Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks
description

Department of Cardiology and Vascular MedicineFaculty of Medicine University of Indonesia
National Cardiovascular Center Harapan Kita
ECG CHANGES IN ISCHEMIA, INJURY AND
INFARCTIONDaniel Tobing, MD, FIHA



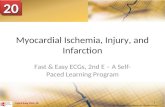
The Electrocardiogram ( ECG )

No ST ElevationNo ST Elevation ST ElevationST Elevation
Acute Coronary SyndromeAcute Coronary Syndrome
Unstable AnginaUnstable Angina NQMINQMI Qw MIQw MI
NSTEMINSTEMI
Myocardial InfarctionMyocardial Infarction
Davies MJ Davies MJ Heart 83:361, 2000Heart 83:361, 2000
Ischemic DiscomfortIschemic DiscomfortPresentationPresentation
Working DxWorking Dx
ECGECG
Biochem. Biochem. MarkerMarker
Final DxFinal DxHamm Lancet 358:1533,2001Hamm Lancet 358:1533,2001


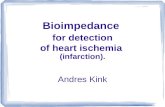
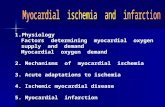
Visualization of the generation ofthe Left Ventricular portion ofthe ECG complex in Lead II
1. Septum depolarizes from the inside out and resulting depolarization wave moves away from the electrode recording Lead II
2. The rest of the ventricle depolarizes counter-clockwise from the inside out and creates the (large arrow) which is essentially, the algebraic sum of all of the small depolarization vectors. This vector is, in a normal heart, almost always moving directly toward Lead II, generating a mostly positive QRS complex
main cardiac vector
Lead II electrode60 downwardrotation angle from the horizontal 0
o
o
60o
Note: compared tothe left ventricle, the right ventricle is muchsmaller and contributeslittle to the overall mainvector of depolarization
(DEPOLARIZATION)

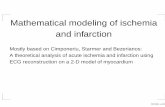
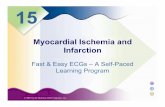
3. Repolarization can be thought of as beginning where depolarization left off
and proceeding clockwise from the lateral wall back to the septum..
4. The repolarization process proceeds at a much slower rate than depolarization so the wave inscribed (T-wave) is wide and rounded. The repolarization vector is moving away from the Lead II electrode so the inscribed T-wave is always positive
the Left Ventricular portion ofthe ECG complex in Lead II(REPOLARIZATION)
Visualization of the generation of



ISCHEMIA
• Imbalance between metabolic needs of the myocardium (demand) and the flow of oxygenated blood to it (supply)
• Affects the generation and impulse conduction delays in depolarization and repolarization
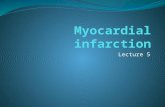
ST and T changes (on ECG)• Significant ST depression, if
– ST segment depression >0.05 mVolt at a point 0.04 second to the right of J point.
– In two or more leads facing the same anatomic area

INJURY
• Prolonged ischemia more than few minutes will cause injury
• Injured cells are still alive but will infarct (die) if ischemia is not corrected
• Do not depolarize completely, electrically more positive than the uninjured areas
viewed on ECG as ST segment elevation
Significant if: elevated > 1 mm in two or more contiguous leads

INFARCTION
• Occurs when blood flow to the heart muscle stops or suddenly decreased
• Infarcted (dead) cells are without function and can not respond to electrical stimuli
• Q wave on ECG

ST depresi dan perubahan gelombang T
• ST depresi dianggap bermakna bila > 0.05 mVolt• Titik J didefinisikan sebagai akhir kompleks QRS dan permulaan segmen ST
Bentuk segmen ST :
• up-sloping ( tidak spesifik )• horizontal ( lebih spesifik untuk iskemia )• down-sloping ( paling terpercaya untuk iskemia )
Perubahan gelombang T pada iskemia kurang begitu spesifik Gelombang T hiperakut kadang2 merupakan satu-satunyaperubahan EKG yang terlihat
ECG CHANGES OF ISCHEMIA

“J point”


SPESIFISITAS DEPRESI SEGMEN ST PADA ISKEMIA

VARIASI SEGMEN ST

Unstable angina DD/ Acute NSTEMI
Tn AS, 65 th, nyeri dada khas infark

ECG CHANGES OF INJURY (ACUTE MYOCARDIAL INFARCTION)

CONCEPT OF RECIPROCITY


ECG CHANGES OF OLD INFARCTION


Recent Inferior MCI with T-wave inversions
Tn DS, 56 th, riwayat nyeri dada khas infark 2 minggu yang lalu

LOCATING
THE MYOCARDIAL INFARCTION

• Sandapan V1 dan V2 menghadap septal area ventrikel kiri
• Sandapan V3 dan V4 menghadap dinding anterior ventrikel kiri
• Sandapan V5 dan V6 ( ditambah I dan avL ) menghadap dinding lateral ventrikel kiri
• Sandapan II, III dan avF menghadap dinding inferior ventrikel kiri
Anatomi Koroner dan EKG 12 sandapan

LOCATING THE MYOCARDIAL INFARCTION


Mid LAD occlusion after the first septal perforator (arrow)
ECG : large anterior MI


Proximal large RCA occlusion
ST elevation in leads II, III, aVF, V5, and V6
with precordial ST depression

Small inferior distal RCA occlusion
ECG changes in leads II, III, and aVF



Subendocardial ischemia. Anterolateral ST-segment depression

Acute anteroseptal myocardial infarction. Hyperacute T-wave changes are noted

Acute anterolateral myocardial infarction

Lateral myocardial infarction

Inferior myocardial infarction. Inferior Q waves with T-wave inversions

Acute inferoposterior myocardial infarction

RBBB + Anterior Infarction

Left bundle branch block






Pseudo Infarct PaternW P W
negative delta wave II,III,aVF






Early repolarization

Left ventricular aneurysm