
EEdE-89. PET-CT and MRI Unusual Findings of Perineural Tumor Spread in Head and Neck Cancer and...
31
eEdE-89
-
Upload
patricia-williamson -
Category
Documents
-
view
218 -
download
5
Transcript of EEdE-89. PET-CT and MRI Unusual Findings of Perineural Tumor Spread in Head and Neck Cancer and...

eEdE-89

PET-CT and MRI Unusual Findings of Perineural Tumor
Spread in Head and Neck Cancer and Review of the Literature
Bachir Zoghbi, Marques Bradshaw, Roshan Arjal, and M. Gisele Matheus

Conflict of Interests: None

Learning Points
•Definition of perineural tumor spread (PNTS)•Clinical Presentation• Imaging findings of distinct modalities•Usual and unusual patterns of PNTS• Treatment implications•Discussion
PNTS & PNI-Definition• Ability of a tumor to grow within and along nerve layers, away from the primary site, using
the nerve as a route of spread (metastatic process)
• Histologically, at a microscopic level, extension of tumor in the nerve compartments is called perineural invasion (PNI). The original definition of PNI by Batsakis is tumor cells in, around, and through the nerves which leads to some controversial interpretations
• Some pathologists define PNI as at least 33% of the circumference of the nerve surrounded by tumor to differentiate from focal abutment of the primary tumor, but the criteria to define small PNI near the primary tumor or spread through perineural tissue is still debatable
• Imaging wise ( CT, MRI , and PET-CT) identification of tumor within the nerve pathway is defined as PNTS

PNTS & PNI-Definition
• The tumor can invade any of the layers of the nerve (epineurium, perineurium, or endoneurium)
Tumor
Epineurium Perineurium
Endoneurium
• The tumor spread may be retro or antegrade and may not be detectable in its entire extension or pathway creating skip lesions

PNTS -Definition
Tumor
Tumor
Frank Netter- Atlas of Human Anatomy
Head & neck tumors
in any compartments, from skin to mucosal space,
may disseminate via
Direct invasion Hematogenic Lymphatic PNTS

• The mechanisms of dissemination remains incompletely understood
• Early theories• Direct invasion and spread through loose collagenous network of the nerve sheath• Lymphatic channels associated with the nerve
• Latest theories • Complex interaction between specific tumor cell types, supporting stroma, and nerves• Neurotrophic growth factors and axonal guidance molecules are involved• Increase activity of proteinases and increase expression of specific cell surface receptors
The earliest theories have fallen out of favor because there are no lymphatic network within the nerve sheath and perineurium actually creates a tight high resistance zone with multiple layers of collagen and basement membrane.
PNTS - Facts
• Theoretically any tumor can use this method of dissemination• Some tumors are more commonly associated to PNTS than others• SCCa (mucosal or cutaneous) shows significant number of PNTS due its high
prevalence• Adenoid cystic carcinoma is associated with PNTS in about 60% of cases• Mucoepidermoid carcinoma has a high association with PNTS• Melanoma, lymphoma, and even basal cell carcinoma had been reported in
isolated case reports
• PNI implies poor prognosis
PNTS -Facts

Clinical Findings
• More than two thirds can be asymptomatic • Those having symptoms may complain of pain, paresthesia,
numbness and motor weakness in the involved nerve distribution • As most involve the facial and the trigeminal nerve: facial paralysis,
trigeminal neuralgia, and masticator muscle weakness is common• In unusual cases, where the metastatic deposition is far from the
primary site, the clinical symptoms are usually underestimated

Imaging Findings
Direct• Abnormalities of the nerve and
adjacent structures
Indirect• Muscular asymmetry due to
denervation atrophy
• Accuracy of the PNTS identification increases with improving tissue contrast MRI>>>>>>>> CT
• Sensitivity and specificity of PET-CT is unknown, but brings metabolic information to the imaging assessment, which is identifiable in some cases even with size below the expected resolution of PET (about 8 mm)

Imaging Findings-CT
• Early, subtle imaging finding
• Loss of the fat attenuation in the neural foramen or expected neural pathway
Example: Axial Face CT image with contrast shows loss of normal fat attenuation in the right greater palatine foramen (arrow) in comparison to normal fat attenuation(arrowhead) on the left. Case of PNTS from right palate SCCa.

Imaging Findings-CT
• Late imaging finding• Asymmetric enlargement of the nerve
pathway filled by soft tissue mass which may or may not enhance
• Remodeling or erosion of the adjacent bone
Example: Face CT image with contrast shows enlargement of the right pterygopalatine fossa (arrowhead) occupied by abnormal soft tissue mass in comparison with normal appearance left pterygopalatine fossa (arrow). Case of PNTS from right tonsillar fossa SCCa.

• The intrinsic high tissue contrast of T1W sequences without fat suppression allows visualization of the affected nerve which is usually abnormally thick• Fat-suppressed T1WI with contrast easily
reveals the abnormally enhancing nerve (a finding that is not specific to PNTS but can also be seen with inflammatory processes)• T2WI may show asymmetrically abnormal
increased signal
Imaging findings-MRI
Examples of PNTS on T1WI with contrast and without fat-sat, show abnormally enlarged and enhancing V2(arrow) and V3 (arrowhead)

Imaging Findings-Challenge Case
• Patient with multiple previous small SCCasof the retroauricular skin with a new preauricular mass (arrow)
• All neural foramina appeared symmetrical And intact (not displayed in this picture)

Imaging Findings-Challenge Case
• PET-CT reveals hypermetabolic activity near the pterygoidplate, which was interpreted as artifactual given low level SUV in comparison to patient’s known tumor
• Retrospective assessment shows a 8 mm round, nonenhancing soft tissue mass(arrow) at the same locationof the subtle metabolic activity

Imaging Findings-Challenge Case
• 6 months latter, after resection and radiotherapy, MRI T1WI reveals PNTS with thickness of auriculotemporal nerve (arrow) and V3 (arrowhead)

Imaging Findings-Challenge Case
• MRI T1WI post contrast without fat-sat reveals PNTS (arrows) with thickness of theauriculotemporal nerve (left figure), cavernous sinus (center), and V2 within the foramen rotundum (right figure)
Although not strongly described in the current literature and limited to a few case series and case reports, PET-CT may reveal hypermetabolic activity in PNTS, even with small lesions that are close to the method’s lowest limits of resolution.
This particular case showed a skip lesion in the left mandibular segment of the 5th CN, as the earliest imaging findings of the PNTS. The lesion was visible on the PET-CT, and most likely the result of retrograde tumor dissemination through facial and auriculotemporal nerve.
The radiation coverage did not include the 5th CN and follow up MRI revealed retro and antegrade progression of the PNTS into the cavernous sinus and rotundum, respectively.
Challenge Case-Discussion

• Linear or round hypermetabolic activity in a nerve pathway• CT images may or may not show
asymmetric thickness of the nerve and destruction or remodeling of the adjacent structures
Example: Previously treated periauricular/scalp SCCa with parotid invasion and PNTS through facial and fifth cranial nerve with neck pain. PET-CT reveals hypermetabolic ativity along the cervical nerve root C3 (arrows)
Imaging Findings- PET-CT

Imaging Findings- Unusual Cases• MRI and PET correlation- same case of the previous slide
Cervical spine MRI axial T2WI (left), T1WI (center), and T1WI C+ (right) reveals, asymmetry of the longus colli muscles, left being smaller than right (arrowhead) with subtle thickness and post contrast enhancement (arrow).

• Diagram shows the presumable unusual, but feasible, pattern of PNTS discussed in the previous slide with skip lesions most likely via GA nerve or LO nerve to C2 and C3 nerve roots
Imaging Findings- Unusual Cases
C1
C2
C3
Great auricular nerve Lesser occipital nerve
Frank Netter- Atlas of Human Anatomy
C3
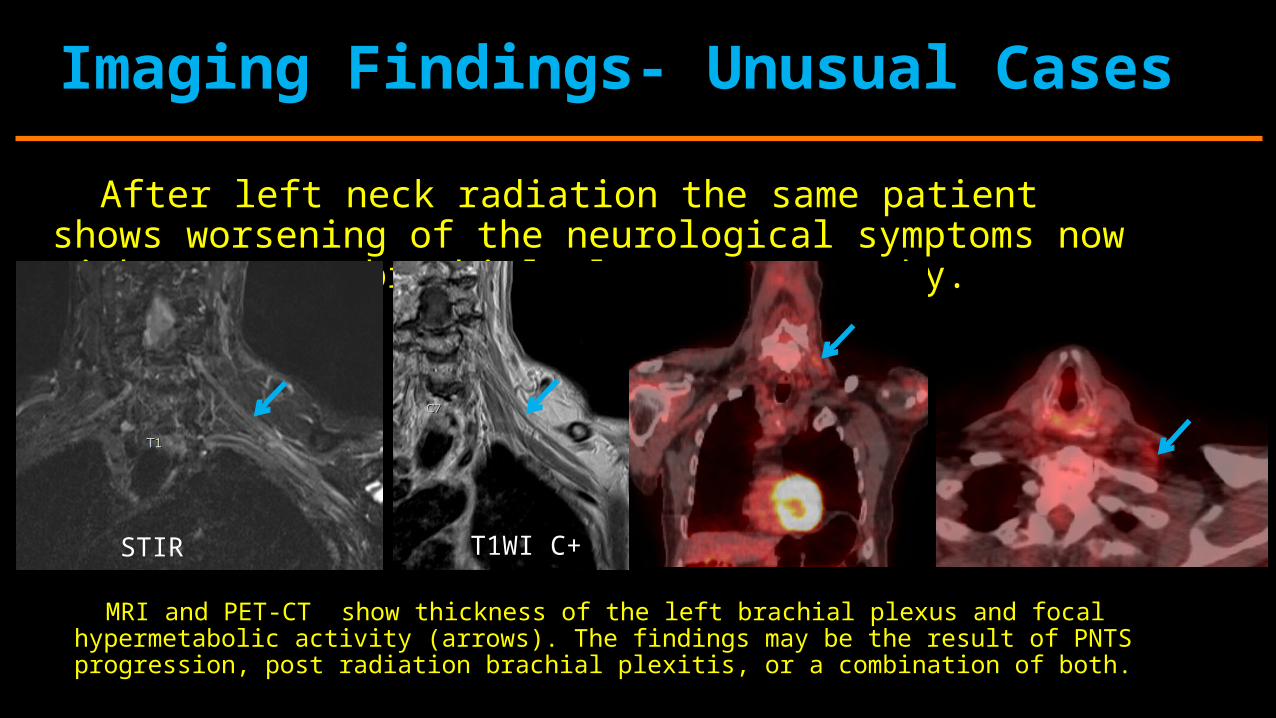
After left neck radiation the same patient shows worsening of the neurological symptoms now with apparent brachial plexus topography.
Imaging Findings- Unusual Cases
MRI and PET-CT show thickness of the left brachial plexus and focal hypermetabolic activity (arrows). The findings may be the result of PNTS progression, post radiation brachial plexitis, or a combination of both.
STIR T1WI C+

• Patient previously treated for right oral tongue SCCa shows interval recurrence in the left paraspinal muscles
Imaging Findings- Third Illustrative Case
• PET-CT reveals a mass lesion with hypermetabolic activity in the left paraspinal muscles (arrowhead) with linear hypermetabolic activity following the left cervical spine nerve root (arrow), which is most likely associated with PNTS

Imaging Findings- Third Illustrative Case
• Patient progressed with worsening neurological symptoms and MRI (T1WI C+) revealed leptomeningeal dissemination of the tumor via PNTS (arrows)
Treatment Implication
In these three patients with different distributions of PNTS over the course of their disease, the combination of varied imaging methods, such as PET-CT and MRI was a key factor for identification of the tumor deposition over the neural pathway and the treatment implications were distinct and markedly significant.• In the first case, change in the radiation coverage could potentially offer better
control of the PNTS, which showed rapid intracranial progression • In the second case, radiation treatment covering the PNTS area was immediately
initiated after PNTS identification• In the third case, leptomeningeal spread was suggested as a potential complication
during clinical discussion based on PET-CT images
Discussion
The last few decades have shown increased awareness of PNTS as
a potential route of metastatic dissemination. The most common pattern of PNTS through facial and trigeminal cranial nerve have been extensively demonstrated and discussed. The marked improvement of diagnostic imaging quality have allowed us to master cranial nerve anatomy and look for findings of tumor involvement. However, neuroradiologists have to keep in mind that this route of tumor dissemination may show uncommon alternative routes of spread that can also be identified with careful and meticulous evaluation of nerve pathways in the head and neck region.

Discussion
The hypermetabolic activity visible on PET-CT can be subtle and easily confused with artifact or pitfalls such as muscular activity, mis-registration, or vascular structure. Therefore, linear or punctate/round metabolic activity should be prudently evaluated as a potential site of PNTS. Anatomic and morphological review of the adjacent nerve pathways should be integrated in the imaging evaluation algorithm.
The accuracy of PET-CT for identification of PNTS is unknown. There are however, sporadic case reports and case series showing that detection of PNTS via PET-CT appears to be a feasible and most likely reliable. Therefore, further investigation for the sensitivity and specificity of PET-CT detection of PNTS, is necessary.

References1. Fabio M. Paes MADS, MD • Adam N. Checkver, MD, Ricardo A. Palmquist, MD • Gabriela De La Vega, MD • Charif Sidani, MD. Perineural Spread in Head and Neck Malignancies: Clinical Significance and Evaluation with 18F-FDG PET/CT1. Radiographics. 2013;33(6).
2. Chong CKOaVF-H. Imaging of perineural spread in head and neck tumours. 2010 International Cancer Imaging Society. 2010;10:S92-8.
3. Moonis G, Cunnane MB, Emerick K, Curtin H. Patterns of perineural tumor spread in head and neck cancer. Magnetic resonance imaging clinics of North America. 2012;20(3):435-46.
4. Santhosh Gaddikeri ABaYA. Perineural Invasion of Skin Cancers in the Head and Neck: An Uncommon Phenomenon Revisited. Otolaryngology. 2014;4(3).
5. Conrad GRMS, Partha MD; Holzhauer, Markus Perineural Spread of Skin Carcinoma to the Base of the Skull: Detection With FDG PET and CT Fusion. Clinical Nuclear Medicine. 2004;29(11).
6. Brea Alvarez B, Tunon Gomez M. Perineural spread in head and neck tumors. Radiologia. 2014;56(5):400-12.
7. Barrett AW, Speight PM. Perineural invasion in adenoid cystic carcinoma of the salivary glands: a valid prognostic indicator? Oral oncology. 2009;45(11):936-40.
8. Liebig C, Ayala G, Wilks JA, Berger DH, Albo D. Perineural invasion in cancer: a review of the literature. Cancer. 2009;115(15):3379-91.

References9.Chirila M, Bolboaca SD, Cosgarea M, Tomescu E, Muresan M. Perineural invasion of the major and minor nerves in laryngeal and hypopharyngeal cancer. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2009;140(1):65-9.10. Lee TJ, Glastonbury CM, Buckley AF, Eisele DW, Hawkins RA. Perineural spread of melanoma demonstrated by F-18 FDG PET With MRI and pathologic correlation. Clin Nucl Med. 2008;33(2):106-8.11. Santhosh Gaddikeri ABaYA. Perineural Invasion of Skin Cancers in the Head and Neck: An Uncommon Phenomenon Revisited. Otolaryngology. 2014;4(3).12. Maroldi R, Farina D, Borghesi A, Marconi A, Gatti E. Perineural Tumor Spread. Neuroimaging Clinics.18(2):413-29.13. Geoffrey D. Parker M, BS, FRACR H. Ric Harnsberger, M. Clinical-Radiologic Issues in Perineural Tumor Spread of Malignant Diseases of the Extracranial Head and Neck. Radiographics. 1991;11:383-9.14. Balink H, de Visscher JG, van der Meij EH. Recurrent head and neck desmoplastic melanoma with perineural spread along the nervus mandibularis revealed by 18F-FDG PET/CT. International journal of oral and maxillofacial surgery. 2014;43(8):941-3.15. Joshua E. Lane MMRW, MD†; David E. Kent, MD. Perineural Involvement of Squamous Cell Carcinoma Presenting With Formication. Psychocutaneous Medicine. 2010.;85.:121-3.

Thank you


















