
EDUCATIONAL WORKSHOPS 2009 CASE PRESENTATION THREE “He’s got another one, doctor” A difficult...
16
EDUCATIONAL WORKSHOPS 2009 CASE PRESENTATION CASE PRESENTATION THREE THREE “He’s got another one, doctor” A difficult case of recurrent MRSA bacteraemia Author: Nick Brown, Addenbrooke’s Hospital Acknowledgement: Sani Aliyu, Sandwell and West Birmingham Hospitals – now Addenbrooke’s Hospital Details of the original case report have been adapted to emphasise particular points
-
Upload
mariah-park -
Category
Documents
-
view
217 -
download
0
Transcript of EDUCATIONAL WORKSHOPS 2009 CASE PRESENTATION THREE “He’s got another one, doctor” A difficult...
EDUCATIONAL WORKSHOPS 2009
CASE PRESENTATION THREECASE PRESENTATION THREE
“He’s got another one, doctor” A difficult case of recurrent MRSA bacteraemia
Author: Nick Brown, Addenbrooke’s Hospital
Acknowledgement:Sani Aliyu, Sandwell and West Birmingham Hospitals – now Addenbrooke’s Hospital
Details of the original case report have been adapted to emphasise particular points

Sponsored through an unrestricted educational grant from Novartis Pharmaceutical Ltd to help support the
cost of developing and hosting this educational workshop series
Background65 y old male
Past history of hypertension and cerebro-vascular disease
July 2003
Aortic aneurysm and complications
Endovascular aortic aneurysm repair (EVAR)
post-operative bleed requiring laparotomy
paraparesis secondary to spinal cord ischaemia
long term suprapubic catheter
longstanding sacral pressure soresAuthor: Nick Brown, Addenbrooke’s Hospital
July 2007Admitted with fever four years after aneurysm repair
Blood cultures MRSA (isolate 1)
X-ray pelvis and transoesophageal echocardiogram (TOE) – normal
2 weeks iv vancomycin plus oral rifampicin, then stopped
Question:
What was the source of infection?
How would you have treated it?
Author: Nick Brown, Addenbrooke’s Hospital

July 20075 days later- pyrexia MRSA again in blood cultures (isolate 2)
Re-started vancomycin plus rifampicin for 4 weeks
Home on doxycycline plus rifampicin for a further 4 weeks
Author: Nick Brown, Addenbrooke’s Hospital

November 2007re-admitted with fever and back pain after 9 days at homeBlood cultures MRSA (isolate 3) Transthoracic echocardiogram (TTE) – normalMagnetic resonance imaging (MRI) spine - normalWCC scan suggestive of increased uptake in lower vertebra1 week vancomycin, then MIC for MRSA strain reported as 3 mg/Lintravenous linezolid for 10 days, then home on further 4 weeks oral
Author: Nick Brown, Addenbrooke’s Hospital
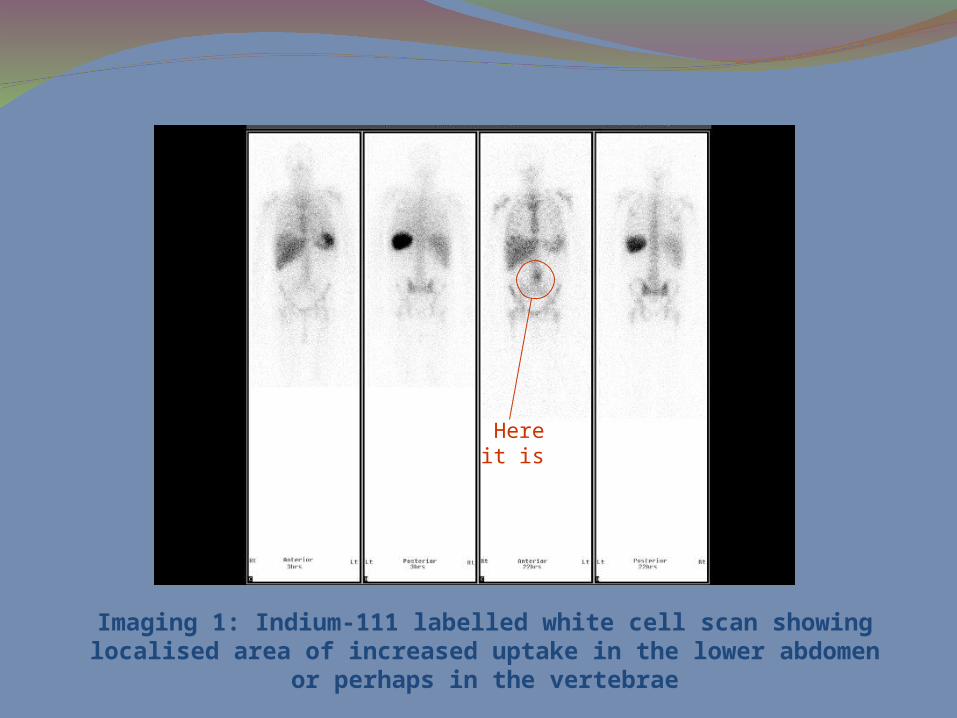
Imaging 1: Indium-111 labelled white cell scan showing localised area of increased uptake in the lower abdomen or perhaps in the vertebrae
Here it is
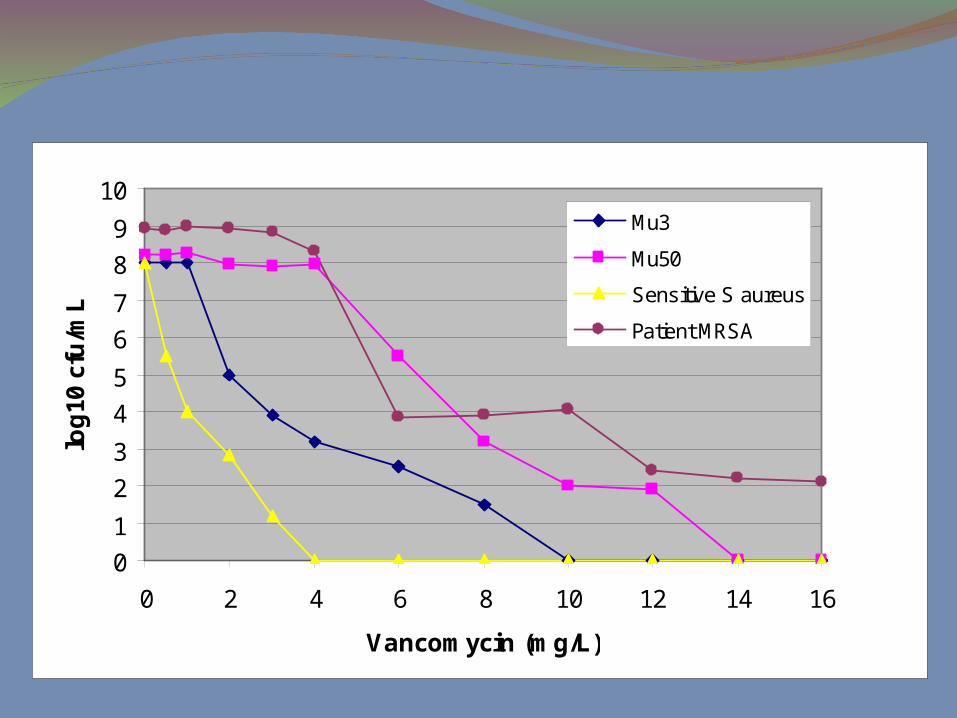
Population analysis of GISA
0
1
2
3
4
5
6
7
8
9
10
0 2 4 6 8 10 12 14 16
Vancomycin (mg/L)
log
10 c
fu/m
L
Mu3
Mu50
Sensitive S aureus
Patient MRSA
January 2008re-admitted in septic shock, day 38 linezolid
MRSA in blood (isolate 4)
intravenous daptomycin - five fold rise in CK, therefore stopped (was on a statin at the same time)
blood cultures MRSA (isolate 5)
Quinupristin/dalfopristin plus fusidic acid for 12 weeks
Author: Nick Brown, Addenbrooke’s Hospital
Late February 2008Blood cultures sterile by week 3 of quinupristin/dalfopristin plus
fusidic acid
inflammatory markers settling
Computerised axial tomography (CT) scan at week 7 – ‘increased thickness of aneurysm wall compared to previous scans’
Author: Nick Brown, Addenbrooke’s Hospital
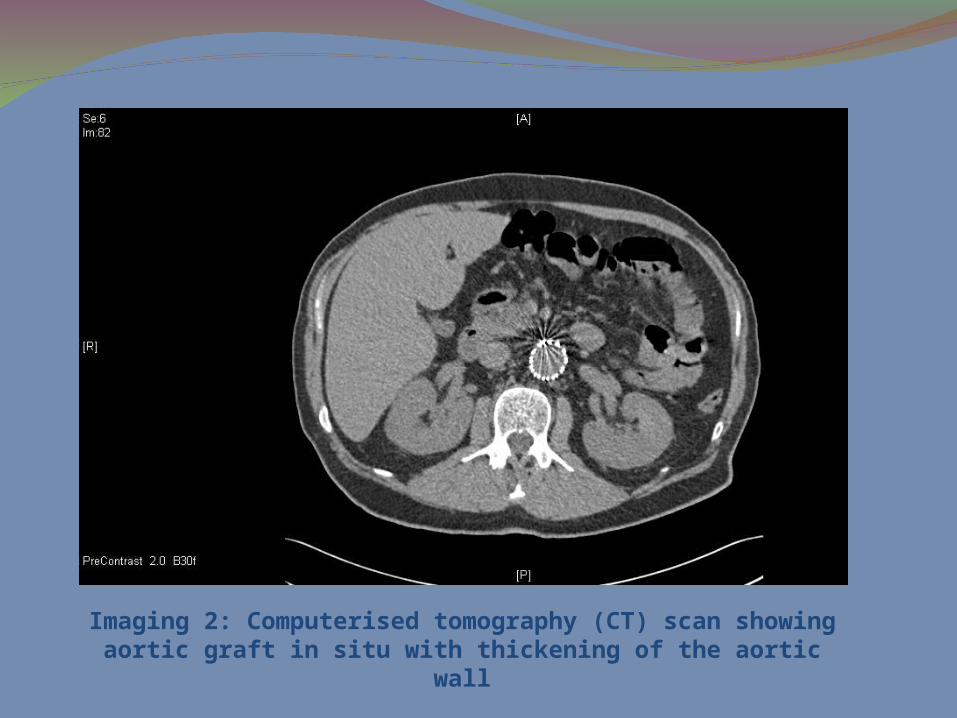
Imaging 2: Computerised tomography (CT) scan showing aortic graft in situ with thickening of the aortic wall
April 2008Cardiothoracic review - no surgical intervention indicated
11 weeks into quinupristin/dalfopristin treatmentseptic again ESBL-producing E. coli in urine and femoral line tipmeropenem for 10 daysquinupristin/dalfopristin discontinued end of 12 weeks
blood cultures just before quinupristin/dalfopristin stopped MRSA (isolate 6)
Author: Nick Brown, Addenbrooke’s Hospital
April 2008Quinupristin/dalfopristin re-started (1 week later) plus daptomycin
4mg/kg
CK levels remain normal
2 weeks - Quinupristin/dalfopristin switched to gentamicin and daptomycin dose increased to 10mg/kg
new femoral line
Author: Nick Brown, Addenbrooke’s Hospital
Mid-July 2008Gentamicin stopped after 4 weeks
MRSA bacteraemia persists (isolate 7)
8 weeks into daptomycin treatment - progressive rise in MIC
daptomycin MIC 0.125 mg/L initially, but peaked at 12.0 mg/L
Isolates now also resistant to rifampicin and fusidic acid
Positron emission tomography (PET) scan confirms aortic graft infection
Author: Nick Brown, Addenbrooke’s Hospital

Imaging 3: Positron emission tomography (PET) scan showing increased tracer activity in relation to the aortic graft
End-July 2008Aortic graft replacedCultures of graft are negative, but S. aureus identified by 16s rDNA
PCRGiven iv linezolid, then oral fosfomycin, doxycycline plus
chloamphenicol for 4 weeks
End-August 2008switched to oral doxycycline alone12 sets of blood cultures negative as at 1 Oct 2008
Author: Nick Brown, Addenbrooke’s Hospital


















