EARLY CHILDHOOD OUTCOMES AT THE BOTSWANA- BAYLOR CHILDREN’S CLINICAL CENTRE OF EXCELLENCE: A...
20
EARLY CHILDHOOD OUTCOMES AT THE BOTSWANA-BAYLOR CHILDREN’S CLINICAL CENTRE OF EXCELLENCE: A REPORT TO THE WHO TECHNICAL REFERENCE GROUP ON PEDIATRIC CARE AND TREATMENT, APRIL 2008 Gabriel M. Anabwani, Executive Director Elizabeth Lowenthal, Associate Director Michelle Eckerle, Pediatric AIDS
-
Upload
melvyn-hugh-maxwell -
Category
Documents
-
view
217 -
download
0
Transcript of EARLY CHILDHOOD OUTCOMES AT THE BOTSWANA- BAYLOR CHILDREN’S CLINICAL CENTRE OF EXCELLENCE: A...

EARLY CHILDHOOD OUTCOMES AT THE BOTSWANA-BAYLOR CHILDREN’S CLINICAL CENTRE OF
EXCELLENCE:A REPORT TO THE WHO TECHNICAL REFERENCE GROUP
ON PEDIATRIC CARE AND TREATMENT, APRIL 2008
Gabriel M. Anabwani, Executive DirectorElizabeth Lowenthal, Associate DirectorMichelle Eckerle, Pediatric AIDS Corps Doctor

Botswana - BackgroundParameterParameter Total or EstimateTotal or Estimate
Population 1,719,996
HIV prevalence in pregnancy 32.4 % (2006)
HIV+ pregnant women delivering per yr 14,215 (2006)
± infant infections per yr without PMTCT 4500
± Current new infant infections per year 900 (2005)
± HIV infected Children <15 yr on ART 6831
Neonatal/Infant/Child mortality rates 33/70/150 per 1000
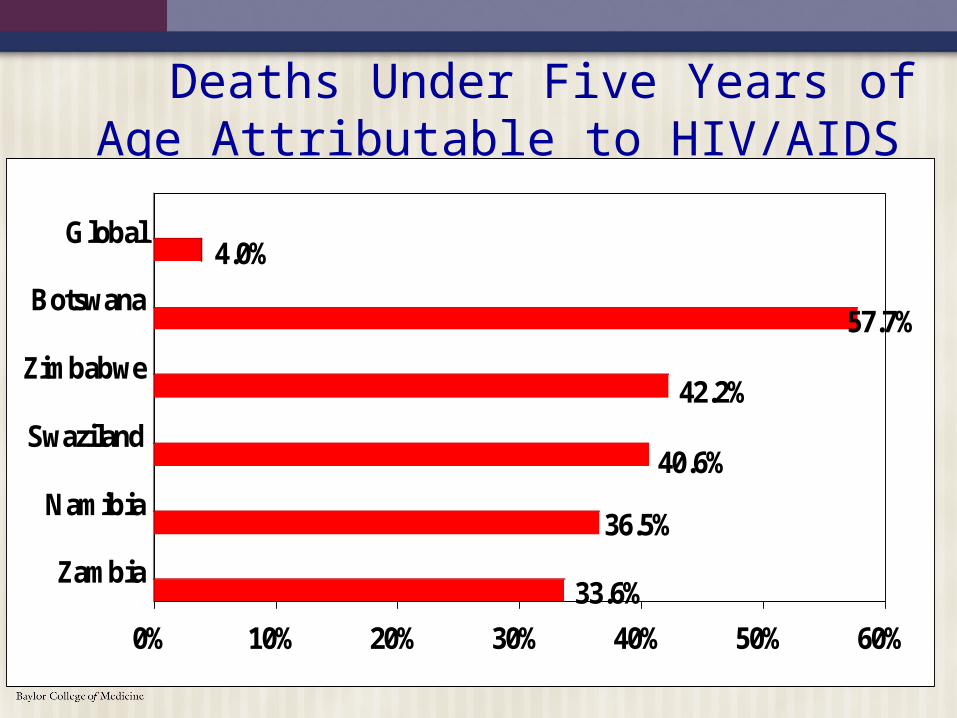
Deaths Under Five Years of Age Attributable to HIV/AIDS
33.6%
36.5%
40.6%
42.2%
57.7%
4.0%
0% 10% 20% 30% 40% 50% 60%
Zambia
Namibia
Swaziland
Zimbabwe
Botswana
Global

Percent of all HIV-positive pregnant women receiving antiretroviral drugs during pregnancy, and changes to drug regimen
Botswana National PMTCT Program, 2002-2006 (Denominator=total number of deliveries x HIV prevalence from surveillance data)
0
10
20
30
40
50
60
70
80
90
100
2002 2003 2004 2005 2006
Year
Per
cen
t re
ceiv
ing
dru
g
AZT (or HAART)
NVP (or HAART)
HAART*
*20-25% of pregnant women are eligible for ARV therapy during pregnancy (CD4<200)
Short-course AZT + SD NVP
Long-course AZT + SD NVP
Short-course AZT only
Source: Situation Analysis (March 2006)

Early Childhood Outcomes
Management According to Botswana National ART Guidelines All received AZT/d4T + 3TC + NVP Criteria: all children <12 months with confirmed HIV
infection (DNA PCR) or >12 months with mild/moderate or severe immune suppression or clinical manifestations
Children initiated on HAART at <36 months of age Outcomes analyzed via database and manual chart
reviews N = 377 Of these 56 patients had incomplete data (transferred
out, lost to follow-up, insufficient laboratory data) Preliminary data analyzed for remaining 321
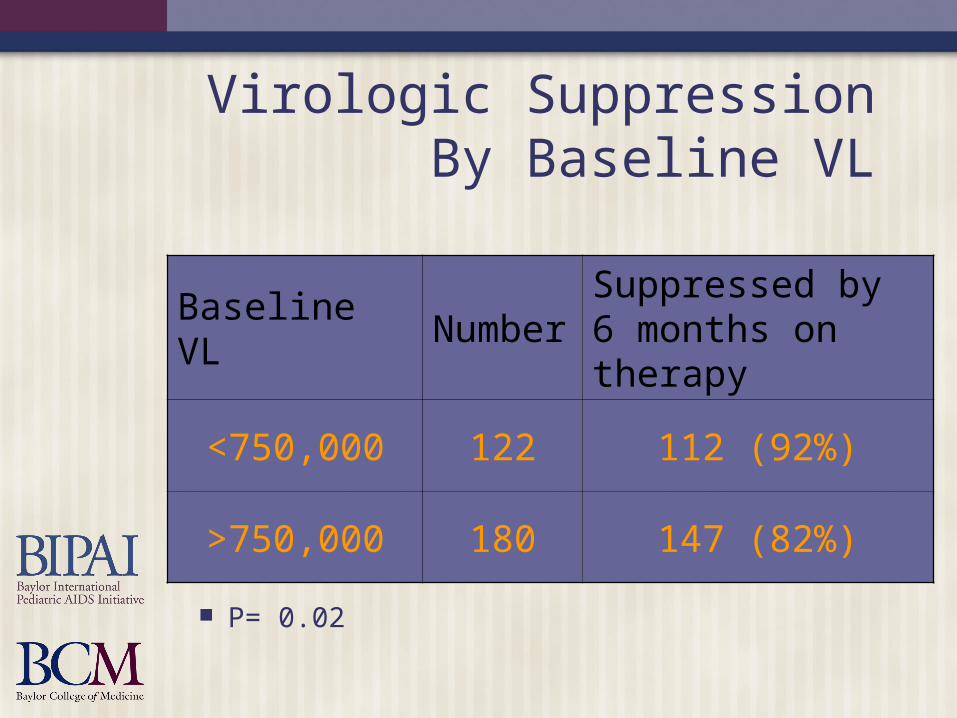
Virologic SuppressionBy Baseline VL
Baseline VL NumberSuppressed by 6 months on therapy
<750,000 122 112 (92%)
>750,000 180 147 (82%)
P= 0.02
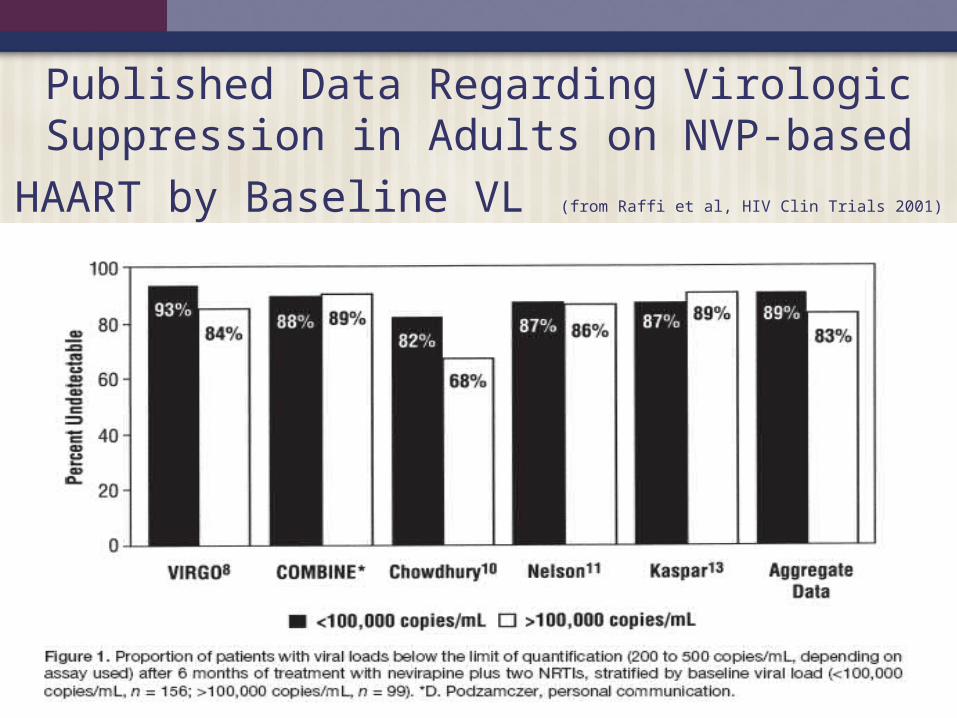
Published Data Regarding Virologic Suppression in Adults on NVP-based HAART by Baseline VL
(from Raffi et al, HIV Clin Trials 2001)
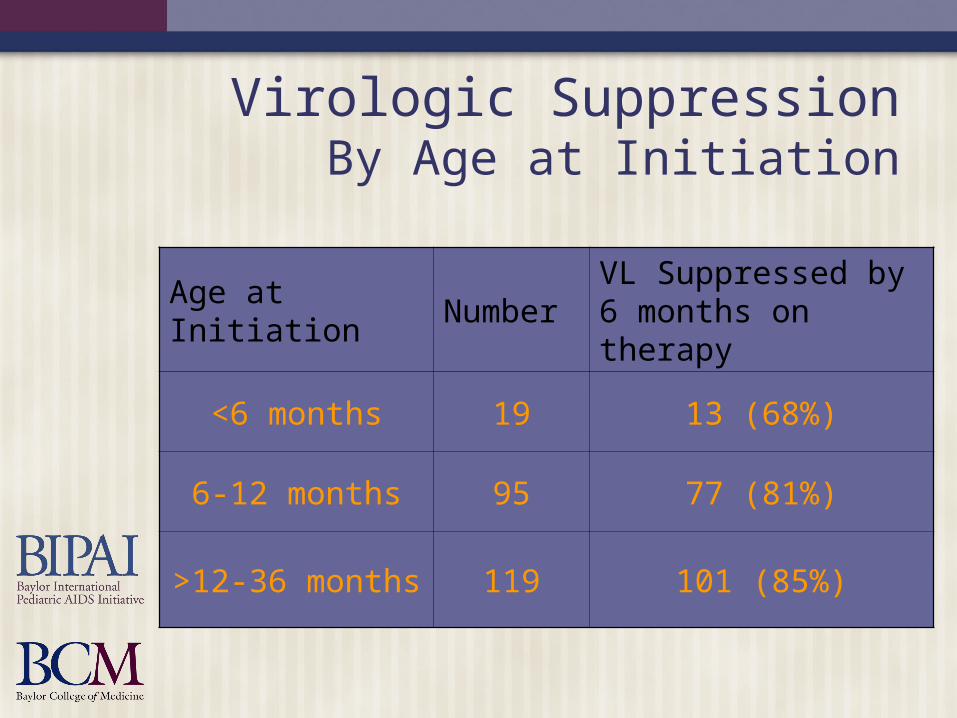
Virologic SuppressionBy Age at Initiation
Age at Initiation NumberVL Suppressed by 6 months on therapy
<6 months 19 13 (68%)
6-12 months 95 77 (81%)
>12-36 months 119 101 (85%)

Since baseline viral load is predictive of virologic failure, can we predict
baseline VL on the basis of age and baseline CD4 count?

Correlation Matriceson BANA2 Trial Patients
Baseline VL >750,000 compared with VL <750,000 with regards to: Age CD4% CD4 absolute count CDC Immunologic category
No statistically significant correlations

Role of PMTCT In Early Infant Outcomes
Standard program is: Maternal AZT started as early as 28 weeks (unless
mother on HAART) sd-NVP to mother sd-NVP to baby at birth 4 weeks of AZT to baby
Mothers rarely know whether sd-NVP was received PMTCT is recorded as:
“yes” - some received “no” - none known to have been received Or “unknown”- not recorded
Based on reported excellent uptake of sd-NVP use by national programme, it is assumed that most children received sd-NVP if some PMTCT is reported

Virologic Suppression Among Children on NNRTI-based 1st line by PMTCT status
112 infants/young children known to have received PMTCT and initiated HAART 85 (76%) achieved a VL<400 on 1st line
187 infants/young children reported to have received no PMTCTand initiated HAART 171 (91%) achieved VL<400 on 1st line
P=0.0003

Virologic Suppression Among Children on NNRTI-based 1st Line by PMTCT Status and Age at Initiation
15 patients initiated HAART at <6 months of age with a follow-up VL confirming virologic suppression (VL <400 copies/ml) or non-suppression at or after 6 months on HAART 10 (67%) suppressed
59 patients initiated HAART between 6 and 12 months of age with a follow-up VL confirming virologic suppression (VL<400 copies/ml) at or after 6 months on HAART 44 (75%) suppressed
P=0.53

No difference between outcomes among patients who initiated before 6 months and after 12 months
15 patients initiated HAART at <6 months of age with a follow-up VL confirming virologic suppression (VL <400 copies/ml) or non-suppression at or after 6 months on HAART 10 (67%) suppressed
42 patients initiated HAART between 1 and 3 years of age with a follow-up VL confirming virologic suppression (VL<400 copies/ml) at or after 6 months on HAART 34 (81%) suppressed
P=0.29

Limitations of Data
Retrospective analysis PMTCT status listed as “yes” or “no” and
may not necessarily be reflective of sd-NVP status
Missing data

Benefits vs. Risks: Early HAART Initiation
A recent chart review of 281 children who initiated HAART >2 years ago at age <3 years at the COE 235 confirmed alive 46 confirmed dead (16%)
93 were CDC category C3 at initiation 66 confirmed alive 27 confirmed dead (29%)
Benefit: children are more likely to live if you initiate HAART before they are very sick and immune suppressed
Note: Because we have liberal initiation criteria, we do not have a comparison of death rates among untreated children

Benefits vs. Risks: Adverse Drug Reactions 1
The charts of the first 110 treatment naïve children who had received HAART at the COE for >52 w were reviewed for ADRs: Mean age = 70 m; Male: female = 1:1 106 (96%) received ZVD+3TC+NVP
4 with Hb<7.5 g/dl received d4T in lieu of ZVD Median VL/CD4% were 310,000/15% 44 (40%) were in CDC immune category 3 Median Hb was:
9.4 g/dl in patients < 24 m 10.6 g/dl in those > 24 m

Benefits vs. Risks: Adverse Drug Reactions 2
Overall Median Hb increased by 52 w: 9.4 to 10.4 among those aged <24 m 10.6 to 11.2 g/dl in those aged >24 m
Median ALT unchanged at 19.0±0.5 u/L over 52 weeks
ADR occurred in 23 (21%) patients: Rash in 17 (74%) Severe anemia (Hb <3 g/dl) in 3 (13%) Vomiting in 3 (13%)

Benefits vs. Risks: Adverse Drug Reactions 3
Rash occurred in first three weeks of therapy: 16/17 (94%) were mild or moderate 1 had Steven’s-Johnson syndrome requiring inpatient
care Severe anemia developed at 3 m in one and at 4 m
in 2 patients All were transfused and switched from ZVD to d4T
Vomiting was mild and resolved without therapy Grade 3 lipase toxicity developed in 2 patients
Subsequently normalized without further intervention Conclusion: HAART in naïve African children
using a regimen consisting of ZVD or d4T + 3TC + NVP was both generally safe and well tolerated.