Effect of Sample Quality on Newborn Screening Results and ...
26
Roanna George Principal Clinical Scientist Welsh Public Health Conference November 2015 Wales Newborn Screening Laboratory, University Hospital of Wales Effect of Sample Quality on Newborn Screening Results and Quality Improvement Implementation
Transcript of Effect of Sample Quality on Newborn Screening Results and ...
Roanna George
Principal Clinical Scientist
Welsh Public Health Conference
November 2015
Wales Newborn Screening Laboratory, University Hospital of Wales
Effect of Sample Quality on Newborn
Screening Results and
Quality Improvement Implementation

Newborn bloodspot screening in
Wales Aims to prevent serious but rare conditions through early
treatment before symptoms develop
~36,500 babies screened per year
Testing for: Six inherited metabolic disorders:
Phenylketonuria (PKU)
Medium chain Acyl-CoA dehydrogenase deficiency (MCADD)
Maple Syrup Urine Disease (MSUD)
Isovaleric Acidaemia (IVA)
Glutaric Aciduria Type 1 (GA1)
Homocystinuria (HCU)
Congenital hypothyroidism (CHT)
Cystic fibrosis (CF)
Sickle cell disorders (SCD)
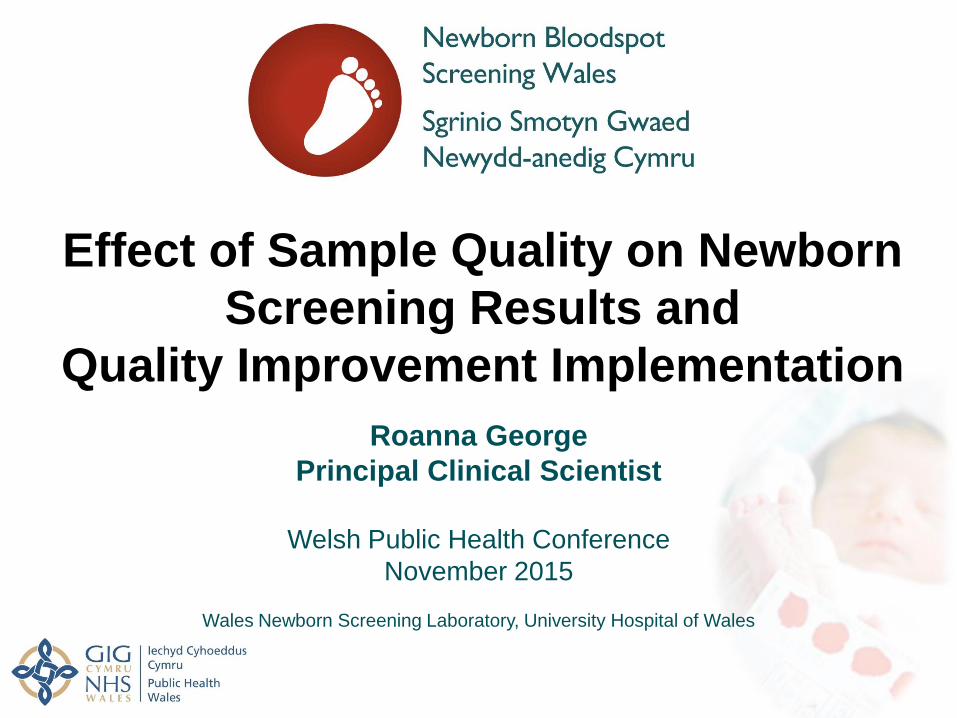
Newborn Bloodspot Screening
• UK newborn screening using bloodspot
samples
• Taken on day 5-8 (including premature or ill
babies)

Sample Quality Guidelines

Does Sample Quality Matter?
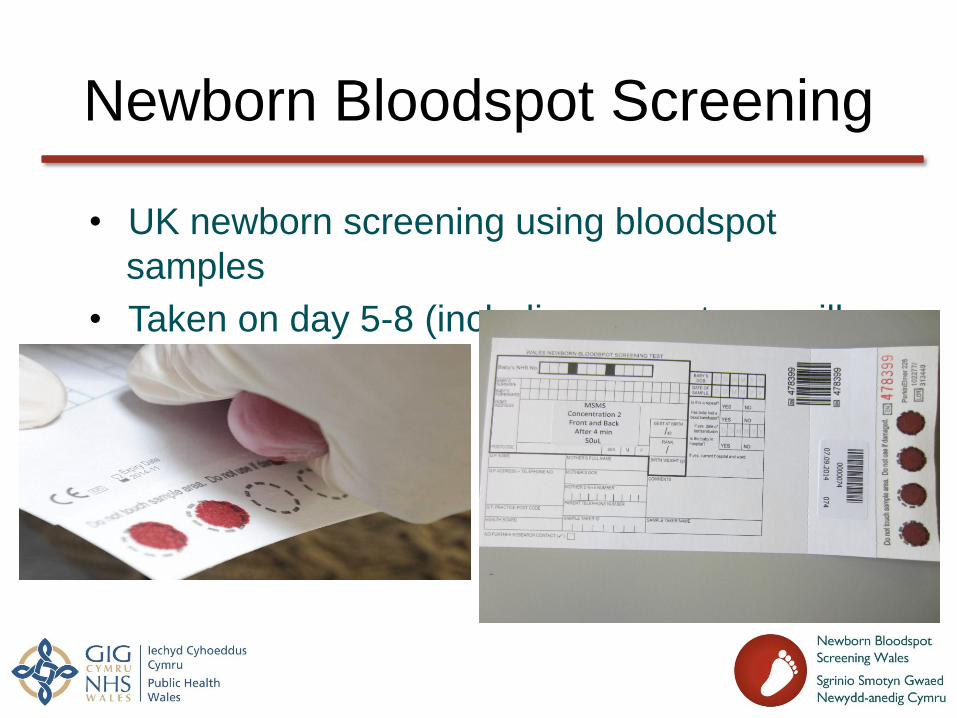
Bloodspot Quality Project
• Aim: • Determine whether bloodspot quality effects screening results
• Methods: • Create whole blood pools at screening cut-off concentrations
• Create cards of different sample quality to compare the results
• Different sample volumes
• Double layered spots
• Samples spotted on the front and back of the card
• Multi-spotted samples
• Insufficient samples
• Compressed samples
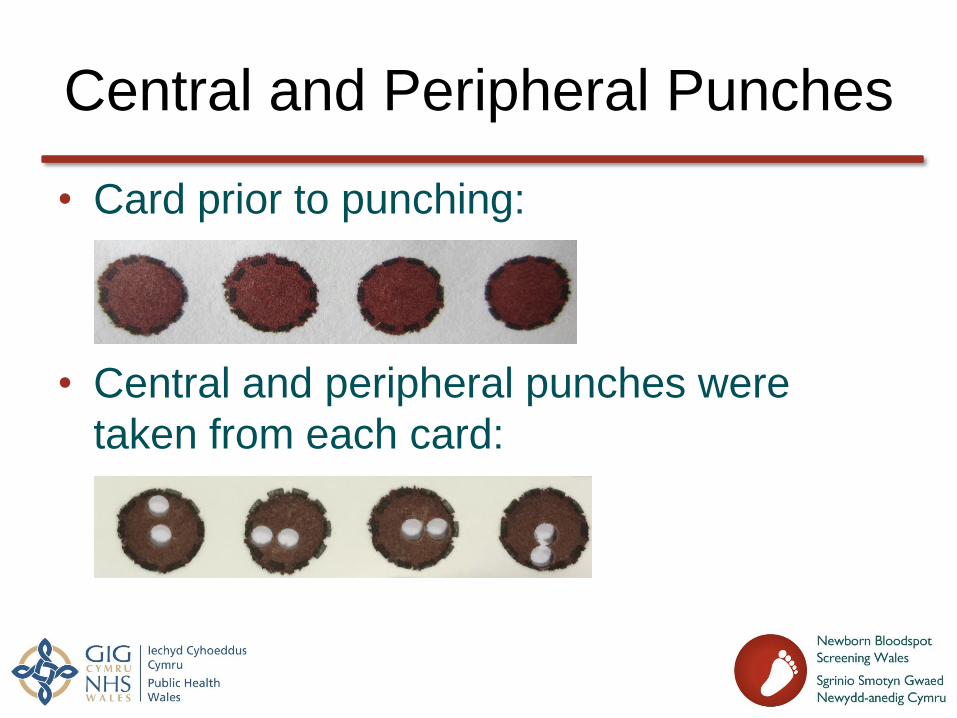
Central and Peripheral Punches
• Card prior to punching:
• Central and peripheral punches were
taken from each card:
Volume Experiments
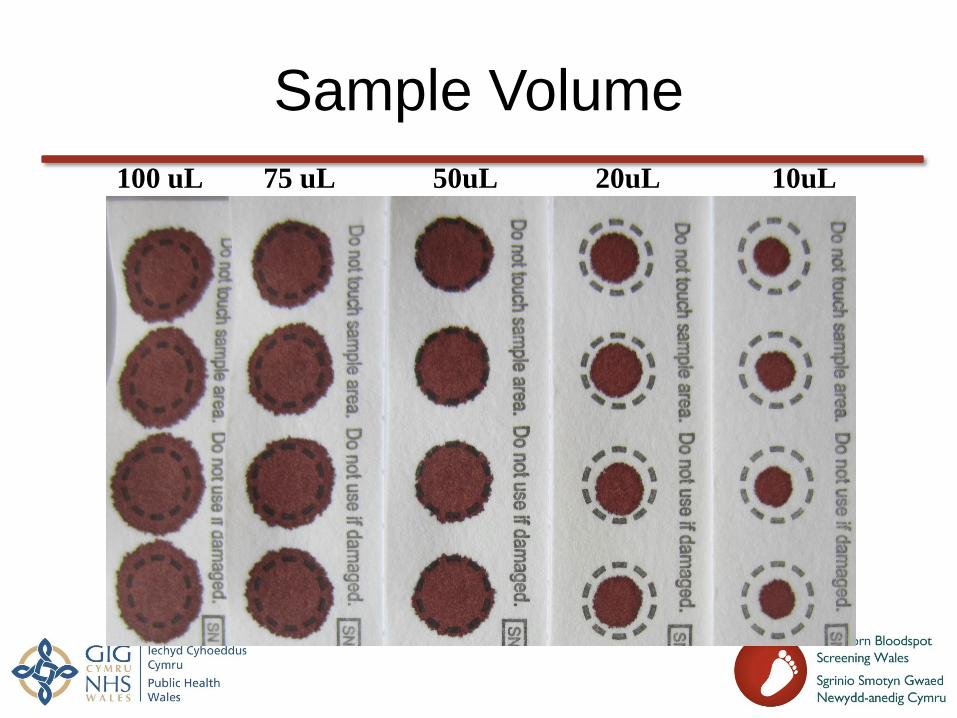
Sample Volume
100 uL 75 uL 50uL 20uL 10uL
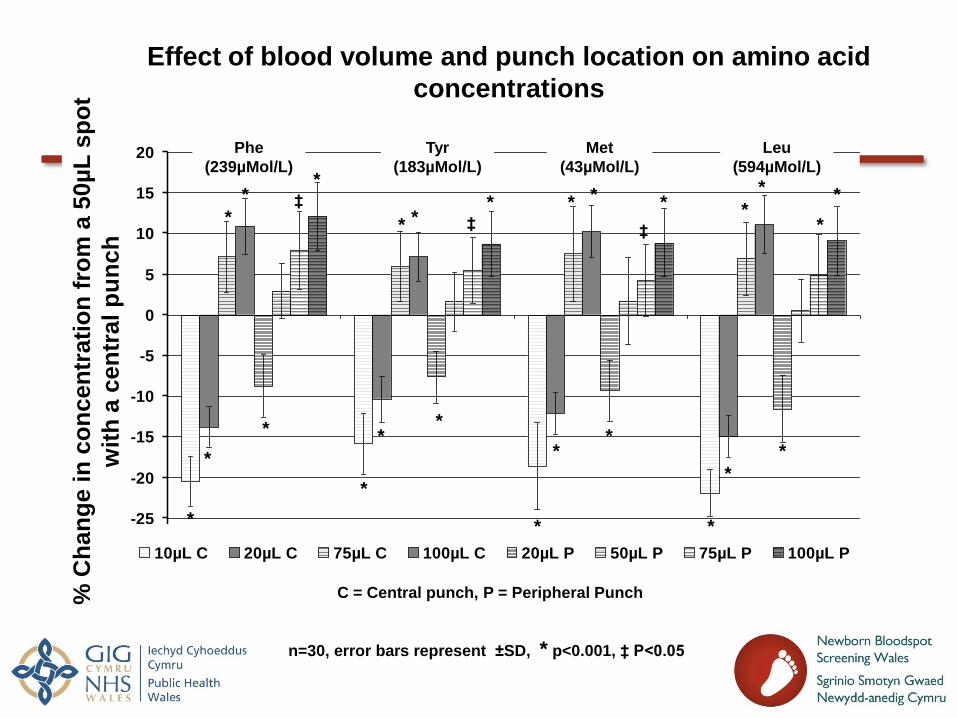
Effect of blood volume and punch location on amino acid
concentrations
-30
-25
-20
-15
-10
-5
0
5
10
15
20
10µL C 20µL C 75µL C 100µL C 20µL P 50µL P 75µL P 100µL P
Phe
(239µMol/L)
Tyr
(183µMol/L)
Met
(43µMol/L)
Leu
(594µMol/L)
n=30, error bars represent ±SD, * p<0.001, ‡ P<0.05
*
‡ *
*
*
*
*
*
* *
*
* *
*
*
*
% C
han
ge in
co
ncen
trati
on
fro
m a
50µ
L s
po
t
wit
h a
cen
tral p
un
ch
* *
*
* *
* * *
* * ‡ ‡
C = Central punch, P = Peripheral Punch

Poor Quality Experiments
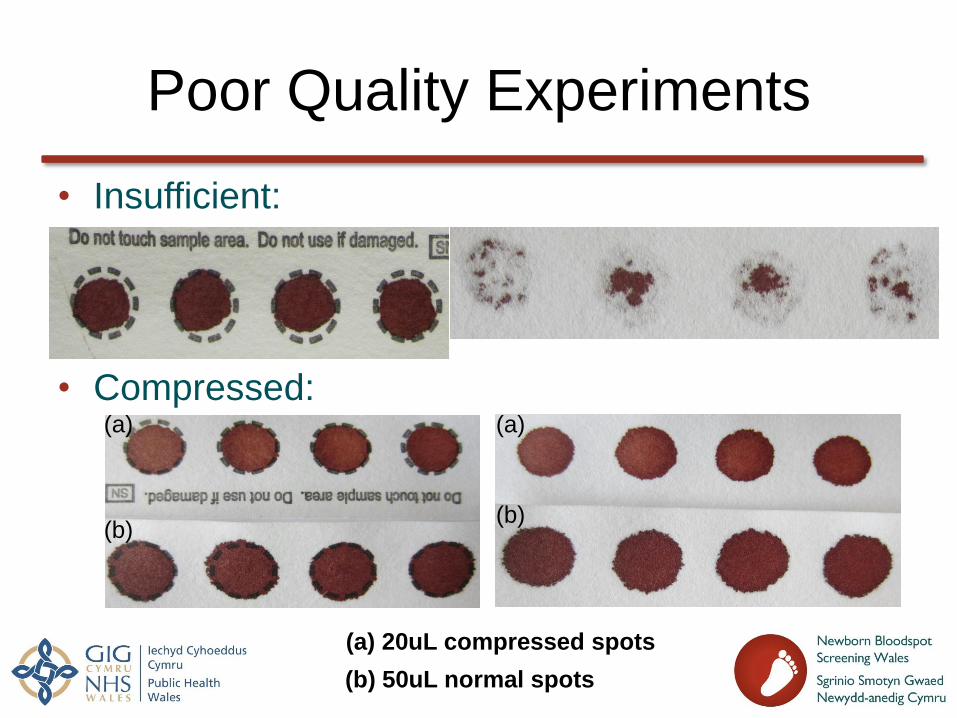
Poor Quality Experiments
• Insufficient:
• Compressed:
(b) 50uL normal spots
(a) 20uL compressed spots
(a) (a)
(b) (b)
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
5
10
15
Insuff C Comp C 20µl P Insuff P Comp P
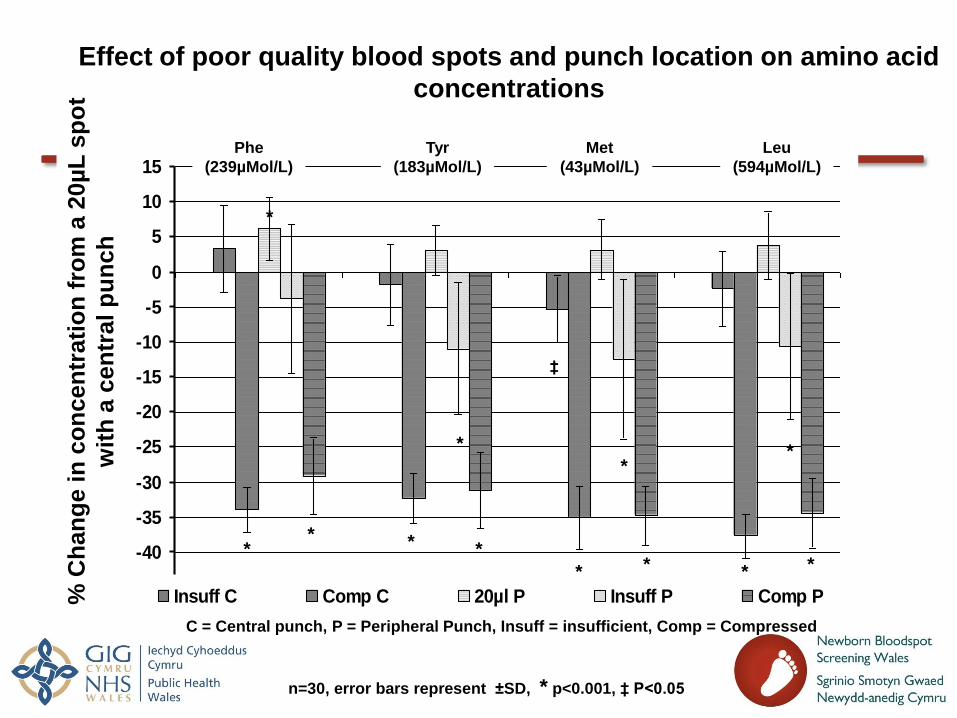
Effect of poor quality blood spots and punch location on amino acid
concentrations
Phe
(239µMol/L)
Tyr
(183µMol/L)
Met
(43µMol/L)
Leu
(594µMol/L)
n=30, error bars represent ±SD, * p<0.001, ‡ P<0.05
*
*
* * *
* *
*
* *
*
% C
han
ge in
co
ncen
trati
on
fro
m a
20µ
L s
po
t
wit
h a
cen
tral p
un
ch
*
‡
C = Central punch, P = Peripheral Punch, Insuff = insufficient, Comp = Compressed
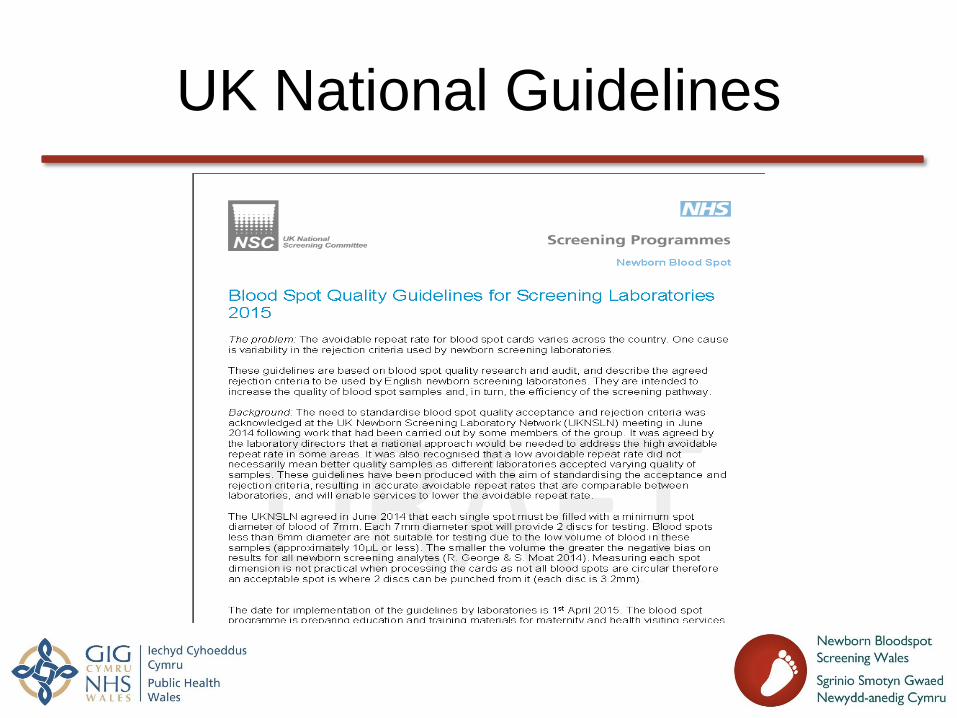
UK National Guidelines
UK National Guidelines
• 4 filled circles
• Can accept over-spotted samples
• Risk of false positive but a case will not be missed
• Must reject:
• Insufficient and multi-spotted samples
• Heterogeneous results and risk of false negative
• Compressed and small volume samples:
• SIGNIFICANT RISK OF NEGATIVE BIAS
• A DISORDER MAY BE MISSED

Case Study
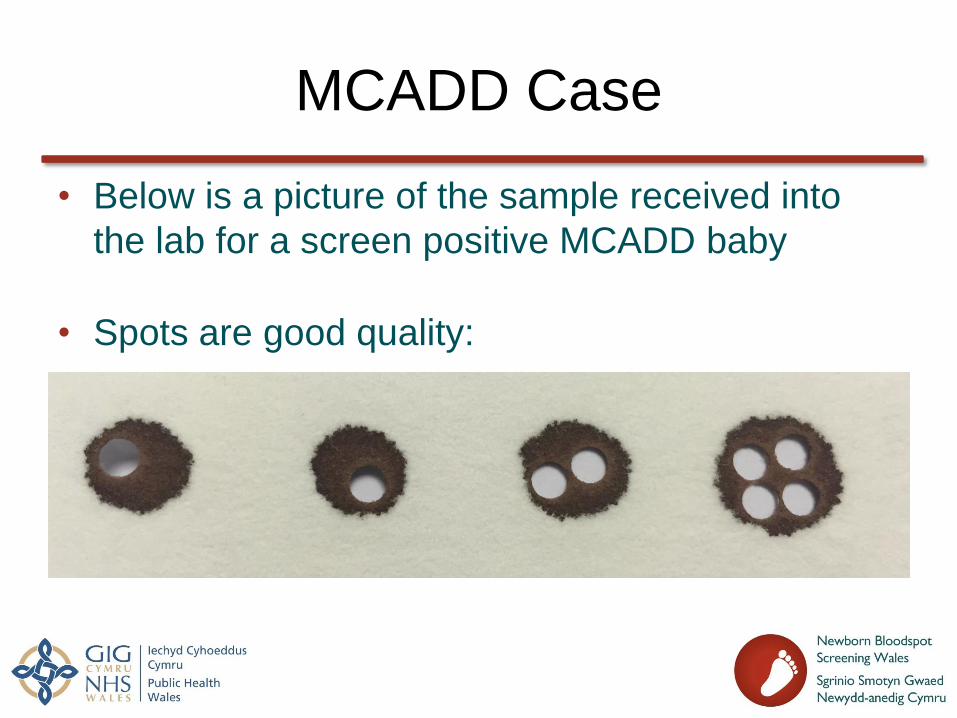
MCADD Case
• Below is a picture of the sample received into
the lab for a screen positive MCADD baby
• Spots are good quality:
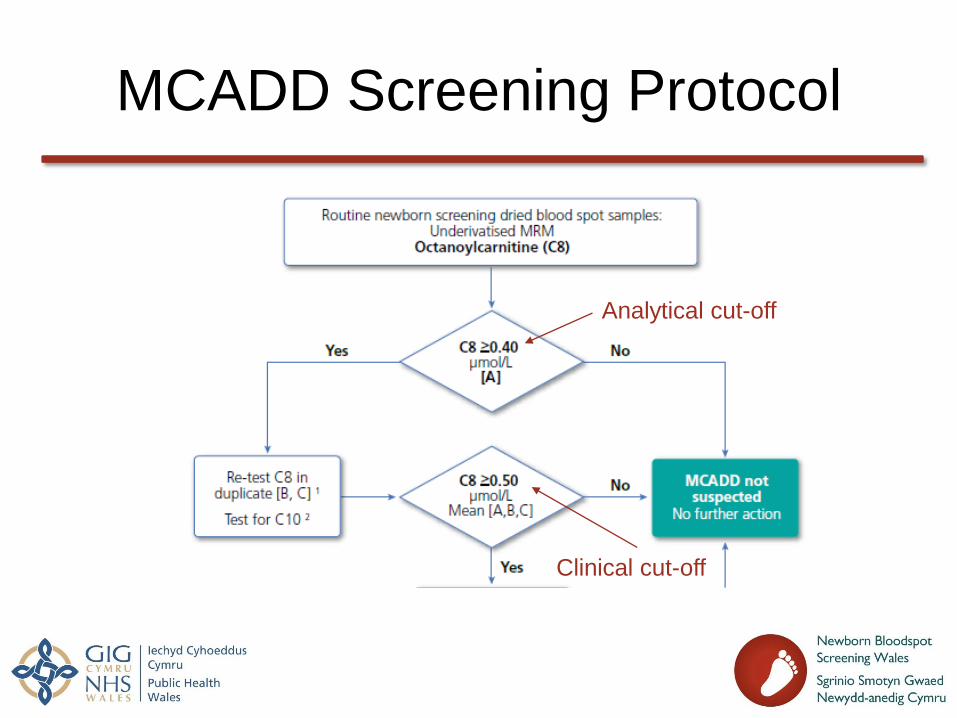
MCADD Screening Protocol
Analytical cut-off
Clinical cut-off
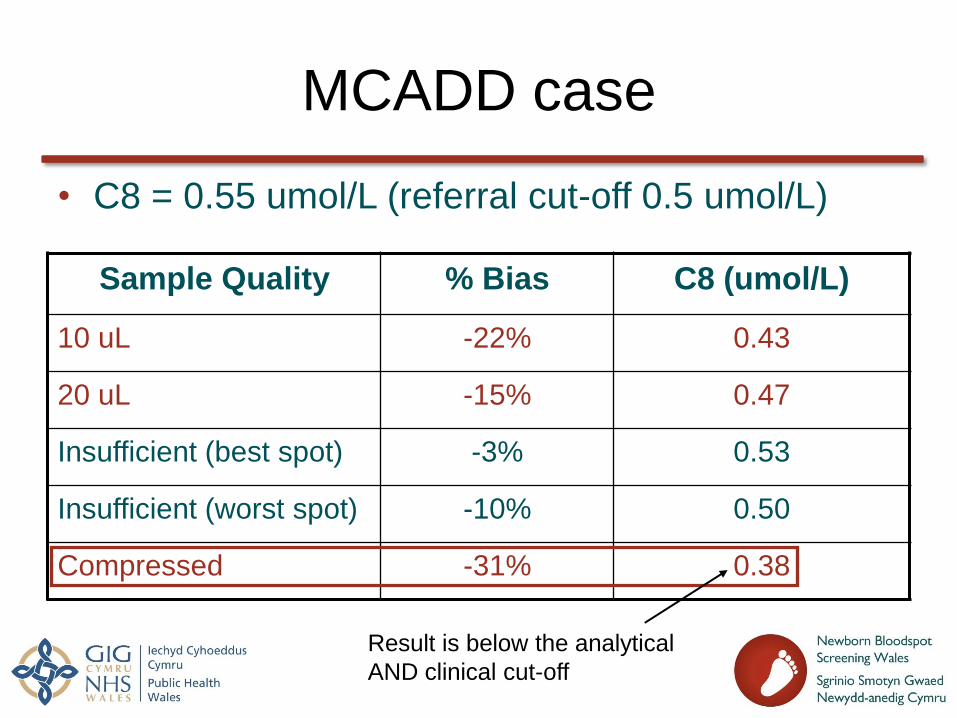
MCADD case
• C8 = 0.55 umol/L (referral cut-off 0.5 umol/L)
Sample Quality % Bias C8 (umol/L)
10 uL -22% 0.43
20 uL -15% 0.47
Insufficient (best spot) -3% 0.53
Insufficient (worst spot) -10% 0.50
Compressed -31% 0.38
Result is below the analytical
AND clinical cut-off

Quality Improvement Strategy

Quality Improvement Strategy
• Set up Poor Quality 1 (PQ1) and Poor Quality 2 (PQ2) categories • PQ2 to act as a warning that sample quality is poor without rejecting
samples
• Monthly feedback to governance leads with sample taker names
• Laboratory introduced step-wise increase in sample rejection
• Training and education, resources include: • Talk on why bloodspot quality matters at midwife training days
• Interactive newborn screening card
• Bloodspot sampling video
• Midwife video
• Lancet audit • Cost of lancets vs cost of re-bleeding babies
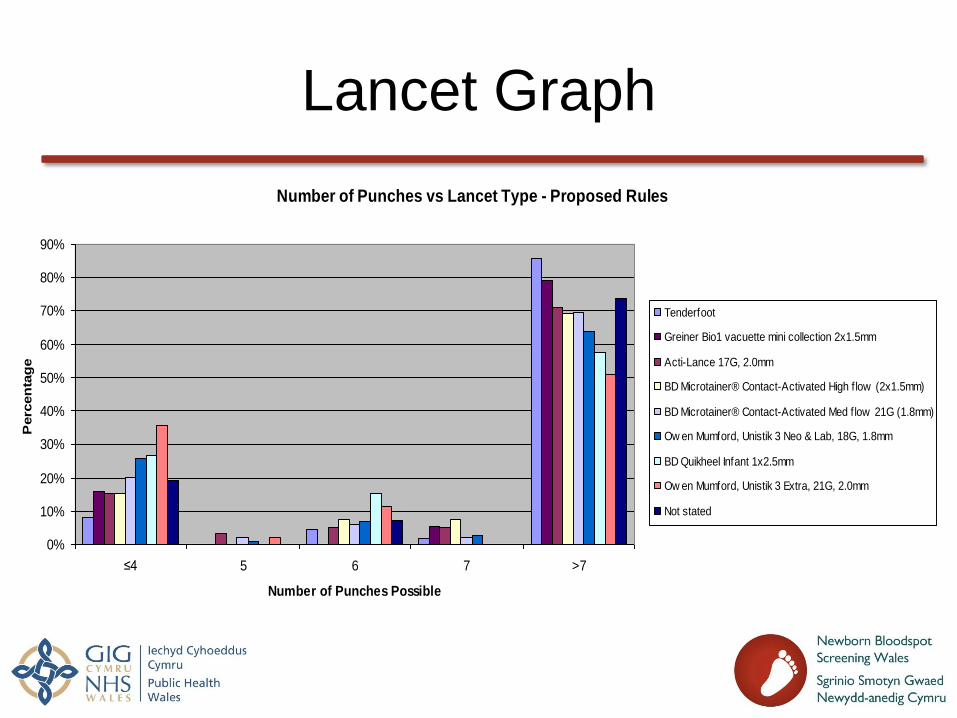
Lancet Graph
Number of Punches vs Lancet Type - Proposed Rules
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
≤4 5 6 7 >7
Number of Punches Possible
Perc
en
tag
e
Tenderfoot
Greiner Bio1 vacuette mini collection 2x1.5mm
Acti-Lance 17G, 2.0mm
BD Microtainer® Contact-Activated High f low (2x1.5mm)
BD Microtainer® Contact-Activated Med flow 21G (1.8mm)
Ow en Mumford, Unistik 3 Neo & Lab, 18G, 1.8mm
BD Quikheel Infant 1x2.5mm
Ow en Mumford, Unistik 3 Extra, 21G, 2.0mm
Not stated
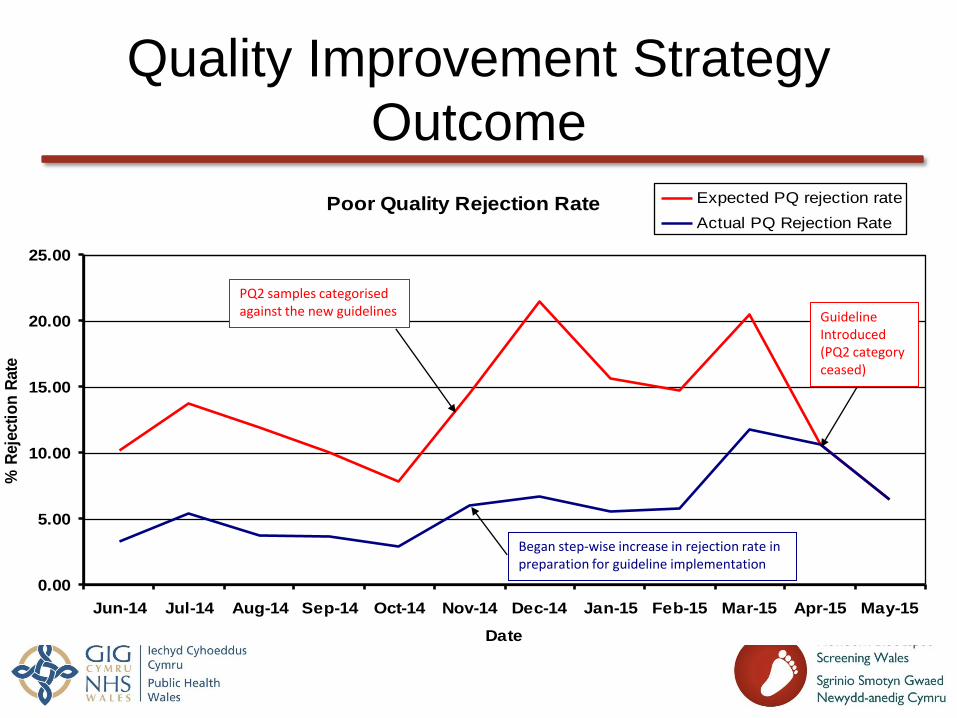
Quality Improvement Strategy
Outcome
Poor Quality Rejection Rate
0.00
5.00
10.00
15.00
20.00
25.00
Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15
Date
% R
eje
cti
on
Rate
Expected PQ rejection rate
Actual PQ Rejection Rate
PQ2 samples categorised against the new guidelines Guideline
Introduced (PQ2 category ceased)
Began step-wise increase in rejection rate in preparation for guideline implementation
Sample Quality
• Sample quality important to:
• Avoid false positives
• Avoid false negatives
• Prevent delay in referral if
repeat samples are required
• Prevent re-bleeding a baby
• Prevent wasting healthcare resources
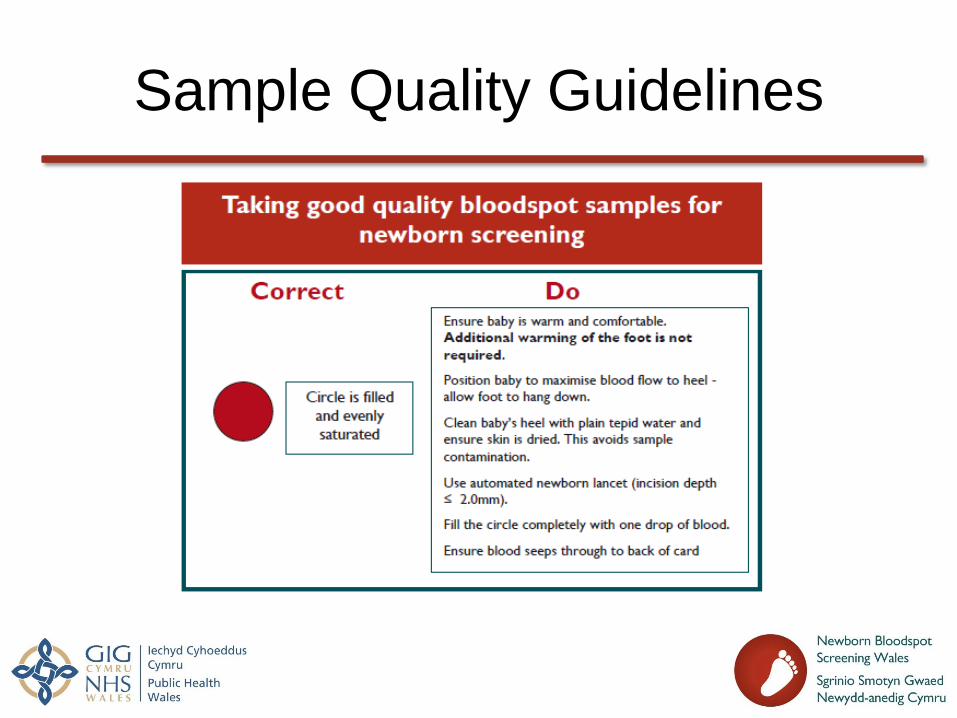
Sample Quality Guidelines
Summary
• Small volume and compressed samples give significant risk of negative bias
• Improvement of sample quality achieved by stakeholder engagement and education and training
• Improvement in bloodspot quality has increased efficiency and prevented: • Wasting healthcare resources
• Harm and anxiety to the baby and parents
• Implementation of bloodspot quality guidelines imperative to ensure accurate screening results and correct outcomes