Effect of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Levels in Children with Chronic...
18
Effect of Vitamin D Supplementation on Serum 25- Hydroxyvitamin D Levels in Children with Chronic Disease Primary investigators: Tania Vander Meulen, MEd, Dietetic Intern Josee Beauchamp, MSc,RD Krista Wadden, RD
-
Upload
alfred-atkins -
Category
Documents
-
view
214 -
download
2
Transcript of Effect of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Levels in Children with Chronic...

Effect of Vitamin D Supplementation on
Serum 25-Hydroxyvitamin D Levels in Children with Chronic
Disease
Primary investigators: Tania Vander Meulen, MEd, Dietetic Intern
Josee Beauchamp, MSc,RDKrista Wadden, RD

Outline
Acknowledgements Introduction Current Literature Objectives Methodology Results Conclusions Questions

Acknowledgements
A special thanks to the following who have contributed to my research project: Beauchamp, J. RD, MSc.; Research advisor Wadden, K. RD; Research advisor Gariepy, L. Ph.D. Candidate; Statistitian Murphy, J. RD; Research Mentor Khouzam, B.DtP, MAP; Research
Coordinator Kennedy, C. RD; Peer Reviewer

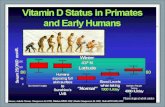
Introduction
40-70% of children with IBD and CF are vitamin D deficient and have low [25(OH)D] (1,2,3) due to: malabsorption impaired hydroxylation of vitamin D altered concentration or activity of 25-
hydroxylase enzyme low albumin levels lack of adequate sunlight increased use of sunscreen steroid therapy
1.Stephenson A. American Journal of Clinical Nutrition 20072. Pappa HM. Pediatrics 20063. Udall JN. American Journal of Clinical Nutrition 2002

Current Literature-25(OH)D
The most accurate way to test vitamin D status is [25(OH)D].
25(OH)D reflects dietary intake: For every 40 IU/day, 25(OH)D increases by
0.70nmol/L (4,6) or 1-2 nmol/L (7). 25(OH)D reflects subcutaneous synthesis:
Vitamin D derived from sunlight exposure can account for 80% of vitamin D levels (23)
How much vitamin D is needed to raise [25(OH)D] above 80nmol/L? Some studies have shown 200-800 IU inadequate in
children with IBD and CF (1,4,6,7,14) Some researchers suggest 1000-1300IU may be
needed (1,6)4. Aris RMJournal of Clinical Endocrinology and Metabolism 20046. Heany RP. American Journal of Clinical Nutrition 20047. Cranney A. University of Ottawa Evidence-based Practice Center 200723. Rayner RJ. Proceedings of the Nutrition Society 1992; 51: 245-50.

Current Literature-BMD
Children with IBD or CF have a 40% greater risk of developing a bone fracture than healthy counterpart (15)
Although [25(OH)D] is often used as a marker of bone health, many researchers have not found a positive correlation between [25(OH)D] and BMD (16,18,19).
BMD lower in IBD subjects compared to healthy subjects, despite normal 25(OH)D levels. (21)
16% of children and young adults with CD (n= 112) had vitamin D deficiency but no association was found between low vitamin D intake and BMD. (22)16.Boyle MP. American Journal of Respiratory and Critical Care Medicine 2005
18. Grey V. American Journal of Pediatric Gastroenterology 2000

Current Literature-Seasonal Influence
[25(OH)D] often higher in summer due to greater sun exposure
49nmol/L difference between late summer and late winter in 30 healthy men (24)
Lower winter concentrations in adult CD patients (25)
33.4% lower [25(OH)D] during the winter months in pediatric IBD subjects (2)
19. O’Sullivan M. Best Practice & Clinical Gastroenterology 200621. Sentongo TA. American Journal of Clinical Nutrition 200222. Paganeli M. Journal of Pediatric Gastroenterology 200524. Barger-Lux J. The Journal of Clinical Endocrinology & Metabolism 2002 25. McCarthy D. Alimentary Pharmacology & Therapeutics 2005

Objectives
Primary Objective:
Determine if a daily increase of vitamin D coming from food and/or supplementation for a period of at least six months would increase [25(OH)D] by 10nmol/L in children with CD, UC, IC and CF that had a [25(OH)D] below 80nmol/L.
Secondary Objectives:1) Compare the success of vitamin D
supplementation in raising [25(OH)D] above 10nmol/L in CD, UC, IC and CF individually.
2) Determine if there was a correlation between 25(OH)D and Z-score lumbar BMD.

Methodology
209 IBD and 14 CF subjects aged 4-18, were assessed for Vitamin D intake (via food frequency/supplement questionnaire) and [25(OH)D] at baseline and again at 6-8 months
Subjects with [25(OH)D] <80nmol/L were encouraged to increase vitamin D by 400 IU via food and/or supplementation.
50 subjects were eliminated due to: Decreased vitamin D intake [25(OH)D] taken at more than 1.5 months of vitamin D
assessment Presence of additional disease (diabetes, sclerosing
cholangitis, celiac disease) Failure to complete second assessment

Methodology
Of the 173 IBD subjects remaining: 104 CD 50 UC 5 IC 14 CF
Demographic data collected: age, DOB, date of diagnosis, diagnosis, gender
Other data collected: sed rate, C-protein, albumin, steroid use, season of assessment (spring vs winter)

Methodology
Bone mineral data collected in 80 subjects via DEXA: lumbar z-score, total body z-score, bone age
Statistical analysis was performed using SPSS software:
Paired t-tests used to compare vitamin D intake and [25(OH)D] at baseline and six to eight months, as well as mean values of [25(OH)D] between season (winter vs summer).
Standard pearson correlations used to correlate [25(OH)D], Z-score lumbar BMD and Z-score total body BMD.
Significance was set at p<0.05 for all analysis

Results
Figure 1. Change in vitamin D intake at baseline and 6-8 months
Change in Vitamin D Intake
0
200
400
600
800
1000
1200
CD UC IC CF total
Subjects
Vit
amin
D (
IU)
baseline
6-8months
**
*
* = p<0.05

Results
Figure 2. Change in [25(OH)D] at baseline and 6-8 months.
Change in [25(OH)D]
0
20
40
60
80
100
120
CD UC IC CF Total
Subjects
[25(
OH
)D]
(nm
ol/
L)
baseline
6-8months* * *
* = p<0.05

Results
All: A significant increase of 329 IU (+- S.E. 28.4) vitamin
D/d raised [25(OH)D] by 14.5 nmol/L (+- S.E. 2.18) within 7.2 months.
CD: A significant increase of 347 IU/d (+-S.E. 32.2) raised
[25(OH)D] by 13.4 nmol/L (+-S.E. 2.92)
UC: A significant increase of 314 IU/d (+-S.E. 62.2) raised
[25(OH)D] by 18.1 nmol/L (+-S.E. 4.1)
IC & CF: No significant change in vitamin D or [25(OH)D]

Results
Relationship between [25(OH)D] and
BMD
Pearson correlation revealed no significant relationship between [25(OH)D] and z-score lumbar BMD (p=0.84), or [25(OH)D] and z-score total body BMD (p=0.82).

Results
Table 2. Increase in [25(OH)D] according to season
Baseline 6-8 Months Difference_Season Subjects (N) Mean Mean Mean S.E.
Winter 23 57.1 68.5 11.4 4.6***Summer 15 59.7 78.3 18.3 8.5***
S.E. = standard error ***p<0.05
To get a true reflection of vitamin D intake alone on [25(OH)D], we eliminated seasonal effect by eliminating those subjects who had both vitamin D assessments in different seasons.
[25(OH)D] According to Season

Conclusions
An increase of 329 IU vitamin D did significantly increase [25(OH)D] by 14.5 nmol/L within 7.2 months.
Despite increase, most subjects still remained below 80nmol/L.
The current recommendation of 400 IU vitamin D is inadequate to normalize serum [25(OH)D] in IBD and CF populations
Vitamin D intake may need to be greater than 1000 IU to raise [25(OH)D] over 80nmol/L.

Questions