Ebola Virus Disease - ust.eduust.edu/conf/yicid/pdf/Workshops/Workshop Hall A/Ebola virus EVD...
45
Yemeni International Congress of Infectious Diseases 16-18 December 2014 University of Science & Technology Hospital Faculty of Medicine & Health Sciences Ebola Virus Disease(EVD)
Transcript of Ebola Virus Disease - ust.eduust.edu/conf/yicid/pdf/Workshops/Workshop Hall A/Ebola virus EVD...

Yemeni International Congress of Infectious Diseases
16-18 December 2014 University of Science & Technology Hospital
Faculty of Medicine & Health Sciences
Ebola Virus Disease(EVD)

Presented by:
Dr Ahmed Ali Qaid Pandemic and Epidemic Disease Officer,WHO
Professor of Community Medicine
Dr Abdullah Abdu Almikhlafy
Assistant Professor of Community Medicine
UST FOM

Ebola The Deadly African
Virus

Ebola Virus Introduction
First appeared in Africa 1976
“African Hemorrhagic Fever”
acute,mostly fatal disease
causes blood vessel “bursting”
systemic (all organs/tissues)
humans and nonhuman primates
Excluding „2000 outbreak
1,500 cases
over 1,000 deaths

Ebola Taxonomy
Scientific Classification
Order: Mononegavirales
Family: Filoviridae
Genus: Ebola like viruses
Species: Ebola
Subtypes
Ebola-Zaire, Ebola-Sudan,Ebola-Ivory Coast
disease in humans
Ebola-Reston disease in nonhuman primates

Learning Objectives
To Recognize the Epidemiological Pattern of Ebola Virus Disease .
To Understand Prevention and Control Methods for Ebola Virus Disease.

Filoviridae or “Filoviruses”
Most mysterious virus group
Pathogenesis poorly understood
Ebola
natural history/reservoirs unknown
exist throughout the world
endemic to Africa Image courtesy of the Centers for Disease Control

Ebola Pathogenesis
Enters Bloodstream
skin, membranes,open wounds
Cell Level
docks with cell membrane
Viral RNA
released into cytoplasm
production new viral proteins/ genetic material
New viral genomes
rapidly coated in protein
create cores
Copyright: Russell Kightley Media, Australia

Ebola Virus Zoonotic virus – bats the most likely reservoir, although
species unknown
Spillover event from infected wild animals (e.g., fruit bats, monkey, duiker) to humans, followed by human-human
transmission
9

Ebola Epidemiology
Reservoirs in Nature largely unknown
possibly infected animals (primates?)
Transmission
direct contact blood/secretions of infected person
possible airborne (Reston primate facility)
Onset of illness abrupt
incubation period: 2 to 21 days
infections are acute and mostly deadly


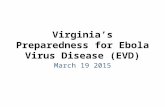
EVD in West Africa up to Epi-Week 45
Source: (i) World Health Organization, (ii) WHO Ebola Response Team: the first 9 months of epidemic and forward projection. N Eng J Med, 2014 Sep 22 {Epub ahead of print]

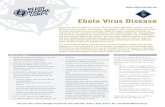
History of EVD Outbreaks (1)
● In 1976, Ebola Virus Disease (EVD) (formerly known
as Ebola Haemorrhagic Fever) was first appeared in 2
simultaneous outbreaks in Sudan and in Democratic
Republic of Congo (DRC).
● Twenty three outbreaks (2388 human cases including
1590 deaths, CFR 67%) have been reported since the
first discovery of EVD in 1976 and up to 2013.


Uganda, 2000 (425)
Côte d’Ivoire 1994 (1)
Gabon, 1994 (44)
1996 (37), 1996 (61) 2001-02 (65)
Sudan, 1976 (284), 1979 (34)
DRC (ex-Zaire), 1976 (318) 1977 (1) 1995 (316)
South Africa 1996 (1)
Congo, 2001-02 (57) 2002 (13) 2003 (143) (35)
Ebola haemorrhagic fevers in Africa
Epidemics
Countries with serological evidence
(n) = number of cases
Countries at risk
Countries w/o serological evidence

EVD: Current Situation in EMR
● Rumours of EVD have been reported from Egypt,
Lebanon, Morocco, KSA, Sudan and UAE.
● Sudan remains the only country in the region that
has experienced previous outbreaks from EVD
● The risk of the spread of EVD to the region region is
possible owing to international travel

Possible EVD importation Route (1)
● International travel by air
─ Traders and businessmen from affected countries in West Africa
─ Transit passengers
─ Returnee UN Peacekeepers from Western Africa
─ Religious pilgrims.

Potential of spreading internationally by air travel:
These were the final destinations of airline travelers in the month of August-September 2014 departing from the affected countries by WHO Region…
Source: Assessing the international spreading risk associated with 2014 Western African Ebola Outbreak. PLOS Current Outbreaks, 2014 Sep2 Edition 1

Possible EVD importation Route (2)
● International travel by land and/or sea
─ Illegal economic migrants to Europe
─ Pilgrims from West Africa
─ Job seekers and seasonal workers

Transmission mode

How contagious is EVD? ?


●H2H Transmission : familial and nosocomial
•Most human infections due to direct or indirect contact with damaged skin, mucous membranes, body fluids of infected patients (blood, saliva, vomitus, urine, stool, semen)

●Amplification : 584 HCWs infected in the
current outbreak of which 329 have died
•Hospital: health care workers, in-patients,
care givers, unsafe injections
•Community: contacts when caring for ill,
funeral

Symptoms and Diagnostic Tests
Early symptoms
muscle aches, fever, vomiting
red eyes, skin rash, diarrhea, stomach pain
Acute symptoms
bleeding/hemorrhaging from skin, orifices, internal organs
Early Diagnosis
very difficult
signs & symptoms very similar to other infections
Laboratory Test PCR detection
ELISA (enzyme-linked immuno-absorbant) assay

Treatment
No Standard Treatment available
Patients receive supportive therapy
treating complicating infections
balancing patient‟s fluids and electrolytes
maintaining oxygen status and blood pressure

Clinical Features
Incubation period 2 to 21 days (3-‐12).
Sudden onset of fever, weakness, muscle pain,
headache and sore throat, conjunctivitis, hiccups,
dysphagia.
followed by vomiting, diarrhea, rash.
internal & external bleeding
often absent or minimal

Late features
Confusion and irritability
Seizures
easy bleeding;
– Rash e.g. ecchymosis, petechiae, purpura
– bleeding from the gums,
– conjunctival hemorrhage
– oozing from puncture sites

Late features
--epistaxis – Hematemesis – hemoptysis – Melaena -unexplained vaginal bleeding in women – haematuria Fever may be absent in late stages Shock (compounded by dehydration)

Classification Criteria
Suspected
Any person, alive or dead, who has (or had) sudden onset of high fever and had contact with a suspected, probable or confirmed EVD case, or a dead or sick animal OR any person with sudden onset of high fever and at least three of the following symptoms: headache, vomiting, anorexia/ loss of appetite, diarrhoea, lethargy, stomach pain, aching muscles or joints, difficulty swallowing, breathing difficulties, or hiccup; or any person with unexplained bleeding OR any sudden, unexplained death.
Probable
Any suspected case evaluated by a clinician OR any person who died from ‘suspected’ EVD and had an epidemiological link to a confirmed case but was not tested and did not have laboratory confirmation of the disease.
Confirmed
A probable or suspected case is classified as confirmed when a sample from that person tests positive for EVD in the laboratory.
Table 3: Ebola case-classification criteria

WHO aims to prevent Ebola outbreaks by
maintaining surveillance for Ebola virus disease and supporting at-risk countries to developed preparedness plans. The document provides
overall guidance for control of Ebola and Marburg virus
outbreaks: Ebola and Marburg virus disease epidemics: preparedness, alert, control, and
evaluation
WHO response

When an outbreak is detected WHO responds by supporting surveillance, community engagement, case management, laboratory services, contact tracing, infection control, logistical support and training and assistance with safe burial practices. WHO has developed detailed advice on Ebola infection prevention and control: Infection prevention and control guidance for care of patients with suspected or confirmed Filovirus haemorrhagic fever in health-care settings, with focus on Ebola
WHO response
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html
http://www.who.int/entity/csr/resources/publications/ebola/filovirus_infection_control/en/index.html

WHO Ebola Response- Overview
The first case of the current Ebola Virus Disease (EVD) was reported in Guinea in March 2014. Since then the outbreak has spread to Sierra Leone, Liberia, Nigeria and Senegal.
A separate Ebola outbreak in the Democratic Republic of Congo was also reported in August 2014.

8 countries affected – High transmission: Guinea, Liberia, Sierra Leone – Recently introduced / low transmission: Mali, Spain, US – Ebola free: Nigeria, Senegal

Prevention
No vaccines!
Patients are isolated
Medical Staff Training western sanitation practices
intake
care during stay
after patient dies
Infection-control Measures complete equipment and area sterilization

Prevention
After Death
Virus contagious in fluids for days
Burial use extreme caution
handling and transport
cultural practices/ religious belief
incinerate all waste !!!!

INFECTION PREVENTION
Consider every person (client or staff)
infectious
Wash hands
Wear gloves
Use physical barriers:
(protective goggles
facemasks and aprons)

To Prevent Ebola The suspected reservoirs for Ebola are fruit
bats.
Transmission to humans is thought to originate from infected bats or primates that have become infected by bats.
Undercooked infected bat and primate (bush) meat transmits the virus to humans.

To Prevent Ebola
Human to human transmission is only achieved by physical contact with a person who is acutely and gravely ill from the Ebola virus or their body fluids
Transmission among humans is almost exclusively among caregiver family members or health care workers tending to the very ill.
The virus is easily killed by contact with soap, bleach, sunlight, or drying. A washing machine will kill the virus in clothing saturated with infected body fluids.

To Prevent Ebola
A person can incubate the virus without symptoms for 2‐21 days, the average being five to eight days before becoming ill. THEY ARE NOT CONTAGIOUS until they are acutely ill.
Only when ill, does the viral load express itself first in the blood and then in other bodily fluids (to include vomit, feces, urine, breast milk, semen and sweat).

If you are walking around you are not infecious to others.. As always practice good hand washing techniques. You will not contract Ebola if you do not touch a dying person with it.

Ebola virus disease (EVD), formerly known as Ebola haemorrhagic fever, is a severe, often fatal illness in humans.
The virus is transmitted to people from wild animals and spreads in the human population through human-to-human transmission.
The average EVD case fatality rate is around 50%. Case fatality rates have varied from 25% to 90% in past outbreaks.
Take-home messages

Community engagement is key to successfully controlling outbreaks. Good outbreak control relies on applying a package of interventions, namely case management, surveillance and contact tracing, a good laboratory service, safe burials and social mobilisation.
Take-home messages

Early supportive care with rehydration, symptomatic treatment improves survival. There is as yet no licensed treatment proven to neutralise the virus but a range of blood, immunological and drug therapies are under development.
There are currently no licensed Ebola vaccines but 2 potential candidates are undergoing evaluation.
Take-home messages

Thank You For your Attention And Listening