EBOLA Viral Disease Ebola latest final combined.pdf · Ebola Viral Disease (EVD) is one of numerous...
83
Ethiopian Public Health Institute (EPHI) September 2014 Addis Ababa, ETHIOPIA EBOLA Viral Disease Interim Guideline
Transcript of EBOLA Viral Disease Ebola latest final combined.pdf · Ebola Viral Disease (EVD) is one of numerous...

Ethiopian Public Health Institute
(EPHI)
September 2014
Addis Ababa, ETHIOPIA
EBOLA Viral Disease Interim Guideline

ii | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
TABLE OF CONTENTS
TABLE OF CONTENTS ............................................................................................................................... II
I. INTRODUCTION TO EBOLA VIRAL DISEASES ............................................................................. 1
1. Background ....................................................................................................................................................... 1
2. Mode of Transmission ....................................................................................................................................... 1
3. Incubation Period .............................................................................................................................................. 2
4. Sensitivity of the Virus ....................................................................................................................................... 2
5. Clinical Features of Ebola Virus Infection .................................................................................................... 2
II. EBOLA VIRUS DISEASE SURVEILLANCE AND LABORATORY DIAGNOSIS....................... 4
1. Purpose of Surveillance ..................................................................................................................................... 4
2. Case Definition of Ebola Virus Disease ............................................................................................................... 4
2.1. Case Definition Ebola Cases before Outbreak ........................................................................................................ 4
2.2. Case definitions During an Ebola Outbreak ............................................................................................................ 5
3. EVD Surveillance and Measures to Take ............................................................................................................. 5
3.1 Screening of Passengers at Ports of Entries ............................................................................................................. 5
3.2. Exposure Levels and Measures to Take if Exposures Encountered ......................................................................... 6
3.3. Contact Tracing and Contact Follow Up ................................................................................................................. 7
3.3 Contact Tracing ....................................................................................................................................................... 8
3.4 Rumors Verification ................................................................................................................................................ 9
3.5 Transporting a Suspected Case ............................................................................................................................. 10
4. Outbreak Investigation, Sample Collection and Shipment ................................................................................ 12
4.1 Outbreak Investigation ......................................................................................................................................... 12
4.2 Confirmation of Diagnosis by Laboratory: Collection of Specimen and Shipment ................................................. 13
III. CASE MANAGEMENT OF PATIENTS ........................................................................................ 14
1. Principles for Clinical Case Management .......................................................................................................... 14
2. Set Up and Organization of the Ebola Treatment Center .................................................................................. 14
2.1 Location ................................................................................................................................................................ 14
2.2 Buildings / Structures ............................................................................................................................................ 14
2.3 Risk Zones ............................................................................................................................................................. 15
2.4 Activities and Facilities in the Different Risk Zones ................................................................................................ 16
2.5 Fencing ................................................................................................................................................................. 17
2.6 Layout of Ebola Treatment Unit ............................................................................................................................ 17

iii | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
2.7 Patient screening area .......................................................................................................................................... 19
3. Patient Care at Ebola Treatment Unit ............................................................................................................... 19
3.1 Medical Staff ......................................................................................................................................................... 19
3.2 Admissions ............................................................................................................................................................ 19
3.3 Laboratory Tests ................................................................................................................................................... 20
3.4 Medical Care ......................................................................................................................................................... 20
3.5 Invasive Procedures .............................................................................................................................................. 21
3.6 Hydration .............................................................................................................................................................. 21
3.7 Management of Shock in EVD Patients ................................................................................................................. 21
3.8 Symptomatic Care ................................................................................................................................................. 25
3.9 Presumptive Treatment ................................................................................................................................. 27
3.10 Nutritional Support ........................................................................................................................................ 27
3.11 Psychological Support ......................................................................................................................................... 28
3.12 Children in the Ebola Treatment Unit .................................................................................................................. 29
3.13 Mothers with breastfeeding children .................................................................................................................. 29
3.14 Maternity and Ebola virus disease ...................................................................................................................... 29
4. Discharge ........................................................................................................................................................ 30
4.1 Discharge Criteria ........................................................................................................................................... 30
4.2 Important Procedures before Discharge ........................................................................................................ 30
4.3 Supportive Treatment and Follow up ............................................................................................................. 30
4.4 Patient Care in the Home Based Support and Risk Reduction ........................................................................ 31
4.5 Laboratory Tests ............................................................................................................................................ 31
4.6 Medical File .................................................................................................................................................... 31
4.7 Psychological Support .................................................................................................................................... 31
4.8 Management of Exposed Individuals ............................................................................................................. 31
IV. INFECTION PREVENTION AND CONTROL ............................................................................ 33
1. General Patient Care ....................................................................................................................................... 33
2. Disinfection in Ebola Treatment Units .............................................................................................................. 33
3. Patient Placement, Staff Allocation, Visitors .................................................................................................... 33
4. Personal Protective Equipment, Hand Hygiene and Other Precautions ............................................................. 34
4.1 Personal Protective Equipment Protocols ...................................................................................................... 34
4.2 Hand Hygiene Protocol ......................................................................................................................................... 36
4.3 Injection Safety ..................................................................................................................................................... 37
4.4 Environmental Cleaning ........................................................................................................................................ 38
2.5 Management of Linen and Blankets ............................................................................................................... 39
5. Waste Management ........................................................................................................................................ 40
6. Moving and Burial of Human Body ................................................................................................................... 42
6.1 Burial Procedure for Patient Dying in the Ebola Treatment Unit: .......................................................................... 42
6.2 Procedure for Burial of Suspect/Probable/Confirmed Patient Dying at Home ...................................................... 44
6.3 Cleaning a Room after Patient Death at Ward ...................................................................................................... 44
6.4 Procedure for house disinfection .......................................................................................................................... 45

iv | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
7. Managing Exposure to Virus ............................................................................................................................ 46
V. COMMUNICATION AND SOCIAL MOBILIZATION .................................................................... 47
1. Overview ......................................................................................................................................................... 47
2. Pre‐Epidemic Phase ......................................................................................................................................... 47
3. Epidemic Phase ............................................................................................................................................... 49
4. Integrated Communication Activities ............................................................................................................... 49
5. Key Messages .................................................................................................................................................. 51

1 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
I. INTRODUCTION TO EBOLA VIRAL DISEASES
1. Background
Ebola Viral Disease (EVD) is one of numerous Viral Hemorrhagic Fevers. It is a severe, often fatal disease in humans and non‐human primates (such as monkeys, gorillas, and chimpanzees).
Ebola virus disease is caused by infection with a virus of the family Filoviridae, genus Ebolavirus. When infection occurs, symptoms usually begin abruptly. The first Ebolavirus species was discovered in 1976 in what is now the Democratic Republic of the Congo near the Ebola River. Since then, outbreaks have appeared sporadically.
There are five identified subspecies of Ebolavirus. Four of the five have caused disease in humans: Ebola virus (Zaire ebolavirus); Sudan virus (Sudan ebolavirus); Taï Forest virus (Taï Forest ebolavirus, formerly Côte d’Ivoire ebolavirus); and Bundibugyo virus (Bundibugyo ebolavirus). The fifth, Reston virus (Reston ebolavirus), has caused disease in non‐human primates, but not in humans.
The natural reservoir host of ebolaviruses remains unknown. However, on the basis of available evidence and the nature of similar viruses, researchers believe that the virus is zoonotic (animal‐borne) with bats being the most likely reservoir.
2. Mode of Transmission
Because the natural reservoir of Ebola viruses has not yet been proven, the manner in which the virus
first appears in a human at the start of an outbreak is unknown. However, scientists believe that the first
patient becomes infected through contact with an infected animal, such as a fruit bat or primate (apes
and monkeys), which is called a spillover event. Person‐to‐person transmission follows and can lead to
large numbers of affected people. In some past Ebola outbreaks, primates were also affected by Ebola,
and multiple spillover events occurred when people touched or ate infected primates.
When an infection does occur in humans, the virus can be spread in several ways to others. Ebola is
spread through direct contact (through broken skin or mucous membranes in, for example, the eyes,
nose, or mouth) with:
blood or body fluids (including but not limited to urine, saliva, sweat, feces, vomit, breast milk,
and semen) of a person who is sick with Ebola
objects (like needles and syringes) that have been contaminated with the virus
infected fruit bats or primates (apes and monkeys)
Contact with infected corpses (human or animal): Bodies of deceased patients or animals that
died of EVD infection are highly contagious because of the high levels of virus in the corpses.
Often traditional burial rituals consist of washing and touching the body to prepare the body and
this practice will lead to infection.
Indirect contact with contaminated objects and environments.
Ebola does not spread through the air or by water, or in general, by food. However, Ebola may be spread
as a result of handling bush meat (wild animals hunted for food) and contact with infected bats. There is
no evidence that mosquitos or other insects can transmit Ebola virus. Only a few species of mammals (for
example, humans, bats, monkeys, and apes) have shown the ability to become infected with and spread
Ebola virus.
2 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Healthcare providers caring for Ebola patients and the family and friends in close contact with Ebola
patients are at the highest risk of getting sick because they may come in contact with infected blood or
body fluids of sick patients.
During outbreaks of Ebola, the disease can spread quickly within healthcare settings (such as a clinic or
hospital). Exposure to Ebola can occur in healthcare settings where hospital staff are not wearing
appropriate protective equipment, including masks, gowns, and gloves and eye protection. Dedicated
medical equipment (preferable disposable, when possible) should be used by healthcare personnel
providing patient care. Proper cleaning and disposal of instruments, such as needles and syringes, is also
important. If instruments are not disposable, they must be sterilized before being used again. Without
adequate sterilization of the instruments, virus transmission can continue and amplify an outbreak.
Once someone recovers from Ebola, they can no longer spread the virus. However, Ebola virus has been
found in semen for up to 3 months. Abstinence from sex is recommended for at least 3 months. If
abstinence is not possible, condoms may help prevent the spread of disease.
3. Incubation Period
The incubation period (period between exposure and development of symptoms) is 2 to 21 days. During
the incubation period the patient is infected with the virus, but is asymptomatic and is not contagious.
During the first days of symptoms the levels of the virus increases and therefore its communicability
increases rapidly. If the patient doesn't manage to establish a proper immune response, then the level of
the virus continues to increase until death occurs. The corpse of a patient who died of EVD infection is
therefore highly contagious. If the immune response is sufficient, then the level of virus decreases
gradually until recovery.
4. Sensitivity of the Virus
It is believed that the Filovirus is not capable of surviving a long time outside the body of an infected
organism. The virus is thought to be able to survive up to some days in a liquid (blood, vomit, corpses,
etc). However, having a lipid (fatty) envelop makes the viruses fragile. Chlorine disinfection, Heat, Direct
sunlight (UV light), Soaps and detergents all destroy the lipid envelop of the virus, thereby killing the
virus.
5. Clinical Features of Ebola Virus Infection
Symptoms start generally and are similar to common diseases like malaria, shigellosis or typhoid. A
clinical diagnosis is therefore difficult. Symptoms develop progressively and filovirus infections can kill
rapidly.
Fever
Severe headache
Muscle pain
Weakness
Diarrhea
Vomiting
Abdominal (stomach) pain
Unexplained hemorrhage (bleeding or bruising)

3 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Symptoms may appear anywhere from 2 to 21 days after exposure to Ebola, but the average is 8 to 10
days.
Recovery from Ebola depends on good supportive clinical care and the patient’s immune response.
People who recover from Ebola infection develop antibodies that last for at least 10 years.
Table 1: Summary of signs and symptoms of EVD
General symptoms: … then often followed by
Intense tiredness and weakness Sudden onset of high grade fever fever Headache Muscle pains Arthralgia Conjunctivitis (1/3 of all patients after 5 days) Nausea and anorexia Painful throat and dysphagia Abdominal pain Hiccups
Chest pain Diarrhea (watery or bloody) Vomiting (sometimes bloody) Orchitis Rash Confusion and irritability Internal and external bleeding (in 30‐50% of
cases, often from mucosa and gingivae) Impaired liver and kidney function Abortion or miscarriage amongst pregnant
women Shock Death

4 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
II. EBOLA VIRUS DISEASE SURVEILLANCE AND LABORATORY DIAGNOSIS
1. Purpose of Surveillance
Considering the infectivity and high case fatality rate of EVD, early detection, timely specimen collection
and processing, immediate isolation of new cases and meticulous contact tracing will limit new chains of
transmission and have a significant impact on control of the epidemic.
With the current EVD outbreak in West Africa countries, Ebola surveillance will be initiated at ports of
entry (airports and land crossing areas) and in the general health system and at community level. The
purpose of this surveillance is:
For early and timely detection of suspected cases and/or outbreaks,
Rapid investigation and early laboratory verification of the etiology,
Contact tracing and follow up of contacts.
Health promotion is one of the priority activities to start with in an intervention. For an efficient
surveillance system, it is important to have a trusting relationship with the community to obtain an
optimum collaboration. The acceptance of being taken to the Ebola Treatment Center or to alert a case
to the surveillance team all depends on the confidence of the community in the intervention and the
health facilities. The teams must be trained to work in tactful and concerned manner that facilitates
developing good relations with the communities.
2. Case Definition of Ebola Virus Disease
2.1. Case Definition Ebola Cases before Outbreak
The following are the case definitions that we need to use for early recognition of suspected cases.
Suspected Case: ‐
A person who has both consistent symptoms and risk factors as follows:
Clinical criteria, a person having fever of greater than 38.60C , and additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, or unexplained hemorrhage;
AND
Epidemiologic risk factors within the past 21 days before the onset of symptoms, such as contact with blood or other body fluids or human remains of a patient known to have or suspected to have EVD; residence in—or travel to—an area where EVD transmission is active*; or direct handling of bats or non‐human primates from disease‐endemic areas.
Probable Case: ‐
A suspected case whose epidemiologic risk factors include high or low risk exposure(s) (see section 3.2 below for levels of exposure risk).
Confirmed Case: ‐
A case with laboratory‐confirmed diagnostic evidence of Ebola virus infection.
Community‐based surveillance: standard case definition
This definition of alert cases for Ebola virus disease has been developed for use by the
community or community‐based volunteers. It may be used for community‐based surveillance
during the pre‐epidemic phase and during the outbreak.

5 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Alert case: Illness with onset of fever and no response to treatment of usual causes of fever in the
area, OR at least one of the following signs: bleeding, bloody diarrhea, bleeding into urine OR any
sudden death.
2.2. Case definitions During an Ebola Outbreak
During an outbreak, the case definitions are likely to be modified to be adapted to new clinical
presentations or different modes of transmission related to the local event.
a. Case definition to be used by mobile teams or health posts and health centres
Suspected Case:
Any person, alive or dead, suffering or having suffered from a sudden onset of high fever and
having had contact with:
a suspected, probable or confirmed Ebola case;
a dead or sick animal (for Ebola)
OR: any person with sudden onset of high fever and at least three of the following symptoms:
headaches
vomiting
anorexia / loss of appetite
diarrhea
lethargy
stomach pain
aching muscles or joints
difficulty swallowing
breathing difficulties
hiccup
OR: any person with inexplicable bleeding
OR: any sudden, inexplicable death.
b. Case definition for exclusive use by hospitals and surveillance teams
Probable case:
Any suspected case evaluated by a clinician
OR: Any deceased suspected case (where it has not been possible to collect specimens for
laboratory confirmation) having an epidemiological link with a confirmed case
Note: if laboratory specimens are collected in due time during the illness, the preceding
categories are reclassified as “laboratory confirmed” cases and “non‐case”.
Laboratory Confirmed Case: Any suspected or probably cases with a positive laboratory result.
Laboratory confirmed cases must test positive for the virus antigen, either by detection of virus
RNA by reverse transcriptase‐polymerase chain reaction (RT‐ PCR), or by detection of IgM
antibodies directed against Ebola.
None Case: Any suspected or probable case with a negative laboratory result. “Non‐case” showed no
specific antibodies, RNA or specific detectable antigens.
3. EVD Surveillance and Measures to Take
3.1 Screening of Passengers at Ports of Entries
With the current evidence of EVD in West Africa, and the declaration of Public Health Emergency of
International Concern, traveller screening – of passengers coming from currently affected countries is
an important activity and contribute to early detection of cases and prevent the importation of a the
disease or to delay such importation.
6 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
WHO advised countries with active EVD to do exit screening of passengers and prohibit passengers
from boarding the flight if sick. Doing the entry screening complements the work of exist screening of
passengers.
Major activities on passengers screening:‐
Raise awareness of EVD and disseminate information among all relevant stakeholders at POE,
Provision of sensitization /orientation to POE public health authorities, POE operators, conveyance operators
Raise awareness among conveyance operators of the need to immediately notify PoE health authorities prior to arrival of any suspected cases.
Ensure that passenger locator forms are on board flights and at the airport, and that airport ground staff and flight crew are trained in managing EVD and environmental contaminants
Provision of training on EVD to crew members, health workers, conveyance operators
Provision of training on the Case definition of EVD, infection prevention
Training of health workers on screening of passengers,
Screening is done with thermal thermometer detector or thermal scanner,
Designation of quarantine place,
Availing the necessary supplies (PPE) and tools (Case investigation form),
Suspected cases should be further screened and ruled for other causes,
Figure below is showing conceptual framework screening of embarking and disembarking passengers.
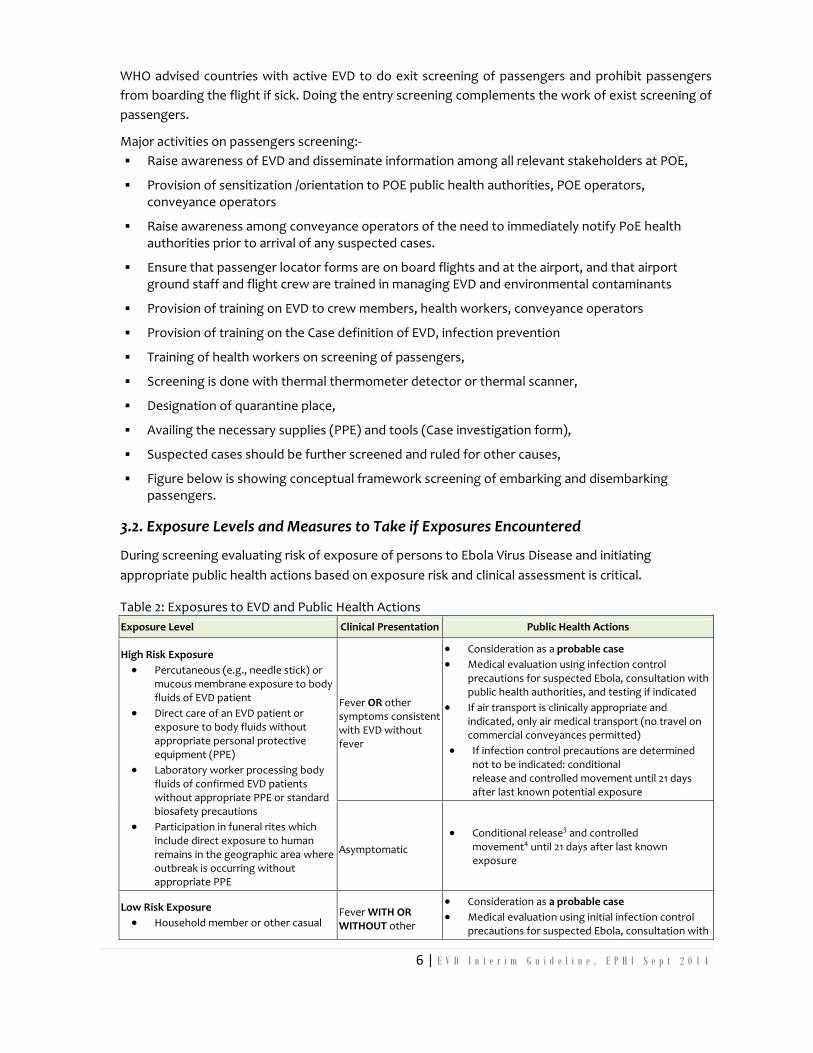
3.2. Exposure Levels and Measures to Take if Exposures Encountered
During screening evaluating risk of exposure of persons to Ebola Virus Disease and initiating
appropriate public health actions based on exposure risk and clinical assessment is critical.
Table 2: Exposures to EVD and Public Health Actions
Exposure Level Clinical Presentation Public Health Actions
High Risk Exposure
Percutaneous (e.g., needle stick) or mucous membrane exposure to body fluids of EVD patient
Direct care of an EVD patient or exposure to body fluids without appropriate personal protective equipment (PPE)
Laboratory worker processing body fluids of confirmed EVD patients without appropriate PPE or standard biosafety precautions
Participation in funeral rites which include direct exposure to human remains in the geographic area where outbreak is occurring without appropriate PPE
Fever OR other symptoms consistent with EVD without fever
Consideration as a probable case
Medical evaluation using infection control precautions for suspected Ebola, consultation with public health authorities, and testing if indicated
If air transport is clinically appropriate and indicated, only air medical transport (no travel on commercial conveyances permitted)
If infection control precautions are determined not to be indicated: conditional release and controlled movement until 21 days after last known potential exposure
Asymptomatic
Conditional release3 and controlled movement4 until 21 days after last known exposure
Low Risk Exposure
Household member or other casual Fever WITH OR WITHOUT other
Consideration as a probable case
Medical evaluation using initial infection control precautions for suspected Ebola, consultation with
7 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
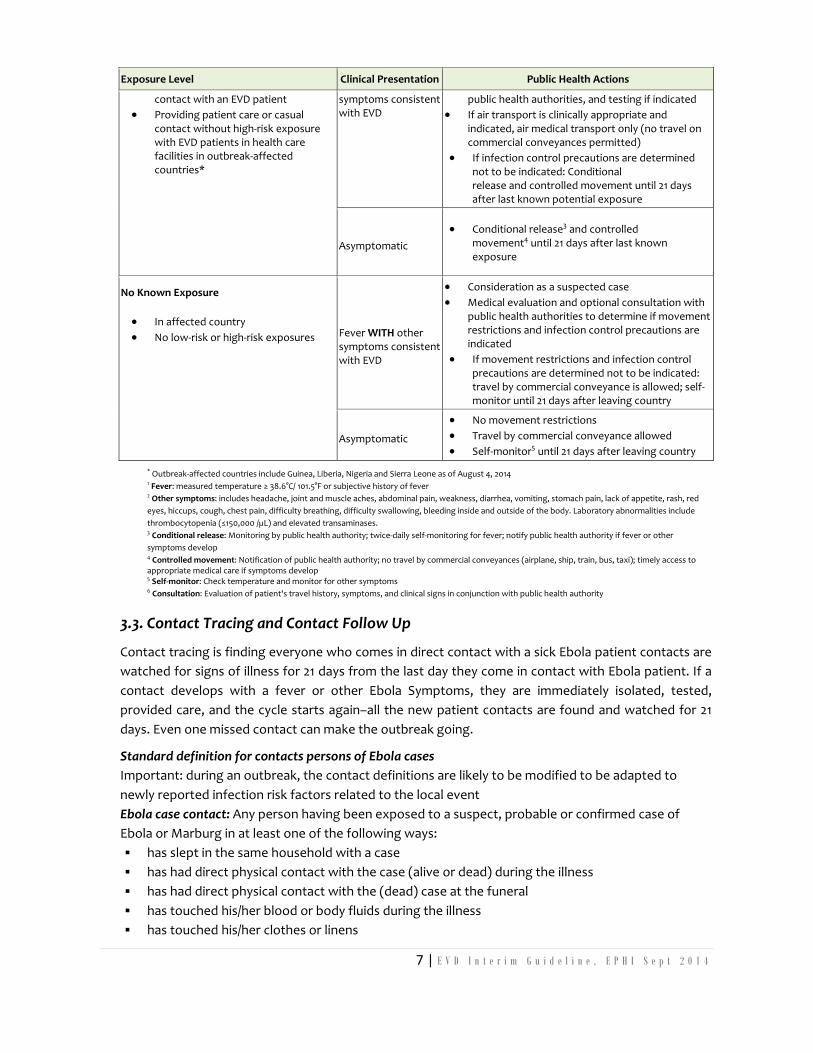
Exposure Level Clinical Presentation Public Health Actions
contact with an EVD patient
Providing patient care or casual contact without high‐risk exposure with EVD patients in health care facilities in outbreak‐affected countries*
symptoms consistent with EVD
public health authorities, and testing if indicated
If air transport is clinically appropriate and indicated, air medical transport only (no travel on commercial conveyances permitted)
If infection control precautions are determined not to be indicated: Conditional release and controlled movement until 21 days after last known potential exposure
Asymptomatic
Conditional release3 and controlled movement4 until 21 days after last known exposure
No Known Exposure
In affected country
No low‐risk or high‐risk exposures Fever WITH other symptoms consistent with EVD
Consideration as a suspected case
Medical evaluation and optional consultation with public health authorities to determine if movement restrictions and infection control precautions are indicated
If movement restrictions and infection control precautions are determined not to be indicated: travel by commercial conveyance is allowed; self‐monitor until 21 days after leaving country
Asymptomatic
No movement restrictions
Travel by commercial conveyance allowed
Self‐monitor5 until 21 days after leaving country
* Outbreak‐affected countries include Guinea, Liberia, Nigeria and Sierra Leone as of August 4, 2014 1 Fever: measured temperature ≥ 38.6°C/ 101.5°F or subjective history of fever 2 Other symptoms: includes headache, joint and muscle aches, abdominal pain, weakness, diarrhea, vomiting, stomach pain, lack of appetite, rash, red
eyes, hiccups, cough, chest pain, difficulty breathing, difficulty swallowing, bleeding inside and outside of the body. Laboratory abnormalities include
thrombocytopenia (≤150,000 /µL) and elevated transaminases. 3 Conditional release: Monitoring by public health authority; twice‐daily self‐monitoring for fever; notify public health authority if fever or other
symptoms develop 4 Controlled movement: Notification of public health authority; no travel by commercial conveyances (airplane, ship, train, bus, taxi); timely access to appropriate medical care if symptoms develop 5 Self‐monitor: Check temperature and monitor for other symptoms 6 Consultation: Evaluation of patient's travel history, symptoms, and clinical signs in conjunction with public health authority
3.3. Contact Tracing and Contact Follow Up
Contact tracing is finding everyone who comes in direct contact with a sick Ebola patient contacts are
watched for signs of illness for 21 days from the last day they come in contact with Ebola patient. If a
contact develops with a fever or other Ebola Symptoms, they are immediately isolated, tested,
provided care, and the cycle starts again–all the new patient contacts are found and watched for 21
days. Even one missed contact can make the outbreak going.
Standard definition for contacts persons of Ebola cases
Important: during an outbreak, the contact definitions are likely to be modified to be adapted to
newly reported infection risk factors related to the local event
Ebola case contact: Any person having been exposed to a suspect, probable or confirmed case of
Ebola or Marburg in at least one of the following ways:
has slept in the same household with a case
has had direct physical contact with the case (alive or dead) during the illness
has had direct physical contact with the (dead) case at the funeral
has touched his/her blood or body fluids during the illness
has touched his/her clothes or linens
8 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
has been breastfed by the patient (baby)
Provided that this exposure has taken place less than 21 days before the identification as a contact
by surveillance teams.
Contacts of dead or sick animals: Any person having been exposure to a sick or dead animal in at least
one of the following ways:
has had direct physical contact with the animal
has had direct contact with the animal’s blood or body fluids
has carved up the animal
has eaten raw bush‐meat
Provided that this exposure has taken place less than 21 days before the identification as a contact by
surveillance teams
Laboratory contacts: Any person having been exposed to biological material in a laboratory in at least
one of the following ways:
has had direct contact with specimens collected from suspected Ebola or Marburg patients
has had direct contact with specimens collected from suspected Ebola or Marburg animal cases
Provided that this exposure has taken place less than 21 days before the identification as a contact by
surveillance teams.
Other infection risk factors include: contact with a hospital where Ebola cases are being treated;
infection; or vaccination in the 21 days preceding the onset of symptoms.
3.3 Contact Tracing
Contact tracing is finding everyone who comes in direct contact with a known sick Ebola patient or a
probable Ebola case. It requires listing all contacts of probable and confirmed cases using a contact
listing form (see annex 3).
The contact person should be followed and monitored for signs of illness for 21 days from the last
day he/she come in contact with Ebola patient or a probable Ebola case using a contact follow‐up
form (see annex 4)
If the contact person is asymptomatic for 21 days after exposure, he released the follow‐up.
Role of Contact Monitors
Review contacts for monitoring and tracing to ensure clear information is available
Visit the homes of listed contacts daily for observation for 21 consecutive days
Report symptomatic cases to supervisor and/or alert coordinator for further management
Review and exclude contacts that have completed 21 days
Submit daily reports about contacts to supervisors
Sensitize communities about referral and denial
Role of Alert Coordinator
Receives and logs in alerts in the alert management database
Disburses response teams for alerts that require immediate action
Presents a daily report of all alerts received and their status to the surveillance meeting
Coordinates with logistics team to ensure response teams are able to do their work
9 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Receive, synthesize daily reports from Supervisors
Role of Woreda supervisor
list all contacts to probable and confirmed cases using a Contact listing form
What Information is required for contact tracing?
Laboratory Result
Total number of contacts listed using the contact listing form
Total number of contacts seen daily
Contacts with symptoms by writing “Y” to the symptoms and immediately reporting to the supervisor.
3.4 Rumors Verification
Rumours of EVD should be treated like real incidents and require urgent verification.
There may be rumors of people dying with haemorrhagic symptoms.
There may be an abnormal and unexpected increase in mortality in a certain area, particularly in members of the same family or one village.
Numerous health staff have fallen sick or died.
Rumours about EVD can reach the surveillance system by different routes:
By the community to the Health extension worker during their visit or Health promotion activities.
Spontaneously by the community member to anybody working in an area or their relative,
Media can report EVD cases or deaths.
As information may be numerous and the right information needs to be gathered before the rumour
verification team will go to see the case. Verify if the symptoms fit in the case definition, and make
sure that relevant information is noted before the verification team goes: e.g. the name of the
suspected case, name of the informant, Gott, Kebele, symptoms and contact history.
If a patient died at home, a medical person should take the clinical history from the family. If there is
a suspicion that the person could have died from Ebola, then the burial team needs to be alarmed to
perform safe burial practices.
Activities:
Each suspect needs to be checked by a medical person that decides if it is a real suspected case and needs to be taken to the Ebola quarantine and isolation ward.
A notification form should be filled in for each rumour (Annex 1). All rumours including the outcome should be registered in a Rumour Registration Book.
If the rumour case is identified as a suspect case, then the patient needs to be transported to the Ebola quarantine unit for assessment and possibly sample taking and admission. The suspected case should not be in contact with anybody until the ambulance team arrives.
As many of the rumour cases might be treatable to common illness, it is advised that always take drugs with you and you need to rule out other treatable diseases/conditions e.g. anti‐malarial, antibiotics and paracetamol.

10 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Whenever you go to verify a rumour take with you at least 3 full PPE clothing with you: for the medical person, the sprayer and 1 spare.
Supplies for Rumor Investigating Team
The following items must be carried in the vehicle. Verify the presence of all items listed in the
following checklist before starting work.
Table 3: Items that are required by rumour investigating teams
3.5 Transporting a Suspected Case
When a suspect case is identified he/she must be transferred to the designated Ebola quarantine or
isolation ward.
To prevent contamination and spreading of infection, patients need to be transported in a safe way. A
pick‐up car with a closed (or open) back is the most preferred and practical to use:
Patients can be transported separately from the transporting staff
Patient is not visible during transport.
The outside is easy to disinfect.
The decision to take a person to Ebola quarantine ward often leads to highly emotional and tense
situations. Communication about the reasons and the procedures to the family and the community is
extremely important to avoid misunderstandings and mistrust.
Item Quantity per person (take spare items for 1 person with you)
Protective Equipment Plastic aprons 1 Goggles 1 Coveralls 1 Head covers 1 Masks 1 Examination gloves (box at least half full) 1 Rubber cleaning gloves 1 pair
Other equipment Total quantity for the team 10-litre spraying machine filled with 0.5% chlorine solution 1 1-litre hand-sprayer filled with 0.05% chlorine solution 1 Plastic sheeting 3m-3m 1 Thermometer 2 Plastic rubbish bags 4 Hand soap 1 bar HTH granules and 1 measuring spoon 1 kg Bucket with lid to hold re-usable protective items after use 1 Guideline for preparing chlorine solutions 1 Tape 1 roll
Medication Anti-malarial: Coartem, oral quinine (pregnant ladies), etc. Oral antibiotics: Ciprofloxacin, amoxicillin, etc. Paracetamol: adults and children Oral Rehydration Solution

11 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Activities
Transportation of suspect cases to the Ebola treatment unit in a safe way.
Spraying of the place where the patient was accommodated.
Spraying of the back of the pick up where the patient was seated
A transport team should be trained, a driver, medical personnel two sprayers are the minimum team
members. They should take 5 PPE with them: 1 for medical person, 2 sprayers, 1 for the caretaker and
1 spare one.
Procedures when transporting the patient to Ebola treatment unit
Take the following items:
2 spraying machines: one for the sprayer dressed up and one for the sprayer undressed.
A mattress with plastic cover to put at the back of the pick up where the patient can lay or sit on during the transport.
Take stretcher to transport patient to the car and from the car to the Ebola ward in case the patient can't walk.
Something that is easy to disinfect on which the patient can step to facilitate to step into the back of the car if the patient can walk.
A bucket with a small amount of a prepared 0.5% solution can be taken at the back of the car in case there is a history of vomiting.
Dressing:
The driver and the health promoter should not be close to the patient and don't need to put on PPE protective clothes. They should be dressed in normal clothes to be as 'normal' and accessible for the population as possible. Explanation will be given to the community about the different steps.
Transporting Patient:
One caregiver can be allowed to support the patient during the transport and should stay on the back of the car with the patient. This person needs to wear protective clothes for caretakers.
If the patient is mobile and can walk alone: The patient will be instructed to take place in the back of the pickup. There is no need for the Rumour verification team to dress up if the patient will not be touched and they keep a distance. When touching anything touched by the patient, for example when closing the back of the pick‐up, examination gloves should be used and these should be sprayed before removal and disposed of safely
If the patient is too weak to walk and needs to be transported with the stretcher: Two people should get dressed up, put the patient on the stretcher and put in the back of the car, together with the caretaker. Dressing and undressing should take place in front of the community in a transparent way. If the patient is heavy, more people need to dress up.
Spraying of the house:
The house where the patient lived when he/she was sick needs to be sprayed. The ambulance team can spray the house before transporting the patient to the Ebola treatment unit or the burial/spraying team can be called. If the house can't be sprayed immediately then the door of the house needs to be locked and no one is allowed to enter the house until the arrival of the Spraying Team. It is advisable to spray the houses of all suspects immediately.

12 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Arrival at the Ebola treatment unit;
The ambulance team should inform the Ebola treatment unit that they will arrive with a patient.
The pick‐up should drive up to the patient's entrance of the Ebola ward.
The back of the pick‐up, the mattress, the bucket (if unused), and other items used need to be properly disinfected with a 0.5% chlorine solution.
4. Outbreak Investigation, Sample Collection and Shipment
4.1 Outbreak Investigation
It is mandatory to establish Ebola Rapid Response Team (ERRT) members at every level to
conduct an investigation of reported Ebola Virus disease. Different experts can be identified
and trained. The RRT should include:
An Epidemiologist
A clinician
A laboratory technician
Environmental health specialist,
Public health officer
A representative of the local health authority,
More professionals based on the type of the PHE.
Partner experts from WHO or Centre for Disease Control (CDC), MSF and others can join to
assist the outbreak investigation.
Before the deployment of the RRTs, all the members of the RRT should be briefed on the
situation, the roles and responsibilities they are expected to play, means, time and frequency
of communication etc. There is a need to assign clear leadership role to one of the team
member based on their level of expertise. Begin the investigation in the most affected places.
Avail relevant resources that are required during the field activity such as,
Different formats (case based formats, line list, outbreak reporting formats)
This guideline and other relevant guidelines and reading materials
Supplies for collecting lab specimens
Supplies that are required for the investigation,
Infection prevention equipment such as personal protective equipment (PPE)
Laptop and wireless network for report writing and communicating reports,
Communication means (Mobile phone, Sat Phone, ‐‐‐) with communication cost if necessary.

13 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
The RRT should be sent as quickly as possible to investigate; the team must have all materials
and equipment necessary for safely carrying out an assessment: examining patients,
collecting samples, and packaging and transporting the samples according to standard.
4.2 Confirmation of Diagnosis by Laboratory: Collection of Specimen and Shipment
(SOP on Lab collection and shipment)

14 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
III. CASE MANAGEMENT OF PATIENTS
1. Principles for Clinical Case Management
Patient safety in hospital is a fundamental right that must be guaranteed to all hospital patients.
Nursing care staff must make the quality of reception, treatment, and care a priority.
Hospital staff must offer psychological support to patients and their families.
Patients and their families have a right to transparent, clear, understandable, accessible, and reliable information.
Each medical intervention requires the free and informed consent of the patient. Consent may be given in writing or orally
In the framework of biomedical research, consent forms must be written in the national language. If the person is unable to give consent (e.g. if they are underage), then the free and informed consent of a parent or legal guardian is required. If the patient is illiterate, then a third party may act as witness.
The patient’s beliefs and religion must be respected.
The patient’s right to privacy and confidentiality must be upheld.
Patients and their families must be given the opportunity to participate in health care decisions that affect them.
2. Set Up and Organization of the Ebola Treatment Center
The setup of the Ebola treatment center should allow activities to be performed in an easy manner with a
clear, rational movement and circulation of people and materials. Minimizing complexity, confusion and
physical exercise contributes to create a safe working environment.
2.1 Location
A single Ebola treatment center is the easiest to manage in terms of training, human resources and
logistics. However, there may be circumstances that require 2 or more settings.
The location of the Ebola should be:
As close as possible to the epicenter of the outbreak to minimize movements,
Easily accessible by cars (ambulance, material, water trucking, etc.),
At a strategic point to have sufficient water supply available,
Spacious to allow adequate space for all activities in the center.
2.2 Buildings / Structures
If there is an isolation area already in use, this can be improved for further use, or a new isolation area
can be built. Existing health structures or other buildings can be used. If no appropriate buildings are
available tent structures can be used, however good infection control will be difficult, and tents can
become extremely hot unless sheltered from the sun.
15 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
To avoid cross infection, suspected, porbable and confirmed cases need to be accommodated in
different rooms or buildings.
Other important issues are:
Beds need to be at least 1 meter separated to ensure privacy and prevent transmission of the
virus.
Wards/patient rooms should have a good ventilation to reduce heat and humidity and to
evacuate chlorine gas.
Use of air‐ conditioner or ventilator is not recommended.
Mosquito net use is not recommendable due the disinfection procedures, but mosquito
screening and insect traps can be installed on windows instead.
2.3 Risk Zones
There are 3 different risk areas in the ebola treatment centers (Isolation Centers) according to their
level of risk of contamination:
A. High‐risk zone
This area is where: Care for suspected, probable and confirmed patients take plac,
Bodies of deceased patient prepared for burial and temporarly stored
Launderying of contaminated clothes carried out.
Waste materials burried or burned.
Laterine and shower for the patients built.
All waste from Low‐risk zone is transferred to the High‐risk zone for disposal.
High‐risk zones outside the isolation facilities may include: Patient’s and deceased patient’s houses.
Morgues.
Medical laboratories and operating theatres.
Traditional health services where by cases visited.
Contamination:
The zone is highly contaminated and everything in this area is considered as being contaminated
including buildings, personal belongings, paperwork, patients and staff (prior to disinfection and
removal of PPE). All materials being used in high‐risk must stay in high‐risk zone.
Clothing:
All the staff entering this area should be dressed in full PPE (Scrub suit, coveralls, goggle or face
shield, face mask, gloves, boots and apron) and adapted PPE for visitors is mandatory. Patients
are not expected to wear PPE and can be admitted in normal clothes.
People:
Only patients, designated staff and authorized visitors are allowed to inter inside the high‐risk
zone.
B. Low‐risk zone
16 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
This area is where:
Dressing of full PPE takes place.
Laundarying of scrub suits, apron, boots, heavy duty gloves done
Store of supplies situated.
Doctors’ room located.
Contamination:
In principle no infectious material should remain, however there is real potential for
contamination to occur due to uncontrolled movement of contaminated people or material from
high riks zone.
Clothing:
All people entering the Low‐risk zone change into scrub suits, gloves and boots.
People:
Medical staff, cleaning staff, water/sanitation and logistic staff, etc.
C. No‐risk zone (Outside the Ebola risk zones)
No infectious material should be present outside the isolation area, but in an epidemic situation infectious material or persons can be anywhere.
General universal precautions to reduce EVD in health settings should be in place.
There is no ‘no‐risk zone’ in an EVD outbreak.
2.4 Activities and Facilities in the Different Risk Zones
Different activities and facilities are required inside the different risk zones in the Ebola treatment
unit.
A. High Risk Zone
Ward or rooms for suspect patients.
Ward or rooms for confirmed patients.
Ward or rooms or space for probable patients.
The following facilities should be available in suspected, probable and confirmed areas (i.e. 1
facility is needed in each area):
Latrines and bathing facilities
Small store for medication and material.
Water collection points (e.g. water taps)
Water point with 40 liter water buckets: 1 bucket for 0.5% chlorine solution and 1 bucket for 0.05% chlorine solutions
Potable water point for patients: 40 liter water bucket or tap
Hand washing point for patients
Laundry area
17 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Shaded area for patients. (If possible close to outside fence to allow communication with relatives/friends that are outside the isolation facilities, but with double fencing or enough space to avoid physical contact or droplets transmission).
One waste zone with burning area, sharps pit and organic waste pit. (Do not use existing ones, as they can’t be reused after the outbreak is declared over.)
One Morgue.
Spare building for possible supplementary facilities (delivery, paediatrics, recovery zone etc.)
B. Low‐risk zone
Laundry and drying area.
Area for the preparation of chlorine solutions.
Doctor’s room: resting area and part of medical file papers will be stored here.
Small pharmacy and store.
Changing room to enter and exit Low‐risk zone.
Changing room to enter and exit High‐risk zone.
C. No‐risk zone (Outside the Ebola risk zones)
Kitchen for patients. (E.g. kitchen from hospital can be used.)
Latrine and shower for staff.
Psychological debriefing room for staff and patients
2.5 Fencing
Fencing is important to mark the different risk zones. By clearly indicated borders between the risk
zones the staffs is aware of entering a different risk level.
A fence should be put around the whole isolation facility to mark the borders between outside the isolation facility and inside the isolation facility. Use mesh fencing for transparency.
Physically separate High‐risk and Low‐risk zones in the Ebola treatment unit by fencing or using existing walls to prevent uncontrolled movements between the zones.
Different latrines, bathing facilities and stores should be created for suspected and confirmed patients to prevent cross infection between confirmed patients to negative suspect cases waiting for the lab results. Separation needs to be well indicated and understandable to prevent confusion amongst the patients and the staff.
2.6 Layout of Ebola Treatment Unit
The Ebola treatment unit layout should fit to the list of the facilities and functions the different risk
zones should serve. Accordingly the ideal lay out of the unit should look like the figure in Annex 5. The
shape can change depending on the existing situation of the space.
Entrance/exit points and disinfection
Numbers of entrance/exit points should be limited to be able to control people going in and
out and to ensure a proper disinfection.
18 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Guards and disinfection points are needed at all entrance/exit points and the points need to
be well accessible for cars.
One entry/exit for entering the Low‐risk area for staff and caregivers.
Hand washing and shoe spraying with 0.05% chlorine solution at entry and exit to avoid taking
contamination into or outside the low risk area.
Two entries/exits for entering/leaving the High‐risk area: One for staff and caregivers (via the
Low‐risk area) with sprayer and disinfection area and one for patients directly
entering/leaving the suspect area with sprayer/guard for disinfection when discharged
patient leaves.
One separate exit for dead bodies close to mortuary.
Changing Rooms
Two different changing rooms are necessary (Example of layout of changing rooms See
Annex 6 and 7)
Changing room 1
Located at the entrance to the Low‐risk zone to take off normal clothing and change into
basic protective clothing when entering the Low‐risk zone.
Also used for take‐off basic protective clothing and change into normal clothing when leaving
the Low‐risk zone.
Important necessities for changing room 1:
Clean scrub suits, boots and gloves in sufficient quantities and sizes available.
Buckets or boxes to put in dirty clothes when changing.
A division for men and women to change clothes.
Shelves or hangers to leave normal (street) clothing.
Changing room 2
Located at the entrance to the High‐risk zone to put on and take off the additional PPE
required in the High‐risk zone.
Important necessities for changing room 2:
Staff entering clean and staff leaving dirty or potentially contaminated the High‐risk area
should not interfere with each other.
Entry path should be separated from the exit path to prevent cross contamination between
‘dirty’ people coming from the High‐risk area and ‘clean’ people from the Low‐risk area.
The border between the different risk zones should be clearly indicated.
Sufficient PPE with gloves in different seizes available.
19 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Mirrors and adequate lighting to check protective gear. When dressing best is to dress in
pairs to be able to check each other when dressing.
Disinfection point for staff leaving the High‐risk area with sprayer and buckets (bowl) with
0.5% and 0.05% chlorine solution and clean water to wipe of the chlorine of the goggles.
2.7 Patient screening area
Screening of patients should be done in No‐Risk zone The health worker needs to dress in glove, face mask and eye goggle
Keep a distance of at least 1 meter from the patient
The patient has to face away from doctor at 90 degrees
Take temperature of the patient from behind
3. Patient Care at Ebola Treatment Unit
3.1 Medical Staff Medical and nursing care should be provided 24 hrs per day and 7 day per week.
Organize 8 hrs shifts. Adequate rest needs to be taken after shifts,
During each shift 2‐3 breaks need to be taken. The staff should undress and go out of the High‐risk area when having a break.
4 Teams can be formed: 1 team for each shift and 1 off.
Each team should contain medical doctor or Health officer and 2‐4 nurses, depending on the amount of patients admitted and the available human resources. It is advisable to work in couples for a good collaboration and to supervise each other.
A medical doctor should supervise and train the staff.
3.2 Admissions Admission should be possible 24 hrs around the clock. All identified suspect or probable cases need to
be admitted in the suspected or probable area until laboratory results are known or clinical discharge
criteria are reached (in absence of a lab).
The following activities need to be done on admission:
Explanation needs to be given to the patient and the patient's attendant about the reason of admission, the procedures and rules in the Ebola treatment unit, the location of toilets and showers and the visiting hours.
Ideally an information paper for patients and one for the patient's attendant should be read and explained.
All material will be provided from inside the Ebola ward to the patients. Items given from outside to the patient may need to be destroyed and this should be well explained to the patient and relatives. Under supervision it is allowed to bring food from home to the patient.
A bed in the suspected area needs to be prepared and indicated to the patient.
Different items need to be given to the patient like mattress, blanket, cup, plate, soap, etc. These items must not be shared in between patients.
Creation of a personal medical file containing the investigation form.
Observation sheet

20 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Symptomatology and vital signs needs to be started on day of admission and continued during the
whole period of stay. Two forms should be filled in: 1 stays in the High‐risk area and 1 in the medical
room in the Low‐risk area.
Treatment sheet
Needs to be filled in with the prescribed treatment by the doctor in charge, also 1 sheet inside and 1
outside high‐risk area.
3.3 Laboratory Tests A lab test needs to be performed if possible on the day of admission. Samples should only be
taken for diagnostic purposes. Discharge decisions are taken on clinical grounds, but in some cases sample results might help in taking the decision. Sample taking is a high‐risk procedure. When taking a sample prudent behaviour and concentration is essential.
PPE doesn't protect a person from a needle stick incident.
If the result is negative and the sample is taken between days 0‐3 after onset of symptoms, the test should be repeated. The second sample needs to be taken on a day more than 3 days after start of symptoms. Also sometimes a clinically obvious case might have a negative laboratory result due to reverse transcriptase inhibitors present in the blood.
If the test is positive for Ebola the patient will need to be transferred to the confirmed area and the area where the patient was accommodated in the suspected ward need to be disinfected.
3.4 Medical Care After attending each patient the gloved hands should be washed with 0.5% chlorine solution
before changing the gloves to prevent spread of infections between patients.
Currently there is no curative treatment for Ebola virus diseases. Only supportive treatment can be offered to the patients. However experience in former outbreaks shows that supportive treatment reduces the suffering of the patients and aggressive invasive supportive treatment might maximize chances of survival.
Detailed data collection on treatment given and treatment outcome needs to be gathered to gain a better understanding and more information about the effects of the different supportive therapies.
Experimental treatments with different types of drugs or vaccines may be considered during an outbreak, if no harm for the patient can be expected and if consent is provided.
Medical equipment for physical examination like blood pressure machines and stethoscopes are difficult to use due to the barrier created by the protective clothing. Moreover the disinfecting procedures needed after each use, with chlorine solutions will destroy the material and reduce the reliability of the equipment.
No digital thermometers should be used. If only digital thermometers are available, each patient should have his own and after discharge or death, the thermometer should be destroyed.
Different levels of supportive treatment may be provided depending on the safety conditions in the isolation ward. Providing basic oral medication and rehydration solutions is easy and involves minimal risk for staff and patients.

21 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
3.5 Invasive Procedures
Invasive procedures like injected drugs, IV fluids and NG tubes are potentially dangerous for the
person performing them. It should be minimized and only be performed when the required safety
conditions are achieved.
Safety conditions for invasive procedures:
Availability of skilled, experienced and well trained staff
Adequate infection control
Sufficient lighting
2 people should perform the invasive procedure: one actually performing the procedure and the other assisting in handing out material and controlling the patient.
Patients should be properly positioned.
Sharp box and all material needed should be taken to the bedside.
Inserted cannulas should be well secured to avoid being pulled out by the patient, resulting in spreading contaminated blood.
Plastic cannulas should be used for IV infusions. Metal needles and butterflies should only be used for injections and not for drips, given the hazard they pose.
No risk should be taken with aggressive or confused patients. Tranquillizers should be given to them before performing dangerous procedures or such procedures should be avoided.
No invasive care should be provided to a patient where a non‐invasive alternative is equally effective, e.g. there is no need for injectable medication if oral medication is sufficient.
If injected treatments are given, medicines with long half‐lives should be chosen to minimize the number of injections that need to be given (e.g. Ceftriaxone).
Each invasive procedure is a dangerous action for the person performing the procedure and his
assistant. Therefore limit the invasive procedures to the absolutely necessary, but keep in mind that
intensive supportive treatment may have a positive impact on the outcome.
3.6 Hydration
Oral hydration
Ebola and Marburg provoke gastro‐intestinal symptoms such as watery diarrhoea, vomiting and anorexia, as well as causing fever. This may result in severe dehydration.
Oral Rehydration Solution (ORS) should be provided to patients able to drink and support needs to be given to weak patients. Patients with light vomiting should be put on anti‐emetics.
IV hydration
Patients with insufficient oral intake, severe diarrhoea or vomiting (insufficient input for increased output) or paralytic ileus should start IV hydration.
Perfusion rate and quantity of fluid depend on the grade of dehydration. Patients need to be monitored for signs of over‐hydration resulting in pulmonary oedema e.g. engorged jugular veins, tachypnoea or tachycardia.
3.7 Management of Shock in EVD Patients
General signs of shock (poor perfusion)
Low BP (SBP <90)
22 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Fast weak pulse
Pallor or cold extremities
Decreased capillary refill
Dizziness or inability to stand
Decreased urine output(<30ml/hour)
Difficulty breathing
Impaired consciousness, lethargy, agitation, confusion.
Assessment of pulse and BP should be taken in the context of the patient's premorbid state, pregnancy, age, and medication. Some pregnant women, patients with chronic illness, and others may normally have a SBP <90 mmHg and have normal mental status, capillary refill, and urine output; they do not have shock.
VHF patients can be in shock from internal haemorrhage or from septic shock. The pathophysiology and the intensive supportive care for VHF are the same for septic shock from a bacterial infection, malaria and other causes of septic shock. Intensive supportive care is the only clinical management that can be provided to these patients and may have a positive impact on disease outcome.
VHF patients may also have co‐infection with bacteria or malaria that can contribute to septic shock. It should also be recognized that VHF patients can also develop hypovolemic shock as a result of haemorrhage.
The shock in a VHF patient may be a combined picture from haemorrhage, disseminated intravascular coagulation (DIC) and from sepsis. Call for help from the most experienced clinician available when a VHF patient develops shock.
Manage septic shock in adolescents and adults
Clinical Diagnosis
Suspected infection plus Hypotension (systolic blood pressure<90mmHg) plus One or more of the
following:
Pulse >100 per minute
Respiratory rate >24 breaths per min ute
Abnormal temperature (<36° C or >38° C).
General principles of managing patients with septic shock
Manage airway (see Quick Check).
Give oxygen (see Quick Check).
Give IV fluid rapidly (see specific fluid recommendations which follow).
Treat underlying cause.
Consider vasopressors if SBP <90 and signs of inadequate perfusion after fluid resuscitation.
Monitor ‐ record ‐ respond.
Give fluids rapidly
First give an initial 1000 ml LR or NS bolus, continue Ringer's lactate (LR) or Normal saline (NS) at 20 ml/kg/hour, not to exceed a maximum of 60 ml/kg in the first 2 hours (including the initial bolus).
Monitor systolic blood pressure (SBP) and clinical signs of perfusion (urine output, mental status).

23 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
If SBP remains <90 and signs of poor perfusion continue after fluid resuscitation over the first 2 hours,
Consider adding vasopressors (dopamine or epinephrine) using the instructions in Appendix D (How to give vasopressors).
To avoid fluid overload, decrease the rate of fluids to 5‐10 ml/kg/hour.
At 2‐6 hours, if SBP rises above 90, continue fluids at 2 ml/kg/hour. However, if the pulse is still high and there are other signs of poor perfusion, patient may still be volume‐depleted and need more fluids.
Watch carefully for signs of fluid overload (increased jugular venous pressure, increasing crepitation on auscultation). If present, decrease the rate of fluid administration. Call for help from more senior clinician to further evaluate overload and decide fluids
Give empirical IV antimicrobials within the first hour.
Antibiotics: Urgently administer broad spectrum antibiotics by IV. Take blood cultures before antibiotics, but do not delay treatment to get blood cultures.
Choice of antibiotics depends on presence of signs of local infection, local disease
Patterns and availability of antibiotics. A good choice is ceftriaxone 2 grams daily IV.
If community‐acquired pneumonia is suspected, refer to your national or institutional guidelines.
ceftriaxone (2 gram daily IV) or ampicillin 2 grams every 6 hours plus gentamicin 1.5 mg/kg IV every 8 hours, plus ciprofloxacin.
Antimalarials: Do bedside RDT for malaria and if positive start artesunate IV, or if not available, IV quinine
In addition to repeated measurement of SBP, pulse, respiratory rate and pulse‐ oximetry, regular clinical examination is important for patients in shock. Pay particular attention to the signs of poor perfusion and signs of fluid overload to help guide on‐going management.
Signs of poor perfusion:
decreased urine output
altered mental status
Signs of fluid overload:
worsening crepitation on auscultation
dyspnoea
elevated JVP
peripheral oedema
Manage septic shock in children
Children can also be infectious. Use standard precautions (see section 7). Signs of shock in children:
Cold hands plus
Weak or absent puIse and either
Capillary refill time > 3 seconds OR
AVPU less than Alert
Children in shock who require bolus fluid resuscitation are lethargic and have cold skin, prolonged
24 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
capillary refill, fast weak pulse and hypotension.
Check whether the child's hand is cold. If so, determine whether the child is in shock.
Check whether the capillary refill time is longer than 3 seconds. Apply pressure to whiten the nail of the thumb or the big toe for 5 seconds. Determine the time from the moment of release until total recovery of the pink colour
If capillary refill is longer than 3 seconds, check the pulse. Is it weak and fast? If the radial pulse is strong and not obviously fast, the child is not in shock. If you cannot feel the radial pulse of an infant (< 1 year old), feel the brachial pulse or, if the infant is lying down, the femoral pulse. If you cannot feel the radial pulse of a child, feel the carotid. (See the Emergency Triage Assessment and Triage guidelines).
General principles of managing children with septic shock
Manage airway.
Give oxygen through nasal prongs or catheter‐ start at 1‐2 litres/min to aim for oxygen
saturation 90%.
Give IV fluid ‐ initial 20 ml/kg LR or NS bolus.
Treat underlying cause
Administer empirical broad spectrum antibiotics (eg ceftriaxone 80 mg/kg once daily)
Antimalarials: Bedside RDT for malaria and if positive, start IV artesunate (or quinine if
artesunate is not available)
Consider vasopressors if failure of fluids and blood to raise SBP and if signs of inadequate
perfusion persist.
Monitor ‐ record ‐ respond.
Initial intravenous fluid resuscitation for children with shock (and no severe malnutrition)
Check that the child is not severely malnourished, as the fluid volume and rate is different
Insert an IV line (and draw blood for emergency laboratory investigations).
Attach Ringer's lactate or normal saline; make sure the infusion is running well.
Infuse 20 ml/kg over 1 hour.
Emergency Fluid management in Severe Malnutrition
Shock: Cold, hands pulse absent, slow (<60 bpm) or weak pulse and either capillary refill >3
seconds or reduced consciousness.
Give 15 ml/kg in 1 hour of Half Strength Darrow's (HSD) in 5% dextrose or Ringers lactate. If
HSD in 5% Dextrose not available it can be made by adding 50 ml 50% dextrose to 450 ml HSD
If child improves:
Repeat this bolus over another 1 hour.
Then switch to oral or ng fluids using ReSoMal at 10 ml/kg/hour for up to 10 hours.

25 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
As soon as conscious introduce F‐75 and appropriately reduce amount of ReSoMal given.
If child does not improve:
Give maintenance IV fluids at 4 ml/kg/hr.
Watch carefully for signs of fluid overload
His is due to Excess of too rapid iv fluid
Incorrect use of hypotonic rather than isotonic crystalloid solutions
Continuation of IV fluids for too long (once plasma leakage has resolved
Use of large volumes of IV fluid in children with severe capillary leakage
Early sign:
fast breathing, chest in drawing, Large pleural effusions, ascites, peri‐orbital or soft tissue
oedema
Late sign:
pulmonary oedema, cyanosis, irreversible shock (often a combination of ongoing hypovolaemia
and cardiac failure)
The management of fluid overload varies depending on whether the child is in or out of shock
Children who remain in shock and show signs of severe fluid overload are extremely difficult
to manage and have a high mortality.
Avoid diuretics, as they will cause further intravascular fluid depletion
Aspiration of large pleural effusions or ascites can be considered to relieve respiratory
symptoms, but the risk of bleeding should be recognized.
If shock has resolved but the child has fast breathing and large effusions, consult with
pediatric expert to consider giving oral or IV furosemide 1 mg/kg once or twice a day for 24
hours (and oxygen therapy)
If shock has resolved and the child is stable, stop IV fluids and keep the child on bed rest for
24‐48 hours. The excess fluid will be re‐ absorbed and lost through urinary diuresis.
Remark:
In case of shock crystalloids should be used. Colloids should be banned as it may affect blood clotting
and evidence of superiority of colloids over crystalloids is lacking in patients with shock.
3.8 Symptomatic Care
Ebola infections often provoke a painful throat and difficulty in swallowing. Therefore the amount of
tablets to be swallowed should be as low as possible and the size of the tablets as small as possible.
Also tablets may be crushed.
Anti‐pyretics:
26 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
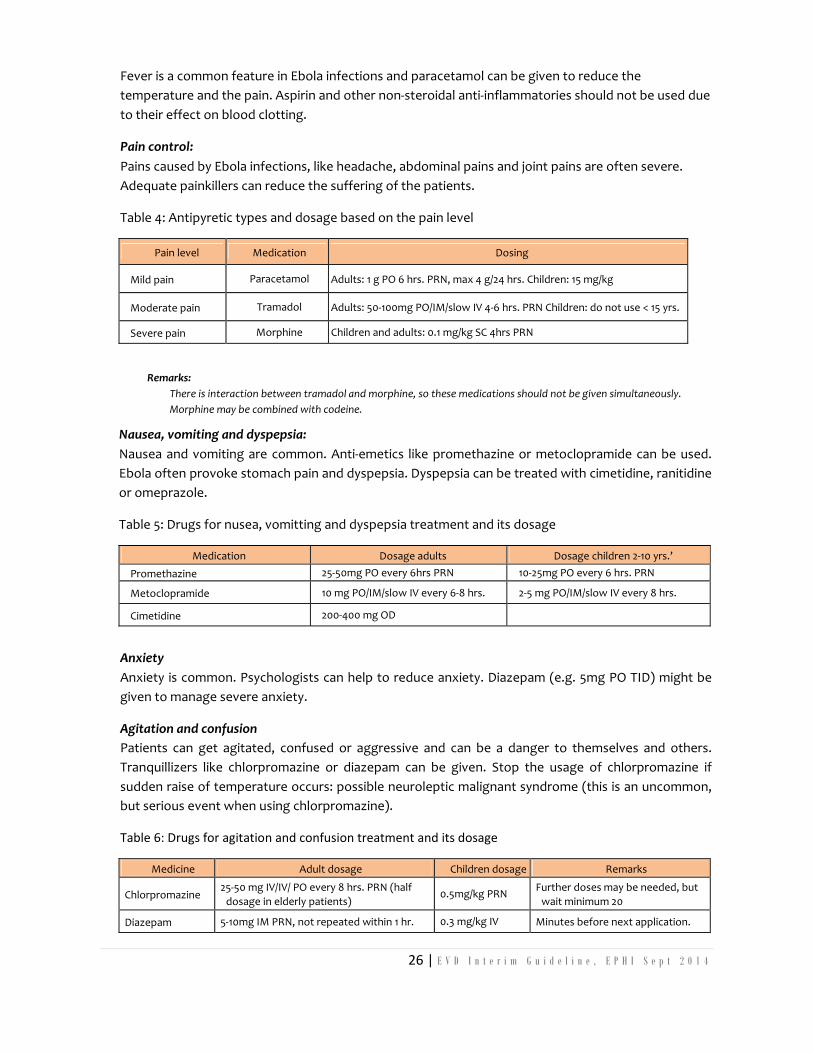
Fever is a common feature in Ebola infections and paracetamol can be given to reduce the
temperature and the pain. Aspirin and other non‐steroidal anti‐inflammatories should not be used due
to their effect on blood clotting.
Pain control:
Pains caused by Ebola infections, like headache, abdominal pains and joint pains are often severe.
Adequate painkillers can reduce the suffering of the patients.
Table 4: Antipyretic types and dosage based on the pain level
Pain level Medication Dosing
Mild pain Paracetamol Adults: 1 g PO 6 hrs. PRN, max 4 g/24 hrs. Children: 15 mg/kg
Moderate pain Tramadol Adults: 50‐100mg PO/IM/slow IV 4‐6 hrs. PRN Children: do not use < 15 yrs.
Severe pain Morphine Children and adults: 0.1 mg/kg SC 4hrs PRN
Remarks:
There is interaction between tramadol and morphine, so these medications should not be given simultaneously.
Morphine may be combined with codeine.
Nausea, vomiting and dyspepsia:
Nausea and vomiting are common. Anti‐emetics like promethazine or metoclopramide can be used.
Ebola often provoke stomach pain and dyspepsia. Dyspepsia can be treated with cimetidine, ranitidine
or omeprazole.
Table 5: Drugs for nusea, vomitting and dyspepsia treatment and its dosage
Medication Dosage adults Dosage children 2‐10 yrs.’
Promethazine 25‐50mg PO every 6hrs PRN 10‐25mg PO every 6 hrs. PRN
Metoclopramide 10 mg PO/IM/slow IV every 6‐8 hrs. 2‐5 mg PO/IM/slow IV every 8 hrs.
Cimetidine 200‐400 mg OD
Anxiety
Anxiety is common. Psychologists can help to reduce anxiety. Diazepam (e.g. 5mg PO TID) might be
given to manage severe anxiety.
Agitation and confusion
Patients can get agitated, confused or aggressive and can be a danger to themselves and others.
Tranquillizers like chlorpromazine or diazepam can be given. Stop the usage of chlorpromazine if
sudden raise of temperature occurs: possible neuroleptic malignant syndrome (this is an uncommon,
but serious event when using chlorpromazine).
Table 6: Drugs for agitation and confusion treatment and its dosage
Medicine Adult dosage Children dosage Remarks
Chlorpromazine 25‐50 mg IV/IV/ PO every 8 hrs. PRN (half
dosage in elderly patients) 0.5mg/kg PRN
Further doses may be needed, but
wait minimum 20
Diazepam 5‐10mg IM PRN, not repeated within 1 hr. 0.3 mg/kg IV Minutes before next application.
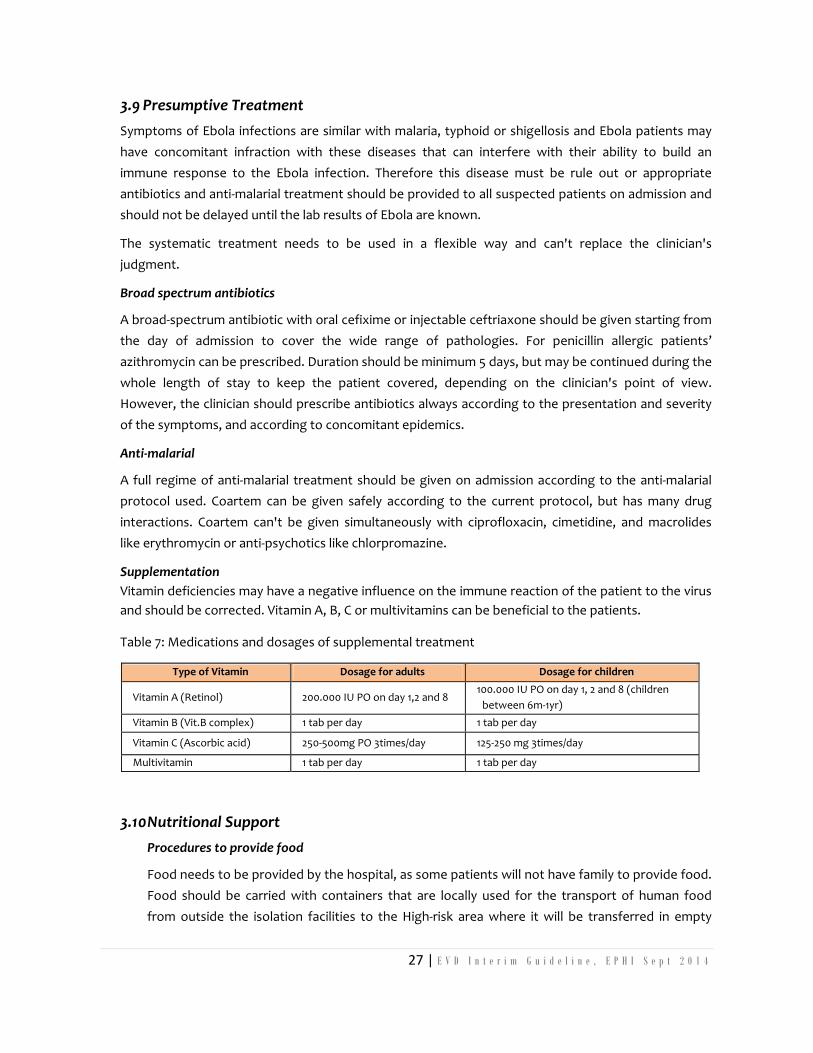
27 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
3.9 Presumptive Treatment
Symptoms of Ebola infections are similar with malaria, typhoid or shigellosis and Ebola patients may
have concomitant infraction with these diseases that can interfere with their ability to build an
immune response to the Ebola infection. Therefore this disease must be rule out or appropriate
antibiotics and anti‐malarial treatment should be provided to all suspected patients on admission and
should not be delayed until the lab results of Ebola are known.
The systematic treatment needs to be used in a flexible way and can't replace the clinician's
judgment.
Broad spectrum antibiotics
A broad‐spectrum antibiotic with oral cefixime or injectable ceftriaxone should be given starting from
the day of admission to cover the wide range of pathologies. For penicillin allergic patients’
azithromycin can be prescribed. Duration should be minimum 5 days, but may be continued during the
whole length of stay to keep the patient covered, depending on the clinician's point of view.
However, the clinician should prescribe antibiotics always according to the presentation and severity
of the symptoms, and according to concomitant epidemics.
Anti‐malarial
A full regime of anti‐malarial treatment should be given on admission according to the anti‐malarial
protocol used. Coartem can be given safely according to the current protocol, but has many drug
interactions. Coartem can't be given simultaneously with ciprofloxacin, cimetidine, and macrolides
like erythromycin or anti‐psychotics like chlorpromazine.
Supplementation
Vitamin deficiencies may have a negative influence on the immune reaction of the patient to the virus
and should be corrected. Vitamin A, B, C or multivitamins can be beneficial to the patients.
Table 7: Medications and dosages of supplemental treatment
Type of Vitamin Dosage for adults Dosage for children
Vitamin A (Retinol) 200.000 IU PO on day 1,2 and 8 100.000 IU PO on day 1, 2 and 8 (children
between 6m‐1yr)
Vitamin B (Vit.B complex) 1 tab per day 1 tab per day
Vitamin C (Ascorbic acid) 250‐500mg PO 3times/day 125‐250 mg 3times/day
Multivitamin 1 tab per day 1 tab per day
3.10 Nutritional Support
Procedures to provide food
Food needs to be provided by the hospital, as some patients will not have family to provide food.
Food should be carried with containers that are locally used for the transport of human food
from outside the isolation facilities to the High‐risk area where it will be transferred in empty

28 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
containers inside the High‐risk area without contact between the containers. In the High‐risk area
it will be divided for the suspected area and the Confirmed area. Some food should be kept in the
Low‐risk area for the caregivers.
Families should also be allowed to provide food for their relatives, as this food is likely to be more
acceptable by the patients. Family can provide food to the patient 'over the fence' of the High‐
risk area under supervision of the staff, and no items should be taken inside the High‐risk area.
Plates inside the High‐risk area need to be disinfected and washed first before food can be
received. Help needs to be given to patients who are not able to eat independently.
Type of food
Ebola infections can provoke anorexia, vomiting and difficulty in swallowing. Inappropriate
feeding can contribute to an ineffective immune response to the infection. Food should be
easy to digest, well balanced and culturally acceptable.
The patient should be encouraged to take Plumpynut, besides the food provided by the
hospital, the hospital or the family. Alternatively porridge can be offered because it is easy to
swallow. NG tube feeding can be considered in severe feeding problems.
Nursing care
Nurses, rather than family members, should provide all basic nursing care, to reduce the risk
of transmission. However often there might not be sufficient nursing staff employed and
then family members may be needed to help providing care like feeding. These family
members must be instructed and supervised and protective clothing should be given.
Relatives involved in basic nursing care will be considered as a contact and will need to be
followed up for 21 days after their last visit to the Ebola treatment unit.
Nursing tasks (to be adapted to the available human resources and work load):
Patient monitoring: check temperature three times daily, Observation for symptoms that
need to be mentioned during the doctor's round.
Medication: (Separate stocks are needed for suspected and confirmed patients.) Medication
should be provided according to doctor's prescription and crossed after the patient's intake.
Call the doctor in case of any medical problem
Provide food, water and ORS and assists where needed and registers quantities.
Hygiene: help bathing in shower or in the bed and ensure clean bed linen for patient.
Explain what you are doing and why to the patient.
3.11 Psychological Support
Psychological support should be offered to all patients and families, ideally from the
beginning of the intervention. However providing psychological care in PPE might be
uncomfortable and difficult: The PPE is physically exhausting for the psychologist/counsellor

29 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
and for the patient it is impossible to see the face of the psychologist (seeing faces helps to
establish a good contact).
For mobile patients an area can be created where the patients can talk over the fence of the
High‐risk area with the psychologist at sufficient distance to prevent contamination.
3.12 Children in the Ebola Treatment Unit
Providing 24‐hour care and psychological support for babies and small children is difficult in
full protective clothing. The staff should provide the care as much as possible. However, for
the wellbeing of both children and parents, parents should be permitted to stay in the Ebola
treatment unit to care for their children.
Protective clothing should be provided and supervised by the staff in the Ebola treatment
unit. Parents/caregivers should take regular breaks and leave the Ebola treatment unit, e.g. at
times when there is food for them available in the Low‐risk area.
Ideally one person should take care of the child to minimize the number of people at risk of
infection, but it might be decided that more caretakers will care for the child during the
admission time. All caregivers will need to be followed up as contacts.
3.13 Mothers with breastfeeding children
There is a high risk that mothers with Ebola infection will infect their children. Therefore
precautions to minimize this risk must be taken:
Stop breastfeeding immediately and provide artificial milk or Plumpy nut (if child is > 6
months). Continue stimulation of milk production and relieve breast congestion with a breast
milk pump.
Separate child from the mother and close monitoring is needed for 21 days. Child is seen as a
close contact. Discourage breastfeeding from another women (wet‐nursing).
3.14 Maternity and Ebola virus disease
Obstetric patients pose special problems in an outbreak:
Vaginal bleeding is a common symptom and obstetric patients are likely to fit the alert or
suspected case definition for EVD.
Patients with EVD are likely to abort or to miscarry and have a very poor prognosis. During an
EVD outbreak it is difficult to differentiate between a 'normal' spontaneous
abortion/miscarriage and one induced by the EVD on clinical grounds alone; a blood sample
will help with the diagnosis. Full term deliveries are rare in Ebola treatment unit, but basic
facilities for deliveries and a private area to conduct them should be installed if possible.

30 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
4. Discharge
4.1 Discharge Criteria
The decision to discharge a patient should be taken on clinical grounds, but if available can be
supported by the laboratory results. A negative PCR means that the virus can't be detected anymore
in the body and the patient is unlikely to be contagious. Patients can be discharged if they meet all
following clinical criteria:
Clinical criteria:
3 days without fever or significant symptoms AND A significant improvement in clinical condition
AND Able to feed, wash and walk independently.
Laboratory support:
Antigen or PCR is negative on day 4 or later after the onset of the symptoms OR PCR turned
negative after having been positive AND patient is clinically cured OR If patients suffers
symptoms, but these are not thought to be due to EVD, 2 negative blood PCR's 48 hrs apart can
be used as discharge criteria. The patient might be referred to another ward.
Fever can be absent in late and terminal stages of the illness and is not a reliable sign for
discharge (or admission). Absence of fever cannot be used alone to plan discharges.
4.2 Important Procedures before Discharge
Disinfection
On discharge all clothes should be disinfected by soaking them for 30 min in a 0.05% chlorine solution,
then wash with soap, rinse with water and then air‐dry. Severely dirty clothes should be burnt. It is
useful when replacement clothing brought by family members is available. All discharged patients
should take a shower with 0.05% chlorine solution and put on his/hers replacement or clean clothes
and avoid any contact with items in the Ebola ward. Disinfect and return other belongings to the
patient. The patient can go to the patient exit where hands and feet will be sprayed. The hospital
belongings like bed, mattress (with plastic protection) and buckets need to be disinfected and may
be reused by another patient. Sheets should be burned and eating utensils thrown away.
Accompany patient to his/her home
Rejection of patients by their communities is a common phenomenon in EVD outbreaks. A medical
person or a health promoter or a psychologist should explain to the family and the community that
they are not contagious anymore and that touching them is not a problem.
4.3 Supportive Treatment and Follow up
Convalescent patients will be weak for some weeks or months and additional help can be
provided:
Provide 1‐2 month supply of vitamin supplements.
Provide Plumpy nut as additional food to the normal food for a Flexible time period;
depending on severity of weakness and poverty of family)
31 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
Provide condoms for 3 months to all male discharged patients and explain the purpose. The
virus can be found in the semen up to 3 months after unset of disease, so theoretically
infecting other people is possible.
Regular visits are recommendable to follow the recovery, to see if additional supportive is
needed and to help integration into the community.
4.4 Patient Care in the Home Based Support and Risk Reduction
The designated caregiver will be the person entering the HBSRR after a proper training is
given. The medical person might accompany the caregiver when entering the HBSRR on the
daily visits, however sometimes daily visits cannot be assured (workload, distances, etc.).
4.5 Laboratory Tests
If possible laboratory tests for confirmation should be taken in the Home Based Support and
Risk Reduction. Use of PPE is compulsory and sufficient light should be there when taking the
sample.
4.6 Medical File
A medical file should be created as for patients admitted in the Ebolatreatment unit with:
notification form, admission and investigation form, observation sheet and treatment sheet
No injected treatment can be provided (no ensured sufficient lighting, no continuous follow
up, etc) but painkillers, oral antibiotics, anti‐malarials and ORS can be given by the caretaker.
4.7 Psychological Support
Psychological support should be provided to the patient, family members and the
community. The psychologist can also play a role in trying to convince the people off
transport to and admission into the Ebola treatment unit.
4.8 Management of Exposed Individuals
Individuals including health workers with percutaneous or mucocutaneous exposure to
blood, body fluids, secretions, or excretions from a patient with suspected EVD should
immediately wash the affected skin surfaces with soap and water. Mucous membranes (e.g.
conjunctiva) should be irrigated with copious amounts of water or eyewash solution.
Exposed persons should be medically evaluated and receive follow‐up care, including fever
monitoring, twice daily for 21 days after exposure. In case of temperature above 38.3°C (101
°F), hospitalize immediately in strict isolation. The incubation period between exposure and
clinical symptoms is a minimum of 48 hours.
Health workers suspected of being infected should be isolated and the same
recommendations outlined in this document must be applied until a negative diagnosis is
confirmed. Contact tracing and follow‐up of family, friends, co‐workers, and other patients

32 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
who may have been exposed to a VHF virus through close contact with the infected health
workers is essential

33 | E V D I n t e r i m G u i d e l i n e , E P H I S e p t 2 0 1 4
IV. INFECTION PREVENTION AND CONTROL
1. General Patient Care
Strengthen and carefully apply standard precautions when providing care to all patients
regardless of the signs and symptoms they present with. This is especially important because the
initial manifestations of EVD may be non‐specific. Hand hygiene is the most important measure.
Gloves should be worn for any contact with blood or body fluid. Medical mask and goggles or
face shield should be used if there is any potential for splashes of blood or body fluids to the face,
and cleaning of contaminated surfaces is paramount.
2. Disinfection in Ebola Treatment Units
The Ebola virus is considered to be fragile and can be destroyed by applying the following
methods:
Disinfection: Through the use of chlorine solution (strength of 0.5% or 0.05% depending on
the purpose) in accordance with the procedures indicated in this guideline.
Alcohol based hand rub
Heat: Through medical waste incineration, sterilization by autoclave or burning.
UV rays: Through the direct exposure to sunlight.
Strict application of universal precautions: Through good hand hygiene by regularly washing
with soap and water.
Change cleaning solutions and refresh equipment frequently while being used during the day, as
they will get contaminated quickly (follow your hospital protocols if available). For preparing
chlorine‐based solutions, see instructions in Annex 6.
3. Patient Placement, Staff Allocation, Visitors
Put suspected or confirmed cases in isolation rooms with an adjoining dedicated toilet, shower,
sink equipped with running water, soap and single‐use towels, alcohol‐based hand rub
dispensers, stocks of medicines, good ventilation, screened windows, doors closed and
restricted access.
if isolation rooms are unavailable, cohort these patients in specific confined areas while
rigorously keeping suspected and confirmed cases separate and ensure the items listed here
for isolation rooms are readily available. Make sure that there is at least 1 meter distance
between patient beds.
Ensure that clinical and non‐clinical personnel are assigned exclusively to EVD patient
care areas and that members of staff do not move freely between the isolation areas
and other clinical areas during the outbreak.
Restrict all non‐essential staff from patient care areas.
Stopping visitor access to the patient is preferred, but if this is not possible, limit their
number to include only those necessary for the patient's well‐being and care, such as
a child's parent.

Do not allow other visitors to enter the isolation rooms/areas and ensure that any
visitors wishing to observe the patient do so from an adequate distance
(approximately 15 m).
Before allowing visitors to EVD patients to enter, screen them for signs and
symptoms of Ebola.
4. Personal Protective Equipment, Hand Hygiene and Other Precautions
4.1 Personal Protective Equipment Protocols
Personal Protective Equipments (PPEs) includes impermeable coveralls or gown, examination
gloves, heavy duty/rubber gloves, head covers, shoe covers, aprons, closed shoes or boots,
facemasks, goggle and face shields. The type of PPEs to be worn depends on the activity we
are handling. However, if one enters to the high risk zone, he/she should wear complete
PPEs.
Gloves (non‐sterile examination gloves) to protect hands.
A disposable, impermeable coveralls or gown to cover clothing and exposed skin.
A surgical mask for mouth and nose protections
Goggles or face shield for eye protection.
Rubber boots (closed, puncture and fluid resistant shoes) to avoid contamination
with blood or other body fluids or accidents with misplaced, contaminated sharp
objects.
Shoe covers to protect the soles of the shoes from dirt that might stick to.
Wear water proof apron when undertaking any strenuous activity (e.g. carrying a
patient) or tasks in which contact with blood and body fluids is anticipated (e.g., the
patient has symptoms like diarrhoea, bleeding or vomiting and/or the environment
could be contaminated with blood or body fluids).
Wear a respirator (FFP2 or EN certified equivalent or US NIOSH‐certified N95), if any
procedures that stimulate coughing or promote the generation of aerosols (e.g.,
aerosolized or nebulised medication administration, diagnostic sputum induction,
bronchoscopy, airway suctioning, endotracheal intubation, positive pressure
ventilation via face mask) is planned to be performed. Avoid aerosol‐generating
procedures if possible.
Do not recycle any single‐use disposable PPE. Carefully clean and decontaminate reusable
equipment.
Dressing and Undressing Protocols of PPE at Ebola Treatment Units
1. Dressing Protocol
Dressing Protocol for Entering Low–Risk Zone from No‐Risk Zone
1. Go to the dressing room in No‐Risk Zone
2. Remove street shoes and street clothes (your own shoes and clothes).

3. Put on scrub suit and your personal rubber boots. Tuck scrub suit into boots.
4. Wash your hands with soap and water or alcohol swab.
5. Put on one pair of disposable gloves.
6. Bath your foot with chlorine.
7. Go into the Low‐Risk Zone.
For those working in the laundry area at the low risk zone follow the following additional
steps
8. Disinfect gloved hands with 0.5% chlorine.
9. Put on face mask 10. Put on goggle 11. Put on heavy duty gloves 12. Put on heavy duty apron
13. Disinfect gloved hands with 0.5% chlorine.
Dressing Protocol for Entering High–Risk Zone from Low Risk‐Zone
1. Go to a dressing room in the Low‐Risk area (dressing room no 2)
2. Disinfect the gloved hand with 0.5% chlorine.
3. Put on the cover‐all (make sure the sleeves are under the 1st layer of glove and put
on a plaster on top of it)
4. Put on the foot cover (if available).
5. Put on a second layer of gloves*1 (should be done after the goggles or face shield
if using heavy duty gloves).
6. Put on the face mask.
7. Put on the hood of coverall (if the coverall do not have hood, put on head cover).
8. Put on goggles or face shield (which ever available)
9. Put on waterproof apron (if you expect exposure with body fluids)
10. Bath your feet in chlorine solution
11. Disinfect the gloved hand with 0.5% chlorine.
12. Go into the high‐risk zone.
NOTE:
In every steps of dressing someone should monitor you to ensure that the dressing is properly done
2. Undressing Protocol
When Leaving High–Risk Zone to Low–Risk Zone
1. Disinfect gloved hands with 0.5% chlorine solution before entering undressing
room
2. Bath your feet in chlorine solution.
3. Enter the undressing room.
4. Peel off disposable apron and dispose safely (throw away in a bio‐hazard plastic
bag).
5. If the apron is to be reused, immerse the apron in the container of 0.5% chlorine solution and after that in the second container 0.05% chlorine solution and hang it close to the second footbath.
1 Always change 2nd layer of gloves when moving from one patient to another while caring. Wash your gloved hand with 0.5% chlorine or alcohol hand rub of the gloved hand before putting on new 2nd layer gloves.

6. Remove the shoe cover (if there is any)
7. Disinfect the outer pair of gloves with 0.5% chlorine solution and remove them.
A. If using surgical gloves: throw away in the waste bin.
B. If using heavy‐duty gloves: place in the bucket containing 0, 05% chlorine solution.
8. Disinfect gloved hands with 0.5% chlorine.
9. Remove goggles, disinfect with 0.5% and rinse with clean water.
10. Hang it close to the second footbath, next to the apron.
11. Disinfect the gloved hands with 0.5%.
12. Remove hood of the coverall (if a separate head cover is used, remove and throw
away in the waste bin).
13. Disinfect gloved hands with 0.5%.
14. Remove coverall and throw away in waste bin.
15. Disinfect gloved hands with 0.5%.
16. Remove mask and throw away in waste bin
17. Disinfect gloved hands with 0.5%.
18. Take goggles and apron with you.
19. Step in the second footbath.
20. Now you are in the Low‐risk area
21. Hang the goggle and the apron.
22. Remove the inner layer gloves and throw away in the waste bin.
23. Wash your hands with 0.05% or use alcohol hand rub.
24. Put a new pair of examination gloves.
When Leaving Low–Risk Zone to No–Risk Zone
1. Proceed to undressing room ‐ changing room 1.
2. Before entering the room, wash gloved hand with 0.5% chlorine.
3. Bath your feet in 0.5% chlorine solution and have boots sprayed.
4. Remove boots using boot remover and put on slipper.
5. Remove gloves and dispose into waste bin.
6. Remove scrub suit and place in collection container for disinfection and washing.
7. Put on street shoes and street clothes (your own clothes and shoes).
8. Wash your hands with soap and water or use alcohol hand‐rub or wash with 0.05%
Chlorine solution.
9. Spray soles of street shoes with 0.5% chlorine solution when exiting the changing
room.
10. If shower facility is available, you can take body shower.
NOTE:
For staff wearing heavy duty gloves, before entering in to changing room 1, remove and immerse the heavy
duty glove in 0.5% chlorine solution and put in the designated area and follow the above steps.
4.2 Hand Hygiene Protocol
Carefully apply the following precautions to avoid any possible unprotected direct contact with
blood and body fluids when providing care to any patient with Ebola, including suspected
cases.
Perform hand hygiene:
before donning gloves and wearing PPE on entry to the isolation room/area,
before any clean/aseptic procedures being performed on a patient,
after any exposure risk or actual exposure with the patient's blood and body fluids,
After touching (even potentially) contaminated surfaces/items/equipment in the
patient's surroundings, and after removal of PPE, upon leaving the care area.
Hand hygiene should be performed within the isolation rooms/areas every time it is needed
according to the above indications during care to a patient, along with change of gloves.
When caring for patients in the same room, it is essential to organize the complete care to each
patient before moving to the next and to perform hand hygiene between touching the patients.
Furthermore, neglecting to perform hand hygiene after removing PPE will reduce or negate any
benefits of the protective equipment. To perform hand hygiene, use chlorine 0.05%, an alcohol‐
based hand rub or soap and running water applying the correct technique recommended by
WHO (Annex 13 and 14).
Always perform hand hygiene with soap and running water when hands are visibly soiled.
Alcohol‐based hand rubs should be made available at every point of care (at the entrance and
within the isolation rooms/areas) and are the standard of care. However, if alcohol‐based hand
rubs are unavailable, perform hand hygiene with soap and running water every time necessary
according to the above indications. If clean water supply is not available, use 0.05% Chlorine
solution for hand hygiene.
4.3 Injection Safety
Each patient should have exclusively dedicated injection and parenteral medication
equipment which should be disposed of at the point of care. Syringes, needles or
similar equipment should never be reused.
Limit the use of needles and other sharp objects as much as possible.
Limit the use of phlebotomy and laboratory testing to the minimum necessary for
essential diagnostic evaluation and patient care.9
If the use of sharp objects cannot be avoided, ensure the following precautions are
observed:
Never replace the cap on a used needle.
Never direct the point of a used needle towards any part of the body.
Do not remove used needles from disposable syringes by hand, and do not bend,
break or otherwise manipulate used needles by hand.
Dispose of syringes, needles, scalpel blades and other sharp objects in
appropriate, puncture‐resistant containers.

Ensure that puncture‐resistant containers for sharps objects are placed as close as
possible to the immediate area where the objects are being used ('point of use') to
limit the distance between use and disposal, and ensure the containers remain
upright at all times. If the sharps container is far, never carry sharps in your hand but
place them all in a kidney dish or similar to carry to the sharps container.
Ensure that the puncture‐resistant containers are securely sealed with a lid and
replaced when 3/4 full.
Ensure the containers are placed in an area that is not easily accessible by visitors,
particularly children (e.g. containers should not be placed on floors, or on the lower
shelves of trolleys in areas where children might gain access).
4.4 Environmental Cleaning
Wear heavy duty/rubber gloves, impermeable gown and boots when cleaning the
environment and handling infectious waste.
In addition, wear facial protection (mask and goggle or face shield) and overshoes if
boots are unavailable, when undertaking cleaning activities with increased risk of
splashes or in which contact with blood and body fluids is anticipated (e.g., cleaning
surfaces heavily soiled with vomit or blood or cleaning areas closer than 1 meter from
a patient with symptoms like diarrhoea, bleeding or vomiting, etc.).
Clean floors and horizontal work surfaces at least once a day with clean water and
detergent. Cleaning with a moistened cloth helps to avoid contaminating the air and
other surfaces with air‐borne particles. Allow surfaces to dry naturally before using
them again.
Dry sweeping with a broom should never be done. Rags holding dust should not be
shaken out and surfaces should not be cleaned with dry rags.
Cleaning should always be carried out from "clean" areas to "dirty" areas, in order to
avoid contaminant transfer.
Do not spray (i.e. fog) occupied or unoccupied clinical areas with disinfectant. This is a
potentially dangerous practice that has no proven disease control benefit.
Procedures for cleaning surfaces or objects contaminated with blood, other body fluids:
Environmental surfaces or objects contaminated with blood, other body fluids,
secretions or excretions should be cleaned and disinfected as soon as possible using
standard hospital detergents/disinfectants (e.g. a 0.5% chlorine solution or a solution
containing 1000 ppm available free chlorine).
Decontaminate the area with 0.5% Chlorine solution for 20 minutes and then remove
the fluid and discard it to the toilet.
Disinfected as soon as possible with 0.5% chlorine solution.

Cleaning floors and horizontal work surfaces:
Clean floors and horizontal work surfaces at least once a day with clean water and
detergent.
Start cleaning from “clean” areas and end to “dirty” areas
Always use a moistened cloth to avoid contaminating the air and other surfaces with
air‐borne particles.
Allow surfaces to dry naturally before using them again.
2.5 Management of Linen and Blankets
Linen and blankets that has been used on patients can be heavily contaminated with body
fluids (e.g. blood, vomit) and splashes may result during handling. Wear complete PPE
(impermeable gown, heavy duty/rubber gloves, boots, facial mask and goggle or face shield),
when handling them.
Soiled linen or blankets should be placed in clearly‐labeled, leak‐proof bags or buckets
at the site of use and the container surfaces should be disinfected before removal
from the isolation room/area. If there is any solid excrement such as faeces or vomit,
scrap off carefully using a flat firm object and flush it down the toilet or in the sluice
before linen or blankets is placed in its container. If the linen or blankets is
transported out of the patient room/area for this procedure it should be put in a
separate container ‐ it should never be carried against the body.
Linen or blankets should be then transported directly to the laundry area in its
container and laundered promptly.
For low‐temperature laundering, wash linen or blankets with detergent and water,
rinse and then soak in 0.05% chlorine for approximately 30 minutes. Linen or blankets
should then be dried according to routine standards and procedures.
Washing contaminated linen or blankets by hand should be discouraged. However, if
washing machines are not available or power is not ensured, take the soiled linen or
blankets out of the container and empty it into a large drum container of hot water
and soap. Soak the linen or blankets in this drum and make sure it is totally covered
with water. Use a stick to stir; then throw out the water and refill the drum with clean
water and add bleach 1000 ppm and allow to soak for 10‐15 minutes. Remove the
linen or blankets and then rinse in clean water. Remove excess water and spread out
to dry. Avoid as much splashing as possible.
If safe cleaning and disinfection of heavily soiled linen or blankets is not possible or
reliable, burn the linen to avoid any unnecessary risks to individuals handling these
items.

5. Waste Management
Wear complete PPE (impermeable gown, heavy duty/rubber gloves, boots, facial mask and
goggle or face shield), when handling infectious waste. Goggles provide greater protection
than face shields from splashes that may come from below when pouring liquid waste from a
bucket. Avoid splashing when disposing of liquid infectious waste.
Waste should be segregated at point of generation to enable appropriate and safe handling.
For details refer to annex 9.
Sharps waste disposal:
Sharp objects (e.g. needles, syringes, glass articles, scalpel blades, cannulas and other
sharps) and tubing that has been in contact with blood or body fluids should be
placed inside puncture resistant waste containers.
These items should be located as close as practical to the patient care area where the
items are used, similarly in laboratories.
Disinfect the outside of the sharps box before transporting. Fill inside of the box with
0.5% chlorine solution before disposal to sharp pit.
Solid medical waste:
All used disposable PPE, non‐sharps and other infectious waste needs to be collected
in leak proof hazard waste bags and placed in covered waste bins.
collect waste bags when it ¾ full and close with a string ,
Pouring 0.5% chlorine solution on top of the waste bags prior to being securely sealed
as pre‐treatment disinfection is recommended. The procedure can create back‐splash,
so care should be taken to protect eyes.
Put new double bags in the bin immediately.
Put bags in a garbage‐bag‐holder or covered bins
Transport garbage bag holder or covered bins using trolley or wheelbarrow (bins
should never be carried against the body)
Put waste bags in a designated pit of appropriate depth (e.g. 2 m)
Disinfect the bins with 0.5% chlorine solution
After each waste load, the waste should be covered with a layer of soil 10 –15 cm
deep.
Waste should be placed in the pit up to the depth of 1.5 m. before totally covered and
sealed.
Burning waste in the pit or an incinerator may be used for short periods during an
outbreak to destroy solid waste.

The area designated for the final treatment and disposal of waste should have
controlled access to prevent entry by animals, untrained personnel or children.
Liquid waste:
All biological infectious liquid waste (i.e. faeces, vomit, urine, etc...) is to be disposed
of in patient latrines and disinfected by pouring 0.5% chlorine solution.
Controlled spills:
Collect the waste in a bucket with 2cm of 0.5% chlorine solution
When waste has been excreted, add enough 0.5% solution to cover
completely the waste
Allow minimum of 15 minutes for chlorine to act
Dispose into a special liquid waste pit or into a pit latrine.
Uncontrolled spills:
First rule: reduce the risk of uncontrolled splashes and spills
Pour 0.5% solutions directly on the spills without splashing
Leave for 15 minutes
Mop up with an absorptive pad or towel
Place the waste into the bucket
The soaked pads should be disposed of into a pit latrine, or into the waste pit
Washing the room
If vomit or excreta are on the bed or on the floor, pour one cup of 0.5% chlorine
solution over it.
Leave it for at least 15 minutes and then mop up with the absorbent pad (green
plastic side up).
The mattress must be covered with the plastic sheeting provided. The sheeting can
then be washed with an absorbent pad soaked with 0.5% chlorine solution.
Organic waste:
Organic waste originating from the human body introduces a huge biohazard and
must be disposed of immediately.
Organic waste can be collected in a double plastic bag supported by a garbage‐bag
holder. Close the bags with a string or tape. Disinfect the outside of the bag.
Organic waste can be disposed of in a specially built organic waste pit. If such a pit is
not available, dispose of into a pit latrine.
Patient’s clothes: move to discharge
Clothes from patients need laundered routinely while in the treatment unit. But upon
death or discharge the clothes should be burned and replaced for discharges.
Laundering in High risk area:
Patients blankets and bed sheets should be washed in high risk area
Wash confirmed, probable and confirmed cases blanket and bed sheets separatly
Label blankets and bed sheets to match the room and bed numbers. Linen and
blanket #1 always be used by bed #1,

Household waste:
All used household outreach kit material (i.e. gloves, masks, surgical gowns etc...) is
to be collected and contained in a waste bag. 0.5% chlorine solution is to be poured
over the top before being sealed.
The outside of the bag is to be sprayed with 0.5% chlorine solution prior disposal
through burning.
6. Moving and Burial of Human Body
The coordinator should be consulted for any decision making on movement and burial of
human body. The handling of human remains should be kept to a minimum.
The community should not spray, wash or wrap up dead body. Any practice of washing the
body in preparation of "clean burials" should be discouraged. Only trained personnel should
handle body during the outbreak.
The burial team should follow the procedures below in principle, but may need some
adaptation to take account of cultural and religious concerns:
6.1 Burial Procedure for Patient Dying in the Ebola Treatment Unit:
Tasks of Ebola treatment unit staff:
Prepare the body and transport to mortuary or hand‐over to the burial team
Following a death of a patient, the nurse in charge covers the body with a blanket.
The nurses put a screen around the bed of the deceased patient and call the burial
team to enter the High‐risk area.
Mobile patients in the ward should leave the ward temporary.
2‐3 people from the burial team and 2‐3 people from the cleaning team enter in full
protective clothing.
Body, blanket and clothes will be sprayed with 0.5% chlorine solution.
Write the name of the deceased person on the outside of the body bag with a
waterproof marker.
Spray the body bag inside.
The body will be wrapped in the blanket and placed with personal clothing in the
body bag.
Spray again inside the body bag, close the body bag securely (zip closed to the face of
the patient) and spray outside the body bag.
Place body bag on stretcher and transport body to the mortuary in the Ebola unit.
Transport of the body out of the mortuary and out of the Ebola treatment unit:
Walk to the morgue and put the prepared body in the body bag on a stretcher.
Carry the stretcher outside the mortuary and the Ebola treatment unit via the special
exit for corpses.
The coffin should be placed at the special exit for corpses and the burial car/pick up
should be parked close to it.

Ask the family if they want to see the face of the deceased person. If they want to see
it, open the body bag and show the face.
Then close the body bag.
If a coffin is used:
Spray the coffin inside with 0.5% chlorine solution.
Put the body in the coffin, close securely and spray outside.
If no coffin is used:
The body will need to be put in 2 body bags.
The second body bag needs to be sprayed inside, and then place the first body bag
with the body inside the second body bag.
Close the second body bag and spray the outside of the second body bag.
After the body is put in the coffin or second body bag:
Spray the stretcher thoroughly.
The Ebola treatment unit team will return dressed to the Ebola ward and the Burial
team will continue the safe burial procedures.
PPE is not required for individuals driving or riding a vehicle to collect human remains,
provided that drivers or riders will not be handling a dead body of a suspected or
confirmed case of EVD.
Burial Team:
The team needs to consist of a driver, 3 people and 1 supervisor (to lower a coffin you need to be minimum 4 persons) The driver’s responsibility is only to transport the team. Not involved on the activity of the burial team.
Tasks of the Burial team staff:
Transport of the body to the gravesite and burry the deceased.
Dressing:
Burial team wears coverall, examination gloves, heavy‐duty gloves and face mask.
Steps to take dead body from morgue on to the pick‐up car
Spray the place where the Ebola unit team walked outside the Ebola unit with a 0.5%
chlorine solution.
Place prepared (coffined or the body prepared in 2 body bags) body at the back of
the pickup and transport to gravesite.
Steps of Burial at the gravesite
Place ropes on ground at two or three intervals (knee, lower back, upper back) to use
to lower coffin into grave, and place coffin on top of the ropes. Latex protection
gloves need to be used when lowering the coffin.
Burial team lower coffin using the ropes into the grave.
Community members may help to lower the coffin and will fill the grave with earth.

Community members required examination gloves and latex protection gloves when
lowering the body.
Back of the pickup needs to be sprayed with 0.5% chlorine solution.
6.2 Procedure for Burial of Suspect/Probable/Confirmed Patient Dying at Home
Before giving protective materials, the supervisor of burial team should enter the
family compound to speak with the responsible person in family.
Explain the burial procedure and provide information on EVD transmission.
Explain why the body must be buried safely and explain the procedure for
disinfection of the body.
Ensure coffin (if used) and grave is prepared (2 meters deep).
Put on fully protective clothing (PPE). (Minimum 2 people.)
Follow procedures for preparation of the body and the use of body bags and/or
coffin.
Preparation of body
Spray the body and the area around body with 0.5% chlorine.
Spray sheet and/or blanket thoroughly with chlorine solution.
Wrap body in blanket and cover completely.
Open body bag and place body and personal clothing inside.
Close body bag securely.
Spray outside of body bag with 0.5% chlorine.
Put in coffin or second body bag as described before.
After removing the body from the house, disinfect the room in which the patient died
as well as the patient’s mattress.
Burn the mattress.
Undress the PPE in front of the community. (If situation allows!)
Put on examination gloves,
Proceed to the gravesite, put latex protection gloves when carrying the coffin to the
grave and lower the coffin/body in double bags as described before.
A Solidarity Kit needs to be provided.
6.3 Cleaning a Room after Patient Death at Ward
Cleaners remove the mattress for spraying with 0.5% chlorine solution and dry in the
sun or burn in case of heavy contamination. (Dirty mattress can be folded and tied
with some strings or cloths.
All remaining clothes and blankets are put in a plastic bag.
Mattress and bags are sprayed with 0.5% solution before transport.
Inform the waste burner that the material must be burned.
Cleaners collect all material used by the patient.
All plastic cups, cutlery, plates; buckets are washed with 0.05% solution and can be
reused by other patients or can be burned.
The bed, window, walls, and the whole floor are disinfected with 0.5% chlorine
solution by pouring with a cup or by spraying.
Put new/clean mattress on the bed.

Remove screen from the bed.
Cleaners remove all cleaning material.
When leaving cleaners and the burial team members thoroughly disinfect aprons,
boots, and gloved hands with 0.5% chlorine solution.
Inform the Nurse in Charge that the ward has been cleaned.
6.4 Procedure for house disinfection
House disinfection must be carried out in a sensitive manner. The process results in the destruction of some of the family’s belongings, and damage to other items may also occur. Clearly explain the procedure to the family, and obtain their agreement. Explain that a Solidarity Kit will be provided to replace the items destroyed.
People Participating
One family member (if they want): he/she must be dressed in full protective clothing
Disinfection team: supervisor, 2 sprayers.
People dressing up
Maximum 4 people will need to dress up and full PPE material should be taken for 5
people
2 sprayers, 1 supervisor, 1 family member and 1 extra PPE should always be taken.
Procedures
After the patient has left the room, the supervisor enters and assesses the area. If the
sprayers are experienced, the supervisor will not need to dress up and can supervise
from outside the house.
The 2 sprayers need to be dressed in PPE and should take 1 spraying machine.
One spraying person should spray everything and the other person should pick up the
clothes, blankets and mattress that need to be sprayed and put it outside to be
sprayed.
A family member may participate if wanted, and need to be fully dressed.
Disinfect by spraying 0.5% chlorine solution:
o General area where the patient was accommodated during his sickness.
o Reusable hard items, such as buckets, furniture, etc. and after the spraying
the family can clean the items with soap and water.
o Bed, windows, walls and the whole floor.
o Latrine.
o Mattress and let dry in the sun. (If not too contaminated or soiled.)
Disinfect by spraying 0.05% chlorine solution (solution to be prepared on the spot in a
basin or bucket provided by family):
o Bedding and clothing (but if very dirty need to be burned!); after disinfection
it can be washed with water and soap and then dried in the sun by the family
members.
o Eating utensils like plates, spoons, cups; after disinfection it can be cleaned
with water and soap by the family members.
In case of heavy contamination:
o Remove mattress, bedding, and clothing for burning.

o Dirty mattress can be folded and tied with some strings or cloths.
o Material to be burnt should be bagged or wrapped in plastic sheeting and
transported to the waste zone at the Marburg/Ebola unit for disposal.
Backfill any waste pits that have been used.
7. Managing Exposure to Virus
Persons including HCWs with percutaneous or muco‐cutaneous exposure to blood,
body fluids, secretions, or excretions from a patient with suspected or confirmed HF
should immediately and safely stop any current tasks, leave the patient care area, and
safely remove PPE.
Remove PPE carefully according to the steps indicated in this document because
exposure during PPE removal can be just as dangerous for nosocomial transmission
of EVD. Immediately after leaving the patient care area, wash the affected skin
surfaces or the percutaneous injury site with soap and water. Accordingly, irrigate
mucous membranes (e.g. conjunctiva) with copious amounts of water or an eyewash
solution, and not with chlorine solutions or other disinfectants.
Immediately report the incident to the local coordinator. This is a time‐sensitive task
and should be performed as soon as the HCW leaves the patient care unit.
Exposed persons should be medically evaluated including for other potential
exposures (e.g., HIV, HCV) and receive follow‐up care, including fever monitoring,
twice daily for 21 days after the incident. Immediate consultation with an expert in
infectious diseases is recommended for any exposed person who develops fever
within 21 days of exposure.
HCWs suspected of being infected should be cared for/isolated, and the same
recommendations outlined in this document must be applied until a negative
diagnosis is confirmed.
Contact tracing and follow‐up of family, friends, co‐workers and other patients, who
may have been exposed to Ebola virus through close contact with the infected HCW
is essential.

V. COMMUNICATION AND SOCIAL MOBILIZATION
1. Overview
Risk communication is about communicating potential risks of a disease outbreak on how to
bring the level of anxiety down and minimize consequent morbidity and mortality.
Like other diseases of international concern, Ebola Viral Disease causes huge level of fear and
anxiety that may lead to irrational thinking and inappropriate actions adding fuel to the
propagation of the disease further.
Due to rampant existence of sources of information, confusions and rumours evolve; mistrust
with regard to what is being undertaken may result. This leads to irrational thinking and
inappropriate actions which further add to the propagation of the disease outbreak.
The way people behave, what they do or do not do as informed has a tremendous impact on
outbreak control. Listening to understand the perception of the people about the disease,
analyze problem behaviors and use of epidemiological information is crucial. Therefore
successful outbreak control eventually depends on participation of individuals, communities and
organizations taking immediate and appropriate immediate action to prevent further
transmission, potential loss of life.
Communicating about risks need to be complemented with other communication approaches to
consciously influence, promote and coordinate specific behaviours requires through sound
planning of integrated communication strategy ( Behaviour Change Communication, social
mobilization and advocacy) informed by principles risk communication: Trust, reporting timely,
transparency and listening the public.
In addition, it will be of utmost important for communicators to understand the pattern of
outbreak situation in phases to anticipate what to respond when. Two major phases; namely pre
epidemic and epidemic can be identified and used to anticipate the information needs of the
general public, the media and stakeholders. Each phase requires unique information and detail
planning including monitoring of activities to take corrective and focused actions.
2. Pre‐Epidemic Phase
This is where planning for most of the work (assessment of risks with communication elements
integrated and of existing communication situation, integrated communication planning and
message development) should be done to boost preparedness.
This is phase is characterized by search for further technical information on the disease outbreak,
basic facts, information sharing, working with stakeholders, policy guidance, mobilization of
resources and logistics, acquiring and imparting skills, etc.
The process to centralize dissemination of information through setting up of coordination
partnerships is crucial to ensure that messages2 are standardized and all involved in the control
are speaking with one voice is imperative.
Measures to inform the public about the risks in order to allay fear and anxiety begin in this
phase.
Immediate Action
Analyze or do rapid assessment to determine what existing resources and ongoing
communication interventions are available.
Establish and strengthen social mobilization coordination teams. Do partners
mapping and foster partnership towards a coordinated communication response plan
and implementation. This stage will help in mobilization of resources, experts and
standardization of messages.
Develop timely, accurate and easily understood communication messages to ensure
that trust and confidence on measures being undertaken are built by the public.
These will help avoid rumors and misinformation and eventually minimize negative
public health impacts.
In consultation with health officials, plan schedule when to release information about
the status of the outbreak situation to maintain high level of transparency with what
is going on. With the support from health experts, message plans should include the
risk level; what is unknown and known about the outbreak, incidence and the
spread, specific measures taken and others what should be taken by individuals,
families, communities, health workers, hunters, etc. Allay public anxiety through
press statement and regular updates with stakeholders and partners such as the
media.
Conduct listening exercises with the people affected, gather and compile available
profile of community culture, behavior, etc. and identify mechanisms to listen public
opinion and concerns through for example – media monitoring of radios, TV,
newspapers and public enquiry phone in lines (call centers), if there are any.
Develop IEC materials targeting the media, health care workers and the general
public
Conduct sensitisation meetings for health care workers including school health teams
and with the epidemic task forces
Conduct media orientation to update with state of preparedness, global and regional
Ebola situation and key messages
2 See key messages at the end of this document

Conduct media talks on basic facts about Ebola (definition, causes, transmission,
treatment, prevention)
Train Health Extension Workers (HEWs) and support for house to house and
community mobilization
3. Epidemic Phase
The finding of a case or cases may create confusions and heighten looking for further
information. It is essential to get facts from reliable source. In other words, through media
monitoring and other means, it is important to gather information, verify this in consultation with
the technical team and provide factual information from the designated source for such task
(FMoH). The response to be given will determine reputation.
One of the best ways at this stage is to show empathy in the communication messages to be
delivered and inform the public the level of risk and plans for containment. Messages should also
focus on allaying anxiety and advise the public the right means of self‐protection, prevention and
collaborating with partners. In as much as possible, even when there is little and incomplete
information, it is better to communicate and explain that more information will be shared as time
goes depending ongoing investigation.
At this stage of epidemic, messages focusing on specific actions and behaviors to prevent spread
protect and measures targeting the public and specific groups need to be widely promoted and
disseminated.
Demand for factual information from the public and the media will be intense. It is important to
head on and fill in the gaps swiftly before rumors and misinformation circulates.
4. Integrated Communication Activities
National / Regional
Continue releasing updates regularly to the public, the media and stakeholders
Hold regular meetings of social mobilization team at all levels to continually monitor
situation, update messages and support implementation
Hold advocacy meetings with different stakeholders at all levels for their support and
contribution to adapting control measures within the community settings and to
identify potential barriers and solutions.
Strengthen multi ‐ sectoral involvement (Education, transportation, immigration, etc.)
for information sharing and promote control measures in respective sector settings
Promote psychosocial assistance and support activities for people affected and their
families
Disseminate IEC materials and messages

Organize and or make use of events to integrate or share information and raise
awareness
Media communications
The media is the most powerful communication network with the capacity to
disseminate outbreak information quickly, reach wider population, hard to reach
areas and everyone through creating discussions. It is important to make use of and
strengthen media communication:
Establish strong link and mechanism to ensure that timely and accurate information
is shared rapidly between the media and technical and social mobilization team
Continue media monitoring to dispel rumours and misinformation and communicate
information and stories that explain outbreak control measures
Share with the Media up‐to‐date information through press releases, regular
meetings and other means of communication
In Health‐Care Facilities
Strengthen health facility based education through provision of guidelines and
promotional materials
Ensure that information concerning the patient is communicated to the family
To the extent possible, facilitate safe family visits to the patient.
Encourage health facility based education
In the Community
Train Health Extension Workers, Health development Army, Volunteers, etc to
conduct intensive community dialogue on the control measures
Provide / disseminate promotional materials – posters, brochures – radio messages,
public meetings)
Understand the views of the population from their sociocultural perspective and
respond to their needs and concerns accordingly
Engage people affected or those in high‐risk occupations (health care workers,
nursing staff, persons conducting burials, traditional healers, hunters, wildlife
officers, ecologists, veterinarians, etc.)
Encourage community compliance with the recommended outbreak control
measures
Strengthen the capacity of HEWs:
o To promote the implementation of standard precautions when caring for sick
people in the home and when handling and disposing of dead animals found in
the forest,
o To promote community participation in epidemiological surveillance at the
community level (reporting, alert)
Promote the organization of safe burials by specialized teams under the supervision
of the medical team, respecting funeral ceremonies
Encourage the community to report Ebola Viral Disease to see a health care worker
(surveillance team) without delay.
Correct myths through providing responses that are both accurate and that resonate
with the community
In collaboration with opinion leaders, make use of events to integrate awareness‐
raising activities
Mobilize all relevant community structures to promote compliance with prevention
programmes and programmes to contain transmission of the disease
5. Key Messages
Ebola is a highly contagious and deadly disease which currently has no cure
Any person is susceptible to Ebola, if they come in contact with the Ebola Virus
There is neither vaccination nor treatment ‐ prevention is currently the only way to
remain free from Ebola.
If you discover or identify a suspected person with signs and symptoms and travel
history to Ebola affected countries, report immediately to health workers Or call a toll
free number 8335, EPHI staff will contact you.
Communicatei “What Ebola is, what causes it, mode of transmission, management,
prevention and means self‐protection when caring persons suspected of disease”.
Please look for the complete set of messages.
i What is Ebola Virus Disease (EVD)?
Ebola is a severe, often fatal illness in humans and animals such as monkeys, gorillas,
chimpanzees and fruit bats which is caused by infection with Ebola virus
EVD outbreaks occur primarily in remote villages in Central and West Africa, near
tropical rainforests
It is very infectious, and kills in a short time, but can be prevented.
How does it Spread?
The natural reservoir of the virus is unknown, but it is believed that Ebola is
introduced into the human population by infected animals.
Ebola spreads from exposure to Ebola virus through direct contact with the blood
and body fluids (such as saliva, urine, stool, sweat, etc.) of an infected person.
Families and friends, or any person can get the disease when they come in close
contact with such body fluids when caring for infected persons.
Exposure to Ebola Virus occurs also from coming to contact with the dead body
especially during the burial ceremonies.
Contact with objects used by infected person such as sharps (needles, razor blades),
syringes, soiled clothing and linen.
Health workers can get Ebola Virus when they treat patients infected with the virus
without wearing proper protective cloths such as eye goggles, masks, gowns, gloves
and take no proper precautions in discarding used needles and syringes.
The time it takes to develop signs and symptoms to be clearly seen in a person is 2 ‐
21 days
Signs and Symptoms of Ebola
EVD is characterized by sudden onset of:
Fever
Headache
Joint and muscle pain
Sore throat and weakness, later followed by
Diarrhea
Vomiting and stomach pain
Red eyes, raised rash
Impaired kidney and liver function, and
In some cases internal and external bleeding occurs.
How can it be Prevented?
There is neither vaccination for prevention nor treatment. Prevention is the only choice
that we all have to focus and advise others.
What are Key messages for prevention and protection?
1. Avoid direct contact with suspected persons who have EVD signs and symptoms and
travel history from West Africa.
2. Report immediately if there is a person suspected of having signs and symptoms of
Ebola and should be taken to an Ebola designated health care facility at 8335.
3. Avoid direct contact with blood and body fluids of a person suffering from Ebola or
dead person by wearing gloves, masks, and eye goggles.
4. Avoid direct contact with bed clothes, soiled clothing and other object used by an
infected person with Ebola
5. Health workers and support staff should wear eye goggles, gowns, gloves, masks,
and boots (protective personal equipment)

6. Burial preparations must be handled by teams oriented in handling body of person
who has died of Ebola; body should be buried immediately. Getting in contact with
the dead body should be avoided at all times and during burial rituals.
7. Avoid bush meat and close contact with Monkeys and Baboons.
8. Avoid handling of dead wild animals in the bushes.
9. Port of entry workers should be aware of how to protect themselves from getting
Ebola.
10. Always get latest updates of information to protect yourself and others.
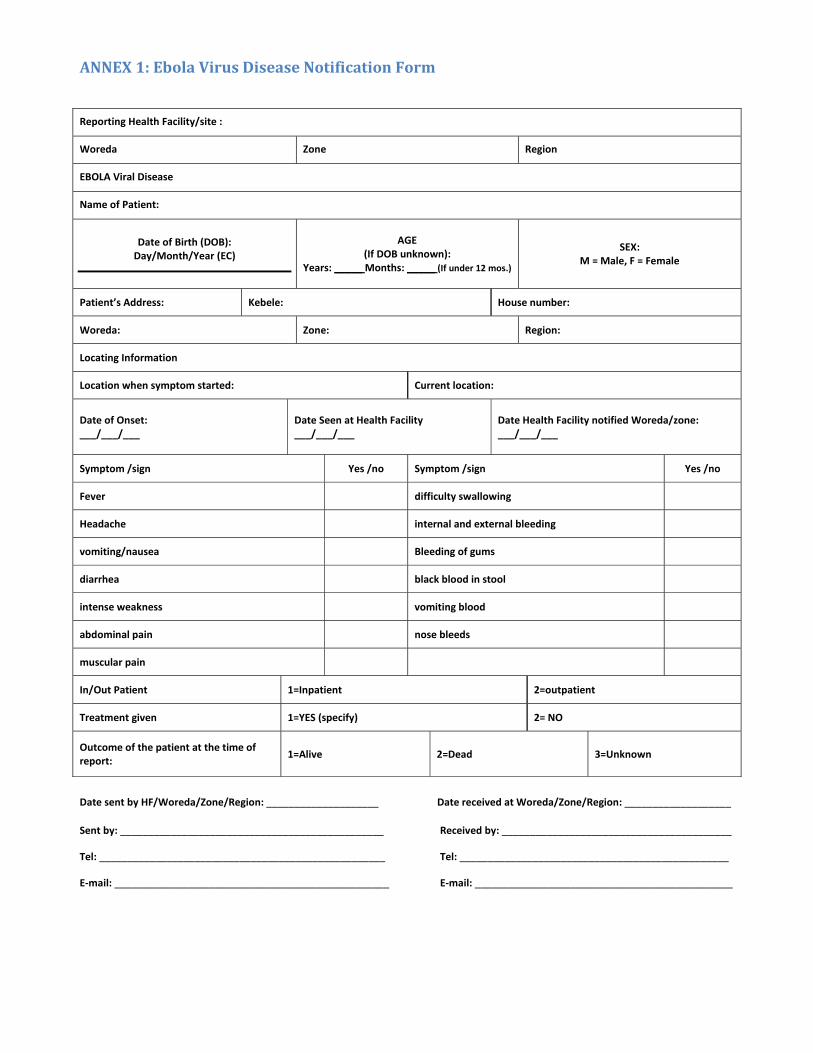
ANNEX 1: Ebola Virus Disease Notification Form
Reporting Health Facility/site :
Woreda Zone Region
EBOLA Viral Disease
Name of Patient:
Date of Birth (DOB): Day/Month/Year (EC)
AGE (If DOB unknown):
Years: _____ Months: _____ (If under 12 mos.)
SEX: M = Male, F = Female
Patient’s Address: Kebele: House number:
Woreda: Zone: Region:
Locating Information
Location when symptom started: Current location:
Date of Onset: ___/___/___
Date Seen at Health Facility ___/___/___
Date Health Facility notified Woreda/zone: ___/___/___
Symptom /sign Yes /no Symptom /sign Yes /no
Fever difficulty swallowing
Headache internal and external bleeding
vomiting/nausea Bleeding of gums
diarrhea black blood in stool
intense weakness vomiting blood
abdominal pain nose bleeds
muscular pain
In/Out Patient 1=Inpatient 2=outpatient
Treatment given 1=YES (specify) 2= NO
Outcome of the patient at the time of report:
1=Alive 2=Dead 3=Unknown
Date sent by HF/Woreda/Zone/Region: ____________________ Date received at Woreda/Zone/Region: ___________________
Sent by: _______________________________________________ Received by: _________________________________________
Tel: ___________________________________________________ Tel: ________________________________________________
E‐mail: _________________________________________________ E‐mail: ______________________________________________

ANNEX 2: Ebola Case Investigation Form 1. NOTIFICATION
1.1 DATE of case detection (DD/MM/YEAR) ______ / ______ / ______ Case ID NUMBER: ______________________________
1.2 REPORTING institution: _______________________________________________________________________________
1.3 Form FILLED in by:
Full NAME: ________________________________________________________TEL:______________________________
1.4 Information PASSED on by (FULL name):
Full NAME: ________________________________________________________TEL:______________________________
1.5 RELATIONSHIP with the patient ________________________________________________________________________
2. IDENTIFICATION
1.6 NAME of patient: ___________________________________________________________________________________
1.7 DATE of birth: ________ / ________ / ________ AGE (in years): _______________ SEX: M F
1.8 ADDRESS:
CELL PHONE number: _______________________________________________________________________________
REGION: ______________________________ DISTRICT /SUB CITY: ______________________________
1.9 NATIONALITY: _____________________________________________________________________________________
1.10 OCCUPATION: (tick the appropriate circle and provide details if necessary)
Planter Homemaker Child Hunter/Bush meat-seller
Health-care worker, specify Health-care facility: _________________________________ Qualification: _____________________________
Mine worker/Gold prospector, specify Mining facility: _______________________________________________________________________
Starting date of mining activity: _______________________________________________________
Pupil/Student Other (specify) _____________________________________________________________
3. PATIENT’s CONDITION
1.11 CONDITION of the patient when found: ALIVE DEAD
1.12 If DECEASED … DATE of death ___________ / ___________ / ___________
1.13 PLACE of death
COMMUNITY (village or neighbourhood): _________________ DISTRICT /sub city: _______________
HOSPITAL (name and department): ____________________ DISTRICT /sub city: ______________
1.14 BURIAL place
NAME of village or neighbourhood: ___________________ DISTRICT /sub city: _______________
4. Clinical HISTORY
1.15 DATE onset of SYMPTOMs ___________ / ___________ / ___________
1.16 NAME of the place where the patient became ill ___________________DISTRICT /sub city: ________________
1.17 Has the patient MOVED around since he/she became ill ? YES NO Don’t Know
If the answer is “YES”, complete the list indicating Kebele, health‐care facilities, and districts:
Kebele _________________ Health‐care facility_____________________ District ___________________
Kebele _________________ Health‐care facility_____________________ District ___________________
Kebele _________________ Health‐care facility_____________________ District ___________________
1.18 Does the patient show any of the following symptoms (tick all applicable)
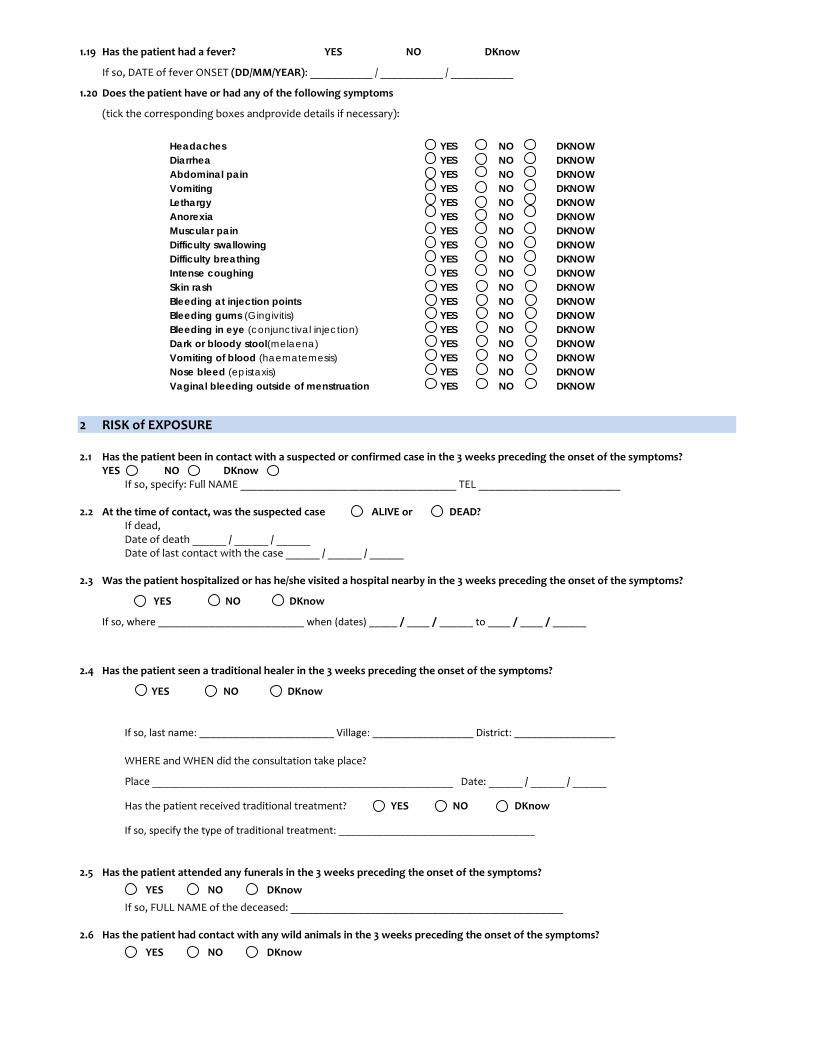
1.19 Has the patient had a fever? YES NO DKnow
If so, DATE of fever ONSET (DD/MM/YEAR): ___________ / ___________ / ___________
1.20 Does the patient have or had any of the following symptoms
(tick the corresponding boxes andprovide details if necessary):
Headaches YES NO DKNOW Diarrhea YES NO DKNOW Abdominal pain YES NO DKNOW Vomiting YES NO DKNOW Lethargy YES NO DKNOW Anorexia YES NO DKNOW Muscular pain YES NO DKNOW Difficulty swallowing YES NO DKNOW Difficulty breathing YES NO DKNOW Intense coughing YES NO DKNOW Skin rash YES NO DKNOW Bleeding at injection points YES NO DKNOW Bleeding gums (Gingivitis) YES NO DKNOW Bleeding in eye (conjunctival injection) YES NO DKNOW Dark or bloody stool(melaena) YES NO DKNOW Vomiting of blood (haematemesis) YES NO DKNOW Nose bleed (epistaxis) YES NO DKNOW Vaginal bleeding outside of menstruation YES NO DKNOW
2 RISK of EXPOSURE 2.1 Has the patient been in contact with a suspected or confirmed case in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow If so, specify: Full NAME ______________________________________ TEL _________________________
2.2 At the time of contact, was the suspected case ALIVE or DEAD?
If dead, Date of death ______ / ______ / ______ Date of last contact with the case ______ / ______ / ______
2.3 Was the patient hospitalized or has he/she visited a hospital nearby in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
If so, where __________________________ when (dates) _____ / ____ / ______ to ____ / ____ / ______
2.4 Has the patient seen a traditional healer in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
If so, last name: ________________________ Village: __________________ District: __________________
WHERE and WHEN did the consultation take place?
Place _____________________________________________________ Date: ______ / ______ / ______
Has the patient received traditional treatment? YES NO DKnow
If so, specify the type of traditional treatment: ___________________________________
2.5 Has the patient attended any funerals in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
If so, FULL NAME of the deceased: ________________________________________________
2.6 Has the patient had contact with any wild animals in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
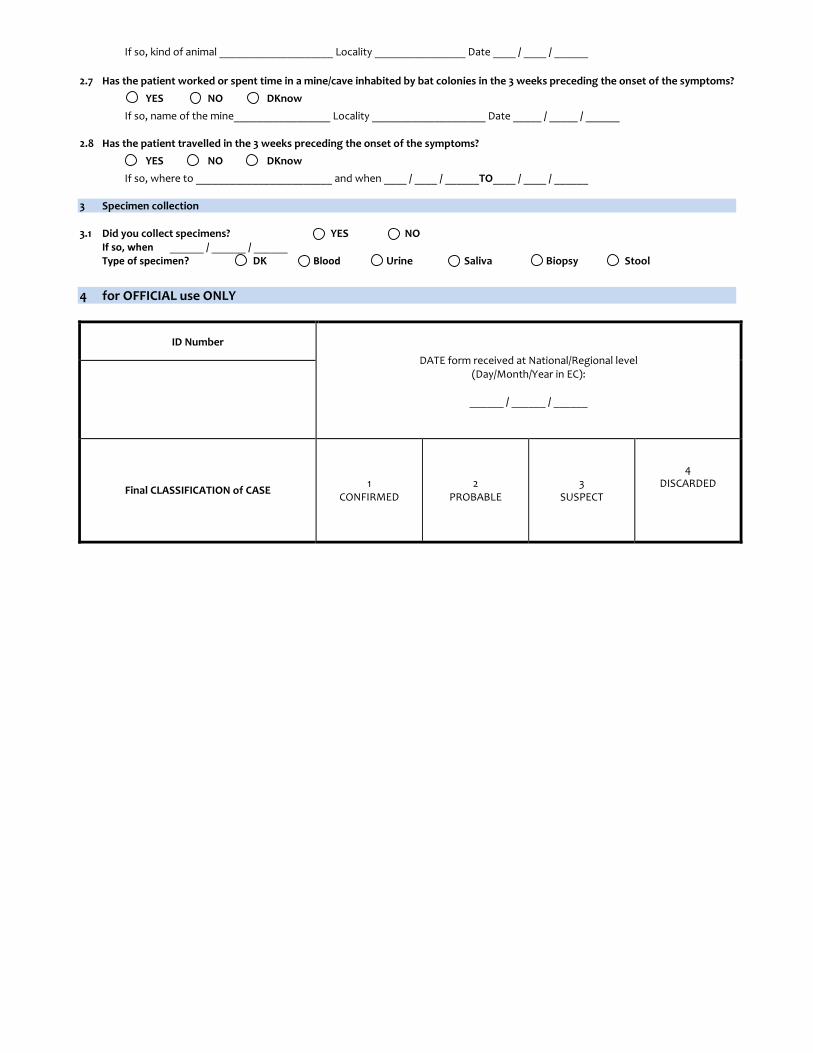
If so, kind of animal ____________________ Locality ________________ Date ____ / ____ / ______
2.7 Has the patient worked or spent time in a mine/cave inhabited by bat colonies in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
If so, name of the mine_________________ Locality ____________________ Date _____ / _____ / ______
2.8 Has the patient travelled in the 3 weeks preceding the onset of the symptoms?
YES NO DKnow
If so, where to ________________________ and when ____ / ____ / ______TO____ / ____ / ______ 3 Specimen collection 3.1 Did you collect specimens? YES NO
If so, when ______ / ______ / ______ Type of specimen? DK Blood Urine Saliva Biopsy Stool
4 for OFFICIAL use ONLY
ID Number
DATE form received at National/Regional level (Day/Month/Year in EC):
______ / ______ / ______
Final CLASSIFICATION of CASE 1
CONFIRMED 2
PROBABLE 3
SUSPECT
4 DISCARDED
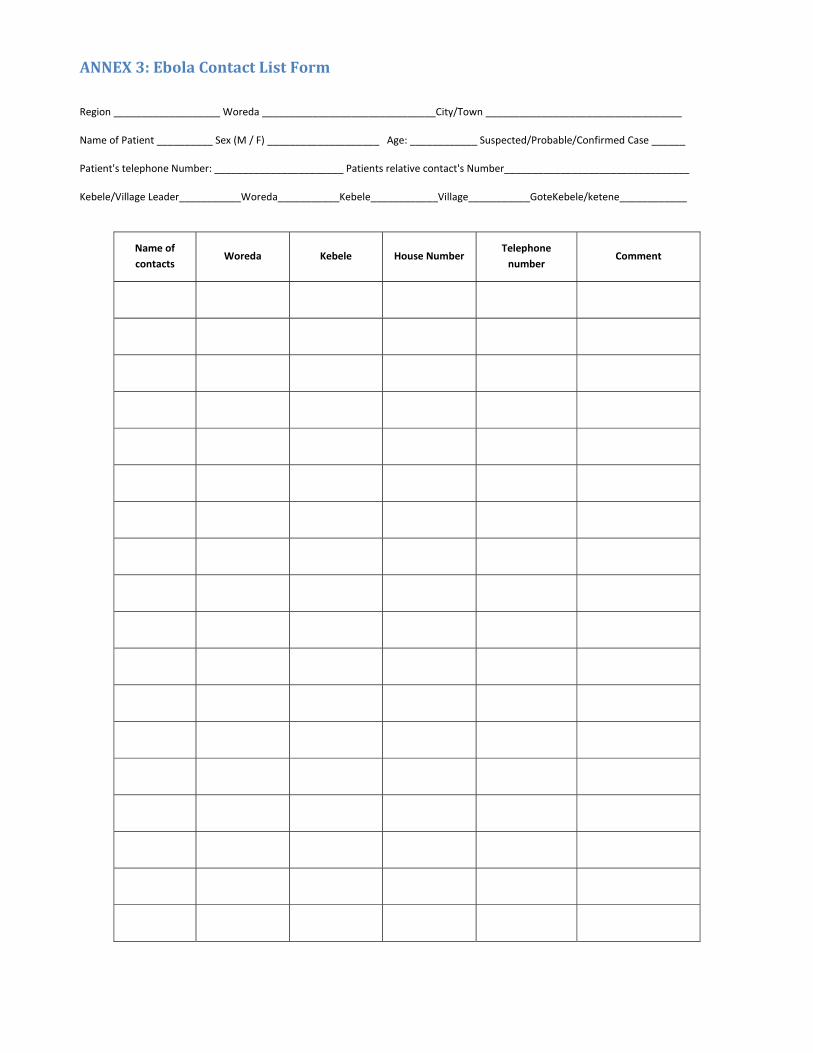
ANNEX 3: Ebola Contact List Form
Region ___________________ Woreda _______________________________City/Town ___________________________________
Name of Patient __________ Sex (M / F) ____________________ Age: ____________ Suspected/Probable/Confirmed Case ______
Patient's telephone Number: _______________________ Patients relative contact's Number_________________________________
Kebele/Village Leader___________Woreda___________Kebele____________Village___________GoteKebele/ketene____________
Name of
contacts Woreda Kebele House Number
Telephone
number Comment
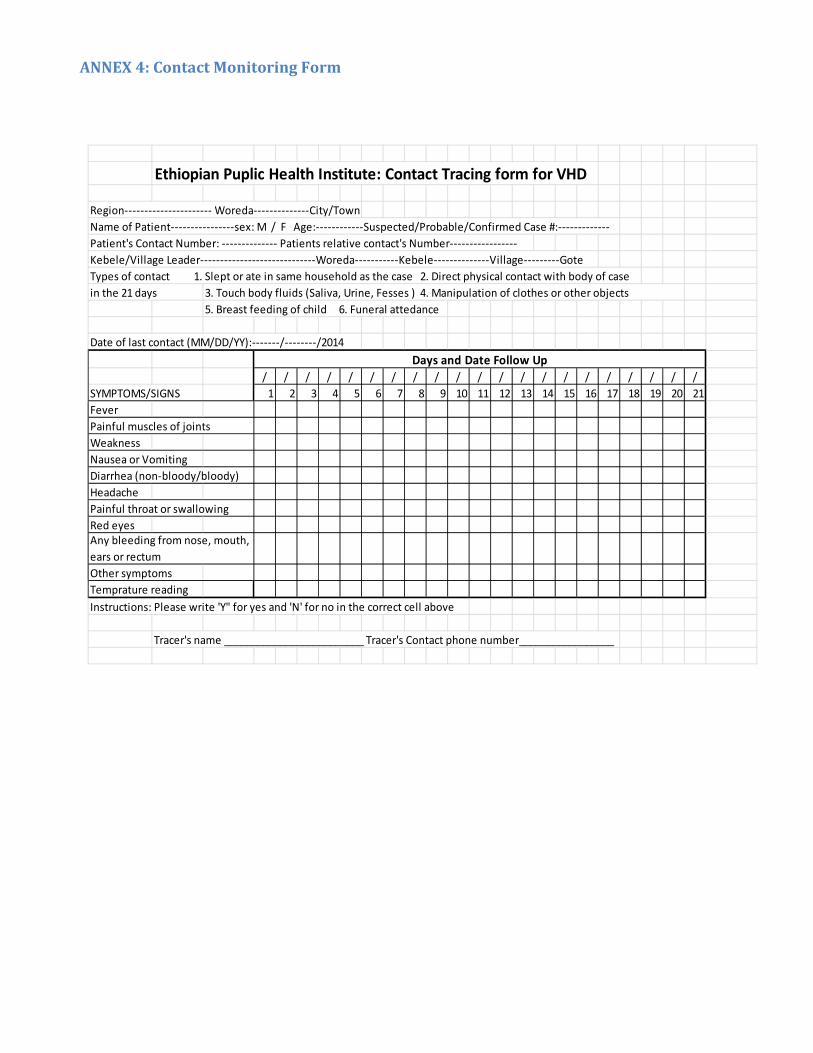
Ethiopian Puplic Health Institute: Contact Tracing form for VHD
Region‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ Woreda‐‐‐‐‐‐‐‐‐‐‐‐‐‐City/Town
Name of Patient‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐sex: M / F Age:‐‐‐‐‐‐‐‐‐‐‐‐Suspected/Probable/Confirmed Case #:‐‐‐‐‐‐‐‐‐‐‐‐‐
Patient's Contact Number: ‐‐‐‐‐‐‐‐‐‐‐‐‐‐ Patients relative contact's Number‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
Kebele/Village Leader‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐Woreda‐‐‐‐‐‐‐‐‐‐‐Kebele‐‐‐‐‐‐‐‐‐‐‐‐‐‐Village‐‐‐‐‐‐‐‐‐Gote
Types of contact 1. Slept or ate in same household as the case 2. Direct physical contact with body of case
in the 21 days
5. Breast feeding of child 6. Funeral attedance
Date of last contact (MM/DD/YY):‐‐‐‐‐‐‐/‐‐‐‐‐‐‐‐/2014
/ / / / / / / / / / / / / / / / / / / / /
SYMPTOMS/SIGNS 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Fever
Painful muscles of joints
Weakness
Nausea or Vomiting
Diarrhea (non‐bloody/bloody)
Headache
Painful throat or swallowing
Red eyes
Other symptoms
Temprature reading
Instructions: Please write 'Y" for yes and 'N' for no in the correct cell above
Tracer's name _________________________ Tracer's Contact phone number_________________
Any bleeding from nose, mouth,
ears or rectum
3. Touch body fluids (Saliva, Urine, Fesses ) 4. Manipulation of clothes or other objects
Days and Date Follow Up
ANNEX 4: Contact Monitoring Form

ANNEX 5: Ground Layout of Ebola Treatment Center
STAFF ENTRANCE/EXIT
Gloved hand washing facility
(0.05% CL)
LOW RISK zone
SCREENING room (tab
WRR WRR
IMMERSION tank
1
IMMERSION tank
2
IMMERSION tank
3
MORGUE
CORPSES
Mini STORE for high risk area
GUARD and
SPRAYER
Laundary washing and drying area
CHLORINE preparation area
WATER point
Gloved hand washing facility
(0.05% CL)
Store room
GUARD and
SPRAYER
STREET SHOES spraying
Bare hand washing facility
(0.05% CL)
Cleaners changing room
DOCTORs’ room
WRR WRR
Chlorine footbath
CHLORINE footbath
STREET SHOES spraying
Hand washing
facility
PATIENT ENTRANCE/EXIT
CHLORINE footbath
Chlorine footbath
CHLORINE footbath
CHLORINE footbath
GLOVED hand washing facility
(0.5% CL)
GLOVED hand washing facility
(0.5% CL)
Laundry washing and drying area
WRR WRR
Sharps pit
Organic pit
Burning pit
CHANGING room
1
CHANGING room 2
Pit for Liquid waste
BARE hand washing facility
(0.05% CL)
bin for SOLID waste
WARD or ROOMs for CONFIRMED cases
SAFETY BOX for sharps
bin for SOLID waste
WARD or ROOMs for PROBABLE cases
SAFETY BOX for sharps
bin for SOLID waste
GLOVED hand washing facility
(0.5% CL)
WARD or ROOMs for SUSPECTED cases
SAFETY BOX for sharps
bin for SOLID waste
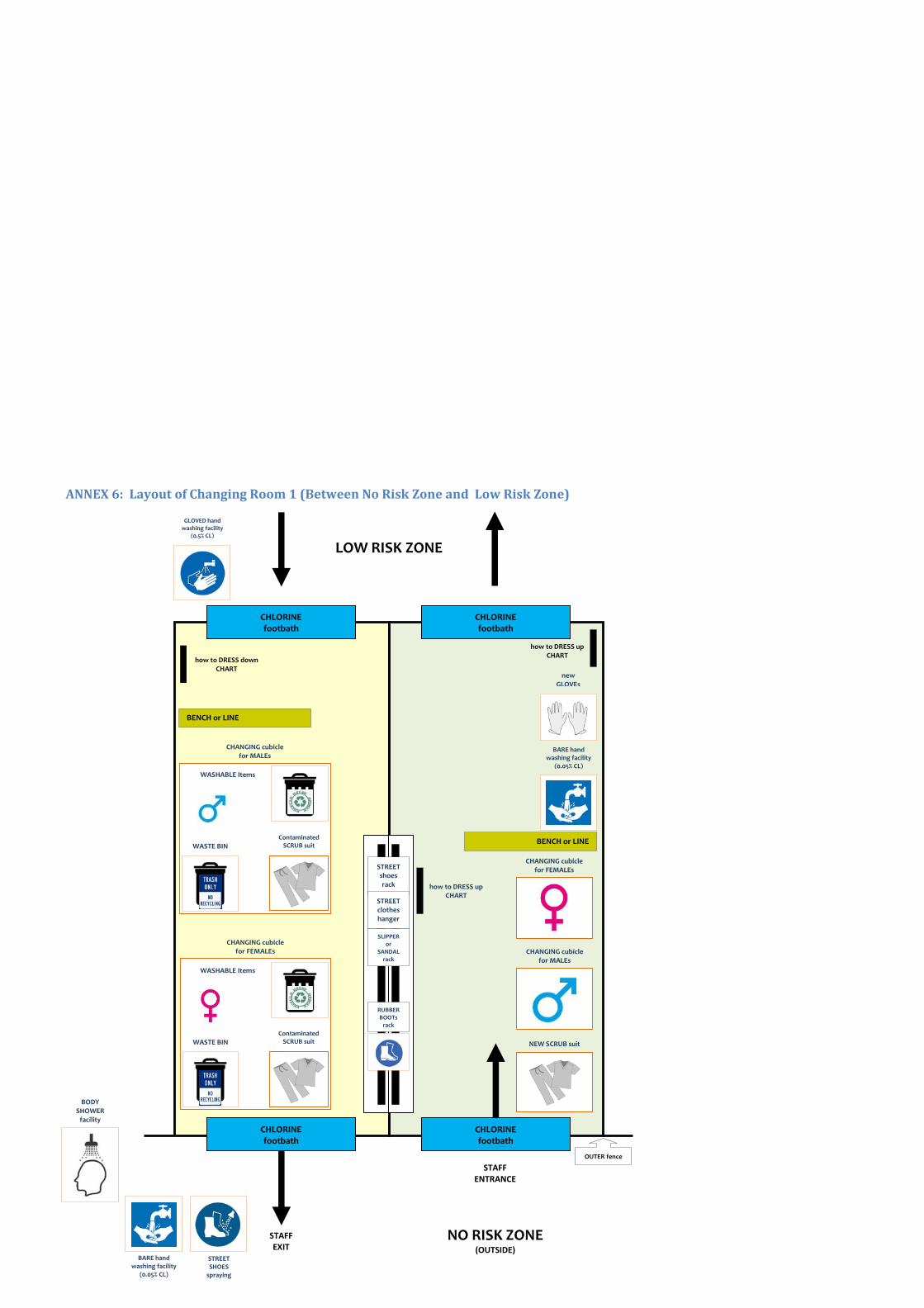
CHLORINE footbath
CHLORINE footbath
CHLORINE footbath
CHLORINE footbath
ANNEX 6: Layout of Changing Room 1 (Between No Risk Zone and Low Risk Zone)
STAFF ENTRANCE
BENCH or LINE
how to DRESS up CHART
BENCH or LINE
how to DRESS down CHART
OUTER fence
NO RISK ZONE (OUTSIDE)
STAFFEXIT
LOW RISK ZONE
BARE hand washing facility
(0.05% CL)
STREET SHOES spraying
BODY SHOWER facility
GLOVED hand washing facility
(0.5% CL)
how to DRESS up CHART
STREET shoes rack
STREET clothes hanger
SLIPPER or
SANDAL rack
RUBBER BOOTs rack
CHANGING cubicle for MALEs
NEW SCRUB suit
BARE hand washing facility
(0.05% CL)
new GLOVEs
CHANGING cubicle for FEMALEs
CHANGING cubicle for FEMALEs
WASHABLE Items
WASTE BIN Contaminated SCRUB suit
CHANGING cubicle for MALEs
WASHABLE Items
WASTE BIN Contaminated SCRUB suit
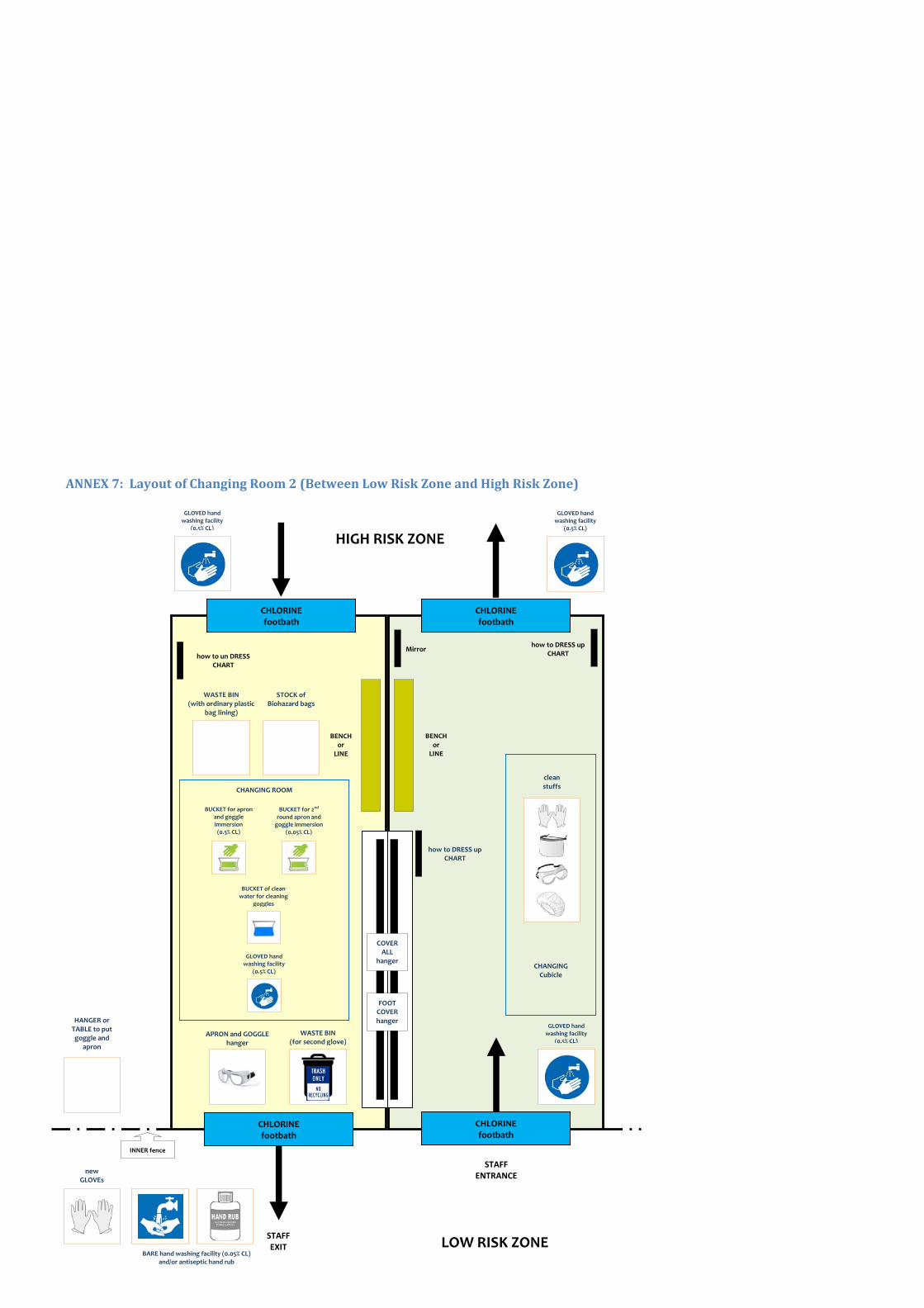
CHLORINE footbath
CHLORINE footbath
CHLORINE footbath
CHLORINE footbath
ANNEX 7: Layout of Changing Room 2 (Between Low Risk Zone and High Risk Zone)
how to un DRESS CHART
WASTE BIN (with ordinary plastic
bag lining)
INNER fence
WASTE BIN (for second glove)
STAFFEXIT LOW RISK ZONE
STAFF ENTRANCE
HIGH RISK ZONE
how to DRESS up CHART
Mirror
APRON and GOGGLE hanger
STOCK of Biohazard bags
CHANGING ROOM
GLOVED hand washing facility
(0.5% CL)
BUCKET for apron and goggle immersion (0.5% CL)
BUCKET for 2nd round apron and goggle immersion
(0.05% CL)
BUCKET of clean water for cleaning
goggles
HANGER or TABLE to put goggle and
apron
CHANGING Cubicle
clean stuffs
how to DRESS up CHART
COVERALL
hanger
FOOT COVER hanger
BENCH or
LINE
BENCH or
LINE
GLOVED hand washing facility
(0.5% CL)
GLOVED hand washing facility
(0.5% CL)
BARE hand washing facility (0.05% CL) and/or antiseptic hand rub
new GLOVEs
GLOVED hand washing facility
(0.5% CL)
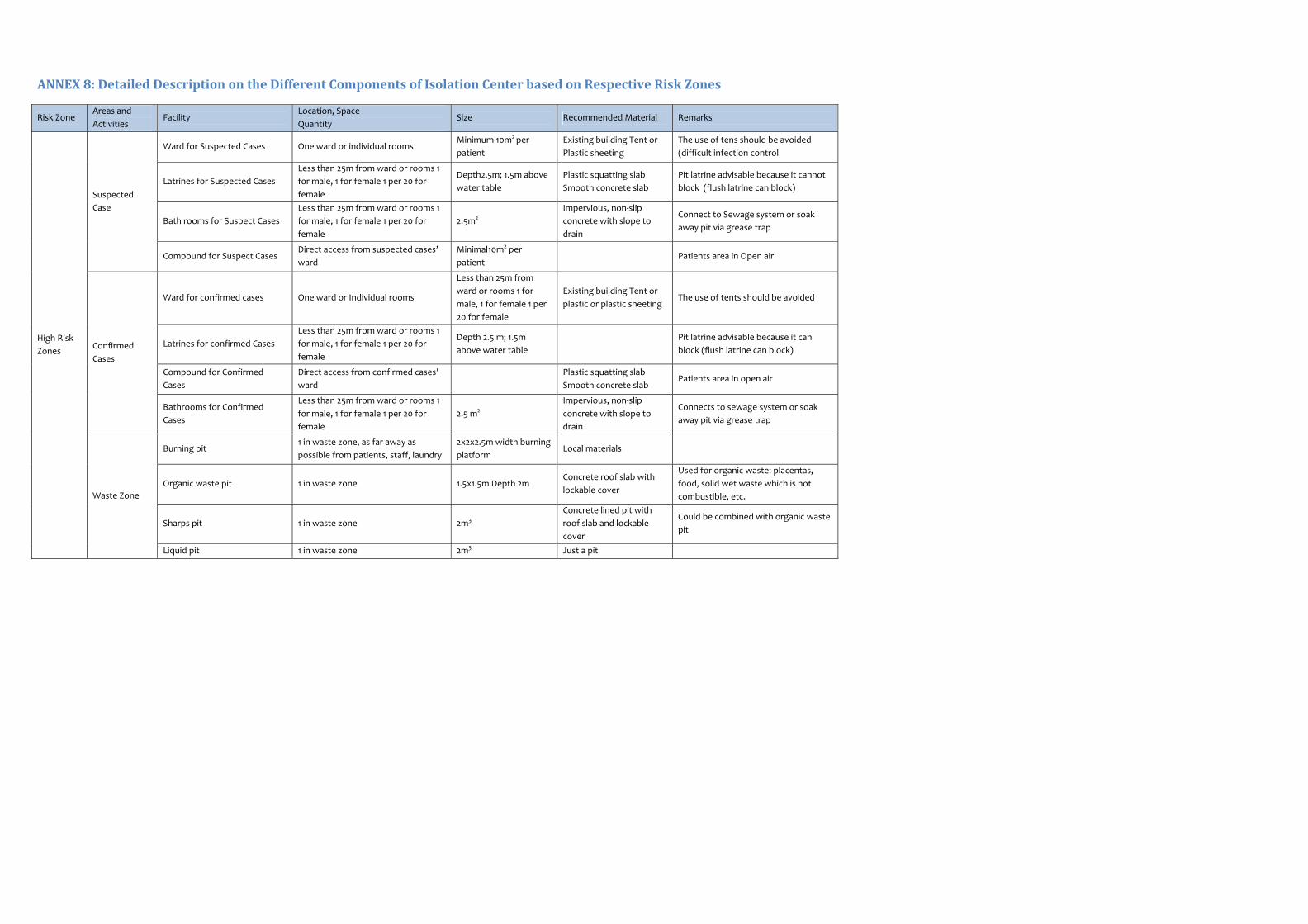
ANNEX 8: Detailed Description on the Different Components of Isolation Center based on Respective Risk Zones
Risk Zone Areas and
Activities Facility
Location, Space
Quantity Size Recommended Material Remarks
High Risk
Zones
Suspected
Case
Ward for Suspected Cases One ward or individual rooms Minimum 10m2 per
patient
Existing building Tent or
Plastic sheeting
The use of tens should be avoided
(difficult infection control
Latrines for Suspected Cases
Less than 25m from ward or rooms 1
for male, 1 for female 1 per 20 for
female
Depth2.5m; 1.5m above
water table
Plastic squatting slab
Smooth concrete slab
Pit latrine advisable because it cannot
block (flush latrine can block)
Bath rooms for Suspect Cases
Less than 25m from ward or rooms 1
for male, 1 for female 1 per 20 for
female
2.5m2
Impervious, non‐slip
concrete with slope to
drain
Connect to Sewage system or soak
away pit via grease trap
Compound for Suspect Cases Direct access from suspected cases’
ward
Minimal10m2 per
patient Patients area in Open air
Confirmed
Cases
Ward for confirmed cases One ward or Individual rooms
Less than 25m from
ward or rooms 1 for
male, 1 for female 1 per
20 for female
Existing building Tent or
plastic or plastic sheeting The use of tents should be avoided
Latrines for confirmed Cases
Less than 25m from ward or rooms 1
for male, 1 for female 1 per 20 for
female
Depth 2.5 m; 1.5m
above water table
Pit latrine advisable because it can
block (flush latrine can block)
Compound for Confirmed
Cases
Direct access from confirmed cases’
ward
Plastic squatting slab
Smooth concrete slab Patients area in open air
Bathrooms for Confirmed
Cases
Less than 25m from ward or rooms 1
for male, 1 for female 1 per 20 for
female
2.5 m2
Impervious, non‐slip
concrete with slope to
drain
Connects to sewage system or soak
away pit via grease trap
Waste Zone
Burning pit 1 in waste zone, as far away as
possible from patients, staff, laundry
2x2x2.5m width burning
platform Local materials
Organic waste pit 1 in waste zone 1.5x1.5m Depth 2m Concrete roof slab with
lockable cover
Used for organic waste: placentas,
food, solid wet waste which is not
combustible, etc.
Sharps pit 1 in waste zone 2m3
Concrete lined pit with
roof slab and lockable
cover
Could be combined with organic waste
pit
Liquid pit 1 in waste zone 2m3 Just a pit

Risk Zone Areas and
Activities Facility
Location, Space
Quantity Size Recommended Material Remarks
Laundry Area
Laundry washing area Away from burning site, adjacent to
laundry lines and water point Around 9m2 Concrete slab
Connect to sewage system or soak
away via grease trap
Laundry drying area Away from burning site, adjacent to
laundry area Around 15m2
Wooden or iron poles,
rope
Preferably in the sun (UV assists in
destroying the Ebola Virus
Corpses Morgue Easy access from patients area with
large exit for ambulance 5x4m
Existing building Tent or
plastic sheeting(roof is
required)
In most of the settings there will be no
morgue, and the corpses will go
directly to the burial ground
Floor should be easy building
SLUICE Disinfection Foot bath, hand washing and
spraying location 1 between high‐risk and low‐risk zone
1.5x2.5m Foot bath:
80x80cm
Concrete or gravel floor
with footbath of plastic
sheeting
Should be full time staffed by a
guard/sprayer; Adjacent to the
changing room
SLUICE Disinfection Foot bath, hand washing and
spraying location 1 between high‐risk and low‐risk zone
1.5x2.5m Foot bath:
80x80cm
Concrete or quarrel floor
with footbath of plastic
sheeting
Should be staffed full time by a
guard/sprayer; Adjacent to the
changing room
Low Risk
Zone
Putting on/off
protective
clothing
Changing room 1 At door between outside and low‐risk
zone 3x4m minimum
Existing building Tent or
plastic sheeting
Separation between risk zones inside
the changing room must be clearly
indicated
Changing room 2 At door between low‐risk zone and
high‐risk zone 3x4m minimum
Existing building Tent or
plastic sheeting
Separation between risk zone inside
the changing room must be clearly
indicated
Disinfection Chlorine preparation Close to water point 3x4m minimum Concrete slab Gravel bed
Must have good drainage into sewage
system or soak away via grease trap
Must be well‐ventilated(chlorine gas in
heavier than air
Administration Doctor’s room 1 room close to the patients area 3x4m minimum Local building material Must NOT be in High risk zone!
Laundry Area
Laundry washing area Away from burning site, adjacent to
laundry lines and water point Around 9m2 Concrete slab
Connect to sewage system or soak
away via grease trap
Laundry drying area Away from burning site, adjacent to
laundry area Around 15m2
Wooden or iron poles,
rope
Preferably in the sun (UV assists in
destroying the Ebola Virus
Security Guard shack Main entrance; Every exit from high‐
risk and low‐risk zone. 4m2
Existing Building Tent or
plastic sheeting
Storage Store room on compound 1 small store on compound for
several days stock 3x4 m
Existing Building Tent or
plastic sheeting

Risk Zone Areas and
Activities Facility
Location, Space
Quantity Size Recommended Material Remarks
SLUICE Disinfection Foot bath, hand washing and
spraying location 1 between outside and low risk zone
1.5x2.5m Foot bath:
80x80cm
Concrete or gravel floor
with footbath of plastic
sheeting
Should be full time staffed by a guard /
Sprayer, adjacent to the changing
room.
OUTSIDE
ISOLATION
UNIT
Storage General store room 1 outside isolation compound 8x4m Existing Building Tent or
plastic sheeting
Kitchen Kitchen for patients and
possible attendants 1 outside isolation compound 4x4m
Existing Building Tent or
plastic sheeting
Respect protocols; see also point III E b
“Kitchen and food for patients and
attendants
Staff room Lunch room for staff 1 outside isolation compound
Staff toilet Latrine 1 per 20 staff 2.5m2 Plastic squatting slap
Smooth concrete slab
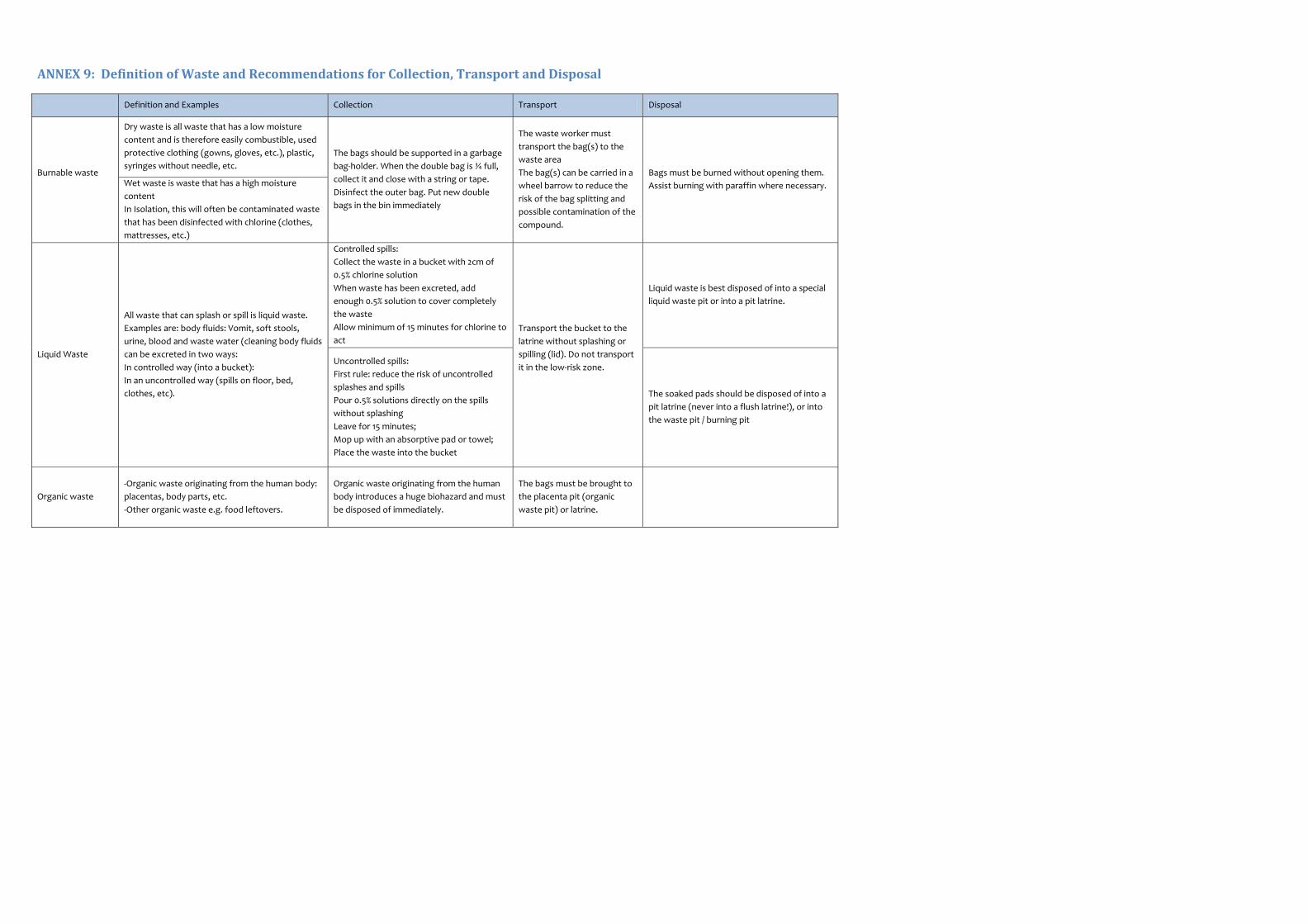
ANNEX 9: Definition of Waste and Recommendations for Collection, Transport and Disposal
Definition and Examples Collection Transport Disposal
Burnable waste
Dry waste is all waste that has a low moisture
content and is therefore easily combustible, used
protective clothing (gowns, gloves, etc.), plastic,
syringes without needle, etc.
The bags should be supported in a garbage
bag‐holder. When the double bag is ¾ full,
collect it and close with a string or tape.
Disinfect the outer bag. Put new double
bags in the bin immediately
The waste worker must
transport the bag(s) to the
waste area
The bag(s) can be carried in a
wheel barrow to reduce the
risk of the bag splitting and
possible contamination of the
compound.
Bags must be burned without opening them.
Assist burning with paraffin where necessary. Wet waste is waste that has a high moisture
content
In Isolation, this will often be contaminated waste
that has been disinfected with chlorine (clothes,
mattresses, etc.)
Liquid Waste
All waste that can splash or spill is liquid waste.
Examples are: body fluids: Vomit, soft stools,
urine, blood and waste water (cleaning body fluids
can be excreted in two ways:
In controlled way (into a bucket):
In an uncontrolled way (spills on floor, bed,
clothes, etc).
Controlled spills:
Collect the waste in a bucket with 2cm of
0.5% chlorine solution
When waste has been excreted, add
enough 0.5% solution to cover completely
the waste
Allow minimum of 15 minutes for chlorine to
act
Transport the bucket to the
latrine without splashing or
spilling (lid). Do not transport
it in the low‐risk zone.
Liquid waste is best disposed of into a special
liquid waste pit or into a pit latrine.
Uncontrolled spills:
First rule: reduce the risk of uncontrolled
splashes and spills
Pour 0.5% solutions directly on the spills
without splashing
Leave for 15 minutes;
Mop up with an absorptive pad or towel;
Place the waste into the bucket
The soaked pads should be disposed of into a
pit latrine (never into a flush latrine!), or into
the waste pit / burning pit
Organic waste
‐Organic waste originating from the human body:
placentas, body parts, etc.
‐Other organic waste e.g. food leftovers.
Organic waste originating from the human
body introduces a huge biohazard and must
be disposed of immediately.
The bags must be brought to
the placenta pit (organic
waste pit) or latrine.

Definition and Examples Collection Transport Disposal
Organic waste can be collected in a double
plastic bag supported by a garbage‐bag
holder. Close the bags with a string or tape.
Disinfect the outside of the bag.
The bags must be brought to
the placenta pit (Organic
waste pit) or latrine.
Organic waste can be disposed of in a specially
built organic waste pit. If such a pit is not
available, dispose of into a pit latrine.
Waste Water ‐Run off water: rain water from the roof, or
compound
Avoid runoff water to flow from higher into
lower risk zones.
Direct wastewater to gutters,
ideally lined with concrete.
Runoff water and wastewater has to be
controlled and directed to safe disposal areas.
If wastewater is disposed of in a soak away, a
grease trap should be installed. The grease
trap must be disinfected before it’s cleaned
‐Waste water: water used for cleaning, from foot
baths, etc.
Wastewater has to be directed and
collected into a soak away or liquid pit.
Sharps
Items that can cause cuts or puncture wounds,
including needles, scalpels, knives, infusion sets,
saws, broken glass, nails, etc.
Sharps containers.
Disinfect outside of the
sharps box before
transporting. Fill inside with
0.5% chlorine solution before
disposal.
Sharps pit

ANNEX 10: Steps on Putting on Personal Protective Equipments with Donning Pictures
CHLORINE footbath
GLOVED hand washing facility
(0.5% CL)
3. Wash your hands with soap
and water or alcohol swab.
4. Put on one pair of
disposable gloves.
5. Bath your foot with
chlorine.
6. Disinfect the gloved hand
with 0.5% chlorine.
CHLORINE footbath
BARE hand washing facility (0.05% CL) or antiseptic handrub
GLOVED hand washing facility
(0.5% CL)
7. Put on the cover‐all (make sure the sleeves are under the 1st layer of glove
and put on a plaster on top of it)
8. Put on the foot cover (if available).
9. Put on a second layer of gloves*1 (should be done after the goggles or
face shield if using heavy duty gloves).
10. Put on the face mask.
11. Put on the hood of coverall (if the coverall do not have
hood, put on head cover).
12. Put on goggles or face shield (which ever available)
13. Put on waterproof apron (if you expect exposure with
body fluids)
14. Bath your feet in chlorine solution
15. Disinfect the gloved hand with 0.5% chlorine.
16. Go into the high‐risk zone.
1. Remove street shoes and street clothes (your own shoes and clothes) in
dressing room 1.
2. Put on scrub suit and your personal rubber boots. Tuck scrub suit into
boots.

ANNEX 11: Steps on Removing Personal Protective Equipments with Pictures
17. Disinfect gloved hands with 0.5%.
18. Take goggles and apron with you.
19. Step in the second footbath.
20. Now you are in the Low‐risk area
21. Hang the goggle and the apron.
22. Remove the inner layer gloves and throw away in the waste bin.
23. Wash your hands with 0.05% or use alcohol hand rub.
24. Put a new pair of examination gloves.
1. Disinfect gloved hands with 0.5% chlorine solution before
entering undressing room
2. Bath your feet in chlorine solution.
3. Enter the undressing room.
4. Peel off disposable apron and dispose safely (throw away in a
bio‐hazard plastic bag).
5. If the apron is to be reused, immerse the apron in the container
of 0.5% chlorine solution and after that in the second container
0.05% chlorine solution and hang it close to the second footbath
(in changing room 2).
6. Remove the shoe cover (if there is any)
CHLORINE footbath
GLOVED hand washing facility
(0.5% CL)
7. Disinfect the outer pair of gloves with 0.5% chlorine solution and
remove them.
A. If using surgical gloves: throw away in the waste bin.
B. If using heavy‐duty gloves: place in the bucket containing 0,
05% chlorine solution.
8. Disinfect gloved hands with 0.5% chlorine.
9. Remove goggles, disinfect with 0.5% and rinse with clean water.
10. Hang it close to the second footbath, next to the apron.
11. Disinfect the gloved hands with 0.5%.
12. Remove hood of the coverall (if a separate head cover is used,
remove and throw away in the waste bin).
13. Disinfect gloved hands with 0.5%.
14. Remove coverall and throw away in waste bin.
15. Disinfect gloved hands with 0.5%.
16. Remove mask and throw away in waste bin
bucket with 0.05%
CHLORINE solution
GLOVED hand washing facility
(0.5% CL)

ANNEX 12: How to Don and Remove Non‐Sterile Examination Gloves
When the hand hygiene indication occurs before a contact requiring glove use, perform hand hygiene by rubbing with an
alcohol‐based hand rub or by washing with soap and water.
1 Take out a glove from its original
box
2 Touch only a restricted surface of the glove
corresponding to the wrist (at the top edge of the cuff)
3 Don the first glove
4 Take the second glove with the bare hand and touch only a restricted surface of glove
corresponding to the wrist
5 To avoid touching the skin of the forearm with the gloved hand, turn the external surface of the glove to be donned on the folded fingers of the gloved hand, thus permitting to glove
the second hand
6 Once gloved, hands should not touch anything else that is not defined by
indications and conditions for glove use
1 Pinch one glove at the wrist level to
remove it, without touching the skin of the forearm, and peel away from the hand, thus
allowing the glove inside out.
2 Hold the removed glove in the gloved hand and slide the fingers of the un‐gloved hand inside between the glove and the wrist. Remove the second glove by rolling it down the hand and fold into the first
glove.
3 Discard the removed gloves.
I. HOW TO DON GLOVES
II. HOW TO REMOVE
4 Then, perform hand hygiene by rubbing with an alcohol‐based handrub or by washing with soap and water
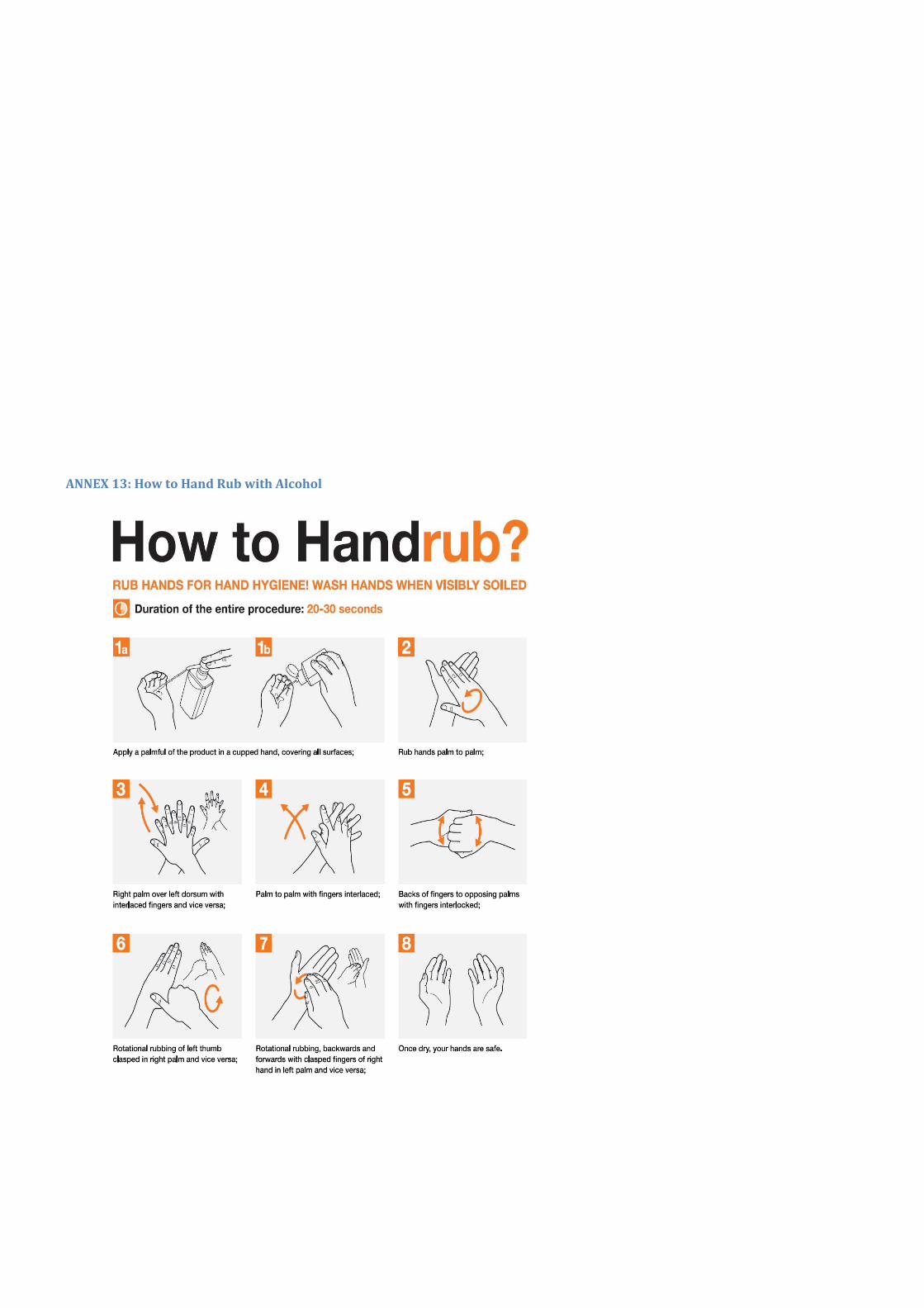
ANNEX 13: How to Hand Rub with Alcohol

ANNEX 14: How to Hand Wash

ANNEX 15: How to Make Chlorine Solutions for Environmental Disinfection
Check concentration (%) concentrate of the chlorine product you are using.
Determine total parts water needed using the following formula:
Total Parts (TP) water = [% Concentrate/% Dilute] ‐1
Mix 1 part concentrated bleach with the total parts water required.
Example 1:
Make a dilute solution (0.5%) from 5% concentrated solution.
Step 1: Calculate TP water: [5.0%/0.5%] – 1 = 10 ‐1= 9
Step 2: Take 1 part concentrated solution and add to 9 parts water.
Step 3: Label properly the prepared 0.5% chlorine solution.
Example 2:
Make a dilute solution for rinsing a gloved hand (0.05%) from 5% concentrated solution.
Step 1: Calculate Total Parts water: [5.0%/0.05%] – 1 = 100 ‐1= 99
Step 2: Take 1 part concentrated solution and add to 99 parts water.
Step 3: Label properly the prepared 0.05% chlorine solution.
Formula for making dilute solutions from dry powders
Check concentration (%) concentrate) of the powder you are using.
Determine grams bleach needed using the formula below:
Grams/Liter = [% Dilute/% Concentrate] x 1000
Mix measured amount of bleach powder with 1 liter of water.
Example:
Make a dilute chlorine‐releasing solution (0.5%) from a concentrated powder (35%).
Step 1: Calculate grams/liter: [0.5%/35%] x 1000 = 14.2 g/L
Step 2: Add 14.2 grams (14 g) to 1 liter of water
Take 1 part concentrated solution and add to 49 parts boiled (filtered if necessary) water.

ANNEX 16: Cleaning and Disinfection of Protective Equipments
Items that require routine and regular disinfection, cleaning and/or laundry are: aprons, goggles, scrub suits,
boots, and reusable gloves.
Disinfection of Aprons
Dip in bucket of 0.5% chlorine solution for 3 minutes and then scrub.
Dip in bucket of fresh 0.5% chlorine solution.
Rinse with clean water.
Hang to dry.
Disinfection of Goggles
Place goggles under a flow of 0.5% chlorine solution for 30 seconds, and
Ensure that all parts of the goggles have been soaked in the solution.
Rinse with clear water!!
Hang to dry in the sun.
Each user is responsible for ensuring that their goggles are disinfected and clean before putting them on.
Disinfection of Scrub Suits
Put scrub suits in fresh 0.05% chlorine solution.
Leave to soak for 30 minutes.
Rinse twice with clear water.
Wash with detergent and fresh water.
Rinse with clear water.
Hang to dry in the sun.
Cleaning and Disinfection of Boots
Put boots in fresh 0.05% chlorine solution.
Leave to soak for 30 minutes.
Rinse twice with clear water.
Dry upside down on sticks driven into the ground.
Disinfection of Reusable Gloves
Household gloves and heavy‐duty gloves can be reused after disinfection and cleaning.
Soak in 0.05% chlorine solution for 30 minutes.
Rinse twice with clean water.
Fill gloves with water and squeeze to check for any leaks.
Dry on sloping racks or on sticks driven into the ground.

ANNEX 17: Caretaker Task Instruction
Dressing and Undressing
The caretaker dresses up with complete PPE just like other health workers if to enter to high risk zone.
How to Provide the Food
Ask the patient to bring his plate to the door and spoon the food into it without touching.
If the patient cannot walk, the caretaker dresses and enters the room, and brings the plate to the door
where another family member spoons the food into it without touching.
How to Wash Utensils
Before entering the room, put a bucket half filled with 0.05% chlorine solution outside the door.
Carefully place the dirty utensils into the bucket without leaving the room or touching the bucket.
After 30 minutes, the bucket can be removed. The contents must be rinsed and washed with soap.
Put utensils in the sun to dry.
How to dispose of feces
Pour 1 cm of 0.5% chlorine solution into the bucket.
After use pour another cup of 0.5% chlorine solution over the contents and put the lid on.
Disinfect the outside of the bucket with 0.5% chlorine solution and place it outside the door.
Leave the bucket for at least 15 minutes, and once undressed and outside the room again, put on
clean gloves and pour the contents carefully into the latrine
Disinfect the latrine once a day with 0.5% chlorine solution.

ANNEX 18: Summary of Implementation of IPC Best Practices during Direct Patient Care and Related Activities
What? How? Who is responsible?
Create isolation rooms or
areas.
‐ Identify single rooms and prioritise these for
patients with known or suspected Ebola virus.
‐ Refer to guidance on setting up an isolation
area.
‐ Coordinator or IPC staff to identify
areas/rooms for patient placement.
‐ Health workers to adhere to
recommendations and report to the
coordinator when a patient is not placed in an
isolation room/area.
Restrict all non‐essential staff
from EVD patient care
rooms/areas.
‐ Ensure that clinical and non‐clinical personnel
are assigned exclusively to patient care areas and
that members of staff do not move freely
between these areas and other clinical areas
during the outbreak.
‐ Cohort staff between areas with suspected and
those with confirmed SVD patients.
‐ Use signage to alert restrictions of staff.
‐ Maintain a log of persons entering the room.
‐ Coordinator and/or IPC staff.
Limit the number of visitors
allowed access to the patient.
‐ Use signage and other communications to alert
restrictions of visitors. Make simple messages
understandable for the public but also be careful
to avoid stigmatization.
‐ Maintain a log of persons entering the room.
‐ Coordinator and/or IPC staff
‐ Involve patient or community representatives,
if available.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.
Ensure that all staff and
visitors correctly use and
remove recommended
personal protective equipment
(PPE).
‐ Ensure the equipment is always available and
promptly at the isolation rooms/areas entry.
‐ Provide staff and visitors with instructions on
the use and correct removal of PPE through
training and reminder posters.
‐ Coordinator and/or IPC staff
‐ Involve patient or community representatives,
if available.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.
‐ Another staff member should be assigned to
supervise the sequence of putting on and
removing PPE by his/her colleague.
Ensure that all staff and
visitors perform hand hygiene
according to the above
recommendations. These hand
hygiene actions should be
performed when
recommended even if PPE is
worn.
‐ Provide staff and visitors with instructions on
the importance of hand hygiene best practices
through training and reminder posters.
‐ Ensure continuous availability of alcohol‐based
hand rub and soap, water and single‐use towels
at the isolation room/areas entry and at the point
of care.
‐ Coordinator and/or IPC staff.
‐ Involve patient or community representatives,
if available.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.

What? How? Who is responsible?
Limit the use of needles and
other sharp objects as much as
possible. If this cannot be
avoided see instructions in the
text.
‐ Provide staff and carers with instructions on the
essential use of needles and sharps through
training and reminder posters.
‐ Ensure the equipment is available to do this.
‐ Health workers to adhere to
recommendations.
Dispose of needles and other
sharp objects safely.
‐ Provide staff and carers with instructions on the
safe disposal of sharps through training and
reminder posters.
‐ Ensure the equipment is available to do this.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.
Create system of safe
management of waste and
linen.
‐ Provide staff and visitors/carers with
instructions on the safe management and
disposal of waste and linen through training and
reminder posters.
‐ Ensure the equipment is available to do this.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.
Limit the use of phlebotomy
and laboratory testing to the
minimum necessary for
essential diagnostic evaluation
and patient care.
‐ Provide staff with training and visual
instructions on the need for essential
phlebotomy and lab testing.
‐ Health workers to adhere to
recommendations.
Only take a patient out of their
room/care area if they are free
of virus, or for essential, life‐
saving tests.
‐ Provide staff with training and visual
instructions on the appropriate times to take the
patient from their care area and on precautions
to take.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.
Undertake cleaning of the
environment and patient care
equipment safely following
recommendations in the text.
‐ Provide staff and visitors/carers with
instructions on cleaning through training and
reminder posters.
‐ Ensure the equipment is available to undertake
recommended cleaning.
‐ Health workers to adhere to
recommendations and report to the
coordinator when they are not followed.

ANNEX 19: Summary of Symptomatic Treatment Of Patients
Symptoms and or signs Treatment
Fever (>38.0 °C) Manage fever with paracetamol Avoid diclofenac, ibuprofen or aspirin due to platelet effects.
Acute significant bleeding/ moderate to severe pallor/ emergency signs of circulatory shock
Transfuse with whole blood
Pain Treat pain with paracetamol (if mild) or morphine if moderate and severe). Avoid diclofenac, ibuprofen or other NSAIDs due to platelet effects.
Difficulty breathing/ respiratory distress
Oxygen: titrate to Sp0 >90% If SpO2 < 90% start adult on 5 litres/minute (nasal prongs); start child at 1‐2
Litres/minute (nasal prongs) Evaluate for pneumonia, wheezing, fluid overload, congestive heart failure and manage accordingly. (Do not share nasal prongs ‐once used by a patient dispose.)
Diarrhoea, vomiting, signs of dehydration
Provide ORS even if no signs of dehydration Monitor signs of dehydration. If no, some or severe dehydration, use Fluid Plans A, B and C, respectively
If severely malnourished child with shock, see Chid pocket book.
Nausea and vomiting are common‐ anti‐emetic medications may provide some relief and facilitate oral rehydration. For adult, give chlorpromazine 25‐50 mg, 4 times daily IM or orally or metoclopramide 10 mg IV/ orally 3 times daily until
Vomiting stops. For children, give promethazine. Monitor for extrapyramidal signs.
Dyspepsia (i.e., "heartburn") In adults and children > 10 years, give omeprazole 20 mg orally daily or magnesium trisilicate, 2 tabs every 8 hours until symptoms resolved. In children 5‐12 years, give magnesium trisilicate: 5‐10 mls, 3 times daily
Convulsions
Approach convulsing patients with caution. Give diazepam to abort seizure if prolonged (rectally if there is not an IV already in place‐ adult 20 mg (4 ml of 10 mg/2ml solution); child 0.5 mg/kg)), then control with phenobarbital loading dose (child: 15 mg/kg over 15 minutes‐ IM or IV); adult: 10 mg/kg.
Signs of hypoglycaemia Test glucose (and monitor regularly) If low, give IV D50 5 ml/kg in child; 25 to 50 ml of D50 in adult Nutritional support
Anxiety Psychological support , Diazepam ‐adults: 5‐15 mg/day in 3 divided doses
Confusion in cooperative patient
Restrain with patient in calm and non‐aggressive fashion. Keep lighting on at night Consider diazepam 5 mg at night (adult)
Confusion and aggression in non‐cooperative patient
Give sedation‐haloperidol 5 mg IM (adult)
Shock See diagnosis and management of septic shock below.
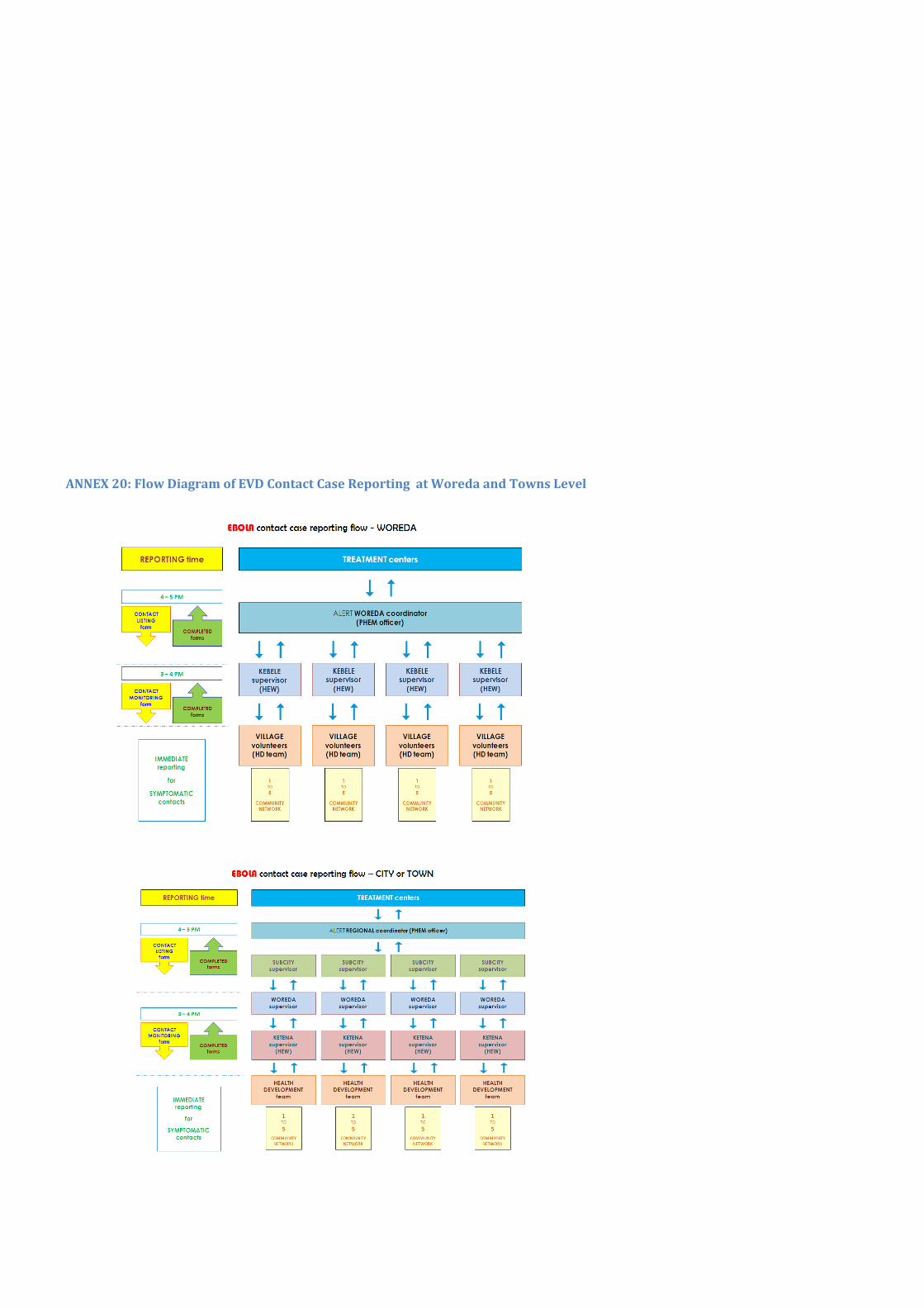
ANNEX 20: Flow Diagram of EVD Contact Case Reporting at Woreda and Towns Level