ECG Workout - Excercises in Arrhythmia Interpretation
415
Jane Huff
-
Upload
astanoaei-ana-maria -
Category
Documents
-
view
43 -
download
6
description
medicine
Transcript of ECG Workout - Excercises in Arrhythmia Interpretation
-
Jane Huff
-
STAFF
Publ1sher J. Christopher Burghardt
AcqulslUoll5 Editor BIll Lamsback
Prod uct DIrector Da~1d Moreau
Senior Product MIUIa$tCf DIane Labus
Editors Karen Comerford, Heather Ditch, Erika KGrs
Editorial AssiSlants Karen I. Kirk, Jeri O'Shea, Unda K. Rullf
Creatln~ Director Doug Smock
Art Di rector Elaine Kasmer
Illustrato r Joseph Clark
Vendor Manllger Belh Martz
Seillor MlUlu!acturlng Coordinator Belh J. Welsh
Production Services 51'! Global
"
TI>e cunacaJ treaUIlelltJ described and TKO!IImended lllll'd. publication are based on rHeuch I nd consult. don with lluf"Ilng. medical, rnd legal authorlUes. To the best of OUr knowledge, these procedures renect
curten~y aooepted pracUce. Neo.'enheleJII. theycan'( be con'!looed absolute and unI -\'enal reoommmdilions. For Individual appllcaUons. all rerommendauons must be considered In I1ghI ofille patient's dlnl aol condlUon and. befor.! Idmlnlstrltion of new or Infrequendy used drugs. In Ugh! of the lillern pacb.ge lnsen lnfonnallon. 11le authon and publlst- dlsda1rn any responslblUty for anyadverse effNIS .... ult. tng from the suggested procedUles. from any undetocted error.;. or from the r~ader. mlsundl'tIUllldlng of the text.
02012 by Upplncott WlUlams &< WlIkIIl .. All fights reserved. Thls book 15 proteaed by ropyrighL No pan of It may be reproduced. ItOd In I reU1evall)'Slem. or transmUted, In any form or by any meanl-f!iearontc. mochanlcal, photoropy. fl'C1)l'dlng. or ath. erwlse-",1thout prior wrhten permission of the pubbsher. eD:I'pt for br1ef quotatlons embodied III crUIe" articles and re_1ews and te9iLnH I nd e.'llluatlon mate'll", pro vlded by publisher 10 Ins!ructon whose IIChooII have adopted III Iccompvtylllg r.nbook. For Infonnatlon. write Upplncotl WlUlams &t WllkJlI5, 323 Non1stown Road, Suite 200. Ambler, PA 190022756.
Prtnted In China. ECGWOOIHII0810
LIwa-y of Cooo~ c .. alOP.I.t.a Pa~Ik.tton ~. Huff. Jane. RN. ECG wodout l'.Ierdses III arThythmla
InterpretlitlOn I lane Huff.-tith ed. p. ; CIl.
Includes IlldCl. ISBN 97'8-1...0151 H5S3-6
I. Anh)lhntla_DlIIgIlOS1s-Problems, n.erdllH,etc. 2. Electrocardiography-
IIlI~rpretatkm-ProbJems. ererdsH, etc. , ""'. [DNLM: I ..... rrh)'lhmlas. cardlac-dlagoosJs--.Probiems and E1erdses. 2. Electrocardiography-Problems and E1erds .... WG 18.2]
RC685.A65H842012 616.1 '2807547076---
-
Preface
Iv
f.CG I~o'froul: Exerdsa;/I Arrhythmia Interpretation, Sb:lh Edition, was written 10 MMst physicians. nurse!, medical and nursinl! 5I:udenls. paramedics, tmell/ency medial teetmi-cians. telemetry tethnictans. and other allifd health ~nonnel in ;w;quirinQ the knowledile and skills essential for ldentilyina twit arrhythmias. It may also bt used as a rderenct for electrocardiogram (ECC) review lor those already knowled2eable in ECG interpretation.
The text is writt~n in a simple manner and lUwtrated \!lith tiguru. tables, boxes, and ECC tracinas. Each chapler is designed to build on the know\edae base I'rom the previous cIla!ten 50 that the beJlinnillJl stu:knl can quickly understand and I/I'35P lhe ba5k cmcepll of electrocardiOll-Ji\Pt\y. An etrort has been made ('(It only to proYide good quoN/y ECG trocirtgs, but abo to provide a 5I.Ifticient number and \Wiety of EGC practice strips 50 the Iwner retls confident In arrhythmia inlerpretllion. There are I.lI.I?r fn) proclice strips - more than any book on /he mQrlrel.
Chapter I provides a disculoSion ofbaJic anatomy alld p/ly$IoJO\IYol the heart. The electri-cal basis of t lectrocardiolOi is disCl.l!sed In Chapter 2. The components of the ECC traclnl! twawforrns, intervals. sellmenl5, and complexes) are described in Chapter 3. Thischaplfr also includes pndice tr.w:inlZS on w3wform identification. Cardiac monitol"$, lead JystflTl.'i, lead placement ECC artifacts.:uld troubleshootinllllXlnllor probltmJ art discu!Sed in Chapter 4. A step-by-step lIuide to rhythm Jtritt :ulalysiJ is provided in Chapter 5. in addition to practice tracin(lS on rhythm strip analYJis. The Indi\'itlual rhythm chapters (Chapter$ 6 throullh 9) iocludt 3 description of each arrllythmia. arrhythmia uampltJ. causes. and ~ment protocols. Current .ld'Janced cardiac life support (ACLS) Iluidelines are incorporated into each arrhythmia chapter as awllcable to Ihe rh>thm discunion. Eadl arrhythmia chapttr abo locludes approximately 100 !trips for self-evaluation. CIlapter 10 presents a \ltlleral discussion of cardiac pacemakel"$ (twes. indications. function, pacemaker terminololZY, rmifimctions. and PJCemaktr analYJ]J), alo~with practice tracinlU. Chapkr II is a postle!! comistinll ofa mix 0( rhythm strips that can bt used as a stlf-evaluation tool or for ttstinll purpOstl.
The text has ~n thou!!htfully revisedartd I!QWIded to include nt.'WfiJlures. updated boxes and tables, additional llIossary terms, and evtn more pr.w:tice rhythm 5trips. SkiJlbulfder rhythm stripj. which are new to this edition. appear inunediate)y IOliowil1ll the practice rhythm strips in Chapters 7. 8. and 9. Each Skillbuilder section provides a mix of strips that test not onlY)IOUr urnknblldinQ. of Information It
-
This hook is dedicated to NO/Jell Grace, a "busy" little girl.
-
Anatomy and physiology of the heart
Description and location of the heart The heart is 11 hollow, four-chambtred muscular organ that lies in the middle of the thoracic cavity between the lungs, behind the sternum, in front oflne spinal column, and just move the diaphragm (Figure 1-1). The top oIthe hellrt (the base) is at approximately the level of the second intercostal space. The bottom of the heart (the Qpex) is formed by the tip or the left wntricie lind is positiooed just above the di,l-phragm to the left of the sternum at the fifth intercostal .5p.'Ke. midclaviculllr line. There. the apex tan be pllipated during ventricular contraction. This physical examination landmark is referred to as the poim of 11JtlXimal impu& (PMI) and is.n indiclltor of the heart's position within the thorax.
The heart is tilted forward and to the left so that the right side of the heart lies toward the front. About tv.-o-thirds of the heart lies to the left 01 the body's midline lind one-third extends to the right. The awrage adult heart is apprO):imately 5- (12 em) long. 3W (8 to 9 em) wide. and 2W (6 cm thick) - II little larger than a normal-sized list. The heart weighs betv.een 7 and 15m (200 and 425 grams). Heart siu and weight are influenced by age. weight. body build. frequency of exercise. and heart disease.
Function of the heart Theheart is thel.udest working organ in the body. The heart functions primarily as a pump 10 circulate blood and supply the body with O()'gen and nutrients. Each day the /lwrage hellrt beats olle r 100.000 times. During an awragt lifetime. the human heart will beat more than 3 billion times.
The heart is capable of adjusting its pump pedormance to meet the needs of the body. As needs increase. as with exercise. the heart responds by accelerating the heart rate to propel more blood to the body. As needs decrease. as with sleep. the heart responds by decreasing the heart rate. resulting in less blood flow to the body.
The heart consists 01: four chambtrs
- two atria that receive incoming blood - tv.o wntricles that pump blood out of the heart
four lIalves that control the fla,y of blood through the heart an electrical conduction system that conducts electrical impulses to the heart. resul ting in muscle controction.
Heart surfaces There are four lTIIIin heart surfaces to consider .... hen dis-cussing the heart: anterior, pos/eriar. inferior. and lateral (Figure 1-2). The heart sudaces are uplained below: anterior - the (ront posterior - the back inferior - the bottom lateral - the side.
_~~?t:= Heart Structure ofthe heart wall Siernum
The heart wall is arranged in three La~'ers (Figure 1-3):
Agu .... 1 1. LocaUoo of Ihe neart In lheltaa)(,
theplln'curdium - the ootennost l
-
2 An ntoOlY and physio logy of the hellrl
Anletio. ----t-{ J\..-_--\-P05terJOf
Interior
F1l1u rI1 2. Hm arfaces.
anchors the heart to the chest and prevents it from shift-ing about in the thorax. The !t1'OU5 pericardium is II con-tinuous membrane that forms two layers: the parietal La~-er lines the inner surface of the fibroU5 ~c and the vi5(:era] layer (81M) called epicardium) lines the outer SlJriace nfthe heart muscle. Between the two layers of the !trous peri cardium is the pericardia] space. or cavity. which is usually filled with 10 to 30 mL of thin. cltaT fluid (the pericardial fluid ) secrded by the serous layers. The primary function of the pericardial fluid is to prOYide lubrication, preventing
EndocaJdium --~
-
Heart chambers The interior of the heart consists of four hollow chambers (Figure 1-4). The two upper chambers. the right atrium "nd the left atrium. "re divided by" w,,11 ""lied the inter-atrial septum. The two lower chambers, the right ven-tricle and the left ventricle. are divided by a thicker wall called the interventricular septum. The two septa divide the heart into two pumping systems - a right heart and a left heart.
The right heart pumps venous (deoxygenated) blood through the pulmonary arteries to the lungs (Figure 1-5). Oxygen and carbon dioxide exchange takes place in the alveoli and arterial (oxygenated) blood returns via the pulmonary veins to the left heart. The left heart then pumps arterial blood to the systemic circulation, where oxygen and carbon dioxide exchange takes place in the organs, tissues, and cells; then venous blood returns to the right heart. Blood How within the body is designed so that arteries carry oxygen-rich blood away from the heart and veim carry oxygen-poor blood back to the heart. This role is reversed in pulmonary circulation: pulmonary arteries carry oxygen_poor blood into the lungs, and pulmonary veins bring oxygen-rich blood back to the left heart.
The thickness of the walls in each chamber is related to the workload periormed by that chambu Both atria are low-pre~ure chambers serving as blood-collecting reservoirs for the ventricles. They add a small amount of force to the moving blood. Therefore, their walls are rela-tively thin. The right ventricular wall is thicker than the walls of the atria, but much thinner than that of the left ventricle. The right ventricular chamber pumps blood a fairly short distance to the lungs against a relatively low resistam;e to flow, The left ventricle has the thickest wall, because it must eject blood through the aorta against a
Inlerventricular ""PI"'" Rgur. 1-4, O\ambers oltho heart.
Heart valves 3
much greater resistance to flow (the arterial pressure in the systemic circulation).
Heart valves There are four valves in the heart: the tricuspid vallie, separating the right atrium from the right ventricle: the pulmonic /!{lIve, separating the right ventricle from the pulmonary arteries: the mitral /!{lIve. separating the left atrium from the left ventricle; and the aortic /!{lIve. sepa-rating the left ventricle from the aorta (Figure 1-5). The primary function of the valves is to allow blood flow in one direction through the hear!"s chambers and prevent a backtlow of blood (regurgitation). Changes in cham-ber pressure govern the opening and closing of the heart valves.
The tricuspid and mitral valves separate the atria from the ventricles and are referred to as the atrioventricular (AV) valves. These valves serve as in-flow valves for the ven-tricles. The tricuspid valve consists of three separate cusps or leaflets and is larger in diamder and thinner than the mitral valve. The tricuspid valve directs blood flow from the right atrium to the right ventricle. The mitral valve (or bicuspid valve) has only two cusps. The mitral valve directs blood How from the left atrium to the left ventricle. Both valves are encircled by tough. fibrous rings (valve rings ). The leaflets of the AV valves are attached to thin strands of fibrous cords called chordae tendineae (heart strings) (Figure 1-6). The chordae tendineae are then attached to papillary muscles, which arise from the walls and floor of the ventricles. During ventricular filling (diastole) when the AV valves are open. the valve leaHets, the chordae tendineae, and the papillary muscles form a funnel. pro-moting blood flow into the ventricles. As pressure increases during ventricular contraction (systole) , the valve cusps close. Backflow of blood into the atria is prevented by con-traction of the papillary muscles and the tension in the chordae tendineae. Dysfunction of the chordae tendineae or a papillary muscle can cause incomplete closure of anAV valvt'. This may result in a regurgitation of blood from the ventricle into the atrium, leading to cardiac compromise. The first heart sound (8,) is the product of tricuspid and mitral valve do.ure. S, i. bed heard at the apex of the heart located on the left side of the chest. fifth intercostal space. middavicular line.
The aortic and pulmonic valves have three cuplike cusps shaped like a half-moon and are referred to as the semi-lunar (SL) vall!e5 . These valves serve as out-flow valves for the ventricles, The cusps of the SL valves are smaller and thicker than the AV valves and do not have the sup-port of the chordae tendineae or papilla!)' muscles. Like the AV valves. the rims of the semilunar valves are sup-ported by valve rings. The pulmona!)' valve directs blood flow from the right ventricle to the pulmonary artery. The aortic valve directs blood flow from the left ventri-cle to the aorta. As pressure decreases during ventricular
-
4 Anatomy and physiology of the h eart
Alveolus 01 lung ~
Pulmonary anerl'" --_-1 (to lungs)
~~\ \\ ~-'-'-_~ Aona (to body)
Superior vena cava (Irom upper body)
Pulmonary veins (from lungs)
Ir---;---- Aortic valve Pulmonic valve --i--::c-.\'}'_
M~ral valv!! Tricuspid valve
Inlerior vena cava (lrom lower body)
"";,---'f-i---- Septum
Figure 1-5. Chambers, YaIves, blood now. RA, light atrium: RV, right wntllcle; LA, left atrkJm: LV, len Y00Ir1c1e.
relaxation (diastole), the valve cU5~ close. BackHow of blood into the ventricles is prevented because ofthe cus~' fibrous strength, their dose approximation. and their 5hilpe. The second heart 50und (s.,) is produced by closure of the aortic and pulmonic SL valws. It is best heard over the second intercostal space on the left or right side of the sternum.
Superior vena cava --------,
"~.""m'----------~~
Inll";o< vona c .. va ________ ---.J
Blood flow through the heart and lungs
-
Blood How through the heart ilfId lungs is traditionally described by tracing the How as blood returns from the sys-temic veins to the right side of the heart, to the lungs, back to the left side of the heart. and out 10 the arterial vessels
~-t--- .,,,. , ...
Descendingaorla.-----------..J
Figure 1-6. Papillary muscles and chordae tendheae.
-
of the systemic circuit (Figure I-S). The right atrium receives venous blood from the Ixxly via two of the bodys largest veins (the superior vena cava and the inferior vena cava) and from the coronary sinus. The superior vena cava returns venous blood from the upper body. The inferior vena cava returns venous blood from the lower Ixxly. The coronary sinus returns venous blood from the heart itself.
As the right atrium fills with blood. the pressure in the chamber increases. When pressure in the right atrium exceeds that of the right ventricle. the tricuspid valve opens, allowing blood to flow into the right ventricle. As the right ventricle fills with blood, the pressure in that chamber increases, forcing the tricuspid valve shut and the pulmonic valve open. ejecting blood into the pulmonary arteries and on to the lungs. In the lungs, the blood picks up oxygen and excretes carbon dioxide.
The left atrium receives arterial blood from the pulmo-nary circulation via the pulmonary veins. As the left atrium fills with blood, the pressure in the chamber increases. When pressure in the left atrium aceeds that of the left wntricle, the mitral valw opens, allowing blood to flow into the left ventricle. As the left ventricle fills with blood. the pressure in that chamber increases, forcing the mitral valve shut and the aortic valve open. ejecting blood into the aorta and systemic circuit, where the blood releases oxygen to the organs, tissues, and cells and picks up carbon dioxide.
Although hlood flow om he Imeed fmm th ... right. sid ... of the heart to the left side of the heart, it is important to realize that the heart worhas tv.o pumps (the right heart and the left heart) working simultaneously. As the right atrium receives venous blood from the systemic circulation. the left atrium receives arterial blood from the pulmonary circulation. As the atria fill with blood, pressure in the atria aceeds that of the ventricles, forcing the AV valves open and allowing blood to flow into the wntricles. Toward the end of ventricular fiJI-ing, the tv.o atria contract, pumping the remaining blood into the ventricles. Contraction of the atria during the final phase of diastole to complete ventricular filling is called the atrial kick. The ventricles are 70% filled before theatria con-tract. The atrial kick adds another 30% to ventricular capac-ity. In nomtal heart rhythms, the atria contract before the wntricles. In abnormal heart rh}1hms, the loss of the atrial kick results in incomplete filling of the ventricles, causing a reduction in cardiac output (the amount of blood pumped out of the heart). Once the ventricles are filled with blood, pressure in the ventricles increases. forcing the AV valves shut and the SL valves open. The ventricles contract simul-taneously, ejecting blood through the pulmonary artery into the lungs and through the aortic valve into the aorta.
Coronary circulation The blood supply to the heart is supplied by the right cor-onary artery. the left coronary artery, and their branches (Figure \-7). There is some individual variation in the ""llnll of ~uruJldry "rl~ry br,,"d,iuK.. bul ill 1!~""r .. J, lI,,,
Coronary circulation 5
right coronary artery supplies the right side of the heart and the left coronary artery supplies the left side of the heart.
The right coronary artery arises from the right side of the aorta and consists of one long artery that travels downward and then posteriorly. The major branches of the right coronary artery are: conus artery sinoatrial (SA) node artery (in 55% of population) anterior right ventricular arteries acute marginal artery AV node artery (in 90% of population) posterior descending artery with septal branches (in 90% of population) posterior left wntricular arteries (in 90% of population).
Dominance is a term commonly used to describe coro-nary vasculature and refers to the distribution of the terminal portion of the arteries. The artery that gives rise to both the posterior descending artery with its septal branches and the posterior left ventricular arteries is considered to be a "domi-nant' system. In approximately 90% of the population, tI-.e right coronary artery (RCA) is dominant. The term can be confusing because in most people the left coronary artery is of wider caliber and penuses the largest percentage of the myo-cardium. Thus, the dominant artery usually does not perfuse the largest proportion of the myocardium. The left coronary artery arises from the left side of the aortaand consists of the left m~in cnmn","y ",1,,-1)'. ~ _.hmt .t ... m. ",hich dividp_. into the left anterior descendingilrtery and the circumflexilrtery. The left anterior descending (LAD) travels downward over the anterior surface of the left ventricle, circles the apex, and ends behind it. The major branches of the lAD are: diagonal arteries right ventricular arteries septal perforator arteries.
The circumfla art~ry travels along the latual aspect of the left ventricle and ends posteriorly. The major branches of the circumflex are: SA node artel)' (in 45% of population) anterolateral marginal artery posterolateral marginal artel)' distal left circumflex artery.
In 10% of the population, the circumflex artery gives rise to the posterior descending artery with its septal branches, terminating as the posterior left ventricular arteries. A left coronary artery with a circumflex that gives rise to both the posterior descending artery and the pos-terior left ventricular arteries is considered a "dominant"' left system. When the left coronary artery is dominant, the entire interventricular .septum is supplied by this artery. lithl ... 1_1 'lJmmari?p-. the cnron~I)' ~rI ... ry di,trihlJlion 10 the myocardium and the conduction system.
The right and left coronary artery branches are intercon-nected by an exlel15ive network of small arteries that provide the potential for cross flow from one artery to the other. These small arteries are commonly called roUa/eral vessels ur wUa/t:TU/ c;;n;u/aliu .. Cundl~rdl cin;uldliul' ""i.l. ill birlh
-
6 AnatoOlY and physiology of the heart
Ri!tIt cor.....-v artery
,,-'I;-----lIl! fTIIIioI coronary art8fy
AcuC .. marginal.""'" ---f---~ Arteria. rlglt vet1n:uiar --t-- 7 -AV node sri.", -----\---j
Septal branch _________ --"''''':'''-::..J''-Figure 1 7. coronary ctaJlatkln.
lib .. ! ! . Coronary arteries
COronary.n.ry Inclltl bllllCll" PortIon of lI'II'ocardlUm I~plld Righi Corona"f artlllY
Left oorona ry 3I1!ry left anterior descendilg (\..AD)
'" of popula~
RighI atrium RigIt wnlridt
~Ieriof wall 0I1eIt ventricle (90%)' Poaeriof ooe-titd of ~ sepllm (9O%f
Anterior wal alief! w:nlril:le AnIIIroIateral waI 01 left Y8llticle Anterior two-llirds 01 intervmtriaJiar septum
Leftatrium AnIIIroIateral waI 0I1eit _triCIe PosIBroIateral war alleft venR:le Posterior wall 0I1ef! Y9n1ric1e
~Ierior wall 01 left ventricle (1 0%)' Posterior one-lin! of ilIIIrYer!IriWa sepbn (IO'!W
Portion 01 condut::tlon . ysttm IUPpl'"
SinoIriaI (SAl node (55")' AbiIJoientricul. (AV) rIXIe and bundle ollis (90%)'
R91t and Ief! boodle brandies
SA node (45%)' AV node and tude of His (10%)'
-
but the vessels do not become functionally significant until the myocardium experiences an ischemic insult. If a block-age occurs in a major coronary artery, the collateral vessels enlarge and provide additional blood flow to those areas of reduced blood supply. HOYtewr, blood flow through the col-lateral vessels isnt sufficient to meet the total needs of the myocardium in most cases. In other vascular beds of the body. arterial blood flow reaches a peak during ventricular contrac-tion (systole) . However, myocardial blood flow is greatest dur-ing ventricular diastole (when the ventricular muscle mass is relaxed) than it is during systole (when the hearts blood vessels are compressed). The blood that has passed through the capillaries of the rq,rocardium is drained by branches of the cardiac veins whose path rufl5 p.:lrallello those of the coronary arteries. Some of these veins empty directly into the
ri~t atrium arxJ ri~t ventricle. but the majority feed into the coronary sinus, ",tJich empties into the right atrium.
Cardiac innervation The heart is under the control of the autonomic nerv-ous system located in the medulla oblongata, a part of the brain stem. The autonomic nervous system regu-lates functions of the body that are involuntary, or not under conscious control. such as blood pressure and heart rate. It includes the sympathetic nervous system and the parasympathetic nertJOus system, each produc-ing opposite effects when stimulated . Stimulation of the sympathetic nervous system results in the release of norepinephrine, a neurotransmitter, which acceler-ates the heart rate. speeds conduction through the AV node, and increases the force of ventricular contrac-tion . This system prepares the body to function under stress ("fight-or-flight" response ). Stimulation of the parasympathetic nervous system results in the release of acetylcholine, a neurotransmitter, which slows the heart rate, decreases conduction through the AV node, and causes a small decrease in the force of ventricular contraction. This system regulates the calmer functions of the body (" rest-and-digest" response). Normally a bal-ance is maintained between the accelerator effects of the sympathetic system and the inhibitory effects of the parasympathetic system.
Cardiac innervation 7
-
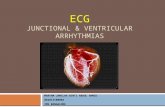
Electrophysiology
Cardiac cells The heart is compostd of thousands of cardiac ce lls. The cardiac ceUs are long and narroY.\ and di\ide at their ends into branches. These branches conned with branches of adjacent cells, forming a branching and anastolTlO5ing network of cells. At the junctions where the branches join togethe r is a spedal~ed cellular membrane of low electri cal resistance, which permits rapid conductionol electrical impulses from one cell to another throughout the cell net-work. Stimulation of one cardiK ce ll initiates stimula.tion of adjacent cells and ultimately leads to cardiac muscle contraction.
Thne are two basic kinds of cardja(: cells in the heart: the m!lOcuniidl cefts (or "working" cells) lIfId the PUCil-maker cells. The myocardial cells are contained in the muscular layer of the walls of the atria and ventricles. The myocardial "'Working" cells art permeated by contractile filaments which, when electrically stimulated. produce myocardial mu~cJe controction. The primary function of the myocardial cells is cardiac muscle contraction, fol-lowed by relaxation. The pacemaker cells are found in the electrical conduction system of the heart and are primar-ily responsible for the spontaneous generation of electrical impulSl$.
Cardiac cells have four primary cell characteristics: Qutomaticit!l - the ability of the pacemaker cells to generate their own electrical impulses spontane(lusly; this characteristic is specific to the pacemaker cells. uritability- the ability of the cardiac cells 10 respond to an eleclrkal impulse: this characteristic is shared by all cardiac cells. conductitity - the ability of cardiac cells 10 conduct an electrical impulse: this characteristic is shared by all cardiac ce lls. contractih"ty - the ability of cardiac cells to cause car-di
-
-Resting cell (polarized Slate)
Depolarii!atioll belllnnir>g (st",.II ... a.led S\ale)
Depolarization oom~ete
Repclarlzalion beginning (reccvery sta!~1
Ftepolanzation complete
~,.L..t ....! __ Lt......!......!_!_~ I - . - - . - I
K' ! i I ,..:.-=-.:-.. ..:. . ...:. .. ...: .. - .:-.:...-:..-.- :./
+ + + + + + + + + +
Rgure 2-1 . Depola'ization lIld repola"lzaUOO 01 a cardiac cen.
activity is occurring and a straight 1in~ (isoelectric line) is recorded on the ECG (Figure 2-5).
Once a cell is stimulated, the membrane permeability changes. Potassium begins to leave the cell, increasing cell permeability to sodium. Sodium rushes into the cell, causing the inside of the cell to become more positive than negatiw (cell is depolarized). Muscle contraction follows d~polariMtion. Depolaril.alion and muscle con-traction are not the same. Depolarization is an electrical event that results in muscl~ contraction, a mechanical event.
After depolarization, the cardiac cell begins to recowr, The sodium-potassium pump is activated to actiwly trans-port sodium out of the cell and mow potassium back into the cell, The inside of the cell becomes more negative than roositi"" (cell i, re[lOl;,ri"ed) and return_, tn it, r,,-,tjng ,tate.
Depolarization of one cardiac cell acts as a stimulus on adjacent cells and causes them to depolarize. Propagation of the electrical impulses from cell to cell produces an electric current that can be ddect~d by skin electrodes and recorded as waves or deflections onto graph paper. called
lh~ECG.
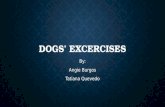
Electrical conduction system of th e h eart 9
Electrical conduction system ofthe heart The heart is supplied with an electrical conduction system that generates and conducts electrical impulses along specialired pathways to the atria and ventricles, causing them to contract (Figure 2-2). The system consists of the sinoatrial node (SA node), the interatrial tract (Bach-mann's bundle), the internodal tracts, the atriowntricular node (...tV node), th~ bundle of His, the ri!/lt bundle branch. the left bundle branch, and the Purlrinje fibers.
The SA node is located in the wall of the upper right atrium near the inlet of the superior vena cava Special-ized electrical cells, called pacemaker cells, in the SA node discharge impulses at a rate of 60 to 100 times per minute. Pacemaker cells are located at other sites along the con-duction system, but the SA node is normally in control and is called the pacemaker of the heart because it P05.!esses the highest level of automaticity (its inherent firing rate is greater than that of the other pacemaker sites). If the SA node filils to generate electrical impulses at its normal rate or stops functioning entirely, or if the conduction of these impulses is blocked, pacemaker cells in second-ary pacemaker sites can a5.!ume control as pacemaker of the heart, but at a much slower rate. Such a pacemaker is called an escape pacemaker because it usually only appears ("",care'') when the f,,-der firing pacemaker (m,,~lIy the SA node) fails to function, Pilcemaker cells in the AV junc-tion generate electrical impulses at 40 to 60 times per minute. Pacemaker cells in the ventricles generate elec-trical impulses at a much slower rate (30 to 40 times per minute or less). In general , the farther av,ay the impulse originates from the SA node, the slower the rate. A beat or series of beats arising from an escape pacemaker is called ilne5capeheatore5cape mythm and is identified according to its site of origin (for example, junctional, ventricular).
As the electrical impulse leaves the SA node, it is con-ducted through the left atria by way of Bachmann's bundle and through the right atria via the internodal tracts, caus-ing electrical stimulation (depolarization) and contraction of the atria. The impulse is then conducted to the AV node located in the lower right atrium near the interatrial Sly f .... l rd.ll!S.
-
10 Electrophysiology
AVnodo
Bundle 01 His
Righi bundle branch
Figure 2-2. ElectrIcal conduction system ollhe hearI.
Mter the delay in the AV node. the impulse moves through the bundle of His. The bundle of His divides into two important conductil1ll pathways called the right bundle branch and the left bundle branch. The right bundle branch conducts the electrical impulse to the right ventricle. The left bundle branch divides into two divisions: the anterior fascicle, which carries the electrical impulse to the anterior wall of the left ventricle. and the posterior fascicle. which
-
Refracto ry and supernonual periods of the cardiac cycle 11
Figure 2- 4. The cardiac cycle.
wntricular repolari1.ation. The U wave, which isn't always present. represents late ventricular repolarization. The QT interval represents total ventricular activity (the time from the oru;et of ventricular depolarization to the end of ven_ tricular repolari1.ation).
The cardiac cycle A cardiac cycle consists of one heartbeat or one PQRST sequence. It represents a sequence of atrial contraction and relaxation followed by ventricular contraction and relaxation. The basic cycle repeats itself again and again (Figure 2-4). Regularity of the cardiac rhythm can be assessed by measuring from one heartbeat to the next (from one R wave to the next R wave, also called the R-R interval) . Belvt'een cardiac cycles. the monitor or ECG recorder returns to the isoelectric line (baseline). the flat line in the ECG during which electrical activity is absent (Figure 2-5). Any waveform abow the isoelectric line is considered a positive (upright) deflection and any wave-form below this line a negative (downward) deflection. A deflection having both a positive and negative compo-nent is called a biphasic deflection. This basic concept
, ,
, , , ,
o , 0 , lsoele
-
12 Electrophysiology
OAS complex
Pwavi TWaV8
~" abwUII fIlati; ;:;:toty Altract
porl'"
Ab.soJute refractory period - During this period the cells absolutely cannot respond to a stimulus. This period extends from the onset of the QRS com pia to the peak of
th~ T wav~. During this tim~ th~ cardiac c~lIs hav~ d~polarized and ar~ in th~ process of ~polarizing. Because the car-diac cells have not repolari~ed to their threshold potential (Ihe le~1 at which a cell must be repolarized before it can be depolarized again) they cannot be stimulated to depolar-ize. In other words. th~ myocardial cells cannot contract, and the cells of the elect ri cal conduction system cannot conduct an electrical impulse during the absolute refrac-tory period . Relative refractory period - During this period the cardiac cells have repolarized sufticiently to respond to a strong stimulus. This period begiru at the peak of the T wave and ends with the end of the T wave. The relative refractory period is also called Ihe vulnerable period of repo/arization. A strong stimulus occurring during the vulnerable period may usurp the primary pacemaker of the heart (usually the SA node) and take over pacemaker control. An example mighl be a prellUllure ventricular con-traction (We) that falls during the vulnerable per iod and takes over control of the heart in the form of ventricular tachycard ia.
Figure 2-8. EIec1rOCMdlographk: paper.
.. po V ......
FIgure :Z 7. Refractory and S!.p9mOnl1al periods .
Supernormal period - During this period the cardiac cells will respond to a Wfilker than normal stimulus. This period occurs during a short portion near the end of the T wave. just before th~ cells have completely repolarized.
ECG graph paper The PQRST sequence is recorded on special graph paper made up of horizontal and vertical lines (Figure 2-8). The horizonlllilines meilSure the duration of the waveforms in seconds of time. Each small square measured hori~ontally
repr~nts 0.04 second in time. The width oflh~ QRS com-plex in Figure 2-9 extends across for 2 small squares and represents 0.08 second (0.04 second x 2 squilres). The ver_ ticallinu measure the voltage or amplitude of the wave-form in millimeters (mm). Each small square meilSured vertically represents I mm in height. The height of Ihe QRS complex in Figure 2-9 extends upward from baseline 16 small $quares and represents 16 mm volti\ge (I mm x 16squaru).
Figure 2- 9 . ORS width: 0.08 second; ORS height: 16 mm.
-
Waveforms, intervals, segments, and complexes
Much of the information that the ECG tracing provides is obtained from the examination of the three prindpall
-
14 Wa\'eforms, intervals, segments, and complexes
A Normal PW3ve B Inverted P wave
c No v>sible P waves D Two P waveS to each OAS
G Flat P w.we SDWlaoth P wav ... J Wavy P w.wes
Figur.3-2. P W3YO exampIDs.
-
Allure 3-3. TIle PR nlllYal.
was delayed longer than normal in the AV node. Prolonged PR intervals are seen in first-degr AV block.
Examples of PR interv.ili are shown in Figure 3-4.
QRScomplex The QR5 complex (Figure 3-5) represents depolariution of the right and left vent ricles. The. QRS complex is larger than the P wave because depolariz.alion of the ventricles involves a larger muscle mass than depolariWion of the atria.
The QR5 complex is composed of three waw deflec-tions: the QU'l:lw. the R u.,,:we. and the S IL'Qt'Ol. The R waYe is a posi tive waveform: the Q waw is II negative wavefonn that precedes the R waw; the 5 wave is a negative wave-form that follows the R wave. The normal QR5 compln is predominantly positiw in lead II (a positive Iud) with a duration of 0.10 second or less.
The QRS complex is measured from the beginning 01 the QRS complex (as the first wave of the compln. leaVi!s baseline) to the end of the QR5 complex (when the last wave of the complex bellins to level out into the ST segment). The point where the QR5 complex meets the 51 segment is called the} point (junction point).
A B c
QRS complex 15
Q S
Figure 3-5. lhe ORS compleX.
Finding the beginning of the QRS complex usually isn 't difficult. Finding the end of the QRS complex. however. is at times a challenge because of elevation or depres sion of the ST segment. Remember, the QRS complex ends as soon as the straight line of the 5T segment begins, even though the straight line may be above or below baseline.
Although the term QRS complex is used, not every QR5 complex contains a Q waYe, R wave. and 5 wave. Many variations exist in the configuration of the QRS complex (Figure 3-6). Whatever the variation. the complex is still called the QRS complex. For example, you might .see a QRS complex with a Q and an R ..... ave. but no S wave (Figure 3-6, example B). an Rand 5 wave without a Q wave (Figure 3-6, eXlWTlple C), or an R wave without a Q or an S wave (Figure 3-6, example 0). If the entire complex is negative (Figure Hi, example F). it is termed a QS com-plex (not a ntgative R wave becauu R waves are always positiYe). Ifs also pouible to have more than one R wave (Figure 3-6, example n and more than one 5 waw; (Figure3-6, example J). Thesecond R wave iscalledRprime ilIld is written R'. The second S wave is called S prime and is writlen 5'. To be labeled separately, II wave must cross
Normal PR Werval 01 0.20 second (0.04 second ~ 5 squa .... ).
Short PR inle
-
16 Waveforms, interval s, segments, and complexes
" Nolchad A
,Jl E A ' Y-
a,
, , f 01- H 1r a , s 1\-,
J S s' K V"",,",, Figure 3-6, DRS Vil"latlons.
the baseline. A wave that changes direction but doesn't crOM the baseline is Cillied a notch. (Figure 3-6. example E. shows a notched R and Figure 3-6. example K. sho.,.,'S a notched S.)
C~pital letters are used to designllte waves of large amplitude (5 mm or more) and lowercase letters are used to designate waves of small amplitude (less than 5 mm). This allows you to visualize a complex mentioned in a textbook when illustrations aren't available. For example. if a complex is described in II text as having an rS wave-form. the reader Ciln easily picture a complex with a small r wave and a big S wave.
An abnormal QRS complex is wide with a duration of 0.12 second or more. An abnormally wide QRS complex may result from: a block in the conduction of impulses through the right or left bundle branch (bundle_branch block) an electrical impulse that has arrived early (as with pre-mature beats) at the bundle branches before repolariza-tion is complde. allowing the electrical impulse to initiate depolarization of the ventricles earlier than usual. result-ing in abnormal (aber rant) ventricular conduction lind causing a wide QRS complex an electrical impulse thaI has been conduded from the atria to the ventricles through an abnormal accessory conduction pathway that bypasses the AV node. allow-ing the electrical impulse to initiate depolari7.ation of
0.12........d 0,011 oeoond 0.0* oeoond 13 ....-e 0.0* MCCI'Od) (2 "",II" 0.(1.1 -oneil (1 oquoN 0.(1.1 oeoondl
0.10oecond o.oeHCond 0.0II0e00nd (210 _ .. . 0,(1.1 oeoondl (1Y,....-e' xO.(I.I MCCI'Od) (2 oquoros x O,(I.I oeoondl
Figure 3-7. DRS examples.
-
ST segment 17
0.'0_ 0.08_ 0.11_ (211. _ .. Ko.OoI _oneil (2_, .0,04 oeoondI (4' _ . 0.04 0Knd)
0.1~__ O,CIe_ 0.'1-'
-
18 Waverorms, intervals, segmem s, a nd complexes
A Noomal ST U51men1 B NomIaI ST MgI1*1!
C Ccnvax eleYIIIion o Concave eI ..... aOOn
G ~d&p", ..", FiIlUnI 3-9. STsogmenl samples.
-
Rgure3-10. Th8TW3Y11.
A Normal TWINe
C T sll. peaked T wave
E Flat T wavs
figure 3-11 . TwaYII examples.
Twave 19
Twave Th~ T wav~ represents v~ntricular r~polari1.ation. Th~ no r mal T wave begins as th~ deflection gradually slopes upward from the ST segment. and end. when the waveform returns to baseline (Figure 310). Nonnal T waves ar~ rounded and slightly asymmetrical (with th~ first part ofth~ T wave grad-ually sloping to the peak and returning more abruptly to baseline). positive in lead II (a positive lead). with an ampli tud~ less than 5 mm. The T wave always follow. the QRS complex ( r~polarization always foll
-
20 Wa\'eforms, intervals, segments, and complexes
Abnormal T waves may be abnormally tall or low, flattened, biphasic, or inverted. Common causes include myocardial ischemia, acute MI, pericarditis, hyperkalemia. ventricular enlargement, bundle-branch block. and subarachnoid hem-orrhage. Significant rebrill di""""e. ,uch as subilrnchnoid hemorrhage, may be associated with dply inverted T waves (called cerebral T waves).
Examples of T waves are shown in Figure 3-11.
QT interval The QT interval represents the time betv.-een the onset of ventricular depolariution and the end of ventricular repo-larization. The QT interval is measured from the beginning of the QRS complex to the end of the T wave (Figure 3-12).
A 1. Numbe, 01 .mall squares belwoon R wav ... '" 31. Hall 01 31", 15.
2. Numbe,oI small squ ares in aT Inlerval" 11 3. Compare the dilfe,80C9: aT inlerval " lass Ihan hal! the
RR Interval (11 small squa,es a,e I .... lhan 15small squar ... ); aT inlerval is ,..,,,,,,,110,Il-0l0 heart mta. (Dumtion of aT i1Ierval: 11 qUa'lIII x 0.04 ~"0.44 """"'.)
Rgure 3-12. OTlnt9lVal.
Duration of the QT interval can be determined by multipl\," ing the number of small squares in the QT interval by 0.04 second (Figure3-13). The length of the QT interval normaJJy
B 1. Numbe, 01 small squarllll beIw""" R WIW8S" 38. Hall DI 38" 19.
2. Numbe, 01 small squar .... in aT inl"",al" 13 3. Compare the dilfemnc:a : aT interval 10 Ie than hall the
R-R int"",aI (13 sma! square. araless than 19 .mal squares): aT inWNaI" """"allor ltd" heart rale. (OoJUl.tlon 01 aT intorval: 13 small IiqUB'1III x 0.04 ....,end" 0.52 secend.)
C 1. Numbe, Dlsmall squares betwlHln R waVil." 18. HaN 01 18,,9.
figure 3-13. aT Interval examples.
2. Numb ... Dlsmall squar .. in aT InieNaI" 13. 3. Compare the diIf ... once: aT inlerval is more than hall Ihe
R-R inlerval (13 small squares 8'" mo", than 9 small squ ares); aT Inlurval is prolonged lor this heart rate. (Dumtion olOT intorval: 13 squares ~ 0.04 second" 0.52 ....,end.)
-
varies according to age. sex. and particularly heart rnte. The QT interval is more prolonged with slow heMt rates.
Generally speaking. the normal QT interval should be less than half the R-R interval (the distance between two consecutive R wavu) when the rhythm is regular. The determination of the QT interval should be made in a lead where the T wave is mod prominent and shouldn't include the U W
-
22 Waveromls, intervals, segments , and complexes
absence isconsidtred abool1T\aL llle U wave represents late repolarization of the wntricles, probably a small ~ment of the wntrides.
The waveform begins as the deflection leaves baseline and ends when the deflection returns to baseline. Normal U wawsare small. rounded. and symmetrical, positive in lead II (a pruitiw lead), and 2 mm or less in amplitude (always smaller than the preceding T wave). The U wave can best be seen when the heart rate is slow.
Abool1T\al U waves are tall (greater than 2 mm in height ). Common causes include hypokalemia, cardio-myopathy. and left wntricular enlargement. among other causes. A large U wave may occasionally be mistaken for a P ....
-
Waveform practice; Labeling wlives 23
Waveform practice: Labeling waves For each of the following rhythm strips (strips 3-1 through 3-14). label the P. Q, R. S. T, and U waves. Some of the strips may not have all of these wa ... efornu. Check )'Our answers with the answer key in the back of the book.
Strip 3-1 , Strip 32,
strip 3-3. Strip 3-4.
strip 3-5. Strip 3-&.
-
24 Waveforms, intervals, segments, and complexes
Strip 3-7, Strip 3-8.
Strip 3-9, Strip 3-10,
Strip 3-11. Strip 3-12,
Strip 3-13. Strip 3-14,
-
fil Cardiac monitors -I'
Purpose of ECG monitoring The electrocardiogram (EeC) iSI! reoordingofthe electrical activity of the heart. The ECC records two basic electrical processes: Drpo/ariZl.ltKJn - the spread 01 the electrical stimulus through tm heart muscle, producing the P wave from the atria and the QRS oomplex from the ventricles. Rrpo/arizotion - the recovery 01 the st imulated mus-cle to the resting state. producing the ST segment. the T walle, lind the U wave.
The depolariultion-repllarization process produces electrical currents thai are transmitted to the surface of the body. This rJectrkaJ activity is detected by electrodes attached to the skin. Mer the electric current is detected. irs amplified, displayed on II monitor screen (oscilloscope), lind Ncorded on ECC graph paper as waves and complexes. The ..... aveforms can then be analyz;ed in iI ~ttmalic man-ner and the ~cardiac rhythm" identified.
Bedside monitoring allows continuOU$ observation of the heart's electrical activity and is used to identify arrhythmias (d isturbances in rate. rhythm. or conduction). evaluate pactmaku function, and evaluate the response to medications (for e:JIdlllple, antiarrhythmies). Continu-ous cardiac monitoring is useful in monitoring patients in critical care units, cardiac stepdown units, surgery suites. outpatient surgery departments, emergency departments, and postaoesthnia reco\'el)' units.
Types ofECG monitoring There are t~'O types of ECG monitoring: hordwirtl 4Ild telemetry. With hardwire monitoring (bedside monitor-ing), electrode pads (conductive gel diKS) a re placed on the patient's chut and attached to a lead-cable sys-tem and then connected to a monitor at the bedside. With telemetry monitoring (portable monitoring). elec-trode pads are attached to tht patient's ches t and con-nected to leads that are attached to a portable monitor transmitter_ Haruwire motliton"ng - Hardwire monitoring uses either a filJf!-leadwire system or a three-leadwire system_
With the fiw,-Ieadwire S)'!i tem (Figure 4-IJ. five elee. trode pads and five leadwires are used. One electrode is placed below the right clavicle (2nd interspace. right
/ , AL+---\!f>! ';jf,f-tLL
FIg"re 4-1. HaOWIre morvtrIng - FtYe Ie8an'lre system. ThIs lluslratlon shc!Ws you wtlere 10 place the electrodes and
attadlleadw~9S using a fNe-leaCWIre system. The IeaCWlres are coIor-c:od9d as tOiIOWS: white - right ann (RAJ black - left ann (LA) green - right leg (Rl) red -left leg (U) broINn - cllest (C).
leads placed in the arm Md leg positions as shoNn al:m )00 to view leads ~ I," aVR, aVL. and aVF. To view chest leads V,-V,. the dMIst lead must be placed in the speeD: chest lead posHkln desired. In this example, the brown chest lead Is In V, posifun.
middavicular line), one below the left clavicle (2nd inter-spa~, Idt midclavkular line), one on the right lower rib cage (8th intenp.xe, right midclavicuJar lint), one on the left lov.-er rib cage (8th interspace, Jdt midclavicular line), and one in achest lead position fY, to V.). The SDc chest lead positions (Figure 4-2) include: V, - 4th intercostal space. right sternal border V, _ 4th intercostal sPi\te, left stunal border V.-midv.-aybetweenVzandV, V, - 5th intercostal space, left midclavicular line V. _ 5th intercostal space, left anterior Miliary line V. - 5th intercostal space, left midaxillary line
lhe right arm (RA) lead is attached to the eledrode pad below the right clavicle: the left arm (LA) lead to the elec-trode pad below the left clavicle; the right leg (RL) lead to the electrode pad on the right lower rib cage; the left
25
-
26 Cardiac monitors
J
I
flgLlre 4-2, Chest load posKIons,
leg (LL) lead to the electrode pad on the left lower rib cage: and the chest lead to the electrode pad of the specific chest position desired (V, through V,l.
With the five-leadwire system for hardwire monitor-ing, you can continuously monitor two l~ads using a lead selector on the monitor. Leads placed in the arm and leg positions allow you to view leads I, II, III, AVR, AVL, and AVF (Figure 4-1). To view chest lead V, to V" the chest lead must be placed in the specific chest lead position desired. Generally, a limb lead (usually I, II. or III) and a chest lead (usually V, or V,) are cho~n to be monitored.
With the three-leadwire system (Figure 4-3), three elec-trode pads and three leadwires are used. One electrode pad is placed below the right clavicle (2nd interspace, right midclavicular line), one below the left clavicle (2nd inter-space, left midclavicular line), and one on the left lower rib cage (8th interspace. left midclavicular line). The RA lead is attach~d to th~ electrode pad below the right clavicle,
Moddk>d CI>oc1 Lc.:>d v, (MCL,)
J
RIILl re 4-3. HardW __ e monKorhg - ThrOO-lerulWire system. lhls IIklslraUon shoWs you where to place the electrodes II1d attach leadwlres using a three-leadWlre system. The lead wires are color-coded as Iollows: white - right arm (RAj black -left arm (LA) red -left leg (LL).
Leads placed in this position will allow you to monitor leads I, II, or III using the lead selector on the mon~or.
the LA lead is attached to the electrode pad below the left clavicle, and the LL lead is attached to the electrode pad on the left loy,-er rib cage. You can monitor either limb leads I. II. or III by turning the lead ~Iector on the monitor. Although you can't monitor chest leads (V, to V,) with a three-leadwire system, you can monitor modified chest leads that provide similar infonnation. To monitor any of these leads. reposition the LL lead to the appropriate posi-tion for the chest lead you want to monitor, and turn the lead ~Iector on the monitor to lead III. Examples of modi-fied chest lead V, (HCL,) and modified chest lead V, (HCL, ) are shown in Figur~ 4-4.
ModIk>d CI>oc1 Lco.d V. (MCL,,)
Figure iI-il. HardWlra monnor1ng - Tllree-leadwlre system: Leads MCL, and MCt... Modified chest leads can be monitored with tho three-leadW __ o system by reposRlon1ng tho len leg (U) lead to the chest position desired and tumlng the lead selector on tho monttor to lead III.
-
I
RguflI 4-5. Telemetry monnorllg - Rve-leadwtre system. lhls illustration shoWs you wtlefe to place the electrodes a1d attach leadwlros USDJ a 11Ye-leadWlru system. The leadWlres are COior-COCIed as TOIIOWS: white - right arm (RAJ black -left arm (LA) green - right leg (RL) red -Ieflleg (LL) brown - chest (C).
With the fiye-Ieadwire system for telemetry monitoring you can monitor anyone of the 121eads using a lead selector on the
mon~or. Leads placed in the convenlionallimb positions allow you to view leads I, II, III, aVR, aVL., and a\'F. To view cheslleads V,-V" the chest lead must be placed in the specific chest lead desired.
Telemetry monitoring - Wireless monitoring, or teteme!!),. gives your patient more freedom than hardwire monitoring. Instead of being connected to a bedside monitor. the patient is connected to a portable monitor transmitter. which can be placed in a pajama pocket or in a telemetry pou,h. Telemetry monitoring systems are available in a five-Ieadwire system and a three-leadwire system.
The five-Ieadwire system for telemetry (Figure 4-5) is connected in the same manner as the fiw-Ieadwire sys-tem for hardwire monitoring with the four limb positions (RA. LA. RL. and LL) in the conventional locations and the 'hest leads pla,ed in the dnired V! to V, location. With this system you can monitor anyone of the 12 leads using a lead selector on the monitor. Leads placed in the limb positioru; as shown in Figure 4-5 allow you to view leads I. II. Ill. AV . AVe' or AV .. To view chest leads V, through V, . the chest lead must be placed in the specific chest lead position desired.
The three-leadwire system for telemetry (Figure 4-6) uses three electrodes and three leadwires. The lead wires are connected to positive. negative. and ground connec-tions on the telemetry transmitter and attached to elec-trode pads placed in specific chest lead positions (leads I. II. III. MCL,. and MCL, ). Only one lead position can be
Troublesh ooting monitor problems 2 7
monitored at a time. and a lead selector on the monitor isn't aVililable.
Applying electrode pads Proper attachment of the electrode pads to the skin is the most important step in obtaining a good quality ECG tra,-ing. Unless there is good contact bet"'een the skin and the electrode pad, distortions of the ECG tracing (artifacts) may appear. An artifact is any abnormal wave, spike. or movement on the ECG tracing that isn't generated by the electrical activity of the heart. The procedure for attaching the electrodes is as follows: Choose monitor lead position. It's helpful to assess the 12-lead ECG to ascertain which lead provides the but QRS complex voltalle and P wave identification. Prepare the skin. Clip the hair from the skin using a clipper; hair interferes with good contact between the electrode pad and the skin. Using a dry washcloth. wipe site free of loose hair. If the patient is perspiring and the electrodes won't stay adhered to skin, apply a thin coot of tincture of benzoin and allow to dry. Attach the electrode pads. Remove pads from packag-ing and check them for moist conductive gel; dried gel can cause loss of the ECG signal. Place an electrode pad on each prepared site. pressing firmly around periphery of the pad and avoiding bony areas. such as the clavicles or prominent rib milrkings. Connect the leadwires. Attru:h ilppropriilte leadwires to the electrode pads according to established electrode-lead positioru;.
Troubleshooting monitor problems Many problems may be encountered during cardiac monitoring. The most common problems are related to patient movement. interference from equipment in or neilr the patient's room. weak ECG signals. poor choice of monitor lead or electrode placement. and poor contact between the skin and electrode-Ieild attachments. Moni-tor problems 'an ,ause artifa't,s on the ECG tracing, making identification of the cardiac rhythm difficult or triggering false monitor alarms (false high-rate alarms ilnd false low-rate alarms) . Some problems are poten-tially serious ilnd require intervention, whereas others are temporary. non-life -threiltening occurrences that will correct themselves. The nurse and monitor technician need to be proficient in recognizing monitoring prob-lems. identifying probable causes. and seeking solutions to correct the problem. The most common monitoring problems are: FalsehifIJ-ratealarms ~ High-voltageartifact potentials are commonly interpreted by the monitor as QRS complexes
-
28 Cardiac monitors
G G G
lead II Lead III
Negative lead - 2nd Interspace right midclavicula, line
N"9IIti .... lead - 2nd Intonp""" right midclavicular Ii""
N&gative lead - 2nd inlelSplOCe lelt midclavicula, line
Podive load - 2nd Interspace left midcIDVic .... a' Ii""
Positive klad -11th Interspa::e left midclavicular II""
Positil'll Iliad - 8111 Inl9f&paoo lelt midclavicula, line
Ground load - 8th InllH'ap""" right midclavicula, line
Ground lead - 8th interspace right midclavlc:ular Ii""
Ground lead - 8111 Interspace 'ight midclavicular ina
ModifIed Chest Lead V, (MCL,) N&g8tive lead - 2nd Interspace 19ft midclavicula, line
Positi .... lead - 4th interspace right 5t&mal borde,
Ground I9I1d - 8th ntar5piICII right midclavicul9, I""
Figure 4-6. Telemetry monRMng: Three-leadwlm system.
G
tdodfted Chest leed V. (MC!..,;) Negative lead - 2nd interspace lelt midclavicula, lina
Positive lead - 5th intlH"space lelt midaxila ry Ina
Grourlllaad - 81t! InllH"spac6 right midclavicula, line
TM II1ree-leadwlrs system uses 1111'98 electrode pads and three leadWlres. Tho leadwlres lI'e connocted to JXlSRlYe. negative, or ground connections on thetelemetry transmitter and attached to spectnc lead posKIons (lead I, lead II. lead III, lead MCL" or lead MCLJ. Only one lead posRIon ClI'1 be monitored at a Dme.A lead selector 1sn1 available.
and acti"ate the high rate alarm. Most high voltage arti facts are related to muscle movements from the piltient turning in bed or moving the extremities (Figure 4-7). Seizure activity can also produce high-voltage artifact potentials (Figure 4-8) . False low-rate alamu - Any disturbance in the trans-mission of the electrical signal from the skin electrode to the monitoring system can activate a false low-rate alarm (Figures 4-9, 4-10, 4-11. and 4-12). This problem is usu-ally caused by ineffective contact bd""een the skin and the electrode-Ieadwire system, resulting from dried conductive
gel, a loo"e electrode, or a disconnected lead wire. Low voltage QRS complexes can also activate the low-rate alarm; if the ventricular waveforms aren't tall enough. the monitor detects no electrical activity and will sound the low-rate alarm. Muscle tremors - Muscle tremors (Fil/ures 4-13 and 4-14) can occur in tense, nervous patients or those shiver-ing from cold or having a chill. The ECG baseline has an uneven, coarsely jagged appearance, obscuring the wave-forms on the ECG tracing. The problem may be continuous or intermittent.
-
Troubleshooting monitor problems 29
Figure 4-7. Patient movement cause: str1ps above shoW pallent turning In bed Of extremity movement. SOIUtIm: Problem Is usually Intermittent and no corractlon Is necesay. Movement tRact C~ be reduced by avoiding placement 01 electrode pads In areas where extremity movemenlls greatesl (bony areas such as the davldes).
FIgure 4-8. Setzln actlVlly C
-
30 Cardiac lllonilOrs
Figuf1l 49, cont~uous straight Ina, QIJs,: DI18C1 conciJc1tt'a gaI,dl!ro"tl8Ctad lead wire, or dlsconn8cted el8ctrooa pad, sotJItm: Qlack ellM:trode-lead syslem; re-prep alii fe-altach electrodes .nI1oacIs as necessary. fJie: A straight line may also h:llcali! the msenc:a 01 electrical acttvfty ~ thell8llt; the patJant must be avaIual9d Immediately !of the presenca 01 a pulse.
Figure 4 1 O. ~termttblnt straIgIIt line. GaUS8: r.ef1actNe contact betWiIen SkIn and electrooa pac:!. SDIIIt/on: Make sure hair Is Clpped .nI electrode pad Is pI;Qd on clean, dry skin; " dlaph:lresls Is a problem, prep skin SII1'ace wtth Unctln 01 benZoin solIIIon.
Figure 4 11 . conUrwus low waveform 'I1tagi. GaUS8:LowYOIIage QftS compleJDIIS. so.tstIon:lUm ~ amplItUde (gain) knob on monlor or change lead positions.
-
Troubleshooting monilor problems 31
Fi llure 4-12. Intermment loW waveform YO!t
-
32 Cardiuc monilOrs
Figure 4-14. .,lBrmltlenl musde 1r1lfl1CX. caUSI1: Muscle trernon thaI ClCClI' nlefmlllenlly. Sdu/fa!: correction Is usually unllBalSSal)'. Nol6: In this str~, the palleR lias two p waves precedtrY;j each ORS complex \S8COOO-degrae atTklVenIrt:utaf block, MOOIIZ 11).11 the muscle trem!n went continUOUS (as In Agulfl 4-13). yQJ wOUlCl be unable 10 identity this S8f1OUS IITt1ythmla.
Figure 4-15. Telemetry-rlllated Interference. cause: ECG sI!1lals 1I"e poorly received ~er the telemetry system causing sharp spIIes nI someUmes kiss 01 signal recepllon. ThIs problem Is usually lfllated to wmk batteries or the transmltlef being usalin the outer fI1nges 01 Ihe ~11on lI"ea lor the base stallon receiver. SdutJon: Ctlange batteries; keep pall8nlln recepUon area 01 base station receivers
Telemetry-related interference - Te lemetry-related artifacts occur ",-hen the ECG signals are poorly received owr a telemetry monitoring 5)'Stem (Figure 4-15). Weak ECC signals are caused by weak batteries or by the trans-mitter being used in the outer fringes of the reception area
of the base station receiYer, resulting in sharp spikes or straight lines on the ECC tracing . Ekdrical interference lAC intmerence) - Electrical interference (Figure 4-16) can occur ",-hen mUltiple pieces of electrical equipment are in use in the patient's room;
-
Troubleshooting monitor problems 33
Figure 4-16. Electrical Interference (N:, Interference). CBUS8: Patient using electrical eq.Jlpment (electric razor. ha~ dryer); muttlple electrtcal equip-ment In use In room; Improperly grounded equipment; loose electrical connecUons or ex-posed w~lng. So/UtJon: K paUent Is using electrical equ~men~ problem Is transient and will wrloclIloolf.If pallunilli nul us-Ing electrical equipment. lIlplug all equ~ment not In contl1u-ous use. remat'e from service lIld report any equipment wtth breaks or wires sIlowhg. lIld ask the electrical engineer to check the wlrhg.
FIgure 4-17. wandertng baseline. CBUS8: Exaggerated resp~atory movements usually swn In paUents In respiratory distress (paUents with chronic obstructlvo pulmonary disease). So/uIIon: AYOId placing electrode pads In lI'BaS where mOYOOler1ts 01 the accessory muscles 1I'lI most exaggerated (Which can be anyw1lere on the
-
Analyzing a rhythm strip
There are filii! basic steps to be fonowed in analyzing II rhythm strip. ~h step should Ix followed in sequence. Eventually this will become II habit and \\;11 enable you to identify II strip quickly and accurately.
Step 1: Determine the regularity (rhythm) ofthe R waves Starting at the left side of the rhythm drip. place an inda card above the first two R waves (Figure 5-1). Using a sharp pencil. mark on the index card .bove the tv.'O R waves. Measure from R wave 10 R wave acro" the rhythm strip. marking on the index card any variation in R wave regular-ity. If the rhythm varies by 0.12 ~nd (3 small squares) or more between the mortesl and longest R wave variation marked on the index card. the rhythm is irregular. If the rhythm doesn't vat'}' or lIaries by Ius than 0. 12 second. the rhythm is considered regular.
Calipers may abo be used, instead of an index card. to determine regularity olthe rhythm strip. R waw regularity is assessed in the same manner as with the index card, by placing the two caliper points on top of two consetutive R waves and proceeding left to right across the rhythm strip. noting any variation in the R-R regularity
The author prefers the index tard method, because eath R wave variation (however slight) can be IJUIrked and meas-ured to determine if a 0_12-second or greater VilTiante e:J[ists between the shorter and longer R-wave variatiom, With
Figure 5-1. Index ca-a.
34
calipers. a variation in the R-wave regularity may be noted, but without marking and measuring between the short-est and longest R-wave variation, there is no way to deter-mine how irregular the rhythm is, Examples of rhythm measurement are shown in Figures 5-2. 5-3. and 5-4.
Step 2: Calculate the heart rate This measurement will al ....
-
Figure 5-2. Regularrhythm; R-R Intervals do not vary.
Figure 5-3. Irregula' rhythm; R-R ~terYais vary by 0.32 second.
Figure 5-4. Regular rhythm; R-R Intervals vary by 0.04 socoOO.
Other hints When rhythm strips have a premature beat (Figure 5-11). the premature beat isn't included in the calculation of the rate . In this example the fin;t rhythm is regular and the heart rate is 68 beats per minute (22 small squares between R waws = 68).
When rhythm strips have more than one rhythm on a 6-second strip (Figure 5-9), rates must be calculated for each rh}1hm. This will aid in the identification of each
Step 2: Calcula te the heart ra te 35
rhythm. In the example. the first rh}1hm is irregular "lUllh~ h~"rl r .. l~ i. 1401>0: .. 1. p'" lUiJlul~ (7 R "' .. "". ill 3 seconds x 20 = 140). The second rhythm is regular and the heart rate is 250 beats per minute (6 small squares between R waws = 250).
When a rhythm coven; It'SI; than 3 seconds on a rhythm strip (Figure 5-10). rate calculation is difficult. but not impossible. In the example. the first rhythm takes up half of a 3-second interval. There are only two R waves.
-
36 Analyzing a rhythm strip
Figure 5 5. ECG graph paper.
Figure So6. Regular rhy1tV1I; 25 small squares between R waves '" 60 heart rate.
Figure 5-7. n-egular fhytIIm; 11 R waves)( 10 '" 110 heartralB.
Therefore , you can't determine if the rhythm is regular or irregular. In this situation. multiply the two R waves by 40 (I Yi second x 40 '" 60 seconds. or the heart rate per minute) to obtain an approximate heart rale of 80 beats per minute. The second rhythm is regular. with a heart rate of 167 beats per minute (9 small squares between R waves '" 167).
As you hav'e seen. rh~1hm strips may have one rhythm or sevoeral rhythms. Therefore, each rhythm stTip may havoe one ans .... -er or several al1SY>ers. Figures 5-8, 5-9, and 510 have two different rhythms and thus MOO different answers. Each rhythm on the strip must be analyzed sepa-rately. When interpreting a rhythm strip. describe the basic underlying rh~thm first. then add additional information.
-
Step 2: Cnlcul nte the henrt rIl te 3 7
Allure 5-8. Rhythm With prematura beat.
Allure 5-9. Rhythm stlp wlltl two dlnerenl mythms.
Agure 5-10. calculallng rate wtIen a mytlvn COYen less IIIan 3 seconds.
-
38 Analyzing a rhythm strip
Figure 5-11 . NonnaiPwaves.
fillure 5-12 . Allllurrnal PWlfYlI!:S.
Figure 5-13. PR Ilterval 0.16 second.
Box 5-1. Rhythm strip analysis
1. De1ermlne regula~ty (rhythm). Z. C~k:U1iI1I! Hill!. 3. examine P waves. 4. Measure PR In1erval. 5. Measure aRS complex.
Flgure 5-14. aRS complex 0.12 seo:.od.
such as normal sinus rhythm with one premature ventric-ular contraction (PVC) (Figure 5-8).
Stl!P 3: Idl!nlify amll!xaminl! P wavl!s Analyze the P waves; one P wave should precede each QRS complex. All P waves should be identical (o r near identical) in size. shape, and position. In Figure 5-11
-
Agure 5-15. ORS complex (l.l(l secooo.
there is one P wave to each QRS complex, and all P waves are the $ame in si~. shape. and position. ]n Figure 5-12 there is one P wave to each QRS complex. but the P waves vary in size. shape. and position across the rhythm strip.
Step 4: Measure the PR interval Measure from the beginning of the P wave as it leaves baseline to the beginning of the QRS complex. Count the number of small squares contained in this interval and multiply by 0.04 second. In Figure 5-13 the PR interval is 0.16 second (4 small squares It 0.04 second", 0.16 sewnd).
Step 5: Measure the QRS complex Measurefrom the beginningoftheQRS complex as it leaves baseline until the end of the QRS complex. when the ST segment begins. Count the number oIsmall squares in this measurement and multiply by 0.04 second. In Figure 5-14 the QRS compt~ takes up 3 small squares and represenb 0.12 second (3 small squares x 0.04 second '" 0. 12 second). In Figure 5-15 the QRS compl~ takes up 2Y.i small squares and represents 0.10 second (2Y.i small squares x 0.04 second '" 0.10 second).
If rhythm strips are analyud using a syslematic step-bystep approach (Box 5-1). accurate interpretation will be achieved mosl of the time.
Step 5: Mellsure the QRS complex 39
-
40 An alyzing a rhythm strip
Rhythm strip practice: Analyzing rhythm strips Analyze thf following rhythm strips using the five-step proceS$ diKulSed in th is chapter. Check )'OUr answen wi th the answer key in the append br: .
Strip 5-1 . 1Wlythm: _________ ", .. " _______ _ Pwave: _____ _ PR il\eMII: DRS t:OII1p1ex: _____ _
Strip 5-2. lIlythm: __________ ,.,,, _______ _ Pwave: _____ _ PR in\eMII: DRS oomplex:' _____ _
Strip 5-3. lIlythm: _________ ""," _______ _ Pwave: ____________ __ PR illeMll: ORS t:OII1plex: _____ _
-
Rhythm strip practice: Analyzing rhythm s trips 41
'.,'5 . ""'",, ________ ... , ______ _ Pwave: ____ _ PR.,IMvaI: ORScomplex: _ ____ _
Strip 5-5. Rhyttwn: _________ .... _______ _ Pwave: _____ _ PR.,IeMII: ORScomplex: ____ _
Strip 5-6. RhytIwn: _________ .... _______ _ Pwave: _____ _ PR.,IeMII: ORScomptex: _____ _
-
42 Analyzing n rhythm strip
SttlpS-7. lIlyIhm: _________ R"" ______ _ Pwave: _____ _ PR illefval: ORS cornpleJ:: _____ _
Strip 5-8. lIlyIhm: _________ R"" _______ _ Pwave: _____ _ PR 1n1eMl1: ORS complex: _____ _
Strip 5-9. FIlythm: _________ ,.,,, _______ _ Pwa'o'e: _____ _ PR inlefval: ORS compleJl: ______ _
-
Rhythm strip practice; Analyzing rhythm strips 43
strip 5-10. 1V1ytIvn: _________ Rate: _______ _ Pwa..,,: _____ ~ PR lilt ..... : OAS complex: _____ ~
strip5-11 . RhytI"rn: _________ Ratt: _______ _ Pwa..,,: _____ ~ PR inlerwt: CRS complex: _____ ~
-
Sinus arrhythmias
Overview The term arrhythmia (abo called dysmythmia) is very general. rderriog to all rhythms other than the nor-ITIlIl rhythm of the heart (normal sinus rhythm). Sinus arrhythmias (Figu re &-1) result from disturbances in impulse discharge or impulse conduction from the sinus node. The sinus node retains its role as pacemaker of the heart. but discharges impulses 100 fast (sinus tachycar-dia) or too slow (sinus bradycardia); discharges impulses irregularly (sinus arrhythmia); fails to discharge an impulse (sinus arrest ); or the impulse discharged is blocked as it exits the sinoatrial (SA) node (SA exit block). Sinus bradycardia. sinus tachycardia. sinus arrhythmia. sinus arrest, and sinus block are all considHed arrhyth-mias. However, sinus bradycardia at rest. sinus tachycar-dia with aen:ist, and sinus arrhythmia associated with the phases of respiration are considered normal responses of the heart
Normal sinus rhythm Normal sinus rhythm (Figure 6-2 and Box 6-1) reflects the heart's normal electrital activity. TIle SA 00!k normally initiates impulses at a rate or 60 to 100 beats per minute.
No rmal sinus rhythm
Since th is rate is faster than other pacemaker sites in the conduction system, the SA node retains control as the pri-mary pa.cemaker of the heart . Sinus rhythm originates in the SA node and the impulse follows the normal Induc-tion pa.thway through the atria, the AV node, the bundle branches, and the ventricles, resulting in normal atrial and ventricular depolarization.
80a i-1. Normal sinus rhythm: Identifying ECG features
Rhythm: "". PW''IIiII:
"' .. 60 to 1 00 tJeallolmlllJle Normal In stze. sIlape, and tinction: posltlYe In 1eaCI1: one P WlIYfI!r9CEide5 each ORS complex
PH IntiIn'aI: Normal (0.12" 0.20 second) QRS comple.: Normal (0.10 sean:! or less)
Normal sinus rhythm is regular with a heart rate between 60 and 100 beats per minute. The P waves are nor-mal in size. shape. and direction: positive in JeadJl (a positive leadl, ... ith one P wave pre
-
Agure &-2. NOrmal sInUs Iflythm. Rb)'Ulm: Regular Rate: 8-4 beats/minute P waVlI: NOrmal ar.IIX"8C8CIe each ORS PRlnlllrYaI: 0.14toO. 16 ll9al1ld DRS complU: 0.06100.08 secood.
nonnallimits. Normal sinus rhythm is the normal rhythm of the heart. No treatment is indicated.
Sinus tachycardia Sinus tachycardia (Figure 63 and So)[ 62) is a rhythm thai originates in the sinus node and di~harges impuL'IeS regularly at a rate bew,et:n 100 and 160 beats per minute. The P waves .re normal in s~e. shape, and direction: po$i live in le
-
46 Sinus nrrhylhmins
heart rate slows down. Sinus tachycardia begins and ends gradually in contrast to other tachycardias ...... hich begin and end suddr:nly.
Sinus tachycardia can be caused by anything that increases sympathetic lone or anything thai decreases pal'Mympathelic lone. Factors commonly associated with sinus tachycardia are: anxiety. ucitement. stress. exertion. exercise fewr. nnemia. shock hypoxia. hypovolemia. hypotension. heart failure. hyperthyroidism pain, pulmonary embolism (sinus tachycardia is the most common arrhythmia seen with pulmonaryemboJism) myocardi;lJ ischemia. myocardial infarction (M!) (sinus tachyeardia persisting after an &cute infarct implies exten-sive heart damage and is generally a bad prognostic sign) drogs that increase sympathetic tone (epinephrine, nortpinephrine, dopamine. dobutamine, tricyclic antide-prtS5ants, isoproterenol. and nitroprusside) drogs that dec re;ue parasympathetic tone (atropine) use of substances such as caffeine, cOGline, and nicotine.
Sinus tachycardia is usually a benign arrhythmia and treatment is directed at correcting the underlying cause (relief of pain, fluid replacement, rtmoval of offending medications or substances, and reducing fever or anxiety). Ho ..... ever, persistent sinus tachycardia should never be ignored in any patient, especially the cardiac p.1lient. A rapid heart rate increases the workload of the heart and ib oxygen requ irements and IT\iJ)' cause a decr\\il$ed stroke volume leading to a decrease in cardiac output. In addi tion, heart rates higher than norm;lJ decrease the amount of time the heart spends in diastole, leading to a decrease in coronary artery perfusion (coronary arteries are perfused
Figure 6-4. RllyItIm: R ...
Sinus bradycardia, Regula'
" ... -P WaY": Sinus PH Interval: 0.20 second ORS complex: 0.06 to 0.00 second
du ring diastole), Sinus tachy
-
Sinus bradycardia can be caused by anything that incrtases potrMympathetic tont or anythinQ that decrtastS sympotthetic t~. It commonly OCCUI1l with the following: during sleep and in athldes in acute inftrior waH!>!1 involving the right coronuy artery. which usually supplies blood to the SA node as a reperfusion rhythm after coronary angioplasty or afte r treatment with thrombolytics v&gal stimulation from vomiting, bearing down (VaJsalva's maneuwr), or carotid sinus pressure !IS a vasovagal reaction. A vasovagal reaction is an utrtme body rtsponse that causes a marked decrease in neart rate (due to vagal stimulation) and a marked decrease in blood preswre (due to vasodilation), This reaction may ocaJr with potin, nausea. vomi ting, fright. or :ltJdden stres.s-ful situations. The combination of extreme bradycardia and hypotension may re:ItJlt in fainting (vaKIYagal syncope). The situation is usually reversed ..... hen the individual is placed into a reaJmbent position, thertby increasing venous return to the heart. If fainting occurs ..... ith the indi-vidual in a recumbent position. it can usually be revel1loed with leg elevation. carotid sinus hypersensitivity syndrome. sleep apnea decreased metabolic rate (hypothyroidism. hypother-mia); hyperkalemia sudden movement from recumbent to an upright posi-tion (common in the elderly) increased intracranial pressure (II. sudden appea rance of sinus bradycardia in 11 pottient with cerebral edema or subdural hematoma is an important clinical obselVation) drugs such .s digoxin, ca lcium channel blockel1l, lind beta blockers degenerative disease of the sinus node (sick sinus syndrome), Pel1listent sinus brAdycardia is the most
Allure 6-5. RII)'II1m:
-P waws: PIt ln18rYaI:
SInus arrflrthmla negular SO beal&mloote Normal In ron1Iguratloo; precede eadI 0fIS 0.12 to 0.1 4 second
ORS complex: 0.06 to 0.08 second
Sinus arrhythmia 47
common and often the earl iest manifestation of sick sinus syndrome, Sick sinus syndrome is a dysfunctioning sinus node ...... hich is manifested on the ECG by marked bradyar-rhythmias al ternating with episodes of tachyarrhythmias and is commonly accompotnied by symptoms :ltJch!lS dizzi-ness. fainting episodes, chest pain. shortnen ofbnath. and heart failure. This syndrome has also been called tachy-brady sfI71drome. Permanent pacemaker implantation is
recomm~nded once patients become symptomatic. Sinus bradycardia doesn't require treatment unless the
patient becomes symptomatic. Some cliniCllI silins lind symptoms requiring treatment include cold. clammy skin: hypotension: shortness of breath, chest pain, changes in menta l status. decrease in urine output, and heart failure. If sinus bradycardia persists, the treatment of choice is atropine, a drug that increases the heart rate bydecrea!iing p.1rllSympathetic tone. 'l'ht usual dost is 0,5 rug IV push every 5 minutes unti l the bradycardia is resolved or a maxi-mum dose of3 mg is given. Atropine must beadministered correctly; atropine administered too slowly or in d05e5 less than 0.5 mg can further decrease the heart rate instead of ifl(:re.uing it. If the rhythm still doesn't resolve lifte r the atropine is administertd. 11 transcutaneous (external) or transvenous potcemaker may be needed. All medications that cause a decrease in heart rate should be reviewed lind disoontinued if indicated. For chronic bradycardia. perma-nent pacing may be indicated.
Sinus arrhythmia Sinus arrhythmia (Figure 6-5 and Box 6-4) is a rhythm that originates in the sinus node and discharges impulses irreg-ularly. The heart rate may be normal (60 to 100 beats per minute) or slow (commonly associated with a brMlycardic
-
48 Sinus arrhythmias
Box , ..... Sinus arrhythmia: Identifying ECG features
Rhythm: Irregular Ratl: Normal (60 to 100 beats/mtlute) or SlOW ~ess \han
60 bealslmlnute) P waves: Normal., slm, shape.1Ild d ~ectlon; posRIvo In
lead II; OI1e Pwave precedes each OAS complex I'A InteMI: Normal (0,12 to 0,20 second) QAS complex: Normal (0.10 secooo or less)
rate). The P wav~ are normal in sne. shape. and direction: positive in lead II (a positive lead). with one P wave pre ceding each QRS complex. The duration of the PR interval and the QRS complex is with in normal limits. The distin guishing feature of this rhythm is the sinus origin ood the rhythm irregularity.
Sinus arrhythmia is commonly lWOCiated with the phas~ of respiration, During inspiration. the sinus node fires faster; during expiration. it slows down. This rhythm is an extremely conunon finding among infants. children. and young adults. but may occur in any agegroup. Sinus arrhythmia is a normal phenomenon that usually doesn't require treatmenl unlen it iSilccompanied bya bradycardia rate that causes symptoms.
Sinus pause (sinus arrest and sinus exit block) Sinus pause is II broad term used to describe rhythms in which there is a sudden failure of the SA node to initiate or conduct an impulse, Two rhythms fall under this category:
Figure &-6. Normal sinus rhythm with sinus block. Rhythm: Bask: rhythm regular; Irregular during pause Ratl: Bask: rhythm 84 boatslmlrute P W3'les: Normal In basic rhythm;:men! rurlng pause
sinus arrest and sinus exit block. Sinus arrest and sinus exit block. two separate arrhythmias with different patho-physiologies (Figur~ 6-6. 6-7. and 68 and Box 6-5), are discuned together because distinguishing between them is at times difficult. and because Iheir treatment and clinical significance are the same.
Box 6-5. Sinus arrest and sinus ellit block: Identifying ECG leabJres Rhythm: Bask: rhythm usually I"lIgular; there Is a sudden
pause In the bask: rhythm (causing Irregularity) with one or mol"ll missing beals; neart rate may slOW dOWn lor seY9r81 beats aner paJS8 ~ernporay rate suppression) 001 returns 10 bask: rate
Rate: lhal oIl.11derlyllg rhythm. usually stlus P Way": Sinus P waY9S with bask: rhythm; absenl dlSlng
""~ P1Itnt,rval: Normal (0.12 to 0.20 second) with DaSI& rl'ly1hm: absent during pause
QRS complex: Normal (0.10 second or less)wllh basic rhythm; absent during pause
DlffMMtlarlffj fH fU" $ SinUI~; Basic rhythm (R-R regJlarlty) I"lIsumes 011 Urns alter
"'"~ SInus Irmt: Bask: rhythm (R-R regJlarlty) doesn't resume on Ume alter pause
Both sinus arr~t and ~inus e)lit block originate in the sinus node and are characterized by a sudden pause in the sinus rhylhm in which one or more beats (cardiac cycles)
PR Interval: 0.16100.18 second In basic rhythm; :ment rurlng pause QRS complex: 0.08100.10 second In basic rhythm; :ment rurlng pause comment: ST-segment depression Is present.
-
Sinus pause (sinus arrest and sinus exit block) 49
Figure 6-7. Normal sinus rhythm with sinus arras!. Rhythm: Basic rhythm regular.I'T~1
-
50 Sinus arrhythmias
figure 6-1, SInus armythmla WIth sinus pause. Rhrthm: Basic rhythm Irr9!rUIar Rate: 60 bBa~lfIJIe P WlI'I": Normal k'I bask; rnylMm; msenlllJrlng pause PR Inltml: 0.1.10 0.16 second In bask: rhythm; rtlsenlllJrtng pause QRS complel: 0.06100.08 second In bask; rhythm; rment IlJrtng pause COmInlIt: Because of the Irregula'lIy of the basic rnythm, slnu:s afTest can't be dIfTlIrantlaled !rom slrus block, and the rnythm Is Inter-
preted using the broad term stills pause.1ndIc:lOIV that BItIw rhythm a1JId be present
suppression is temporary and will cause a brief irregularity in the underlying rhythm. but after sewral cycles the basic rate and rhythm will return. An example of rate suppres sion is shown in Figure 6-8.
Differentiating bet'o\'een the two rhythms involves com paring the length of the pause with the underlying pop or R-R interval to determine if the underlying rh}-1hm resumes on time after the pause. This can be determined only if the underlying rhythm is regular. If the underlying rhythm is irregular. as in sinus arrhythmia (Figure 6-9). it's impossible to distinguish sinus "rrest from sinus ait block. In this case, the rhythm would best be interpreted using the broad term sinus pause. indicating thilt either rhythm could be present. Froma clinical viewpoint. distin-guishing belY.-een sinus arrest and sinus exit block usually isn't essential.
Sinus arrest or sinus exit block can be caused by numer-ous factors. including: increase in vagal (parasympathetic) tone on the SA node myocardial ischemia or infarction use of certain drugs such as digoxin. beta blocken, or calcium channel blockers.
The patient may become symptomatic if the pauses associated with sinus arrest or sinus exit block are fre-quent or prolonged. Another danger is that the SA node may lose pacemaker cont rol. 'Nhen the sinus node sl
-
Sinus pause (sillus arrest and sillus exit block) 51
Table 6-1. Sinus arrhythmias: Summary 01 Identifying ECG features
Rhythm Ral. (bIatsl p W3W1 (lead II) PR Interval DRS complex minute)
Normal sinus R~'" 6010 100 Positive in lead II; nonnal Normal (0.12 to Normal (0.10second rhythm in sim, shape, and 0.20 second) .... ,
direction; 0IIII P wave precedes each CfIS
""""" Sinus R~"" 40"60 Positive in lead II; nonnal Normal (0.12 to Normal (0.10 second bradycardia in sim, shape, and 0.20 second) .... ,
dirvction; 0IIII P wave precedes each CfIS
""""" Sinus "" ... 100 to 160 Positive in lead II; nonnal Normal (0.12 10 Normal (0.10second tachycardia in sim, shape, and o.20second) .... , direction; 0IIII P wave precedes each CfIS
""""" Sinus trreg ..... 6010 tOO(nonnaI) Pooitive in tead II; norm.1 Norm31 (0.12 to Nonn3I (0. to .cond alThytlvnia or< 60 (slow) in sim, shape, and 0.20 second) .... ,
direction; 0IIII P wave precedes each CfIS
""""" Sinus block Basic ~ usually That of oodertying Sirul P waves willi basic Normal (0.12 Normal (0.10 second and sinus regular, !here is a sOOden rhythm, usually rhythm; absent dJring 10 0.20 second) or less) with basic
.~, pause in !he basic rhythm ,~ ,.~ with basic rhythm; absent (caJsing irreguarity) with rhythm; absent d!Jing pause one or more missing IUing pause beats; temporary rete suppr9ssion common loIowing pau&e
Ddfersntiatirtg fealUrBII Sirusbio:k: Basic ~ resumes on
time after pause
Sirusarrest Basic ~ does not resume on time after .. ~
Nuts: H the basic rhythm is iITll9Uar (sinus alThythmia~ sinus arrest cant be differentiated lrom sinus block. and !he rhythm is interpretoo as sinus arrhythmia with sirllS pause.
-
52 Sinus arrhythmias
Rhythm strip practice: Sinus arrhythmias Analyze the following rhythm strips by following the five basic steps:
!>Ieasure PR interval. Measure QRS complex.
Determine rhythm regularity. Cakulatehearl rate (this usually refers to the ventricu-Iilr rate. but if atrial rate differs you nd to calculate both). Identify and examine P waves.
Interpret the rhythm by comparing this data with the ECG characteristics for each rhythm. All rhythm strips are lead II, a positive lead, unless otherwise noted. Check your ansVt'ers with the answer keys in the appendix.
Strip &-1. Rhythm: __________ Rate: _______ _ Pwave: ______ _ PR interval: ORS complex: ______ _ Rhythm interpretalion: __________________________ _
Strip &-2. Rhythm: __________ Rate: _______ _ P wave: ______ _ PR interval: ORS cornplex: ______ _ Rhythm interp-etation: ________________________ _
Strip &-3. Rhythm: __________ Rate: _______ _ Pwaw: ______ _ PR intel'lal: QRS complex: ______ _ Rhythm interpretalion: __________________________ _
-
Rhythm slrip practice: Sinus arrhythmins 53
Strip 6-4. RIryItvT1: _________ _ _______ _ Pwa..-e: _____ _ PRInIefVal: ORScomplex:, _____ _ IIJythm interpretation: _____________________ _
strip 6-5. Rhythm: _________ "'. _______ _ Pwa...e: _____ _ PRinteMlI: ORScompla:' ____ _
""""'''0''01'''''' __ ------------------
Sbip 6-6. Rhyttvn: _________ Rate: _______ _ Pwa..-e: _____ _ PRInIefvai: ORScomplex:, _____ _ IIlyttwn interpretation:
----------------
-
54 Sinus nrrhylhmioJ
Strip6-7.RhyIIvn: _________ _ ______ _ Pwave: ____ _ PR inleMll: ORS complex: _____ _ IIlythm Interp-etmon: ______________________ _
Strip 6-B.lllythm: _________ _ _______ _ Pwave: _____ _ PR 1n1eMll: ORS complex:' _____ _
IIlythmlnt~~: ______________________ _
Strip 6-9. RhytIwn: _________ '"'" _______ _ Pwave: ______ _ PR inlefval: ORS romplex:, _____ _ IIlythm Interpretmon: ______________________ _
-
Rhythm strip practice: Sinus arrhythmias 55
Strip6-10. Rhythm: _________ Rale: _______ _ Pwave: _____ _ PR Interval: ORS compleK: ______ _ Rhythm inlerpretation: __________________________ _
Strip 6-11 . Rhythm: __________ Rale: _______ _ Pwave: _____ _ PA interval: ORS complex: _____ _ Rhythm inlerpretation: __________________________ _
Strip6-12. Rhythm: __________ Rala: _______ _ Pwave: _____ _ PR interval: ORS complex: ______ _ Rhythm inlerpretalion: __________________________ _
-
56 Sinus arrhythmias
Strip 6-13. Rhythm: ________ Rate: ______ _ Pwave: _____ _ PR interval: ORS complex:
----
Rhythm Interpretatkln: ________________________ _
Strip 6-14. Rhythm: _________ Rate: _______ _ Pwave: ______ _ PR interval: OIlS complex: _____ _ Rhythm inlerpretalion: __________________________ _
Strip 6-15. Rhythm: _________ Rale: _______ _ Pwav8: ______ _ PR interval: ORS complex: ______ _ Rhythm inlerpretalion: __________________________ _
-
Rhythm snip praclice: Sinus arrh)1.hmias 57
Strip 6-Hi. Rhythm: _________ "". _______ _ Pwa",,: _____ _ PH inielVillll: ORS complex: ______ _ RhyIhmlnt8fPfMalion: ______________________ _
Strip 611, fIlythm: ________ Rate: ______ _ Pwa"": _____ _ PR inieMi: QRScornp/ex:, _____ _ RIrythm Inrerpretafun: ______________________ _
Strip6-18.Rhythm: __________ _ _______ _ Pwa",,: _____ _ PRinterval: ORScomplelC ______ _ RhyItn1 inteqlf8lation: ________________________ _
-
58 Sinus arrhythmias
Strip 6-19. fIJyttrn: ____ _____ _ _______ _ PwaY8: _____ _ PR rnervai: ORS complex:
----
Rhythm Interpntalbn: ____________________ _
Strip 5-20. Rhyttrn: ________ _ ______ _ Pwa .... : _____ _ PR ilterval: ORS cornpleJ.: _____ _ Rhythm Interpret8tIon: ______________________ _