Introduction to Virtualization Lewis Talley – InSource Solutions.
GI EpidemiologySECOND EDITION
Diseases and Clinical Methodology
Edited by Nicholas J. Talley G. Richard Locke III Paul Moayyedi
Joe West Alexander C. Ford Yuri A. Saito
with
website
GI Epidemiology
GI EpidemiologyDiseases and Clinical MethodologySecond Edition
Edited by
Nicholas J. Talley, MD, PhD, M Med Sci (Clin Epi), FRACP,FAFPHM, FRCP, FACP, FACG, AGAFPro Vice-Chancellor and Dean (Health and Medicine), and ProfessorSenior Staff Specialist (Gastroenterology), John Hunter HospitalUniversity of NewcastleCallaghan, NSW, Australia
G. Richard Locke III, MDProfessor of MedicineGI Epidemiology/Outcomes UnitDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
Paul Moayyedi, BSc, MB ChB, PhD, MPH, FRCP, FRCPC,AGAF, FACGActing Director of the Farncombe Family Digestive Health Research InstituteDirector of Division of GastroenterologyMcMaster UniversityHamilton, ON, Canada
Joe West, BMedSci, BM BS, MRCP, MSc, PhD, PGDipAssociate Professor and Reader in Epidemiology; Honorary Consultant GastroenterologistDivision of Epidemiology and Public HealthUniversity of NottinghamNottingham, UK
Alexander C. Ford, MBChB, MD, FRCPAssociate Professor and Honorary Consultant GastroenterologistLeeds Teaching Hospitals TrustLeeds, West Yorkshire, UK
Yuri A. Saito, MD, MPHAssistant Professor of MedicineDirector, GI Epidemiology/Outcomes UnitDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
This edition first published 2014 C© 2014 by John Wiley & Sons, Ltd; 2007 by Blackwell PublishingRegistered office: John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex,
PO19 8SQ, UK
Editorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USA
For details of our global editorial offices, for customer services and for information about how to applyfor permission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwell
The right of the author to be identified as the author of this work has been asserted in accordance withthe UK Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording orotherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without the priorpermission of the publisher.
Designations used by companies to distinguish their products are often claimed as trademarks. Allbrand names and product names used in this book are trade names, service marks, trademarks orregistered trademarks of their respective owners. The publisher is not associated with any product orvendor mentioned in this book. It is sold on the understanding that the publisher is not engaged inrendering professional services. If professional advice or other expert assistance is required, the servicesof a competent professional should be sought.
The contents of this work are intended to further general scientific research, understanding, anddiscussion only and are not intended and should not be relied upon as recommending or promoting aspecific method, diagnosis, or treatment by physicians for any particular patient. The publisher and theauthor make no representations or warranties with respect to the accuracy or completeness of thecontents of this work and specifically disclaim all warranties, including without limitation any impliedwarranties of fitness for a particular purpose. In view of ongoing research, equipment modifications,changes in governmental regulations, and the constant flow of information relating to the use ofmedicines, equipment, and devices, the reader is urged to review and evaluate the information providedin the package insert or instructions for each medicine, equipment, or device for, among other things,any changes in the instructions or indication of usage and for added warnings and precautions. Readersshould consult with a specialist where appropriate. The fact that an organization or Website is referredto in this work as a citation and/or a potential source of further information does not mean that theauthor or the publisher endorses the information the organization or Website may provide orrecommendations it may make. Further, readers should be aware that Internet Websites listed in thiswork may have changed or disappeared between when this work was written and when it is read. Nowarranty may be created or extended by any promotional statements for this work. Neither thepublisher nor the author shall be liable for any damages arising herefrom.
Library of Congress Cataloging-in-Publication Data
GI epidemiology : diseases and clinical methodology / edited by Nicholas J. Talley, G. Richard LockeIII, Paul Moayyedi, Joe West, Alexander C. Ford, Yuri A. Saito. – Second edition.
p. ; cm.Includes bibliographical references and index.ISBN 978-0-470-67257-0 (hardback : alk. paper) – ISBN 978-1-118-72707-2 – ISBN
978-1-118-72708-9 (ePdf) – ISBN 978-1-118-72709-6 (ePub) – ISBN 978-1-118-72710-2 (mobi)I. Talley, Nicholas Joseph, editor of compilation. II. Locke, G. Richard, III, editor of
compilation. III. Moayyedi, Paul, editor of compilation. IV. West, Joe, editor of compilation.V. Ford, Alexander C., editor of compilation.
[DNLM: 1. Gastrointestinal Diseases–epidemiology. 2. Epidemiologic Methods. WI 140]RC801616.3′3–dc23
2013018951
A catalogue record for this book is available from the British Library.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in printmay not be available in electronic books.
Cover design by Nathan Harris
Set in 9/11.5pt Sabon by Aptara Inc., New Delhi, India
1 2014
http://www.wiley.com/wiley-blackwell
Contents
Contributors, viii
Foreword, xiv
Preface, xv
About the companion website, xvi
Part 1: Gastrointestinal Diseases and Disorders: The PublicHealth Perspective
1 The Burden of Gastrointestinal and Liver Disease Around the World, 3Hannah P. Kim, Seth D. Crockett, & Nicholas J. Shaheen
Part 2: How to Critically Read the GastrointestinalEpidemiology Literature
Introduction and Overview, 17Joe West
2 How to Read a Cohort Study, 18Laila J. Tata
3 How to Read a Case-Control Study, 30Joe West, Laila J. Tata, & Timothy R. Card
4 How to Read a Randomized Controlled Clinical Trial, 39Matthew J. Grainge
5 How to Read a Systematic Review and Meta-Analysis, 48Alexander C. Ford & Paul Moayyedi
6 How to Decide if Any of This Matters, 58Kate M. Fleming & Timothy R. Card
Part 3: How to Do Clinical Research in GI
7 How to Develop and Validate a GI Questionnaire, 67Enrique Rey & G. Richard Locke III
8 How to Do Population-Based Studies and Survey Research, 75Sanjiv Mahadeva & Hematram Yadav
9 How to Find and Apply Large Databases for Epidemiologic Research, 83Jonas F. Ludvigsson, Joe West, Jessica A. Davila, Timothy R. Card, &
Hashem B. El-Serag
10 How to Do Genetic and Molecular Epidemiologic Research, 98Yuri A. Saito
v
CONTENTS
11 Diagnostic Studies, 106Paul Moayyedi
12 Randomized Controlled Trials, 113Paul Moayyedi & Richard H. Hunt
Part 4: Epidemiology of Major GI Diseases
13 Epidemiology of GERD, Barrett’s Esophagus and Esophageal Cancer, 121David Armstrong
14 Epidemiology of Helicobacter Pylori Infection, Peptic Ulcer Disease andGastric Cancer, 135Grigorios I. Leontiadis & Olof Nyrén
15 Epidemiology of Dyspepsia, 158Alexander C. Ford & Nicholas J. Talley
16 Epidemiology of Upper Gastrointestinal Bleeding, 172Colin J. Crooks, Joseph Sung, & Timothy R. Card
17 Epidemiology of Celiac Disease, 185Alberto Rubio-Tapia, Jonas F. Ludvigsson, & Joseph A. Murray
18 Measuring Utilization of Endoscopy in Clinical Practice, 196Frances Tse & Alan Barkun
19 Epidemiology of Colorectal Carcinoma, 213Harminder Singh, Joselito M. Montalban, & Salaheddin Mahmud
20 Epidemiology of Irritable Bowel Syndrome, 222Rok Seon Choung & Yuri A. Saito
21 Epidemiology of Constipation, 235Brian E. Lacy & John M. Levenick
22 Epidemiology of Diverticular Disease, 249Robin Spiller & David Humes
23 Epidemiology of Infectious Diarrhea, 262Christina M. Surawicz & Crenguta Stepan
24 Epidemiology of Inflammatory Bowel Disease, 273Edward V. Loftus, Jr.
25 Epidemiology of Fecal Incontinence, 285Adil E. Bharucha
26 Epidemiology of Gallstones and Biliary Tract Cancers, 296Guy D. Eslick & Eldon A. Shaffer
27 Epidemiology of Pancreatitis, 306Dhiraj Yadav, Santhi Swaroop Vege, & Suresh T. Chari
28 Epidemiology of Pancreatic Cancer, 313Aravind Sugumar & Santhi Swaroop Vege
29 Epidemiology of Hepatitis B and C in the United States, 322Sumeet K. Asrani & W. Ray Kim
vi
CONTENTS
30 Epidemiology of Alcoholic Liver Disease, 332Sumeet K. Asrani & William Sanchez
31 Epidemiology of Cirrhosis and Hepatocellular Carcinoma, 344Joe West & Guruprasad P. Aithal
32 Epidemiology of Nonalcoholic Fatty Liver Disease (NAFLD), 357Guruprasad P. Aithal, Kshaunish Das, & Abhijit Chowdhury
33 Epidemiology of Common Tropical GI Diseases, 373Magnus Halland, Rodney Givney, & Anne Duggan
34 Nutritional Epidemiology and GI Cancers, 383Linda E. Kelemen & Ilona Csizmadi
35 The Epidemiology of Obesity Among Adults, 394Cynthia L. Ogden, Brian K. Kit, Tala H.I. Fakhouri, Margaret D.
Carroll, & Katherine M. Flegal
Index 405
vii
Contributors
Guruprasad P. Aithal, BSc, MBBS, MD,FRCP, PhD
Co-Director, NIHR Nottingham Digestive DiseasesBiomedical Research Unit
Nottingham University Hospitals NHS Trust andUniversity of Nottingham
Nottingham, UK
David Armstrong, MA, MB BChir, FRCP, FRCPC,AGAF, FACG
Professor of MedicineFarncombe Family Digestive Health Research
Institute & Division of GastroenterologyMcMaster UniversityHamilton, ON, Canada
Sumeet K. Asrani, MDHepatologyBaylor University Medical CenterDallas, TX, USA
Alan Barkun, MD, MScDivision of GastroenterologyMontreal General Hospital SiteThe McGill University Health CentreMontreal, QC, Canada
Adil E. Bharucha, MDProfessor of MedicineDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
Timothy R. Card, PhD, FRCPAssociate Professor and Honorary Consultant
GastroenterologistDivision of Epidemiology and Public HealthNottingham City HospitalUniversity of NottinghamNottingham, UK
Margaret D. Carroll, MSPHDivision of Health and Nutrition
Examination SurveysNational Center for Health StatisticsCenters for Disease Control and PreventionHyattsville, MD, USA
Suresh T. Chari, MDProfessor of MedicineDivision of Gastroenterology and
HepatologyMayo Clinic College of MedicineRochester, MN, USA
Rok Seon Choung, MD, PhDDepartment of Internal MedicineInstitute of Digestive Diseases and NutritionKorea UniversitySeoul, South Korea
Abhijit Chowdhury, MBBS, MD, DMDivision of HepatologySchool of Digestive and Liver DiseasesIPGME & R, Kolkata, India
Seth D. Crockett, MD, MPHAssistant Professor, Division of
GastroenterologyUniversity of North Carolina School
of MedicineUniversity of North Carolina at
Chapel HillChapel Hill, NC, USA
Colin J. CrooksDivision of Epidemiology and
Public HealthNottingham City HospitalUniversity of NottinghamNottingham, UK
viii
CONTRIBUTORS
Ilona Csizmadi, MSc, PhDResearch Scientist, Department of Population
Health ResearchAlberta Health Services-Cancer CareDepartments of Community Health Sciences
and OncologyFaculty of MedicineUniversity of CalgaryCalgary, AB, Canada
Kshaunish Das, MBBS, MD, DMDivision of GastroenterologySchool of Digestive and Liver DiseasesIPGME & R, Kolkata, India
Jessica A. Davila, PhDAssociate Professor of MedicineProgram Chief, Health Services Research
Methodology and Statistics CoreBaylor College of MedicineMichael E. DeBakey VA Medical CenterHouston, TX, USA
Anne Duggan, PhD, FRACP,B.Med, MHP
Conjoint ProfessorDepartment of GastroenterologyJohn Hunter HospitalNewcastle, NSW, Australia
Hashem B. El-Serag, MD, MPHChief, Gastroenterology and HepatologyChief, Clinical Epidemiology and
OutcomesBaylor College of MedicineHouston, TX, USA
Guy D. Eslick, DrPH, PhD, FACE, FFPHAssociate Professor of Surgery and Cancer
EpidemiologyThe Whiteley-Martin Research CentreDiscipline of SurgeryThe University of SydneySydney, Australia
James E. Everhart, MD, MPHChief, Epidemiology and Clinical Trials BranchDivision of Digestive Diseases and NutritionNational Institute of Diabetes and Digestive and
Kidney DiseasesNational Institutes of HealthBethesda, MD, USA
Tala H.I. Fakhouri, PhD, MPHNational Center for Health StatisticsCenters for Disease Control and PreventionHyattsville, MD;Epidemic Intelligence ServiceCenters for Disease Control and PreventionAtlanta, GA, USA
Katherine M. Flegal, PhDOffice of the DirectorNational Center for Health StatisticsCenters for Disease Control and PreventionHyattsville, MD, USA
Kate M. Fleming, MA, MSc, PhDLecturer in Gastrointestinal EpidemiologyDivision of Epidemiology and Public HealthNottingham City HospitalUniversity of NottinghamNottingham, UK
Alexander C. Ford, MBChB, MD, FRCPAssociate Professor and Honorary Consultant
GastroenterologistLeeds Teaching Hospitals TrustLeeds, West Yorkshire, UK
Rodney Givney, BScMed (Hons), MBBS, FRCPA,PhD, MPH
Division of MicrobiologyHunter Area PathologyPathology North & Newcastle UniversityNew South Wales, Australia
Matthew J. Grainge, MSc, PhDAssociate ProfessorDivision of Epidemiology and Public HealthNottingham City HospitalUniversity of NottinghamNottingham, UK
ix
CONTRIBUTORS
Magnus Halland, BMed, BMedSci (Hons), MPHConjoint LecturerUniversity of NewcastleCallaghan, NSW, Australia
David J. Humes, BSc, MBBS, MRCS, PhDLecturer in SurgeryNottingham Digestive Disease Centre Biomedical
Research UnitDivision of SurgeryUniversity of NottinghamNottingham, UK
Richard H. Hunt, FRCP, FRCPEd, FRCPC,MACG, AGAF
Professor, Farncombe Family Digestive DiseaseResearch Institute and Division ofGastroenterology
McMaster University Health Science CentreHamilton, ON, Canada
John M. Inadomi, MDCyrus E. Rubin Professor of MedicineHead, Division of GastroenterologyUniversity of WashingtonSeattle, WA, USA
Steven J. Jacobsen, MD, PhDDirector of ResearchResearch and EvaluationSouthern California Permanente Medical GroupPasadena, CA, USA
Linda E. Kelemen, MSc, ScDResearch Scientist, Department of Population
Health ResearchAlberta Health Services-Cancer CareDepartments of Medical Genetics and OncologyUniversity of CalgaryCalgary, AB, Canada
Hannah P. KimDivision of Gastroenterology and HepatologyUniversity of North Carolina School of MedicineUniversity of North Carolina at Chapel HillChapel Hill, NC, USA
W. Ray Kim, MDAssociate Professor of MedicineGI Epidemiology/Outcomes UnitDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
Brian K. Kit, MD, MPHDivision of Health and Nutrition Examination
SurveysNational Center for Health StatisticsCenters for Disease Control and PreventionHyattsville, MD, USA
Brian E. Lacy, PhD, MDProfessor of MedicineDartmouth Medical SchoolDirector, GI Motility LaboratorySection of Gastroenterology and HepatologyDartmouth-Hitchcock Medical CenterLebanon, NH, USA
Grigorios I. Leontiadis, MD, PhDAssociate ProfessorDepartment of MedicineDivision of GastroenterologyMcMaster UniversityHamilton, ON, Canada
John M. Levenick, MDClinical Instructor in MedicineSection of Gastroenterology and HepatologyDartmouth-Hitchcock Medical CenterLebanon, NH, USA
Joseph Lipscomb, PhDProfessor of Public Health and Georgia Cancer
Coalition Distinguished Cancer ScholarDepartment of Health Policy & ManagementRollins School of Public HealthEmory UniversityAtlanta, GA, USA
G. Richard Locke III, MDProfessor of MedicineGI Epidemiology/Outcomes UnitDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
x
CONTRIBUTORS
Edward V. Loftus, Jr, MDProfessor of MedicineDirector, Inflammatory Bowel Disease Interest GroupDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
Jonas F. Ludvigsson, MD, PhDProfessor in Clinical EpidemiologySenior PediatricianKarolinska Institutet and Örebro University HospitalStockholm, Örebro, Sweden
Sanjiv Mahadeva, MRCP, MDLecturer and Consultant GastroenterologistDivision of Gastroenterology, Department of
MedicineFaculty of MedicineUniversity of MalayaKuala Lumpur, Malaysia
Salaheddin Mahmud, MD, PhD, FRCPCAssistant Professor of MedicineCommunity Health Sciences, University of Manitoba;Epidemiology, CancerCare ManitobaWinnipeg, MB, Canada
L. Joseph Melton III, MD, MPHProfessor of EpidemiologyDepartment of Health Sciences ResearchMayo Clinic College of MedicineRochester, MN, USA
Paul Moayyedi, BSc, MB ChB, PhD, MPH, FRCP,FRCPC, AGAF, FACG
Acting Director of the Farncombe Family DigestiveHealth Research Institute
Director of Division of GastroenterologyMcMaster UniversityHamilton, ON, Canada
Joselito M. Montalban, MD, MCHMDepartments of Internal Medicine and Community
Health SciencesUniversity of ManitobaWinnipeg, MB, Canada
Joseph A. Murray, MDProfessor of MedicineDivision of Gastroenterology and
HepatologyMayo Clinic College of MedicineRochester, MN, USA
Olof Nyrén, MD, PhDProfessor of Clinical EpidemiologyDepartment of Medical Epidemiology
and BiostatisticsKarolinska InstitutetStockholm, Sweden
Cynthia L. Ogden, PhD, MRPDivision of Health and Nutrition Examination
SurveysNational Center for Health StatisticsCenters for Disease Control and PreventionHyattsville, MD, USA
Judith M. Podskalny, PhDDirector, Research Fellowship and Career
Developmentand Digestive Disease Centers ProgramsDivision of Digestive Diseases and NutritionNational Institute of Diabetes and Digestive
and Kidney DiseasesNational Institutes of HealthBethesda, MD, USA
Dawn Provenzale, MD, MSAssociate Professor of MedicineDirector, Durham Epidemiologic Research and
Information CenterDirector, GI Outcomes ResearchDuke University Medical CenterDurham, NC, USA
Linda Rabeneck, MD, MPH, FRCPCVice President, Prevention and Cancer Control
Cancer Care OntarioProfessor of Medicine, University of TorontoToronto, ON, Canada
xi
CONTRIBUTORS
Enrique Rey, MD, PhD, AGAFProfessor of MedicineFunctional GI Disorders UnitDivision of Digestive DiseasesHospital Clinico San Carlos, Universidad
ComplutenseMadrid, Spain
Alberto Rubio-Tapia, MDDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
Yuri A. Saito, MD, MPHAssistant Professor of MedicineDirector, GI Epidemiology/Outcomes UnitDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
William Sanchez, MDAssistant Professor of MedicineDivision of Gastroenterology and HepatologyMayo Clinic College of MedicineRochester, MN, USA
William J. Sandborn, MDProfessor of Medicine and Adjunct Professor of
SurgeryChief, Division of GastroenterologyDirector, UCSD IBD CenterUniversity of California San Diego and UC San
Diego Health SystemLa Jolla, CA, USA
Philip Schoenfeld, MD, MSEd, MSc (Epi)Professor of MedicineUniversity of Michigan School of MedicineAnne Arbor, MI, USA
Eldon A. Shaffer, MD, FRCPCProfessor of MedicineDivision of GastroenterologyUniversity of CalgaryCalgary, AB, Canada
Nicholas J. Shaheen, MD, MPHProfessor of Medicine and EpidemiologyDirector, Center for Esophageal Diseases
and SwallowingUniversity of North Carolina School of MedicineChapel Hill, North Carolina, USA
Harminder Singh, MD, MPHAssistant Professor of MedicineDepartments of Internal Medicine and Community
Health Sciences, University of Manitoba;Division of GastroenterologyUniversity of Manitoba IBD Clinical and
Research Centre;Department of Medical Oncology and Haematology,
CancerCare Manitoba;Winnipeg, MB, Canada
Robin SpillerNottingham Digestive Disease Biomedical
Research UnitUniversity of Nottingham, Queen’s Medical CentreNottingham, UK
Crenguta Stepan, MDUniversity of WashingtonValley Medical CenterSeattle, WA, USA
Aravind Sugumar, MDAssistant Professor of MedicineDepartment of Gastroenterology and HepatologyUniversity of Kansas Medical CenterKansas City, KS, USA
Joseph Sung, MD, PhDChairman and Professor of MedicineDepartment of Medicine & TherapeuticsPrince of Wales Hospital, ShatinThe Chinese University of Hong KongNT, Hong Kong
Christina M. Surawicz, MDProfessor of MedicineSection Chief, Gastroenterology, Harborview
Medical CenterAssistant Dean for Faculty DevelopmentUniversity of Washington School of MedicineSeattle, WA, USA
xii
CONTRIBUTORS
Nicholas J. Talley, MD, PhD, M Med Sci (Clin Epi),FRACP, FAFPHM
Pro Vice-Chancellor and Dean (Health andMedicine), and Professor
University of NewcastleCallaghan, NSW, Australia
Laila J. Tata, BSc, MSc, PhDAssociate Professor of EpidemiologyDivision of Epidemiology and Public HealthUniversity of NottinghamNottingham, UK
Frances Tse, MDDivision of GastroenterologyMcMaster UniversityMcMaster University Medical CentreHamilton, ON, Canada
Santhi Swaroop VegeProfessor of MedicineDivision of Gastroenterology and HepatologyMayo ClinicRochester, MN, USA
Joe West, BMedSci, BM BS, MRCP, MSc, PhD, PGDipAssociate Professor and Reader in Epidemiology;
Honorary Consultant GastroenterologistDivision of Epidemiology and Public HealthUniversity of NottinghamNottingham, UK
Ingela Wiklund, PhDSenior Research LeaderEvideraLondon, UK
Dhiraj Yadav, MD, MPHDivision of Gastroenterology and HepatologyUniversity of Pittsburgh Medical CenterPittsburgh, PA, USA
Hematram Yadav, MBBS, MPH, MBA,MRSH, FAMM
Department of Community MedicineFaculty of MedicineInternational Medical UniversityKuala Lumpur, Malaysia
xiii
Foreword
This volume presents an authoritative overview of cur-rent understanding regarding the epidemiology of gas-trointestinal diseases and will serve well those work-ing in research or clinical medicine who are seekingto answer questions regarding the causes of such dis-eases. All major gastrointestinal disease entities arecovered in 23 topic-orientated chapters, each with aset of key points and some testing multiple choicequestions, and the reader can jump straight into theirdisease of interest knowing that the state of the art inepidemiology will be presented in a clear and concisemanner. But this book offers much more. It is reallytwo books in one: in addition to the topic-orientatedchapters, an extensive series of introductory chap-ters outlines the major study designs in epidemiol-ogy and summarizes the main areas of methodologyunderlying each design. This provides an importantgrounding in critical appraisal to guide those wish-ing to delve deeper into the literature. Many of themethodological complexities are reviewed further inthe web supplement to the book. These elements com-bined with the “how to do clinical research” sectionsprovide a primer in gastrointestinal epidemiologyon a par with many standard general epidemiologytextbooks.
Professional epidemiologists frequently complainthat clinicians in a particular field, who may spenda decade or more honing their diagnostic and thera-peutic skills, often think they can acquire an under-standing of epidemiology as an incidental by-productwithout ever seriously considering the necessary meth-ods involved. This book can act as a corrective to
such tendencies and it is to be hoped that all thoseseeking an understanding of the epidemiology of aspecific gastrointestinal disease will read the first 12chapters of the volume (along with the supplement)so they can evaluate the strengths and limitationsof the methods employed and hence the certainty orotherwise of the conclusions. Unfortunately no text-book can force a reader to prepare him/herself in thisway but this volume leaves no excuse and stands incontrast to many others seeking to cover the sameground.
As medical knowledge expands at an ever increasingpace, the broad understanding of disease distributionand dynamics provided by epidemiology remains offundamental importance if prevention is going to beplaced on the agenda. Many gastrointestinal diseasesare fully preventable while others remain enigmatic intheir aetiology. This volume covers the full spectrumand ultimately addresses the key public health ques-tion for each disease – can it be prevented on the basisof present knowledge and, if so, how? Readers are,however, equipped not only with the answer but theweight and texture of evidence leading to the answer.The editors are to be congratulated on assemblinga group of expert gastroenterologists/epidemiologistswho can pull this evidence together.
David FormanHead, Section of Cancer Information
International Agency for Research on CancerLyon, France
October 2013
xiv
Preface
A rich tradition of epidemiologic research exists in gas-troenterology, and the 2nd edition of GI Epidemiol-ogy aims to provide a comprehensive expert roadmap.Why is it critically important to study and under-stand the epidemiology of gastrointestinal and liverdiseases? Health professionals strive to cure disease,and epidemiology can provide vital clues about diseasepathogenesis and etiology. Case-control and cohortstudies as well as clinical trials and meta-analysesinform gastroenterology practice but to interrogatethe information requires skills in epidemiology. Torationally apply testing, physicians need to understandthe prevalence of disease in their practices. Under-taking rigorous clinical research relies on appropri-ate study design and this is the core of epidemiology.For priorities in the health system, policy makers relyon knowledge of the burden of illness, while govern-ment and nongovernment funders of research use suchinformation to help determine resource distribution.
Knowledge continues to explode; this new editionof GI Epidemiology has been completely revised andupdated by experts from around the world. We have
proudly built on the success of the 1st edition, whichhas become the standard textbook in the field, witha more global focus, expanded methodological guid-ance, increased illustrations, summaries of key points,and coverage of all major diseases and syndromes.In addition to the 35 chapters in print, a further 10chapters online cover additional background materialincluding further insights into specific methodologicalissues and how to secure research funding. Multiplechoice questions have been included to aid learning.
We hope you will enjoy reading GI Epidemiology.The best and brightest minds in gastroenterology andepidemiology have contributed to this volume, andwe are very grateful for their diligent efforts. Despitean increasing interest in and understanding of the epi-demiology of gastrointestinal diseases, many vital gapsremain. We look forward to many of the readers ofthis book being inspired to fill these gaps. The Editorsremain passionate about the discipline of GI Epidemi-ology and we welcome you to the field.
Nicholas J. Talley, MD, PhD,on behalf of the Editors
xv
Companion website
This book is accompanied by a website:
ADDITIONAL CHAPTERS: AVAILABLE ONLINE AT:www.wiley.com/go/talley/giepidemiology.com
Part 1: Gastrointestinal Diseasesand Disorders: The PublicHealth Perspective
1 The Importance of GI Epidemiology, 3G. Richard Locke III & Nicholas J. Talley
Part 2: Methodological Issues inGI Epidemiology
2 Overview of Epidemiologic Methodology, 11L. Joseph Melton III & Steven J. Jacobsen
3 Patient-reported Outcomes, 16Ingela Wiklund
4 Clinical Trials, 23William J. Sandborn
5 Decision Analysis, 33John M. Inadomi
6 Health Economics, 40Dawn Provenzale & Joseph Lipscomb
7 Systematic Reviews, 57Philip Schoenfield
8 Meta-analyses, 63Paul Moayyedi
9 A Career in GI Epidemiology, 71Linda Rabeneck
10 Funding Opportunities at the National Institutesof Health, 77James E. Everhart & Judith M. Podskalny
http://www.wiley.com/go/talley/giepidemiology.com
PART ONE
Gastrointestinal Diseasesand Disorders: The PublicHealth Perspective
1 The burden of gastrointestinal andliver disease around the worldHannah P. Kim1, Seth D. Crockett2, & Nicholas J. Shaheen31Division of Gastroenterology and Hepatology, University of North Carolina School ofMedicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA2Division of Gastroenterology, University of North Carolina School of Medicine, University ofNorth Carolina at Chapel Hill, Chapel Hill, NC, USA3Center for Esophageal Diseases and Swallowing, University of North Carolina School ofMedicine, Chapel Hill, North Carolina, USA
Key points� Gastrointestinal and liver diseases are amongthe most common diseases worldwide, withdiarrheal disease, malignancies, and liver dis-ease having a substantial toll on worldwidemortality.� Many of these diseases are preventable andpossibly curable.� There is wide variability in the incidence, man-agement, and mortality associated with thesedisease states throughout the world.� Understanding trends in GI illness and the fac-tors responsible for variability in incidence andoutcomes will allow clinicians, public healthprofessionals, policy makers, and healthcareorganizations to intervene in a more logicalway and allocate resources to meet the needsof afflicted patients and decrease the burden ofgastrointestinal and liver diseases.
Introduction
Gastrointestinal and liver diseases represent a signifi-cant global health problem, and cause approximately
8 million deaths per year worldwide [1]. In developedcountries, GI malignancies are among the leadingcauses of death. In developing countries, diarrhealdisease and viral liver infections are highly prevalentand are responsible for significant mortality. Theseand other diseases are tracked by internationaland regional health organizations. These trackingmeasures allow for some assessment of the globalburden of GI disease, and may allow identification ofimportant temporal trends.
Below we highlight sources of burden of GI illnessinternationally. Using international databases, we willhighlight some important trends in diarrheal diseaseand childhood mortality, explore the burden of gas-trointestinal malignancies, and discuss the toll of sev-eral selected liver diseases. Because valid internationalestimates are not available for some gastrointestinalconditions, we report regional data with respect tothe toll of other selected GI diseases.
Much of the data demonstrated below has been col-lected as part of various projects conducted by theWorld Health Organization (WHO). Geographicalregions that are discussed throughout this chapter arebased on the six officially delineated WHO regions:Africa, the Americas, Eastern Mediterranean, Europe,Southeast Asia, and Western Pacific. A map delineat-ing each region can be found at: http://www.who.int/about/regions/en/index.html.
GI Epidemiology: Diseases and Clinical Methodology, Second Edition. Edited by Nicholas J. Talley et al.C© 2014 John Wiley & Sons, Ltd, with the exception of original artwork which is C© Mayo Foundation for Medical Education and Research.Published 2014 by John Wiley & Sons, Ltd. Companion website: www.wiley.com/go/talley/giepidemiology
3
http://www.who.int/about/regions/en/index.htmlhttp://www.wiley.com/go/talley/giepidemiologyhttp://www.who.int/about/regions/en/index.html
CHAPTER 1
Diarrheal disease
Global burden
An estimated 2.5 billion cases of diarrhea occur annu-ally in children under five years of age [2], with anestimated frequency of 2–3 episodes per child per yearin developing countries [3]. Diarrheal disease is thesecond leading cause of mortality in this age groupworldwide, after pneumonia. Responsible for over15 % of deaths of children less than five years of age,diarrheal disease accounts for more than 1.3 milliondeaths each year. It is also responsible for more deathsthan HIV/AIDS, malaria, and measles combined [1].
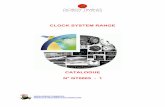
Figure 1.1 displays the number of under-5 deathssecondary to diarrheal disease by WHO region. Diar-rheal death is much more common in the developingworld, with over 56 % of deaths occurring in Africa.Africa and Southeast Asia combined account fornearly 80 % of all under-5 diarrhea-related deaths.Furthermore, 75 % of childhood deaths attributableto diarrheal disease can be found in just 14 devel-oping countries, led by India, Nigeria, and theDemocratic Republic of the Congo [4]. This islargely due to contamination of drinking water andcompromised sanitation in these countries. Childrenin these countries develop nutritional deficiencies, andare more susceptible to repeated episodes of diarrheaand severe dehydration, also contributing to the high
0
200
400
600
800
Southeast
Asia
Africa Western Eastern
Med PacificEuropeAmericas
Nu
mb
er o
f d
eath
s (t
hou
san
ds)
Figure 1.1 Deaths secondary to diarrheal disease amongchildren aged �5 years by WHO region, 2008. Source:WHO Health statistics and health information systems –child mortality by cause.
incidence of mortality due to diarrhea in developingnations [2].
Efforts to reduce the number of childhood deathssecondary to diarrheal disease in the 1970s and 1980shave favorably impacted the burden of diarrheal dis-ease. These efforts included increasing oral rehydra-tion therapy and the implementation of programsto educate caregivers on proper treatment. Whilethe overall incidence rates of diarrheal disease haveremained stable throughout the past three decades,there has been a decrease in diarrhea-associated deaths[3]. Estimates have shown a steady decline with4.6 million deaths per year in the 1960s and 1970s,3.3 million deaths per year in the 1980s, 2.5 milliondeaths per year in the 1990s, and 1.5 million deathsin 2004 [2, 5–7]. Despite this improvement, diarrheacontinues to be an unacceptably common cause ofchildhood death, especially in developing countries.
Gastrointestinal malignancies
Global burden
Cancer is the leading cause of death in developednations and is the second leading cause of deathin developing nations [8]. GLOBOCAN is a WHOproject which estimates the international burden ofcancer using population-based cancer registries [9].Gastrointestinal cancers were responsible for nearlyone-third of new cancer cases in 2008. Table 1.1displays incidence of, and mortality from, gastroin-testinal cancers worldwide, as well as their rankamong all major cancer sites. Colorectal cancer con-tinues to have the highest incidence rate among gas-trointestinal malignancies and is the third most com-monly occurring cancer worldwide, with over 1.2 mil-lion new cases estimated in 2008. Hepatocellular,esophageal, and pancreatic cancers are of particularimportance because of their high mortality; in fact,mortality-to-incidence ratios approach one interna-tionally. Colorectal cancer is associated with a muchbetter prognosis, with a mortality-to-incidence ratio ofapproximately 0.5. Assessment of the three most com-monly occurring gastrointestinal malignancies world-wide demonstrates marked variation in incidence andmortality. Colorectal and gastric cancers will be dis-cussed in the following two sections and liver cancerwill be discussed in a later section.
4
THE BURDEN OF GASTROINTESTINAL AND LIVER DISEASE AROUND THE WORLD
Table 1.1 Incidence and mortality of gastrointestinal cancers worldwide, 2008
Incidence Mortality
Rank among Rank among ICD-10 Crude CrudeGI sites all sites Cancer site code Numbers rate† ASR§ Numbers rate† ASR§
1 3 Colorectum∗ C18-21 1,235,108 18.3 17.3 609,051 9.0 8.22 4 Stomach C16 988,602 14.6 14.1 737,419 10.9 10.33 6 Liver C22 749,744 11.1 10.8 695,726 10.3 10.04 8 Esophagus C15 481,645 7.1 7.0 406,533 6.0 5.85 13 Pancreas C25 278,684 4.1 3.9 266,669 4.0 3.76 15 Lip, oral cavity C00-08 263,020 3.9 3.8 127,654 1.9 1.97 21 Gallbladder C23-24 145,203 2.2 2.0 109,587 1.6 1.5
Source: GLOBOCAN 2008.∗Includes anal cancer.†Crude rates are per 100,000.§ASR, age-standardized rates per 100,000.
Colorectal cancer
Colorectal cancer is the third highest incident cancer,and fourth most common cause of death from can-cer worldwide, with over 609,000 deaths estimatedin 2008. Approximately 60 % of colorectal cancercases are found in developed regions; however, onlyapproximately 53 % of deaths attributable to colorec-tal cancer are found in these same regions. Of note,the incidence rate of colorectal cancer in Africa is asmall fraction of that in Europe, but is associated withcancer-related mortality in nearly all cases.
In the last three decades, the United States has wit-nessed a decrease in the incidence rate of colorectalcancer and an even greater decrease in the mortalityrate. The extent to which decreasing colorectal cancermortality can be attributed to earlier detection of col-orectal cancer and improved methods of treatment isdebated [10]. Unfortunately, those in less developedregions, where proper resources are lacking, sufferpoorer prognoses.
Gastric cancer
Gastric cancer is the second most common gastroin-testinal cancer and the fourth most common cancerworldwide. It was responsible for nearly 1 millionnew cancer cases and approximately 737,000 cancerdeaths in 2008, making it the number one GI-relatedcancer killer worldwide. More than 70 % of the new
cases and more than 75 % of deaths occurred inless developed regions. The incidence rate of gastriccancer is greatest in the Western Pacific, with nearlyhalf of all cases being found in China (463,000 cases)and with highest incidence rates among the Republicof Korea and Japan. The lowest rates of gastric cancercan be found in Africa, Southeast Asia, and the East-ern Mediterranean regions. Regional variation may bepartially attributed to differences in dietary patternsand the prevalence of Helicobacter pylori infection[8]. While gastric cancer is one of the leading causesof cancer death, individuals with gastric cancer in theWestern Pacific tend to have better prognoses thanthose in other regions, possibly due to the increaseduse of screening methods and earlier detection ofcancer [11].
Selected diseases of the liver
Hepatitis B
An estimated 2 billion people worldwide have beeninfected with the hepatitis B virus (HBV). More than350 million people have chronic liver infections, andapproximately 600,000 persons die annually due toacute or chronic consequences of the virus. HepatitisB is estimated to be the cause of 30 % of cirrhosis and53 % of hepatocellular carcinoma [12]. Hepatitis B isendemic in China and other parts of Asia, with mostinfections occurring during childhood, and 8–10 %
5
CHAPTER 1
of the adult population being chronically infected. Incontrast, less than 1 % of the population in WesternEurope and North America is chronically infected[13].
In developing countries, HBV is largely trans-mitted during childbirth and early childhood infec-tions. In developed countries, transmission is primar-ily through high-risk sexual behavior and IV druguse, as well as from migration of infected individu-als from high prevalence areas [14]. Those infectedat a young age are most likely to develop chronicinfections. Whereas about 90 % of infants �1 yearinfected with HBV will develop chronic infections,about 90 % of healthy adults who are infected willcompletely recover within six months. Approximately25 % of adults who become chronically infected dur-ing childhood die from HBV-related liver cancer orcirrhosis [15].
Hepatitis C
An estimated 3–4 million people are infected withhepatitis C virus (HCV) each year with a total of130–170 million people chronically infected interna-tionally. Additionally, more than 350,000 people diefrom hepatitis C-related liver diseases annually. Hep-atitis C is estimated to be the cause of 27 % of cirrho-sis and 25 % of hepatocellular carcinoma worldwide[12]. Although HCV infection is found worldwide,high rates of infection are found in Egypt (22 %),Pakistan (4.8 %), and China (3.2 %) [16]. The mainmode of transmission in these countries is secondaryto injections using contaminated needles. Other modesof transmission include contaminated blood transfu-sions, organ transplants, IV drug use with contami-nated needles, and pre- or perinatal transmission froman HCV-infected mother.
Viral hepatitis in the United States
It is clear that the toll of hepatitis B and hepatitis Cinfections is significant worldwide. Interestingly, datafrom the US Centers for Disease Control and Preven-tion (CDC) demonstrates a decrease in reported casesand incidence of hepatitis B and C in the United States(Table 1.2) [17]. The incidence per 100,000 popula-tion of acute hepatitis B has decreased from 3.8 in1998 to 1.3 in 2008. Also, the incidence per 100,000population of acute hepatitis C has decreased from 1.3
Table 1.2 Incidence per 100,000 population of acutehepatitis B and hepatitis C in the United States by year,1998–2008
Hepatitis B Hepatitis C
Year Number Incidence Number Incidence
1998 10,258 3.8 3,518 1.31999 7,694 2.8 3,111 1.12000 8,036 2,9 3,197 1.12001 7,844 2.8 1,640c 0.7c
2002 8,064 2.8 1,223d 0.5d
2003 7,526 2.6 891d 0.3d
2004 6,212 2.1 758 0.32005 5,494 1.8 694 0.22006 4,713a 1.6a 802 0.32007 4,519 1.5 849 0.32008 4,033b 1.3b 878b 0.3b
Source: CDC Viral Hepatitis Statistics and Surveillance.aExcludes cases from Arizona.bExcludes cases from Delaware.cExcludes cases from New Jersey and Missouri.dExcludes cases from Missouri.
in 1998 and has been ≤ 0.3 since 2003. The cause ofthese secular trends remains unclear, but may reflectchanging practices in the IV drug user community, ora cohort effect.
Liver cancer
Liver cancer is the third most common gastrointestinalcancer and the fifth most common cancer worldwide.Almost 750,000 new liver cancer cases and 700,000deaths are estimated to have occurred in 2008, withover 80 % of new cases and deaths occurring in lessdeveloped regions. There were an estimated 694,000deaths from liver cancer in 2008, and because of itshigh fatality (overall ratio of mortality to incidenceof 0.93), liver cancer is the third most common causeof death from cancer worldwide. Within liver can-cers, hepatocellular carcinoma constitutes the majorhistological subtype, accounting for 70–85 % of thetotal liver cancer toll worldwide. Cholangiocarcino-mas (intra- and extrahepatic bile duct cancers) arerelatively rare, but high rates have been found in areassuch as Thailand and other parts of eastern Asia sec-ondary to endemic liver fluke infection [8].
6
THE BURDEN OF GASTROINTESTINAL AND LIVER DISEASE AROUND THE WORLD
0
10
20
30
Southeast
Asia
EuropeEastern
Med
AmericasAfrica Western
Pacific
Ra
te p
er 1
00
,00
0
Incidence
Mortality
Figure 1.2 Incidence and mortality rates of liver cancer byWHO region, 2008. Source: GLOBOCAN 2008.
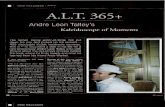
Figure 1.2 shows the distribution of liver cancerincidence and mortality by WHO region. The highestincidence and mortality rates are found in the WesternPacific, with more than half of new cases and deathsoccurring in China [9]. Incidence and mortality ratesare significantly lower in all other regions. The signif-icantly higher incidence of liver cancer in the West-ern Pacific is largely due to the elevated prevalence ofchronic hepatitis B virus (HBV) infection. HBV infec-tion is responsible for approximately 60 % of totalliver cancer in developing countries and for about23 % of total liver cancer in developed countries [18].Similarly, chronic hepatitis C virus (HCV) infectionaccounts for about 33 % and 20 % of total liver can-cers in developing countries and developed countries,respectively.
Selected gastrointestinal diseases
Clostridium difficile infections
Clostridium difficile is a spore-forming, gram-positivebacillus that can cause disease ranging from mild diar-rhea to fulminant colitis and death. This pathogen isrecognized as the most common infectious cause ofhealthcare-related diarrhea [19]. Mutations that con-fer antibiotic resistance, increase toxin production,or facilitate sporulation have substantially increasedthe prevalence and virulence of this opportunisticpathogen [20]. During the mid and late 1990s, thereported incidence of C. difficile infection (CDI) in
0
100
200
300
400
200920072005200320011999199719951993
Nu
mb
er o
f d
isch
arg
es (
thou
san
ds)
Figure 1.3 Trend of Clostridium difficile infection dischargediagnoses from hospital admissions, 1993–2009. Source:HCUP Nationwide Inpatient Sample (NIS), 1993–2009.
acute care hospitals in the United States remainedstable at 30–40 cases per 100,000 population. In2001, this number rose to almost 50 and continuedto increase, resulting in 84 per 100,000 reported casesin 2005, a nearly threefold increase since 1996 [21].Figure 1.3 displays the trend of US hospital dischargediagnoses of CDI over a 17-year period (1993–2009).Parallel to the increasing prevalence of this diseaseis its increasing severity and fatality. For example, inEngland, CDI was listed as the primary cause of deathfor 499 patients in 1999, 1998 patients in 2005, and3393 patients in 2006 [21].
In addition, while CDI has traditionally affectedelderly or severely ill hospital and nursing homepatients, a 2005 US CDC advisory noted increasedinfection in populations not previously considered atrisk, including young and healthy persons who havenot been exposed to a hospital or healthcare environ-ment or antimicrobial therapy [22]. Transmission insuch cases may be attributable to close contact withpatients who have CDI and direct person-to-personspread.
Gastroesophageal reflux disease
A major trend in gastroesophageal reflux disease(GERD) is an observed increase in its prevalence overthe past two decades. Europe and North Americahave shown an increase in the prevalence of refluxsymptoms, and studies of the same source population
7
CHAPTER 1
over time have demonstrated an increase in preva-lence in the United States, Singapore, and China [23].Prevalence in Western countries has been estimated at10–20 %, using criteria of at least weekly heartburnand/or acid regurgitation [24]. According to a reviewusing the US National Ambulatory Medical Care Sur-vey (NAMCS), the rate of US ambulatory care visitsfor GERD increased from 1.7 per 100 persons to 4.7per 100 persons from 1990–1993 to 1998–2001 andcontinues to be a frequent cause of consultation inprimary care [25].
The incidence of a GERD diagnosis and the demo-graphic factors associated with the diagnosis wereassessed using the UK General Practice ResearchDatabase [26]. In this study, 7159 patients were identi-fied with a new GERD-related diagnosis in 1996, cor-responding to an incidence among individuals aged2–79 years of 4.5 new diagnoses per 1000 person-years. The incidence was age-related and increasedwith age until 69 years, with a slight decrease there-after. Women had a slightly higher risk of developingGERD than men in patients over 50 years of age (rateratio = 1.3).
Inflammatory bowel disease
Although a major cause of gastrointestinal illness andhealthcare utilization, reliable data on inflammatorybowel disease rates are not available in most regionsof the world. When examining the age-adjusted timetrends of US physician visits secondary to Crohn’sdisease and ulcerative colitis (UC) from 1960–2006,physician visits for Crohn’s disease increased almostfourfold over a 30-year period from the early 1960sto the early 1990s, from about 120 to 400 physicianvisits per 100,000 people. Since then, the rates ofCrohn’s disease visits appear to have leveled off.Physician visits for UC actually slightly decreasedduring the same 30-year period from about 400 to300 physician visits per 100,000 people. With respectto sex differences, physician visits for Crohn’s diseaseremained about 1.4-fold more frequent in womenthan men. Between 1960 and 1984, physician visitsfor UC were 1.3-fold more frequent by women thanby men; however, during more recent periods, therates of physician visits for UC by men and womenhave become more similar [27].
From 1951 to 2005, there has been a nearly 80 %decrease in mortality from UC from approximately
5.6 to 1.2 deaths per million population in a totalof 21 countries [28]. On the other hand, from 1951to 1975, mortality from Crohn’s disease increasedalmost twofold from 0.8 to 1.5 deaths per million pop-ulation. Since then, mortality from Crohn’s disease hasbeen decreasing and paralleling the trend of UC.
Gastrointestinal diseases responsiblefor hospitalization
While gastrointestinal illness is a major cause of hospi-talization throughout the world, reliable data on hos-pitalization rates for various illnesses are not avail-able internationally. Table 1.3 demonstrates the mostcommon gastrointestinal and liver causes of hospital-ization, ordered by number of reports at discharge,using the National Inpatient Sample, a 20 % stratifiedsample of US community hospitals. Acute pancreatitis,gallstone diseases, diverticulitis without hemorrhage,and acute appendicitis were each responsible for over200,000 hospitalizations. Aspiration pneumonia wasthe fifth cause of hospitalization, and was also in theoverall top 30 causes of hospitalization for any diseaseentity.
Limitations of the data
The data that were used for the above analyses areof the highest quality information available to assessthe overall global burden of gastrointestinal diseases.However, there are some limitations that meritattention.
Ideally, all data would come from vital registrieswith complete coverage and medical certification ofcause of death. For countries with incomplete orno vital registration system, epidemiologic studies,systematic reviews, and statistical modeling wereused. For countries with incomplete data or no dataregarding cause of death, the distribution of deathswas estimated using statistical models, proportionalmortality, and natural history models. The 2008 esti-mates made available by the WHO were created usingWHO’s extensive databases and based on informationprovided by Member States, as well as on system-atic reviews and analyses carried out by CHERG(the Child Health Epidemiology Reference Group).
8
Tab
le1.
3M
ost
com
mon
gast
roin
test
inal
prin
cipa
ldis
char
gedi
agno
ses
from
hosp
ital
adm
issi
ons,
2009
∗
Ran
kR
ank
ICD
-9-
%�
Med
ian
Tot
alho
spit
alM
edia
nA
ggre
gate
In-h
ospi
tal
amon
gam
ong
CM
Tot
al#
from
LO
Sda
ys†
cost
sco
st(U
SD,
deat
hsG
Idx
alld
xco
de(s
)Pr
inci
pald
iagn
osis
Adm
issi
ons
2000
(day
s)(t
hous
ands
)(U
SD)
thou
sand
s)n
(%)
121
577.
0A
cute
panc
reat
itis
274,
119
+30
4.0
1,40
96,
096
2,59
9,68
62,
631
(1.0
)2
41,
574.
0,C
hole
lithi
asis
wit
hch
olec
ysti
tis‡
226,
216
−14
3.0§
819
8,32
2§2,
208,
531
959
(0.4
)76
574.
13
2756
2.11
Div
erti
culit
isw
itho
uthe
mor
rhag
e21
9,13
3+
414.
01,
099
6,07
72,
115,
989
1,23
5(0
.6)
429
540.
9A
cute
appe
ndic
itis
207,
345
+22
1.0
362
6,59
21,
491,
402
90(0
.04)
530
507.
0A
spir
atio
npn
eum
onia
188,
930
+6
6.0
1,47
59,
030
2,52
3,29
922
,273
(11.
8)6
3755
8.9
Non
infe
ctio
usga
stro
ente
riti
s/co
litis
151,
856
+36
2.0
462
4,09
077
5,02
048
6(0
.3)
744
578.
9G
astr
oint
esti
nalh
emor
rhag
eN
OS
140,
497
+22
3.0
612
6,09
01,
155,
971
4,91
4(3
.5)
846
560.
9In
test
inal
Obs
truc
tion
NO
S13
4,43
1+
443.
060
05,
098
1,01
8,43
72,
812
(2.1
)9
4727
8.01
Mor
bid
obes
ity
132,
448
+31
42.
028
810
,689
1,64
2,29
313
7(0
.1)
1057
8.45
Clo
stri
dium
diffi
cile
infe
ctio
n11
0,55
3+
237
5.0
761
6,77
41,
119,
213
4,03
8(3
.7)
1173
560.
81In
test
inal
adhe
sion
sw
ith
obst
ruct
ion
83,1
83+
237.
073
611
,853
1,45
3,23
82,
265
(2.7
)12
948.
8V
iral
gast
roen
teri
tis
66,8
42+
292.
018
13,
677
298,
507
108
(0.2
)13
9653
0.81
Eso
phag
ealr
eflux
65,6
34−3
22.
016
24,
366
386,
229
n/a∗
∗
1410
056
2.12
Div
erti
culo
sis
wit
hhe
mor
rhag
e64
,222
−63.
029
15,
818
552,
906
713
(1.1
)
∗ Wei
ghte
dna
tion
ales
tim
ates
from
HC
UP
Nat
ionw
ide
Inpa
tien
tSa
mpl
e(N
IS),
2009
,Age
ncy
for
Hea
lthc
are
Res
earc
han
dQ
ualit
y(A
HR
Q).
Tot
alnu
mbe
rof
wei
ghte
ddi
scha
rges
inth
eU
nite
dSt
ates
base
don
HC
UP
NIS
=39
,434
,956
.† T
otal
hosp
ital
days
per
year
for
allp
erso
nsw
ith
each
diag
nosi
s,es
tim
ated
byth
epr
oduc
tof
num
ber
ofdi
scha
rges
and
mea
nL
OS.
‡ IC
D-9
-CM
code
sfo
r“c
alcu
lus
ofga
llbla
dder
wit
hac
ute
chol
ecys
titi
s”(5
74.0
)an
d“c
alcu
lus
ofga
llbla
dder
wit
hot
her
chol
ecys
titi
s”(5
74.1
)co
mbi
ned
for
this
diag
nosi
s.T
otal
num
ber
ofdi
scha
rges
,agg
rega
tech
arge
san
dco
sts,
and
in-h
ospi
tald
eath
sre
pres
ent
sum
from
both
.§ M
edia
nL
OS
and
med
ian
cost
spr
esen
ted
for
mos
tco
mm
onIC
D-9
-CM
code
sin
this
cate
gory
(574
.0).
∗∗T
oofe
wev
ents
toge
nera
tea
stab
lees
tim
ate
inth
isca
tego
ry[(
stan
dard
erro
r/w
eigh
ted
esti
mat
e)�
0.30
].D
x,di
agno
sis;
ICD
-9-C
M,I
nter
nati
onal
Cla
ssifi
cati
onof
Dis
ease
s,9t
hed
itio
n,C
linic
alM
odifi
cati
on;%
�,p
erce
ntch
ange
;LO
S,le
ngth
ofst
ay;U
SD,U
Sdo
llars
;N
OS,
not
othe
rwis
esp
ecifi
ed.
CHAPTER 1
Incidence data for cancers are associated with somelevel of delay as this type of data requires time tobe compiled; while the numbers within this chapterare the most current available, there is a several yeartime lag. More recent data about individual regionsmay be found in reports from the registries themselves.Information from most of the developing countriesmay be considered of relatively limited quality, butthis information remains the only source of informa-tion for these regions. Mortality statistics collectedand made available by the WHO have the advan-tages of national coverage and long-term availability;however, some datasets are of lesser quality than oth-ers. For some countries, coverage of the population isincomplete, resulting in low estimated mortality rates.In other countries, the quality of cause of death infor-mation is poor. While almost all the European andAmerican countries have comprehensive death reg-istration systems, most African and Asian countries(including the populous countries of Nigeria, India,and Indonesia) do not. Of course, a major concernregarding data from developing countries is detectionbias. In countries with limited medical technology andresources, the burden of undiagnosed cancer is likelysubstantial and is not quantifiable.
Data for some of the selected gastrointestinalillnesses was not readily available from regionaldatabases; therefore, the data in the above discussionis largely from studies that have accessed such primarydatabases and performed their own analyses.
Data derived from administrative databases, such asthe NIS data, may suffer from the use of data primarilyfor billing purposes. Therefore, the fidelity of codingdata to clinical information must be considered. Themedian and aggregate costs are estimates, calculatedfrom hospital charges, and the data are by level ofdischarge (e.g. a single patient could be representedby multiple discharges). Also, in analyzing the trends,some trends may represent epiphenomena. For exam-ple, an increase in morbid obesity discharges may bedue to increasing popularity of obesity surgery, forwhich morbid obesity is the principal coded dischargediagnosis.
Implications
Gastrointestinal and liver diseases are responsible forsignificant morbidity and mortality worldwide. The
above statistics attest to the toll of these diseases.Beyond merely describing the terrible impact of thesediseases, an understanding of the epidemiology ofgastrointestinal and liver disease allows consider-ation of improvement of systems-based practicesand public policy. Many individuals suffer frompreventable disease states such as childhood diarrhea,malignancy, and various liver diseases. Millionsof children annually die preventable deaths due todiarrheal disease. Cancer prognosis may be poorerin developing countries due to late detection andlack of access to resources and standard treatment.Numerous cases of gastrointestinal cancers couldbe prevented by vaccinations for viral hepatitis andimproved screening, as well as by promoting physicalactivity, implementing programs for tobacco control,and healthier dietary intake. In addition, data shouldbe updated regularly in order to track progress, aswell as to spot temporal trends in disease burden thatmight merit reallocation of resources to address thechanges.
Multiple choice questions
1 Which of the following is not associated with anincreased incidence of childhood diarrhea?
A Inconsistent access to a clean water supplyB Residing in the WHO Africa or Southeast AsiaregionC Chronic nutritional deficienciesD Availability of oral rehydration solutions
2 Which GI-related malignancy resulted in the mostestimated number of deaths in the year 2008?
A Colorectal cancerB Stomach cancerC Liver cancerD Esophageal cancerE Pancreatic cancer
3 Which gastrointestinal principal discharge diagno-sis has had the greatest percentage increase from 2000to 2009?
A Clostridium difficileB Acute pancreatitisC Morbid obesityD Intestinal obstruction NOSE Diverticulitis without hemorrhage
10
THE BURDEN OF GASTROINTESTINAL AND LIVER DISEASE AROUND THE WORLD
Appendix 1.A
Sources
Diarrheal diseaseEstimates used in this section are based on data fromthe Global Health Observatory (GHO), a repositorythat provides access to over 50 datasets on priorityhealth topics including mortality and burden ofdisease, produced by the World Health Organization(WHO) (http://apps.who.int/ghodata/). Estimates forthe distribution of causes of death among childrenaged �5 years can be accessed through “World HealthStatistics” → “Cause-specific mortality and morbid-ity” → “Causes of death among children” of theGHO data repository. Measurement and estimationmethods can be found at: http://apps.who.int/gho/indicatorregistry/App_Main/view_indicator.aspx?iid=89.
In collaboration with the Child Health Epi-demiology Reference Group (CHERG), the WHODepartment of Health Statistics and Informaticsprepared country-level estimates of child deathsunder 5 years of age by cause for the year 2008. Theseestimates are derived from WHO databases, informa-tion provided by Member States, as well as systematicreviews and analyses carried out by CHERG.Country-level data was combined to achieve datafor each WHO region. Mortality data on diarrhealdisease and other causes of death in children aged�5 years, as well as the methods used to obtain theseestimates can be accessed at: http://www.who.int/healthinfo/statistics/mortality_child_cause/en/index.html.
Gastrointestinal malignanciesThe estimates used in this section are based onGLOBOCAN 2008, a standard set of worldwide esti-mates of cancer incidence and mortality producedby the International Agency for Research on Cancer(IARC) under the auspices of WHO. This project wasdeveloped to provide up-to-date estimates of the inci-dence of, and mortality from major cancers for allnations in the world. GLOBOCAN allows individualsto obtain current estimates for major cancers catego-rized by region, sex, and age groups.
Incidence data were derived from population-basedcancer registries, either national or subnational areas.In developing countries, incidence data is often avail-
able only from major cities. Mortality data was col-lected and provided by WHO. While not all datasetsare complete and of the same quality (coverage ofthe population is incomplete or cause of death isinaccurate), it is the most accurate and thoroughinformation available. Provisional estimates of age-and sex-specific deaths from cancer for 2008 havebeen used for regions without death information orwhere statistics are considered unreliable. Nationalpopulation estimates for 2008 were extracted fromthe United Nation (UN) population division’s 2008revision using geographical definitions as defined bythe UN. The methods used to estimate incidenceand mortality of cancers for each country can befound at GLOBOCAN data sources and methods:http://globocan.iarc.fr/.
Selected diseases of the liverThe data used in the discussions of hepatitis B andC are derived from WHO estimates of burden ofdisease. The WHO media center has over 100 factsheets on various health-related topics such as differ-ent infections, disease states, and health risks, whichcan be found at: http://www.who.int/mediacentre/factsheets/en/. The hepatitis B and hepatitis C factsheets were last updated in July 2012. The dataincluded in the discussion about liver cancer is derivedfrom GLOBOCAN 2008, discussed in the previoussources section.
Hepatitis B and hepatitis C trend data wereobtained from the Centers for Disease Control andPrevention (CDC) – Viral Hepatitis Statistics andSurveillance, which can be found at: http://www.cdc.gov/hepatitis/Statistics/index.htm.
Gastrointestinal diseases responsible forUS hospitalizationThe most common inpatient gastroenterology andhepatology discharge diagnoses for the United Statesmay be compiled using the Nationwide InpatientSample (NIS). The NIS is one of the databases inthe Healthcare Cost and Utilization Project (HCUP)(http://hcupnet.ahrq.gov/). NIS is the only nationalhospital database with charge information on allpatients, regardless of payer, including persons cov-ered by Medicare, Medicaid, private insurance, andthe uninsured. The most recent version, NIS 2009,contains all discharge data from 1050 hospitalslocated in 44 states, representing a 20 % stratified
11
http://apps.who.int/ghodatahttp://apps.who.int/gho/indicatorregistry/App_Main/view_indicator.aspx?iid=89http://www.who.int/healthinfo/statistics/mortality_child_cause/en/index.htmlhttp://globocan.iarc.frhttp://www.who.int/mediacentre/factsheets/en/http://www.cdc.gov/hepatitis/Statistics/index.htmhttp://hcupnet.ahrq.govhttp://www.who.int/healthinfo/statistics/mortality_child_cause/en/index.htmlhttp://www.who.int/healthinfo/statistics/mortality_child_cause/en/index.htmlhttp://apps.who.int/gho/indicatorregistry/App_Main/view_indicator.aspx?iid=89http://apps.who.int/gho/indicatorregistry/App_Main/view_indicator.aspx?iid=89http://www.who.int/mediacentre/factsheets/en/http://www.cdc.gov/hepatitis/Statistics/index.htm
CHAPTER 1
sample of US community hospitals. The samplingframe for the 2009 NIS sample is a sample of hospi-tals that comprises approximately 95 % of all hospitaldischarges in the United States.
The NIS database was queried for the rank orderof the principal discharge diagnosis (i.e. InternationalClassification of Diseases Clinical Modification, 9thedition (ICD-9-CM) for all patients in all hospitals.From the top 100 diagnoses, we identified the gas-troenterology and hepatology diagnoses among them,which were subsequently rank-ordered after combin-ing related diagnosis codes. We then performed a sep-arate query for each individual ICD-9-CM code (orgroup of codes) to acquire data on mean and medianlength of stay (LOS), median charges and costs, aggre-gate charges (i.e. “the national bill”) and aggregatecosts, and number of inpatient deaths associated witheach diagnosis or diagnosis group. We also performeda temporal analysis for the number of admissions forthe top principal GI diagnoses between the years 2000and 2009 to identify relevant trends.
Total hospital days were estimated by the productof the mean LOS and the number of discharges foreach diagnosis. Total charges were converted to costsby HCUP using cost-to-charge ratios based on hospi-tal accounting reports from the Centers for Medicare& Medicaid Services (CMS). Cost data are presentedpreferentially, as costs tend to reflect the actual costsof production, while charges represent what the hos-pital billed for the case.
References
1 Global Health Observatory [Internet database]. WorldHealth Organization (2008). Available from: http://apps.who.int/ghodata/ (accessed July 27, 2011).
2 Johansson E, Wardlaw T. (2009) Diarrhoea: Why chil-dren are still dying and what can be done, UNICEF/World Health Organization, New York/Geneva.
3 Boschi-Pinto C, Lanata CF, Black RE. (2009) Theglobal burden of childhood diarrhea, in Maternal andChild Health: Global Challenges, Programs, and Policies(ed. J Ehiri), Springer, pp. 225–43.
4 Child mortality by cause [Internet database]. WorldHealth Organization (2008). Available from: http://www.who.int/healthinfo/global_burden_disease/cod_2008_sources_methods.pdf (accessed July 27, 2013).
5 Snyder JD, Merson MH. The magnitude of the globalproblem of acute diarrhoeal disease: a review of active
surveillance data. Bull World Health Organ 1982;60(4):605–13.
6 Bern C, Martines J, de Zoysa I, Glass RI. The magnitudeof the global problem of diarrhoeal disease: a ten-yearupdate. Bull World Health Organ 1992;70(6):705–14.
7 Kosek M, Bern C, Guerrant RL. The global burdenof diarrhoeal disease, as estimated from studies pub-lished between 1992 and 2000. Bull World Health Organ2003;81(3):197–204.
8 Jemal A, Bray F, Center MM, et al. Global cancer statis-tics. CA: Cancer J Clin 2011;61(2):69–90.
9 Ferlay J, Shin HR, Bray F, et al. (2010) GLOBOCAN2008 v1.2, Cancer Incidence and Mortality Worldwide:IARC CancerBase No. 10 [Internet database]. Interna-tional Agency for Research on Cancer, Lyon, France.Available from: http://globocan.iarc.fr (accessed August11, 2011).
10 Sandler RS. Editorial: colonoscopy and colorectal cancermortality: strong beliefs or strong facts? Am J Gastroen-terol 2010;105(7):1633–5.
11 Lee KJ, Inoue M, Otani T, et al. Gastric cancer screen-ing and subsequent risk of gastric cancer: a large-scalepopulation-based cohort study, with a 13-year follow-upin Japan. Int J Cancer 2006;118(9):2315–21.
12 Perz JF, Armstrong GL, Farrington LA, et al. The contri-butions of hepatitis B virus and hepatitis C virus infec-tions to cirrhosis and primary liver cancer worldwide.J Hepatol 2006;45(4):529–38.
13 Hepatitis B [Internet database]. WHO Media cen-tre. Available from: http://www.who.int/mediacentre/factsheets/fs204/en/index.html (last accessed May 6,2013).
14 Ahmed F, Foster GR. Global hepatitis, migration andits impact on Western healthcare. Gut 2010;59(8):1009–11.
15 Te HS, Jensen DM. Epidemiology of hepatitis B and Cviruses: a global overview. Clin Liver Dis 2010;14(1):1–21, vii.
16 Hepatitis C [Internet database]. WHO Media cen-tre. Available from: http://www.who.int/mediacentre/factsheets/fs164/en/index.html (accessed August 19,2011).
17 Viral Hepatitis Statistics and Surveillance [Internetdatabase]. Centers for Disease Control and Prevention(CDC). Available from: http://www.cdc.gov/hepatitis/Statistics/index.htm (accessed September 08, 2011).
18 Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer2006;118(12):3030–44.
19 Dubberke ER, Wertheimer AI. Review of current liter-ature on the economic burden of Clostridium difficileinfection. Infect Control Hosp Epidemiol 2009;30(1):57–66.
12
http://apps.who.int/ghodata/http://www.who.int/healthinfo/global_burden_disease/cod_2008_sources_methods.pdfhttp://globocan.iarc.frhttp://www.who.int/mediacentre/factsheets/fs204/en/index.htmlhttp://www.who.int/mediacentre/factsheets/fs164/en/index.htmlhttp://www.cdc.gov/hepatitis/Statistics/index.htmhttp://apps.who.int/ghodata/http://www.who.int/healthinfo/global_burden_disease/cod_2008_sources_methods.pdfhttp://www.who.int/healthinfo/global_burden_disease/cod_2008_sources_methods.pdfhttp://www.who.int/mediacentre/factsheets/fs204/en/index.htmlhttp://www.who.int/mediacentre/factsheets/fs164/en/index.htmlhttp://www.cdc.gov/hepatitis/Statistics/index.htm