Edited by Karen Marshall, Respiratory Nurse Consultant ...
5
Page 1 of 5 Observations Adults Assessment of respiration Edited by Karen Marshall, Respiratory Nurse Consultant, Newcastle-upon-Tyne NHS Hospitals Foundation Trust ©2021 Clinical Skills Limited. All rights reserved The function of the respiratory system is to supply the body’s tissues with sufficient oxygen for effective metabolism, while removing waste carbon dioxide. Respiration can be divided into two components: “external” respiration is the drawing of air into the lungs, while “internal” respiration is the process whereby the gases in the lungs are exchanged with those in the blood and tissues (see “Gaseous exchange in the lungs”, below). Assessment of respiration is a routinely performed but complex skill (Smith et al., 2011). The healthcare professional can assess external respiration by carefully recording the respiratory rate, the depth and pattern of breathing and, importantly, how much effort the patient makes to breathe. For example, note whether the patient finds it hard to talk because of difficulty in breathing. Observe whether the patient is using the accessory muscles in their neck to breathe, as this is a sign of laboured breathing. The accessory muscles assist with deep breathing; they should not normally be used while a person is at rest. To assess internal respiration, consider factors such as skin pallor or cyanosis (a bluish colour of the skin). Poor tissue oxygenation is one possible cause of restlessness or confusion, although there are many causes for this behaviour. A pulse oximeter can quickly assess the oxygen saturation of haemoglobin delivered to the tissues (usually referred to as “sats”). Oxygen saturation is regarded as the “fifth vital sign” (O’Driscoll et al., 2017). It is best practice to set a target oxygen saturation when a patient is admitted to hospital; the recommended target range for acutely ill patients is 95–98 per cent, or 88–92 per cent for patients at risk of hypercapnic respiratory failure such as those with chronic obstructive pulmonary disease (COPD) (O’Driscoll et al., 2017). It is important not to neglect to take the respiratory rate with other observations; this is particularly true for critically ill patients and those with respiratory or cardiovascular conditions. Changes in respiratory rate, along with changes in heart rate, are the most sensitive and earliest indicators of a patient’s deterioration in condition (Rolfe, 2019). It is therefore important to record the respiratory rate on admission as a baseline observation and to record it again when other observations are taken, particularly if you suspect a change in either the respiratory pattern or the overall condition of the patient. A “track and trigger” system, such as NEWS2, will alert those recording clinical observations to any worsening of the patient’s condition, so that they can inform appropriate staff (NHS Improvement, 2018; O’Driscoll et al., 2017; RCP, 2017). Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution. When you first assess the patient, check that you can see the chest moving clearly enough for you to record the rate. You may place the patient’s arm on their chest, with your hand between arm and chest, as in the illustration, while you take other observations such as the pulse. In this way, when you come to assess respirations, your hand is already in place. You can move smoothly from assessing the pulse to assessing respiration and the patient should not notice. Breathing is normally involuntary; however if the patient knows that you are recording their breathing, they will become aware of it and may alter their breathing pattern and rate. Although there is no agreement on a standardised approach (Smith et al., 2011), it is considered best practice to record the respiratory rate for a full minute, as this will allow more time to detect alterations in the breathing pattern (Wheatley, 2018). Oxygen and carbon dioxide move between the alveoli (air sacs) in the lungs and the capillaries by diffusing through the alveolar membrane and capillary walls. Oxygen moves from the alveoli where its concentration is high into the capillaries where it is lower; in other words, it is “moving down a concentration gradient”. Carbon dioxide moves from the capillaries to the alveoli by the same process and is exhaled. The concentration gradient of oxygen is steeper than that of carbon dioxide so its diffusion is more rapid. 13.7 kPa Oxygen 5.3 kPa 5.3 kPa 5.9 kPa Carbon dioxide Alveolus Capillary Gaseous exchange in the lungs Basic technique Select your PPE according to national guidance, local policy and your risk assessment !
Transcript of Edited by Karen Marshall, Respiratory Nurse Consultant ...
Page 1 of 5
ObservationsAdults
Assessment of respirationEdited by Karen Marshall, Respiratory Nurse Consultant, Newcastle-upon-Tyne NHS Hospitals Foundation Trust
©2021 Clinical Skills Limited. All rights reserved
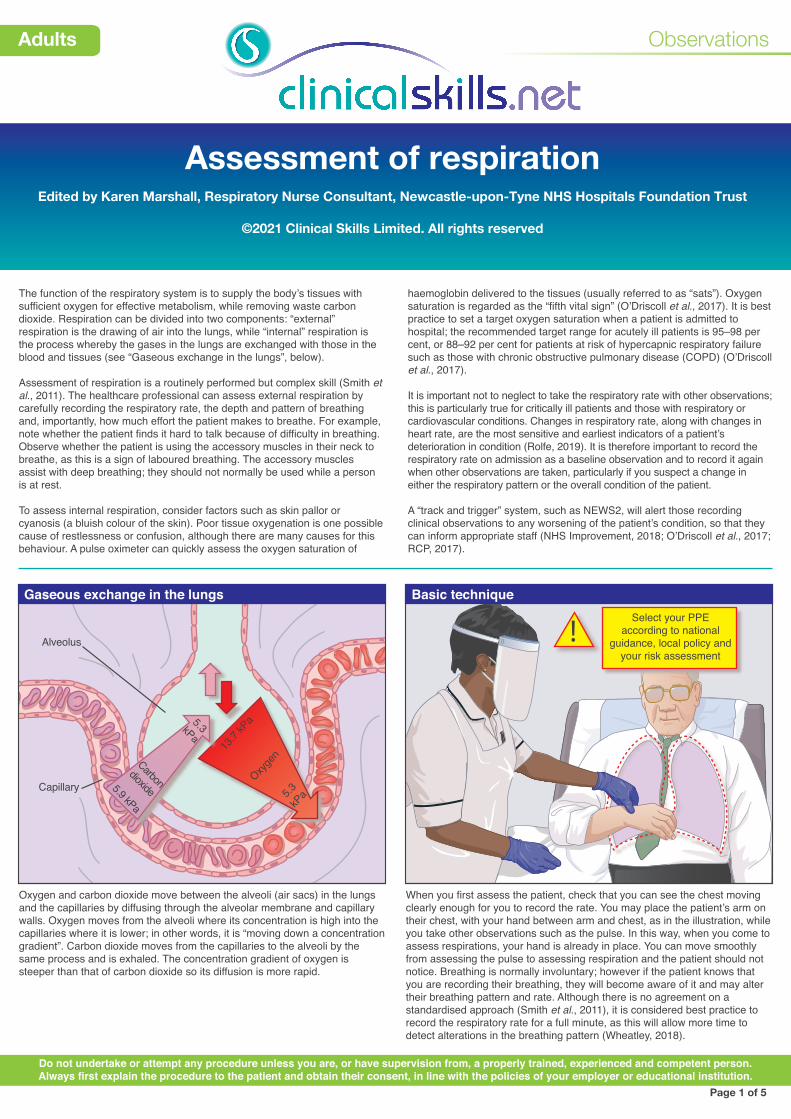
The function of the respiratory system is to supply the body’s tissues with sufficient oxygen for effective metabolism, while removing waste carbon dioxide. Respiration can be divided into two components: “external” respiration is the drawing of air into the lungs, while “internal” respiration is the process whereby the gases in the lungs are exchanged with those in the blood and tissues (see “Gaseous exchange in the lungs”, below).
Assessment of respiration is a routinely performed but complex skill (Smith et al., 2011). The healthcare professional can assess external respiration by carefully recording the respiratory rate, the depth and pattern of breathing and, importantly, how much effort the patient makes to breathe. For example, note whether the patient finds it hard to talk because of difficulty in breathing. Observe whether the patient is using the accessory muscles in their neck to breathe, as this is a sign of laboured breathing. The accessory muscles assist with deep breathing; they should not normally be used while a person is at rest.
To assess internal respiration, consider factors such as skin pallor or cyanosis (a bluish colour of the skin). Poor tissue oxygenation is one possible cause of restlessness or confusion, although there are many causes for this behaviour. A pulse oximeter can quickly assess the oxygen saturation of
haemoglobin delivered to the tissues (usually referred to as “sats”). Oxygen saturation is regarded as the “fifth vital sign” (O’Driscoll et al., 2017). It is best practice to set a target oxygen saturation when a patient is admitted to hospital; the recommended target range for acutely ill patients is 95–98 per cent, or 88–92 per cent for patients at risk of hypercapnic respiratory failure such as those with chronic obstructive pulmonary disease (COPD) (O’Driscoll et al., 2017).
It is important not to neglect to take the respiratory rate with other observations; this is particularly true for critically ill patients and those with respiratory or cardiovascular conditions. Changes in respiratory rate, along with changes in heart rate, are the most sensitive and earliest indicators of a patient’s deterioration in condition (Rolfe, 2019). It is therefore important to record the respiratory rate on admission as a baseline observation and to record it again when other observations are taken, particularly if you suspect a change in either the respiratory pattern or the overall condition of the patient.
A “track and trigger” system, such as NEWS2, will alert those recording clinical observations to any worsening of the patient’s condition, so that they can inform appropriate staff (NHS Improvement, 2018; O’Driscoll et al., 2017; RCP, 2017).
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
When you first assess the patient, check that you can see the chest moving clearly enough for you to record the rate. You may place the patient’s arm on their chest, with your hand between arm and chest, as in the illustration, while you take other observations such as the pulse. In this way, when you come to assess respirations, your hand is already in place. You can move smoothly from assessing the pulse to assessing respiration and the patient should not notice. Breathing is normally involuntary; however if the patient knows that you are recording their breathing, they will become aware of it and may alter their breathing pattern and rate. Although there is no agreement on a standardised approach (Smith et al., 2011), it is considered best practice to record the respiratory rate for a full minute, as this will allow more time to detect alterations in the breathing pattern (Wheatley, 2018).
Oxygen and carbon dioxide move between the alveoli (air sacs) in the lungs and the capillaries by diffusing through the alveolar membrane and capillary walls. Oxygen moves from the alveoli where its concentration is high into the capillaries where it is lower; in other words, it is “moving down a concentration gradient”. Carbon dioxide moves from the capillaries to the alveoli by the same process and is exhaled. The concentration gradient of oxygen is steeper than that of carbon dioxide so its diffusion is more rapid.
mention NEWS2 chart (RCP, 2017)?
13.7
kPa
Oxyge
n5.3
kP
a
5.3kPa
5.9 kPaCarbon
dioxideAlveolus
Capillary
Norma Charles
Senior Practic
e
Development Nurse
Beckham & Victoria Hospitals
NHS Trust
NHS
Gaseous exchange in the lungs Basic techniqueSelect your PPE
according to national guidance, local policy and
your risk assessment!

NHS
The Royal Beckham and Victoria Trust
NHS Trust
Sarah Nader
Health Care Assistant
Expiry Date: 11/11/21
ID Number: 285113846
NHS
NHS
The Royal Beckham and Victoria Trust
NHS Trust
Sarah Nader
Health Care Assistant
Expiry Date: 11/11/21
ID Number: 285113846
NHS
Preparation of patient
Age
Newborn
2–12
Teenager
Adult
Rate (breaths/min)
30–50
20–30
12–20
12–18
Respiratory rates
Observations
Adults
Assessment of respiration Page 2
General respiratory observation Patient’s breath as a sign of health problems
Allow the patient to rest for about 5 minutes so that the assessment is a true reflection of the resting respiratory rate. You may need to expose the chest, so ensure privacy.
The respiratory rate varies with age, as shown in the chart above. Make a note of deviations from the patient’s normal baseline respiratory pattern, such as the depth or rhythm of breathing.
Remember to assess for the effects of internal respiration. Examine the colour of the skin, including the extremities, and the colour of the nail beds, for signs of pallor or cyanosis. Finger clubbing (shown) can be a sign of long-term cardiac or respiratory disease. The causes of this sign are poorly understood and it can be seen in a variety of conditions, or may have no clinical significance.
Note any unusual odour of the patient’s breath. Bad breath is often caused by poor oral hygiene but can also indicate various health problems.
An inspection of the chest and a review of the patient’s notes may reveal a variety of deformities, such as those shown above. In the normal chest, the sternum is usually flat, but the ribs and clavicles are prominent. Remember that, at rest and in normal breathing, accessory muscles should not be used. Breathing should cause a symmetrical rising and falling of the chest. A barrel chest is a physical sign particularly associated with chronic respiratory conditions such as emphysema; it also occurs in some populations who live at altitudes above 15,000 feet. Deformities of the spine can interfere with the mechanics of breathing.
Page 2 of 5
Do not undertake or attempt any procedure unless you have been assessed and signed off as competent by a properly trained, experienced and competent mentor. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Normallateral
Barrelchestlateral
Kyphosis Scoliosis
Inspection of the chest
Odour Indication
Sweet/fruity odour
Faecal odour
Ketoacidosis in diabetic patients
Intestinal obstruction
Signs of respiratory effort
Observations
Adults
Assessment of respiration Page 3
Airway: open the airway Breathing: look, listen and feel
Patterns of breathing
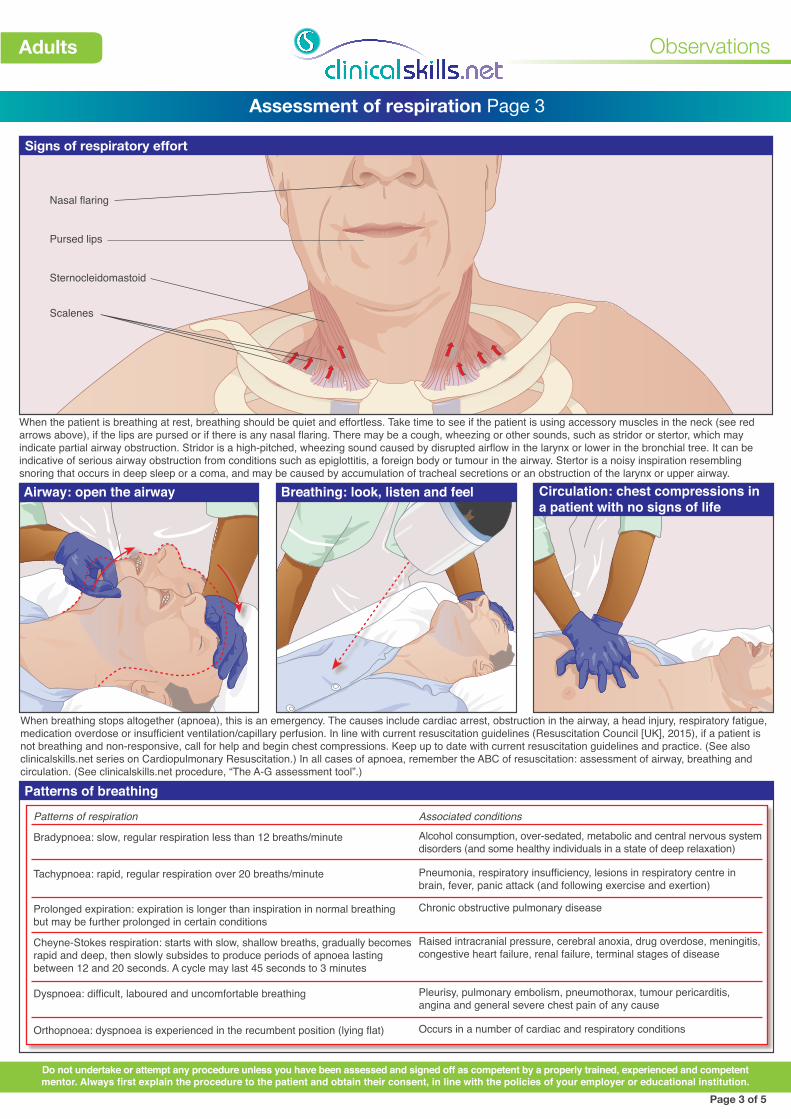
When the patient is breathing at rest, breathing should be quiet and effortless. Take time to see if the patient is using accessory muscles in the neck (see red arrows above), if the lips are pursed or if there is any nasal flaring. There may be a cough, wheezing or other sounds, such as stridor or stertor, which may indicate partial airway obstruction. Stridor is a high-pitched, wheezing sound caused by disrupted airflow in the larynx or lower in the bronchial tree. It can be indicative of serious airway obstruction from conditions such as epiglottitis, a foreign body or tumour in the airway. Stertor is a noisy inspiration resembling snoring that occurs in deep sleep or a coma, and may be caused by accumulation of tracheal secretions or an obstruction of the larynx or upper airway.
When breathing stops altogether (apnoea), this is an emergency. The causes include cardiac arrest, obstruction in the airway, a head injury, respiratory fatigue, medication overdose or insufficient ventilation/capillary perfusion. In line with current resuscitation guidelines (Resuscitation Council [UK], 2015), if a patient is not breathing and non-responsive, call for help and begin chest compressions. Keep up to date with current resuscitation guidelines and practice. (See also clinicalskills.net series on Cardiopulmonary Resuscitation.) In all cases of apnoea, remember the ABC of resuscitation: assessment of airway, breathing and circulation. (See clinicalskills.net procedure, “The A-G assessment tool”.)
Page 3 of 5
Do not undertake or attempt any procedure unless you have been assessed and signed off as competent by a properly trained, experienced and competent mentor. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
Patterns of respiration
Bradypnoea: slow, regular respiration less than 12 breaths/minute
Tachypnoea: rapid, regular respiration over 20 breaths/minute
Prolonged expiration: expiration is longer than inspiration in normal breathing but may be further prolonged in certain conditions
Cheyne-Stokes respiration: starts with slow, shallow breaths, gradually becomes rapid and deep, then slowly subsides to produce periods of apnoea lasting between 12 and 20 seconds. A cycle may last 45 seconds to 3 minutes
Dyspnoea: difficult, laboured and uncomfortable breathing
Orthopnoea: dyspnoea is experienced in the recumbent position (lying flat)
Associated conditions
Alcohol consumption, over-sedated, metabolic and central nervous system disorders (and some healthy individuals in a state of deep relaxation)
Pneumonia, respiratory insufficiency, lesions in respiratory centre in brain, fever, panic attack (and following exercise and exertion)
Chronic obstructive pulmonary disease
Raised intracranial pressure, cerebral anoxia, drug overdose, meningitis, congestive heart failure, renal failure, terminal stages of disease
Pleurisy, pulmonary embolism, pneumothorax, tumour pericarditis, angina and general severe chest pain of any cause
Occurs in a number of cardiac and respiratory conditions
Sternocleidomastoid
Scalenes
Pursed lips
Nasal flaring
Circulation: chest compressions in a patient with no signs of life
CHANGE IF PINK
THERAPY EQUIPMENPIPELINE PROTECTE
0
20
4060
80
100
HIGH VACUUMHIGH FLOW
AIR
AIR
AIRo2
15
10
OXYGEN
LITRES
perMINUTE
5
1
o2
Oxygen
o2
15
10
5
1OXYGEN
per MINUTE
LITRES
o 2
Jenny
Murray
Senior Practice
Development Nurse
The Royal Victoria and Beckham Hospitals NHS
100100
8080
6060
4040
2020
D
OB:
5-S
ept-
1983
Sex:
F
N
HS
No:
460
955
786
7
6812
07
N
ame:
SAS
AY S
allam
CHANGE IF PINK
THERAPY EQUIPMENPIPELINE PROTECTE
0
20
4060
80
100
HIGH VACUUMHIGH FLOW
o2
15
10
OXYGEN
LITRES
perMINUTE
5
1
o2
Oxygen
o2
15
10
5
1OXYGEN
per MINUTE
LITRES
o 2
Jenny
Murray
Senior Practice
Development Nurse
The Royal Victoria and Beckham Hospitals NHS
DOB: 5-Sept-1983
Sex: F
N
HS No: 460 955 7867
681207
Name: SASAY Sallam
AIR
AIR
AIR
100100
8080
6060
4040
2020
Observations
Adults
Assessment of respiration Page 4
Page 4 of 5
Do not undertake or attempt any procedure unless you have been assessed and signed off as competent by a properly trained, experienced and competent mentor. Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
(b) Observation of sputum
Obtaining a sputum sample
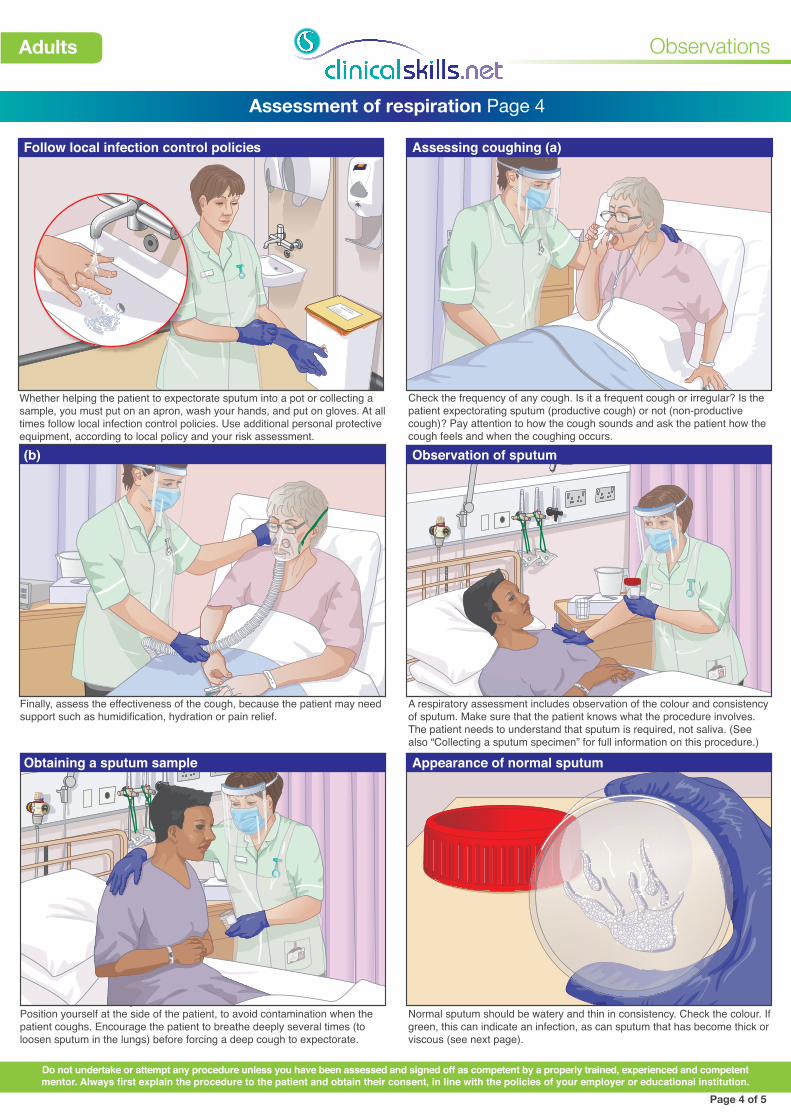
Check the frequency of any cough. Is it a frequent cough or irregular? Is the patient expectorating sputum (productive cough) or not (non-productive cough)? Pay attention to how the cough sounds and ask the patient how the cough feels and when the coughing occurs.
Finally, assess the effectiveness of the cough, because the patient may need support such as humidification, hydration or pain relief.
Appearance of normal sputum
A respiratory assessment includes observation of the colour and consistency of sputum. Make sure that the patient knows what the procedure involves. The patient needs to understand that sputum is required, not saliva. (See also “Collecting a sputum specimen” for full information on this procedure.)
Whether helping the patient to expectorate sputum into a pot or collecting a sample, you must put on an apron, wash your hands, and put on gloves. At all times follow local infection control policies. Use additional personal protective equipment, according to local policy and your risk assessment.
Position yourself at the side of the patient, to avoid contamination when the patient coughs. Encourage the patient to breathe deeply several times (to loosen sputum in the lungs) before forcing a deep cough to expectorate.
Normal sputum should be watery and thin in consistency. Check the colour. If green, this can indicate an infection, as can sputum that has become thick or viscous (see next page).
CLINICAL
WASTE ONLY
• No GLASS
• NO LIQUIDS
• NO GENERAL WASTE
Assessing coughing (a)Follow local infection control policies

Observations
Adults
Assessment of respiration Page 5
Page 5 of 5
Do not undertake or attempt any procedure unless you are, or have supervision from, a properly trained, experienced and competent person.Always first explain the procedure to the patient and obtain their consent, in line with the policies of your employer or educational institution.
100100
8080
6060
4040
2020
NEWS key0 1 2 3
DATETIME
≥2521-2418-2015-1712-14
9-11≤8
≥97 on O295-96 on O293-94 on O2
≥93 on air88-9286-8784-85≤83%
≥9694-95 92-93
≤91
A+BRespirationsBreaths/min
DATE OF BIRTH:
FULL NAME:
3
31
2
3
12
3
12
3
12
DATE OF ADMISSION:
A+BSpO2 Scale 1Oxygen saturation (%)
SpO2 Scale 2†
Oxygen saturation (%)Use Scale 2 if target range is 88-92% eg in hypercapnic respiratory failure
†ONLY use Scale 2 under the direction of a qualified clinician
25/6
Jill Payle21/05/1939
25/6 26/61700 2100 0700
(b) Mucopurulent sputum
Reporting and recording observations
In conditions such as bronchiectasis and pneumonia, there may be some discolouration.
Frothy sputum, sometimes pink in colour, can indicate pulmonary oedema.
Blood in the sputum may be frank blood (red); if the blood is old, it will be dark brown. Rusty coloured sputum may indicate bacterial pneumonia. Other causes include trauma, pulmonary embolus and carcinoma.
When sputum is mucoid with black specks, the patient may have suffered smoke inhalation.
It is usual to record the respiratory rate together with the oxygen saturation of haemoglobin (from pulse oximetry) and the fraction of inspired oxygen (if oxygen is given). Assess for any changes, look at the trends, and take action if you have any concerns.
(d) Mucoid sputum
Mucoid sputum appears white or opalescent. This is often seen in asthma or chronic bronchitis, but it does not mean that infection is present.
(e) Haemoptysis
(a) Frothy sputum (c) Black contamination
Dispose of the sputum container according to local infection prevention and control policy, remove and dispose of gloves and apron, and wash your hands when you have finished the procedure. Change the sputum pot regularly, at least every 12 hours.
Disposal and hygiene
(f) Purulent sputum
Purulent sputum is thick and viscous. There may be a range of colours, from yellow, dark green or brown to redcurrant jelly. A green colour generally indicates a chest infection.