Early Detection of Hospitalized Patients with Previously...
27
Early Detection of Hospitalized Patients with Previously Diagnosed Obstructive Sleep Apnea Using Computer Decision Support Alerts R. Scott Evans, Vrena B. Flint, Tom V. Cloward, William Beninati, James F. Lloyd, Kimberly Megwalu, Kathy J. Simpson, Ahmed M. Alsharit, Shayna B. Balls, Robert J. Farney Intermountain Healthcare Salt Lake City, Utah Evans RS, et al. Stud Health Technol Inform 2013;192:505‐9. 1
-
Upload
duongtuyen -
Category
Documents
-
view
217 -
download
1
Transcript of Early Detection of Hospitalized Patients with Previously...

Early Detection of Hospitalized Patients with Previously Diagnosed
Obstructive Sleep Apnea Using Computer Decision Support Alerts
R. Scott Evans, Vrena B. Flint, Tom V. Cloward, William Beninati, James F. Lloyd, Kimberly Megwalu, Kathy J. Simpson, Ahmed M. Alsharit,
Shayna B. Balls, Robert J. Farney
Intermountain HealthcareSalt Lake City, Utah
Evans RS, et al. Stud Health Technol Inform 2013;192:505‐9.
1

Obstructive Sleep Apnea
• OSA: worldwide problem affecting 2‐14% of the general population…most patients remain undiagnosed. Higher in hospitalized patients?
• OSA patients are at elevated risk for hypoxemia, cardiac arrhythmias, cardiorespiratory arrest, heart failure, stroke and death during hospitalization.


Obstructive Sleep Apnea• Positive airway pressure (PAP) is the therapy of
choice for the treatment of hospitalized patients with OSA.
• Providing proper PAP therapy to hospitalized patients depends upon early recognition of OSA.

Obstructive Sleep Apnea
• Clinical screening questionnaires are used to identify hospitalized patients with OSA; especially before surgery
• Moreover, many patients are admitted to the hospital with a previous diagnosis of OSA that is not reported.

Obstructive Sleep Apnea• Thus, many patients with OSA do not receive
appropriate therapy during hospitalization due to the lack of information from previous inpatient and outpatient encounters.
• Large enterprise data warehouses (EDWs) provide the ability to monitor patient encounters over wide geographical areas.

Background• Intermountain Medical Center (IMC) is a 456‐bed
teaching hospital and is Intermountain Healthcare’s (IH) Level One trauma facility
• IH is comprised of 22 hospitals, 197 clinics, instacares, physician offices and home health.


Background• Integrated EMR contains most clinical information
including bedside charting by respiratory therapy.
• Extensive EDW where most clinical and business information is updated every night from all inpatient and outpatient facilities and provides the ability to generate decision support alerts as soon as patients are admitted.

Data Driver


Study DesignJanuary 2012 through October 2012
• PAP if patients wore a PAP mask at home, if their medical history reflected a PAP prescription or O2
recommended. • Respiratory therapy director and a nurse practitioner
from the sleep medicine service followed up and documented the respiratory therapy evaluation and patient visits for 500 patients alerted as having previous documentation of OSA.

Category 2012N (%)
2011N (%)
Total patients 18150 17545Patients with OSA documentation 5037 (28) 4733 (27)
Av. age; yr 63.2 62.8Female 2270 (45) 2108 (45)Av. days of hospitalization 4.25 4.8Av. cost of hospitalization 16138 15738Received respiratory therapy 1975 (39)* 1676 (35)SPO2 < 90% 2358 (47)** 2350 (50)SPO2 < 90% & > 24 hrs after
admission1858 (37)** 1902 (40)
Transferred to ICU 293 (5.8) 268 (5.7)Expired 93 (1.8) 111 (2.3)
Comparison of patients with (2012) and without (2011) OSA Monitor Alerts
* P < 0.0002. **P < 0.006.

Placed on PAP 1671 (33)* 1396 (29)Av. days to PAP placement 1.1 1.2Total days of PAP use 4634 4729Av. days of hospitalization 4.7 5.5Av. cost of hospitalization 16784 17063SPO2 < 90% 933 (56)# 845 (61)SPO2 < 90% & > 24 hrs after
admission780 (47)## 735 (53)
Transferred to ICU 112 (7) 96 (7)Expired 12 (0.7) 18 (1.3)
Category 2012N (%)
2011N (%)
* P < 0.0002. # P < 0.03. ##P < 0.002

Not placed on PAP 3366 (67) 3337 (71)
Av. days of hospitalization 3.9 4.0
Av. cost of hospitalization 14802 13858
SPO2 < 90% 1425 (42)# 1505 (45)
SPO2 < 90% & > 24 hrs afteradmission
1078 (32)** 1167 (35)
Transferred to ICU 181 (5) 172 (5)
Expired 81 (2.4) 93 (2.8)
Category 2012N (%)
2011N (%)
**P < 0.006. # P < 0.03.
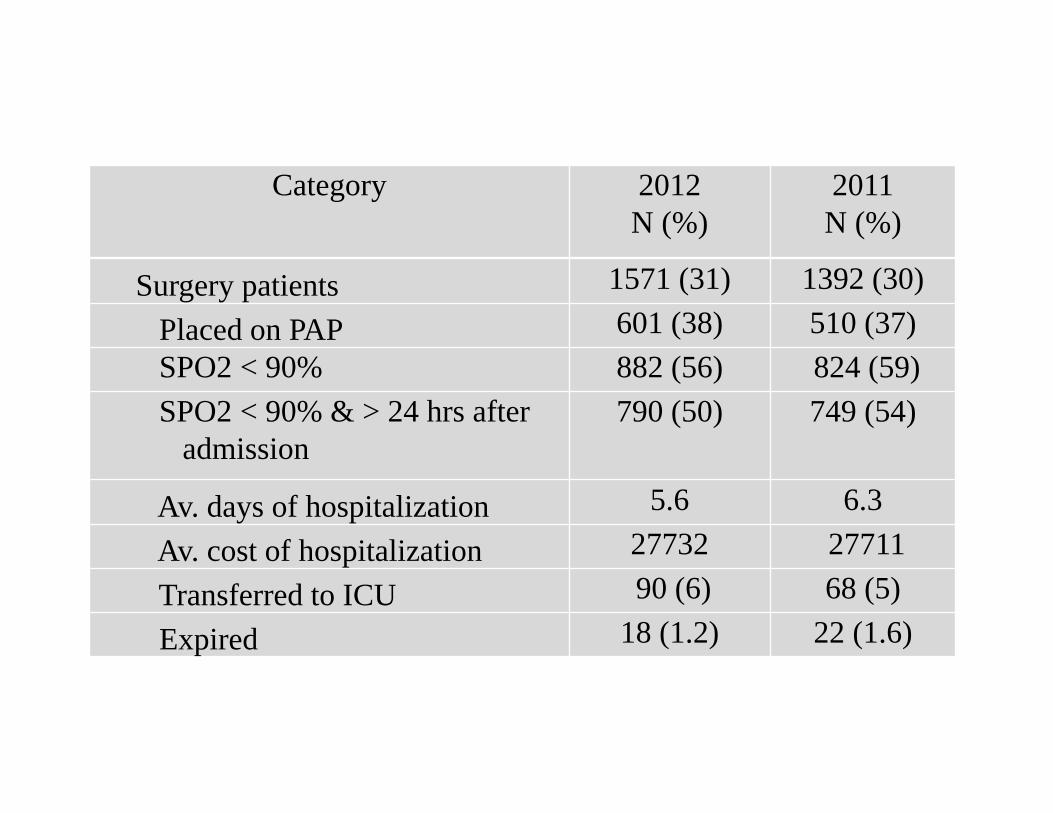
Surgery patients 1571 (31) 1392 (30) Placed on PAP 601 (38) 510 (37)SPO2 < 90% 882 (56) 824 (59)SPO2 < 90% & > 24 hrs after
admission790 (50) 749 (54)
Av. days of hospitalization 5.6 6.3 Av. cost of hospitalization 27732 27711Transferred to ICU 90 (6) 68 (5) Expired 18 (1.2) 22 (1.6)
Category 2012N (%)
2011N (%)

Category 2012N (%)
2011N (%)
Non-surgery patients 3466 (69) 3341 (70)
Placed on PAP 1070 (31) * 886 (27) SPO2 < 90% 1476 (43)** 1526 (46) SPO2 < 90% & > 24 hrs after
admission1068 (31)** 1153 (35)
Av. days of hospitalization 3.6 4.1
Av. cost of hospitalization 11412 11982
Transferred to ICU 203 (6) 200 (6)
Expired 75 (2.2) 89 (2.7)* P < 0.0002. **P < 0.006.

Category 2012N (%)
2011N (%)
Total MET calls 148 181Patients with OSA documentation 44 (30) 63 (35)
MET = medical emergency team
(19 fewer OSA patients, 11% decrease; p = 0.4068).

500 OSA alerted patients followed by respiratory director and nurse practitioner from the sleep service
• 141 (28%) were placed on PAP‐50 (36%) requested by RT.
• 113 (23%) patients admitted to having OSA but declined PAP because of the discomfort.
• 92 (18%) denied having OSA although they did have previous ICD9 coding documenting otherwise.
• 14 (3%) patients were subsequently placed on a ventilator.

SUMMARY1. OSA is highly prevalent and undertreated in
hospitalized patients.2. Computer alerts resulted in significantly more OSA
patients receiving appropriate medical care and significantly fewer experienced hypoxemia.
3. The impact was greater for non‐surgery patients compared to surgery patients.
4. Installed at 12 other IH hospitals with RT Depart.5. Installed at all 22 hospital as required by the IH
Opiod Safety Committee.

OSA/Asthma/COPD Risk pts for the past 12 HrsRunTime: 10/30/2014.18:00
Name EMPI Account Admit Age Sex Room R.E.T. BMI Opioids P-OSA P-Asthma P-COPD FEV1 FVC FEV1/FVC
Respiratory Evaluate and Treat
11/01/2013 to 10/31/2014OSA: 31,494OSA & Asthma: 5,990OSA & COPD: 4,198OSA & Asthma & COPD: 1,573
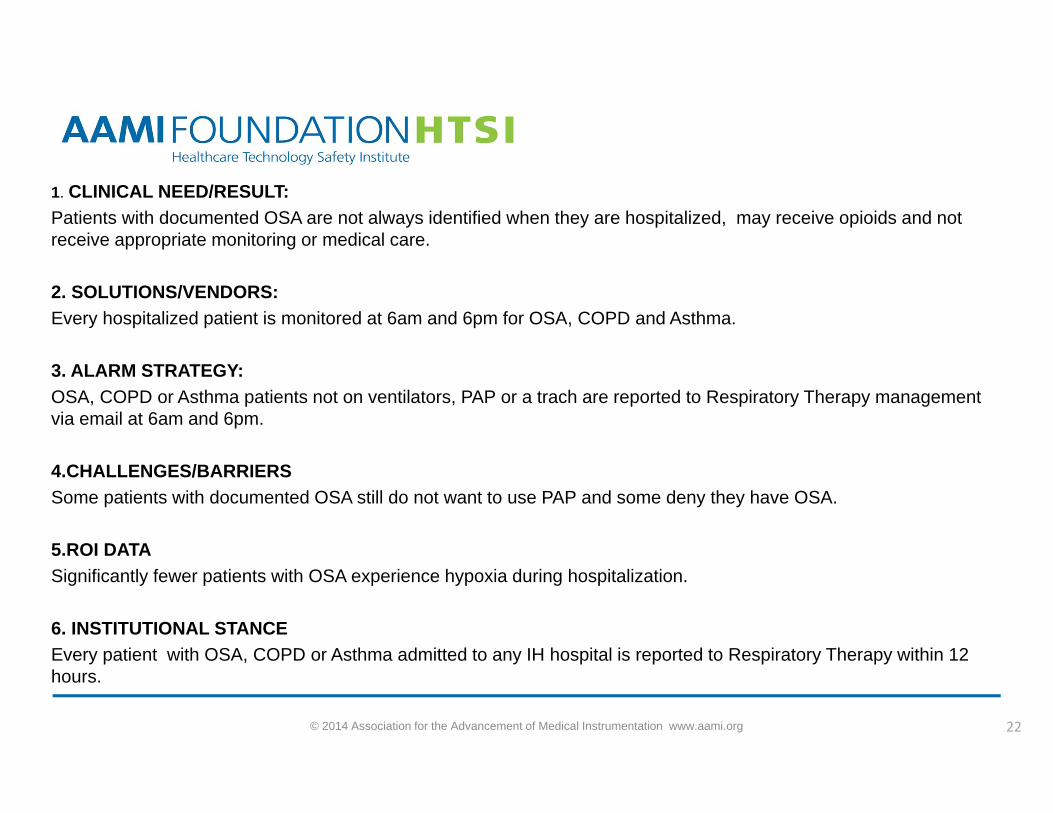
1. CLINICAL NEED/RESULT:Patients with documented OSA are not always identified when they are hospitalized, may receive opioids and not receive appropriate monitoring or medical care.
2. SOLUTIONS/VENDORS: Every hospitalized patient is monitored at 6am and 6pm for OSA, COPD and Asthma.
3. ALARM STRATEGY:OSA, COPD or Asthma patients not on ventilators, PAP or a trach are reported to Respiratory Therapy management via email at 6am and 6pm.
4.CHALLENGES/BARRIERSSome patients with documented OSA still do not want to use PAP and some deny they have OSA.
5.ROI DATASignificantly fewer patients with OSA experience hypoxia during hospitalization.
6. INSTITUTIONAL STANCEEvery patient with OSA, COPD or Asthma admitted to any IH hospital is reported to Respiratory Therapy within 12 hours.
© 2014 Association for the Advancement of Medical Instrumentation www.aami.org 22



STOP BANG Questionnaire1. Snoring: Do you snore loudly (louder than talking/enough to be heard through closed
doors)?
2. Tired: Do you often feel tired, fatigued, or sleepy during daytime?
3. Observed: Has anyone observed you stop breathing during your sleep?
4. Blood pressure: Do you have or are you being treated for high blood pressure?
5. BMI: BMI more than 35 kg/m2?
6. Age: Age over 50 yr old?
7. Neck circumference: Neck circumference greater than 40 cm?
8. Gender: Gender male?
High risk of OSA: answering yes to three or more.


OSA patients placed on PAPBoth study years
Average age (62.8 vs. 63.2)
Percent female (40 vs. 47; p < 0.0001)
BMI (38.47 vs. 35.45; p< 0.03)
Charlson comorbidity scores (5.9 vs. 5.9)
Patient choice and lack of knowledge of potential harm