Effect of topical corticosteroids on seasonal increases in epithelial eosinophils and mast cells in...
9
Effect of topical corticosteroids on seasonal increases in epithelial eosinophils and mast cells in allergic rhinitis: a comparison of nasal brush and biopsy methods M. R. JACOBSON, S. JULIUSSON*, O. LO ¨ WHAGEN², B. BALDER², A. B. KAY‡ and S. R. DURHAM Upper Respiratory Medicine, Imperial College School of Medicine at the National Heart and Lung Institute, London, UK, *Department of Lung Medicine, University Hospital of Iceland, Reykjavik, Iceland, ²Sahlgrenska Hospital, Go ¨theburg, Sweden and ‡Allergy and Clinical Immunology, Imperial College School of Medicine at National Heart and Lung Institute, London, UK. Summary Background Nasal brushing and nasal biopsy are well-tolerated sampling techniques. Seasonal grass pollen-induced rhinitis is characterized by epithelial mast cell infiltration and seasonal increases in both epithelial and sub-mucosal eosinophils. Objective To compare the ability of the nasal brush and nasal biopsy techniques to detect natural seasonal increases in eosinophils and mast cells, and to assess the influence of topical corticosteroid. Methods Nasal brush samples and nasal biopsies were collected from 46 grass pollen- sensitive seasonal rhinitis patients before the grass pollen season and at the peak of the pollen season following 6 weeks’ treatment with either fluticasone propionate aqueous nasal spray (200 mg, twice daily) or placebo nasal spray. Results Placebo patients showed seasonal increases in epithelial eosinophils both with nasal brushing (P < 0.0001) and biopsy (P < 0.001). Epithelial mast cell numbers also increased during the pollen season as detectable by brushing (P < 0.0001) and biopsy (P < 0.03). Changes in cell numbers measured by nasal brushing correlated with those observed with nasal biopsy, both for eosinophils and mast cells (P < 0.05). Sub-mucosal eosinophils but not mast cells also increased during the pollen season (P < 0.002). Nasal brushing and biopsy revealed that fluticasone treatment inhibited seasonal increases in epithelial eosinophils (P < 0.00001) and epithelial infiltration by mast cells (nasal brushing P < 0.00001 and nasal biopsy P < 0.01). Fluticasone also inhibited seasonal increases in sub- mucosal eosinophils (P < 0.001) and significantly reduced nasal symptoms (P < 0.001). Conclusion Nasal brushing harvests sufficient inflammatory cells from the surface of the nasal mucosa to be used in lieu of nasal biopsies in observation of the effect of drugs on the nasal epithelium. Keywords: biopsy, corticosteroids, eosinophils, mast cells, nasal brushing, seasonal allergic rhinitis Clinical and Experimental Allergy, Vol. 29, pp. 1347–1355. Submitted 21 August 1998; revised 9 December 1998; accepted 30 January 1999. Introduction Seasonal allergic rhinitis due to grass pollen is characterized by nasal discharge, blockage, sneezing and itching. One of Clinical and Experimental Allergy, 1999, Volume 29, pages 1347–1355 1347 q 1999 Blackwell Science Ltd Correspondence: S. R. Durham, Upper Respiratory Medicine, Imperial College School of Medicine at National Heart and Lung Institute, Dovehouse Street, London SW3 6LY, UK.
Transcript of Effect of topical corticosteroids on seasonal increases in epithelial eosinophils and mast cells in...

Effect of topical corticosteroids on seasonal increases in
epithelial eosinophils and mast cells in allergic rhinitis: a
comparison of nasal brush and biopsy methods
M. R. JACOBSON, S. JULIUSSON*, O. LOÈ WHAGEN², B. BALDER², A. B. KAY³and S. R. DURHAM
Upper Respiratory Medicine, Imperial College School of Medicine at the National Heart and Lung Institute, London, UK,
*Department of Lung Medicine, University Hospital of Iceland, Reykjavik, Iceland, ²Sahlgrenska Hospital, GoÈtheburg,
Sweden and ³Allergy and Clinical Immunology, Imperial College School of Medicine at National Heart and Lung Institute,
London, UK.
Summary
Background Nasal brushing and nasal biopsy are well-tolerated sampling techniques.
Seasonal grass pollen-induced rhinitis is characterized by epithelial mast cell in®ltration and
seasonal increases in both epithelial and sub-mucosal eosinophils.
Objective To compare the ability of the nasal brush and nasal biopsy techniques to detect
natural seasonal increases in eosinophils and mast cells, and to assess the in¯uence of
topical corticosteroid.
Methods Nasal brush samples and nasal biopsies were collected from 46 grass pollen-
sensitive seasonal rhinitis patients before the grass pollen season and at the peak of the
pollen season following 6 weeks' treatment with either ¯uticasone propionate aqueous nasal
spray (200 mg, twice daily) or placebo nasal spray.
Results Placebo patients showed seasonal increases in epithelial eosinophils both with
nasal brushing (P < 0.0001) and biopsy (P < 0.001). Epithelial mast cell numbers also
increased during the pollen season as detectable by brushing (P < 0.0001) and biopsy
(P < 0.03). Changes in cell numbers measured by nasal brushing correlated with those
observed with nasal biopsy, both for eosinophils and mast cells (P< 0.05). Sub-mucosal
eosinophils but not mast cells also increased during the pollen season (P< 0.002). Nasal
brushing and biopsy revealed that ¯uticasone treatment inhibited seasonal increases in
epithelial eosinophils (P < 0.00001) and epithelial in®ltration by mast cells (nasal brushing
P < 0.00001 and nasal biopsy P < 0.01). Fluticasone also inhibited seasonal increases in sub-
mucosal eosinophils (P < 0.001) and signi®cantly reduced nasal symptoms (P < 0.001).
Conclusion Nasal brushing harvests suf®cient in¯ammatory cells from the surface of the
nasal mucosa to be used in lieu of nasal biopsies in observation of the effect of drugs on the
nasal epithelium.
Keywords: biopsy, corticosteroids, eosinophils, mast cells, nasal brushing, seasonal
allergic rhinitis
Clinical and Experimental Allergy, Vol. 29, pp. 1347±1355. Submitted 21 August 1998;
revised 9 December 1998; accepted 30 January 1999.
Introduction
Seasonal allergic rhinitis due to grass pollen is characterized
by nasal discharge, blockage, sneezing and itching. One of
Clinical and Experimental Allergy, 1999, Volume 29, pages 1347±1355
1347q 1999 Blackwell Science Ltd
Correspondence: S. R. Durham, Upper Respiratory Medicine, Imperial
College School of Medicine at National Heart and Lung Institute,
Dovehouse Street, London SW3 6LY, UK.

the prominent features of allergic rhinitis is the in®ltration
of the nasal mucosa by in¯ammatory cells. These cells
secrete mediators and cytokines which give rise to the
symptoms and regulation of the disease. We previously
used the biopsy technique to demonstrate that seasonal
allergic rhinitis is accompanied by local tissue eosinophilia
and epithelial migration of tryptase-only (MCT) mast cells
[1]. These cellular increases are thought to be regulated by
the local production and release of cytokines such as IL-4,
IL-5 and IL-6. Immunoreactivity for these particular cyto-
kines has been localized to mast cells and in addition, to
eosinophils in the case of IL-5, in the nasal mucosa of
patients with seasonal allergic rhinitis [2]. We have shown a
seasonal increase in IL-5 mRNA expression in the nasal
mucosa of patients with seasonal allergic rhinitis [3].
Various techniques are available to sample the cellular
component of the nasal mucosa. Nasal lavage, mucosal
scraping, mucosal imprints, blown secretions, nasal
smears and nasal brushings all sample the mucosal surface
and secretions [4]. Nasal brushing is thought to harvest a
proportion of the cells within the nasal epithelial lining and
thus provide more information than nasal lavage [5]. Nasal
brushing is a simple, safe, noninvasive, well-tolerated
technique which is useful for repeated harvesting of cells
from the nasal mucosa [6] and also for studying the nasal
surface of children [7,8]. Nasal brushing yields cell samples
with well-preserved cytological detail, easy to identify on
morphological criteria [5,9]. Nasal biopsy, although more
invasive, is also a well-tolerated technique [10]. Nasal
biopsy is advantageous in that it enables studies of both
the nasal epithelium and sub-mucosa providing a broader
picture of the pathogenesis of allergic rhinitis. Nasal biopsy
and brushing have previously only been compared in an
allergen -challenge study assessing the dynamics of nasal
eosinophilia during a period of prolonged allergen exposure
[6]. Nasal mucosal scraping has been used to assess the
effect of intranasal ¯uticasone propionate [11] but this paper
is novel in its use of nasal brushings to assess the effect of
corticosteroids on the in¯ammatory cells of the nasal
epithelium.
Topical steroids are highly effective in the treatment of
allergic rhinitis [12,13]. Pretreatment with intranasal ster-
oids inhibits the seasonal in¯ux of eosinophils and mast
cells into the nasal secretions and mucosa of patients with
seasonal allergic rhinitis [2,14,15]. Fluticasone propionate
aqueous nasal spray is a topically active corticosteroid
molecule of known ef®cacy [16,17] and minimal systemic
adverse effects.
This study compares the nasal brush and nasal biopsy
techniques with regards to their ability to detect natural
seasonal changes in both eosinophils and mast cells. In
addition we tested the ability of these techniques to allow
observation of drug-induced changes.
Materials and methods
Patients
Forty-six non-smoking timothy grass pollen-sensitive
patients were recruited from the outpatient clinic of the
Asthma and Allergy Centre, Department of Medicine,
Sahlgrenska Hospital, GoÈtheburg, Sweden. They were
selected on the basis of (1) a clinical history of moderate
to severe hay fever for at least 2 years, and (2) a positive skin
prick test (weal diameter greater than 5 mm) to grass pollen
extract (Phleum pratense Soluprick; ALK, Horsholm, Den-
mark). Venous blood was taken for measurement of total
and allergen-speci®c IgE concentrations by ELISA. Patients
were excluded if they had a history of birch pollen allergy,
perennial allergy, had received immunotherapy in the last
5 years or had taken oral or topical corticosteroids in the
previous 6 months.
Study design
The study was performed with the approval of the hospital
Ethics Committee and the written informed consent of all
participants. The 46 patients were divided into two groups
(moderate and severe) on the basis of their disease severity
as determined by clinical history and their skin prick test.
`Severe' � history of symptoms on most days for at least 10
weeks during the pollen season and a skin prick test
> 10 mm; `moderate' � patients with seasonal symptoms
who did not ful®l all of the above criteria. Patients in each
group were then randomized separately to receive either
¯uticasone propionate aqueous nasal spray 200 mg twice
daily (Flixonase, Glaxo, Sweden) or matched placebo spray
(containing the aqueous diluent) to ensure an even distribu-
tion of disease severity in the active and placebo groups.
Baseline nasal brushing followed by nasal biopsy of the
opposite nostril was performed out of season at a time when
all patients were asymptomatic. There was a two week run-
in period during which patients recorded symptoms on a
diary card. Repeat nasal sampling took place 6 weeks after
treatment with ¯uticasone or matched placebo spray timed
to correspond with the week following the peak pollen
count. The side of biopsy/brush was reversed relative to
the baseline samples.
Diary cards
Patients were provided with 2-week diary cards throughout
the study period and were asked to keep a daily record of all
their symptoms of rhinitis namely: nasal blockage; sneez-
ing; rhinorrhoea (nasal discharge) and nasal itching. Symp-
toms were individually assessed using a four-point rating
scale from 0 (no symptoms) to 4 (breathing through nose
very dif®cult, more than 10 episodes a day of sneezing,
1348 M. R. Jacobson et al.
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355

persistent distraction of discharge and itching). The diary
card symptom scores were summarized by the percentage of
symptom-free days for each symptom separately.
Nasal brushing
A commercially available 5.5 mm diameter nylon brush
(Doft AB, OÈ sthammar, Sweden) was used for cell sampling.
The brush was placed between the nasal septum and the
inferior turbinate and removed gently whilst being rotated
90 8 [5]. No anaesthesia was used. After sampling the brush
was placed immediately in a 3-mL plastic tube containing
2 mL phosphate-buffered saline. The brush was then shaken
vigorously in the solution and carefully brushed off against
the side of the wall. Aliquots (100 mL) of the cell suspension
were loaded into a cytocentrifuge (Cytocentrifuge II, Shan-
don Southern Products Ltd, Cheshire, UK), spun for 7 min at
750 r.p.m., and air dried prior to storing at ÿ 80 8C wrapped
in foil.
Nasal biopsy
Local anaesthesia of the inferior nasal turbinate was
achieved using 3% cocaine and 0.025% adrenaline. After
10 minutes a 2.5-mm biopsy was taken using Gerritsma
forceps [10]. Biopsies were snap frozen and stored at
ÿ 80 8C for immunohistology.
Immunohistology
Immunohistology was performed on 6-mm cryostat sections
(®xed for 7 min in 60 : 40; acetone : methanol) using the
alkaline phosphatase-anti-alkaline phosphatase method as
described previously [1]. Anti-major basic protein (MBP)
antibody, BMK13 (IgG1) was kindly provided by Miss J.
Barkans and Dr R. Moqbel to quantify the total number of
eosinophils in samples. Monoclonal antibody recognizing
mast cell tryptase (IgG1) labelled with alkaline phosphatase
was obtained from Chemicon International, London, UK.
Cytospin slides were brought to room temperature then
®xed in methanol (5 min) prior to incubation with BMK13
or were ®xed in Carnoys ¯uid (60% ethanol: 30% chloro-
form: 10% glacial acetic acid) for 15 min prior to incubation
with antitryptase. Human allergen-challenged nasal biopsies
were used as positive controls and mouse IgG1 (anti-
Aspergillus niger glucose oxidase) was used as a negative
control (Dako Ltd, High Wycombe, UK).
Quanti®cation
Slides were counted blind using an Olympus BH2 micro-
scope (Olympus Optical company Ltd, Tokyo, Japan) with
an eye piece grid (0.202 mm2 at 200 ´ magni®cation). At
least two tissue sections (giving a minimum of six micro-
scope ®elds) were counted per patient. For epithelial counts
the cross-sectional area of the nasal epithelium was quanti-
®ed by use of a computer-assisted graphics tablet. Counts
were expressed per square millimetre of epithelium. Sub-
mucosal counts were made one grid depth (0.45 mm)
beneath the basement membrane and were expressed as
mean counts per square millimetre of sub-mucosa. Cytospin
eosinophil counts were made in the four ®elds of view
labelled `1' in Fig. 1. A total of 300 cells were counted at
each position. If there were less than 300 cells in ®eld 1 then
counts continued in ®elds 2 and 3 as necessary. The number
of eosinophils within this 300 was recorded. The results for
the four areas were summed and the number of eosinophils
was recorded as a percentage of the total cell count.
Cytospin mast cell counts were made by counting all the
mast cells within the cytospin. The total cell count for the
entire cytospin was then estimated by counting the number
of cells in the four ®elds labelled `1' (Fig. 1) and multi-
plying up. Mast cells were expressed as a percentage of total
cells.
Statistical analysis
Wilcoxon matched-pairs signed rank test was used for
within-group comparisons (peak season counts minus pre-
season counts). Between group comparisons were made
using the Mann Whitney U-test. Correlations were per-
formed using Spearman's rank method. P-values less than
Topical corticosteroid use in rhinitis 1349
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355
3
1 1
332
1 2
2 1
3 2
Fig. 1. Diagrammatic representation of cytospin demonstrating the
position of microscope ®elds of view at ´ 20 magni®cation.
0.05 were considered statistically signi®cant. Statistical
tests were performed using a standard computer package
(MiniTab Inc., PA, USA).
Results
All 46 patients completed the study and underwent two
nasal biopsies and two nasal brushings. The ¯uticasone
group (n� 23) and placebo group (n� 23) were well
matched for age, gender, disease severity and for their
degree of grass pollen sensitivity as determined by skin
prick tests and allergen-speci®c IgE antibody concentrations
(Table 1). With the exception of two patients all patients had
suffered from seasonal rhinitis for at least 5 years.
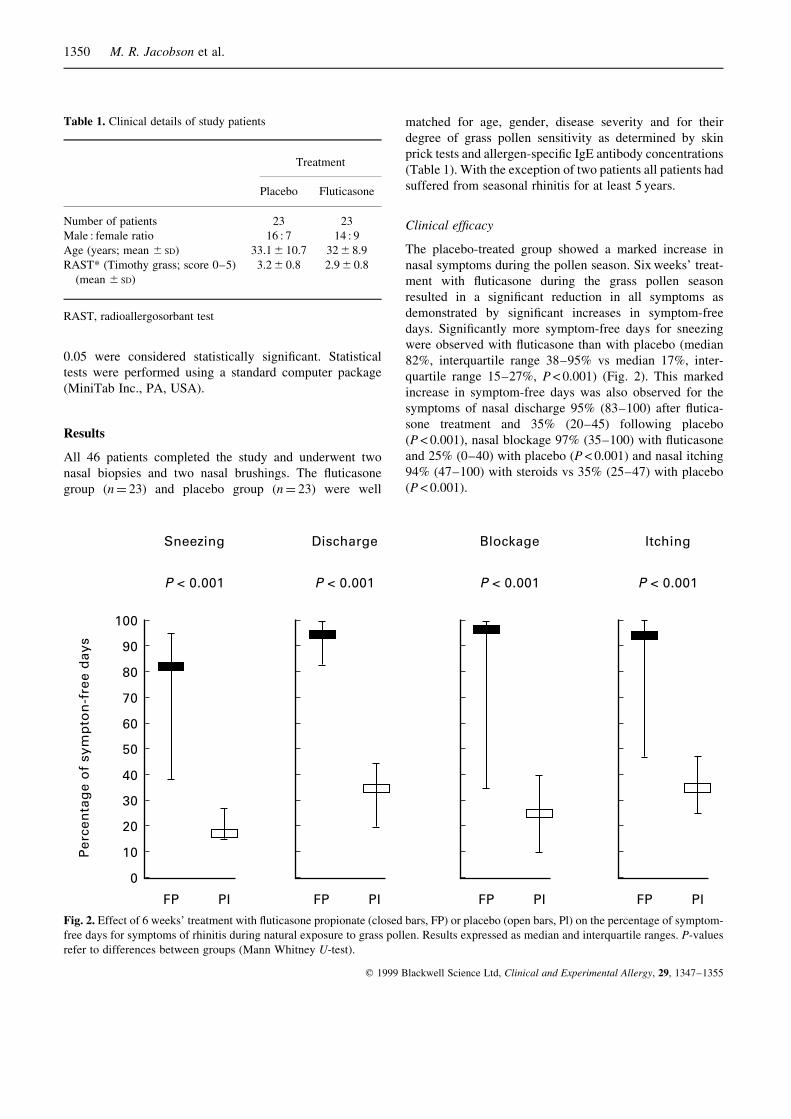
Clinical ef®cacy
The placebo-treated group showed a marked increase in
nasal symptoms during the pollen season. Six weeks' treat-
ment with ¯uticasone during the grass pollen season
resulted in a signi®cant reduction in all symptoms as
demonstrated by signi®cant increases in symptom-free
days. Signi®cantly more symptom-free days for sneezing
were observed with ¯uticasone than with placebo (median
82%, interquartile range 38±95% vs median 17%, inter-
quartile range 15±27%, P< 0.001) (Fig. 2). This marked
increase in symptom-free days was also observed for the
symptoms of nasal discharge 95% (83±100) after ¯utica-
sone treatment and 35% (20±45) following placebo
(P < 0.001), nasal blockage 97% (35±100) with ¯uticasone
and 25% (0±40) with placebo (P < 0.001) and nasal itching
94% (47±100) with steroids vs 35% (25±47) with placebo
(P < 0.001).
1350 M. R. Jacobson et al.
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355
Table 1. Clinical details of study patients
Treatment
Placebo Fluticasone
Number of patients 23 23
Male : female ratio 16 : 7 14 : 9
Age (years; mean 6 SD) 33.1 6 10.7 32 6 8.9
RAST* (Timothy grass; score 0±5) 3.2 6 0.8 2.9 6 0.8
(mean 6 SD)
RAST, radioallergosorbant test
100
90
80
70
60
50
40
30
20
10
0
Per
cen
tag
e o
f sy
mp
ton
-fre
e d
ays
Sneezing
P < 0.001
FP PI
Discharge
P < 0.001
FP PI
Blockage
P < 0.001
FP PI
Itching
P < 0.001
FP PI
Fig. 2. Effect of 6 weeks' treatment with ¯uticasone propionate (closed bars, FP) or placebo (open bars, Pl) on the percentage of symptom-
free days for symptoms of rhinitis during natural exposure to grass pollen. Results expressed as median and interquartile ranges. P-values
refer to differences between groups (Mann Whitney U-test).
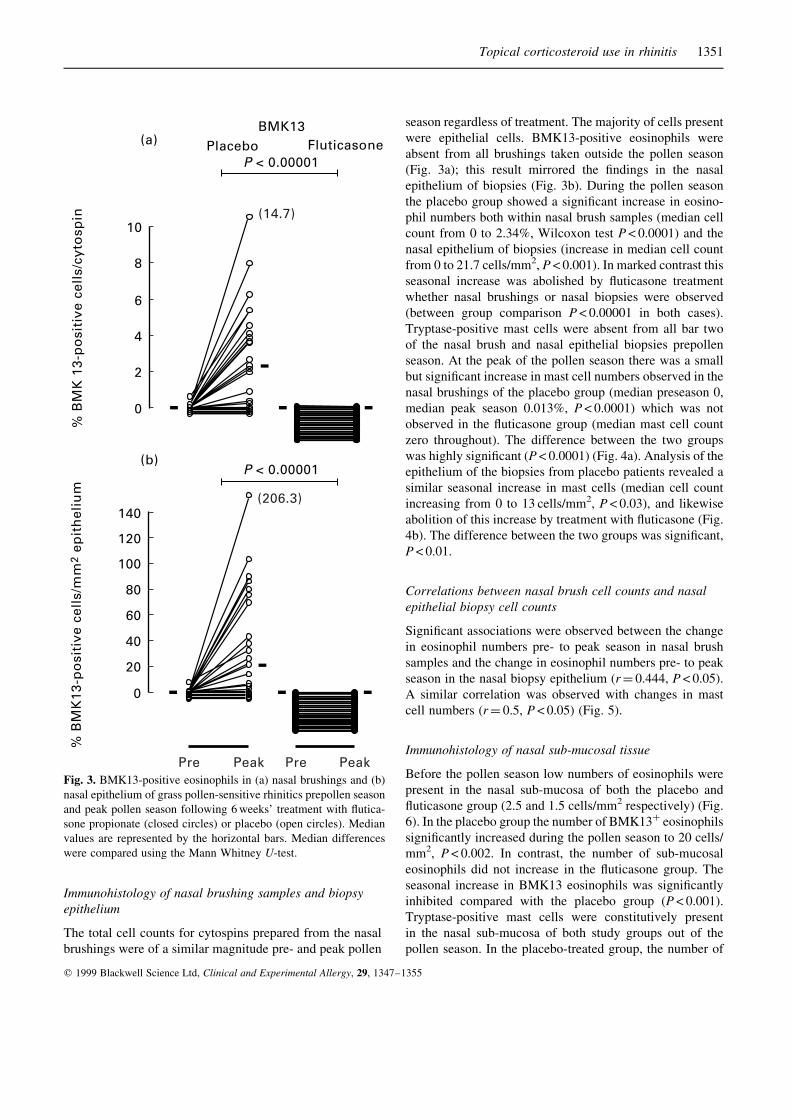
Immunohistology of nasal brushing samples and biopsy
epithelium
The total cell counts for cytospins prepared from the nasal
brushings were of a similar magnitude pre- and peak pollen
season regardless of treatment. The majority of cells present
were epithelial cells. BMK13-positive eosinophils were
absent from all brushings taken outside the pollen season
(Fig. 3a); this result mirrored the ®ndings in the nasal
epithelium of biopsies (Fig. 3b). During the pollen season
the placebo group showed a signi®cant increase in eosino-
phil numbers both within nasal brush samples (median cell
count from 0 to 2.34%, Wilcoxon test P< 0.0001) and the
nasal epithelium of biopsies (increase in median cell count
from 0 to 21.7 cells/mm2, P < 0.001). In marked contrast this
seasonal increase was abolished by ¯uticasone treatment
whether nasal brushings or nasal biopsies were observed
(between group comparison P< 0.00001 in both cases).
Tryptase-positive mast cells were absent from all bar two
of the nasal brush and nasal epithelial biopsies prepollen
season. At the peak of the pollen season there was a small
but signi®cant increase in mast cell numbers observed in the
nasal brushings of the placebo group (median preseason 0,
median peak season 0.013%, P< 0.0001) which was not
observed in the ¯uticasone group (median mast cell count
zero throughout). The difference between the two groups
was highly signi®cant (P< 0.0001) (Fig. 4a). Analysis of the
epithelium of the biopsies from placebo patients revealed a
similar seasonal increase in mast cells (median cell count
increasing from 0 to 13 cells/mm2, P < 0.03), and likewise
abolition of this increase by treatment with ¯uticasone (Fig.
4b). The difference between the two groups was signi®cant,
P < 0.01.
Correlations between nasal brush cell counts and nasal
epithelial biopsy cell counts
Signi®cant associations were observed between the change
in eosinophil numbers pre- to peak season in nasal brush
samples and the change in eosinophil numbers pre- to peak
season in the nasal biopsy epithelium (r� 0.444, P < 0.05).
A similar correlation was observed with changes in mast
cell numbers (r� 0.5, P < 0.05) (Fig. 5).
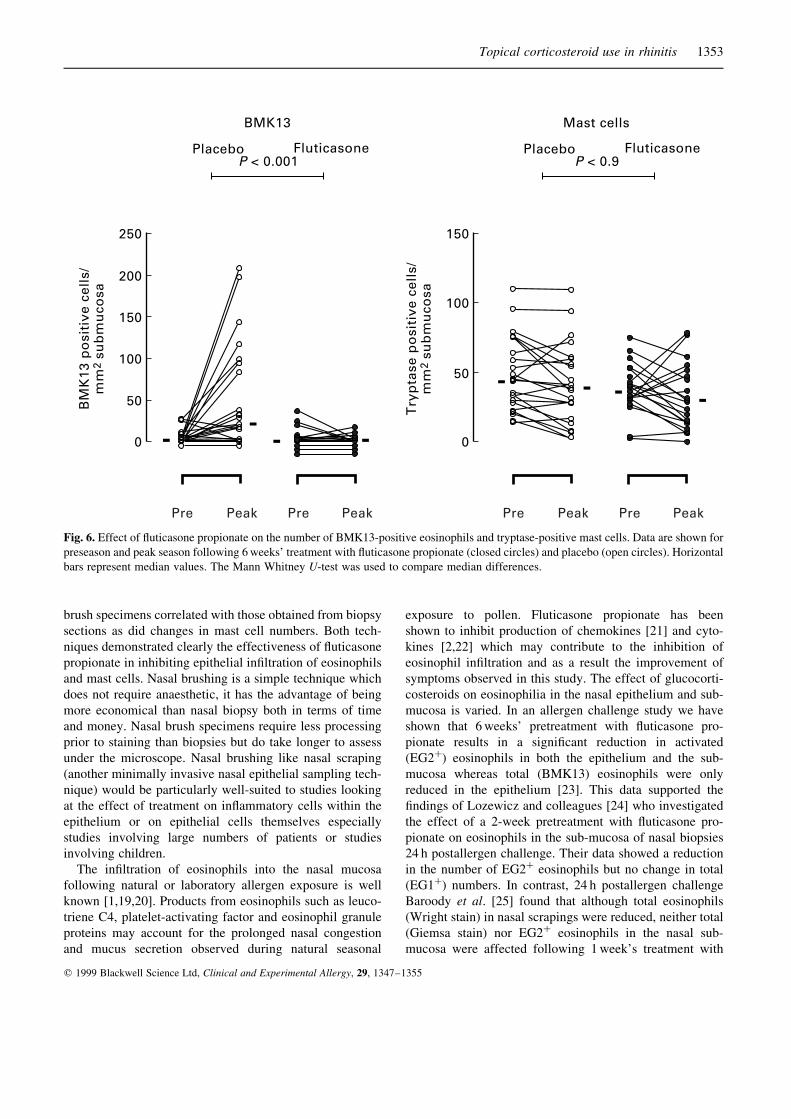
Immunohistology of nasal sub-mucosal tissue
Before the pollen season low numbers of eosinophils were
present in the nasal sub-mucosa of both the placebo and
¯uticasone group (2.5 and 1.5 cells/mm2 respectively) (Fig.
6). In the placebo group the number of BMK13� eosinophils
signi®cantly increased during the pollen season to 20 cells/
mm2, P< 0.002. In contrast, the number of sub-mucosal
eosinophils did not increase in the ¯uticasone group. The
seasonal increase in BMK13 eosinophils was signi®cantly
inhibited compared with the placebo group (P< 0.001).
Tryptase-positive mast cells were constitutively present
in the nasal sub-mucosa of both study groups out of the
pollen season. In the placebo-treated group, the number of
Topical corticosteroid use in rhinitis 1351
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355
10
8
6
4
2
0
% B
MK
13-
po
siti
ve c
ells
/cyt
osp
in
(a)
(b)
BMK13Placebo Fluticasone
P < 0.00001
(14.7)
100
120
140
80
60
40
20
0
% B
MK
13-p
osi
tive
cel
ls/m
m2
epit
hel
ium
P < 0.00001
(206.3)
Pre Peak Pre PeakFig. 3. BMK13-positive eosinophils in (a) nasal brushings and (b)
nasal epithelium of grass pollen-sensitive rhinitics prepollen season
and peak pollen season following 6 weeks' treatment with ¯utica-
sone propionate (closed circles) or placebo (open circles). Median
values are represented by the horizontal bars. Median differences
were compared using the Mann Whitney U-test.

sub-mucosal mast cells did not change during the pollen
season. Furthermore, in contrast with the epithelial ®ndings,
¯uticasone treatment had no effect on sub-mucosal mast cell
numbers.
Discussion
We have shown that nasal brushing and nasal biopsy both
detect an increase in epithelial eosinophils and mast cells
during seasonal grass pollen-induced rhinitis. Nasal brush-
ing and nasal biopsy both revealed total inhibition of the
seasonal increases in epithelial eosinophils and mast cells
following ¯uticasone therapy. Seasonal sub-mucosal eosi-
nophilia was observed in the nasal biopsies and this was also
inhibited by ¯uticasone treatment whereas sub-mucosal
mast cells were unaffected by treatment. This anti-in¯am-
matory effect of ¯uticasone propionate was paralleled by
signi®cant reductions in nasal symptoms.
Our study has shown that nasal brushing is a useful
alternative to nasal biopsy for sampling the nasal epithe-
lium. Eosinophil and mast cell numbers within the brush-
ings were low but compared favourably with those obtained
by other groups [6,18]. The counting technique used
ensured unbiased counts in which small but highly signi®-
cant changes in cell numbers could be detected. Within the
placebo group the change in eosinophil numbers (peak
season minus preseason) measured using cell counts from
1352 M. R. Jacobson et al.
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355
0.075
0.05
0.025
0
%T
ryp
tase
po
siti
ve c
ells
/cyt
osp
in
(a)
(b)
Mast cellsPlacebo Fluticasone
P < 0.00001
(0.34)
(0.16)
100
120
140
80
60
40
20
0
Try
pta
se p
osi
tive
cel
ls/m
m2
epit
hel
ium
P < 0.01
(171.6)
Pre Peak Pre PeakFig. 4. Tryptase-positive mast cells in (a) nasal brushings and (b)
nasal epithelium of grass pollen-sensitive rhinitics prepollen
season and peak pollen season following 6 weeks' treatment with
¯uticasone propionate (closed circles) or placebo (open circles).
Median values are represented by the horizontal bars. Median
differences were compared using the Mann Whitney U-test.
220200
120100
80604020
0
∆ B
MK
13 c
ells
/m
m2
epit
hel
ium
∆ % BMK 13 cells/cytospin
(a)
10 150 5
r = 0.444P < 0.05n = 21
200150100
500
−50−100
∆ M
ast
cell
s/m
m2
epit
hel
ium
∆ % Mast cells/cytospin
(b)
0.25 0.30 0.350 0.05 0.10 0.200.15
r = 0.5P < 0.05n = 19(4)
Fig. 5. Comparison of changes in the number of (a) BMK13-
positive eosinophils and (b) tryptase-positive mast cells recorded
in nasal brushings and the nasal epithelium (peak season cell count
minus preseason cell count). Spearman's rank correlation was
performed.
brush specimens correlated with those obtained from biopsy
sections as did changes in mast cell numbers. Both tech-
niques demonstrated clearly the effectiveness of ¯uticasone
propionate in inhibiting epithelial in®ltration of eosinophils
and mast cells. Nasal brushing is a simple technique which
does not require anaesthetic, it has the advantage of being
more economical than nasal biopsy both in terms of time
and money. Nasal brush specimens require less processing
prior to staining than biopsies but do take longer to assess
under the microscope. Nasal brushing like nasal scraping
(another minimally invasive nasal epithelial sampling tech-
nique) would be particularly well-suited to studies looking
at the effect of treatment on in¯ammatory cells within the
epithelium or on epithelial cells themselves especially
studies involving large numbers of patients or studies
involving children.
The in®ltration of eosinophils into the nasal mucosa
following natural or laboratory allergen exposure is well
known [1,19,20]. Products from eosinophils such as leuco-
triene C4, platelet-activating factor and eosinophil granule
proteins may account for the prolonged nasal congestion
and mucus secretion observed during natural seasonal
exposure to pollen. Fluticasone propionate has been
shown to inhibit production of chemokines [21] and cyto-
kines [2,22] which may contribute to the inhibition of
eosinophil in®ltration and as a result the improvement of
symptoms observed in this study. The effect of glucocorti-
costeroids on eosinophilia in the nasal epithelium and sub-
mucosa is varied. In an allergen challenge study we have
shown that 6 weeks' pretreatment with ¯uticasone pro-
pionate results in a signi®cant reduction in activated
(EG2�) eosinophils in both the epithelium and the sub-
mucosa whereas total (BMK13) eosinophils were only
reduced in the epithelium [23]. This data supported the
®ndings of Lozewicz and colleagues [24] who investigated
the effect of a 2-week pretreatment with ¯uticasone pro-
pionate on eosinophils in the sub-mucosa of nasal biopsies
24 h postallergen challenge. Their data showed a reduction
in the number of EG2� eosinophils but no change in total
(EG1�) numbers. In contrast, 24 h postallergen challenge
Baroody et al. [25] found that although total eosinophils
(Wright stain) in nasal scrapings were reduced, neither total
(Giemsa stain) nor EG2� eosinophils in the nasal sub-
mucosa were affected following 1 week's treatment with
Topical corticosteroid use in rhinitis 1353
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355
Fig. 6. Effect of ¯uticasone propionate on the number of BMK13-positive eosinophils and tryptase-positive mast cells. Data are shown for
preseason and peak season following 6 weeks' treatment with ¯uticasone propionate (closed circles) and placebo (open circles). Horizontal
bars represent median values. The Mann Whitney U-test was used to compare median differences.

beclomethasone propionate. In a natural allergen exposure
study Bradding et al. [2] found that 6 weeks' treatment with
once-daily ¯uticasone propionate resulted in inhibition of
seasonal increases in activated (EG2�) eosinophils. We
con®rmed this ®nding following 6 weeks' treatment with
twice-daily ¯uticasone propionate [3]. In this current study
we observed dramatic inhibition of both epithelial and sub-
mucosal BMK13 eosinophils demonstrating that intranasal
steroids can be highly effective in in¯ammatory cell reduc-
tion both in the super®cial and deeper compartments of the
nasal mucosa.
Mast cells are found constitutively in the nasal sub-
mucosa but are not generally found in the nasal epithelium
outside of the pollen season [1,2,23,26,27]. The seasonal
increase in epithelial mast cells is well documented
[1,2,26,27]. These cells are known to be in an activated
state as shown by degranulation evident by electron micro-
scopy [28] and increased levels of the mast cell mediators
histamine and tryptase in nasal lavage ¯uid [29]. Mast cell
degranulation results in histamine, tryptase, prostaglandin
(PG)D2, PGF2 and bradykinin release with the subsequent
induction of nasal symptoms of sneezing, nasal discharge
and transient nasal blockage. Mast cell degranulation con-
tributes to the eosinophilic mucosal in¯ammation seen in
rhinitis since mast cells contain preformed pro-eosinophilic
cytokines and mRNA for IL-4, IL-5, IL-6 and TNF-a [2,30].
As seen in our current and previous studies [1,26] sub-
mucosal mast cell numbers do not change during the pollen
season. The epithelial increase in mast cells is thought to
result from redistribution of mast cells [26,31]. Mast cell
proliferation may also contribute to the number of mast cells
in the nasal epithelium and subepithelial layer of allergic
patients [32]. Since glucocorticosteroids do not prevent
mast cell degranulation [33,34] the improvement in symp-
toms observed in this study must result in part from the
inhibition of mast cell occupation of the nasal epithelium. In
vitro and in vivo evidence suggests that glucocorticoids
decrease tissue mast cell numbers by downregulating
tissue stem cell factor production which is required for the
survival of local mast cells [35,36].
Seasonal grass pollen-induced rhinitis is characterized by
epithelial in®ltration of eosinophils and mast cells, and since
topical corticosteroids have a marked effect on the in¯am-
matory cells of the nasal epithelium nasal brushing is an
appropriate cell-harvesting method to use in studies looking
at treatment effects. The nasal biopsy technique allows more
detailed studies of the nasal mucosa.
Acknowledgements
This study was supported by grants from the Medical
Research Council, UK and ®nancial assistance from Glaxo
Wellcome, UK.
References
1 Bentley AM, Jacobson MR, Cumberworth V et al. Immuno-
histology of the nasal mucosa in seasonal allergic rhinitis:
increases in activated eosinophils and epithelial mast cells. J
Allergy Clin Immunol 1992; 89:877±83.
2 Bradding P , Feather IH , Wilson S , Holgate ST , Howarth PH.
Cytokine immunoreactivity in seasonal rhinitis: regulation by a
topical corticosteroid. Am J Respir Crit Care Med 1995;
151:1900±6.
3 Masuyama K , Till SJ , Jacobson MR et al. Nasal eosinophilia and
IL-5 mRNA expression in seasonal allergic rhinitis: effect of
topical corticosteroids. J Allergy Clin Immunol 1998; 102:610±7.
4 Pipkorn U , Karlsson G. Methods for obtaining specimens from
the nasal mucosa for morphological and biochemical analysis.
Eur Respir J 1988; 1:856±62.
5 Pipkorn U , Karlsson G , Enerback L. A brush method to
harvest cells from the nasal mucosa for microscopic and
biochemical analysis. J Immunol Methods 1988; 112:37±42.
6 Godthelp T , Holm AF , Fokkens WJ et al. Dynamics of nasal
eosinophils in response to a nonnatural allergen challenge in
patients with allergic rhinitis and control subjects: a biopsy and
brush study. J Allergy Clin Immunol 1996; 97:800±11.
7 Chapelin C , Coste A, Reinert P et al. Incidence of primary
ciliary dyskinesia in children with recurrent respiratory dis-
eases. Ann Otol Rhinol Laryngol 1997; 106:854±8.
8 Gilain L, Escudier E, Chapelin C, Boucherat M, Faulcon V,
Peynegre R. Brush technique in cytological analysis of the
nasal mucosa. A critical and comparative analysis. Ann Oto-
laryngol Chir Cervicofac 1992; 109:397±401.
9 Gilain L, Chapelin C, Boucherat M, Peynegre R, Escudier E.
Evaluation of the brushing technique in nasal cytology. Bull
Assoc Anat (Nancy) 1994; 78:5±8.
10 Fokkens WJ, Vroom TM, Gerritsma V, Rijntjes E. A biopsy
method to obtain high quality specimens of nasal mucosa.
Rhinology 1988; 26:293±5.
11 Meltzer EO, Orgel HA, Rogenes PR, Field EA. Nasal cytology
in patients with allergic rhinitis: effects of intranasal ¯utica-
sone propionate. J Allergy Clin Immunol 1994; 94:708±15.
12 Mygind N, Dahl R. The rationale for use of topical corticoster-
oids in allergic rhinitis. Clin Exp Allergy 1996; 26 (Suppl.
3):2±10.
13 Mygind N. Glucocorticosteroids and rhinitis. Allergy 1993;
48:476±90.
14 Gomez E, Clague JE, Gatland D, Davies RJ. Effect of topical
corticosteroids on seasonally induced increases in mast cells.
Br Med J 1988; 296:1572±3.
15 Bascom R, Wachs M, Naclerio RM, Pipkorn U, Galli SJ,
Lichtenstein LM. Basophil in¯ux occurs after nasal antigen
challenge: effect of topical corticosteroid pretreatment. J
Allergy Clin Immunol 1988; 81:580±9.
16 Howland WC, Hampel FCJ, Martin BG, van Ratner PHBJ,
Field EA. The ef®cacy of ¯uticasone propionate aqueous nasal
spray for allergic rhinitis and its relationship to topical effects.
Clin Ther 1996; 18:1106±17.
17 Wiseman LR, Ben®eld P. Intranasal ¯uticasone propionate. A
reappraisal of its pharmacology and clinical ef®cacy in the
treatment of rhinitis. Drugs 1997; 53:885±907.
1354 M. R. Jacobson et al.
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355

18 Nonaka M, Nonaka R, Jordana M, Dolovich J. GM-CSF, IL-8,
IL-1R, TNF-alpha R, and HLA-DR in nasal epithelial cells in
allergic rhinitis. Am J Respir Crit Care Med 1996; 153:1675±
81.
19 Pipkorn U, Karlsson G, Enerback L. The cellular response of
the human allergic mucosa to natural allergen exposure. J
Allergy Clin Immunol 1988; 82:1046±54.
20 Varney VA, Jacobson MR, Sudderick RM et al. Immuno-
histology of the nasal mucosa following allergen-induced
rhinitis. Identi®cation of activated T lymphocytes, eosino-
phils, and neutrophils. Am Rev Respir Dis 1992; 146:170±
6.
21 Weido AJ, Reece LM, Alam R, Cook CK, Sim TC. Intranasal
¯uticasone propionate inhibits recovery of chemokines and
other cytokines in nasal secretions in allergen-induced rhinitis.
Ann Allergy Asthma Immunol 1996; 77:407±15.
22 Masuyama K, Jacobson MR, Rak S et al. Topical glucocorti-
costeroid (¯uticasone propionate) inhibits cells expressing
cytokine mRNA for interleukin-4 in the nasal mucosa in
allergen-induced rhinitis. Immunology 1994; 82:192±9.
23 Rak S, Jacobson MR, Sudderick RM et al. In¯uence of
prolonged treatment with topical corticosteroid (¯uticasone
propionate) on early and late phase nasal responses and cellular
in®ltration in the nasal mucosa after allergen challenge. Clin
Exp Allergy 1994; 24:930±9.
24 Lozewicz S, Wang J, Duddle J et al. Topical glucocorticoids
inhibit activation bt allergen in the upper respiratory tract. J
Allergy Clin Immunol 1992; 89:951±7.
25 Baroody FM, Rouadi P, Driscoll PV, Bochner BS, Naclerio
RM. Intranasal beclomethasone reduces allergen-induced
symptoms and super®cial mucosal eosinophilia without affect-
ing submucosal in¯ammation. Am J Respir Crit Care Med
1998; 157:899±906.
26 Enerback L, Pipkorn U, Granerus G. Intraepithelial migration
of nasal mucosal mast cells in hay fever. Int Arch Allergy Appl
Immunol 1986; 80:44±51.
27 Viegas M, Gomez E, Brooks J, Gatland D, Davies RJ. Effect of
the pollen season on nasal mast cells. Br Med J Clin Res Ed
1987; 294:414.
28 Trotter CM, Orr TS. A ®ne structure study of some cellular
components in allergic reactions. 1. Degranulation of human
mast cells in allergic asthma and perennial rhinitis. Clin
Allergy 1973; 3:411±25.
29 Rasp G, Hochstrasser K. Tryptase in nasal ¯uid is a useful
marker of allergic rhinitis. Allergy 1993; 48:72±4.
30 Ying S, Durham SR, Jacobson MR et al. T lymphocytes and
mast cells express messenger RNA for interleukin-4 in the
nasal mucosa in allergen-induced rhinitis. Immunology 1994;
82:200±6.
31 Enerback L, Pipkorn U, Olofsson A. Intraepithelial migration
of mucosal mast cells in hay fever: ultrastructural observations.
Int Arch Allergy Appl Immunol 1986; 81:289±97.
32 Kawabori S, Kanai N, Tosho T. Proliferative activity of mast
cells in allergic nasal mucosa. Clin Exp Allergy 1995; 25:173±
8.
33 Schleimer RP, Schulman ES, MacGlashan DWJ et al. Effects
of dexamethasone on mediator release from human lung
fragments and puri®ed human lung mast cells. J Clin Invest
1983; 71:1830±5.
34 Cohan VL, Undem BJ, Fox CC, Adkinson NFJ, Lichtenstein
LM, Schleimer RP. Dexamethasone does not inhibit the release
of mediators from human mast cells residing in airway, intes-
tine, or skin. Am Rev Respir Dis 1989; 140:951±4.
35 Finotto S, Mekori YA, Metcalfe DD. Glucocorticoids decrease
tissue mast cell number by reducing the production of the c-kit
ligand, stem cell factor, by resident cells: in vitro and in vivo
evidence in murine systems. J Clin Invest 1997; 99:1721±8.
36 Kim YK, Nakagawa N, Nakano K, Sulakvelidze I, Dolovich J,
Denburg J. Stem cell factor in nasal polyposis and allergic
rhinitis: increased expression by structural cells is suppressed
by in vivo topical corticosteroids. J Allergy Clin Immunol
1997; 100:389±399.
Topical corticosteroid use in rhinitis 1355
q 1999 Blackwell Science Ltd, Clinical and Experimental Allergy, 29, 1347±1355



![Diagnosis and Management of Rhinitis: Complete Guidelines ... · different forms of rhinitis (allergic, non-allergic, occupational rhinitis, hormonal rhinitis [pregnancy and hypothyroidism],](https://static.fdocuments.us/doc/165x107/5d61f07588c993197b8b51b8/diagnosis-and-management-of-rhinitis-complete-guidelines-different-forms.jpg)