
Ectopic eruption of the maxillary central permanent
7
VOLUME 37 • NUMBER 9 • OCTOBER 2006 677 QUINTESSENCE INTERNATIONAL Tooth eruption is the axial movement of a tooth through an alveolar process, from its intraosseous development position to occlu- sion with the opposing tooth. 1 During this phase various disturbances can occur, among them ectopic eruption, which is defined as a deviation from the normal erup- tion pattern, making the tooth erupt out of position, 1–6 and possibly causing resorption of adjacent primary teeth. 4,6–13 According to the degree of resorption, these teeth may exfoliate precociously or be indicated for extraction, with or without the presence of painful symptoms. 2 Ectopic eruption may be reversible or irre- versible. In the first case, it is resolved sponta- neously when the tooth erupts in its normal position. In the second case, the tooth remains retained until the precocious exfolia- tion of the primary tooth involved or treatment is begun. 2,3,6,7,10–12,14,15 In the literature, the preva- lence of ectopic eruption of maxillary perma- nent first molars varies from 3.1% 16 to 4.3%. 2 Of these eruptions, 59% are reversible and 41% are irreversible. 2 In individuals with a cleft lip and/or palate, the prevalence of ectopic eruption increases to around 20.0% 17 to 21.8%. 8 For the mandibular permanent first molars, the occurrence is more rare, 4,14,18 as for the maxillary permanent central incisors. There is no consensus about which sex is most affected, 10,16 as some authors indicate females, 1,8 and others males. 2,6 Ectopic eruption of the maxillary central permanent incisors and mandibular first permanent molars: Report of an unusual case Luciana Pomarico, DDS, MSD 1 / Laura Guimarães Primo, DDS, MSD, PhD 2 /Denise Noce, DDS 3 Ectopic eruption is a disturbance in which the tooth does not follow its usual course. Among its more important etiologic factors are macrodontism, shortened arch length, pos- terior positioning of the maxilla, atypical eruption angle, and genetic factors. This article reports a rare case of ectopic eruption of 4 permanent teeth, maxillary central incisors and mandibular first molars, in a child aged 7 years and 11 months, in which the treatment consisted of extracting the maxillary primary central incisors and making an orthodontic intervention on the mandibular arch. A bilateral fixed appliance containing 2 hooks with loops, 1 buccal and the other lingual, was placed on the mandibular primary first molars. The hooks were activated in a niche made of light-curing resin on the occlusal surface of the mandibular permanent molars, to bring about the distal drift of these teeth. After 6 months, complete eruption of the mandibular permanent molars occurred, and a slight displacement of the maxillary permanent central incisors toward the median line was noted. The importance of early, adequate treatment is discussed. (Quintessence Int 2006;37:677–683) Key words: tooth eruption, ectopic; orthodontics, interceptive; dentition, permanent; molar; incisor; pediatric dentistry 1 Assistant Professor of Pediatric Dentistry, Veiga de Almeida University, Rio de Janeiro, Brazil. 2 Associate Professor, Department of Pediatric Dentistry and Orthodontics, Federal University of Rio de Janeiro, School of Dentistry, Rio de Janeiro, Brazil. 3 Pedodontist and Orthodontist, Department of Pediatric Dentistry and Orthodontics, Federal University of Rio de Janeiro, School of Dentistry, Rio de Janeiro, Brazil. Reprint requests: Dr Luciana Pomarico, Praia do Flamengo 370/202 – Flamengo, 22210-030 Rio de Janeiro, RJ, Brazil. Fax: 55 (21) 2551-4354. E-mail: [email protected]
Transcript of Ectopic eruption of the maxillary central permanent

VOLUME 37 • NUMBER 9 • OCTOBER 2006 677
QUINTESSENCE INTERNATIONAL
Tooth eruption is the axial movement of a
tooth through an alveolar process, from its
intraosseous development position to occlu-
sion with the opposing tooth.1 During this
phase various disturbances can occur,
among them ectopic eruption, which is
defined as a deviation from the normal erup-
tion pattern, making the tooth erupt out of
position,1–6 and possibly causing resorption
of adjacent primary teeth.4,6–13
According to the degree of resorption,
these teeth may exfoliate precociously or be
indicated for extraction, with or without the
presence of painful symptoms.2
Ectopic eruption may be reversible or irre-
versible. In the first case, it is resolved sponta-
neously when the tooth erupts in its normal
position. In the second case, the tooth
remains retained until the precocious exfolia-
tion of the primary tooth involved or treatment
is begun.2,3,6,7,10–12,14,15 In the literature, the preva-
lence of ectopic eruption of maxillary perma-
nent first molars varies from 3.1%16 to 4.3%.2
Of these eruptions, 59% are reversible and
41% are irreversible.2 In individuals with a cleft
lip and/or palate, the prevalence of ectopic
eruption increases to around 20.0%17 to
21.8%.8 For the mandibular permanent first
molars, the occurrence is more rare,4,14,18 as for
the maxillary permanent central incisors.
There is no consensus about which sex is
most affected,10,16 as some authors indicate
females,1,8 and others males.2,6
Ectopic eruption of the maxillary central permanent incisors and mandibular first permanent molars: Report of an unusual caseLuciana Pomarico, DDS, MSD1/
Laura Guimarães Primo, DDS, MSD, PhD2/Denise Noce, DDS3
Ectopic eruption is a disturbance in which the tooth does not follow its usual course.
Among its more important etiologic factors are macrodontism, shortened arch length, pos-
terior positioning of the maxilla, atypical eruption angle, and genetic factors. This article
reports a rare case of ectopic eruption of 4 permanent teeth, maxillary central incisors and
mandibular first molars, in a child aged 7 years and 11 months, in which the treatment
consisted of extracting the maxillary primary central incisors and making an orthodontic
intervention on the mandibular arch. A bilateral fixed appliance containing 2 hooks with
loops, 1 buccal and the other lingual, was placed on the mandibular primary first molars.
The hooks were activated in a niche made of light-curing resin on the occlusal surface of
the mandibular permanent molars, to bring about the distal drift of these teeth. After 6
months, complete eruption of the mandibular permanent molars occurred, and a slight
displacement of the maxillary permanent central incisors toward the median line was
noted. The importance of early, adequate treatment is discussed. (Quintessence Int
2006;37:677–683)
Key words: tooth eruption, ectopic; orthodontics, interceptive; dentition, permanent;
molar; incisor; pediatric dentistry
1Assistant Professor of Pediatric Dentistry, Veiga de Almeida
University, Rio de Janeiro, Brazil.
2Associate Professor, Department of Pediatric Dentistry and
Orthodontics, Federal University of Rio de Janeiro, School of
Dentistry, Rio de Janeiro, Brazil.
3Pedodontist and Orthodontist, Department of Pediatric
Dentistry and Orthodontics, Federal University of Rio de
Janeiro, School of Dentistry, Rio de Janeiro, Brazil.
Reprint requests: Dr Luciana Pomarico, Praia do Flamengo
370/202 – Flamengo, 22210-030 Rio de Janeiro, RJ, Brazil. Fax:
55 (21) 2551-4354. E-mail: [email protected]
Pomarico.qxd 8/11/06 9:21 AM Page 677

678 VOLUME 37 • NUMBER 9 • OCTOBER 2006
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
Concerning localization, there is no differ-
ence regarding distribution per hemiarch2,16
nor whether it is unilateral or bilateral.2,10 Its
etiology is associated with macrodontism,
shortened arch length,1,7,13,16,19 posterior posi-
tioning of the maxilla,1,13,16,20 atypical eruption
angle,1,7,13,16 retarded calcification of some
affected permanent molars,16 familial tenden-
cies,6,8,21 and genetic factors.8
This article describes a rare case of
ectopic eruption of maxillary permanent cen-
tral incisors and mandibular permanent first
molars as well as the treatment given.
CASE REPORT
A male patient, aged 7 years and 11 months,
was referred to the pediatric dentistry clinic
of a public university by his dentist, with a
chiefly esthetic complaint about bad posi-
tioning of his anterior teeth. His medical his-
tory did not reveal anything noteworthy.
The clinical examination showed caries
lesions only on the mesial and buccal surfaces
of the maxillary primary central incisors, which
was confirmed by analysis of panoramic and
periapical radiographs. It was also found that
the patient had a Class III malocclusion, with
anterior mandibular tooth crowding of 3.0 mm.
The maxillary primary central incisors, which
were still in place, showed little root resorption.
The maxillary permanent central incisors had
erupted outside their axis, in the region of the
maxillary permanent lateral incisors and
through the palatine, causing exfoliation of the
maxillary primary lateral incisors (Figs 1a to
1d). The mandibular permanent first molars
had also erupted ectopically, suggesting that
the ectopic eruption was causing an initial
resorption of the distal root of the mandibular
right primary second molar (Figs 2a and 2b).
Additionally, it was noted that the mandibular
right permanent first molar showed hypoplasia
on its buccal surface.
A dental cast was made and, after exam-
ining the mixed dentition using the Moyers
method, a negative discrepancy of 11.6 mm
was found in the maxillary arch and 3.2 mm
in the mandibular arch. Although the
patient’s oral hygiene was good, biofilm had
accumulated in the region of the mandibular
permanent first molars.
The treatment plan consisted of extracting
the maxillary primary central incisors and
making an appliance to correct the ectopic
eruption of the mandibular permanent first
molars. The appliance was cemented on the
mandibular primary first molars; it contained
two hooks with loops, one buccal and the
other lingual, that were activated in a niche
made of light-curing resin tag on the occlusal
surface of the mandibular permanent first
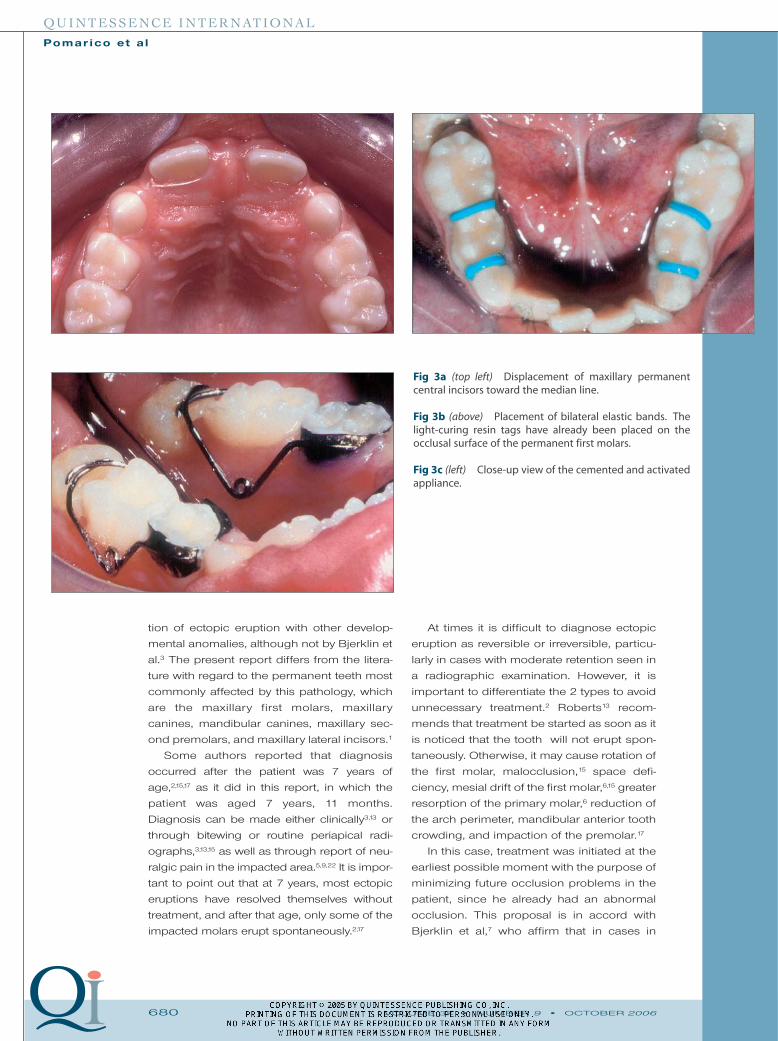
molars. Three weeks later, a slight displace-
ment of the permanent central incisors
toward the median line (Fig 3a) was noted. To
separate the mandibular primary molars,
elastic bands were inserted for 2 days (Fig
3b) so that the appliance could be cemented
bilaterally (Fig 3c). After cementation, the
patient returned each week to control
hygiene, monitor the mesial drift of the maxil-
lary permanent central incisors, and to acti-
vate the mandibular appliance.
Clinical and radiographic examination at 3
months confirmed the disimpaction of the
mandibular left permanent first molar and of
the mandibular right permanent first molar at
4 months. After correction, retention was
maintained for 1 month between the
mandibular primary second molars and the
permanent first molars, to avoid mesial tip-
ping (Fig 4a); it was later exchanged for elas-
tic bands. The patient was kept under obser-
vation at appointments every 2 weeks until
complete eruption of the mandibular perma-
nent molars, which occurred after 6 months
(Figs 4b to 4e). The patient was then sent for
orthodontic evaluation and subsequent cor-
rection of his malocclusion at a suitable age.
DISCUSSION
Of the etiologic factors mentioned, the short-
ened arch length was present in the case
reported above. The patient showed irre-
versible ectopic eruption of the maxillary per-
manent central incisors and of the mandibu-
lar permanent first molars, as well as hypo-
plasia. This simultaneous occurrence was
also reported by Pulver,16 who found associa-
Pomarico.qxd 8/11/06 9:21 AM Page 678

VOLUME 37 • NUMBER 9 • OCTOBER 2006 679
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
Fig 1a Intraoral situation of patient at 7 years and 11months.
Fig 1b Maxillary arch.
Fig 1c Panoramic radiograph of patient at 7 years and 6months, showing ectopic eruption of the maxillary perma-nent central incisors and mandibular permanent firstmolars.
Fig 1d Periapical radiograph ofthe maxillary anterior region.
Fig 2a Left bitewing radiograph. Fig 2b Right bitewing radiograph.
Pomarico.qxd 8/11/06 9:21 AM Page 679
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
tion of ectopic eruption with other develop-
mental anomalies, although not by Bjerklin et
al.3 The present report differs from the litera-
ture with regard to the permanent teeth most
commonly affected by this pathology, which
are the maxillary first molars, maxillary
canines, mandibular canines, maxillary sec-
ond premolars, and maxillary lateral incisors.1
Some authors reported that diagnosis
occurred after the patient was 7 years of
age,2,15,17 as it did in this report, in which the
patient was aged 7 years, 11 months.
Diagnosis can be made either clinically3,13 or
through bitewing or routine periapical radi-
ographs,3,13,15 as well as through report of neu-
ralgic pain in the impacted area.5,9,22 It is impor-
tant to point out that at 7 years, most ectopic
eruptions have resolved themselves without
treatment, and after that age, only some of the
impacted molars erupt spontaneously.2,17
At times it is difficult to diagnose ectopic
eruption as reversible or irreversible, particu-
larly in cases with moderate retention seen in
a radiographic examination. However, it is
important to differentiate the 2 types to avoid
unnecessary treatment.2 Roberts13 recom-
mends that treatment be started as soon as it
is noticed that the tooth will not erupt spon-
taneously. Otherwise, it may cause rotation of
the first molar, malocclusion,15 space defi-
ciency, mesial drift of the first molar,6,15 greater
resorption of the primary molar,6 reduction of
the arch perimeter, mandibular anterior tooth
crowding, and impaction of the premolar.17
In this case, treatment was initiated at the
earliest possible moment with the purpose of
minimizing future occlusion problems in the
patient, since he already had an abnormal
occlusion. This proposal is in accord with
Bjerklin et al,7 who affirm that in cases in
680 VOLUME 37 • NUMBER 9 • OCTOBER 2006
Fig 3a (top left) Displacement of maxillary permanentcentral incisors toward the median line.
Fig 3b (above) Placement of bilateral elastic bands. Thelight-curing resin tags have already been placed on theocclusal surface of the permanent first molars.
Fig 3c (left) Close-up view of the cemented and activatedappliance.
Pomarico.qxd 8/11/06 9:21 AM Page 680
VOLUME 37 • NUMBER 9 • OCTOBER 2006 681
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
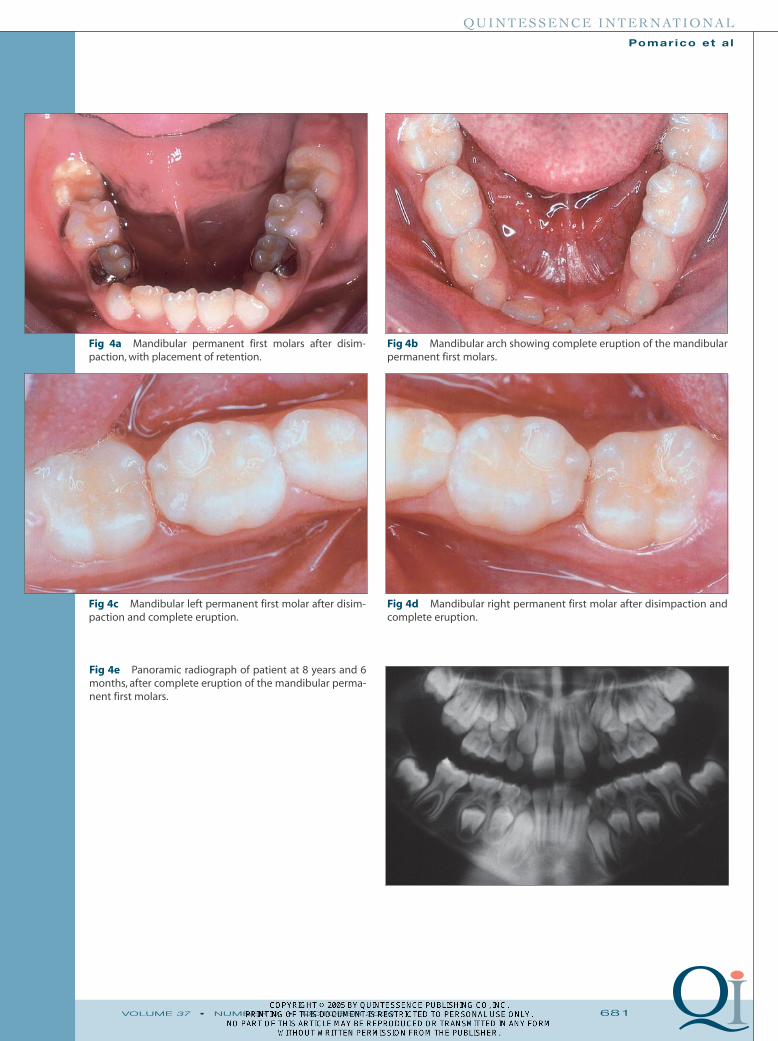
Fig 4e Panoramic radiograph of patient at 8 years and 6months, after complete eruption of the mandibular perma-nent first molars.
Fig 4a Mandibular permanent first molars after disim-paction, with placement of retention.
Fig 4b Mandibular arch showing complete eruption of the mandibularpermanent first molars.
Fig 4c Mandibular left permanent first molar after disim-paction and complete eruption.
Fig 4d Mandibular right permanent first molar after disimpaction andcomplete eruption.
Pomarico.qxd 8/11/06 9:21 AM Page 681

682 VOLUME 37 • NUMBER 9 • OCTOBER 2006
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
which other malocclusion problems occur,
the plan for the correction of ectopia should
be part of the total orthodontic treatment. It is
interesting to note that Pulver,16 in his study,
verified a low prevalence of patients with
Class III malocclusions suffering from
ectopic eruption—like the patient in the pres-
ent report—in spite of these individuals hav-
ing shortened arch length and retroposi-
tioned maxilla, which are related to the etiol-
ogy of ectopic eruption. In some cases,
because of the positioning of the tooth,
cleaning of the area is difficult.2 In addition,
there is no self-cleaning zone, which may
give rise to a greater caries risk. This fact was
noted in the present report, in which a
greater accumulation of biofilm was detected
on the impacted first molars.
Ectopic eruption can be corrected in 2
ways, by interproximal separation13,23,24 or by
distal drift of the ectopic molar,5,13,24–26
depending upon the degree of impaction.24
Hirayama and Chow23 suggested the use of
elastic separators and steel wire, placed
between the affected tooth and its adjacent
neighbor. The treatment in this case consisted
of a fixed appliance with 2 loops soldered to a
band cemented on the mandibular primary
first molars and activated to a resin tag bond-
ed to the occlusal surface of the impacted
molar. These devices, however, should only
be used as a basis when there is sufficient
root structure to ensure stability, ie, when
there is little root resorption,24,26 as in the pres-
ent case. Otherwise it may cause pain, infec-
tion,24 a dentoalveolar abscess, and ankylo-
sis.22 Pulver and Croft26 used a similar device,
although the band was placed on the primary
second molar. Similar treatments have been
reported in the literature, with slight differ-
ences such as duration of treatment,5 arch
involved,24 and association with other thera-
pies such as hemisection of the primary molar
involved18 and extraction with orthodontic
treatment.14 It is important to stress that failure
to begin orthodontic treatment after extracting
the primary tooth may result in mesial drift of
the permanent molar, space loss, malocclu-
sion, and periodontal problems.12
The treatment period of the case
described was 3 to 4 months, although there
are reports in the literature of treatments last-
ing from 3 weeks27 to 6 months.23 In this
report, in addition to the tooth disimpaction
period, it was necessary to place elastic
bands to avoid mesial drift of the permanent
first molar until it had fully erupted. This fact
is in accordance with Lin,25 who also used
this method after disimpacting the first per-
manent molar. An important factor in the
treatment of this patient was that a fixed
appliance was used for which the patient’s
cooperation was not necessary.
Two further aspects should be empha-
sized. The first concerns the absence of pain
in the area during the treatment, which is rel-
evant particularly in view of the patient’s
young age. The second is the rapid solution
of the problem, which facilitated the cleans-
ing of the area, thus lessening the risk of
caries.
CONCLUSION
A meticulous clinical examination is impor-
tant, always accompanied by routine radi-
ographs, to detect the presence not only of
caries lesions, but also of developmental
anomalies. Although the prevalence of
ectopic eruption is not very high, particular-
ly of the irreversible type, this condition can
occur. Pediatric dentists should be pre-
pared to make a correct diagnosis and to
plan the most suitable treatment for each
patient to avoid any damage, such as the
resorption of the primary second molar. In
the case presented in this article, a simple
appliance was placed to correct the ectopy
of the permanent molars and to minimize
the occurrence of severe malocclusion in
the future, since this patient already had an
abnormal occlusion. As presented, this
method of correcting molar ectopy may be
considered efficient and easy to use and
can facilitate early treatment, leading to a
very satisfactory result.
Pomarico.qxd 8/11/06 9:21 AM Page 682

VOLUME 37 • NUMBER 9 • OCTOBER 2006 683
QUINTESSENCE INTERNATIONAL
Pomar ico et a l
REFERENCES
1. Burdi AR, Moyers RE. Desenvolvimento da dentição
e da oclusão. In: Moyers RE (ed). Ortodontia. Rio de
Janeiro: Guanabara Koogan, 1991:86–126.
2. Bjerklin K, Kurol J. Prevalence of ectopic eruption of
the maxillary first permanent molar. Swed Dent J
1981;5:29–34.
3. Bjerklin K, Kurol J,Valentin J. Ectopic eruption of the
maxillary first permanent molars and association
with other tooth and developmental disturbances.
Eur J Orthod 1992;14:369–375.
4. Duncan WK, Ashrafi MH. Ectopic eruption of the
mandibular first permanent molar. J Am Dent Assoc
1981;102:651–654.
5. Groper JN. A simplified treatment for correcting an
ectopically erupting maxillary first permanent
molar. J Dent Child 1985;52:374–376.
6. Kurol J, Bjerklin K. Ectopic eruption of maxillary first
permanent molars: Familial tendencies. J Dent Child
1982;49:35–38.
7. Bjerklin K, Gleerup A, Kurol J. Long-term treatment
effects in children with ectopic eruption of the
maxillary first permanent molars. Eur J Orthod
1995;17:293–304.
8. Bjerklin K, Kurol J, Paulin G. Ectopic eruption of the
maxillary first permanent molars in children with
cleft lip and/or palate.Eur J Orthod 1993;15:535–540.
9. Croll TP, Barney JI. An acid etch composite resin
retained wire for correction of an ectopically erupt-
ing permanent first molar.Pediatr Dent 1982;4:61–63.
10. Kimmel NA, Gellin ME, Bohannan HM, Kaplan AL.
Ectopic eruption of maxillary first permanent
molars in different areas of the United States. J Dent
Child 1982;49:294–299.
11. Kurol J, Bjerklin K. Resorption of maxillary second
primary molars caused by ectopic eruption of the
maxillary first permanent molar: A longitudinal and
histological study. J Dent Child 1982;49:273–279.
12. Kurol J, Bjerklin K. Treatment of children with
ectopic eruption of maxillary first permanent molar
by cervical traction. Am J Orthod 1984;86:483–492.
13. Roberts MW. Treatment of ectopically erupting
maxillary permanent first molars with a distal
extended stainless steel crown. J Dent Child 1986;
53:430–432.
14. Groper JN. Ectopic eruption of a mandibular first
permanent molar: Report of an unusual case. J Dent
Child 1992;59:228–230.
15. Kurol J, Bjerklin K. Ectopic eruption of maxillary first
permanent molars: A review. J Dent Child 1986;53:
209–214.
16. Pulver F. The etiology and prevalence of ectopic
eruption of the maxillary first permanent molar. J
Dent Child 1968;35:138–146.
17. Silva Filho OG, Albuquerque MVP, Kurol J. Ectopic
eruption of maxillary first permanent molars in chil-
dren with cleft lip. Angle Orthod 1996;66:373–380.
18. Auychai S, Feigal RJ, Walker PO. Management of
mandibular molar ectopic eruption using primary
molar hemisection: Case report. Pediatr Dent
1996;18:399–402.
19. McDonald RE, Avery DR. Erupção dos dentes:
Fatores locais, sistêmicos e congênitos que influen-
ciam o processo. In: McDonald RE, Avery DR (eds).
Odontopediatria. Rio de Janeiro: Guanabara
Koogan, 2001:129–150.
20. Canut JA, Raga C. Morphological analysis of cases
with ectopic eruption of the maxillary first perma-
nent molar. Eur J Orthod 1983;5:249–252.
21. Bjerklin K, Kurol J. Ectopic eruption of the maxillary
first permanent molar: Etiologic factors. Am J
Orthod 1983;84:147–155.
22. Croll TP. Correction of first permanent molar ectopic
eruption. Quintessence Int 1984;15:1239–1246.
23. Hirayama K, Chow MH. Correcting ectopic first per-
manent molars with metal or elastic separators.
Pediatr Dent 1992;14:342–343.
24. Weinberger SJ. Correction of bilateral ectopic erup-
tion of first permanent molars using a fixed appli-
ance. Pediatr Dent 1992;14:382–383.
25. Lin YJ. Ectopically erupting mandibular first perma-
nent molar: Treatment of a case. J Clin Pediatr Dent
1996;21:31–33.
26. Pulver F, Croft W. A simple method for treating
ectopic eruption of the first permanent molar.
Pediatr Dent 1983;5:140–141.
27. Halterman CW. A simple technique for the treat-
ment of ectopically erupting permanent first
molars. J Am Dent Assoc 1982;105:1031–1032.
Pomarico.qxd 8/11/06 9:21 AM Page 683








![Stainless steel double loop appliance to correct ... · the transitional dentition period in children. Ectopic eruption reflects the eruption of a tooth in an abnormal position [1].](https://static.fdocuments.us/doc/165x107/5ed571a667cf9358876c08ee/stainless-steel-double-loop-appliance-to-correct-the-transitional-dentition.jpg)









