Early Diagnosis and Treatment of STEMI - UH EMS-Institute · 3/24/2011 1 Early Diagnosis and...
19
3/24/2011 1 Early Diagnosis and Treatment of STEMI Use and Impact of Pre-Hospital Electrocardiogram John Coletta, M.D., F.A.C.C. Disclosures • None Case • 75 yo called EMS for chest pain – Onset of pain less than 1hr – Upon EMS arrival patient was hemodynamically stable. – Patient was administered ASA 325mg and oxygen – Pre-hospital ECG was performed
Transcript of Early Diagnosis and Treatment of STEMI - UH EMS-Institute · 3/24/2011 1 Early Diagnosis and...

3/24/2011
1
Early Diagnosis and Treatment of STEMI
Use and Impact of Pre-Hospital Electrocardiogram
John Coletta, M.D., F.A.C.C.
Disclosures
• None
Case
• 75 yo called EMS for chest pain– Onset of pain less than 1hr– Upon EMS arrival
patient was hemodynamicallyp y ystable.
– Patient was administered ASA 325mg and oxygen
– Pre-hospital ECG was performed

3/24/2011
2
Case
Case
• ECG transmitted to St John Medical Center
• Cath Lab activated…
Introduction
• “This is 911, what is your emergency?...”
• Scope of the problem:– Estimated 500,000 cases of STEMI each year
nationwide
– 1/3 of patients with STEMI will die in the first 24hrs from the onset of ischemia
Antman EM, Anbe DT, Armstrong PQ, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). 2004. Available at www.acc.org/clinical /guidelines/stemi/index.pdf
3/24/2011
3
Introduction
• Scope of the problem: (cont’d)
– About half (53%) of patients with STEMI utilized EMS for transfer to the hospitalEMS for transfer to the hospital
• 16% DROVE THEMSELVES
– 1 in 300 patients transferred to the hospital by private vehicle suffer cardiac arrest en route
Antman EM, Anbe DT, Armstrong PQ, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). 2004. Available at www.acc.org/clinical /guidelines/stemi/index.pdf
Outline
• Definitions
• Cause
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case
Outline
• Definitions– ST Elevation
– STEMI
Thromb s– Thrombus
• Cause
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case

3/24/2011
4
Definitions
• ST Elevation Myocardial Infarction
– Occlusion of epicardial coronary vessel resulting in transmural infarction of myocardium
• Cell death / necrosis
– Identified by history and ECG• ECG
– Changes suggestive of STEMI in 2 contiguous leads– New left bundle branch block
Definitions
• What is ST elevation?– Elevation of the ST segment above the TP segment
TP segment no electrical acti it– TP segment – no electrical activity• Line drawn between consecutive TP segments defines
the “baseline”
TP P T
Electrocardiogram

3/24/2011
5
Definitions
• Thrombus
– Complex of platelets, thrombin and fibrin
– Similar to a brick wall• Bricks = platelets
• Mortar = fibrin and thrombin
Outline
• Definitions
• Cause– Plaque rupture
Th b f i– Thrombus formation
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case

3/24/2011
6
Cause
• Thrombus– Found in >90% of patients with STEMI
– Found in 35-70% of patients with USA/NSTEMI
Antman EM, Anbe DT, Armstrong PQ, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). 2004. Available at www.acc.org/clinical /guidelines/stemi/index.pdf
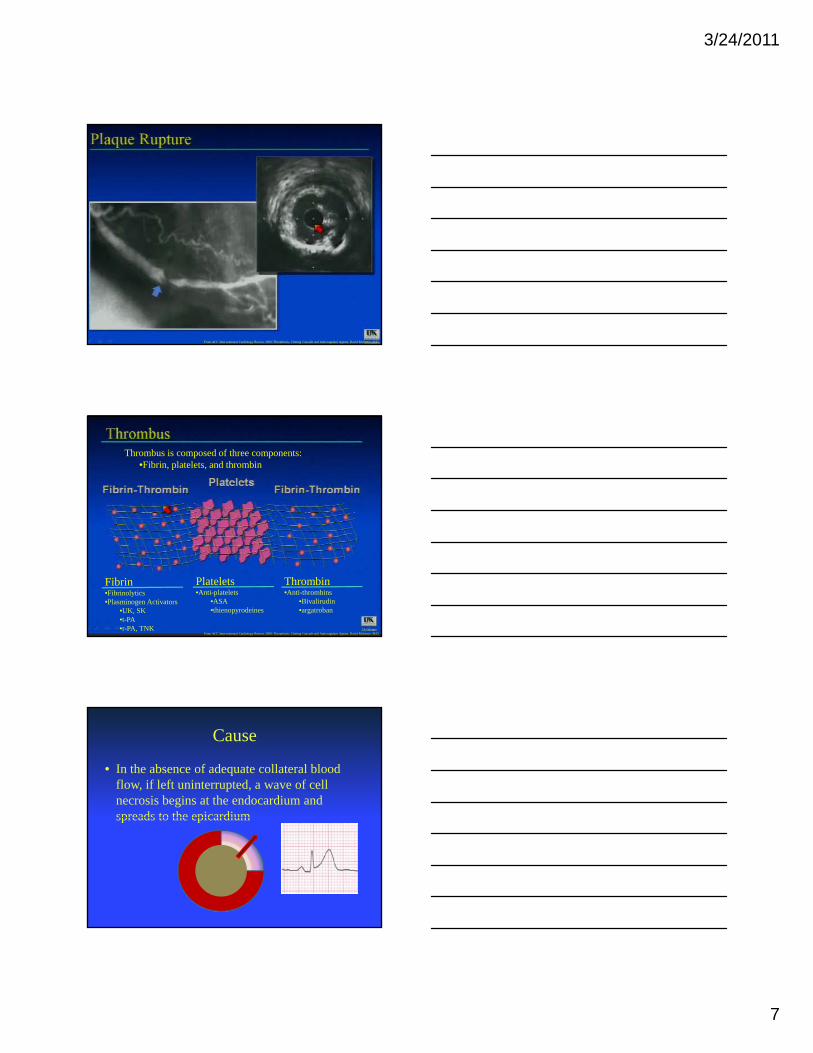
Thrombus
• Abrupt rupture of lipid rich plaque
• Presentation of plaque contents to bloodstream
• Activation of platelets and coagulation cascade
• Thrombus formation
• Abrupt occlusion of epicardial coronary artery
Progression of Plaque Formation
Antman EM, Anbe DT, Armstrong PQ, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). 2004. Available at www.acc.org/clinical /guidelines/stemi/index.pdf
3/24/2011
7
From ACC Interventional Cardiology Review 2008: Thrombosis, Clotting Cascade and Anticoagulant Agents, David Molireno, M.D.
Thrombus is composed of three components:•Fibrin, platelets, and thrombin
Fibrin•Fibrinolytics•Plasminogen Activators
•UK, SK•t-PA•r-PA, TNK
Platelets•Anti-platelets
•ASA•thienopyrodeines
Thrombin•Anti-thrombins
•Bivalirudin•argatroban
From ACC Interventional Cardiology Review 2008: Thrombosis, Clotting Cascade and Anticoagulant Agents, David Molireno, M.D.
Cause
• In the absence of adequate collateral blood flow, if left uninterrupted, a wave of cell necrosis begins at the endocardium and spreads to the epicardiumspreads to the epicardium

3/24/2011
8
Outline
• Definitions
• Cause
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case
Survival
• Despite many advances in treatment there is an abysmal change in overall mortality for STEMI patients
• First described in 1967, the Killip classification is a fast and simple tool for determining in-hospital mortality
Survival

3/24/2011
9
One Year Mortality
Cardiac Survival
• Relationship of door-to-balloon time to cardiac survival in patients treated for STEMI with primary percutaneous coronary intervention

3/24/2011
10
Pre-Hospital ECG (phECG)
• Symptom onset to reperfusion1. Symptom onset to EMS arrival
2. EMS arrival-to-hospital arrival
3 Hospital arri al to diagnostic ECG3. Hospital arrival-to-diagnostic ECG
4. Diagnostic ECG-to-drug/balloon
• Overwhelming evidence that phECG can reduce the time to reperfusion

3/24/2011
11
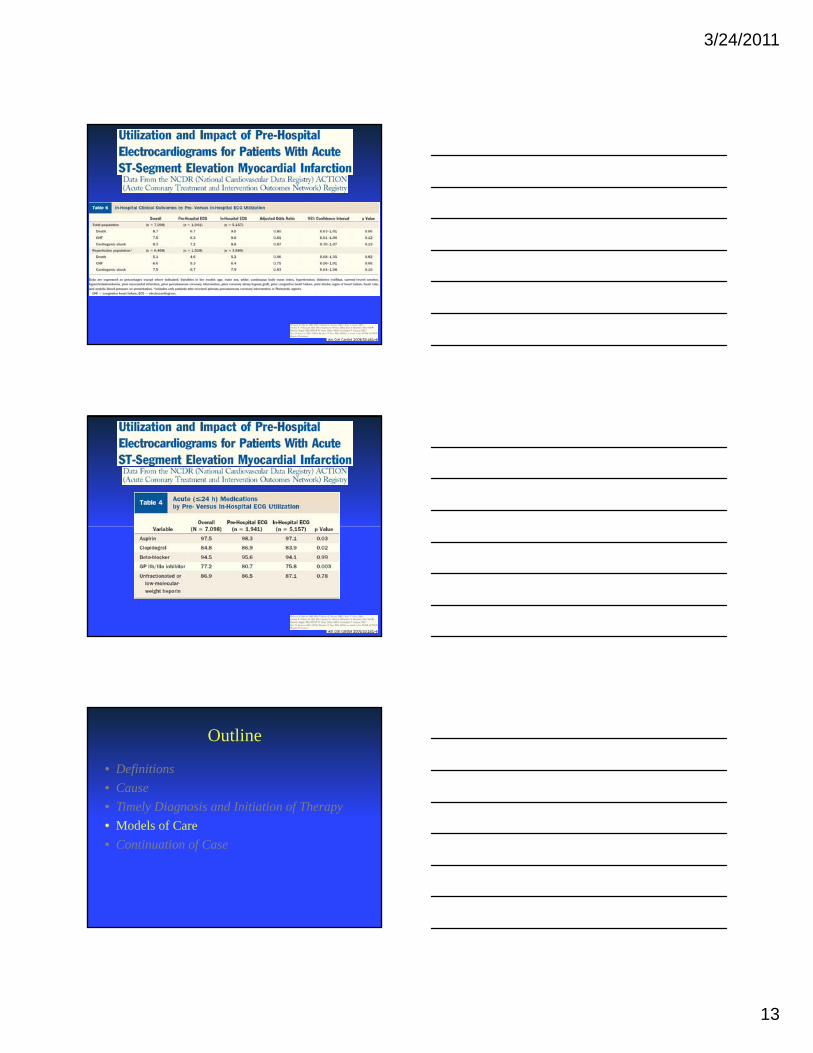
• A significantly higher proportion of patientsproportion of patients with phECG fell within guideline timelines
GREAT! … RIGHT!?
• In 2007, of all patients transported to hospitals
by EMS for STEMI only 27% utilized phECG

3/24/2011
12
Pre-Hospital ECG (phECG)
• Symptom onset to reperfusion1. Symptom onset to EMS arrival
2. EMS arrival-to-hospital arrival
3 Hospital arri al to diagnostic ECG3. Hospital arrival-to-diagnostic ECG
4. Diagnostic ECG-to-drug/balloon
• Overwhelming evidence that phECG can reduce the time to reperfusion
3/24/2011
13
Outline
• Definitions
• Cause
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case

3/24/2011
14
Models of Care
Can EMS Obtain ECG
• 90% of EMS serving largest 200 US cities have ECG available in ambulance
f h CG h l b h O• Use of phECG has recently been shown NOTto increase time from symptom onset to hospital arrival
Can EMS Interpret / Communicate ECG

3/24/2011
15
Barriers to phECG Programs
• Cost– Upgrading equipment
• Acquisition, transmission, receiving
– Training– Training
• Risk of bypassing ER– Misdiagnosis
• Intracranial hemorrhage
• Aortic dissection
Barriers to phECG Programs
• Patient – reluctance to call 9-1-1
• EMS– In whom do we obtain a phECG?
• ~5% pts calling EMS for CP have STEMI
• Which symptoms warrant phECG
Barriers to phECG Programs
• Other thoughts…– Will PCI-capable hospitals benefit financially from
patients being diverted from non-PCI-capable facilities
– No specific reimbursement for phECG• If changed, would this lead to overuse
– Who will oversee this use?

3/24/2011
16
Decreasing Door-to-Balloon
Outline
• Definitions
• Cause
• Timely Diagnosis and Initiation of Therapy
• Models of Care
• Continuation of Case
Case
• 75yo with chest pain…
• EMS arrival 1740
• ECG 1744
• Arrival to SJMC 1758…

3/24/2011
17
99% Mid Left Circumflex

3/24/2011
18
Case
17501750
1810
1820
1825
Case

3/24/2011
19
Case
Summary
• STEMI caused by abrupt vessel closure– >90% due to thrombus
• Rapid restoration of flow is associated with decreased morbidity and mortality
• Despite a ailabilit phECG are nder sed in the• Despite availability phECG are underused in the US
• Use of phECG is associated with decreased door to treatment times
• Most importantly, phECG shows significant trends to decreased morbidity and mortality
Thank You
![Cycle 8 report draft 3 - COnnecting REpositories(STEMI) [M] Patients with prehospital diagnosis of STEMI (confirmed on ECG) MC Care bundle for STEMI (M1 + M2 + M3 + M5) Exception to](https://static.fdocuments.us/doc/165x107/5e3775c3f813a914420739db/cycle-8-report-draft-3-connecting-repositories-stemi-m-patients-with-prehospital.jpg)