Effect of Blood Sampling, Processing, and Storage on the … · 2017-04-14 · tested for C3, C4,...
8
558 Am J Clin Pathol 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL © American Society for Clinical Pathology AJCP / Original Article Effect of Blood Sampling, Processing, and Storage on the Measurement of Complement Activation Biomarkers Shangbin Yang, PhD, 1 Michael McGookey, 1 Yi Wang, PhD, 2 Spero R. Cataland, MD, 1 and Haifeng M. Wu, MD 1 From the 1 Department of Pathology and Internal Medicine, College of Medicine, The Ohio State University, Columbus, and 2 Translational Medicine, Alexion Corporation, Cheshire, CT. Key Words: Complement activation; Biomarker; Thrombotic microangiopathy; Diagnosis; Specimen handling Am J Clin Pathol April 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL ABSTRACT Objectives: Recent studies have shown that complement hyperactivation contributes to development of thrombotic microangiopathy. The evaluation of complement biomarkers is known to be influenced by inappropriate specimen handling. However, there has been no study fully addressing this topic. Methods: Blood from each donor was subjected to 62 different handling conditions prior to complement assays. Results: Complement biomarkers (C4d/C3a/factor Bb/C5a/ C5b-9) are stable at room temperature (RT) for up to 4 hours in whole blood containing citrate or EDTA. However, under similar conditions, levels of C4d and C3a were significantly higher in serum than those in plasma. Thawing of the samples on ice or at RT had no significant effect on complement levels. In contrast, thawing at 37°C resulted in striking increases in levels of the complement system in serum and citrated plasma but not in EDTA plasma. Up to four freeze/thaw cycles on ice or RT did not substantially increase the levels of C3a, factor Bb, C5a, and C5b-9 but had a significant effect on C4d. Long-term storage of citrated plasma at –80°C for up to 6 years had no significant effect on levels of complement factors. Conclusions: The results from this study thus provide crucial guidelines for future investigations using complement biomarkers to define the role of complement system in disease. Complement dysregulation is known to contribute to a wide range of disease processes. 1-5 Recent studies strongly suggest that complement hyperactivation plays an essential role in the development of various clinical phenotypes of thrombotic microangiopathies (TMAs). 6,7 Atypical hemo- lytic uremic syndrome (aHUS) is a type of TMA caused by excessive complement activation secondary to either an inherited defect and/or acquired antibody impairing the regulatory function of the complement system. The genetic abnormalities in patients with aHUS may involve regulators of complement-alternative pathways such as factor H, factor I, or complement activation factors. 8 A specific complement inhibitor, eculizumab, has been approved by the US Food and Drug Administration for the treatment of aHUS. 4,9,10 New studies also have shown that complement activation biomarkers are elevated in patients with another type of TMA, thrombotic thrombocytopenic purpura (TTP). 11,12 The severity of increases in complement biomarker lev- els appears related to worse clinical outcomes in TTP. 13 Involvement of the complement system in TTP’s disease course is also supported by a report that a patient with TTP refractory to plasma exchange therapy achieved long-term remission after being treated with a complement inhibitor (anti-C5). 14 Furthermore, in patients with hematopoietic stem cell transplant (HSCT)–associated TMA, a study has shown a high prevalence of factor H–related gene deletion and factor H autoantibodies, suggesting that dysregulation of the complement-alternative pathway may contribute to the pathogenesis of post-HSCT TMA. 15 Taken together, these studies support the role of complement dysfunction in the development of TMA and provide a basis for using comple- ment biomarkers clinically to evaluate patients with TMA.
Transcript of Effect of Blood Sampling, Processing, and Storage on the … · 2017-04-14 · tested for C3, C4,...

558 Am J Clin Pathol 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
AJCP / Original Article
Effect of Blood Sampling, Processing, and Storage on the Measurement of Complement Activation Biomarkers
Shangbin Yang, PhD,1 Michael McGookey,1 Yi Wang, PhD,2 Spero R. Cataland, MD,1 and Haifeng M. Wu, MD1
From the 1Department of Pathology and Internal Medicine, College of Medicine, The Ohio State University, Columbus, and 2Translational Medicine, Alexion Corporation, Cheshire, CT.
Key Words: Complement activation; Biomarker; Thrombotic microangiopathy; Diagnosis; Specimen handling
Am J Clin Pathol April 2015;143:558-565
DOI: 10.1309/AJCPXPD7ZQXNTIAL
ABSTRACT
Objectives: Recent studies have shown that complement hyperactivation contributes to development of thrombotic microangiopathy. The evaluation of complement biomarkers is known to be influenced by inappropriate specimen handling. However, there has been no study fully addressing this topic.
Methods: Blood from each donor was subjected to 62 different handling conditions prior to complement assays.
Results: Complement biomarkers (C4d/C3a/factor Bb/C5a/C5b-9) are stable at room temperature (RT) for up to 4 hours in whole blood containing citrate or EDTA. However, under similar conditions, levels of C4d and C3a were significantly higher in serum than those in plasma. Thawing of the samples on ice or at RT had no significant effect on complement levels. In contrast, thawing at 37°C resulted in striking increases in levels of the complement system in serum and citrated plasma but not in EDTA plasma. Up to four freeze/thaw cycles on ice or RT did not substantially increase the levels of C3a, factor Bb, C5a, and C5b-9 but had a significant effect on C4d. Long-term storage of citrated plasma at –80°C for up to 6 years had no significant effect on levels of complement factors.
Conclusions: The results from this study thus provide crucial guidelines for future investigations using complement biomarkers to define the role of complement system in disease.
Complement dysregulation is known to contribute to a wide range of disease processes.1-5 Recent studies strongly suggest that complement hyperactivation plays an essential role in the development of various clinical phenotypes of thrombotic microangiopathies (TMAs).6,7 Atypical hemo-lytic uremic syndrome (aHUS) is a type of TMA caused by excessive complement activation secondary to either an inherited defect and/or acquired antibody impairing the regulatory function of the complement system. The genetic abnormalities in patients with aHUS may involve regulators of complement-alternative pathways such as factor H, factor I, or complement activation factors.8 A specific complement inhibitor, eculizumab, has been approved by the US Food and Drug Administration for the treatment of aHUS.4,9,10 New studies also have shown that complement activation biomarkers are elevated in patients with another type of TMA, thrombotic thrombocytopenic purpura (TTP).11,12 The severity of increases in complement biomarker lev-els appears related to worse clinical outcomes in TTP.13 Involvement of the complement system in TTP’s disease course is also supported by a report that a patient with TTP refractory to plasma exchange therapy achieved long-term remission after being treated with a complement inhibitor (anti-C5).14 Furthermore, in patients with hematopoietic stem cell transplant (HSCT)–associated TMA, a study has shown a high prevalence of factor H–related gene deletion and factor H autoantibodies, suggesting that dysregulation of the complement-alternative pathway may contribute to the pathogenesis of post-HSCT TMA.15 Taken together, these studies support the role of complement dysfunction in the development of TMA and provide a basis for using comple-ment biomarkers clinically to evaluate patients with TMA.

AJCP / Original Article
Am J Clin Pathol 2015;143:558-565 559 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
Assays for C3, C4, and CH50 have been used routinely for evaluation of complement pathways in clinical laborato-ries. However, these tests are generally not sensitive to the alterations in the complement system that occur in many dis-eases. For instance, in patients with aHUS and evidence of a genetic mutation, less than 50% show abnormal results when tested for C3, C4, and CH50 levels,16-20 and consequently, these complement levels are not routinely used to diagnose, monitor, and manage patients with aHUS. We hypothesize that the downstream proteolytic fragments of the comple-ment system are more sensitive to subtle dysregulation in the complement pathway. These candidate downstream biomarkers include C3a, C4d, terminal pathway activation product C5b-9 and C5a, and a product of the amplification loop, complement factor Bb. We and others have recently evaluated the performance of these downstream complement biomarkers and provided supporting evidence for their appli-cation in clinical evaluation of various types of TMAs.11,13,21
The analysis of complement biomarker levels in research studies and in the clinic is complex and subject to significant inaccuracies due in part to variation in sample collection and handling.20,22-24 Despite the considerable concern for potential false-positive results in the tests for complement biomarkers, there has been a lack of studies fully inves-tigating preanalytical effects on complement biomarker assays. In this study, we performed a detailed evaluation of how specimen sampling, processing, and storage condi-tions affect the results of biomarker assays for complement activation products C3a, C4d, C5a, C5b-9, and factor Bb. The objective of the study is to provide guidelines for clini-cal and research laboratories with regard to the handling of specimens for complement assays and ultimately to ensure that more accurate and reliable complement assays are being used in both clinical and research evaluation of patients with abnormal complement functions.
Materials and Methods
Standard Protocol for Sample ProcessingBlood from three study donors was collected in three
types of tubes: anticoagulated with EDTA, 3.6% sodium citrate, and without anticoagulant for preparation of serum. Upon blood draw, the serum collection tubes were inverted five times, allowed to stand at room temperature (RT) for 30 minutes, and then spun at 1,300g for 10 minutes. The supernatant was collected, aliquoted, and frozen in a –80°C freezer. For both EDTA and citrate anticoagulated speci-mens, samples were spun at 1,000g for 10 minutes to obtain an initial plasma preparation. After transferring the initial plasma to a new tube, the sample underwent a second spin
at 12,000g for 2 minutes to obtain the final platelet-poor plasma for study. All samples were processed as quickly as possible after blood collection from study donors. All spins were carried out in a refrigerated (4°C) centrifuge. Upon completion of processing, the samples were aliquoted and immediately frozen in a –80°C freezer.
Effect of Blood Handling Prior to Sample ProcessingTo evaluate the effect different handling conditions
have on test results, we subjected the citrate and EDTA whole-blood samples to various storage conditions before centrifugation to obtain the plasma samples. After the blood draws, one set of blood samples was stored at RT for 1, 2, 4, and 8 hours, respectively, before being processed for plas-ma. A second set of samples was stored in a 4°C refrigerator for 3, 24, and 48 hours prior to being processed.
Effect of Sample Thawing ConditionsSerum, citrate, and EDTA plasma frozen (–80°C)
samples were thawed under three different conditions: (1) sample aliquots (200 mL for each sample) were placed on the top of an ice bucket for thawing. On average, it took around 30 minutes for the samples to be thawed completely under this condition. (2) Sample tubes were placed in a RT water bath for 5, 10, 30, and 60 minutes. (3) Sample tubes were placed in a 37°C water bath for 5, 10, 30, and 60 minutes. Upon completion of each thawing condition, the sample tube was immediately placed on ice and then stored in a –80°C freezer until complement biomarker assays were performed for comparison.
Effect of Different Freeze/Thaw CyclesMultiple aliquots were made from each study sample
and then frozen (–80°C) immediately after the initial pro-cessing. For this study, different sets of study samples were subjected to a different number of freeze/thaw cycles (one to four times). For the samples undergoing multiple freeze/thaw process, the initially frozen samples were thawed in a RT water bath with frequent monitoring. Immediately upon thawing, the samples were put on ice and transferred into a –80°C freezer for the next freezing cycle.
Effect of Long-Term Storage of Citrate Plasma Samples From Patients With TTP
To determine the stability of complement biomarkers during long-term storage, we compared the performance of biomarkers in samples obtained over time from patients with TTP and stored over a 6-year period at –80°C. In our TTP cohort, there were a total of 88 episodes of TTP from 51 patients with TTP between 2006 and 2012. At the time of each TTP episode, the pretreatment sample was collected in citrated blood and processed freshly according to the

Yang et al / Preanalytical Effect on Complement Biomarker Tests
560 Am J Clin Pathol 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
standard protocol, and then 20 aliquots from each sample were banked immediately at –80°C. For this study, one aliquot from each of these 88 samples was thawed in 2012, and the levels of complement biomarkers were measured for comparison. All samples banked from 2006 to 2012 were thawed only once for study.
Complement Biomarker AssaysComplement biomarkers C4d, factor Bb, C3a, C5a, and
C5b-9 were measured by using commercial enzyme-linked immunosorbent assay kits. The assay kits for C4d (A008), factor Bb (A027), C3a (A031), and C5b-9 (A020) were from Quidel (Santa Clara, CA). The assay kit for C5a (557965) was from BD Biosciences (Franklin Lakes, NJ). The analyti-cal performance of these assays was examined prior to the start of this study. Initial analysis of the C5b-9 assay resulted in unsatisfactory test reproducibility (interassay coefficient of variation [CV] >50%) using the manufacturer’s protocol. Subsequently, we evaluated various assay conditions and their effects on the test performances of all complement assays. In the end, we modified the assay procedures for all assays by including 10 mmol/L EDTA and 1% bovine serum albumin in both assay buffer and sample diluent. By using the modified assay protocols, all assays in this study per-formed well for all three types of specimen (EDTA plasma, citrate plasma, and serum) with an interassay CV of less than 15%. Two additional quality control reagents, made locally from patient samples, were included in each assay to ensure quality performance during the entire study. An acceptable performance range for the quality control reagents was established prior to the start of the experiments.
Data AnalysisThe samples collected from three study donors were
assayed in duplicate, and the mean value from each donor was used for calculation. The data in the tables represent the mean and SD from the three study subjects. To illustrate the effect from different sample processing conditions, the data were normalized to corresponding controls shown in each of the tables. To analyze the complement biomarker data from patients with TTP, the data obtained were log-transformed to meet normal distribution for comparison. The data from
each year were compared to each other and their differences determined using one-way analysis of variance (ANOVA) Duncan’s multiple-range test with a significance of .05. All analysis was run by SPSS version 19 (SPSS, Chicago, IL).
Results
We first evaluated complement biomarker levels in dif-ferent sample types. As shown in ❚Table 1❚, when samples were collected in EDTA- or citrate-anticoagulated tubes, plasma complement biomarker levels were very similar to each other. In contrast, the serum samples lacking citrate or EDTA obtained from the same group of study partici-pants exhibited increased levels of complement biomarkers C4d and C3a. The mean values of C4d and C3a in serum were approximately two times higher than those in EDTA or citrate plasma, although statistical significance was not reached in this study involving limited sample sizes (n = 3). The levels of C5a, C5b-9, and factor Bb in serum, however, were similar to that in citrate or EDTA plasma.
Next, we examined how delaying sample processing affected the measurement of complement biomarkers. For both citrate and EDTA plasma, the results from different handling conditions were calculated as a ratio to the result obtained when the sample was processed freshly and imme-diately frozen at –80°C. Any results with a ratio greater than 1.5 were marked as meaningful (values in bold). As shown in ❚Table 2❚, complement proteins were relatively stable in citrated blood. Storage in a refrigerator or at RT for 3 to 4 hours prior to sample processing did not significantly affect the assay results. When the sample was stored for longer peri-ods of time (>4 hours) at RT or (>24 hours) at 4°C, the levels of factor Bb, C5a, and C5b-9 biomarkers did not change sig-nificantly; however, levels of C4d and C3a were significantly increased. When blood was collected in EDTA tubes, the complement factors, including C4d and C3a, were generally more stable during storage. All five biomarkers were not sig-nificantly altered after storing at RT for up to 8 hours or when samples were stored in a refrigerator for 24 hours. Storage in a refrigerator for 48 hours prior to processing, however, was associated with increased C4d and C3a levels.
❚Table 1❚Complement Biomarker Levels Under Different Blood Collection Conditionsa
Sample Type
Mean (SD), ng/mL
C4d (279-1,846 ng/mL) Bb (244-961 ng/mL) C3a (7-242 ng/mL) C5a (19-48 ng/mL) C5b-9 (34-238 ng/mL)
Citrate plasma 140.5 (6.0) 680.2 (115.2) 70.3 (6.8) 34.0 (5.1) 56.4 (13.4)EDTA plasma 145.3 (7.9) 878.7 (142.5) 86.7 (26.3) 38.5 (7.1) 73.2 (29.8)Serum 257.2 (116.2) 857.6 (84.9) 196.3 (77.5) 39.9 (7.5) 82.3 (36.6)
a The values for mean and SD were calculated from three study donors. Reference ranges for each biomarker were established using commercially available citrate plasma samples from individual healthy donors (n = 40), purchased from George King.

AJCP / Original Article
Am J Clin Pathol 2015;143:558-565 561 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
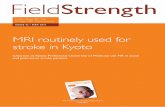
❚Figure 1❚ shows the effects of different thawing condi-tions on the measurement of complement biomarkers. As shown in Figure 1A, most complement proteins were stable when the samples were thawed in an RT water bath for up to 60 minutes. The only exception was factor Bb in serum, which increased about twofold after thawing for 60 minutes. In contrast, all biomarkers except C4d were increased sub-stantially and in a time-dependent manner when the serum or citrate sample was thawed at 37°C (Figure 1B). For exam-ple, after 1 hour of incubation, the amount of complement terminal pathway activator C5b-9 increased by 220- and 70-fold in serum and citrate plasma, respectively, whereas C4d levels were only slightly increased. In contrast to serum or citrate plasma samples, the complement factors in EDTA plasma were very stable. None of the biomarkers exhib-ited more than 1.5-fold changes over their baselines after a 1-hour incubation at 37°C. For all three types of specimen, thawing samples on ice for 3 hours led to no substantial changes in any of the five biomarkers (data not shown).
❚Table 3❚ shows the effect that different numbers of freeze/thaw cycles have on the complement biomarkers. For all three types of samples, there were no substantial changes in factor Bb, C3a, C5a, and C5b-9 levels over four freeze/thaw cycles performed either on ice or at RT. C4d levels in all three sample types, however, showed a greater than 1.5-fold increase following one to two freeze/thaw cycles at RT. When the samples were thawed on ice, the C4d levels in serum and citrate plasma exhibited a greater than 1.5-fold increase after three freeze/thaw cycles.
In our TTP biorepository, pretreatment citrate plasma from each episode of TTP was collected, processed, and banked from each episode of TTP using a standard proto-col. The number of TTP episodes encountered ranged from seven to 15 per year between 2006 and 2012. A total of 88 pretreatment samples were obtained from 51 patients with
TTP during this period. We hypothesized that if long-term storage at –80°C were to affect complement biomarker levels, the levels would demonstrate a trend over time. The measurement of complement biomarker levels was per-formed in 2012 to evaluate if there were significant differ-ences between the TTP samples collected in each of these 7 years. As shown in ❚Figure 2❚, the levels of the five comple-ment biomarkers remained relatively similar. No significant difference was observed in the mean values of C4d, factor Bb, C3a, C5a, and C5b-9 over this time period, using a one-way ANOVA Duncan’s multiple-range test.
Discussion
The study to define the sample requirements for a bio-marker assay is a key analytical step prior to the process for clinical validation of a new biomarker. Deferring from an epidemiology study that defines the biological variations of a biomarker’s performance in a population, the sample requirement analysis evaluates the effect of preanalytical factors that influence the test result. There is no scientific evidence that various sample handling conditions would affect individual people’s samples in different ways. Thus, in a typical sample requirement study, the variables include sample collecting method (eg, EDTA plasma, citrate plasma, serum), sample storage condition, sample storage time, sample freeze/thaw cycles, and so on. In this study, each donor’s sample was subjected to a total number of 62 vari-ous handling conditions for analysis. For each of the han-dling conditions, the assay was performed in duplicates, and the mean result from three study donors was shown. The data from this work therefore provide important guidelines for future studies regarding determination of the reference range for each of the complement biomarkers and evaluation
❚Table 2❚Effect of Different Storage Times Prior to Sample Processinga
Complement Biomarker
Citrate Whole Blood EDTA Whole Blood
Time at Room Temperature Before Processing
Time Refrigerated Before Processing
Time at Room Temperature Before Processing
Time Refrigerated Before processing
1 h 2 h 4 h 8 h 3 h 24 h 48 h 1 h 2 h 4 h 8 h 3 h 24 h 48 h
C4d (279-1,846 ng/mL) 0.95 (0.07)
0.96 (0.12)
1.05 (0.12)
1.34 (0.20)
0.93 (0.09)
1.80 (0.10)
2.40 (0.12)
0.96 (0.03)
1.00 (0.22)
1.10 (0.34)
1.35 (0.40)
0.92 (0.21)
1.32 (0.20)
1.58 (0.38)
Bb (244-961 ng/mL) 1.03 (0.06)
1.02 (0.08)
1.05 (0.06)
1.07 (0.10)
0.99 (0.04)
1.00 (0.09)
1.02 (0.03)
0.99 (0.06)
0.94 (0.01)
0.94 (0.04)
0.95 (0.05)
0.88 (0.04)
0.94 (0.05)
0.95 (0.11)
C3a (7-242 ng/mL) 1.02 (0.08)
1.04 (0.08)
1.31 (0.30)
1.94 (0.68)
0.88 (0.02)
1.06 (0.23)
1.53 (0.65)
1.07 (0.10)
1.12 (0.06)
1.16 (0.02)
1.26 (0.07)
1.04 (0.06)
1.41 (0.32)
2.49 (1.48)
C5a (19-48 ng/mL) 0.94 (0.04)
0.95 (0.11)
0.92 (0.12)
0.97 (0.11)
0.92 (0.04)
0.99 (0.11)
0.84 (0.06)
1.00 (0.03)
1.01 (0.09)
0.99 (0.09)
0.98 (0.09)
1.03 (0.03)
1.05 (0.08)
1.11 (0.13)
C5b-9 (34-238 ng/mL) 1.01 (0.13)
0.98 (0.12)
1.06 (0.16)
1.27 (0.34)
1.00 (0.16)
0.90 (0.10)
0.88 (0.06)
1.05 (0.11)
0.98 (0.10)
0.95 (0.03)
1.02 (0.02)
0.94 (0.12)
1.00 (0.09)
1.08 (0.15)
a For comparison, all values are normalized as ratios to the results obtained when the samples were processed immediately (see the data from Table 1). Values greater than 1.5 times of baseline values are shown in bold.

Yang et al / Preanalytical Effect on Complement Biomarker Tests
562 Am J Clin Pathol 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
Citrate plasmaEDTA plasmaSerum
Fold
Cha
nges
(Co
mp
are
to C
ont
rol W
itho
ut In
cub
atio
n)
0.0
1.0
2.0
3.0
0.0
0.5
5 10 30
Incubation Time (min)
60
0.0
1.0
2.0
3.0
1.0
1.5
0.0
0.5
1.0
1.5
0.0
0.5
1.0
1.5
C5b-9
C5a
C3a
Bb
C4d
Citrate plasmaEDTA plasmaSerum
Fold
Cha
nges
(Co
mp
are
to C
ont
rol W
itho
ut In
cub
atio
n)
0
1
2
3
0
5
10
15
20
0
7
14
21
28
35
0
3
6
9
12
0
100
200
300
5 10 30
Incubation Time (min)
60
C5b-9
C5a
C3a
Bb
C4d
A B
❚Figure 1❚ Effect of thawing conditions on the measurement of complement biomarkers. Citrate/EDTA plasma and serum samples from three healthy donors were thawed in a room temperature (A) or 37°C (B) water bath for 5, 10, 30, and 60 minutes. The mean ± SD fold of changes is shown.

AJCP / Original Article
Am J Clin Pathol 2015;143:558-565 563 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
of clinical utility of these biomarkers in disease diagnosis and prognosis.
In clinical laboratories, serum samples are routinely used for immunologic tests, including evaluation of the com-plement system. Citrated plasma samples are primarily used for study of the coagulation pathway. Many programs in the field of hemostasis have established biorepositories of plas-ma specimens collected longitudinally from patient cohorts. Given the recent discovery for the role of complement dys-regulation in the development of TMAs, these banked citrate plasma samples are a valuable clinical resource for further defining the interaction between complement and coagu-lation systems.11-13,25,26 Because of the ability of EDTA to inhibit complement activation in blood samples, some investigators have recommended using EDTA plasma for the study of complement activation.27,28 Thus, it is important to evaluate and compare how sample storage and processing affect the study results of the complement system in all three types of blood collection conditions.
When blood samples are freshly processed for plasma, there are very small differences in the level of C4d, factor Bb, C3a, C5a, and C5b-9 between citrate and EDTA plasma samples. However, C4d and C3a levels in serum from the same individuals are markedly higher than that in the plasma samples. The data suggest that complement analysis should be performed using the same type of blood specimen from the study cohort for comparison.
For research studies, blood samples are often drawn from study patients and then stored for a period before laboratory staff is available to process and bank the sample. Therefore, it is important to assess how temporary storage
after blood draw affects the study results. The data from this study suggest that complement factors are stable for a few hours prior to processing when blood is collected in either citrate or EDTA tubes and stored at RT or 4°C. However, when longer storage is anticipated prior to sample process-ing, EDTA blood is the preferred choice since it can keep complement factors largely stable for up to 8 hours at RT or 24 hours at 4°C.
In both clinical and research laboratories, samples are often collected, processed, and then frozen for later analysis. There is no standard procedure regarding how to thaw the specimen for complement study. Potentially, samples may be thawed on ice, at RT, or in a 37°C water bath. The length of thawing time is another factor likely affecting the study results. Our data suggest that when serum or citrate plasma is used for study, one should avoid using 37°C water baths to thaw the samples. Even with only a few minutes of incuba-tion at 37°C, there are significant increases of complement activation in both serum and citrate plasma, particularly for the components in alternative (factor Bb) and common/terminal pathways (C3a, C5a, C5b-9). In contrast, thawing in an RT water bath only minimally affects the test results as long as the samples are transferred in a timely manner on ice upon thawing. The complement factors in EDTA plasma are, however, relatively stable when samples are thawed at 37°C. In our study, the thawing conditions on ice were also evaluated and showed that the complement factors were not substantially affected when the samples were thawed and kept on ice for up to 3 hours.
The results from our study on the effect of freeze/thaw cycles suggest that complement factors in both alternative
❚Table 3❚Effect of Different Freeze/Thaw Cyclesa
Sample Type/Complement Biomarker
Sample Thawed on Ice Sample Thawed in Room Temperature Water Bath
2 Cycles 3 Cycles 4 Cycles 1 Cycle 2 Cycles 3 Cycles 4 Cycles
Citrate plasma C4d (279-1,846 ng/mL) 1.23 (0.16) 1.85 (1.36) 2.07 (1.53) 1.79 (0.58) 2.57 (1.38) 2.73 (1.32) 3.13 (1.43) Bb (244-961 ng/mL) 0.96 (0.03) 0.96 (0.02) 0.93 (0.06) 1.00 (0.08) 0.95 (0.08) 0.97 (0.02) 0.97 (0.03) C3a (7-242 ng/mL) 1.00 (0.03) 1.00 (0.07) 1.09 (0.04) 1.02 (0.02) 1.02 (0.05) 0.99 (0.06) 0.99 (0.09) C5a (19-48 ng/mL) 0.98 (0.09) 0.98 (0.06) 0.99 (0.07) 0.99 (0.05) 0.97 (0.09) 0.96 (0.07) 0.99 (0.06) C5b-9 (34-238 ng/mL) 0.98 (0.10) 0.96 (0.08) 1.18 (0.17) 1.03 (0.10) 1.10 (0.14) 1.18 (0.20) 1.15 (0.33)EDTA plasma C4d (279-1,846 ng/mL) 1.18 (0.30) 1.22 (0.28) 1.32 (0.37) 1.14 (0.23) 2.11 (0.92) 2.15 (0.70) 1.96 (0.72) Bb (244-961 ng/mL) 0.96 (0.09) 0.95 (0.02) 0.90 (0.05) 0.94 (0.05) 0.96 (0.05) 0.95 (0.06) 0.91 (0.03) C3a (7-242 ng/mL) 1.01 (0.11) 0.98 (0.14) 0.98 (0.06) 1.01 (0.15) 0.95 (0.10) 1.01 (0.10) 1.02 (0.05) C5a (19-48 ng/mL) 0.97 (0.10) 0.92 (0.13) 0.98 (0.04) 0.98 (0.02) 0.96 (0.03) 0.96 (0.02) 0.96 (0.08) C5b-9 (34-238 ng/mL) 1.03 (0.18) 1.05 (0.16) 1.16 (0.10) 0.91 (0.09) 1.06 (0.17) 1.08 (0.21) 1.12 (0.20)Serum C4d (279-1,846 ng/mL) 1.16 (0.12) 1.56 (0.36) 1.80 (0.47) 1.72 (0.48) 1.68 (0.42) 1.74 (0.23) 1.76 (0.54) Bb (244-961 ng/mL) 1.01 (0.02) 1.02 (0.03) 1.03 (0.06) 0.96 (0.14) 0.96 (0.12) 0.96 (0.10) 0.96 (0.06) C3a (7-242 ng/mL) 0.94 (0.03) 0.98 (0.02) 0.98 (0.10) 0.99 (0.07) 1.01 (0.05) 1.03 (0.05) 1.01 (0.14) C5a (19-48 ng/mL) 0.95 (0.04) 1.00 (0.02) 0.99 (0.01) 1.01 (0.09) 1.03 (0.11) 1.01 (0.09) 1.01 (0.02) C5b-9 (34-238 ng/mL) 1.05 (0.13) 1.15 (0.21) 1.37 (0.31) 1.07 (0.26) 1.16 (0.33) 1.21 (0.27) 1.26 (0.32)
a For comparison, all values are calculated as ratios to the results from the sample thawed once on ice. Values greater than 1.5 times of baseline values are shown in bold.

Yang et al / Preanalytical Effect on Complement Biomarker Tests
564 Am J Clin Pathol 2015;143:558-565 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
and terminal pathways are stable after as many as four freeze/thaw cycles for all three types of specimen. The clas-sic pathway component C4d is only marginally elevated upon the freeze/thaw process.
Many biological samples are stored long term in biore-positories. There are questions regarding how stable comple-ment factors are during the long-term storage at –80°C. Logistically, it is hard to set up an experiment to directly determine the effect of long-term storage on the integrity of the samples. Such study would involve the measurement of complement factors in the samples at the time of collection, store the samples for many years, and then measure the sam-ple again using the same method with an identical analyti-cal precision for comparison. To address this scientifically important issue in a feasible way, we examined the comple-ment biomarker levels in the banked samples from our TTP cohort. It is known that patients with acquired TTP exhibit
increased levels of complement activation at the time of an acute episode.11,12,25 Our data show that there is no apparent trend of increases in complement biomarker levels over time in samples stored at –80°C. The overall mean and distribu-tion of complement activation profiles do not vary signifi-cantly across the span of the past 6 years. The data strongly suggest that there is no significant complement activation in citrate plasma during long-term storage at –80°C. Although this study is not without limitations, it nevertheless clarifies, in the best way possible, an important issue regarding the impact of long-term sample storage on complement studies.
In summary, the analysis of complement biomarker lev-els is complex and subject to significant inaccuracies from sample collection and handling. Complement biomarker values in both research studies and the clinic should be interpreted carefully and in the context of all other available information. For both basic and clinical research, investiga-tors must handle the study samples correctly to adequately evaluate activity of the complement system.
1. Same type of blood samples (EDTA plasma, citrate plasma, or serum) must be used in the same research and clinical study for comparison.
2. For citrate plasma samples, blood drawn from study participants should be processed within 4 hours if stored at RT and within 3 hours if refrigerated to prevent possible in vitro activation of the complement pathway.
3. For EDTA plasma samples, blood can be temporarily stored at RT for up to 8 hours or at 4°C for 24 hours prior to processing.
4. We strongly recommend thawing frozen samples either in an RT water bath or on ice. Frozen serum and citrate plasma samples should never be thawed at 37°C to avoid in vitro activation of complement factors.
5. Samples are acceptable for assays of complement biomarkers in alternative and common/terminal pathways for up to four freeze/thaw cycles using a proper procedure.
6. Complement factors appear stable in citrated plasma when stored up to 6 years at –80°C.
Address reprint requests to Dr Wu: Dept of Pathology and Internal Medicine, The Ohio State University College of Medicine, 164 Hamilton Hall, 1645 Neil Ave, Columbus, OH 43210; [email protected].
This work was supported in part by a US government grant R01 FD003932 and the research grants from Alexion Corporation and Answering TTP foundation.
References 1. Lynch AM, Murphy JR, Byers T, et al. Alternative
complement pathway activation fragment Bb in early pregnancy as a predictor of preeclampsia. Am J Obstet Gynecol. 2008;198:385.e1-9.
1
2
2006
(n =
15)
2007
(n =
7)
2008
(n =
15)
2009
(n =
13)
2010
(n =
15)
2011
(n =
12)
2012
(n =
11)
C5b-9
Log
-Tra
nsfo
rmed
Co
mp
lem
ent
Bio
mar
ker
Leve
ls
2C5a
3
4C3a
3
4 Bb
3
4 C4d
❚Figure 2❚ The effect of long-term storage at –80°C on the measurement of complement biomarkers. The data of complement biomarkers from each year were log-transformed to meet normal distribution. The mean ± SD values are plotted for comparison.

AJCP / Original Article
Am J Clin Pathol 2015;143:558-565 565 DOI: 10.1309/AJCPXPD7ZQXNTIAL
© American Society for Clinical Pathology
2. Roumenina LT, Loirat C, Dragon-Durey MA, et al. Alternative complement pathway assessment in patients with atypical HUS. J Immunol Methods. 2011;365:8-26.
3. Chen M, Daha MR, Kallenberg CG. The complement system in systemic autoimmune disease. J Autoimmun. 2010;34:J276-J286.
4. Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med. 2009;361:1676-1687.
5. Ajona D, Pajares MJ, Corrales L, et al. Investigation of complement activation product c4d as a diagnostic and prognostic biomarker for lung cancer. J Natl Cancer Inst. 2013;105:1385-1393.
6. Karpman D, Tati R. Complement activation in thrombotic microangiopathy. Hamostaseologie. 2013;33:96-104.
7. Noris M, Mescia F, Remuzzi G. STEC-HUS, atypical HUS and TTP are all diseases of complement activation. Nat Rev Nephrol. 2012;8:622-633.
8. Kavanagh D, Goodship TH. Atypical hemolytic uremic syndrome, genetic basis, and clinical manifestations. Hematology. 2011;2011:15-20.
9. McKeage K. Eculizumab: a review of its use in paroxysmal nocturnal haemoglobinuria. Drugs. 2011;71:2327-2345.
10. Lapeyraque AL, Malina M, Fremeaux-Bacchi V, et al. Eculizumab in severe Shiga-toxin-associated HUS. N Engl J Med. 2011;364:2561-2563.
11. Reti M, Farkas P, Csuka D, et al. Complement activation in thrombotic thrombocytopenic purpura. J Thrombosis Haemost. 2012;10:791-798.
12. Westwood JP, Langley K, Heelas E, et al. Complement and cytokine response in acute thrombotic thrombocytopenic purpura. Br J Haematol. 2014;164:858-866.
13. Wu TC, Yang S, Haven S, et al. Complement activation and mortality during an acute episode of thrombotic thrombocytopenic purpura. J Thromb Haemost. 2013;11:1925-1927.
14. Chapin J, Weksler B, Magro C, et al. Eculizumab in the treatment of refractory idiopathic thrombotic thrombocytopenic purpura. Br J Haematol. 2012;157:772-724.
15. Jodele S, Licht C, Goebel J, et al. Abnormalities in the alternative pathway of complement in children with hematopoietic stem cell transplant–associated thrombotic microangiopathy. Blood. 2013;122:2003-2007.
16. Pickering MC, de Jorge EG, Martinez-Barricarte R, et al. Spontaneous hemolytic uremic syndrome triggered by complement factor H lacking surface recognition domains. J Exp Med. 2007;204:1249-1256.
17. Ariceta G, Besbas N, Johnson S, et al. Guideline for the investigation and initial therapy of diarrhea-negative hemolytic uremic syndrome. Pediatr Nephrol. 2009;24:687-696.
18. Noris M, Caprioli J, Bresin E, et al. Relative role of genetic complement abnormalities in sporadic and familial aHUS and their impact on clinical phenotype. Clin J Am Soc Nephrol. 2010;5:1844-1859.
19. Taylor GM, Richards S, Wade R, et al. Relationship between HLA-DP supertype and survival in childhood acute lymphoblastic leukaemia: evidence for selective loss of immunological control of residual disease? Br J Haematol. 2009;145:87-95.
20. Nilsson B, Ekdahl KN. Complement diagnostics: concepts, indications, and practical guidelines. Clin Dev Immunol. 2012;2012:962702.
21. Cataland SR, Holers VM, Geyer S, et al. Biomarkers of the alternative pathway and terminal complement activity at presentation confirms the clinical diagnosis of aHUS and differentiates aHUS from TTP. Blood. 2014;123:3733-3738.
22. Baatrup G, Sturfelt G, Junker A, et al. Effects of coagulation temperature on measurements of complement function in serum samples from patients with systemic lupus erythematosus. Ann Rheum Dis. 1992;51:892-897.
23. Mollnes TE, Garred P, Bergseth G. Effect of time, temperature and anticoagulants on in vitro complement activation: consequences for collection and preservation of samples to be examined for complement activation. Clin Exp Immunol. 1988;73:484-488.
24. Vladutiu AO, Winiarski BM. Complement C3 in serum and plasma, as measured by radial immunodiffusion with four commercial kits. Clin Chem. 1976;22:267-269.
25. Turner NA, Moake J. Assembly and activation of alternative complement components on endothelial cell-anchored ultra-large von Willebrand factor links complement and hemostasis-thrombosis. PLoS One. 2013;8:e59372.
26. Tati R, Kristoffersson AC, Stahl AL, et al. Complement activation associated with ADAMTS13 deficiency in human and murine thrombotic microangiopathy. J Immunol. 2013;191:2184-2193.
27. Pfeifer PH, Kawahara MS, Hugli TE. Possible mechanism for in vitro complement activation in blood and plasma samples: futhan/EDTA controls in vitro complement activation. Clin Chem. 1999;45(pt 1):1190-1199.
28. Sinosich MJ, Teisner B, Brandslund I, et al. Influence of time, temperature and coagulation on the measurement of C3, C3 split products and C4. J Immunol Methods. 1982;55:107-114.