
Education - POCUS Journalpocusjournal.com/wp-content/uploads/2017/04/POCUS...Rapid Diagnosis of...
7
OCT 2016 vol. 01 iss. 03 Education Practice Research Editorial Board Emergency Department/FAST Dr. Joseph Newbigging, MD Dr. Louise Rang, MD Critical Care Dr. Suzanne Bridge, MD Anesthesiology Dr. Rob Tanzola, MD Dr. Rene Allard, MD Internal Medicine Dr. Barry Chan, MD Cardiology Dr. Amer Johri, MD Julia Herr, MSc Case Files: Rapid Diagnosis of Pericardial Effusion Case Reports: FAST Ultrasound Interpretation in Trauma Resuscitation Incarcerated femoral hernia containing ovary, unusual presentation of uncommon groin hernia ISSN: 23698543
Transcript of Education - POCUS Journalpocusjournal.com/wp-content/uploads/2017/04/POCUS...Rapid Diagnosis of...

OCT 2016 vol. 01 iss. 03
Education PracticeResearch
Editorial Board
Emergency Department/FASTDr. Joseph Newbigging, MDDr. Louise Rang, MD
Critical CareDr. Suzanne Bridge, MD
AnesthesiologyDr. Rob Tanzola, MDDr. Rene Allard, MD
Internal MedicineDr. Barry Chan, MD
CardiologyDr. Amer Johri, MDJulia Herr, MSc
Case Files:
Rapid Diagnosis of Pericardial Effusion
Case Reports:
FAST Ultrasound Interpretation in Trauma Resuscitation
Incarcerated femoral hernia containing ovary, unusual presentation of uncommon groin hernia
ISSN: 23698543
12 | POCUS J | OCT 2016 vol. 01 iss. 03
Visit the online article to view additional content from these cases: pocusjournal.com/article/20160103p12
Mr. DB was a 95 year old man who presented to the emer
gency department with dyspnea progressing over the last 3 months. Chest xray demonstrated an enlarged cardiac silhouette.
He had a past medical history significant for coronary artery disease, hypertension and a lobectomy due to tuberculosis.
A point of care cardiac ultrasound was conducted by an internal medicine resident as part of his physical examination in the emergency department. A large pericardial effusion was found. There were no clinical signs of tamponade.
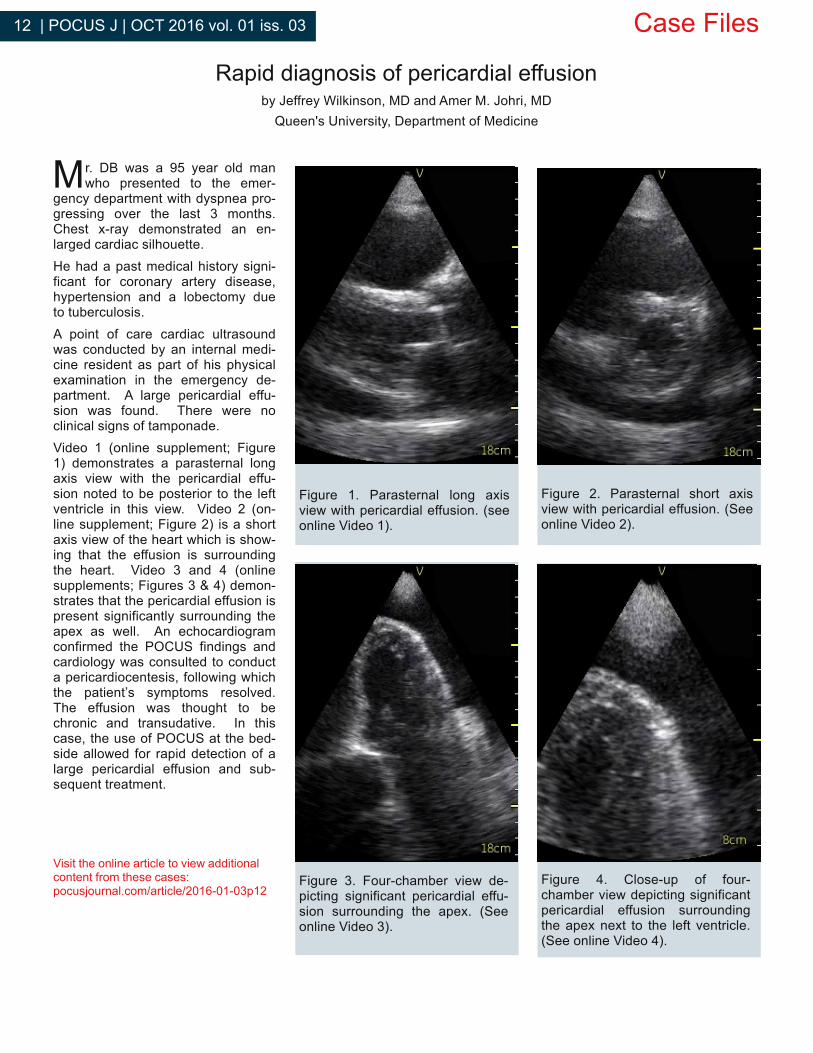
Video 1 (online supplement; Figure 1) demonstrates a parasternal long axis view with the pericardial effusion noted to be posterior to the left ventricle in this view. Video 2 (online supplement; Figure 2) is a short axis view of the heart which is showing that the effusion is surrounding the heart. Video 3 and 4 (online supplements; Figures 3 & 4) demonstrates that the pericardial effusion is present significantly surrounding the apex as well. An echocardiogram confirmed the POCUS findings and cardiology was consulted to conduct a pericardiocentesis, following which the patient’s symptoms resolved. The effusion was thought to be chronic and transudative. In this case, the use of POCUS at the bedside allowed for rapid detection of a large pericardial effusion and subsequent treatment.
Case Files
Rapid diagnosis of pericardial effusionby Jeffrey Wilkinson, MD and Amer M. Johri, MD
Queen's University, Department of Medicine
Figure 3. Fourchamber view depicting significant pericardial effusion surrounding the apex. (See online Video 3).
Figure 1. Parasternal long axis view with pericardial effusion. (see online Video 1).
Figure 2. Parasternal short axis view with pericardial effusion. (See online Video 2).
Figure 4. Closeup of fourchamber view depicting significant pericardial effusion surrounding the apex next to the left ventricle. (See online Video 4).
OCT 2016 vol. 01 iss. 03 | POCUS J | 13 Case Report
FAST ultrasound interpretation in trauma resuscitation
FAST Background
Focused Assessment with Sonography for Trauma (FAST) is an
integral adjunct to primary survey in trauma patients (14) and is incorporated into Advanced Trauma Life Support (ATLS) algorithms (4). A collection of four discrete ultrasound probe examinations (pericardial sac, hepatorenal fossa (Morison’s pouch), splenorenal fossa, and pelvis/pouch of Douglas), it has been shown to be highly sensitive for detection of as little as 100cm3 of intraabdominal fluid (4,5), with a sensitivity quoted between 6098%, specificity of 8498%, and negative predictive value of 9799% (3).. Further increasing sensitivity, ATLS recommends a repeat FAST exam in 30 minutes to increase sensitivity in slow bleeds, or early posttrauma presentations in the case that the first exam was negative (4). Recently, the Extended FAST (EFAST) exam has become standard and includes assessment for posttraumatic pneumothoraces (6).
With respect to trauma resuscitation, FAST exam offers the opportunity for quick, serial exams to identify potentially fatal conditions, including peritoneal free fluid and pericardial tamponade (1). It is indicated for the triage of blunt trauma patients (7) to direct decision making (1). In penetrating abdominal trauma FAST selects for patients requiring emergent exploratory laparotomy (5).
Case Summary
A 38year old male was transferred to a Level 1 Trauma Center from a peripheral Emergency Department. Approximately four hours prior he was a belted frontpassenger in a motor vehicle collision with intrusion to the passenger side at speeds approximately 50km/h. There was no loss of consciousness, but the patient endorsed sudden rightsided abdominal pain. Upon arrival at the
peripheral Emergency Department, the patient was tachycardic between 130150bpm, though hemodynamically stable. Primary survey identified right upper and lower abdomen tenderness, persistent tachycardia despite crystalloid resuscitation, and peritoneal free fluid on EFAST exam.
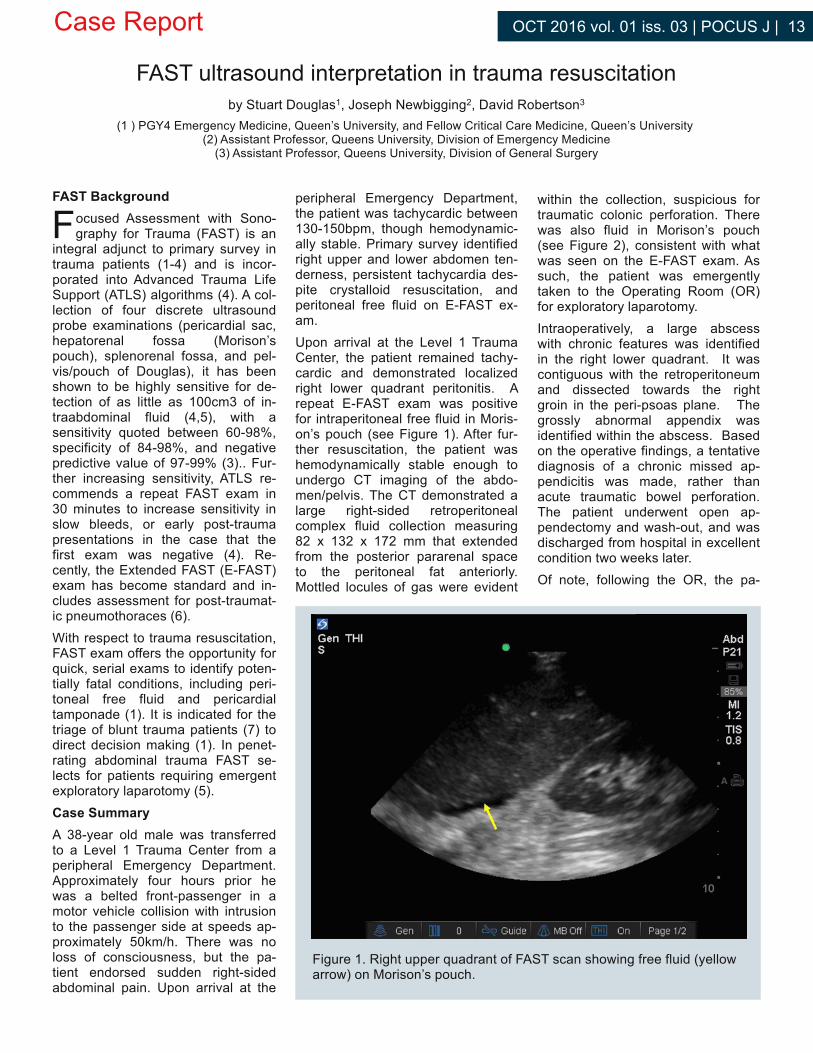
Upon arrival at the Level 1 Trauma Center, the patient remained tachycardic and demonstrated localized right lower quadrant peritonitis. A repeat EFAST exam was positive for intraperitoneal free fluid in Morison’s pouch (see Figure 1). After further resuscitation, the patient was hemodynamically stable enough to undergo CT imaging of the abdomen/pelvis. The CT demonstrated a large rightsided retroperitoneal complex fluid collection measuring 82 x 132 x 172 mm that extended from the posterior pararenal space to the peritoneal fat anteriorly. Mottled locules of gas were evident
by Stuart Douglas1, Joseph Newbigging2, David Robertson3
(1 ) PGY4 Emergency Medicine, Queen’s University, and Fellow Critical Care Medicine, Queen’s University (2) Assistant Professor, Queens University, Division of Emergency Medicine(3) Assistant Professor, Queens University, Division of General Surgery
within the collection, suspicious for traumatic colonic perforation. There was also fluid in Morison’s pouch (see Figure 2), consistent with what was seen on the EFAST exam. As such, the patient was emergently taken to the Operating Room (OR) for exploratory laparotomy.
Intraoperatively, a large abscess with chronic features was identified in the right lower quadrant. It was contiguous with the retroperitoneum and dissected towards the right groin in the peripsoas plane. The grossly abnormal appendix was identified within the abscess. Based on the operative findings, a tentative diagnosis of a chronic missed appendicitis was made, rather than acute traumatic bowel perforation. The patient underwent open appendectomy and washout, and was discharged from hospital in excellent condition two weeks later.
Of note, following the OR, the pa
Figure 1. Right upper quadrant of FAST scan showing free fluid (yellow arrow) on Morison’s pouch.

14 | POCUS J | OCT 2016 vol. 01 iss. 03
Visit the online article to view additional content from this case: pocusjournal.com/article/20160103p1314
tient reported that he had been assessed for right lower quadrant pain and diagnosed with a partial small bowel obstruction one month prior to this presentation. He reported ongoing abdominal pain and significant weight loss since that assessment. In retrospect, it was felt that his original smallbowel obstruction diagnosis was actually an ileus from acute appendicitis.
Limitations of FAST
EFAST exam has become an integral adjunct to trauma resuscitation. In skilled hands it is a powerful tool with ability to drastically improve patient outcomes. Although fast, noninvasive, and sensitive, EFAST examination should be interpreted skilfully. An appreciation for EFAST limitations and sensitivity is required for successful trauma resuscitation.
Of note, decreased sensitivity for intraabdominal injury has been linked to specific patient populations, including those with higher Injury Severity Scores (3), and hemodynamically stable patients with blunt abdominal injury (7). Negative FAST exams in these cohorts should be interpreted with caution, and consid
eration of further investigations or serial exams considered. Further recognized limitations include failure to identify retroperitoneal or solid organ injuries, failure to recognize clotted blood as hematoma, and difficult patient groups including those that are obese (8).
As portrayed in this case report, EFAST offers little ability to discern the specific fluid identified (8). Free fluid on EFAST could be blood, but could also be urine, ascites, bile, pus, peritoneal dialysate fluid, or bowel contents. In the setting of trauma, peritoneal free fluid must be considered blood, and the trauma patient resuscitated appropriately, with CT imaging as tolerated versus emergent exploratory laparotomy. This case illustrates an interesting example of a trauma patient’s EFAST exam that was falsely positive for blood in the peritoneum.
References1. Kool DR, Blickman JG. Advanced trauma life support. ABCDE from a radiological point of view. Emerg Radiol. 2007;14:135141.2. Jehle DVK, Stiller G, Wagner D. Sensitivity in detecting free intraperitoneal fluid with the pelvic views of the FAST exam. Am J Emerg med. 2003;21:476478. 3. Becker A, Lin G, McKenney MG, Marttos A, Schulman CI. Is the FAST exam reliable in severely injured patients? Injury. 2010;41(5):479483.4. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support for Doctors – ATLS Student Course Manual, Eighth Edition. Chicago: American College of Surgeons, 2008. Print. 5. Quinn AC, Sinert R. What is the utility of the Focused Assessment with Sonography in Trauma (FAST) exam in penetrating torso trauma? Injury. 2011;42:4824876. Kirkpatrick AW, Sirois M, Laupland KB, Liu D, Rowan K, Ball CG, Hameed SM, Brown R, Simons R, Dulchavsky SA, Hamiilton DR, Nicolaou S. Handheld thoracic sonography for detecting posttraumatic pneumothoraces: The Extrnded Focused Assessment with Sonography for Trauma (EFAST). The Journal of Trauma. 2004. 57;288295.7. Miller MT, Pasquale M, Bromberg WJ, Wasser T, Cox J. Not so Fast. The Journal of Trauma: Injury, Infection, and Critical Care. 2003;54(1):5260.8. Lewiss RE, Saul T, Del Rios M. “Focus on: EFAST – Extended Focused Assessment with Sonography for Trauma.” American College of Emergency Physicians – Clinical & Practice Management. American College of Emergency Physicians. Jan, 2009. Web June 13, 2016.
Figure 2. Axial image CT abdomen demonstrating free fluid to Morison’s pouch.

OCT 2016 vol. 01 iss. 03 | POCUS J | 15 Case Report
Incarcerated femoral hernia containing ovary, unusual presentation of uncommon groin hernia
by Priyank Gupta, MD, FRCR1; Hadiel Kaiyasah, MRCS Glasgow2; Mahra AlSuwaidi, MRCS Glasgow2
(1) Dubai health authority, Rashid hospital, radiology department, UAE.(2) Dubai health authority, Rashid hospital, general surgery department, UAE.
Of all groin hernias, femoral hernias account for around 2–8%.
They occur four to five times more commonly in females than males and have a peak incidence in those between 30 and 60 years old [1,2]. In adult population, femoral hernias are more commonly found in patients with previous inguinal hernia repair [3]. We present an unusual case of a 28 yearold woman who presented to our institution with an incarcerated femoral hernia containing the right ovary & fallopian tube occurring after inguinal hernia repair. The point of care ultrasound that was done in the emergency department had helped in prompt diagnosis of the condition, hence sending the patient to operation theatre for urgent surgical intervention.
Case Presentation: A 28yearold female presented to the emergency department with a sudden onset of abdominal pain in the right iliac fossa and suprapubic area. The pain was dull, mild to moderate in severity with no radiation. Patient gave history of chronic right groin swelling that was reducible for the last 2 months. Prior to presentation to accident & emergency department, she developed an irreducible swelling. There was no associated vomiting or constipation. Of note in her surgical history was significant for Left inguinal hernia repair ten years ago. She was normotensive and afebrile at presentation. Examination revealed a scar in the left inguinal region. Her abdomen was soft. There was an irreducible firm tender lump palpated below the level of the right inguinal ligament and lateral to the pubic tubercle.
Investigations: All her laboratory tests were within normal limits. The patient was reviewed by the surgical oncall doctor who made the provisional diagnosis of irreducible right femoral hernia based on the clinical
examination. Initially a point of care ultrasound (POCUS) was done by the attending surgical doctor, who was able to appreciate a localized cystic swelling within the hernia sac. A departmental Ultrasonography of the right groin area was obtained to confirm the findings of POCUS. It revealed a welldefined rounded soft tissue echogenicity lesion with a well defined cystic component containing no internal septations or mural nodules. The lesion was located subcutaneously anterior & medial to the femoral vein & reaching medially up to the level of pubic symphysis with no obvious intraabdominal extension (Figure 1A). The lesion was not reducible and did not change in the size on Valsalva maneuver or cough impulse. No evidence of any peristalsis or free fluid noted within contents of the swelling. Color Doppler imaging revealed central branching pattern of vascularity consistent with ovarian vasculature pattern (Figure 1B). The ultrasound findings were in keeping with right femoral hernia with the ovary within the hernia sac.
Treatment: The patient was admitted under the care of the general surgery team with provisional diagnosis of an incarcerated right femoral hernia with a plan for urgent laparoscopic repair of the right femoral hernia. Intraoperatively, exploration revealed no fluid in the abdomen and no signs of bowel obstruction. A hernia sac was present protruding down towards the femoral canal. The contents were reduced & found to be the ovary and fallopian tube (online Figure S1). Both structures were looking viable. The anatomy of the area was clarified and dissected reaching to the pubic tubercle medially and the inguinal ligament superiorly and laterally. A prolene mesh was applied and fixed using endoscopic clips (takar). The peritoneum was closed and the abdomen deflated.
Outcome and FollowUp: Patient was doing well postoperatively and responded well to the planned management. She had an uneventful recovery and was discharged home on the next day. Follow up after 6 weeks revealed no complication.
Discussion: The anatomical location of the ovaries and fallopian tube at a level below femoral ring makes herniation of these structures through it unusual, particularly in adults [4]. According to the most acceptable theory, the primary cause for the formation of femoral hernia is a congenitally narrow posterior inguinal wall attachment onto Cooper’s ligament with a resultant enlarged femoral ring, while the secondary aetiology is a state of prolonged and increased intraabdominal pressure, which forces preperitoneal fat into the congenitally large femoral ring [1,5,6]. However, it should be noted that in younger ages with femoral hernias, processes responsible for elevated intraabdominal pressure are rarely encountered. Due to the rigid ligamentous borders & relatively narrow lumen, incarceration occurs more frequently in femoral hernias than other abdominal hernias [7,8]. The incidence of recurrent femoral hernia occurring after inguinal herniorraphy has been reported to be up to 35% [8]. The increased incidence of femoral hernia after inguinal herniorraphy may be due to an overlooked hernia or a new spontaneous hernia due to weakening of the femoral region caused by inguinal herniorraphy [8,9]
Femoral hernias typically present as a painless or painful groin lump, although may present simply as groin pain or with features of their complications such as obstruction. The differential diagnoses include inguinal hernia, lipoma, saphena varix, enlarged lymph nodes, femoral artery

16 | POCUS J | OCT 2016 vol. 01 iss. 03
aneurysm, sarcoma, obturator hernia, psoas abscess, psoas bursa, and in males, ectopic testis [4,10]. Different contents in femoral hernias have been reported in the literature, such as small intestine, omentum, bladder, cecum, colon, appendix (what is known as De Garengeot’s hernia), Meckel’s diverticulum (Littre hernia), testis, ovary, and even stomach or kidney [11,12].
The preoperative diagnosis of femoral hernia is a challenging issue. In previous reports, the clinical diagnostic accuracy ranged from 25% to 40% [13]. The ovary is quite sensitive to ischemia [14,15]. Should it tort or become incarcerated in a femoral hernia sac, a delay in diagnosis may necessitate its resection [16]. Imaging studies could prove to be a valuable preoperative investigation in women of childbearing age presenting with femoral hernia. Nowadays POCUS is a valuable tool in the initial assessment of irreducible hernia cases, whether performed by the emergency physician or the attending surgeon. The most important points to keep in mind while performing POCUS are:
• Femoral hernia is visualized as a subcutaneous swelling in contact with the femoral vein.
• Assess the contents of hernia sac, whether loop of bowel within or a cystic swelling (e,g ovary like in our case).
• In cases where bowel loops are within a hernia sac, observe for signs of strangulation, such as oedematous bowel wall or absent peristalsis.
Doppler ultrasound may identify reduced blood flow in ovaries suggestive of torsion. Crosssectional
imaging with CT may be similarly beneficial in identifying a groin hernia containing an ovary provided it causes no delay in the timing of surgery [17].
Operative management of an incarcerated femoral hernia containing an ovary follows the same surgical principles for femoral hernia repair. Intraoperative Reduction of the sac content should be attempted in reproductive young woman and children without any ovarian and tubal abnormalities [18], provided that any lifethreatening complication such as acute salpingitis does not exist [19]. If the ovary can't be preserved due to inviability, a salpingooophorectomy is to be undertaken. Hernia repair could be done via mesh plug repair, which is considered to have the lowest recurrence rate [1].
Conclusion: Incarcerated femoral hernia containing ovary, is an unusual presentation of uncommon groin hernia. The point of care ultrasound that was done in the emergency department had helped in prompt bedside clinical diagnosis of the condition, hence early urgent surgical intervention & better outcome.
Visit the online article to view additional content from this case: pocusjournal.com/article/20160103p1516
hernia. Ann Surg 1961; 154(6):2532.7. Ichinokawa M, Okada T, Sasaki F. Incarcerated femoral hernia with ovary and fallopian tube torsion in an infant: a rare occurrence. Pediatr Surg Int 2008; 24:1149–51. 8. Ludington LG. Femoral Hernia and Its Management: With Particular Reference to Its Occurrence Following Inguinal Herniorrhaphy. Ann Surg 1958; 148(5):823826.9. Glassow F. Recurrent inguinal and femoral hernia. Brit Med J 1970; 1(5690):215216.10. Alzaraa A. Unusual contents of the femoral hernia. ISRN Obstet Gynecol 2011; 2011:717924. 11. Zacharakis E. An unusual presentation of Meckel diverticulum as strangulated femoral hernia. South Med J 2008; 101:9698.12. Marioni P. Metastatic carcinoma with small intestine in a femoral hernia. Can Med Assoc J 1960; 82:10811082.13. AlShanafey S, Giacomantonio M. Femoral hernia in children. J Pediatr Surg 1999; 34:11041106. 14. Anders JF, Powell EC. Urgency of evaluation and outcome of acute ovarian torsion in pediatric patients. Arch Pediatr Adolesc Med 2005; 159:53255.15. Yamashita Y, Sowter M, Ueki M, et al. Adnexal torsion. Aust N Z J Obstet Gynaecol 1999; 39:1747.16. Gurer A, Ozdogan M, Ozlem N, et al. Uncommon content in groin hernia sac. Hernia 2006; 10:1525.17. Suzuki S, Furui S, Okinaga K, et al. Differentiation of femoral versus inguinal hernia: CT findings. AJR Am J Roentgenol 2007; 189:W78–83.18. Amarin ZO, Hart DM. Inguinal ovary and fallopian tube—an unusual hernia. Int J Gynaecol Obstet 1988; 27:141143.19. Roth CG, Varma JD, Tello R. Gastrointestinal/genitourinary case of the day. Incarcerated inguinal hernia of the left fallopian tube and ovary. AJR Am J Roentgenol 1999; 173:787, 791792.
References:1. Hachisuka T. Femoral hernia repair. Surg Clin North Am 2003; 83:1189–205. 2. Lytle WJ. Inguinal anatomy. J Anat 1979; 128(Pt 3):581–94. 3. Mikkelsen T, BayNielsen M, Kehlet H. Risk of Femoral hernia after inguinal herniorrhaphy. Br J Surg 2002; 89:486488.4. King R. Congenital, strangulated femoral hernia in an infant aged six months containing the ovary and fallopian tube. Br J Clin Pract 1978; 32(7):209–210.5. Dahlstrand U, Wollert S, Nordin P, et al. Emergency femoral hernia repair: a study based on a national register. Ann Surg 2009; 249(4):672–676. 6. McVay CB, Savage LE. Etiology of femoral
Figure 1. Transverse view of the ultrasound scan of the groin swelling revealed ovary lying anterior & medial to the femoral vein

OCT 2016 vol. 01 iss. 03 | POCUS J | 17
About Us
Physicians, Researchers, and Educators are invited to contribute articles to upcoming issues of POCUS Journal.
Types of Contributions:
Case Files: short communications of a single cases that highlight the utility of pointofcare ultrasound.
Case Reports: longer communications of a single cases that highlight the utility of pointofcare ultrasound.
Letters: short communications on the topics of research, education, or editorials focused on pointofcare ultrasound.
There are no costs associated with publication in POCUS Journal. For detailed information, visit pocusjournal.com/about/instructionstoauthors.
For inquiries or proposed topics, please contact the editors at [email protected].
Call for Submissions
POCUS Journal is dedicated to the advancement of research and the promotion of education in the field of vascular medicine.
POCUS journal is a publication of VascNet, and can be found online at pocusjournal.com
As a publication of VascNet, you can receive email updates when a new issues is available by subscribing to the VascNet email newsletter. Visit pocusjournal.com/subscribe/
To submit your case study or letter for publication in POCUS Journal, visit pocusjournal.com/submit
POCUS Journal is a publication of VascNet
VascNet is a research network researchers, clinicians, and experts in the field of cardiovascular medicine.
Visit us at vascnet.com to learn more.
VascNet94 Stuart St., Kingston, ON Canada, K7L 3N6
ISSN: 23698543
The online version of the OCT 2016 issue of POCUS Journal is available at pocusjournal.com/issue/vol01iss032016 and includes additional media and images from the case studies.












![Challenges in Management of Pericardial Effusion in ... · [5,6]. It has been demonstrated that cardiac tamponade, a serious hemodynamic medical emergency as a result of pericardial](https://static.fdocuments.us/doc/165x107/5ceb108588c993886b8bfeff/challenges-in-management-of-pericardial-effusion-in-56-it-has-been-demonstrated.jpg)





