Echocardiographie Criteria for Normal
7
Echocardiographie Criteria for Normal Newborn Infants By ARTiHR D. HAGAN, CDR, MC, USN, WILLIAM J. DEELY, CDR, MC, USN, DAVID SAHNN, M.D., AND WILLIAM F. FRIEDMAN, M.D. SUMMARY Echocardiograms were obtained from 200 normal newborn infants ranging from 6 to 10 pounds in weight and from 10 to 72 hours in age. A continuous recording technique is described em- ploying a 5 MHz transducer. Criteria have been established for a normal echocardiographic pro- file in the full-term neonate. This profile consists of obtaining quantitative measurements of mitral valve excursion and velocity, tricuspid valve excursion and velocity, pulmonary artery di- ameter, aortic root diameter, left atrial diameter, and interventricular septal thicknesses. In ad- dition, qualitative assessment is made of the septal contour, position of the aortic root to pulmo- nary artery, continuity of mitral valve with posterior aortic root, and continuity of tricuspid valve with anterior aortic root. No correlation was found between the magnitude of any one parameter and either body surface area or weight. The establishment of normal echocardiographic criteria for the newborn may be expected to significantly facilitate application of this noninvasive tech- nique to infants born with congenital heart disease. Additional Indexing Words: Ultrasound Ultrasound cardiography Noninvasive techniques Echocardiographic profile Echocardiography IT MAY be expected that echocardiography will provide progressively more information about various forms of acquired and congenital heart disease. In this regard, there is a relative paucity of anatomic and physiologic ultrasound measurements in infants and children when compared to the large body of data for normal and abnormal adult hearts. While the altered anatomy of several specific congenital cardiac malformations may be detected From the Cardiology Service, Department of Medicine, and the Clinical Investigation Center, U. S. Naval Hospital, San Diego, California; and the Division of Pediatric Cardiology, School of Medicine, University of California, San Diego, California. Supported in part by the Bureau of Medicine and Surgery, Navy Department, Clinical Investigation Program, CICC 3-16-033, and by USPHS Grants HL 12373 and HL 05846. Dr. Friedman was the recipient of USPHS Research Career Development Award HL 41737 from the National Heart and Lung Institute. The opinions or assertions contained herein are those of the authors and are not to be construed as official or as reflecting the views of the Navy Department. Address for reprints: CDR A. D. Hagan, Head, Cardiology, U. S. Naval Hospital, San Diego, California 92134. Received May 10, 1973; revision accepted for publication August 3, 1973. Circulation, Volume XLVJII, December 1973 by ultrasound in infants, the range of normal for the dimensions and motion of all cardiac structures has not yet been defined precisely for the neonate.1-'0 Most previously reported studies of normal infants have been limited by the use of 2.25 to 3.5 MHz transducers with data display on Polaroid film.4' 5, 9-12 The determinations that form the basis of this report were obtained with a5 MHz transducer and a continuous recording technique. The present findings provide an echocardiographic profile for normal, full-tern infants. Methods Cardiac echograms were obtained from 200 normal, full-term infants ranging in age from 10 to 72 hr (aver- age= 37 hr). The group consisted of 100 males and 100 females and weights ranged from 6 to 10 pounds (average = 7.6 pounds). A Picker Echoview II interfaced with a Honeywell strip chart recorder was employed. The transducer by Aerotec Corporation has a center frequency of 5.0 mHz with an active element diameter of one-fourth inch. It is a non-focused, highly damped transducer which permits more superior resolution and definition of cardiac structures in the newborn than is possible using a 2.25 or a 3.5 MHz transducer. It has a repetition rate of 1,000 impulses/sec and is a sound transmitter for 1 microsecond and a sound receiver for 999 microseconds. 1 Airless contact between transducer and skin was achieved with a water soluble gel. All ultrasound 1221 by guest on February 19, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Echocardiographie Criteria for Normal

Echocardiographie Criteria for NormalNewborn Infants
By ARTiHR D. HAGAN, CDR, MC, USN, WILLIAM J. DEELY, CDR, MC, USN,
DAVID SAHNN, M.D., AND WILLIAM F. FRIEDMAN, M.D.
SUMMARYEchocardiograms were obtained from 200 normal newborn infants ranging from 6 to 10 pounds
in weight and from 10 to 72 hours in age. A continuous recording technique is described em-
ploying a 5 MHz transducer. Criteria have been established for a normal echocardiographic pro-
file in the full-term neonate. This profile consists of obtaining quantitative measurements ofmitral valve excursion and velocity, tricuspid valve excursion and velocity, pulmonary artery di-ameter, aortic root diameter, left atrial diameter, and interventricular septal thicknesses. In ad-dition, qualitative assessment is made of the septal contour, position of the aortic root to pulmo-nary artery, continuity of mitral valve with posterior aortic root, and continuity of tricuspid valvewith anterior aortic root. No correlation was found between the magnitude of any one parameterand either body surface area or weight. The establishment of normal echocardiographic criteriafor the newborn may be expected to significantly facilitate application of this noninvasive tech-nique to infants born with congenital heart disease.
Additional Indexing Words:Ultrasound Ultrasound cardiographyNoninvasive techniques
Echocardiographic profile Echocardiography
IT MAY be expected that echocardiography willprovide progressively more information about
various forms of acquired and congenital heartdisease. In this regard, there is a relative paucity ofanatomic and physiologic ultrasound measurementsin infants and children when compared to the largebody of data for normal and abnormal adult hearts.While the altered anatomy of several specificcongenital cardiac malformations may be detected
From the Cardiology Service, Department of Medicine,and the Clinical Investigation Center, U. S. Naval Hospital,San Diego, California; and the Division of PediatricCardiology, School of Medicine, University of California,San Diego, California.
Supported in part by the Bureau of Medicine andSurgery, Navy Department, Clinical Investigation Program,CICC 3-16-033, and by USPHS Grants HL 12373 and HL05846.
Dr. Friedman was the recipient of USPHS ResearchCareer Development Award HL 41737 from the NationalHeart and Lung Institute.The opinions or assertions contained herein are those of
the authors and are not to be construed as official or asreflecting the views of the Navy Department.
Address for reprints: CDR A. D. Hagan, Head,Cardiology, U. S. Naval Hospital, San Diego, California92134.
Received May 10, 1973; revision accepted for publicationAugust 3, 1973.
Circulation, Volume XLVJII, December 1973
by ultrasound in infants, the range of normal for thedimensions and motion of all cardiac structures hasnot yet been defined precisely for the neonate.1-'0Most previously reported studies of normal infantshave been limited by the use of 2.25 to 3.5 MHztransducers with data display on Polaroidfilm.4' 5, 9-12 The determinations that form the basisof this report were obtained with a 5 MHztransducer and a continuous recording technique.The present findings provide an echocardiographicprofile for normal, full-tern infants.
MethodsCardiac echograms were obtained from 200 normal,
full-term infants ranging in age from 10 to 72 hr (aver-age= 37 hr). The group consisted of 100 males and100 females and weights ranged from 6 to 10 pounds(average = 7.6 pounds).A Picker Echoview II interfaced with a Honeywell
strip chart recorder was employed. The transducer byAerotec Corporation has a center frequency of 5.0 mHzwith an active element diameter of one-fourth inch. It isa non-focused, highly damped transducer whichpermits more superior resolution and definition ofcardiac structures in the newborn than is possible usinga 2.25 or a 3.5 MHz transducer. It has a repetition rateof 1,000 impulses/sec and is a sound transmitter for 1microsecond and a sound receiver for 999 microseconds.
1 Airless contact between transducer and skin wasachieved with a water soluble gel. All ultrasound
1221
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

HAGAN ET AL.
recor(lings were obtained in "slow sweep" or M-modedisplay alonig with the infant's electrocardiogram.Traciings were calibrated for 1 cm anterior-posteriordistance and 0.5 see horizontal duration. Maximumnear and far gain control settings were employed ancdrecording paper speed adjusted to provide the bestquality for each infaint's heart rate. Examinations wereperformed in the newborn nursery with the infants in asupine position in their respective bassinets. Sedationwas not administered, although a bottle or pacifiernipple was occasionally required to quiet the infant.The mitral leaflets were identified by posterior
directioni of the beam of the transducer placed alongthe left sternal border over the third or foturthintercostal space. Since the sternuinm and r1ibs are notcalcified in the ne(onate, they offer no significanitinitefcieiece in recording the substernial echoes of tlheriglht ventriclular wall. Occassionally the transducer wasdirected in a slight infero-lateral direction to record themitral valve (fig. 1). The trictuspid valve echo wasobtained by a slight medial angulation withloutdisplacing the transdtucer. Often, both mitral andtricuspid valve echoes were recorded simultaneously.
In order to record echoes from the aortie valve andaortic root the traansducer xvas directed superiorly anidrightward at the level of the third left intercostal space.Normal mitral-aortic valve continuity was identified asechoes from anterior mitral leaflet, mitr-al annulus. and
posterior aortic root were recorded continuously at thesame depth (fig. 2). Infrequently, identification of theaortic valve necessitated placement at the level of thesecond intercostal space. The wall of the left atriumwas detected poster-ior to the aortic root and the leftven.triele posterior to the mitral valve. The pulmon evalve was identified in most infants by directing thetransducer in either the seconid or third intercostalspaces laterally from the left sternal border. In adultswe have identified the pulmonic valve by directing thetransducer in the second intercostal space in a lateraldirection so that it lies anterioily, laterally, and slightlyceplalad to the aortic valve. In contrast, in occassionalinfanits in this study, the aortic root was visualizedsimultanieotusly juist poster ior to the pulmonary artery(fig. 3).The excursion or mobility of either the mitral oi}
tricuspid valves was measured from the D to E points(fig. 1). The anterior movement encotunter-ed from theC to D points was con-isidered to reflect motion of themitral annuilus due to left venitricuilar ejection, and tlhusC to D movement was not used to assess individualleaflet mobility.
Interventricular septal thickness and contour wasidentified best when recording at the level of either themitral or tricuspid valves. Car.e was taken to measuretlickeness only where shape echoes were recorded fromboth right and left ventricuilar (LV) en-docardlial
cw RV -tS
-~~~ - e < vi-
<- tXd :> v l\ nQ~~~~4 t ,,V.'CD
PP ,Q" .,o4 _,'..'\fl< A .S."s's# ^-r4EG~~~~~~~~~~~~~~k
Figure 1
Diagram and evchograxphic recordingJ w>ith the transduZcer (lirected at the level of the mitrall valve. Inthe dialgra,rrlS =sternuam CW -chest wall, ARtV anzterior rigrht ventricle, RV -right vientricular cav-ity, LVS =inlterventricular septum, LV =left ventricuzlar cavity, AO-aorta, AMV - nterior mitral vazlve,PMIV p>osterior mitral valve, LA =left atrium, PPM po.sterior paupillary mu.scle, PLV -posterior left ven-t1ricle. In the recordinzg, T =tricuespid annulus, S = septumn, AM! anterior mitral leaflet, PMl = posteriormitral leaflet7 END - enzdocardium, anzd EPI =epicardium. Enld-systolic (.small arrow) anld end-diastolic(large arrow) diameters of the left venltricle are idenatified. End-diastole iS better seen in subsequent cycles.CDEFA ideJntifies the respective positions of the ansterior mitral leaflet during systole and diastole.
Circulation, Volume XL VIII, December 1973
1222
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

ECHOCARDIOGRAPHIC CRITERIA FOR INFANTS
;S >E: '4r Pa" z
4' f t x/4'S>% ;~v i
I4~*6a;
4 - 5~S i,S4 o
0
.*. L4A
'A
i' ,_,t
Figure 2
StweCeping the transdcncer from the mitral valve to the aortic valve establishes the normal continuity ofthe anterior mitral leaflet and the posterior aortic root as well as the septal-anterior aortic root conti-nuiity. RV = right ventricuilar wall, S septumn AM =
LV = posterior lcft venitricuilar wall, Ao= aorta, LA
surfaces. Since the tricuspid annulus and anterior aorticroot lie at the same depth as the septuim, a mixture ofechoes from two sources must be avoided. Theii,distinction was accomplished readily by recordiingcontinuously as the transducer was directed to sweepfrom the full excursioni of the tricuspid valve withseptum to the aortic root.
Although the LV epicardial echo is prominent andeasily identified, the LV endocardial echo is often lessdistinct. The position found best for measurlng internalleft ventricular dimensions was at the mitral valve levelsuch that timing of end-systole and end-diastole couldbe assessed directly from the anterior mitral leaflet (fig.1). In this manner, end-systole is more accuratelyrecognized than is often possible using the peakanterior excursion of the LV endocardial echo. Theinternal dimensions of the left venitricle were measuredfrom the LV endocardial septal surface to thecorresponding LV posterior wall endocardial echo.The internal diameters of the right ventricle (RV)
were measured similarly, i.e., from the RV endocardialecho to the corresponiding endocardial septal surface atend-systole and enid-diastole, usin-g the mitral valve fortiming purposes (fig. 4). In newborns, the enidocardialecho of the RV wall could not be recorded satisfactorilyCirculation, Volume XLVIII, December 1973
aniterior mitral leaflet, PM = posterior mitral leaflet,= left atriuim.
with low frequency transducers, but was well delin-eated with the 5 MHz transducer employed in thisstudy.
ResultsMitral anid tricuspid valve measurements are
compared iil table 1. Although the mean velocityan-d excursion of thc anterior tricuspid leaflet wasgreater than the anterior mitral leaflet, the ranigesoverlapped and did not differ significantly. Theposterior mitral leaflet is easily identified in 91% ofthe study group.The pulmonary artery anid aortic root diameters
are given in table 2. The difference between end-systole and end-diastole in the external diameter ofthe aortic root was always less thani 1 mm. In eachneoniate in xvhom the puilmonary artery could beidentified (80% of the entire group), the exterinaldiameter of the latter vessel was larger than theaorta (P < 0.005).Average valuies for left atrial diameters are
provided in table 2. This dimension was measured
1223
7f
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

HAGAN ET AL.
W..
e '- ' . ,v,s
_TRICUSPID
VALVE
MITRALVALVE
The pulnionic valve is recorded anteriorAn = aorta.
from the endocardial surface of the left atrium tothe outer margini of the posterior aortic root at bothenid-systole and end-diastole. Diameters in end-systole were 2.4-4.3 mm greater than in end-diastole. The reflected echoes from the left atrial(LA) wall were usually identified as a straight line.However, increased LA wall motioni was notedoften while sweeping the transducer from posterioraortic root to the mitral valve just prior to recordingthe transition to LV wall. This accentuated LA wallmotion near the mitral annulus was anterior indiastole anid posterior in systole.
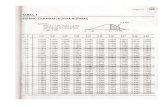
Table 1
Velocity (mm/see) Excursion (mm)
TricuspidRtanlge 610- 116 7.0)- 14.0}M.I.ean - s. 93, - 2 93) .2
MitralRange 60 - 130 6.0 - 12.0Meanlm 80 {i= 1 8.1 - .1
Figure 3
and slightly lateral to the aortic valve. PA= pulmonary artery,
The interventricular septum ranged in thicknessfrom 1.8 to 4 mm (mean = 2.7 mm). Septal motionis normnally posterior during systole anid anteriordurinig diastole with the best quality recording siteat the level of either atrioventricular valve. Onoccasion, variability in septal contour was notedwith a diminiution in anterior-posterior excursionwhen echoes were recorded at a more inferior
Table 2
Pullmornary arlerv (liatimeter (mm)Ra1 ge
Meall
ALeti root(liadameter (niiin)Rallge
L.eft- at m'ini di ameil ter1 ( uml )
Mean hSI.
Inlter venlt ul thickness (inni)Range
Mlean 'si,1
9.4 i 3.1 1.1 .2
8.1 - 12.01 0. .() 6
.-).( - 1 0. ()i.
4.0
2.7 .04
Circulation, Volurne XLVIII, December 1973
122,
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

ECHOCARDIOGRAPHIC CRITERIA FOR INFANTS
W
. ,.
* ,wA '-*N'X,At% 4;t'AM1 N'1 iA 7
Ii
'/
& , 1
Figure 4
The right ventricular wall thickness and internal diamrnter,s are showvn here. The arrows identify end-systolicand end-diastolic diameters utilizing the anterior mitral leaflet for timing purposes. EPI = epicardium,END = endocardium, S = septum, AM = anterior mitral leaflet, PM = posterior mitral leaflet.
position, below the level of the mitral or tricuspidvalve. In addition, it was noted that the septalcontour could erroneously be interpreted as illus-trating paradoxical motion if anterior aortic rootechoes were superimposed.The internal diameters and wall thicknesses of
the right and left ventricles are compared in table 3.Posterior LV wall thickness was not significantlydifferent from RV wall thickness at either end-systole or end-diastole. Although the RV and LVinternal diameter ranges overlap, the LV diameters
Table 3
Right ventricle Lef t ventricle
End-,sx'vtolic wacll thickniess (mrn)Ralnge 3.:3 7.3 2.51 6.0Mea,in ;i5.0) . 1 4.3) .1
End-diastolic wall thickness (rmii)R'anige 2.0 4.7 1.6 3.7AIealln =E= 81x. 3.0 .1 2.6 .1
Kiid-s,ystoli(c diaimet;er (ninm)Range 5.5) - 11.4 8.0 18.6Meai - si 9.4 4 .2 13.3-- .3
End-diaisitolic (diameter (rnin)Range 6.1 15.0 12.0 23A.;3Meani ; i,, 11.4 .4 18.7 .3
Circulation, Volume XLVIII, December 1973
were always greater than the RV diameters ixn thesalme neonate.
DiscussionAll valves aind chambers except the right atrium
can be idenitified in the newborn inifanit byemploying the continuous recording technique anda 5 MHz transducer. Use of the latter transducerallows excellent resolution and more refined detailof all echographie recordings of the inifanit heartthan is possible with lower frequency transducers.Further, the applicationi of a continuous recordingtechnique enables more accurate measurements ofall parameters than is possible with Polaroid filmdisplay. With the latter technique, Meyer andKaplan have described a substantially sloweranterior mitral leaflet velocity in inifanits whencompared to adults.10 Similar results have beenobtained in our laboratory with Polaroid filmrecordings. However, the improved techniquesemployed in the presenit study reveal a much highervelocity of the mitral leaflet in the same infantswithout significant differences when coompared toestablished adult values. The most frequent errorleading to a false impression of slow mitral leafletvelocitv is failture to record echoes frnom the tip of
1225
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

HAGAN ET AL.
the leaflet. Thus, this same error wvill also result in areduced value when the extent of excursion of theleaflet is calculated.The pulmonary valve and artery were not as
consistently recorded (80% of cases) as the aorticvalve and aortic root which were identified in allthe infants. Although the grouped data for thediameters of the pulmonary artery and aortic rootoverlapped, in each infant in whom both weremeasured the pulmonary artery was always largerthan the aortic root.The interventricular septum was recorded easily
at the level of the tricuspid and mitral valves andthe septal contour and degree of anterior-posteriorexcursion was found to vary slightly in the sameneonate by varying the transducer angulation.Septal thickness was not significantly different fromthe end-diastolic wall thickness of the left ventricle(2.7 + .04 and 2.6 + .1 mm, respectively).Only a few previously reported studies have
defined normal right ventricular dimensions ineither infants or adults, and echoes from the RVepicardium have been employed in all ofthese.10 12. 13 In order to accurately obtain thesemeasurements a well defined RV endocardial echomust be recorded. Since different sites of the RVfree wall are recorded with changes in the angle ofthe transducer beam, the endocardial echo is oftenaltered slightly, suggesting a change in thickness.This phenomenon would appear to result from thevariation in the angles of the echo beams as theyare reflected from RV trabeculations. Anterior RVand posterior LV wall thicknesses do not varysignificantly at either end-systole or end-diastole.Although internal diameter ranges of the twoventricles overlap, the LV diameters always exceedthe RV in each individual infant.Attempts were made in this study to correlate
each ultrasound measurement with weight andbody surface area, but no significant correlationswere found to exist. Thus, our findings in thisregard are in contrast to tho,se reported recently bySolinger, Elbl and Minhas.14
In conclusion, the current study establishesnormal echocardiographic criteria for assessment ofthe full-term neonate. In order to obtain a completeultrasound profile, quantitative measurements aremade of the atrioventricular valves' excursions andvelocities, pulmonary artery and aortic root diame-ters, left atrial diameter, interventricular septal
thickness, right and left ventricular diameters andwall thicknesses. In addition, qualitative assessmentis made of the septal contour, position of the aorticroot and pulmonary artery, continuity of mitralvalve with posterior aortic root, and continuity oftricuspid valve with anterior aortic root. Theestablishment of normal echocardiographic criteriafor the newborn will greatly facilitate the applica-tion of ultrasound to infants suspected of havingcongenital heart disease.
References1. ULTRAN LB, SEGAL BL, LIKOFF W: Echocardiography
in congenital heart disease. Am J Cardiol 19: 74,1967
2. CHESLER E, JOFFEE HS, VECHT R, BECK W, SCHMREV: Ultrasound cardiography in single ventricle andthe hypoplastic left and right heart syndromes.Circulation 42: 123, 1970
3. CHESLER E, JOFFEE HS, BECK W, SCHEmE V:Echocardiographic recognition of mitral-semilunarvalve discontinuity: An aid to the diagnosis of originof both great vessels from the right ventricle.Circulation 43: 725, 1971
4. CHESLER E, JOFFEE HS, BECK W, SCHRIBE V:Echocardiography in the diagnosis of congenitalheart disease. Pediatr Clin North Am 18: 1163,1971
5. LUNDSTROm NR, EDLER I: Ultrasoundcardiography ininfants and children. Acta Paediatr Scand 60: 117,1971
6. KOTrLER MN, TABATZNIK B: Recognition of Ebstein'sanomaly by ultrasound technique. Circulation 44(suppl II): II-34, 1971
7. SOLINGER RE, ELBL F, MINHAs K: Echocardiographyin congenital heart disease. Lancet 2: 1093, 1971
8. SOLINGER RE, ELBL F, MmiAs K: Echocardiographyin congenital heart disease in neonates and infants.Circulation 44 (suppl II): II-228, 1971
9. LUNDSTROM NR: Ultrasoundcardiographic studies ofthe mitral valve region in young infants with mitralatresia, mitral stenosis, hypoplasia of the leftventricle, and cor triatriatum. Circulation 45: 324,1972
10. MEYER RA, KAPLAN S: Echocardiography in thediagnosis of hypoplasia of the left or right ventriclesin the neonate. Circulation 46: 55, 1972
11. WINSBERIG F: Echocardiography of the fetal andnewborn heart. Invest Radiol 7: 152, 1972
12. TAJIK AJ, CAU CT, RirrER DG, SCHATTENBERG TT:Echocardiographic pattem of right ventricular dia-stolic volume overload in children. Circulation 46:36, 1972
13. DIAMOND MA, DILLON JC, HAINE CL, CHANG S,FEIGENBAUM H: Echocardiographic features of atrialseptal defect. Circulation 43: 129. 1971
14. SOLINGETR R, ELBL F, MINHAs K: Echocardiography inthe normal neonate. Circulation 47: 108, 1973
Circulation, Volume XLVIII, December 1973
122:6
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from

ARTHUR D. HAGAN, WILLIAM J. DEELY, DAVID SAHN and WILLIAM F. FRIEDMANEchocardiographie Criteria for Normal Newborn Infants
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1973 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.48.6.1221
1973;48:1221-1226Circulation.
http://circ.ahajournals.org/content/48/6/1221Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer in the
Permissions in the middle column of the Web page under Services. Further information about this process is availableOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on February 19, 2018http://circ.ahajournals.org/
Dow
nloaded from