Ectopic Pregnancy1.pptx

of 89
-
Upload
muhammad-abeesh -
Category
Documents
-
view
216 -
download
0
Transcript of Ectopic Pregnancy1.pptx
-
8/17/2019 Ectopic Pregnancy1.pptx
1/89
PREGNANCYECTOPIC
AREZ ESMAIL QADR
SHAMAL M. AZIZ
-
8/17/2019 Ectopic Pregnancy1.pptx
2/89
Normal pregnancy implantation
Pregnancy is the period during which a
woman carries a developing fetus normally
in the uterus, starting from conception
(fertilization of ova) until the baby born.
After ovulation the ovum is picked up by the
fimbria of fallopian tubes and then swept
by ciliary action towards the ampulla where
fertilization occurs.
As soon as the zygote develops it begins
dividing very rapidly, it remains in the fallopian
tube for 3 ! days untill reaches morula stage
("3# cell stage)
-
8/17/2019 Ectopic Pregnancy1.pptx
3/89
Normal pregnancyimplantation$he embryo proceeds through the isthmus to the uterine cavity for up
to %# hours, by the si&th day it enters the uterus and begins to
penetrate the decidua (endometrium) this is called implantation
which takes place within the uterine cavity in normal positioned
pregnancy .
$hen h' is produced by trophoblast, which can be detected in the
serum of the mother in the first week after implantation, its level
doubles every 3!" hours in normal healthy pregnancy starting
from * to *+ ,++, till reaching +++ -/0
1elay or obstruction of the passage of fertilized egg down the fallopian
tube to the uterus may result in implantation in the fallopian tube or
ovary or peritoneal cavity, this known as ectopic pregnancy which
eventually most fails to develop , and the h' fails to raise
dramatically as happens in the normal intra uterine pregnancy.
-
8/17/2019 Ectopic Pregnancy1.pptx
4/89
Normal pregnancyimplantation
-
8/17/2019 Ectopic Pregnancy1.pptx
5/89
Ectopic pregnancy ?
-
8/17/2019 Ectopic Pregnancy1.pptx
6/89
Ectopic pregnancyDefinition:
An ectopic pregnnc!, or ecc!"i" , is a complication of pregnancy 2ccurs when the
site of implantation is outside of the womb (uterine cavity) either in the tubes,ovaries or
abdominal cavity, ith rare e&ceptions, ectopic pregnancies are not viable, Pregnancy
can even occur in both the womb and the tube at the same time (heterotopic
pregnancy).
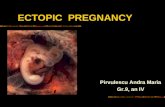
C#""ifiction:
tubal pregnancy4
$he vast ma5ority of ectopic pregnancies 6*6" 7 implant in the 8allopian tube,
among these4
"+7 in the ampulla
+7 in isthmus
* 7 in fimbria
#7 interstitial #7 in a rudimentary horn of a bicornuate uterus
-
8/17/2019 Ectopic Pregnancy1.pptx
7/89
classifcation $%Nont&'# ectopic pregnnc!
9are sites (#*7) are: $he ovaries,
broad ligaments,
Abdominal cavity and peritoneum
cervi&.
(%Heterotopic pregnnc!
in rare cases of ectopic pregnancy )*)+++, there may be two fertilized eggs,
one outside the uterus and the other inside. $his is called a heterotopic
pregnancy.
2ften the intrauterine pregnancy is discovered later than the ectopic, mainly
because of the painful emergency nature of ectopic pregnancies.
-
8/17/2019 Ectopic Pregnancy1.pptx
8/89
classifcation
;ince ectopic pregnancies are normally discovered and removed veryearly in the pregnancy, an ultrasound may not find the additional
pregnancy inside the uterus. hen h' levels continue to rise after
the removal of the ectopic pregnancy, there is the chance that a
pregnancy inside the uterus is still viable. $his is normally
discovered through an ultrasound
Although rare, heterotopic pregnancies are becoming more
common, likely due to increased use of -
-
8/17/2019 Ectopic Pregnancy1.pptx
9/89
Common sites for ectopicpregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
10/89
epidemiology
Inci,ence-
##/+++ live births
/+++ pregnancies
-n ;A from 6%+ = 66# , the risk *& increased from ! to 6 / +++
pregnancies
ft#it! rte :
fatality rate from ectopic pregnancies dropped almost 6+7 (from 3*.*
per +++ ectopics to 3." per +++ ectopics).
1espite the sharp improvement in the fatality rate by the end of thisperiod of time, ectopics were still the second leading cause of
maternal mortality in the ;A (accounting for #7 of all maternal
deaths in 6"%).
-
8/17/2019 Ectopic Pregnancy1.pptx
11/89
Why?
$he reason for the increase in ectopic pregnancy during this timeperiod is not entirely clear, but it was thought that the increase of
risk factors were responsible for a significant portion of the
increased number of cases of ectopic pregnancy.
-
8/17/2019 Ectopic Pregnancy1.pptx
12/89
Risk actors
Any mechanism that interferes with the normal function of fallopian
tube increases the risk of ectopic pregnancy
$he mechanism canbe4
Anatomical: scarring that blocks transport of the egg8unctional: impaired tubal mobility
-
8/17/2019 Ectopic Pregnancy1.pptx
13/89
Ri" /ctor Ri" 0
High Risk P-1
$ubal corrective surgery $ubal sterilization
Previous >P
-n utero 1>; e&posure
-1
1ocumented tubal pathology
Moderate Risk -nfertility
Previous genital infection
?ultiple partners
Slight risk
Previous pelvic or abdominal surgery
;moking
1ouching
-ntercourse before " weeks
#*
#.+
6.3
".*
".3
*.
!.#!*
3."#
#.*#
#.*3.%
#.
+.633."#.3#.*
.3.
.
-
8/17/2019 Ectopic Pregnancy1.pptx
14/89
Risk actors
)%Hi"tor! of pe#1ic infection
P-1 is the most common risk factor for ectopic pregnancy " folds increases the risk, due to destruction of the fallopian tubes.
'hlamydia (a common se&ually transmitted disease) and onorrhea
are both able to grow within the fallopian tubes and cause:
tremendous damage to the endosalpin& (lining of the inner tubal
lumen), #agglutination (sticking together) of the mucosal folds in the tube
3peritubal adhesions (scar tissue).
. the risk of an ectopic pregnancy is greater when the woman with the
infection is younger
2ther pelvic or lower abdominal infections can also result in pelvic
adhesions and an increase in the ectopic pregnancy rate (such as
appendicitis).
$he chances of another ectopic in the same fallopian tube also in the
other tube are increased *&
-
8/17/2019 Ectopic Pregnancy1.pptx
15/89
Risk actors
$%Hi"tor! of "&rger! on t2e f##opin t&'e" or 3it2in t2e pe#1i":
$ubal ligation in the past # years,hen a bilateral tubal ligation (tubes
tied) is followed by either an une&pected pregnancy (failed tubal
ligation) or is @reversed@ with a tubal reanastomosis (tubalreconstruction) there is an increased risk of a tubal ectopic
pregnancy.
hen a woman has a history of pelvic surgery that is associated with
significant adhesion formation (such as myomectomy) there is alsoan increased risk of an ectopic pregnancy.
-
8/17/2019 Ectopic Pregnancy1.pptx
16/89
Risk actors
(% Prior 2i"tor! of ectopic pregnnc!.
hen an ectopic pregnancy in the fallopian tube is treated conservatively
(by preserving the tube), there is a roughly + fold increase the risk of
recurrence in the same tube
4%Hi"tor! of I5D &"e. $he use of an -1 is a classic @risk factor@ forectopic pregnancy. Actually, all but the progesterone containing -1s
are relatively protective against ectopic pregnancy while the -1 is in
place. $hat is, the number of ectopic pregnancies in women using an
-1 for contraception is about one half that of women using no
contraception. owever, of -1 pregnancies there is a greater chance
of an ectopic location (3!7) since the number of intrauterine
pregnancies with an -1 in place is markedly reduced.
-
8/17/2019 Ectopic Pregnancy1.pptx
17/89
Risk actors
Additionally, -1s can be associated with infections of the uterine
cavity and fallopian tubes (especially 5ust after insertion) which can
independently increase the chance for an ectopic pregnancy..
$he reason for this increase in the nomber of >Ps with progesterone
-1 is not clear. A theory is that somehow the progesterone
enhances tubal implantation.
-
8/17/2019 Ectopic Pregnancy1.pptx
18/89
Risk actors
6%Hi"tor! of Diet2!#"ti#'e"tro# 7DES 8e9po"&re in &tero. $his drug is a is a synthetic nonsteroidal estrogen that was used for
certain conditions, including breast and prostate cancers ,8rom
about 6!+ to 6%+, 1>; was given to pregnant women under the
mistaken belief it would reduce the risk of pregnancy complicationsand losses
0ater researches has shown that this drug has many bad medical
effects and female babies of women who used it were at risk of
developmental abnormalities of the genital system
$heir tubes are more likely to be abnormal and predispose to ectopicpregnancy, these females were known as 1>; daughters
-
8/17/2019 Ectopic Pregnancy1.pptx
19/89
Risk actors
%Hi"tor! of ,e"tr&ction of t2e &terine c1it! or #ining.
;uch as history of uterine synechiae (scar tissue) from previous
surgery (like endometrial ablation for dysfunctional bleeding ) or
presence of multiple submucosal fibroid tumors this cause a largerpercentage of the pregnancies to implant in a space other than the
uterine cavity.
;imilar to the situation with -1s, the total ectopic pregnancy rate may
not be increased but when a pregnancy does occur the reduced
likelihood of an intrauterine pregnancy increases the relativepercentage of ectopic pregnancies.
-
8/17/2019 Ectopic Pregnancy1.pptx
20/89
Risk actors
;%Hi"tor! of non%infectio&" pe#1ic inf#
-
8/17/2019 Ectopic Pregnancy1.pptx
21/89
Risk actors
>%5"e of ""i"te, repro,&cti1e tec2no#og! 7"&c2 " I?/ 7in 1etroferti#i@tion8 n, GI/T 7g
-
8/17/2019 Ectopic Pregnancy1.pptx
22/89
Tubal pregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
23/89
Pathophysiology
$he trophoblast develops in the fertilized ovum and invades deeplyinto the tubal wall.
8ollowing implantation, the trophoblast produces h' which
maintains the corpus luteum.
$he corpus luteum produces oestrogen and progesterone which
change the secretory endometrium into decidua. $he uterusenlarges up to " weeks and becomes soft.
$he tubal pregnancy does not usually proceed beyond "+weeks due
to4
C lack of decidual reaction in the tube,
C the thin wall of the tube,
C the inadeBuacy of tubal lumen,
C bleeding in the site of implantation as trophoblast invades.
-
8/17/2019 Ectopic Pregnancy1.pptx
24/89
Pathophysiology
;eparation of the gestational sac from the tubal wall leads to its
degeneration, and fall of h' level, regression of the corpus luteum
and subseBuent drop in the oestrogen and progesterone level.
$his leads to separation of the uterine decidua with uterine bleeding.
/te of t&'# pregnnc!
$ubal mole
$ubal abortion
$ubal rupture
-
8/17/2019 Ectopic Pregnancy1.pptx
25/89
Fate o tubal pregnancy
)% T&'#
-
8/17/2019 Ectopic Pregnancy1.pptx
26/89
Fate o tubal pregnancy
-f e&pulsion was complete the bleeding usually ceases but it may
continue due to incomplete separation or bleeding from the
implantation site.
-
8/17/2019 Ectopic Pregnancy1.pptx
27/89
Fate o tubal pregnancy
(%T&'# r&pt&re:?ore common if implantation occurs in the narrower portion of the tube
which is the isthmus.
9upture may occur in the
antimesenteric border of the tube.
sually profuse bleeding occurs D
intraperitoneal haemorrhage.
-f rupture occurs in the mesenteric border
of the tube, broad ligament haematomawill occur.
-
8/17/2019 Ectopic Pregnancy1.pptx
28/89
presentation
>arly symptoms are either absent or subtle. 'linical presentation of
ectopic pregnancy occurs at a mean of %.# weeks after the last
normal menstrual period, with a range of * to " weeks
$he most common presenting symptoms that are suggestive for >Pare4
-
8/17/2019 Ectopic Pregnancy1.pptx
29/89
Clinical traid !"s#
Amenorhea
ectopic
pregnancy
Abdominal pain Abnormal vaginal bleeding
-
8/17/2019 Ectopic Pregnancy1.pptx
30/89
symptoms
Pin n, ,i"co
-
8/17/2019 Ectopic Pregnancy1.pptx
31/89
symptoms
#ee,ing
-
8/17/2019 Ectopic Pregnancy1.pptx
32/89
signs Gener# e9
-
8/17/2019 Ectopic Pregnancy1.pptx
33/89
signs
?gin# e9
-
8/17/2019 Ectopic Pregnancy1.pptx
34/89
diagnosis
$he diagnosis can be difficult
Gour doctor may perform some tests to help confirm suspected ectopic
pregnancy including:
1etailed history of (cycle, pregnancy, P-1,infertility, gynaecological
surgery, contraceptionF)Proper general, abdominal, vaginal e&amination and vital signs
-nvestigations4 including
-
8/17/2019 Ectopic Pregnancy1.pptx
35/89
$iagnosis
).2or
-
8/17/2019 Ectopic Pregnancy1.pptx
36/89
$iagnosis
Proge"terone
$he second most common hormone after h' in pregnancy is
progesterone.
enerally, a progesterone concentration of greater than #* ng/m0 is
highly correlated with a normal intrauterine pregnancy while aconcentration of less than * ng/m0 is highly correlated with an
abnormal and nonviable pregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
37/89
$iagnosis
$%5#tr"o&n,
-n general, a positive Hh' test with empty uterus by sonar I adne&ial
mass indicates ectopic pregnancy.
1iscriminatory h' zones4 1iagnosis of ectopic pregnancy is made if there is4
An empty uterine cavity by abdominal sonography with b h' value
above +++ m-/ml.
An empty uterine cavity by vaginal sonography with b h' value
above #+++ m-/ml.
-
8/17/2019 Ectopic Pregnancy1.pptx
38/89
%ltrasound
-
8/17/2019 Ectopic Pregnancy1.pptx
39/89
$iagnosis(%C,ocente"i"
in this test, a needle is inserted into the space at the top of the vagina, behindthe uterus and in front of the rectum to aspirate fluid and
1etermines if there is blood in the space behind the uterus
-f nonclotting blood is aspirated from the 1ouglas pouch , intraperitoneal
haemorrhage is diagnosed. Eut if not, ectopic pregnancy cannot be
e&cluded.
-
8/17/2019 Ectopic Pregnancy1.pptx
40/89
$iagnosis
4%#pro"cop! or #proto
ectopic pregnancy. 2ften if a tubal abortion or tubal rupture has occurred.0aparoscopy4 an endoscope is inserted through a small incision in the
womanJs abdomen
$his allows you to see the fallopian tubes and other organs
$his takes place in an operating room with anaesthesia
-
8/17/2019 Ectopic Pregnancy1.pptx
41/89
%ncommon &ites o EctopicPregnancy
'ornual angular pregnancy#Pregnancy occurs in the blind rudimentary horn of a bicornuate
uterus.
3'ervical pregnancy
!2varian pregnancy
*Abdominal (peritoneal) pregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
42/89
Cornual angular pregnancy
-t is implantation in the interstitial portion of the tube.
-t is uncommon but dangerous because when rupture occurs bleeding
is severe and disruption is e&tensive that needs hysterectomy.
-n some cases, the pregnancy is e&pelled into the uterus and rupture
does not occur.
'''(reeli)edoctor(co
-
8/17/2019 Ectopic Pregnancy1.pptx
43/89
-
8/17/2019 Ectopic Pregnancy1.pptx
44/89
Cer)ical pregnancy -mplantation in the substance of the cervi& below the level of uterine
vessels.?ay cause severe
vaginal bleeding.
'an be diagnosed by
trans vaginal ultrasound
-
8/17/2019 Ectopic Pregnancy1.pptx
45/89
*)arian pregnancy
Aetio#og!:
K Pelvic adhesions.
K 8avourable ovarian surface for implantation as in ovarian
endometriosis.
Pt2ogene"i":
K 8ertilization of the ovum inside the ovary or,
K implantation of the fertilized ovum in the ovary.
-
8/17/2019 Ectopic Pregnancy1.pptx
46/89
*)arian pregnancy
Spiege#'erg criteri for diagnosis of ovarian pregnancy4
K $he gestational sac is located in the region of the ovary,
K the ectopic pregnancy is attached to the uterus by the ovarian
ligament,
K ovarian tissue in the wall of the gestational sac is proved
histologically,
K the tube on the
involved side is intact.
'''(reeli)edoctor(co
"bd i l i l#
-
8/17/2019 Ectopic Pregnancy1.pptx
47/89
"bdominal peritoneal#pregnancy
T!pe":
Pri
-
8/17/2019 Ectopic Pregnancy1.pptx
48/89
"bdominal peritoneal# pregnancy
Digno"i":
Hi"tor!: of amenorrhoea followed by an attack of lower abdominal
pain and slight vaginal bleeding which subsided spontaneously.
A',o
-
8/17/2019 Ectopic Pregnancy1.pptx
49/89
"bdominal peritoneal# pregnancySpeci# in1e"tigtion":
P#in %r!4 shows abnormal lie. -n lateral view, the foetusovershadows the maternal spines .
5#tr"o&n,: shows no uterine wall around the foetus
Mgnetic re"onnce i
-
8/17/2019 Ectopic Pregnancy1.pptx
50/89
DI//ERENTIAL
DIAGNOSISDD
-
8/17/2019 Ectopic Pregnancy1.pptx
51/89
-
8/17/2019 Ectopic Pregnancy1.pptx
52/89
SepticAbortion
'reatenedAbortion
Pyosalpin)
PelvicAbcess
'*isted#varian
Cyst
Acute pelvicinflammatory
disease
Rupture of+ollicle or
Corpus&uteum Cyst
Degeneratingleiomyoma
RetrovertedGravidUterus
(2) Gynecologic disorders
-
8/17/2019 Ectopic Pregnancy1.pptx
53/89
R9
TREATMENT
% c t o p i c
-
8/17/2019 Ectopic Pregnancy1.pptx
54/89
• % , P % C ' A " '
M A " A G % M % " '
- • M % D I C A &
M A " A G % M % " '
. • S U R G I C A & M A " A G % M % " '
Tret
-
8/17/2019 Ectopic Pregnancy1.pptx
55/89
EPECTANT
MANAGEMENT
-
8/17/2019 Ectopic Pregnancy1.pptx
56/89
M Criteri for "e#ection
= asymptomatic women no evidence
of rupture or hemodynamicinstability
= less than ++ ml fluid in the pouch
of 1ouglas
= h' less than +++ iu/l at initialpresentation
= Adne&al mass less than 3cm
= they should ob5ective evidence of
resolution, such as declining bh'levels.
= $hey must be fully compliant and
must be willing to accept the
potential risks of tubal rupture.
-
8/17/2019 Ectopic Pregnancy1.pptx
57/89
= +nitial ollo' up
M t'ice 'eekly 'ith serialhC,measurements
M 'eekly by trans)aginal e-aminations
= .y the frst 'eek
M drop in /C, le)el
M "dne-al mass si0e
=*ther'ise reassess the options1edical2&urgical#
= + the all o /C, 3 reduction in si0e oadne-al mass satisatory
M 'eekly hC, and trans)aginal ultrasounde-aminations
M#"I'#RI"G
-
8/17/2019 Ectopic Pregnancy1.pptx
58/89
M 789:6; o pregnancies o unkno'nlocation resol)e spontaneously 'ithe-pectant management
M Ectopic pregnancy 'as subse; o cases opregnancy o unkno'n location
M +nter)ention has been sho'n to be
re
-
8/17/2019 Ectopic Pregnancy1.pptx
59/89
MEDICAL
MANAGEMENT
$
-
8/17/2019 Ectopic Pregnancy1.pptx
60/89
M &election criteria
= 1inimal symptoms 3 The patient must behemodynamically stable
= no signs or symptoms o acti)e bleeding orhaemoperitoneum(
= "bsence o oetal heart beat
= Normal F.C@%3Eurea 3 electrolytes#@AFTli)erunction tests#
M E-clusion criteria
= "ny hepatic dysunction@ thrombocytopeniaplatelet count 4=66@666#@ blood dyscrasiaWCC
45666 cells cm!#( = $iBculty or un'illingness o patient orprolonged ollo'up a)erage ollo'up !8days#(
= Ectopic mass D!(8cm
= The presence o cardiac acti)ity in an ectopicpregnancy
CRI'%RIA for M%DICA& MA"AG%M%"'
-
8/17/2019 Ectopic Pregnancy1.pptx
61/89
• M e t ( o t r e ) a t eS$S'%MIC
• i n j e c t i o n s o f p r o s t a g l a n d i n s , p o t a s s i u m c h l o r i d e O R
h y p e r o s m o l a r g l u c o s e O R l o c a l m e t h o t r e x a t e
CA&&$
-
8/17/2019 Ectopic Pregnancy1.pptx
62/89
-
8/17/2019 Ectopic Pregnancy1.pptx
63/89
-
8/17/2019 Ectopic Pregnancy1.pptx
64/89
AD0IC%S
M Patient should be gi)en inormation onpreerably'ritten#
= Need or urther treatment
= "d)erse eects
M Women should be able to return easily or
assessment at any time during ollo'upM "d)ice
= a)oid se-ual intercourse during treatment
= to maintain uid intake
= use reliable contraception or three months
ater methotre-ate has been gi)en@ barrier orhormonal#
= ")oid e-posure to sunlight(
M G ")oid alcohol and )itamin preparationscontaining olic acid until the hormone le)el isback to 0ero(
M ")oid aspirin or drugs such as +buproen or
-
8/17/2019 Ectopic Pregnancy1.pptx
65/89
= 6+7 successful treatment with single dose
regime.
= 9ecurrent ectopic pregnancy rate + = #+7.
= $ubal patency appro&imately "+7.
= ! 7 of medical management second dose of
methotre&ate
= %*7 would e&perience abdominal pain
separation pain. $his usually occurs between
day 3%
= +7 would finally reBuire surgical management
*%TC*1E
-
8/17/2019 Ectopic Pregnancy1.pptx
66/89
-
8/17/2019 Ectopic Pregnancy1.pptx
67/89
S5RGICALMANAGEMENT
(
-
8/17/2019 Ectopic Pregnancy1.pptx
68/89
-
8/17/2019 Ectopic Pregnancy1.pptx
69/89
E1ER,ENC H
-
8/17/2019 Ectopic Pregnancy1.pptx
70/89
-
8/17/2019 Ectopic Pregnancy1.pptx
71/89
M et help call senior /'onsultant on call
M AE' of resuscitation
= give facial o&ygen
= ;ite two -< lines , commence -< fluids (crystalloid) = ;end blood for 8E', 'lotting screen and crossmatch at least ! units
of blood.
M insert indwelling catheter
M arrange theatre for laparotomy
M whilst awaiting transfer to theatre continue fluid resuscitation and ensure
intensive monitoring of haemodynamic state
M do not wait for EP and pulse to normalise prior to transferresuscitation
and surgery need to go hand in hand.
M Pfannensteil incision,
M salpingectomy and wash out of abdomen
M assess bloods /consider '
-
8/17/2019 Ectopic Pregnancy1.pptx
72/89
Aaparascopy *R laparatomy??
M 0aparoscopy has become the recommended approach inmost cases.
M 0aparotomy is usually reserved for patients4
who are hemodynamically unstable
patients with cornual ectopic pregnancies.
for surgeons ine&perienced in laparoscopy and in patients
where laparoscopic approach is difficult
-
8/17/2019 Ectopic Pregnancy1.pptx
73/89
-
8/17/2019 Ectopic Pregnancy1.pptx
74/89
Aaparoscopy
• Aess intraoperati)e
blood loss
• &horter operation time
• &horter hospital stay
• Ao'er analgesicre
-
8/17/2019 Ectopic Pregnancy1.pptx
75/89
Salpingectomy #R Salpingotomy 11
M S#pingecto
where there is tubal rupture
M S#pingoto
-
8/17/2019 Ectopic Pregnancy1.pptx
76/89
&alpingectomy &alpingotomy
•
There may be a highersubse
-
8/17/2019 Ectopic Pregnancy1.pptx
77/89
Per"i"tent trop2o'#"t
M hen salpingotomy is done, protocols should
be in place for the identification and treatment
of women with persistent trophoblast.
M ?onitoring serum ' levels would help to
identify the persistent trophoblast.
M ?ost >asily $reated ith ?$O
-
8/17/2019 Ectopic Pregnancy1.pptx
78/89
H e t e r o t r o p i c
C e r 1
i c # A ' ,
o
-
8/17/2019 Ectopic Pregnancy1.pptx
79/89
%vacuation and cervical pac2ing *itaemostatic agent as 3brin glue andgau4e5
Arterial emboli4ation
If bleeding continues or e)tensiverupture occurs ysterectomy isneeded5
Cer)ical pregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
80/89
M 0aparotomy and inoculation of the
ectopic pregnancy and
reconstruction of the ovary if
possible. 2therwise, removal of theaffected ovary is indicated.
M 2varian cystectomy is the
preferred treatment
M $reatment with ?$O andprostaglandin in5ection has also
been reported
*)arian pregnancy
-
8/17/2019 Ectopic Pregnancy1.pptx
81/89
/ i
-
8/17/2019 Ectopic Pregnancy1.pptx
82/89
/eterotropic pregnancy
M 1epends upon
the state of the
woman
and the skill ofthe doctor.
M .;urgical
0 i th id l i l th d t
http://www.womens-health.co.uk/diaglap.asphttp://www.womens-health.co.uk/diaglap.asp
-
8/17/2019 Ectopic Pregnancy1.pptx
83/89
M 0aparoscopy is the ideal surgical method to
remove an ectopic pregnancy before it ruptures
without interrupting the viable pregnancy. Although the intrauterine pregnancy can still
survive if the ectopic pregnancy ruptures, there
is an increased danger of miscarriage. $he
surgery must be done with great skill and it isimportant that bleeding be addressed Buickly.
?edical therapies include in5ecting the ectopic
pregnancy in order to terminate the gestation.
" ti $
http://www.womens-health.co.uk/diaglap.asphttp://www.womens-health.co.uk/miscarr.asphttp://www.womens-health.co.uk/miscarr.asphttp://www.womens-health.co.uk/diaglap.asp
-
8/17/2019 Ectopic Pregnancy1.pptx
84/89
"nti $
M Non "en"iti@e, 3o
-
8/17/2019 Ectopic Pregnancy1.pptx
85/89
"$I+CE
M Lot using -'1
M Lot using progesterone only pills
M $reatment for any P-1
M 8ollow up by ' that should disappear after month
M 1o ; after !+ day to see patency of the tube
Mse barrier method of contraceptionM $iming of pregnancy, visit specialist in any
missed period
C*1PA+C"T+*N
-
8/17/2019 Ectopic Pregnancy1.pptx
86/89
M 9ecurrence of ectopic
M -nfertility
M ;hock N death
M $ubal rupture N organ damageM Psychological
M ;urgical 9&
M ?edical 9&
C*1PA+C"T+*N
Progno"i"
-
8/17/2019 Ectopic Pregnancy1.pptx
87/89
Progno"i"
M 8ertility following ectopic pregnancy
depends upon several factors, the most
important of which is a prior of infertility.
$he treatment choice history , whethersurgical or nonsurgical, also plays a role.
8or e&le, the rate of intrauterine
pregnancy may be higher following
methotre&ate compared to surgicaltreatment. 9ate of fertility may be better
following salpingostomy than
salpingectomy.
Reference
http://en.wikipedia.org/wiki/Infertilityhttp://en.wikipedia.org/wiki/Infertility
-
8/17/2019 Ectopic Pregnancy1.pptx
88/89
Reference
=(,ynecology 3 obstetrci by Tenteachers =th edition
5(RC*, guidelines Royal college oobstetric 3 gynecology#!("C*,"merican college oobstetric 3 gynecology#
7("&R1"merican society oreproducti)e medicine#8(Wikipedia (comJ(Ai)emedicine(com:($r("braham laparascopy Iideo#
-
8/17/2019 Ectopic Pregnancy1.pptx
89/89
'/A"6
$#U