EATING DISORDERS ON CAMPUS: WORKING TOGETHER TO … Disorders II.pdf• Intense fear of gaining...
94
EATING DISORDERS ON CAMPUS: WORKING TOGETHER TO PROMOTE EFFECTIVE EVALUATION, REFERRAL, MANAGEMENT AND STUDENT MOTIVATION FOR CHANGE New York State College Health Association Annual Meeting Saratoga Hotel and Conference Center October 11, 2007 1:55-3:10 p.m. Mary Tantillo PhD RN CS FAED Director, Eating Disorders Recovery Center of Western NY Unity Health System Clinical Associate Professor, Department of Psychiatry University of Rochester Medical Center
Transcript of EATING DISORDERS ON CAMPUS: WORKING TOGETHER TO … Disorders II.pdf• Intense fear of gaining...

EATING DISORDERS ON CAMPUS: WORKING TOGETHER TO PROMOTE EFFECTIVE
EVALUATION, REFERRAL, MANAGEMENT AND STUDENT MOTIVATION FOR CHANGE
New York State College Health AssociationAnnual Meeting
Saratoga Hotel and Conference CenterOctober 11, 20071:55-3:10 p.m.
Mary Tantillo PhD RN CS FAEDDirector, Eating Disorders Recovery Center of Western NY
Unity Health SystemClinical Associate Professor, Department of Psychiatry
University of Rochester Medical Center
EATING DISORDERS ARE DISEASES OF DISCONNECTION
- Disconnect patient from herself and others- Disconnect family from other families- Disconnect family from staff- Disconnect treatment team from one another

DSM-IV TR Criteria for Anorexia Nervosa
• Refusal to maintain weight at or above minimally normal weight for age and height or failure to make expected weight gain (<85% ofthat expected).
• Intense fear of gaining weight or becoming fat,even though underweight.
• Disturbance in how weight and shape are experienced; undue influence of weight andshape on self-evaluation, or denial of seriousness of current low body weight.
• In postmenarcheal females, amenorrhea (absence of 3 consecutive menstrual cycles).

DSM-IV TR Criteria for Bulimia Nervosa• Recurrent episodes of binge eating (eating in a
discrete period of time an amount of food larger than most people would eat during the same time and under the same circumstances; sense of lackof control).
• Recurrent inappropriate compensatory behaviorto prevent weight gain.
• Binge eating and compensatory behaviors occurat least twice per week x 3 months.
• Self-evaluation is unduly influenced by body shape and weight.
• Disturbance does not occur exclusively during episodes of Anorexia Nervosa.
DSM-IV TR Criteria for Binge Eating Disorder• Recurrent episodes of binge eating (eating in a
discrete period of time an amount of food larger than most people would eat during the same time and under the same circumstances; sense of lackof control).
• Binge eating is associated with 3 or more of following:
– eating much more rapidly than normal– eating until uncomfortably full– eating large amounts of food when not hungry– eating alone because of embarrassment – feeling disgusted with oneself, depressed, guilty
• Binge eating occur at least 2 days per week x 6 months.
• Marked distress regarding binge eating is present.
Comorbid Psychiatric Illness and Eating Disorders
Affective Disorders Anxiety Disorders Substance Abuse Personality Disorders

Affected Biological Systems• Neurologic (CNS and PNS)• Skin and Hair• Cardiovascular• Hematologic• Hepatic• GI: motility, absorption• Endocrine (hypothalamic)
– Thyroid– Growth hormone– Adrenal – Gonads
• Musculoskeletal
Kreipe RE. Assessment of Weight Loss in the Adolescent. Ross Labs. Columbus, OH 1988. Drawing by C. Lyons, MD

Anorexia Nervosa: Signs and Symptoms• Weight loss• Fatigue• Weakness• Dizziness• Headache• Palpitations• Decreased Pulse, RR, B/P, body temp• Cold/cyanotic extremities• Intolerance of the cold• Amenorrhea• GI complaints - e.g., bloating, constipation, vomiting, abdominal pain
• Polyuria• Lanugo• Brittle hair and nails/hair loss• Sleep disturbances

Bulimia Nervosa: Signs and Symptoms• Erosion of dental enamel• Periodontal disease• Dental caries• Weakness/lethargy/fatigue• Headache• GI complaints, e.g, constipation,
vomiting, bloating, abdominal pain• Edema (ankle, periorbital)• Palpitations• Menstrual/fertility problems • Swollen salivary glands• Mouth ulcers• Frequent sore throats• Esophageal burning• Gastroesophageal erosions• Hematemesis• Scarring on dorsum of hand

Week 1:•Wt 91#; •S.G. 1.018;•HR: 62 →70;•36.9°C
Weekly visits
Week 5:•Wt 91#; •S.G. 1.020;•HR: 44→82•35.3°Cl
Recheck Wt. (observed) and physical exam
(Kreipe, 2007)

Warning Signs of Eating Disorders• Preoccupation with weight, food, calories, fat
grams, and dieting• Dramatic weight loss• Refusal to eat certain foods• Frequent comments about being fat (despite wt loss)
• Anxiety about being fat or gaining weight• Denial of hunger• Food rituals• Consistent excuses at meal times• Rigid exercise routine (despite illness,
fatigue, injury)

Warning Signs of Eating Disorders• Social withdrawal• Evidence of binge eating (disappearance of large amounts of food in short periods of time
• Existence of wrappers and containers indicating intake of large amounts of food
• Containers of laxatives and diuretics• Leaving the table right after meals• Creation of complex life style, schedule or
rituals to make time for binge-purge episodes• In general, behaviors and attitudes indicating wt loss,dieting and control of food are primary concerns

Mortality and Eating Disorders
• Eating Disorders have the highest mortality rate of all psychiatric illnesses .
• The mortality rate for Anorexia Nervosa is 5.6% per decade and up to 20% during a 20 year follow-up.
• Leading causes of death are suicide and cardiac arrest (starvation and electrolyte imbalance).
EATING DISORDERS AND SUBSTANCE ABUSE: A LETHAL
COMBINATIONSuicide:• For women 15-24, the death rate is 12 times higher for
women with anorexia nervosa as compared to women in the general population.
• Alcohol–abusing women attempt suicide 4 times more often than non-alcoholic women. Among adults with alcohol use disorders, the suicide rate is equal to men. However, women attempt more often.
EATING DISORDERS – DISEASES OF DISCONNECTION
Biopsychosocial Risk Factors:Biology: Serotonergic Disturbance; Starvation;
Binging/PurgingPsychology: Disconnections; Relational
mismatchesSocio-Cultural: Toxic Societal Values that objectify
women’s (and men’s) bodies and teachus to value ourselves from the outside in
Spirituality: Hopelessness; Meaninglessness; Isolation

Genes and Environment
Family aggregation, twin, and linkage andassociation studies all suggest a role for genetic risk & environment:
- Heritability estimates: AN – 48%-76%; BN – 54%-85% - Family morbidity and comorbidity- What is inheritable may be eating regulatory mechanisms, temperament and character styles, and biologic predispositions such as ovarian hormone activity
- chromosome 1 (AN-R) and 10 (BN)- polymorphisms on various candidate genes regulating body
weight, appetite, eating behavior, and serotonin- disconnection in how brain integrates information

Genes and Environment
Genotype can moderate the impact of environmentalpathogens on a person and another variable, e.g., perceived mutuality or social support, can moderate thatgene by environment interaction (Caspi, 2006).
Genes are not our destiny. Resilience, healing andgrowth can be moderated by environmentalfactors.
“Genes load the gun; The environment pulls the trigger.” (Bray, 1986)
Need to understand the impact of disconnections on thedevelopment and maintenance of eating disorders.
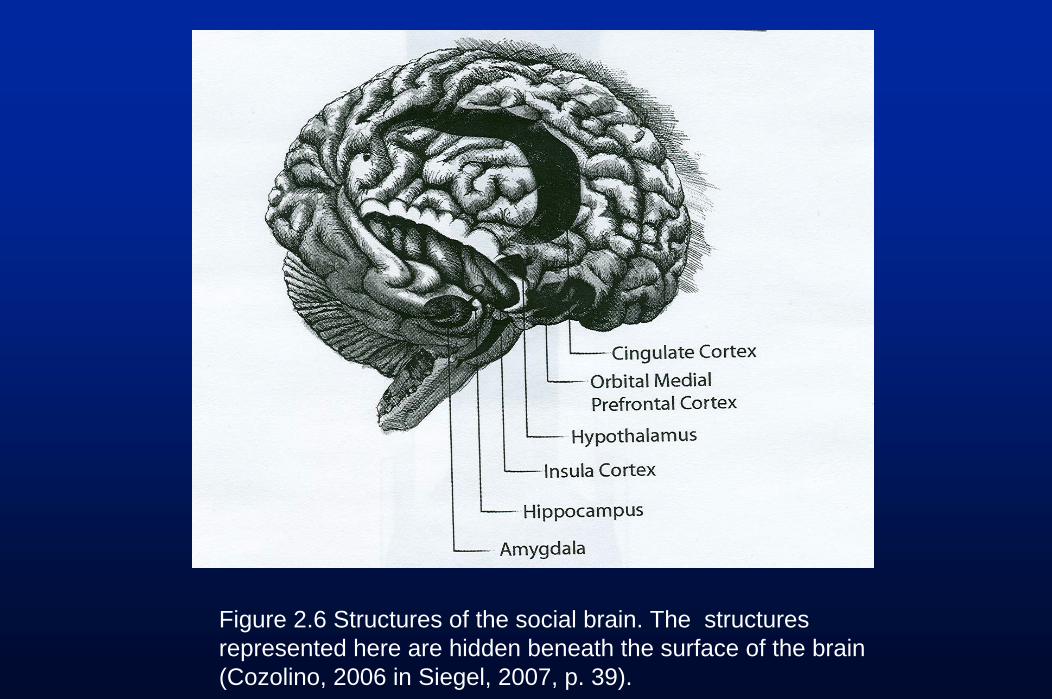
Figure 2.6 Structures of the social brain. The structures represented here are hidden beneath the surface of the brain (Cozolino, 2006 in Siegel, 2007, p. 39).

Disconnections Within the Brain1. Consistent findings:
a) unilateral hypometabolism, predominantly in thetemporal region (66-75%)
b) severe deficits in executive functioning (e.g., cognitiverigidity (poor set shifting) and in visuo-spatial memory(66%)
2. The hypometabolism & cognitive deficits persist at follow up, independent of weight/BMI, mood, EDE
3. There is a significant correlation between thehypoperfusion and the cognitive deficits
(Lask, 2006)

Key Dysfunctions in AN and Their Primary Structures
i) Distorted body image Somato-sensory cortex
ii) Increased anxiety Amygdala
iii) OCD and excessive drive Basal ganglia
iv) Enhanced sense of reward Nucleus accumbens
v) Visuo-spatial deficits Parietal cortex
vi) Executive impairments Frontal cortex
How might these be connected? (Lask, 2006)

Frontal
(executive deficits)
Amygdala
(extreme anxiety)
Parietal Lobe
(visuospatial deficits)
Somato-sensory Cortex
(Distorted BI)
Basal Ganglia
(obsessional drive)
Insula
Nucleus Accumbens(reward)
Hippocampus
(contextual memory)
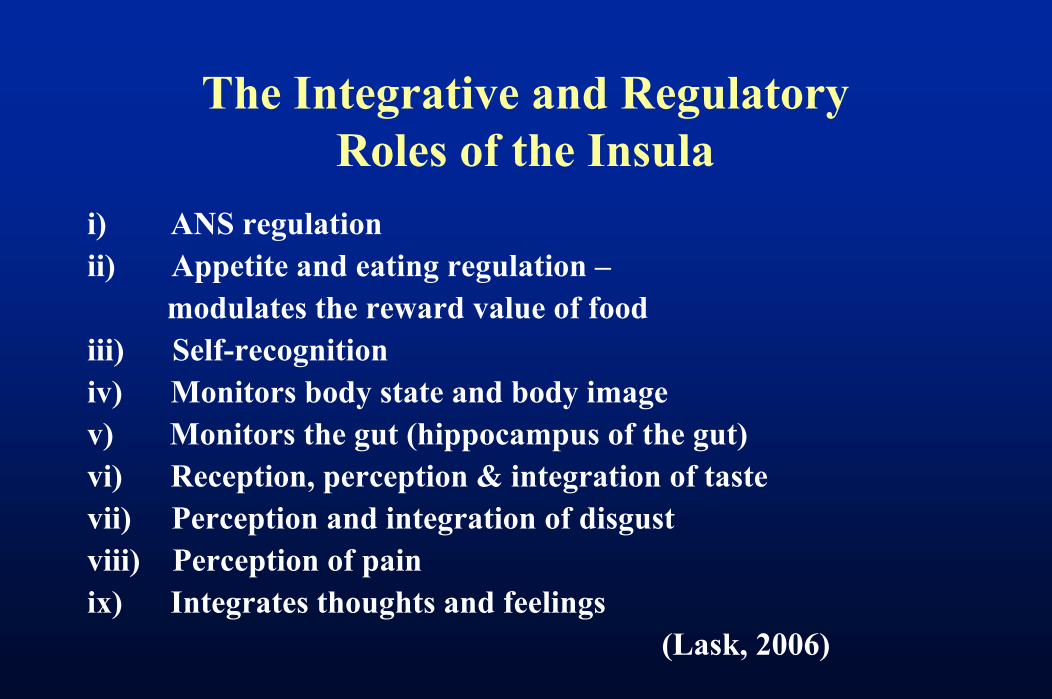
The Integrative and Regulatory Roles of the Insula
i) ANS regulationii) Appetite and eating regulation –
modulates the reward value of foodiii) Self-recognitioniv) Monitors body state and body imagev) Monitors the gut (hippocampus of the gut)vi) Reception, perception & integration of tastevii) Perception and integration of disgustviii) Perception of pain ix) Integrates thoughts and feelings
(Lask, 2006)
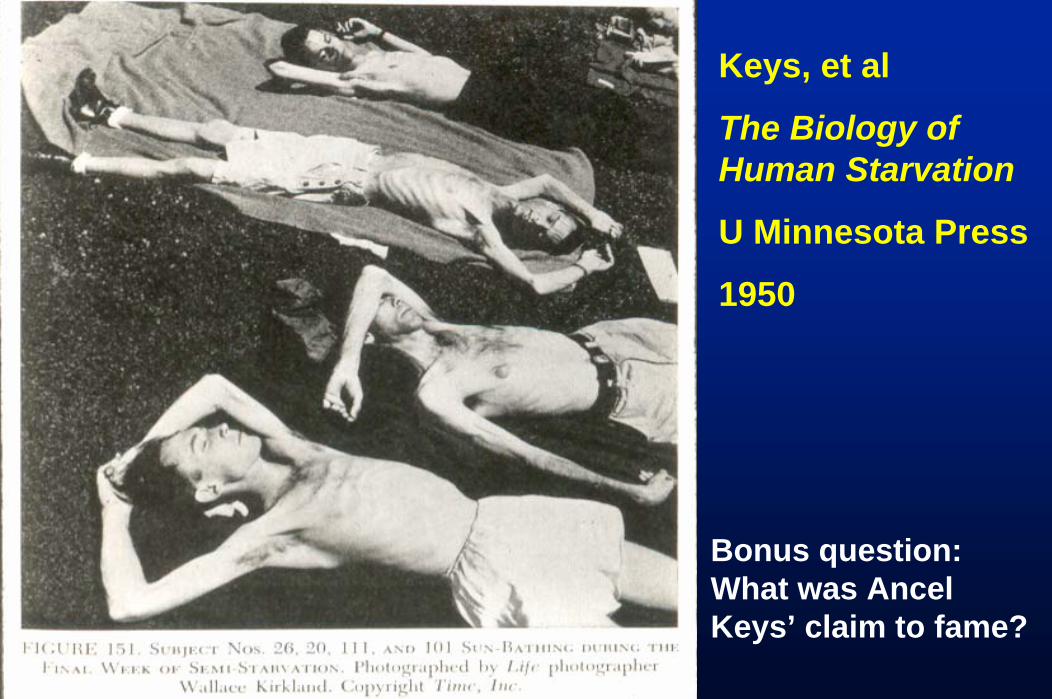
Keys, et al
The Biology of Human Starvation
U Minnesota Press
1950
Bonus question: What was AncelKeys’ claim to fame?

SYMPTOMS OF LOW ENERGY INTAKE (STARVATION)
• Irritability• Depression• Obsessive-Compulsive
traits• Social withdrawal• Conflict• Food related habits• Body image distortion• Loss of appetite
Kreipe, 2005
• Hair• Skin• Headache• Fainting, dizziness• Chest pain• Constipation• Loss of menses• Fatigue, weakness
• Cold intolerance

SIGNS AND SYMPTOMS OF VOMITING OR LAXATIVE ABUSE
Physical health Mental health
• Guilt• Depression• Anxiety• Confusion
Kreipe, 2005
• Weight loss• Electrolyte disturbance
– ↓ K– ↑ CO2
• Dental enamel erosion• Low blood volume• Knuckle calluses
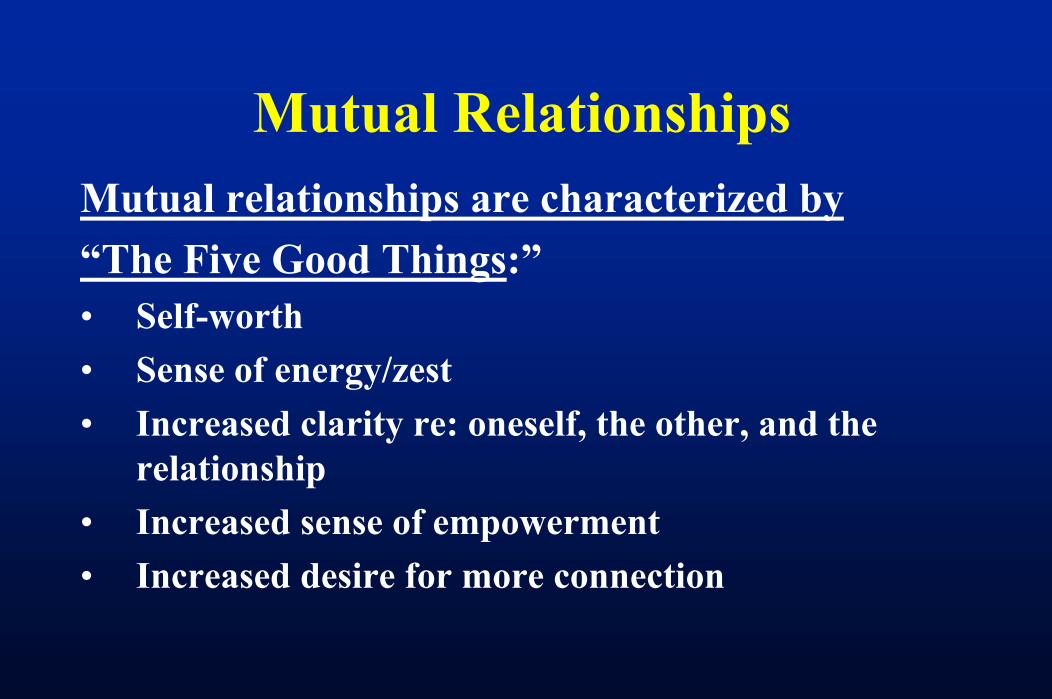
Mutual RelationshipsMutual relationships are characterized by “The Five Good Things:”• Self-worth• Sense of energy/zest• Increased clarity re: oneself, the other, and the
relationship• Increased sense of empowerment• Increased desire for more connection

I YOUWE
Mutual relationships honor the integrity of the connectionbetween people and space for each person in the connection.Mutual relationships allow for difference in connection.

Relational Images and Meanings that Lead to Strategies for Disconnection
Relational Image: When I try to convey myexperience, no one is listening to me.Relational Meaning: This is because I amunlovable, unworthy, defective, to blame.Strategies for Disconnection: (To avoid thepain r/t the above image and meanings and tomaintain available connections) – e.g., eatingdisorder behaviors/thoughts & denial of illness.
My mother called to say she had left my daughter’s birthday cake out on the counter. She said she forgot to put it away. She knew this could be a trigger for me. I said, “That’s OK, mom. It’s too late anyway.” I had already binged on the cake…I didn’t want her to make that cake anyway. My daughter had planned for me to get her a special princess cake, but my mother said she needed to bake her one. She didn’t listen to me. She never listens to me…I guess my binging took care of all that.
(Holly, 1/05)

Disconnecting from Oneself to Maintain Connections
“In situations with family, it’s so inappropriate to have different opinions,…the smallest trace of being different makes it easier to not be liked…I was so cautious of the way I sat and the words I used when I was over there tonight. I didn’t want to make a wrong move, make the wrong comment, or even sit, walk wrong. I have to close off every part of myself when I’m with them. I have to lock it away.”
(Betty, 10/21/03)

Toxic Sociocultural Values• Thinness, ultra-independence, control, appearance,
performance, consumerism, individualism bordering on narcissism, etc.
• Linking control and success with thinness and appearance• Objectifying women’s bodies• Socializing women and men to value themselves from the
outside in• Multiple, ambiguous, and contradictory role expectations for
women • Doing vs. Being (together) e.g., decreased family meals• Emphasis on the “I” and the “me,” not the “we”

Spirituality and Disconnection
• Meaninglessness• Isolation – Condemned isolation• Aloneness
EATING DISORDERS: DISEASES OF DISCONNECTION
Eating disorders are “diseases of disconnection” in which a biogenetically vulnerable individual has difficulty staying connected to and developing an authentic sense of self within relationships with others. This struggle is intensified with the effects of starvation, binging or purging and a culture that emphasizes thinness, appearance, and performance.
Key Evaluation Questions for Eating Disorders
• Any recent changes in weight?• History of weight fluctuations?• What were meals eaten day before
exam? Is this a typical pattern of eating?
• Is the patient binge eating?• Amount of exercise in a week?• Regularity of menstrual periods?• Any compensatory mechanisms?
SCREENING TOOLS FOR WOMEN WITH EATING DISORDERS AND ALCOHOL
USE DISORDERS
SCOFF (Morgan & Lacey, 2000)• Do you make yourself sick because you feel
uncomfortably full?• Do you worry that you have lost control over how
much you eat?• Have you recently lost more than 14 lbs in a 3 month
period?• Do you believe yourself to be fat when others see you
as too thin?• Would you say that food dominates your life?• Each “yes” = 1 point; a score of 2 points indicates a
likely diagnosis of anorexia nervosa.

Eating Disorders: Dispelling Myths
• A patient can have normal lab values and have an eating disorder and be medically compromised
• Realize that a subgroup of patients starve themselves to look like they are in a “normal weight range for height and age.”
• Eating Disorders occur at any weight.

Essential Labs and Studies for Eating Disorders
• Serum electrolytes• Creatinine• BUN• Thyroid Function Test• CBC with differential• Blood glucose level• Urinalysis

Indicated Labs and Studies for Eating Disorders
• EKG• Cardiac ultrasonography• Liver enzymes• Stool specimens - guiac tests• GI radiographic studies• GI endoscopic studies• Serum Amylase• Calcium, Magnesium, Phosphorus• Bone Density Studies

Indicated Labs and Studies for Eating Disorders
• EKG• Cardiac ultrasonography• Liver enzymes• Stool specimens - guiac tests• GI radiographic studies• GI endoscopic studies• Serum Amylase• Calcium, Magnesium, Phosphorus• Bone Density Studies

Female Athlete TriadDisordered Eating
Amenorrhea Osteoporosis
The Female Athlete Triad• Disordered Eating: includes the full spectrum of
abnormal eating behaviors, ranging from simple dieting to clinical eating disorders (American College of Sports Medicine,1997). DE directly and indirectly relates to sports participation. Leads to amenorrhea.
• Amenorrhea: Loss of menstruation – either not having first menstrual cycle (menarche) or missing periods (esp. 3 consecutive cycles). Many causes. A common one is body system energy drain that has the hypothalamus turn off reproductive system. Decreased estrogen leads to osteoporosis.
• Osteoporosis: characterized by low bone mass and deterioration of bone tissue, resulting in bone fragility and increased risk of fracture (National Osteoporosis Foundation, 2003). Decreased estorgen → bone growth.

Female Athlete Triad• Triad usually begins with disordered eating (DE).• DE occurs in all sports, but more frequently in sports
emphasizing thinness/leanness.• DE can negatively affect athletic performance.• Amenorrhea in athletes is often due to an imbalance of eating
and training.• Amenorrhea may be the “norm,” but is not “normal.” • Prolonged amenorrhea can result in loss of bone
(osteopenia/osteoporosis), which in turn,• Increases the risk of fractures, especially stress fractures.• Some of the bone loss may be irreversible.• Good nutrition is a key factor for good health.• Good health is what is necessary for good athletic
performance. (NCAA, 2005)

Female Athlete TriadThe focus in working with the student-athlete who is affected bydisordered eating or has other symptoms of the Triad should bemore on her health and nutrition, and less on her weight.
• Does this focus imply that the athlete’s weight is unimportant?
• Does this focus mean that performance is unimportant? • The answer to both questions is “No;” it simply means that:
Nothing is more important than the athlete’sphysical and mental health.
(NCAA, 2005)

Female Athlete Triad• Attempted weight loss (dieting) is the primary
precursor to an eating disorder (ED) or DE • When a coach or other individual involved with an
athlete’s sport asks that athlete to lose weight, s/he has no way of knowing if the athlete already has an ED or is at risk for developing one.
• Pressure or even a suggestion from a coach to lose weight may significantly increase the individual’s risk of developing an ED or worsen an ED
• Cuts both ways: Perfectionism, compliance, hard-working, compulsiveness, positive connection with coach
(NCAA, 2005)
Risks for DE and the Triad in the SportEnvironment
• Belief that a ↓ in body weight or body fat enhancesperformance
• Sport body stereotypes• The similarity of good athlete traits and DE/eating disorder
symptoms• Presumption of health, based on good performance • Revealing uniforms or sport attire • Competitive thinness (college age & sports performance
related)• Pressures associated with sport (DE = coping strategy)
(NCAA, 2005)

Female Athlete TriadInstead of focusing on weight or body fat to increaseperformance, focus on health, including:
1. Nutrition – Many college students overeat, undereat, binge-eat, are on unhealthy diets, eat low nutrient-dense foods, and eat on unusual schedules. All athletes should be provided with sound nutritional information.
2. Sleep/rest - Many student-athletes are regularly getting fewer than six hours sleep each night. Another factor that decreases resilience and performance.
3. Substance use - (alcohol, prescription drugs, illegal drugs, nicotine, and dietary or “ergogenic” supplements). These can be risky and may be on the NCAA’s banned substance list.
4. Numerous psychological factors (cognitive and emotional) that can affect performance.
A focus in these areas does not put the athlete at risk. These factors can enhance performance by improving physical andpsychological health. (NCAA, 2005)
Female Athlete TriadShould an athlete be judged to be “overweight” basedon an accepted health standard (i.e., body mass indexhealthy range), or based on a profile of elite athletes inher particular sport?
• Because weight is a health issue, a health standard should be used.
• Profile of elite athletes is descriptive, not predictive, i.e., it describes characteristics of successful athletes.
• Conforming to a particular weight/body fat composition does not ensure performance enhancement.
• Profile does not reveal how athletes ate (healthy or restrained eating? Eating disordered?)
(NCAA, 2005)

Approaching the Student with Female Athlete Triad
• Someone in authority• Good relationship with athlete• Easy manner of relating• Convey caring and concern, not criticism• Told privately – focus on health• Inform re: arranged evaluation• Considered “injured” until evaluation complete and
recommendations offered (standard policy)• No training or competition till agreement to evaluation• Convey confidence re: the practitioner• Referral agent meets with practitioner/Collaboration and
Communication
(NCAA. 2005)

CONDITIONS UNDER WHICH THE SYMPTOMATIC ATHLETE SHOULD NOT be
ALLOWED TO TRAIN OR COMPETE
1. Medical condition that precludes sport participation.
2. Meets diagnostic criteria for anorexia nervosa or EDNOS (weight less than 85 percent of recommended standards, fear of weight gain, denial of seriousness of weight loss, body image disturbance).
3. Training or sport participation plays an integral role (used in an unhealthy way) in the disordered eating
(NCAA, 2005)
CONDITIONS UNDER WHICH THE SYMPTOMATIC ATHLETE MIGHT BE ALLOWED TO TRAIN/ COMPETE
1. Has DE, and perhaps BN, but does not meet AN criteria or EDNOS with symptoms similar to AN.
2. Athlete evaluated both medically and psychologically by health-care providers and found not to be at additional risk by training or competing
3. Athlete is in treatment and is progressing.
4. Athlete agrees to, and complies with, a list of health maintenance criteria, including, but not limited to:
-compliance with all treatment appointments and recommendations-especially recommendations regarding eating and weight-energy expenditure accompanied by an adjustment in caloric intaketo maintain therapeutic goals regarding weight gain/maintenance.

Symptomatic Athletes Must Be In TreatmentRecovery without treatment is unlikely • Athlete becomes ↑ isolated from the team, getting ↓ support
and making her DE more difficult to monitor. • Deterioration physically and psychologically at some point.• Her performance will ↓. • Poorer performance ↑ pressure on her, as she often defines
and identifies herself by her athletic performance. • She also worries that her coaches, teammates, family and
friends will be disappointed.• The ↑ pressure leads to a ↑ need for her symptoms, as DE is a
way to deal with pressures in her life.
(NCAA, 2005)

Treatment Improves Athletic Performance and Mindset
When the athlete is well, she should be able to use hertime more efficiently and perform better.
Her DE not only affects her negatively through malnutrition, muscle weakness, and dehydration, italso negatively affects her psychologically byincreasing depression and anxiety, and decreasingconcentration.
(NCAA, 2005)
Prevention Strategies for Coaches toDecrease Risks in the Athletic Environment
1. De-emphasize weight. 2. Do not compare one athlete’s body/performance to another athlete’s
body/performance (the other high performance athlete may have an eating disorder)
3. Remember young women are sensitive about their weight and body image4. Enhance performance without a focus on weight 5. Promote development of mental and emotional skills (imagery, positive
self-talk, goal-setting, mental preparation, mindfulness, and relaxation training)
6. Recognize individual differences in athletes (athlete profiles describe but don’t predict)
7. Increase education of athletes, coaches athletic trainers, and other sport personnel (re: DE, eating disorders, nutrition, Female Athlete Triad)
8. Involvement by Sport Governing Bodies (NCAA).
(NCAA, 2005)
The physical attributes of the athleteestablish the ceiling on performance, the mental and emotional skills of theathlete determine how close she comesto reaching that ceiling.
(NCAA, 2005)

EATING DISORDERSMEDICAL MANAGEMENT
Anorexia Nervosa and Amenorrhea:• 20% experience amenorrhea before onset of
weight loss• 50% experience amenorrhea during dieting• 30% experience amenorrhea only after
substantial weight loss

EATING DISORDERSMEDICAL MANAGEMENT
Anorexia Nervosa and Amenorrhea:• Menses can be expected to resume at a weight
approximately 90%-92% of average body weight for height (Golden, et al. 1997; Kreipe & Mou, 2000)
• May need to gain more weight to ovulate than menstruate
EATING DISORDERSMEDICAL MANAGEMENT
AMENORRHEA:- May take up to 6 months after reaching 90% of
IBW to resolve- A good predictor is reaching a weight 5 lbs abovethe weight at which menses were lost.
- May persist if emotional conflicts go unresolved, as well as continued poor nutrition (low fat intake), and overexercise
- No increased incidence of infertility in recoveredpatients
- Patient can become pregnant despite amenorrhea
(Matos, 2005)
EATING DISORDERS MEDICAL MANAGEMENT
OSTEOPOROSIS- Peak bone mass reached at an early age (17-22)- Achieving optimal peak bone mass depends on:
- Heredity- Eating Disorder disease processes- Lifestyle
- nutrition (low calcium & phosphate; decreasedanimal protein; increased soda pop; highsodium; high caffeine, vegetarian diet)
- cigarette smoking- low physical activity level- increased alcohol- stress-related enhanced cortisol secretion
EATING DISORDERS MEDICAL MANAGEMENT
OSTEOPOROSIS- Long-term risk for any fracture increased by2.9 fold
- Spinal bone density is 2.5 SD below normalin 50% of women with AN
- Young estrogen deficient women can lose 3-5% bone mass/year
- Major bone loss occurs in trabecular bone, i.e., spine vs. cortical bone (arm/hip)

EATING DISORDERSMEDICAL MANAGEMENT
OSTEOPOROSIS- Treat with 400-800 IU/day Vitamin D and 1500 mg/day
Calcium- Ensure proper nutrition, weight gain, and activity level- For refractory cases use biphosphonates or nasal
calcitonin- Estrogen replacement with AN patients is much less
effective than with postmenopausal women

EATING DISORDERSMEDICAL MANAGEMENT
OSTEOPOROSIS- Body weight, esp. fat cell mass, and muscle
strength are positive predictors of bone mineral density in young woman.
“Having an eating disorder is like being in a frying pan surrounded by horrendous flames. On the other side of those flames is recovery. My therapist and others are on the recovery side telling me to step out of the pan into the flames and to walk through the fire to reach recovery. I think to myself, “Are they nuts?!” Don’t they know how frightened I am to step into the fire? It will destroy me. I will die.This frying pan (eating disorder) is safe and protective because I know how to live in it. I know how to “be” in the pan.”
Cindy Nappa Bitter, 2001

Anxiety, fear, and terror can occur as one decides to give up strategies
for disconnection that ensured psychic survival and preservation
of available relationships. (Tantillo, Nappa Bitter, & Adams, 2000)
Stages of Change Model (Prochaska & DiClemente)
• Pre-contemplation: no perceived need to change, denial
• Contemplation: able to consider change, ambivalent
• Preparation: ready to change
• Action: implementation of plan to change
• Maintenance: feedback to maintain change

Processes of Change• Consciousness-raising • Helping Relationships• Social Liberation• Emotional Arousal• Self-reevaluation• Commitment• Countering• Environmental Control• Reward
- Prochaska, Norcross, & Diclemente, 1994
Support for Change in College Health Settings
Consciousness-Raising, Helping Relationships, and Social Liberation•Provide information about
–Illness–Recovery process–How we get in our own way
• Therapeutic relationship (alliance)/support groups and recoveredpeer mentors
• Awareness of influence of language, environment and social norms• Self-monitoring/Journalling (food, emotions, relationships)• Discuss/write about how the eating disorder helps or hinders the
student achieve life goals and live out values.
(Prochaska, Norcross, & DiClemente, 1994)
MOTIVATIONAL PRINCIPLES
• Express empathy• Develop discrepancy• Avoid argumentation• Roll with resistance• Support Self-efficacy
(Miller & Rollnick, 2002)

Women with eating disorders require mutually empathic and empowering
relationships to work through the intense denial, ambivalence, and fear
that keep them stuck in the early stages of change.
(Tantillo, Nappa Bitter, & Adams, 2000)

Moving from Contemplation to Action
I feel I have changed since being in the group. When Ithought of giving up my eating disorder before, I would feel petrified. I would feel the fear right here, like in mychest. I don’t feel that so much anymore. I feel readier togive it up…less frightened. Like I won’t lose all of me if Ido. I used to be afraid that if I gave up the eating disorder,I would lose a sense of me. Like I would vaporize, becomeinvisible…cease to exist. Like without the eating disorder there would be nothingness.
(Missy, 4/2/02)

Healing within a Relational Therapy Approach
• Occurs through development of mutual connections• Understanding the connections between one’s
relationships with food, self, and others• Perceived mutuality = recognizing we impact others
and allowing ourselves to be open to the influence of others
• Patient and therapist grow through interaction• Emphasis on validation, self-empathy, mutuality and
empowerment

Healing within a Relational Therapy Approach
RT promotes development of mutualempathy and empowerment through:• Focus on patient & therapist authenticity• Use of real relationship• Attention to transferential relationship• Use of judicious self-disclosure

Relational/Cultural Theory emphasizes that mutuality involves not only the therapist’s ability to appreciate her/his impact on the patient, but also an openness to being moved by what the patient says and does, and a willingness to convey to the patient that s/he has been moved.
(Miller & Stiver, 1997; Tantillo, Nappa Bitter Adams, 2001).

Therapist Self-Disclosure within a Relational Therapy Approach
Therapist self-disclosure promotes a sense of perceived mutuality because it helps the patient recognize that the therapist has been moved in response to her experience or behavior. This process leads to increased self-empathy as the patient realizes her experience does matter and can be part of relationship (Miller, 1999; Tantillo, 2004).
The therapist’s ability to remain aware of her/his own strategies for disconnection is important for movement with the patient along the entire spiral of change, but is especially critical in helping a patient contemplate and eventually commit to change.
(Tantillo, Nappa Bitter Adams, 2001).
Each dynamic in relationship is viewed as a means of maintaining connection or as a strategy for disconnection (e.g., food restriction, binging, purging, denial of illness, social isolation). These strategies of disconnection are the patient’s response to a central relational paradox , i.e., an intense longing for mutual relationships and a fear of allowing oneself to participate in these relationships because of severe anxiety, past hurts, and violations.
(Fedele, 1994; Tantillo, Nappa Bitter Adams, 2001).

Health Care Provider Approach
• Validation (shame/secrecy)• Direct and specific questions• Don’t assume• Cognitive distortions, reasoning errors (all/nothing thinking,
overgeneralizations, negative mental filtering, etc.)• Be genuine, real (not opaque and distant)• Warmth and humor • Be consistent and persuasive• Educate• Team approach and good communication helps avoid
splitting
A Relational/Motivational Approach to Treatment of Eating Disorders
• Identify patient’s and family’s goals for treatment• Learn the patient’s and family’s language• Raise consciousness re: stages and processes of change in
recovery, the illness, and ways a patient may get in his/her own way.
• Help patient identify where s/he is on spiral ofchange and convey acceptance of this.

A Relational/Motivational Approach to Treatment of Eating Disorders (continued)
• Emphasize careful preparation for change to achieve action and sustained commitment to change
• Discuss and normalize feelings of denial/ambivalence• Acknowledge the adaptive nature of the illness• Identify meanings and purposes of the eating disorder• Acknowledge that changing eating behaviors involves change
in one’s self-concept and relationships.
A Relational/Motivational Approach to Treatment of Eating Disorders (continued)
• Provide a relational reframing of the etiology and maintenance of and recovery from eating disorders
• Empathize with patient’s strategies for disconnection, while holding out the possibility that the illness may not be allowing her/him to meet life goals.
• Teach self-monitoring (identify connections among relationships with self, others, and food/the illness)
• Examine pros and cons of continuing or stopping eating disorder behaviors

A Relational/Motivational Approach to Treatment of Eating Disorders (continued)
• Examine discrepancies between patient’s life goals/values and what they actually accomplish and experience with the illness
• Foster emotional arousal related to discrepancies and the negative effects of the eating disorder
• Examine the growth-fostering potential of patient’s relational environments
• Identify supports/resources for recovery• Educate patients and families re: enabling vs. helping
relationships
A Relational/Motivational Approach to Treatment of Eating Disorders (continued)
• Discuss the difference between mutual and non-mutual relationships. Encourage relationships that allow the patient to differentiate within and deepen connection
• Discuss how a lack of perceived mutuality in relationships obstructs commitment to change
• Educate how healing and growth occur in the context of connections with oneself and others
• Discuss pros/cons of maintaining non-mutual relationshipsand related changes

A Relational/Motivational Approach to Treatment of Eating Disorders (continued)
• Acknowledge the patient’s strengths in terms of caring for others while also encouraging a balance between self-care and care for others
• Review personal choices in terms of patient’s eating disorder and how these are congruent or incongruent with their overall life goals
• Introduce techniques for self-reevaluation (e.g., evaluation of present (negative consequences of the illness), as well as a forward looking assessment (a healthier and changed view of oneself).
• Emphasize the importance of thinking before acting, identifying all/nothing thinking, creating a new image of oneself in relationships with others without illness, and making realistic, informed decisions.

Moving from Contemplation to Action (continued)
Now after being in group, I feel like I am still in the dark,but I am not so scared about being there. It’s like when you close your eyes and you see darkness, but there is a light on in the room. It’s not as dark…I am not asscared now. I still don’t know where I am going or what comes next or what’s out there or who or what I will be.But at least I am not as scared to find these things out and to move in a new direction.
(Missy, 4/2/02)

Potential Obstacles/Challenges in Referring and Managing Students with Eating Disorders
• School personnel anxiety, lack of educationand training
• Inconsistency/Lack of communicationamong school personnel (e.g., coach and health services, mental health), with family, and/or with outside professionals
•Family Shame/Assumption of Blame,Parental anger or denial

Potential Obstacles/Challenges in Referring and Managing Students with Eating Disorders
(continued)
• Not understanding that the Eating disorder decreases the student’s ability to make healthy decisions (they are adults but are impaired)
• Lack of a trusted person to routinely eat with the student and monitor intake
• Lack of routine check-in meetings with all team members and student/family
Referral to and Collaboration with Mental Health Care Providers
• Identify individuals/programs in your area and know their treatment model www.nyeatingdisorders.org
• Frame therapist as specialist who helps you help the patient – Psychiatrist--medication, hospitalization, therapy– Psychologist--psychological testing, therapy– Social Worker, Nurse Therapist, Counselor--therapy
• Identify specific problems prior to referral• Cognitive-behavioral therapy/Relational Therapy • Family Therapy key in treatment of A.N. especially with
adolescents and young adults(Kreipe, 2005)
Referral to and Collaboration with Mental Health Care Providers
• Be confident about the referral with the studentand family.
• Emphasize the need for consultation for you, thestudent, and family.
• Reinforce the student is not crazy.• Focus on the interplay between mind and body.• Educate the student/family re: a psychiatric
evaluation.

Referral to and Collaboration with Mental Health Care Providers (continued)
• Say why you have chosen a particulartherapist/consultant/provider.
• Negotiate the kind of collaborative relationship and communication you wouldlike to have on the treatment team.
• Specify roles and responsibilities (weekly weigh-ins, lab work, lunch supervision, etc.).

Referral to and Collaboration with Mental Health Care Providers (continued)
• Ensure good communication with team members in school (e.g. school nurse, coach,counselors, teachers, etc.)
• Maintain consistency of treatment plan.• Clearly identify for student and family
supportive school personnel.• Set up check-in times with team and
student/family.
Collaboration among School Personnel, Mental Health Providers, and Family
• Externalize the illness.• Use an empowering and non-blaming/non-shaming approach with student and family.
• Decrease isolation and refer families to Eating Disorders Network Support Meetings andstudents to support groups
• Encourage parents to work as a team and as collaboratively as possible with the student (more challenging with AN - parents encouraged to take charge of refeeding till student is more stable when students are ill < 3 yrs and < 19 yrs of age)

Collaboration among School Personnel, Mental Health Providers, and Family
• Validate the burden incurred by the illness. • Educate and share information• Encourage parents get respite and support for themselves.
• Monitor for strain on all family members, e.g., siblings.
• Encourage student and family to connect in ways that don’t involve the eating disorder.
• Remember that high expressed emotion is not helpful for the student.
• Foster communication/problem-solving skills.• Clarify roles of all adults involved with the
patient.

Get Real HelpHow to help a student:
• Trust your concerns• Share your concerns in a supportive and warm way• Mention specific examples (discussion from your interviews and observations/reports from others)
• Share your feelings about what you have observed,discussed and heard from others
• Be prepared with resources: - www.nyeatingdisorders.org- www.NationalEatingDisorders.org- NEDA Information & Referral Helpline: 800.931.2237
© 2003-2005 National Eating Disorders Association - www.NationalEatingDisorders.org