Ebstein's anomaly: Presentation and outcome … 70 Steli sS Anomaly;: Presentation and Outcome From...
7
1 70 Steli s SAnomaly ; : PresentationandOutcomeFromFetustoAdult DAVIDS .CELERMAJER,MB,BS,MSc,FRACP,CATHERINEBULL,MA .MRCP, JANICEA .TILL, Mme, BS,BSc,*SEAMUSCULLEN,MB,CtiB,MRCPI,* VASSILIOSP .VASSILLIKOS,MD,tIAND .SULLIVAN,BMEDSet,MB,CHB,FRACP, LINDSEYALLAN, MD, FRCP,*PETROSNIHOYANNOPOULOS, D,§ JANESOMERVILLE,MB,FRCP,FACC,*JOHNE .DEANFIELD,MB, BCHIR, MRCP London,England,United Kingdom Objectives . Thisstudywasconductedtoinvestigatethepresen- tationandoutcomeofpatientswithEbstein'sanomalyofthe tricuspidvalve . Background. Ebstein'sanomalymaypresentatanyageand hasahighlyvariableclinicalcourse .Previousnaturalhistory studieshavebeenbasedonclinicalandangiographicdiagnosis andhaveincludedmainlyolderchildrenandadults .Echocardi- ography,however,hasfacilitatedfetalandneonataldiagnosisso thatthenaturalhistoryneedstoberedefined . Metho:lt . We reviewed 220 cases of Ebstein'sanomalypresent- ingfrontfetaltoadultlifebetween1958and1991,withIto34 yearsoffollow-up. Results.The mostcommonpresentation in eachagegroupwas abnormalroutineprenatalscanforfetuses(86%),cyanosisfor neonates(74%),heartfailurefor infants(43%),incidentalmur- murforchildren(63%)andarrhythmiaforadolescentsandadults (42%) .Early presentation wasfrequentlyassociatedwithother cardiaclesions,usuallypulmonarystenosisoratresia .Surgery Ebstein'sanomalyhasanextremelyvariablenaturalhistory (1-3) .Itmaypresentatanyage,withavarietyofhemo- dynamicandelectrophysiologicsequelae .Ifthedeformityof thetricuspidvalveissevere,neonatalcongestiveheart failureorevenintrauterinedeathmayoccur(4,5) .Incon- trast,patientswithisolatedminortricuspidvalvedisplace- mentmayremainasymptomaticuntillateadultlife(6) . Inthemostrecent(1974)largestudy(7)ofthenatural history,<7%of505subjectswere<Iyearoldatdiagnosis (7) .Byfailingtoincludepatientswhoarenowdiagnosedby FromtheCardiothoracicUnit .HospitalforSickChildren .GreatOrrnond Street ;'GrownUpCongenitalHeartUnitandDepartmentofPaediatric Cardiology,RoyalBromptonandNationalHeartandLungHospital ;tDe- partmentofCardiology .St .Bartholomew'sHospital ;'+DepartmentofPerina- talCardiology,Guy'sHospital ;and§DepartmentofCardiology .Hammer- smithHospital,London,England .UnitedKingdom .Dr.Celerma)ePspresent addressisDepartmentofCardiology .TheChildren'sHospital,BridgeRoad, Camperdown2050 .Sydney,NewSouthWales,Australia . ManuscriptreceivedMay14 .1993 ;revisedmanuscriptreceivedJuly30, 1993,acceptedAugust5,1993 . Address for corre ace Dr .JohnE .Deanfield,CardiothoracicUnit, HospitalforSickChildren,GreatOtrnondStreet,LondonWCIN3JH, England,UnitedKingdom . ©1994bytheAmericanCollegeofCardiology wasundertakenatsomesein(39%)ofthe220patients . Actuarialsurvivalforalllivebonpatientswas 67% at1yearand 59% at10years.Therewere58deaths,including26fromheart failure,19perioperativeandgsudden .Predictorsofdeath includedechocardiographicgradeofseverityatpresentation (relativerisk2 .7foreachincreaseingrade,95%confidencelimits 1 .6to4.6), fetalpresentation(6 .9,confidencelimits1 .6to16 .5) andrightventricularoutflowtractobstruction(2 .1,confidence limits1 .1to4 .4).Morbiditywasmainlyrelatedtoarrhythmias andlatehemodynamicdeterioration .Of155survivors,129(83%) wereinfunctionalclassIand1(67%)werereceivingno medicaltherapy . Conclusions.In Ebstein'sanomaly,fetalandneonatalpresen- tationisassociatedwithapooroutcomeandcanbepredictedby theechocardiaphicappearanceandpresenceofassociated lesions .Inolderchildrenandadults,incidentalfindingsand arrhythmiasarecommonandthelong-termoutcomeissuperior . (JAmCollCordial1994,23:170-6? PEDIATRIC CARDIOLOGY JACCVol .23 .No .1 January1994 :170-6 echocardiographyinfetalorneonatallife,thisandother earlynaturalhistorystudies(8-10)haveaninevitablebias towardfactorsthatfavorsurvival .Wethereforestudied220 casesofEbstein'sanomaly,presentingfromfetaltoadult lifeanddiagnosedbetween1959and1991,todefinethe patternofpresentation,outcomeandfactorspredictiveof survival . Methods Subjects.Ebstein'sanomalywasdefinedasanydegreeof inferiordisplacementoftheproximalattachmentsofthe tricuspidvalveleafletsfromtheatrioventricular(AV)valve ring(3) .All220patientswithEbstein'sanomalyandcon- cordantcardiacconnectionsidentifiedfromrecordsofcar- diaccatheterization,echocardiographic,electrophysiologic, surgery,in-patientandnecropsudatabetween1958and1991 atfiveLondonhospitals(TheHospitalforSickChildren GreatOrmondStreet,TheRoyalBromptonNationalHeart andLungHospital,Guy'sHospital,TheHammersmith HospitalandSt.Bartholomew'sHospital)wereincluded . Patientswithvariantssuchasthosewithanimperforate 0735.1097194156.00
Transcript of Ebstein's anomaly: Presentation and outcome … 70 Steli sS Anomaly;: Presentation and Outcome From...

1 70
Steli s S Anomaly;: Presentation and Outcome From Fetus to AdultDAVID S. CELERMAJER, MB, BS, MSc, FRACP, CATHERINE BULL, MA . MRCP,
JANICE A. TILL, Mme, BS, BSc,* SEAMUS CULLEN, MB, CtiB, MRCPI,*
VASSILIOS P. VASSILLIKOS, MD,t IAN D. SULLIVAN, BMEDSet, MB, CHB, FRACP,LINDSEY ALLAN, MD, FRCP,* PETROS NIHOYANNOPOULOS, D,§JANE SOMERVILLE, MB, FRCP, FACC,* JOHN E . DEANFIELD, MB, BCHIR, MRCP
London, England, United Kingdom
Objectives . This study was conducted to investigate the presen-tation and outcome of patients with Ebstein's anomaly of thetricuspid valve .
Background. Ebstein's anomaly may present at any age andhas a highly variable clinical course . Previous natural historystudies have been based on clinical and angiographic diagnosisand have included mainly older children and adults . Echocardi-ography, however, has facilitated fetal and neonatal diagnosis sothat the natural history needs to be redefined .
Metho:lt. We reviewed 220 casesofEbstein's anomaly present-ing front fetal to adult life between 1958 and 1991, with I to 34years of follow-up.
Results. The most common presentation in each age group wasabnormal routine prenatal scan for fetuses (86%), cyanosis forneonates (74%), heart failure for infants (43%), incidental mur-mur for children (63%) and arrhythmia for adolescents and adults(42%). Early presentation was frequently associated with othercardiac lesions, usually pulmonary stenosis or atresia. Surgery
Ebstein's anomaly has an extremely variable natural history(1-3) . It may present at any age, with a variety of hemo-dynamic and electrophysiologic sequelae . If the deformity ofthe tricuspid valve is severe, neonatal congestive heartfailure or even intrauterine death may occur (4,5) . In con-trast, patients with isolated minor tricuspid valve displace-ment may remain asymptomatic until late adult life (6) .
In the most recent (1974) large study (7) of the naturalhistory, <7% of 505 subjects were < I year old at diagnosis(7). By failing to include patients who are now diagnosed by
From the Cardiothoracic Unit. Hospital for Sick Children . Great OrrnondStreet ; 'Grown Up Congenital Heart Unit and Department of PaediatricCardiology, Royal Brompton and National Heart and Lung Hospital ; tDe-partment of Cardiology . St . Bartholomew's Hospital ; '+Department of Perina-tal Cardiology, Guy's Hospital ; and §Department of Cardiology . Hammer-smith Hospital, London, England. United Kingdom . Dr. Celerma)eP s presentaddress is Department of Cardiology . The Children's Hospital, Bridge Road,Camperdown 2050. Sydney, New South Wales, Australia .
Manuscript received May 14 . 1993 ; revised manuscript received July 30,1993, accepted August 5, 1993 .
Address for corre ace Dr. John E . Deanfield, Cardiothoracic Unit,Hospital for Sick Children, Great Otrnond Street, London WCIN 3JH,England, United Kingdom .
©1994 by the American College of Cardiology
was undertaken at some s e in (39%) of the 220 patients .Actuarial survival for all livebon patients was 67% at 1 year and59% at 10 years. There were 58 deaths, including 26 from heartfailure, 19 perioperative and g sudden. Predictors of deathincluded echocardiographic grade of severity at presentation(relative risk 2 .7 for each increase in grade, 95 % confidence limits1 .6 to 4.6), fetal presentation (6 .9, confidence limits 1 .6 to 16 .5)and right ventricular outflow tract obstruction (2 .1, confidencelimits 1 .1 to 4 .4). Morbidity was mainly related to arrhythmiasand late hemodynamic deterioration . Of 155 survivors, 129 (83%)were in functional class I and 1 (67%) were receiving nomedical therapy .
Conclusions. In Ebstein's anomaly, fetal and neonatal presen-tation is associated with a poor outcome and can be predicted bythe echocardi aphic appearance and presence of associatedlesions. In older children and adults, incidental findings andarrhythmia s are common and the long-term outcome is superior .
(J Am Coll Cordial 1994,23:170-6?
PEDIATRIC CARDIOLOGY
JACC Vol . 23 . No . 1January 1994 :170-6
echocardiography in fetal or neonatal life, this and otherearly natural history studies (8-10) have an inevitable biastoward factors that favor survival . We therefore studied 220cases of Ebstein's anomaly, presenting from fetal to adultlife and diagnosed between 1959 and 1991, to define thepattern of presentation, outcome and factors predictive ofsurvival .
Methods
Subjects. Ebstein's anomaly was defined as any degree ofinferior displacement of the proximal attachments of thetricuspid valve leaflets from the atrioventricular (AV) valvering (3) . All 220 patients with Ebstein's anomaly and con-cordant cardiac connections identified from records of car-diac catheterization, echocardiographic, electrophysiologic,surgery, in-patient and necropsu data between 1958 and 1991at five London hospitals (The Hospital for Sick ChildrenGreat Ormond Street, The Royal Brompton National Heartand Lung Hospital, Guy's Hospital, The HammersmithHospital and St. Bartholomew's Hospital) were included .Patients with variants such as those with an imperforate
0735.1097194156.00

JACC Vol . 23, No . Ilanuary 1994 :170-6
Table t . Major Presenting Feature off Ebstein's Anomaly in 220 Subjects
tricuspid valve or with AN' and ventriculoarterial discor-dance ("corrected transposition") were excluded .
Case notes, chest X-ray films, 12-lead electrocardiograms(ECGs), echocardiograms, surgical reports and autopsy datawere reviewed to confirm the diagnosis . Echocardiographicgrade of severity was `alculated for all 74 subjects in whoman echocardiogram at presentation was available (5) . Thisinvolved calculating the ratio of the combined area of theright atrium and atrialized right ventricle to that of thefunctional right ventricle and left heart in a four-chamberview at end-diastole . This ratio is used to define fourgrades of increasing severity: ratio <00 = grade 1, ratio 0 .5to 0.99 = grade 2, ratio I to I A9 f= grade 3 and ratio 2 :1 .5 =grade 4 . Left ventricular function is difficult to quantify inEbstein's anomaly because most patients have paradoxicmotion of the ventricular septum . In this series, left ventric-ular dysfunction was therefore defined as severely impairedcontraction of the left ventricular posterior wall on echocar-diography or as global hypokinesia of the left ventricle onanglography.
Investigations and management decisions were deter-mined by the patient's cardiologist in each case . Antibioticprophylaxis against endocarditis was advised for all patients ."Junctional" tachycardia refers to AV or AV node reentrant
tachycandt .Statistical methods. Kaplan-Meier survival curves for the
overall group and different clinical subgroups (antenatal,ages 0 to 2, 2 to 18 and >18 years) were generated (11) .Estimated posteonceptional age was used for survival curvesfor fetal life ; for all other curves, postnatal age wii ., used .When elective termination of pregnancy occurred, the fetuswas withdrawn alive from the analysis at that time . Patientscontributed to each analysis only from the time of referral toour institutions ; this staggered entry is relevant when animportant proportion of patients present late . Multivariateanalysis was performed using only variables that could beassessed at presentation and that were available for >50% ofsubjects (presenting feature, associated defects, age at diag-nosis, pre-excitation, era of diagnosis and chest X-ray filmbut not echocardiographic grade) . Patients were censored atdeath, whether "natural" or postoperative, and survivalbeyond the last contact with our hospitals was not pre-surned. Factors predictive of outcome were explored by
CELERMAJER FT AL .PRESENTATION AND OUTCOME IN FASTEIN'S ANOMALY
Age groups are : neonate = 0 to i month . infant = -2 years, child = tEdO years, adolescent = ~ 18 years and adult>18 years (at time of prescritation) .
171
univariate and multivariate analysis using a Cox proportionalhazards model (12) . Relative risks are indicated with 95%confidence limits . Proportions were compared using thechi-square test . and statistical significance was inferred atp < 0 .05,
ResultsThe age at presentation was 18 weeks' gestation to 68
years (median 36 days) . There were 21 fetuses, 88 neonates(0 to I month of age at presentation) . 23 infants ( :52 years),50 children ( :5;10 years) . 15 adolescents ( :s18 years) and 23adults (> 18 years) . Of the 220 subjects, 13 presented before1960, 26 from 1961 to 1970, 45 from 1971 to 1980 and 122from 1981 to 1990 (14 presented in 199t) . Them were 88 male(409c') and 120 female (55%) subjects ; gender was not deter-mined in 12 fetuses who died or were terminated beforebirth . Follow-up ranged from 12 months to 34 years (median6 years, >5 years in 125 subjects). Of 162 survivors, 133(82%) had been seen within the last 2 years .
Presenting features. The mode of presentation differedfor each age group (Table 1) . In subjects <2 years old,presentation with a hemodynamic problem was significantlymore common than in older patients (72% vs . 29%, p <0.01), whereas presentation with an electrophysiologic prob-lemm was more common in subjects >10 years of age (43% vs .10%,p<0.01) .
Associated cardiac defects (other than a patent foramenovate or atrial septal defect) were present in 76 (35%) andwere more common in the younger age groups (8017c offetuses, 50% of neonates, 48% of infants, 14% of childrenand 8% of adolescents and adults) (Fig . 1, Table 2) .
Investigations. On the chest X-ray film at presentation (in171 of 208 postnatal cases), the cardiothoracic ratio was 40%to 59% in 69 (40%), 60% to 89% in 99 (58%) and ?901`/c in 3(2%). The 12-lead EGG revealed pre-excitation in 41 (20%) .In subjects without pre-excitation, a prolonged PR intervalwas present in 34%, right atrial enlargement in 71% andcomplete or incomplete right bundle branch block in 51% . Atwodivonsisonal echocardiogram at presentation was avail-able in 74 of 136 patients presenting since 1980 and showedseverity of grade I in 13 subjects (18%), grade 2 in 32 (43%),grade 3 in 20 (27%) and grade 4 in 9 (12%) .
Fetusn = 211
Neonate)n = 88)
!Am(n = 23)
Md(n = 50)
Adokescent(a = 15)
Adult(n = 23)
Total v;)(n = 220)
Cyanosis (I 6ti 1 83 03 ;Heart failure 0 9 i0 4 2 6 31 04)Incidental murrnui 0 8 1 33 5 3 52123)Arrhythmia 1 S 1 6 6 10 29(13)Abnormal fetal scan I 1, 0 0 0 0 0 13(8)Other 2 1 1 0 0 3 7(3)
172
CELERMAJER ET AL .PRESENTATION AND OUTCOME IN EBSTEIN'S ANOMALY
Fetus(no-21)
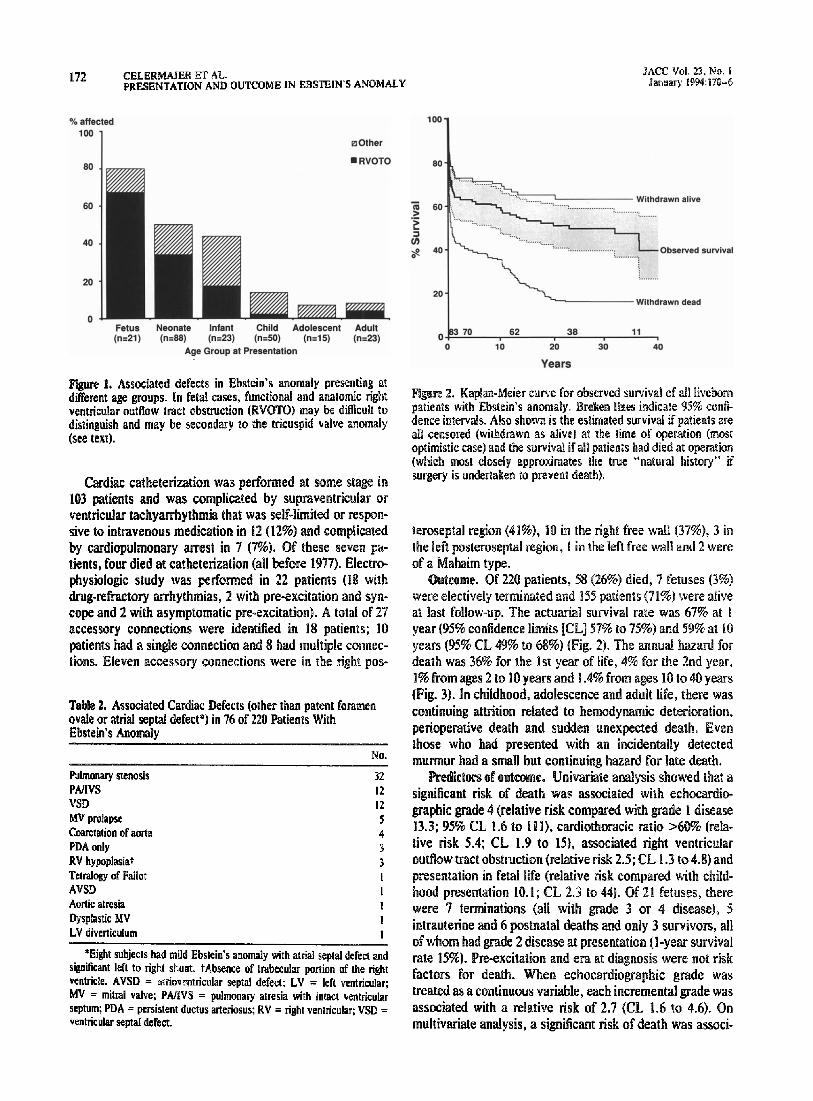
Figure 1 . Associated defects in Ebstein's anomaly presenting atdifferent age groups . In fetal cases, functional and anatomic rightventricular outflow tract obstruction (RVOTO) may be difficult todistinguish and may be secondary to the tricuspid valve anomaly(see text).
Cardiac catheterization was performed at some stage in103 patients and was complicated by supraventricular orventricular tachyarrhythmia that was self-limited or respon-sive to intravenous medication in 12 (12%) and complicatedby cardiopulmonary arrest in 7 (7%) . Of these seven pa-tients, four died at catheterization (all before 1977) . Electro-physiologic study was performed in 22 patients (18 withdrug-refractory arrhythmias, 2 with pre-excitation and syn-cope and 2 with asymptomatic pre-excitation) . A total of 27accessory connections were identified in 18 patients ; 10patients had a single connection and 8 had multiple connec-tions. Eleven accessory connections were in the right pos-
Table 2. Associated Cardiac Defects (other than patent foramenovate or atrial septal defect*) in 76 of 220 Patients WithEbstein s Anomaly
Neonate
Infant(u=eli)
(ne23)Age Group at Presentation
Child Adolescent Adult(n=5O)
(n®1a)
in_23)
*Eight subjects had mild Ebslein s anomaly with atrial seplal defect andsignificant left to right shunt . tAbsence of trabecular portion of the rightventricle. AVSU = atriovrntricular septal defect ; LV = left ventricular ;MV = mitral valve ; PAIIVS = pulmonary atresia with intact ventricularseptum; PDA = persistent ductus arteriosus ; RV = right ventricular ; VSD =ventricular septal defect.
JACC Vol . 23, No . IJanuary 1994 :170-6
Figure 2. Kaplan-Meier curve far observed survival of all livebornpatients with Ebstein's anomaly . Broken tines indicate 95% confi-dence intervals . Also shown is the estimated survival if patients areall censored (withdrawn as alive) at the time of operation (mostoptimistic case) and the survival if all patients had died at operation(which most closely approximates the true "natural history" ifsurgery is undertaken to prevent death) .
teroseptal region (41%), 10 in the right free wall (37%), 3 inthe left posteroseptal region, I in the left free wall and 2 wereof a Mahaim type .
Outcome . Of 220 patients, 58 (26%) died, 7 fetuses (3%)were electively terminated and 155 patients (71%) were aliveat last follow-up. The actuarial survival rate was 67% at Iyear (95% confidence limits [CL) 57% to 75%) and 59% at 10years (95% CL 49% to 68%) (Fig. 2) . The annual hazard fordeath was 36% for the Ist year of life, 4% for the 2nd year,1 % from ages 2 to 10 years and 1 .4% from ages 10 to 40 years(Fig. 3). In childhood, adolescence and adult life, there wascontinuing attrition related to hemodynamic deterioration,perioperative death and sudden unexpected death. Eventhose who had presented with an incidentally detectedmurmur had a small but continuing hazard for late death .
Predictors of outcome. Univariate analysis showed that asignificant risk of death was associated with echocardio-graphic grade 4 (relative risk compared with grade I disease13.3 ; 95% CL 1 .6 to 11l), cardiothoracic ratio >60% (rela-tive risk 5.4; CL 1 .9 to 15), associated right ventricularoutflow tract obstruction (relative risk 2 .5; CL 1 .3 to 4 .8) andpresentation in fetal life (relative risk compared with child-hood presentation 10.1 ; CL 2.3 to 44) . Of 21 fetuses, therewere 7 terminations (all with grade 3 or 4 disease), 5intrauterine and 6 postnatal deaths and only 3 survivors, allof whom had grade 2 disease at presentation (l-year survivalrate 15%). Pre-excitation and era at diagnosis were not riskfactors for death. When echocardiographic grade wastreated as a continuous variable, each incremental grade wasassociated with a relative risk of 2 .7 (CL 1 .6 to 4.6). Onmultivariate analysis, a significant risk of death was associ-
No .
Pulmonary stenosis 32PMVS 12VSD 12MV prolapse 5Coarctation of aorta 4PDA only 3RV hypoplasiat 3Tetralogy of FallotAVSDAortic atresiaDysplastic MVLV diverticulum
tIII1

ACC Vol, 23, No . 1January 1994 :170-6
Mg-dre 3 . Kaplan-Meier survival curves forthe fetal cases and the ages of 0 to 2, 2 to 18and > 18 years (see Methods) . The x axis forthe Rol eases refers to estimated poqwn-ceptional age ; for the other three survivalcurves, the x axis refers to postnatal age .
2 - 18 pam
ated with fetal relative to childhood presentation (relativerisk 6 .9, CL 1 .6 to 16.5) and presence of right ventricularoutflow tract obstruction (relative risk 2 .1 CL 1 .1 to 4 .4) .
Surgery. The findings from 86 patients who underwentsurgical treatment are shown in Figure 4 . The indications foroperation wene persistent cyanosis or heart failure, or both,in the neonate and hemodynamic : problems leading to func-tional class III or IV symptoms or arrhythmias refractory todrug treatment, or both, in older subjects .
Figure 4. Surgery for Ebstein's anomaly, Palliation in-cludes aortopulmonary (n = 12) and cavopulmonary (n= 2) shunts and pulmonary valvotomy (n = 12) ."Closed" operation is any other procedure not involv-ing cardiopulmonary bypass ; "open" operation doesinvolve bypass. Numbers in parentheses denote peri-operative deaths in each group . ASD = atrial septaldefect ; EP = electrophysiologic ; OP = operation ; TV =tricuspid valve . *Valve repair in 12 patients and valvereplacement in 20 . Three of these patients had electronphysiologic surgery with their tricuspid valve operation,one of whom died perioperatively. "Includes two pa-tients with ventricular septal defect closure, one withrepair of tetralogy of Fallot and one with a Fontan-typerepair .
CELERMMER ET AL .PRESENTATION AND OUTCOME IN EBSTEIN*S ANOMALY
Cap
Yuan
In* Years
Yom
173
Years
In the 32 patients who had tricuspid valve surgery (at age8 days to 46 years), the risk was more related to ge atpresentation than to age at operation . The perioperativemortality rate was 50% (8 of 16 patients) for those whosecondition was diagnosed in the 1st year of life (13 of whomwere operated on after infancy) and 0% for the 16 patientswhose condition was diagnosed after age 1 year (p < O .OW 11) .Seventeen patients had a second operation and two requireda third procedure (tricuspid valve replacement) .

174
CELERMAJER ET AL .PRESENTATION AND OUTCOME IN EBSTEIN'S ANOMALY
Morbidity . Twenty-eight neonates with initial resolutionof neonatal cyanosis later developed heart failure or cyano-sis, or both (2 to 18 years after initial presentation) ; I I ofthese had evidence of left ventricular dysfunction . Of 220patients, 74 (34%) have had arrhythmias at some stage and13 others have pre-excitation but no symptoms to date . Themost common arrhythmias were junctional tachyrardia (43patients), atriall flutter or fibrillation (28 patients) and ven-tricular tachycardia (15 patients); several patients had morethan one type of arrhythmia documented . Supraventriculararrhythmias tended to be recurrent and drug refractory, with42 (57%) of 74 patients requiring two or more antiarrhythrnicmedications to achieve symptomatic control . Bradyarrhythamia was less common ; AV block occurred in five patients (inrelation to surgery in two and to cardiac catheterization inthree) .
There were two cases of paradoxic embolism, both caus-ing hemiparesis in young adults who had been in sinusrhythm ; one child had a cerebral abscess . The only case ofdocumented endocarditis affected the tricuspid valve of a62-year old man who died of progressive tricuspid regurgi-tation.
Mortality . Death was due to congestive heart failure in 26(45%) of 58 patients, was perioperative in 19 (33%), suddenand unexpected in 8 (14%), related to cardiac catheterizatunin 4 and of noncardiac origin in one child . The deaths fromheart failure occurred in neonates managed conservatively(I I patients, all before 1980), children who were initially wellbut developed late hemodynamic problems (13 patients,associated with left ventricular dysfunction in 8 and withprogressive tricuspid valve dysfunction, right heart dilationor atrial fibrillation in 5) and 2 older adults (I with severedisease considered inoperable and the other with tricuspidvalve endocarditis) . Of the eight patients who died suddenly,four had previously documented arrhythmias (atrial flutter orfibrillation late after tricuspid valve surgery in three, ventric-ular tachycardia in one), one had had recent symptomaticdeterioration and three had no antecedent event that couldbe identified. No patient who died suddenly had pre-excitation .
Survivors . Of the 155 survivors, 129 (83%) were in func-tional class 1, 23 (159%) in class II, 3 (2%) in class III and nonein class IV when last assessed . Most survivors were receiv-ing no medical therapy (104 (67%) of 155 patients ; 20 werereceiving digoxin only, 9 were receiving digoxin and diureticdrugs and 22 were receiving another antiarrhythmic agent) .
DiscussionThis study has shown that fetuses, neonates and infants
with Ebstein's anomaly usually present with hemodynamicsequelae of severe tricuspid valve displacement and rightventricular abnormalities and have a poor prognosis . Thereis an early death hazard due to heart failure and intrauterinecardiomegaly causing pulmonary hypoplasia (13) and a con-tinuing later hazard due to hemodynamic deterioration in
JACC Vol. 23, No . IJanuary 1494:170-6
childhood or adolescence, perioperative death or suddendeath. In contrast, childhood Ebstein's anomaly usuallypresents with an incidental murmur, and the outlook ;s good .The main clinical problem for adolescents and adults withEbstein's anomaly is arrhythmia . This may be due to thenatural history of pre-excitation, progressive atrial dilationor the association of both .
Associated cardiac defects were common in patientspresenting early (Fig . 1). In fetal life, functional and ana-tomic right ventricular outflow obstruction are di cult todistinguish (14), and severe tricuspid regurgitation maysimulate pulmonary atresia (15) . Structural pulmonary valveabnormalities are most likely secondary to the tricuspidvalve anomaly (I1), resulting from low anterograde flowduring outflow tract development (161 .
The true "natural history" of Ebstein's anomaly cannotbe determined because many patients underwent surgicaltreatment . Survival data have therefore been presented inthree ways (Fig . 2) : the observed survival, the most optimis-tic case (patients withdrawn as alive at time of operation)and the worst case (patients withdrawn as dead at time ofoperation) . The true natural history lies between the ob-served and worst case curves, but probably closer to thelatter because patients in our series were usually operated onwhen they were severely symptomatic .
Limitations of study . This study included all 220 patientsreferred to five London teaching hospitals over a 30-yearperiod, even those with minor tricuspid valve displacementand those with serious associated defects. This confirms therelative rarity of this condition . The majority of children withhemodynamic problems, unexplained murmurs and arrhyth-mias from Southeast England and most adults with cyanosisor arrhythmias would have been referred to one of thesehospitals over the duration of the study. The proportion ofpatients with undiagnosed Ebstein's anomaly has probablychanged over the study period . Some patients will have diedwithout a diagnosis and others will be alive with as yetunrecognized Ebstein's anomaly; the net effect of suchpatients on the survival curves presented in this report isuncertain.
The median age at presentation was <I year, underscor-ing the impact of echocardiography on the diagnosis ofcongenital heart disease in fetuses and infants and thechange in pattern of referrals for Ebstein's anomaly in thelast decade . These data, however, reflect only the medicalpractice at our institutions over a particular time frame,which has evolved during the period of the study . Importantpotential sources of bias also exist as a result of the inevita-ble individualization of the timing and type of investigationsand treatment .
Morbidity and mortality . Endocarditis was rare in thisseries, with only one case documented in >1,000 patient-years of follow-up. Although the "natural" risk of valveinfection cannot be determined, there is a low risk if antibi-otic prophylaxis is recommended . Paradoxic embolism wasalso rare, and we do not routinely undertake anticoagulant

JACC Vol . 23, No . 7January 199d :179 .-5
therapy in patients it sinus rhythm . Arrhythmias werecommon particularly in the older age groups and wereusually related to accessory AV connections and atrialflutter or fibrillation . These arrhvthmias tended to be recur-rent and resistant to drug treatment (M . Catheter ablationfor accessory connections has not been performed often inEbstein's anomaly and is difficult because most connectionsare right-sided, the right atrium is large and the anatomy ofthe right AV rip-, is distorted . Arrhythmia surgery is feasible,and both short- and long-term results are good for appropri-ately selected cases (18). Some cases of late sudden deathmay be related to arrhythmias ; however, it is not knownwhether routine noninvasive or invasive electrophysiologictesting or treatment of any detected arrhythrias will mini-mize the risk of this complication .
Late hemodynamic deterioration may be due to increasedright to left shunting and right or left heart failure, or both .The incidence of late left ventricular dysfunction cannot beestimated from this study because serial measurements werenot routinely perforated . Furthermore, left veu1ricuial dys-function is especially difficult to assess in Ebstein's anomalybecause of paradoxic septal motion, which inihaenees theestimation of ejection fraction and fractional shortening . Thetrue incidence of left ventricular dysfunction is probablyunderestimated because only patients with very poor poste-rior wall contraction were included .
The association between Ebstein's anomaly and leftventricular abnormalities has been previously noted `19,20),and Saxena et al . (21) have recently documented unsus-pected abnormalities in left ventricular function and limita-tion in exercise capacity in mildly symptomatic adults .Exercise testing may therefore be useful in assessing cardiacperformance, given the limitations of echocardiographicindexes. The cause of left ventricular dysfunction is unclear,but may be due to chronic cyanosis, right heart dilation andseptal abnormalities (22) and increased left ventricular fibro-sis (16) .
Management. Echocardiography is the most importantdiagnostic test in Ebstein's anomaly, permitting accurateassessment of the anatomy and distal attachments of thetricuspid valve, the size and contractility of the functionalright ventricle and the overall grade of disease severity .Cardiac catheterization is rarely required, other than forelectrophysiologic study or for investigation of associatedcardiac defects .
Neonates . Newborns with isolated Ebstein's anomalyand cyanosis usually show spontaneous improvement aspulmonary vascular resistance decreases (13) . Those inwhom persistent cyanosis is due to associated right ventric-ular outflow obstruction do well after surgical palliation iftheir Ebstein's anomaly is not severe (echocardiographicgrade I or 2). The results of tricuspid valve surgery werepoor, however, for neonates and infants with symptomaticheart failure and severe Ebstein's anomaly, and this proba-bly reflects more severe disease requiring intervention inearly life. Possible strategies for these children include the
CELERMAJER El A
175PPESENTATLON AND OUTCOME IN EBSTEIN'S ANOMALY
creation of functional tricuspid atresia (by closing the tricus-pid valve and excising the atrial septum) with insertion of asystemic to pulmonary artery shunt (24), with a view to laterFontan-type surgery, or heart transplantation (25) .
Older children and adults, In this group the most com-men indication for tricuspid valve surgery was worseningcongestive heart failure . Operations early in this series wereusually valve replacement, but valve repair has been under-taken where possible since the reports of excellent periop-erative results in highly selected patients by fair et al . (26),who described creation of a monocusp valve and transverseplication of the atrialized right ventricle, and by Carpentieret al . (27), who described longitudinal plication .
In patients whose heart failure is due to increasingtricuspid regurgitation and right atrial enlargement, tricuspidvalve surgery should improve symptomatic status . In manyof our patients with late hemodynamic deterioration, how-ever, there was evidence of poor left ventricular function ; inthese patients, tricuspid valve surgery may not necessarilyimprove functional status or long-term outco e . Prospectivestudy is required to determine whether serial measurementof echocardiographic grade of disease severity, left ventric-ular function or exercise tolerance might predict symptom-atic deterioration and the need for surgery .
Some investigators (29) have suggested on the basis ofretrospective data that tricuspid valve surgery is indicatedfor asymptomatic patients with a cardiothoracic ratio X65%because this may be a better predictor than functional statusof late sudden death . In our series, sudden death was rare inpatients who did not undergo operation, even in those withcardiomegaly . Furthermore, sudden death may occur inpatients with mild disease and a normal heart size on thechest X-ray film (29) . Because surgery carries a significantrisk, even in older children and adults, and there is noevidence to date that it reduces the hazard for sudden death,we do not currently perform tricuspid valve surgery inasymptomatic patients .
Clinical implications . The management of Ebstein'sanomaly therefore depends on the age at presentation,anatomic severity of the lesion, presence of associateddefects and clinical features . Fetal Ebstein's anomaly has anappalling outlook, and prenatal counseling should take thisinto account . Grade I or 2 disease in neonates and infantshas a good outcome and palliation should be undertaken forassociated lesions, but grade 3 or 4 disease in young childrenhas a poor prognosis. Older children and adults can bemanaged medically until symptoms appear, when good re-sults may be obtained by valve surgery, particularly valverepair . In all age groups, however, there is an increasing riskof arrhythmias (17) and a persistent risk of late hemody-namic deterioration and sudden death .
We thank Mary Jane Potter for expert secretarial assistance .
176
CELERMAJER ET AL.PRESENTATION AND OUTCOME IN EBSTEIN'S ANOMALY
References1 . Lev M, Liberthson RR, Joseph RH, et al . The pathologic anatomy of
Ebstein's anomaly. Arch Pathol 1970,90334-43 .2 . Zuherbuhler JR . Allwork SP, Anderson MP. Anderson RA. The spectrum
of Ebstein's anomaly of the tricuspid valve, I Thorne Cardiovasc Stag1979;77.- 202-11 .
3 . Anderson ER, Zuberbuhler JR, Anderson RH, Becker AE, Lie JT.Morphologic spectrum of Ebstem's anomaly of the heart: a review . MayoChn Proc 1979:54:174-80.
4 . Roberson DA, Silvennan NH . Ebstein's anomaly : echocardiographic andclinical features in the fetus and neonate . J Am Coll Cardiol 1989 ;14 :13W-7.
5 . Celerm4er DS, Cullen S, Sullivan ID, Spiegelhaller DJ, Wyse RKH,Deanfield JE . Outcome in neonates with Ebstein's anomaly. I Am CollCardiol 1992 ;19:1041-6 .
6. AdamsJCL, Hudson R . A case of Ebsicin's anomaly surviving to age 79 .Br Heart 11956,18:129-3 1 .
7 . Watson H. Natural history of Ebstein's anomaly of tricuspid valve inchildhood and adolescence : an international cooperative study of 505cases, Br Heart J 1974,36.417-27 .
8 . Kumar AE, Fyler DC, Miettinen OS. Nadas AS. Ebstein's anomaly :clinical profile and natural history . Am I Cardiol 1971 ;28 :84-95.
9 . Giuliani ER, Foster V . Brandenburg RO, Mair DD . Ebstein's anomaly :the clinical features and natural history of Ebstein's anomaly of thei,~cuspjd valve . Mayo Clin Proc 1979;54:163-73 .
10 . Leung MP, Baker EJ, Anderson RH, Zuberbuhlei JR. Cineangiographicspectrum of Ebstein's anomaly : its relevance to clinical presentation andoutcome. I Am Coll Cardiol 190 :11 :154-61 .
11 . Kaplan EL, Meier P. Nonparametric estimations from incomplete obser .vations. J Am Stat Assoc 1958 ;53 :457-81 .
12 . Cox DR . Oakes D. Analysis of Survival Data . London : Chapman andHall . 1984:91-110.
13 . Lang D. Oberhoffer R, Cook A, et al . Pathologic spectrum of malforma-tions of the tricuspid valve in prenatal and neonatal life . J Am Coll Cardiol1991 ;17:1161-7.
14 . Sharland GK, Chita SK . Allan LD . Tricuspid valve dysplasia or displace-ment in intra-uterine life . J Am Coll Cardiol 1991,17:944-9,
IS . Yeager SB, Parness 1R . Sanders SP. Severe tricuspid regurgitationsimulating pulmonary alresiaa in the fetus . Am Heart 119880 15:906-8,
16 . Celermajer DS, Dodd SM. Greenwald SE . Wyse RKH . Deanfield JE .Morbid anatomy in neonates with Ebstein's anomaly of the tricuspid
JACC Vol . 23, No. IJanuary 1994 :170-6
valve : pathophysiologic and clinical implications- J Am Coll Cardiol1992 ;19:1049-53 .
17 . Till J, Celemajer DS, Dearfield JE . The natural history of arrhythmia inEbstein's anomaly (abstract) . J Am Coll Cardiol 1992,19 Suppl A: 273A .
18 . Pressley IC, Wharton M, Lang ASL . Lowe J E, Gallagher JJ, PrystowskyEN. Effect of Ebstein's anomaly on short- and long-teen outcome ofsurgically treated patients with Wolff-Parkinson-White syndrome . Circu-lation 1992 :86 :1147-55.
19 . Monibi AA . Neches WH . Lennox CC, Park S. Mathews RP, ZuberbublerJR. Left ventricular anomalies associated with Ebstein's malformation ofthe tricuspid valve . Circulation 1978:57 :303-6.
20 . Sharma S, Rajani M, Mukhopadhyay S, Aggarwal S, Shrirastava S .Tandon R. Angiographic abnormalities of the morphologically left ventri-cle in the presence of Ebstein's malformation . Int I Cardiol 1989 ;22 :109-13 .
21 . Saxena A, Fong LV, Tristam NJ, Ackery DWI, Keeton BR . Late nonin-vasive evaluation of cardiac performance in mildly symptomatic olderpatients with Ebstein's anomaly of the tricuspid valve : role of radionu-clide imaging. J Am Coll Cardiol 1991 .17 :182-6 .
22. Benson LN. Child IS, Schwayer M, Perloff KJ, Schelberl HR . Leftventricular geometry and function in adults with Ebstein's anomaly of thetricuspid valve . Circulation 1987,75 :353-9.
23. Kirklin JW, Barralt-Boyes BG . Cardiac Surgery, New York : Wiley,1986:889-910.
24. Starnes VA, Pitlick PT . Bernstein D, Griffin ML, Choy M . Shomway NE .Ebstein's anomaly appearing in the neonate : a new surgical approach .J Thorac Cardiovasc Surg 1991 ;101 :1082-7 .
25. Mayer JE Jr, Perry S, O'Brien P, el al . Orihotopic heart transplantationfor complex congenital heart disease . I Thorac Cardiovasc Surg 19%,99:484-92 .
26. Mair DD . Seward JB, Driscoll DH . Danielson GK . Surgical repair ofEbstein's anomaly: selection of patients and early and late operativeresults . Circulation 1985 :72 Suppl 1111-70-6 .
27. Carpentier A, Chauvaud 5, Mace L . et al . A new reconstructive operationfor Ebstein's anomaly of the tricuspid valve . I Thorac Cardiovasc Surg1988:96 :91-101 .
28. Gentles TL, Calder L. Clarkson PM . Neutze JM . Predictors of long-termsurvival with Ebstein*s anomaly of the tricuspid valve . Am I Cardiol1992:69 :377-81 .
29. Rossi L,Thiene G . Mild Ebstein's anomaly associated with supraventric-ular tachycardia and sudden death : clinicomorphologic features in 3patients . Am I Cardiol 1984 :53 :332-4 .