Effect of omega-3 fatty.acids canine atopic dermatitis · 2017. 11. 1. · Effect of omega-3...
5
Effect of omega-3 fatty.acids on canine atopic dermatitis Twenty-nlne dogs were lncluded ln a double-bllnded, placebo+ontrolled, randomlsed trlal and were orally suppfemented for 10 weeks wlth elther flax oll (2OO mg/kg/dayl, elcosapentaenolc acld (5O mg/RC/day) and docosahexaenolc acld (35 mg/Rg/day) ln a commerclal preparatlon, or mlneral oll as a placebo. For each dog, cllnlcal scores were determlned based on a scorlng system developed prlor to the trlal. Total omegao and omega3 lntake and the ratlo of omega6:omega-3 (omega-6:3) were calculated before and after the trlal. The dogs' cllnlcal scores lmproved ln those supplemented wlth flax oll and the commerclal preparatlon, but not ln the placebo group. No correlatlon was ldentlfled between total fatty acld lntake or omega6:3 ratlo and cllnlcal scores. Based on the results of thls study, the total lntake of fatty aclds or the omega€:3 ratlo do not seem to be the maln factors ln determlnlng the cllnlcal response. R. S. Mueu-en, K. V. FrEsEr-ER*, M. J. FEnu¡N, S. Z¡sEl*, R. A. W RosvcHur, G. K, Ocrr-vrE ¡r.¡o T. L. GREe¡¡wnLr* Journal of Small An¡mal Pract¡ce (2OO4) 45,293-297 Department of Clin¡cal Sc¡ences, and x Department of veter¡nary Teach¡ng Hospital, College of Veterinary Medicine and B¡omedical Sciences, Colorado State Un¡versltf Fort Colllns, CO 80523, USA R. Mueller's current address is Medizinische Tierkl¡nik, Veter¡naerstr. 13, 80539 Munich, Germany G. Og¡lvie's current address is CVS Angel Care Cancer Center, 100 N Rancho Santa Fe, San Marcos, cA 92024, USA IIIRODUGnOil Canine atopic dermatitis is a common skin disease in small animal practice (Scott and Paradis 1990). h is defined as an inherent predisposition to the development of immunoglobulin (lg) E antibodies to envi- ronmental allergens, resulting in clinical signs following exposure to these allergens (Halliwell and Gorman 1989). Sympto- maric trearment modalities for canine atopic dermatiris inclucle glucocorticoids, anrihistamines and fatry acid supplemen- tation (Griffin 1993, Mueller 1993, Scott and orhers 2001). The only specific treat- ment for atopic dermatitis is allergen- specific immunotherapy wherein allergens identified by intradermal testing or serum resring for allergen-specific IgE are injected subcutaneously. Allergen-specific immu- notherapy must usually be pursued For months before an improvement in clinical signs is seen and it is not effective in all patients (Scotr and others 1993, Mueller and Bettenay 1996). For these reasons, symptomatic therapies are often explored. Because adverse reacrions to glucocorticoid therapy are common, more attention has been paid recenrly to treatments that have been associated with fewer adverse effects, such as antihistamines and fatty acid sup- plementation (Campbell 1993, Paterson 1994). Bsenrial fatry acids have been used to treat humans with atopic dermatitis (Price 1984, Biagi and others 1988, Fiocchi and others 1994, Paterson 1995, Henz and orhers 1999) and allergic asthma (Stenius- Aarniala and others 1989, Okamoto and others 2000), and have been shown to modulate the infìammatory response in humans, mice and rats (Higgs 1985, Horii and others 1991, Schafer and Kragealle 1991, Vatanabe and others 1994, Teren- cio and others 1998). Oral fatry acid sup- plementation has been noted to decrease rhe inflammation and pruritus associated with canine atopy (Bond and Lloyd I 992b, Scort and others 1992, Logas and Kunkle 1994). These benefits have been related to supplementation with certain omega-6 fatty acids (gamma-linoleic acid [GLA]) (Scarffand Lloyd 1992), combinations of GLA and omega-3 fatty acids such as eicosapentaenoic acid (EPA) and docosa- hexaenoic acid (DHA) (Bond and Lloyd 1992a, Scott and others 1992), variable doses of omega-3 fatry acids (Logas and Kunkle 1994) or omega-3 supplemented whole diets with fixed omega-6:omega-3 (omega-6:3) ratios (Scott and others 1997). Emphasi.s has recently been placed on the use of omega-3 latty acid sup- plementation at doses higher than the manufacturer's recommendation in the management of canine atopic dermatitis. Combination supplements of EPA and DHA given in the range of 66 mglkglday have been noted ¡o clinically benefit pruritic dogs (Logas and Kunkle 1994). The use of flax oil as a source of potentially beneficial omega-3 fatty acids has also been recommended.'Io che authors' knowledge, there are no published data in the veteri- nary literature to substatrtiate claims of efficacy. The purpose of this randomised, double-blinded, placebo-controlled study l()t R¡..¡\1. ()I S\r^1.1.,\NlIri\l. PRi\(--lr(:[ . V()L 45. lUNlì 2004 293
Transcript of Effect of omega-3 fatty.acids canine atopic dermatitis · 2017. 11. 1. · Effect of omega-3...

Effect of omega-3 fatty.acids oncanine atopic dermatitis
Twenty-nlne dogs were lncluded ln a double-bllnded,
placebo+ontrolled, randomlsed trlal and were orally
suppfemented for 10 weeks wlth elther flax oll (2OO mg/kg/dayl,elcosapentaenolc acld (5O mg/RC/day) and docosahexaenolc
acld (35 mg/Rg/day) ln a commerclal preparatlon, or mlneral
oll as a placebo. For each dog, cllnlcal scores were determlned
based on a scorlng system developed prlor to the trlal. Total
omegao and omega3 lntake and the ratlo of omega6:omega-3
(omega-6:3) were calculated before and after the trlal. The dogs'
cllnlcal scores lmproved ln those supplemented wlth flax oll
and the commerclal preparatlon, but not ln the placebo group.
No correlatlon was ldentlfled between total fatty acld lntake or
omega6:3 ratlo and cllnlcal scores. Based on the results of thls
study, the total lntake of fatty aclds or the omega€:3 ratlo do not
seem to be the maln factors ln determlnlng the cllnlcal response.
R. S. Mueu-en, K. V. FrEsEr-ER*,
M. J. FEnu¡N, S. Z¡sEl*,R. A. W RosvcHur, G. K, Ocrr-vrE
¡r.¡o T. L. GREe¡¡wnLr*
Journal of Small An¡mal Pract¡ce (2OO4)45,293-297
Department of Clin¡cal Sc¡ences,and x Department of veter¡naryTeach¡ng Hospital, College ofVeterinary Medicine and B¡omedicalSciences, Colorado State Un¡versltfFort Colllns, CO 80523, USA
R. Mueller's current address isMedizinische Tierkl¡nik,Veter¡naerstr. 13, 80539Munich, Germany
G. Og¡lvie's current address is CVS
Angel Care Cancer Center, 100 N
Rancho Santa Fe, San Marcos,cA 92024, USA
IIIRODUGnOil
Canine atopic dermatitis is a common skin
disease in small animal practice (Scott and
Paradis 1990). h is defined as an inherentpredisposition to the development ofimmunoglobulin (lg) E antibodies to envi-
ronmental allergens, resulting in clinicalsigns following exposure to these allergens(Halliwell and Gorman 1989). Sympto-maric trearment modalities for canine
atopic dermatiris inclucle glucocorticoids,anrihistamines and fatry acid supplemen-
tation (Griffin 1993, Mueller 1993, Scottand orhers 2001). The only specific treat-ment for atopic dermatitis is allergen-
specific immunotherapy wherein allergens
identified by intradermal testing or serum
resring for allergen-specific IgE are injected
subcutaneously. Allergen-specific immu-notherapy must usually be pursued For
months before an improvement in clinicalsigns is seen and it is not effective in all
patients (Scotr and others 1993, Muellerand Bettenay 1996). For these reasons,
symptomatic therapies are often explored.Because adverse reacrions to glucocorticoid
therapy are common, more attention has
been paid recenrly to treatments that have
been associated with fewer adverse effects,
such as antihistamines and fatty acid sup-
plementation (Campbell 1993, Paterson
1994).
Bsenrial fatry acids have been used totreat humans with atopic dermatitis (Price
1984, Biagi and others 1988, Fiocchi and
others 1994, Paterson 1995, Henz and
orhers 1999) and allergic asthma (Stenius-
Aarniala and others 1989, Okamoto and
others 2000), and have been shown tomodulate the infìammatory response inhumans, mice and rats (Higgs 1985, Horiiand others 1991, Schafer and Kragealle
1991, Vatanabe and others 1994, Teren-
cio and others 1998). Oral fatry acid sup-
plementation has been noted to decrease
rhe inflammation and pruritus associated
with canine atopy (Bond and Lloyd I 992b,
Scort and others 1992, Logas and Kunkle1994). These benefits have been related tosupplementation with certain omega-6
fatty acids (gamma-linoleic acid [GLA])(Scarffand Lloyd 1992), combinations ofGLA and omega-3 fatty acids such as
eicosapentaenoic acid (EPA) and docosa-
hexaenoic acid (DHA) (Bond and Lloyd1992a, Scott and others 1992), variable
doses of omega-3 fatry acids (Logas and
Kunkle 1994) or omega-3 supplemented
whole diets with fixed omega-6:omega-3(omega-6:3) ratios (Scott and others
1997).Emphasi.s has recently been placed
on the use of omega-3 latty acid sup-
plementation at doses higher than the
manufacturer's recommendation in the
management of canine atopic dermatitis.Combination supplements of EPA and
DHA given in the range of 66 mglkgldayhave been noted ¡o clinically benefit
pruritic dogs (Logas and Kunkle 1994).
The use of flax oil as a source of potentially
beneficial omega-3 fatty acids has also been
recommended.'Io che authors' knowledge,
there are no published data in the veteri-
nary literature to substatrtiate claims ofefficacy. The purpose of this randomised,
double-blinded, placebo-controlled study
l()t R¡..¡\1. ()I S\r^1.1.,\NlIri\l. PRi\(--lr(:[ . V()L 45. lUNlì 2004 293

was to evaluate the infìuence of supple-mentation with flax oil and a commercialproduct containing EPA and DHA on rhe
clinical signs ofatopic dogs.
¡IAÏERIA].S AND iIEÍHOD8
Approval for the study was obtained fromthe Animal Care and Use Committeeof Colorado State Universiry. Dogs withnon-seasonal aropic dermaticis were
included in the study. Atopic dermatitiswas diagnosed by history clinical examina-tion and exclusion ofdifferential diagnoses
such as food adverse reactions or scabies
with appropriate tesrs or trearments as
described elsewhere (Mueller 1993, Scortand others 1993,2001). Offending aller-
:...T: *.* identified with an intradermal
Dogs were fed the same recorded rypeand amount of diet for eight weeks prior toand during latty acid supplementation.The total amounrs of omega-3 and omega-6 latry acids received before and during thetrial were calculated for each dog using themanufacturer's informa¡ion outlining rhefatty acid contenr of rhe used commercialdiet and adding the fatry acid content ofthe administered supplement.
Each dog was assigned to one of threegroups of I 0 dogs using a table of randomnumbers and simple randomisarion. Thegroups were treated, ar a dose ofar least onecapsule per 5 kg of bodyweighr, with a com-mercial latry acid supplemenr (3V Caps;
DVM Pharmaceuticals), flax oil capsules
containing 570 mgof c-linolenic acid and170 mg of linoleic acid per capsule, or a
placebo containing mineral oil. Thus rhe
dose range for each animal varied from 50
to 85 mg ol tsPA/kg and 35 to 55 mg ofDHA,/kg every 24 hours for the dogs r€ceiv-
ing the commercial fatry acid supplement,arrd from 200 ro 335 mg/kg of flax oil every
24 hours for the second group. Neirherowner nor clinician was aware of the narureof the supplementation. Supplements were
given lor l0 weeks. Owners and clinicianscornpleted evalu:rtion forms immediately
before and after the fatry acid therapy.
Owner clinical scores were obtained byadding the scores for pruritus, skin lesions
and medication. Pruritus was scored o¡r a
continuous visual analogue scale o[ 0 to30, 0 being no pruritus, 30 being intense
pruritus noted at all times. Each observed
skin lesion (erythema, papule or crust) was
counted separately and graded as: mild,1.5 points; moderate, 3 points; and severe,
4'5 points. No concurrent medication was
scored as 0 poinrs, topical therapy as 5points and anrihisramines as l0 points.Frequent antibiotic therapy (more than 21
days during the I 0-week study) scored 20poinrs, while less frequent ântibioricadministration during this period scoredl0 points. The score Êor glucocorticoidswas determined by the dose. A calculateddaily average dose of I mg/kg or more
scored 40 points, benveen 0'5 mg/kg and Img/kg daily scored 30 points, becween 0.2mg/kg and 0.5 mg/kg daily scored 20
points and less than 0.2 mg/kg daily scored
l0 points. The overall maximum score foran animal was I17.5 points.
Clinician clinical scores were obtainedsimilarl¡ but prurirus scored 0 whenabsent, l0 poinrs when mild (scrarching
was not seen in the waiting or examinationroom, bur could be induced), 20 pointswhen moderate (scratching, licking or rub-bing could be observed in the examinationor waiting room, but ceased during the
examination) and 30 points when severe(scratching, rubbing or licking occurred
during the examination).'fhe nrean total number of positive
inrradermal reactions was derermined foreach group and compared wirh a Kruskal-Vallis resr. 'lotal dierary omega-3 andomega-6 farry acid inrakes before and afrersupplementation were calculated byadding dietary intake and supplementaryfatty acid content together.'fhe total latryacid intake of the three groups was com-pared with a Kruskal-Vallis test. Subjec-rive evaluations ofpruritus, performed by
continuous scale plotting, were quanri-rared and rhe scale distances were evaluared
xs corìtirìuous data lor normaliry of distri-
bution by the Kolmogorov-Smirnov test.
Normally disrributed data were compared
over time by one-way analysis of variance(ANOVA). Group means were compared
by a Kruskal-Vallis test, and clinician andowner scores within groups by a lVilcoxon
marched pair test. A Pearson's test was used
to evaluate correlations between intake ofomega-3 and omega-6 fatry acids oromega-6:3 ratio and clinician scores. Thecorrelation between clinician and ownerscores was also examined with a Pearsont
resr. A P value of less than 0'05 was consid-
ered significant.In addition to statistical evaluation, the
dietary inrake of fatry acids and the omega-
6:3 rario of the dogs responding fully totherapy were compared with a correspond-
ing number ofdogs in the same groups notresponding ât all to detect possible differ-ences that could not be identified with the
statistical evaluation, due to the large stan-
dard deviatio¡r of most values withingrouPs.
REIUtls
Thirry dogs were included in the study. Alldogs had positive intradermal testsi the
mean number of positive reactions was
nine in the placebo group (range three tol8) and l0 in borh the group treated witha commercial product and the flax oilgroup (ranges four to 19 and four to 22,
respectively). There was rro significantdifference in positive reactions between
groups using a Kruskal-Vallis test
(P=0.87).
Supplemerrtation was discontinued forone dog in rhe placebo group when irdeveloped diarrhoea. 1wenry-nine dogs
completed the study. Of these 29 dogs, l3dogs had been on antihistamines withincomplete Íesponse prior to the study. Inall dogs these antihistamines were contin-ued ar the same dose until the end ofthe study. Similarl¡ l3 dogs received
weekly shampoo therapy at the beginningofthe srudy and rhis continued unchanged
rhroughour the study. In one dog,
294 l()l. R\i\1. ()F S\1,\l l. ^\l\1,\l
I'RÀ(. I l(:t: . V()1. 45 ' JUNL 200.í

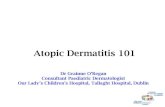
Table 2. Glinical scores reported by owners and cliniciansbefore and after treatment with placebo, flax oil or acommercial product (mean t standard dev¡at¡on)
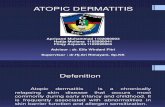
fable 1. Total d¡etary intake of omega-3 and omoga-6 fattyac¡ds and standard deviation ¡n dogs supplemented withplacebo, flax oil or commercial EPA,/DHA capsules (meant standard deviation)
PlaceboFlax o¡lCommercial capsules
Om¡|Þel¡fty.oE¡(l'{,/l(t lod}ll.l¡rll
84r73327t437r LrA7
Om.Éahttyældr(rrylr¡ùffiil|
509r196468r199426iL74
Pretreatmentclin¡c¡an scoresPost treatmentclinlclan scores(P value)rPretreatmentownef scofesPost-tr€atmentownef scores(P valuelr
Plsbo
29.Or10.0
23.5i7'9(P=0.2e7)
36.8r11
30'2r14(P=0'313)
Flrroll Comilældc.e.llh.
25.2t12.2 31114.5
18.1113.0 15.4111.1(P=0.0o8) (P=0.01)
2e,7*L3.2 29'9115.6
20,5ÈL2'5 I7.3Ìll'2(P=0,004) (P=0.02)
'P wtues obl8¡ned by compsfirE cllnlcsl swæ ot clhlcimg/trnêB bofole 8nd âff.or
treatment wilñ a w¡lcoxon matched p8lß test
shampoo therapy was added during thestudy. None ofthese shampoos containedfatry acids.
Three dogs were on glucocorticoidmaintenance therapy prior to inclusion,with unsatisfactory results. In all threedogs, the dose was less then 0.2 mglkgldayand was continued throughout the study.In one of these dogs, the dose could be
decreased further, but due co the low ini¡ialdose the score assigned was unchanged.Two ofthe dogs improved by 25 per cenrin pruritus scores. One o[ these dogs was
on placebo, the other on commercial sup-plement. 'fhe last dog was on commercial
supplement without any improvement.Antibiotics were administered in seven
dogs prior to the study. Six dogs were onantibiotics at the end of the srudy. Fourdogs had developed a pyoderma during rhe
study. Two dogs received antibiotics as
pulse maintenance therapy prior to inclu-sion and throughout rhe srudy.
The daily dierary inrakes of omega-3and omega-6 fatry acids were calculated byadding the fatty acid content of the con-sumed diet and the supplement ('Iable l).'l-he dierary inrake of omega-3 arrd omega-6 farry acids was nor differenr berween thethree groups at the beginning of the trial(P=0'546 and P=0.489, respectively).'Ihedietary intake of omega-3 fatry acids morethan doubled with supplementation in the
group receiving the commercial capsules(to 141x67 mg/kg, P=0.0001) andquadrupled in the flax oil group (ro
326¡436 mg/kg, P=0.001 l).'l'he omega-6i¡rtake increascd by an average of l7 percent in the fìax oil group (to 5481218mg/kg, P=0.579).
There were no significant differences
between groups at the beginning of the
trial for clinical scores determined by clin-icians (P=0.623) or owners (P=0.612)
('lable 2). Clinical scores for dogs receiving
flax oil and commercial EPA/DHA sup-
plemenrs improved significantly duringthe l0 weeks of supplementation com-
pared with the control group (P=0.008,
P=0.01 and P=0.297, respectively) (Table
2). The mean scores o[dogs receiving the
commercial EPA/DHA supplement and
the flax oil capsules at the end of the studywere lower than those of dogs receiving
placebo. However, the difference was notsignificant lor owner or clinician scores.
Improvement of more than 50 per centwas seen in the owner scores of two dogs
and the clinician score of one dog in theplacebo group and in both scores of lourdogs in the group receiving flax oil cap-
sules. Five of the dogs receiving commer-cial EPA/DHAcapsules improved by more
than 50 per cent according to cliniciansand four of these improved based on
owner scores. Complete clinical remissionwith no other treatmerrt but the supple-menration was seen in two dogs receiving
commercial EPA/DHA capsules and one
dog given flax oil capsules. Irr rwo o[ these
dogs, supplementarion was discontinuedand clinical signs recurred. Dogs improved
again when supplementation was resumed.
In the third dog, supplementation was
administered continuously aFter the studyand no recurrence occurred during a l2-monrh follow-up period.
'l'here was ge nerally a good correlationbetween owner and clinician scores,
betwee¡r overall owner scores (the sum of
their pruritus, clinical and medicationscores) and owner pruritus scores, and
overall clinician scores and clinician pruri-tus scores (P=0.001, 12=0.754). Ownerand clinician scores differed by more than
20 per cent for judging improvement inseven ofrhe 29 dogs completing the study.
Owner scores revealed a better improve-menr in wvo dogs; clinician scores revealed
a better improvement in five dogs.
There was no correlation between clini-cian score and omega-3 fatry acid intake(P=0.19), omega-6 fatry acid intake(P=0.84) or omega-6:3 ratio (P=0'18).
Comparing the dogs in remission on ther-
apy with the corresponding dogs notimproving at all, there were no obvious dif-ferences in the dietary intake of omega-3
or omega-6 latty acids or the omega-6:3
ratio, or in the clinical scores at the s¡art olsupplementation.
DtsGUtStoil
Prurirus scores, overall clinician scores and
overall owner scores associated extremely
well for all groups before and after fattyacid supplementation. 'fhis suggests thatthe scoring system was valid and that the
degree of pruritus is generally a good indi-cator of the severiry of atopic dermatitis indogs.
Supplementation with essential lattyacids has been reported as a successful
alternative to glucocorticoid rherapy in the
rrearment of pruritic dermatoses in dogs
(Bond and Lloyd 1992b, Logas and Kun-kle 1994) and cats (Harvey 1991, 1993,Logas and Kunkle 1993). Proposed mech-
,()UR\i\l. ()F Sñl^1.1. ^Nll\1,\1.
PR^(;l l(:lì . VOl.45. JUNIÌ 2004 295

anisms of acrion include modulation ofeicosanoid production, inhibition of cellu-lar activation and an increase in the epider-
mal barrier funcrion, Eicosapentaenoic
acid (omega-3) and dihomogammalinoleicacid (IDHGLA], omega-6) both competewirh arachidonic acid ([AA], omega-6) as a
substrate For ryclo-oxygenæe and 5-lipoxy-genase, which converts these latry acids to
prostaglandins (PGs) and leukotrienes(LIs), respectively (Wright 1991). Pro-inflammatory PGs such as PGE2 and
PGF2,, and LIs such as LIB4 are derivedfrom AA. Eicosanoids derived fromDHGLA and EPA have less inflammatoryor anti-inflammatory action (Miller and
others 1991, Gallai and others 1995).
Increases in anti-infl ammatory eicosanoids
and concurrent decreases in their pro-inflammatory counterparts presumably
decrease cutaneous inflammation.Decreased concentrations of cutaneousLTB4 and decreased production of LTBa
by activated neutrophils have been
reported in dogs alter receiving diets withlower omega-6:3 rarios and diets higher inomega-3 farry acids, respectively (Vaughn
and others I 994, Byrne and others 2000).A number of clinical studies have been
published evaluating fatry acid supplemen-tation for the treatrnent ol canine atopicdermatitis. However, to the authors'
knowledge, none have quantifìed the totalfatry acid intake by calculating rhe sum ofdietary intake and supplementation.In this stud¡ intake of omega-3 and
omega-6 fatty acids, as well as their ratios,varied enormously beFore the ¡rial due tovariable dietary intake (240 rc 942 mglkgomega-6, 20 ro 260 mg/kg omega-3 fattyacids and 0'84:l to 20:l omega-6:3 ratio)and during the rrial due to the combina-tion of dietary intake and supplementation('lable l).
However, rhere was no correlarionberween omega-3 inrake, omega-6 in¡ake
or omega-6:3 ratio and pruritus scores,
clinician scores or owner scores before and
afrer the rrial. 'Ihis suggests rhac rhe effec-
tive dose depends on more than the totalintake or ratio ofessentiâl fatcy acids. fu of
yer unidentified individual idiosyncraticfactors may be relevant for individualresponses. Fatry acids can influence the
immune system by acting as second mes-
sengers, regulators of signal transducing
molecules or transcription factors (Hwang
2000). They have been reported to sup-
press interleukin-2 (lL-2) production and
mononuclear cell proliferation (Endres
and others 1993). To what degree directeffecrs of fatry acids on immune functionare responsible for the clinical effects ofomega-3 supplementation in the atopicdog is unknown.
In this stud¡ the response to flax oilsupplementation was less pronounced
than supplementation with a commercialproduct containing EPA and DHA. Flax
oil contains predominantly c-linolenicacid which is desaturated and elongated invarious steps to EPA, a subsrrate compet-ing with AA for cyclo-oxygenase and
lipoxygenase to be processed to less inflam-matory eicosanoids. Final concentrations
of EPA attained are therefore potentiellywidely variable, depending on the capabil-
ities oF the individual to process the u-linolenic acid as outlined above. To the
authors' knowledge, there are no data
quantirying this conversion in the dog todate. In contrast, commercial EPA/DHAcapsules contain predominantly EPA,
which should be immediately available forcompetitive metabolism with AA. Based
on rhe resuks in this stud¡ it is difficult toderermine rhe preferred fatry acid (a-linolenic acid versus EPA and DHA) lorsupplementation in dogs with atopic der-
matitis, due ro the small number of dogs irr
each group.In this stud¡ approximately half of the
l0 dogs in each treatmenr group improved
by more than 50 per cent. Completeremission was achieved in l0 to 20 per
cent ofdogs. However, although the onlysignificant improvement irr scores withrrearment was seerr in dogs treated with the
commercial producr containing EPA and
DHA, there was no significant difference
berween treatment groups and the placebo
group (in which one dog improved by
296 J()URN..^I. OF Srf,\t.t. ANIM^l. PR^(;rlcli . v()L 45. JUN[ 2004
more than 50 per cent) at the end of the
study. Neither total intake of omega-3 or
omega-6 fatry acids nor their ratio was cor-
related to clinical improvemen¡. Further
studies with larger numbers of animals are
needed to explore these findings furtherand to examine the benefit of supplements
conraining predominantly omega-6 fatry
acids for the treatment of canine atopic
dermatltis.
AcknowlodÉementsThis study was financially supported bya grant from the Shipley Foundation. Theplacebo capsules and the commercial fatry
acid supplements were kindly donated by
DVM Pharmaceuticals, Miami, FL, USA.
Reference¡BÁcl, P. 1., EoRooNr,4., Mag, M., Rlccl, G., FAN€u, C.,
PARmEr, A. & CEccoúNr, E. (1988) A long-term studyon lhe use of even¡ng primrose oil (Efamol) in atopicch¡ldren. O/ugs undet Expeûmental and Cl¡nicalResearch L4,285-290
8oND, R. & LLoyo, D. H. (1992a) A double.blindcompar¡son of ol¡ve oil and a combinâtiûn of even¡ngprimrose orl and f¡sh o¡l in the management ofcanine atopy. Veteìnaty Recoñ L31, 558.560
BoNo, R. & LLoyo, D. H. (1992b) Random¡zed single.blind comparison of an evening pr¡mrose oil and fsho¡l combination and concentrates of these oils in themanagement of can¡ne alopy. Veteilnaty OermatoLog/3,215-2L9
8YRNE, K. P., CAMpsEr"L, K. 1., DAVS, C. 4., SCHÂEFF€R,
D. J. & TRouÍ, H. F. (2000) fhe effects of d¡etaryn.3 vs n.6 fatty ac¡ds on ex.vivo LTB4 generationby canrne neutrophrls. Vetet¡nary Dermaloloqy 1!,L23-L3t
CAMPB€L!, K. L. (1993) Clinrcal use of fatly ac¡d sup-plementations an dogs. veleûnary Dematologtt 4,167.173
EñoR€s, S., MEyoAN, S. N., GxoRE Nt, R., ScHtNDLrR, R.
& 0rNARErro, C. A. (1993) Dietary supplementat¡onwrth n-3 fatty acids suppresses ¡nterleukin'2 pro.
duct¡on and mononuclear cell Otolile'alton- Journal
ol Leu\ocyte Eiologl 54, 599.603Frocc¡r, 4., SAt , M.. SrcNoRoNt, P., EaNDEMU, G., AGos.
Toir, C. & RN , E. (1994) The eflicacy aôd salety olgamma.lrnolenrc ac¡d tn the treatment of rnfanlileatopic dermal¡trs. Journal of lntemalional MedicalResearch 22, 24-32
GatLA, v., SaRcHTEU-r, P., TR€QU^¡RIN,4., FR¡tcEscHlN, M,,FroRrDr, 4., FrR€Nz€, C., A[8ERn, 4., DIB€NEDsÍo, D. &STRAGLrono, E. (1995) Cßok¡ne secretion and
e¡cosanord productron rn the peripheral bl00dmononuclear cells of mult¡ple sclelosrs patients
undergoing dietary supplementat¡on wrth n'3 polyun'
salurated fatty acrds. Journal of Neuro¡mmunologtl56, 143.153
GRrffiN, C. E. (1993) Canine atoprc drsease. ln: Currentvetefnary Dermatology. Eds c. E. Gntfrñ, K. w.Kwochka and J. M. Macdonald. Mosby, St. Lours.pp 99-120
Har-r"rwÉr-L, R. E. W. & GoRMN, N. (1989)Atoplc disease.ln: Veternary Clinical lmmunology. Eds R. E. w. Hal.lrwell and N. Gorman. W. B. Saunders, Ph¡ladelphra.
þþ 232-252

HaRv€y, R. G. (1991) Management of feline mrl¡ary der-mat¡t¡s by supplement¡ng the d¡et w¡th essential fattydcids, Veteúnaty Record L28, 326-329
HaRv€y, R. G. (1993) Effects of vary¡ng proport¡ons ofeven¡ng pr¡mrose o¡l and fish o¡l on cats with crust-¡ng dermatos¡s ('m¡l¡ary dermat¡trs'1. Veter¡naryRecoñ I33,208.2tr
HEM, 8. M.,JAsroNsKA, S., VN 0E KERuoF, P. C., SÍNGL,G., Br^szc¿yx, M., VaNoËRvarx, P. G., VE€NHU|Z€N, R.,Muccu, R. & RaEo€RsroRFF, 0. (1999) Double'blind,mult¡centre añalysis of the efficacy of borage o¡lin patients with atopic ec¿ema. Sritisñ Journal oÍDe m atologtt L4O, 685-688
Hrccs, G. A. (1985) The effects of d¡etary ¡ntake ofessent¡al tatty ac¡ds on prostaglandin andleukotriene synthesis. Proceedings of the Nutritionsociety ¿14, 181.187
HoRn, T., SAloucHr, K., Ko8^yasHr, Y., Saro, K., WATaNABE,
S., YosHrDA, Y. & oKUyAilA, H. (1991) Effect of d¡etaryalpha¡¡nolenate on platelet-activating factor produc.t¡on in rat peritoneal polymofphonuclear leukocßes.)ounal of lmmunology 147, 1607.1613
HwANc, D. (2000) Fatly acids and immune responses- a new perspect¡ve in searching fof clues to mech.anism. Annual Rev¡ews of Nuùit¡on 20, 431-456
LocÁs, D. & KuNKr.€, G. A. (1994) Double-bl¡nded cross-over study with marine oil supplementat¡on conlain.ing high.dose eicosapentaeno¡c ac¡d for thetreatment of canine pruritic skin disease. VeteùnatyOermatoloqtt 5,99-\04
LoGAs, 0. B. & KUN(LE, G. A. (1993) Double-blindedstudy exam¡n¡ng the etfects of even¡ng pr¡mrose oilon fel¡ne prur¡tic dermalilis. Veteùnaty Dennatolog,y4, 181.184
Mrr[ER, C. C., laNc, W., ZrBoH, V. A. & FLflcHER, M. P.
(1991) D¡etary supplementat¡on w¡th ethyl ester con.centrates of f¡sh o¡l (n.3) and borage orl (n.6)polyunsaturated fatty ac¡ds induces epidermal gen.eration of local putatrve anti-inflammatory metabo-liles, Jounal of lnvesl¡gal¡ve Oetmatologtt 96,98.103
MUErl€R, R. S. (1993] D¡agnosis and management ofcanine atop¡c d¡sease. Australian Veterinary Prccti.tioner 23,20-27
MUELLER, R. S. & BEîENÀY, S. V. (1996) Long-term¡mmunotherapy of 146 dogs with atopic dermatat¡s -a retrospect¡ve study. Áusl/álian Veleilnaty Pâctitionet28, L28.L32
oxÁÀlolo, M., MÍsuNo8u, F., AsHrDÁ, K., MrFUr{E, T., Hosa{,Y., TsucÉNo, H., HaÂÂDA, S. & fNEMr, Y. (2000)Eflects of d¡etary supplementat¡on with n-3 fattyac¡ds compared wilh n.6 tatty acids on bronchialasthma. lntemal Med¡cine 39, LO7 -IL!
PArERsoN, S. (1994) Use of ant¡histamrnes to controlprur¡tus ¡n atopic dogs. Journal of smail An¡rnalPrcct¡ce 35, 4L5-419
P^r€RsoN, S. (1995) Additive benel¡ts ol EFAS in dogswith atopic dermatit¡s after part¡al response to anti.h¡stam¡ne therapy. Jouñal of Sñall Animal Practice36, 389.394
PRrcÊ, M. L. (1984) lhe role of diet in the managementof atopic eczema. Huñan Nuttit¡on. Applíed Nutrition38,409.415
SCARFF, 0. H. & Lroyo, D. H. (1992) Double bl¡nd,placebo.controlled, crossover study of evening pr¡m.rose o¡l in the treatmenl of canine alopy. Veter¡naryRecord t31,97-99
SCHAFER, L. & KRAGBAT-!g, K. (1991) Supplementat¡onwith even¡ng primrose o¡l in atopic dermatitis: ef fecton fatty ac¡ds ¡n neutrophils and epaderm¡s. ¿ip¡ds26, 557-560
Scorr, D. W., Mru.ER, W. H. & GRrrnN, C. E. (2001) Canineatop¡c disease. ln: Small Animal 0ermatology. W. B.Saunders, Philadelphia. pp 574.601
Scor, D. W., Mrr[ER, W. H., oEcxfR, G. A. & W€[uNGroN,
J. R. (1992) ComÞar¡son of the clin¡cal efficacy oftwo commercial fatty ac¡d supplements (Efavet andoVM Derm Caps), even¡ng pr¡mrose o¡1, and coldwater marine fish oil in the management of allerg¡cprur¡tus in dogs: a double.bl¡nded study. Cornel,Veteilnar¡an 82, 3L9-329
ScorT, 0. w., M|tlER, W. H., RE|NHÂRI, G. A., MoHAMMED,
@ British Small Animal Veterinary Association. All rights reserved
H. O. & BacLADr, M. S. (1997) Effect of an omega3/omega 6 fatty acid.conta¡n¡ng commercial lamband r¡ce d¡et on pruritus in atoptc dogs: results of asingle.bl¡nded sludy. Canad¡an Journal ol VeteñnaryResea/c¡, 61, 145.153
Scorf, D. W. & PARAÞrs, M. (1990) A survey ofcan¡ne and feline skin d¡sordels seen iñ a univelsitypract¡ce: small animal clin¡c, Un¡versity ol Montreal,sr Hyac¡nthe, Quebec (1987-1988\. Canad¡anveter¡naty Journal 31, 830.835
ScorT, K. V., wxrTE, S. D. & RosYcHUK, R. A. W. (1993)A retrospect¡ve study of hyposensit¡zat¡on rn atop¡cdogs ¡n a flea.scarce env¡ronñenl. ln: Advânces¡n Veter¡nary Dermatology. Eds P. J. lhrke, l. S.Mason and S. D. White. Pergamon Press, New York.pp 79.87
SreHrus-A¡n¡uu. 8., ARo, 4., HsuLtNEN, 4., AHoLÂ, 1.,
SEpmLA, E. & VApAÂTAto, H. (1989) Even¡ng pr¡moseoil and fish oil are ¡neffect¡ve as supplementarytreatment of bronch¡al asthma. Ännals oÍ Aileryy62,534-537
tERÊr\cro, M. C., FERRÂI\o|Z, M. 1., PosaDAs, 1., RotG, E., DE
RosA, S., 0E Grulto,4., PAyÁ, M. & ALCARÁ¿, M. J.
(1998) Suppression of leukolriene B4 and tumournecrosis factor alpha release in acute ¡nflammatoryresponses by novel prenylated hydroquinone der¡v.at¡ves. /Vauny, SctlmiedeberÉ,s Archives of Pharma-cotogy 357, 565-572
VaucrN, D. M., RETNHARÍ, G. A., SwaM, F. S., LAUIÊN, S.o., GaRN€R, C.4., BouDREAx, M. K., SñNo, J. S., HoFF
MAN, C. E. & CoNNER, B. (1994) Evaluatton of effectsof dietary n-6 to n-3 fatty ac¡d ratios on leukotíene8 synthes¡s rn dog skin and neulroph¡ls. Vete¡¡natyDematology 5, 163-L73
WATAM8E, S., SaxÄ, N., YÂsur, Y., K|MURA, Y., KoBAYASHI,
T., MrzurNr, T. & oKUYNA, H. (1994) A h¡gh alpha-linolenate diet suppresses anl¡gen-inducedimmunoglobulin E response and anaphylact¡cshock ¡n m¡ce. Journal ol NuìÍ¡lion 124, 1566-1573
WRrcHr, S. (1991) Essent¡al fatty ac¡ds and the skln.Br¡tish Joumal of Dematology t25, 5O3-5L5
JOUR\¿\Ì- ()l: SIÍ^I.1.,\NlIr.\1. PR¡\(iilCl- . \/Ol.45. lUt'iti 2004 297