = 29 0,15
Biometrical DataNumberAge (years )Size (em)Weight (kg)Sex M :F
Anamnestic DataDuration of low back pain (ys)Duration of present comp laints
less than a weeklonger than a weeklonger than 3 mon ths
other painnoat 1-2 sitesat> 2 sites
Pain characteristicwith physical activit yalso at restworse with physical activity
Pain originspecificunspecific
Origin of low back painview physician(several answers possible )
lumbar discOsteophytesArthrosisSpondylosisSkoliosisScheuermannSpinal stenosisSakroiliacalSpondylitisInfectionSciatic
Pain maximum(several answers possible)
morninglate morninglunch timeafternooneveningnight
Pain radiation(several answers possible )
shoulderbacklegarmgroin
In addition to low back pain(several answers possible )
cervical painthoracic pain
Gro up H Group P
n = 54 n = 5555,7 ± 11,7 53,0 ± 11,4167 ± 8 166 ± 966 ± 19 72 ± 1218 :36 16:39
15,3 ± 12,1 13,3 ± 13,2
n= 4 n = 2n= 8 n = 4n = 42 n = 49
n = 9 n = 14n = 34 n = 27n = 11 n = 14
n= 1 n= 0n = 17 n = 16n = 36 n = 39
n= 9 n = 8n = 45 n = 47
p
0.230,590,060,63
0,110,18
0,33
0,50
0,76
» statistical relevance is not of clinical importance
6 S. Chrubasik et al.
Table 1. (continued)
Group H Group P p
Pretreatment 0,99no n= 1 n= 1regular n = 32 n= 32irregular n = 21 n = 22
Pretreatment (ys) 8,4:!: 10,2 7,2:!: 11,8 0,16Kind of PretreatmentNonopioids
not employed n = 20 n = 19successful employed n = 23 n = 25without success employed n = 11 n = 11
Opioidsnot employed n = 49 n = 49successful employed n= 5 n= 2without success employed n= ° n= 4
Muscle relaxantsnot employed n = 39 n = 42successful employed n= 7 n= 9without success employed n= 8 n= 4
Antidepressantsnot employed n = 51 n = 52successful employed n= 1 n= °without success employed n= 2 n= 3
Gymnasticsnot employed n= 5 n = 11successful employed n = 30 n = 23without success employed n = 19 n = 21
Physiotherapynot employed n= 3 n= 4successful employed n = 29 n = 26without success employed n = 22 n = 25
Transcutaneous nerve stimulationnot employed n = 47 n = 50successful employed n= 5 n= 1without success employed n= 2 n= 4
Acupuncturenot employed n = 36 n = 39successful employed n= 8 n= 4without success employed n = 10 n = 12
Local anaestheticsnot employed n = 27 n = 40successful employed n = 11 n= 8without success employed n = 16 n= 7
Reversible nerve blocksnot employed n = 51 n = 54successful employed n= 1 n= °without success employed n= 2 n= 1
Professional activity n = 26 n = 31 0,39
Daily hours of work (hrs) 7,6:!: 2,9 7,5 ± 2,5 0,72Complaints related to work 0,84
no n = 21 n = 22
yes n =26 n = 24unclear n= 7 n= 9
Physical impairment 0,36
during the last 6 months< 14 days n= 8 n= 5
> 14 days n = 46 n = 50Unemployment 0,42
no n = 43 n = 47yes n = 11 n= 8
Sport activity n = 24 n = 17 0,14
Effectiveness of Harpagophytum procumbens in treatment of acute low back pain 7
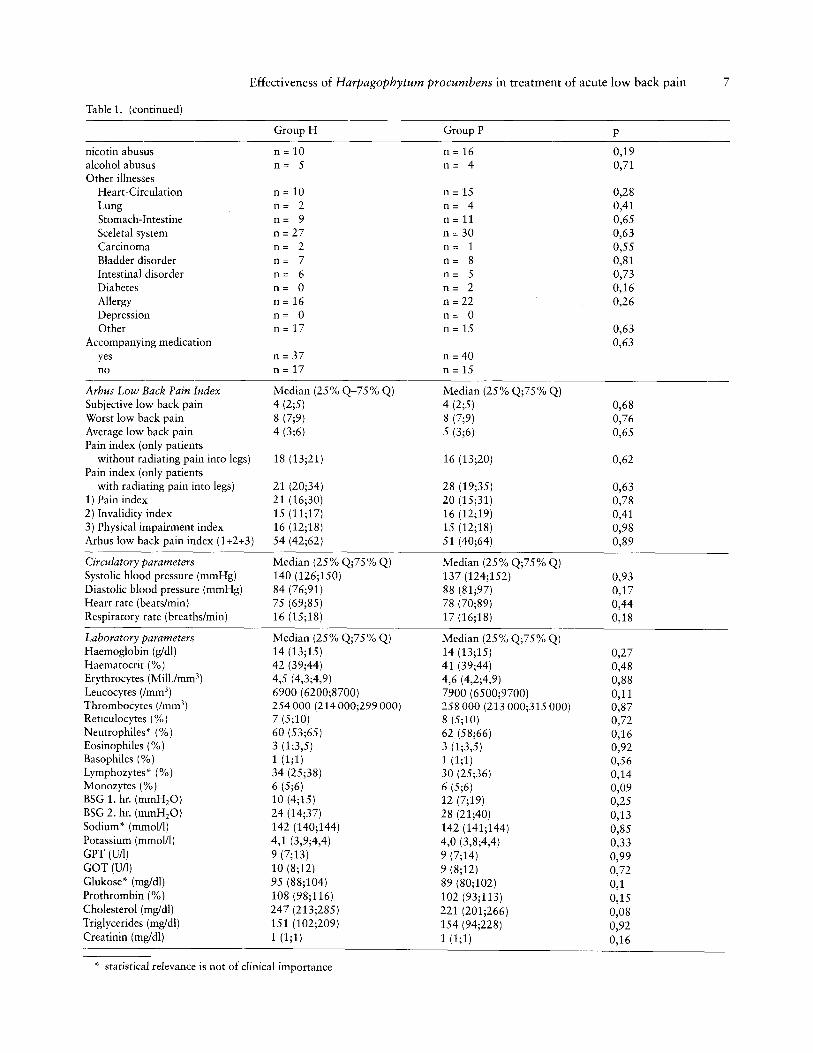
Table 1. (continued)
Group H Group P p
nicotin abusus n = 10 n = 16 0,19alcohol abusus n= 5 n= 4 0,71Other illnesses
Heart-Circulation n = 10 n = 15 0,28Lung n= 2 n= 4 0,41Stomach-Intestine n= 9 n = 11 0,65Sceletal system n = 27 n = 30 0,63Carcinoma n= 2 n= 1 0,55Bladder disorder n= 7 n= 8 0,81Intestinal disorder n= 6 n= 5 0,73Diabetes n= ° n= 2 0,16Allergy n = 16 n = 22 0,26Depression n= ° n= °Other n = 17 n = 15 0,63
Accompanying medication 0,63yes n = 37 n = 40no n = 17 n = 15
Arhus Low Back Pain Index Median (25% Q-75 % Q) Median (25% Q;75% Q)Subjective low back pain 4 (2;5) 4 (2;5) 0,68Worst low back pain 8 (7;9) 8 (7;9) 0,76Average low back pain 4 (3;6) 5 (3;6) 0,65Pain index (only patients
without radiating pain into legs) 18 (13;21) 16 (13;20) 0,62Pain index (only patients
with radiating pain into legs) 21 (20;34) 28 (19;35) 0,631) Pain index 21 (16;30) 20 (15;31) 0,782) Invalidity index 15 (11;17) 16 (12;19) 0,413) Physical impairment index 16 (12;18) 15 (12;18) 0,98Arhus low back pain index (1+2+3) 54 (42;62) 51 (40;64) 0,89
Circulatory parameters Median (25% Q;75% Q) Median (25% Q;75% Q)Systolic blood pressure (mmHg) 140 (126;150) 137 (124;152) 0,93Diastolic blood pressure (mmHg) 84 (76;91) 88 (81;97) 0,17Heart rate (beats/min) 75 (69;85) 78 (70;89) 0,44Respiratory rate (breaths/min) 16 (15;18) 17 (16;18) 0,18
Laboratory parameters Median (25% Q;75% Q) Median (25% Q;75% Q)Haemoglobin (g/dl) 14 (13;15) 14 (13;15) 0,27Haematocrit (%) 42 (39;44) 41 (39;44) 0,48Erythrocytes (Mill.zmm-) 4,5 (4,3;4,9) 4,6 (4,2;4,9) 0,88Leucocytes (fmm3) 6900 (6200;8700) 7900 (6500;9700) 0,11Thrombocytes (fmm3 ) 254000 (214000;299000) 258000 (213000;315000) 0,87Reticulocytes (%) 7 (5;10) 8 (5;10) 0,72Neutrophiles" (%) 60 (53;65) 62 (58;66) 0,16Eosinophiles (%) 3 (1;3,5) 3 (1;3,5) 0,92Basophiles (%) 1 (1;1) 1 (1;1) 0,56Lymphozytes" (%) 34 (25;38) 30 (25;36) 0,14Monozytes (%) 6 (5;6) 6 (5;6) 0,09BSG 1. hr. (mmHzO) 10 (4;15) 12 (7;19) 0,25BSG 2. hr. (mmH2O) 24 (14;37) 28 (21;40) 0,13Sodium" (mmol/l) 142 (140;144) 142 (141;144) 0,85Potassium (rnrnol/l) 4,1 (3,9;4,4) 4,0 (3,8;4,4) 0,33GPT (D/l) 9 (7;13) 9 (7;14) 0,99GOT (D/l) 10 (8;12) 9 (8;12) 0,72Glukose* (mg/dl) 95 (88;104) 89 (80;102) 0,1Prothrombin (%) 108 (98;116) 102 (93;113) 0,15Cholesterol (mg/dl) 247 (213;285) 221 (201;266) 0,08Triglycerides (rng/dl) 151 (102;209) 154 (94;228) 0,92Creatinin (mg/dl) 1 (1;1) 1 (1;1) 0,16
* statistical relevance is not of clinical importance

8 S. Chrubasik et al.
Table 2. Pain scores, patient days with and without Tramadolconsumption and daily Tramadol consumption (mg).
VRS Patient Days Days Tramadol0-4 Days without with Consumption
Tramadol Tramadol Median, range
0-1 1143 1081 62 20 (3;70)2-3 196 875 321 20 (5;100)4 59 20 39 20 (5;100)
The relative change in the Arhus index
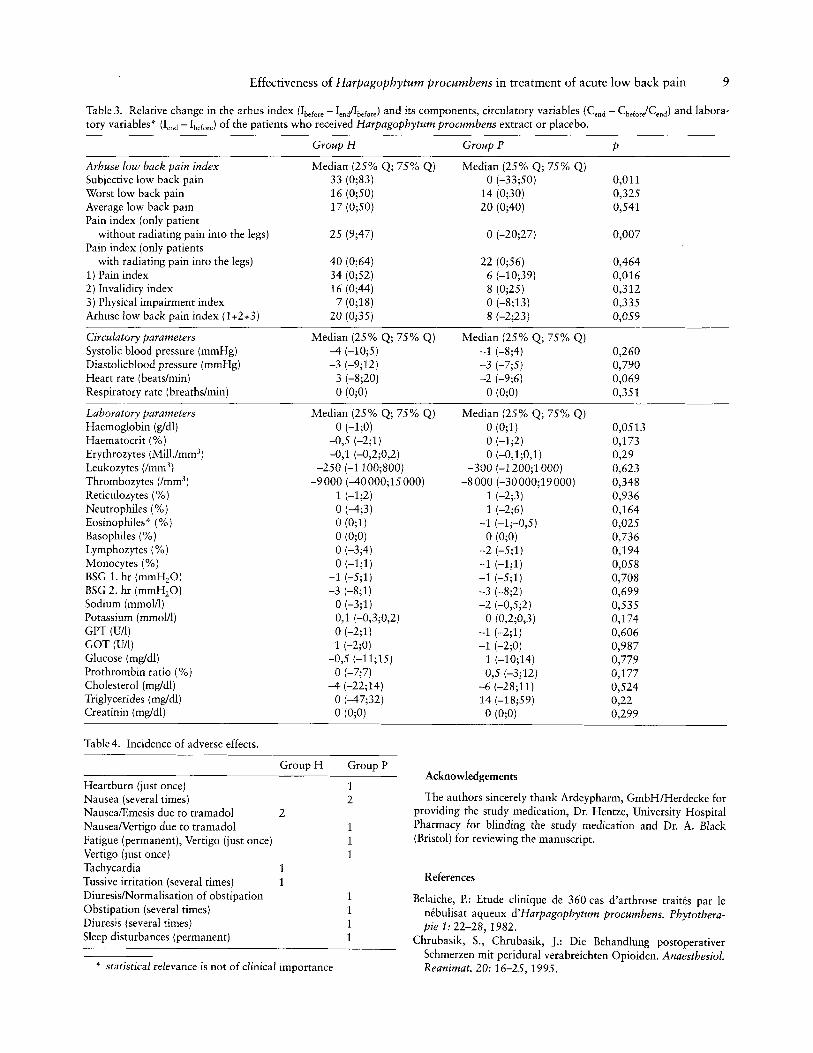
The Arhus index improved significantly in both groups(Wilcoxon paired rank sum) (Table 3). There was a medianchange of 20% relative to the initial value in group Handof 8% in group P. There was a 5.9% probability that thedifference between groups in the percentage change hadarisen by chance; this fell short of the stipulated criterionfor being considered significant. When the percentagechanges in the components of the Arhus index were considered separately (Table 3), the reductions in invalidity andphysical impairment tended to be greater in group H,though this did not approach significance but the change inthe pain index had only a 1.6% likelihood of arising bychance, and would have been considered highly significantif it had been the sole and principle measure of effectiveness. When this was examined further, the reduction in painwas confined almost entirely to the subgroup of patientswhose pain did not radiate to one or both legs.
Vital signs and laboratory measurements
There were insignificant changes in arterial blood pressure, heart rate and breathing rate, or in hematological andbiochemical screens, between the beginning and the end ofthe study, and between the two groups (Table 3). Table 4shows the incidence of clinical symptoms that were reported by patients in the two groups. The patient (group H)who suffered from sudden tachycardia after climaticchange and stopped taking the medication was treated withHarpagophytum procumbens after returning from vacationand tolerated the medication after that without any complaints.
Discussion
Four weeks of treatment with Harpagophytum procumbens appeared to have caused a greater number of patientsto become pain-free than did placebo, and a greater percentage reduction in the pain component of the Arhus lowback pain index (particularly in patients with no radiationto the legs). However, the rules of the randomized controlled study did not allow these conclusions to be drawndefinitively, because neither measure of effectiveness had
been stipulated beforehand as the principal outcome measure.
A change in Tramadol consumption was chosen as theprincipal outcome measure on the simplistic assumptionthat greater pain would tend to lead to greater consumption but that was probably confounded by the fact thatmost patients prefered a degree of pain to some of the sideeffects that can accompany most conventional analgesictreatments, including Tramadol. This cyclohexan derivativeacts, in part, through the opioid receptors and may producea range of opioid effects including nausea, emesis and sedation.
The Arhus index, although a promising convenient clinical tool for surveying the state of low back pain in asample, has been little used to study the effects of interventions and there is scant information whether interventions change all its components together or only some ofthem. Though the rules for this clinical trial of the effectsof Harpagopbytum procumbens prevent the investigatorsfrom drawing definitive conclusions, the trial is nevertheless valuable. Practicing phytotherapists may be reassuredby the absence of indentifiable clinical, hematological orbiochemical side effects. They may be happy on that basisto be more pragmatic in accepting a larger than 5% riskof being wrong in taking as valid the indications of benefit in the supplementary measurements of effectiveness.Those who prefer the more rigorous approach of the clinical trial will see the study as a possible valuable influenceon the design of a definitive study. It will be legitimate toconduct a fuller "post mortem" on alternative outcomemeasures that might have been examined with more elaborate and potentially more informative statistical approaches, so that information that was not available to
this study may be available to its successors. The successors need not necessarily restrict themselves to the question of whether an arbitrarily chosen dose of Harpagophytum has a detectable effect against placebo. There isprobably enough indication of safety to support futurestudies on the effects of higher dosage - to obtain clinicaldose-response characteristics.
Conclusion
Rigorous adherence to the accepted rules governing theconduct of clinical trials in general, and the declared rulesfor the study in particular, prevent the indications of benefit from Harpagopbytum procumbens from being acceptedwith 95% confidence. There are nonetheless sufficient indications of safety and benefit to suggest that further trialswill be worthwhile, and this study has amassed informationinvaluable planning them.
Effectiveness of Harpagopbytum procumbens in treatment of acute low back pain 9
Table 3. Relative change in the arhus index (Ibelare - Ienilbefare) and its components, circulatory variables (Cend - Cbefar/Cend) and laboratory variables* (lend - Ibelore) of the patients who received Harpagophytum procumbens extract or placebo.
Arhuse low back pain indexSubjective low back painWorst low back painAverage low back painPain index (only patient
without radiating pain into the legs)Pain index (only patients
with radiating pain into the legs)1) Pain index2) Invalidity index3) Physical impairment indexArhuse low back pain index (1+2+3)
Circulatory parametersSystolic blood pressure (mmHg)Diastolicblood pressure (mmHg)Heart rate (beats/min)Respiratory rate (breaths/min)
Laboratory parametersHaemoglobin (g/dl)Haematocrit (%)Erythrozytes (Mill.zrnrn")Leukozytes (/mm3 )
Thrombozytes (imm 3 )
Reticulozytes (%)Neutrophiles (%)Eosinophiles* (%)Basophiles (%)Lymphozytes (%)Monocytes (%)BSG 1. hr (mmHzO)BSG 2. hr (mmHzO)Sodium (rnmol/l)Potassium (mmol/l)GPT (UlI)GOT (U/I)Glucose (rng/dl)Prothrombin ratio (%)Cholesterol (rng/dl)Triglycerides (mg/dl)Creatinin (rng/dl)
Group H Group P p
Median (25% Q; 75% Q) Median (25% Q; 75% Q)33 (0;83) 0(-33;50) 0,01116 (0;50) 14 (0;30) 0,32517 (0;50) 20 (0;40) 0,541
25 (9;47) 0(-20;27) 0,007
40 (0;64) 22 (0;56) 0,46434 (0;52) 6 (-10;39) 0,01616 (0;44) 8 (0;25) 0,312
7 (0;18) 0(-8;13) 0,33520 (0;35) 8 (-2;23) 0,059
Median (25% Q; 75% Q) Median (25% Q; 75% Q)-4 (-10;5) -1 (-8;4) 0,260-3 (-9;12) -3 (-7;5) 0,790
3 (-8;20) -2 (-9;6) 0,0690(0;0) 0(0;0) 0,351
Median (25% Q; 75% Q) Median (25% Q; 75% Q)0(-1;0) 0(0;1) 0,0513
-0,5 (-2;1) 0(-1;2) 0,173-0,1 (-0,2;0,2) 0(-0,1;0,1) 0,29
-250 (-1100;800) -300 (-1200;1000) 0,623-9000 (-40000;15000) -8000 (-30000;19000) 0,348
1 (-1;2) 1 (-2;3) 0,9360(-4;3) 1 (-2;6) 0,1640(0;1) -1 (-1;-0,5) 0,0250(0;0) 0(0;0) 0,7360(-3;4) -2 (-5;1) 0,1940(-1;1) -1 (-1;1) 0,058
-1 (-5;1) -1 (-5;1) 0,708-3 (-8;1) -3 (-8;2) 0,699
0(-3;1) -2 (-0,5;2) 0,5350,1 (-0,3;0,2) 0(0,2;0,3) 0,1740(-2;1) -1 (-2;1) 0,606
-1 (-2;0) -1 (-2;0) 0,987-0,5 (-11;15) 1 (-10;14) 0,779
0(-7;7) 0,5 (-3;12) 0,177-4 (-22;14) -6 (-28;11) 0,524
0(-47;32) 14 (-18;59) 0,220(0;0) 0(0;0) 0,299
Table 4. Incidence of adverse effects.
Group H Group P
Heartburn (just once) 1Nausea (several times) 2Nausea/Emesis due to tramadol 2NauseaNertigo due to tramadol 1Fatigue (permanent), Vertigo (just once) 1Vertigo (just once) 1Tachycardia 1Tussive irritation (several times) 1Diuresis/Normalisation of obstipation 1Obstipation (several times) 1Diuresis (several times) 1Sleep disturbances (permanent) 1
* statistical relevance is not of clinical importance
Acknowledgements
The authors sincerely thank Ardeypharm, GmbH/Herdecke forproviding the study medication, Dr. Hentze, University HospitalPharmacy for blinding the study medication and Dr. A. Black(Bristol) for reviewing the manuscript.
References
Belaiche, P.: Etude c1inique de 360 cas d'arthrose traites par Ienebulisat aqueux d'Harpagophytum procumbens. Phytotherapie 1: 22-28,1982.
Chrubasik, 5., Chrubasik, J.: Die Behandlung postoperativerSchmerzen mit peridural verabreichten Opioiden, Anaesthesio!.Reanimat, 20: 16-25, 1995.

lOS. Chrubasik et al.
Chrubasik, 5., Wink, M.: Zur Wirksamkeit von Harpagophytumprocumbens. Forsch. Komplementiirmed. 2: 323-5,1995.
Chrubasik, 5., Ziegler, R.: Ruckenschmerzen, Therapiestrategie.Zschr. Allgem. Med. 1996 in press.
Chrubasik, 5., Sporer, E, Wink, M.: Zum Wirkstoffgehalt in Arzneimitteln aus Harpagophytum procumbens. Forschende Komplementarmed. in press, 1996.
Fairbank, J. C. T., Couper, J., Davies, J. B., O'Brian, J.: The Oswestry low back pain disability questionnaire. Physiotherapy66: 271-3, 1980.
Frymoyer, J. W.: Back pain and Sciatica. New Engl. J. Med. 318:291-300,1988.
Grahame, R., Robinson, B.v.: Devil's claw (Harpagopbytum procumbens}: pharmacological and clinical studies. Ann. Rheumatic Dis., 40: 12, 1981.
Greenough, C. G., Fraser, R. D.: Assessment of outcome in patientswith low-back pain. Spine 17: 36-41, 1992.
Harper, A.C., Harper, D.A., Lambert, L.J., DeKlerk, N.H., Andrews, H. B., Ross, EM., Straker, L.]., Lo, S.K: Developmentand validation of the Curtin back screening questionnaire(CBSQ): a discriminative disability measure. Pain 60: 73-81,1995.
Hildebrandt, J., Pfingsten, M., Ensink, E B.: Die Problematik derTherapie von Ruckenschrnerzen. Anasthesiol. Intensivmed.Notfallmed. 28: 148-155, 1993.
Hildebrandt, j.: Schmerzen am Bewegungsapparat, Ruckenschmerzen. In: Lehrbuch der Schmerztherapie, Hrsg. Zenz, M.,Jurna, I., Wissenschaftliche Verlagsgesellschaft Stuttgart, 351,1993.
Lawlis, G. E, Cuencas, R., Selby, D., McCoy, C. E.: The development of the Dallas Pain Questionnaire. Spine 14: 511-16,1988.
Lecomte, A., Costa, ]. P.: Harpagophytum dans l'arthrose. 37 LeMagazine N° 15, 1992.
Lehmann, T. R., Brand, R. A., Gorman, T.W.O.: A low-back Rating Scale. Spine 8: 308-16, 1983.
Manniche, c., Asmussen, K., Lauritsen, B., Vinterberg, H., Kreiner, S., Jordan, A.: Low Back Rating Scale: validation of a toolfor assessment of low back pain. Pain 57: 317-326,1994.
Million, R., Hall, W., Nilsen, K. H., Baker, R. D., Jayson, M. I. v..Assessment of the progress of the back-pain patient. Spine 7:4-12,1982.
Pinget, M., Lecomte, A.: Etude des effets de l'harpagophytum enrhumatologie degenerative. 37 Le magazine N° 10,1990.
Portenoy, R. K, Foley, K M.: Chronic use of opioid analgesics innon-malignant pain: report of 38 cases. Pain 25: 171-186,1986.
Spratt, K E, Lehmann, T. R., Weinstein, J. N., Sayre, H. A.: A newapproach to the low-back physical examination. Spine 15:96-102,1990.
Vallfors, B.: Acute, subacute and chronic low back pain: clinicalsymptoms, absenteeism and working environment. Scand. J. Rehab. Med. Suppl. 1: 1-98, 1985.
Waddell, G.: Clinical assessment and lumbal impairment. Clin.Orthop. ReI. Res. 221: 209-13,1984.
Waddell, G., Main, c.].: Assessment of severity in low-back disorders. Spine 9: 209-13,1984.
Zimmermann, W.: Erfahrungen mit Harpagophytum. Phys. Med.Reh. 18: 317-319, 1977.
Zimmermann, M.: Opioide fur nicht tumorbedingte chronischeSchmerzen? Schmerz 4: 121-122, 1990.
Address
S. Chrubasik, Department of Internal Medicine I, University Hospital, Bergheimerstr.58, 69115 Heidelberg, Germany.


















